")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Clinical Relevance of Profilin Sensitization Concerning Oral Allergy Syndrome in Birch Pollen Sensitized Patients
Authors Högerle C , San Nicolo M, Gellrich D, Eder K, Gröger M
Received 9 November 2021
Accepted for publication 16 January 2022
Published 19 February 2022 Volume 2022:15 Pages 249—255
DOI https://doi.org/10.2147/JAA.S348650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Catalina Högerle, Marion San Nicolo, Donata Gellrich, Katharina Eder, Moritz Gröger
Department of Otorhinolaryngology, Head and Neck Surgery, Ludwig-Maximilians-University Munich, München, Germany
Correspondence: Catalina Högerle, Department of Otorhinolaryngology, Head and Neck Surgery, Ludwig-Maiximilians-Universität München, Marchioninistr. 15, München, D- 81377, Germany, Tel +49 89 4400 73892, Fax +49 89 4400 76892, Email [email protected]
Purpose: Many plant food allergens contain homologs to the major birch allergen Bet v 1; therefore, the majority of patients with birch pollen allergy suffer from oral allergy syndrome. We studied the relevance of sensitization of Bet v 1 and co-sensitization with profilin concerning the clinical manifestations of an oral allergy syndrome.
Patients and Methods: A total of 1119 patients with a positive skin prick test to birch and diagnostic for specific IgE to the allergen components Bet v 1 and profilin were analyzed retrospectively regarding complaints in the upper and lower airways, with demographic data as well as oral and gastrointestinal allergy symptoms.
Results: Patients with simultaneous specific IgE to the allergen components Bet v 1 and profilin have to deal more often with an oral allergy syndrome and intestinal reactions. They also suffer more frequently and severely from rhinitis symptoms and show a higher tendency for asthma. No increased number of systemic reactions was seen.
Conclusion: Patients with birch allergy recognizing both allergens have more probabilities of suffering from an oral allergy syndrome, and allergologists should be aware of this in order to give better advice to their patients.
Keywords: oral allergy syndrome, clinical relevance of allergens, birch pollen sensitization, profilin co-sensitization, component resolved diagnostic
Introduction
Oral allergy syndrome (OAS) has been clinically recognized as a unique presentation of food allergy for more than 80 years and remains a significant diagnostic and therapeutic challenge to both practicing and research allergologists.1–3 OAS represents the most common food allergy in adults, with a prevalence in patients with pollen allergies ranging from 9.6% to 55% worldwide.4 Symptoms of OAS are usually limited to the oropharyngeal area and occur shortly after ingesting a raw fruit or vegetable.3 Typical symptoms are itching, tingling and/or swelling of the lips, tongue, palate or throat, but also reactions beyond the oral cavity eg laryngeal swelling with dyspnea, eczema, circulatory problems or gastrointestinal complaints may occur. And even though considered rare, severe reactions have also been reported, including anaphylaxis in up to 1.7% as stated in a survey by Ma et al.3,5 OAS is caused by an IgE cross-reactivity between an aeroallergen and a characteristically similar plant-derived protein like the pathogenesis-related or pathogen response (PR) proteins (eg PR-10).3 A key member of the PR-10 family is the major birch tree allergen Betula verrucosa (Bet v 1). Another cause of OAS was uncovered when Valenta et al cloned and identified a novel birch allergen, Bet v 2.6 Bet v 2 was found in patients with and without birch allergy and led to the realization that a larger, non-PR-related protein family was capable of causing OAS: the profilins. Profilins are panallergens, present in almost all eukaryotic cells and responsible for cross-reactivity between pollen, latex and plant foods, and considered to be an important confounding factor in extract-based diagnosis.7 Profilin food allergy is thus considered to be a secondary effector of primary respiratory allergic disease.8,9 It is known that around 70% of birch allergic individuals develop allergic symptoms against certain foods containing homologous cross-reactive allergens to the major birch allergen Bet v 1.10–12 Still, the clinical relevance of sensitization to Bet v 1 versus co-sensitization to Bet v 1 and profilin concerning OAS remains unclear. The aim of this study was to analyze the relationship between oral allergy syndromes and the specific IgE pattern towards Bet v 1 and profilin in patients with positive skin prick test (SPT) to birch. Further, we questioned whether component-resolved diagnostics might add a benefit to the clinical diagnosis of OAS.
Materials and Methods
The Department of Oto-Rhino-Laryngology, Head&Neck Surgery of the Ludwig-Maximilians-University in Munich runs an anonymized allergy database that contains all patient information and diagnostic results. We retrospectively scanned this database for patients who had a positive skin prick test (SPT) to birch between September 2002 and April 2018. A total of 1148 patients had received diagnostics for specific IgE to the allergen components Bet v 1 and profilin (Bet v 2 and/or Phl p 12). Based on the serological pattern, we divided the patient collective into the following groups: Bet v 1 positive and profilin negative (group A, n=800 patients), Bet v 1 positive and profilin positive (group B, n=121 patients), as control group Bet v 1 negative and profilin negative (group C, n=198 patients) and Bet v 1 negative and profilin positive (group D, n=29). As we wanted to have a look at the relevance of profilin in context of birch pollen allergic patients, individuals with characteristics “Bet v 1 -/profilin +” were not informative in our context, and therefore this group was not analyzed. The final study cohort included 1119 patients.
For SPT the solutions by ALK-Abelló, Wedel, Germany had been used. We had performed SPT to birch, hazel, alder, ash, timothy grass, rye, mugwort, pellitory, ragweed, Dermatophagoides pteronyssinus, Dermatophagoides farinae, dog, cat, Alternaria and Aspergillus. The SPT has been considered positive with a wheal ≥3 mm in diameter (divided into the following categories: ≥3 to 4 mm; ≥4 to 5 mm; ≥5 to 6; ≥6 mm) in combination with histamine dihydrochloride solution at 1 mg/mL as positive control and allergen-free saline solution as negative control, read 20 min after application.13,14 The procedure and classification were in line with European standards and published guidelines.13,14 The FEIA (fluorescence enzyme immunoassay) method was used to detect IgE reactivity to allergen components Bet v 1 and profilin (Bet v 2 and/or Phl p 12) with a commercially available test kit (UniCAP, Thermo Fisher Scientific, Freiburg, Germany). All procedures were in accordance with the manufacturer'́s instructions. Results were reported as concentrations (kU/L).
Further, the medical history was registered, partially by a standardized clinical history questionnaire containing demographic data, living environment, complaints of the upper and lower airways, gastrointestinal symptoms and oral allergy symptoms. The clinical symptoms were assessed by a standardized questionnaire (an extended version of the standardized German adapted version of the Rhinoconjunctivitis Quality of Life Questionnaire by Juniper). Oral allergy syndrome was verified by means of case history only by using a standardized interview. We documented patient-reported immediate adverse reactions after ingestion of plant foods. Overall, the following fields of interest were interrogated: diagnosis from the allergic symptom complex, general experience with food, reactions to food, allergic rhinitis and atopic comorbidities (Table 3).
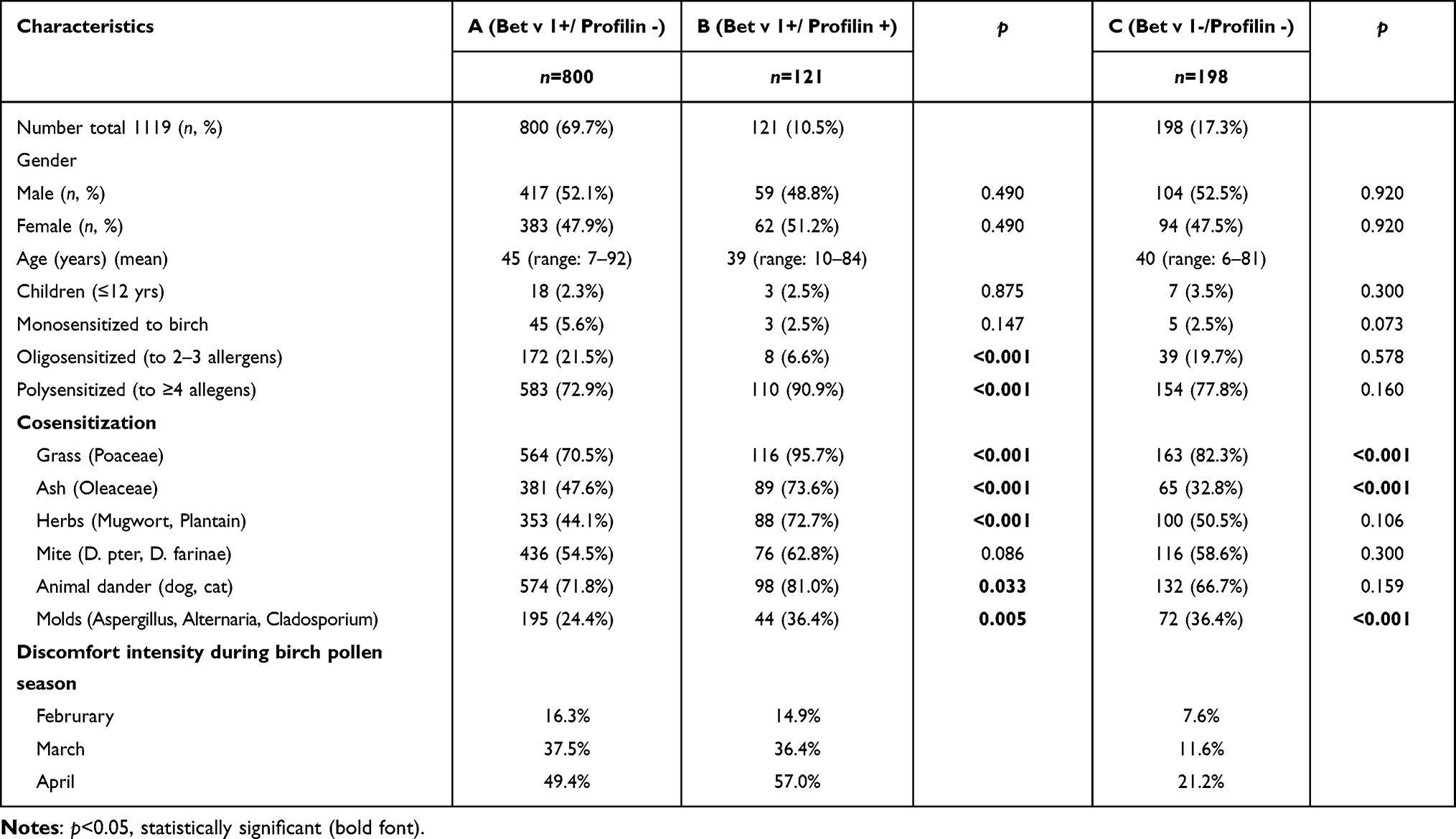 |
Table 1 Demographic and Clinical Data of the Three Study Groups |
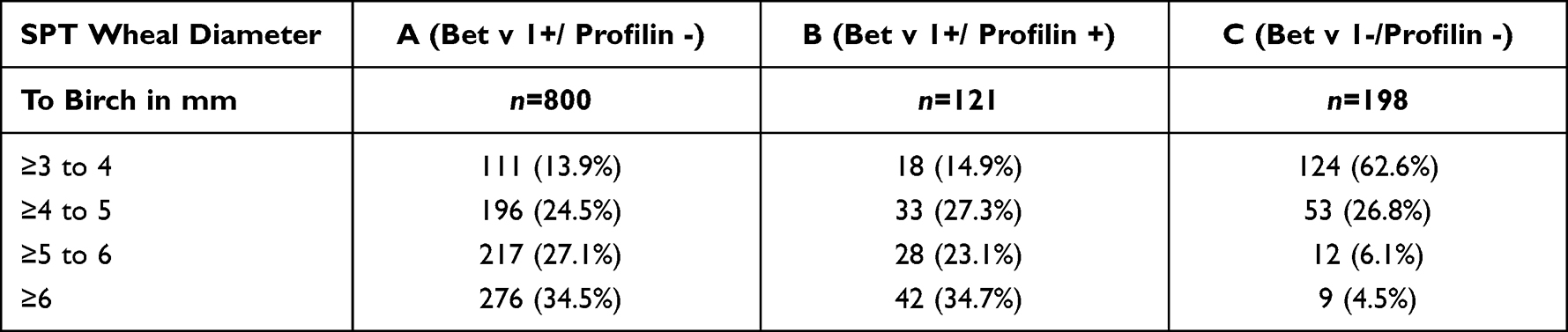 |
Table 2 SPT Values to Birch in the Study Cohort |
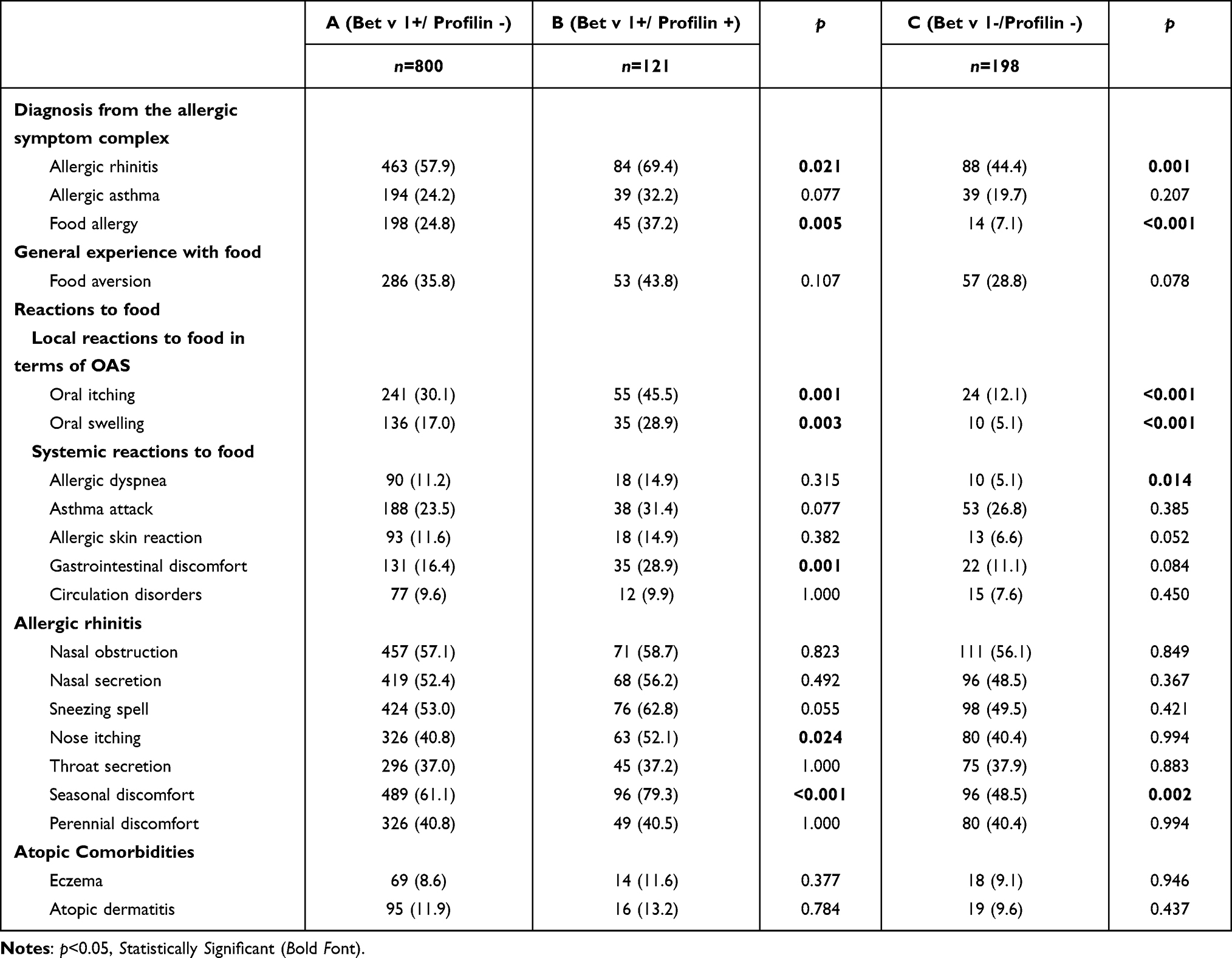 |
Table 3 Reported Clinical Manifestations of Symptoms of the Study Population Group A Compared to Group B and C (Percentage in Parentheses) |
The present study has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All patients provided written informed consent for the use of their anonymized data for scientific research and gave consent to publish these results. The ethics committee of the medical faculty of the Ludwig-Maximilians-University Munich has exempted this study from requiring ethical approval (project number 21–1019 KB) due to the use of already in clinical routine acquired fully anonymized data.
Statistical analysis was performed using R, version 3.5.1 (R Core Team (2018), Vienna, Austria) and Excel (Microsoft, Redmond, WA, USA). The parametric Pearson’s chi-square test was utilized for testing statistically significant differences between the groups. A p-value of <0.05 was considered significant.
Results
The database query with the above-mentioned inclusion criteria resulted in 1119 patients. Table 1 summarizes the demographic and clinical data of the study population. The three groups are very comparable with regard to demographic aspects – with a well-balanced gender distribution and age range, including a similar percentage of children under 12 years. In terms of the SPT wheal diameters to birch, groups A and B were comparable, whereas group C showed some differences (Table 2). Regarding mono-, oligo- and poly-sensitization (Table 1), group A contained more than twice as many mono-sensitized patients as the other groups. Group B only showed around one-third of oligo-sensitized and a much higher number of poly-sensitized patients compared to similar results in groups A and C. The discomfort intensity during tree pollen season increased in all groups from February to April (Table 1).
The results of reported clinical manifestations of allergies and allergic symptoms are shown in Table 3. Comparing groups A and B, there is a statistically significant difference concerning the incidence of local symptoms of an OAS including oral itching, oral swelling and of the systemic symptoms gastrointestinal discomfort in favor of group B, whereas there was no statistically significant difference in the incidence of systemic reactions to food in in terms of anaphylactic symptoms as circulation disorders, dyspnea and skin reactions. Concerning diagnosis from the allergic symptom complex, food allergy and allergic rhinitis were statistically significantly more frequent in group B; looking at allergic rhinitis symptoms in detail, nose itching and seasonal discomfort were reported significantly more frequently among the patients in group B. In concordance with significantly more symptoms reported in group B, the rate of realized allergen-specific immunotherapy was statistically higher in group B (n=53 of 121, 43.80%) compared to group A (n=217 of 800, 27.13%; p<0.001). In spite of this result, patients assessed the positive outcome of their hyposensitization similarly (group B: n=18 of 121 (33.96%); group A, n=73 of 273 (33.64%)).
Patients from group A compared to the control group (group C) also suffered statistically significantly more often from OAS symptoms, such as oral itching and oral swelling, and diagnosis from the allergic complex, such as allergic rhinitis and food allergy. Regarding anaphylactic symptoms, patients from group A seem to be more frequently affected; however, only concerning dyspnea was a statistically significant difference to group C revealed. In terms of rhinitis symptoms, group A mentioned statistically significantly more often seasonal discomfort. An equal number of realized hyposensitization (group A: n=217 of 800, 27.13%; group C: n=40 of 198, 20.20%), and positive outcome of hyposensitisation (group A: n=73 of 273, 26.74%; group C: n=13 of 40, 32.50%) was also reported by group A when compared to group C.
The top three triggers of the OAS in groups A and B were the same foods, with nuts as number one trigger followed by apple and stone fruits. Among patients in group C, the most frequent triggers of oral allergy syndrome symptoms were also nuts but were followed by stone fruits (peach, cherry, nectarine, apricot, plum or yellow plum), carrot and kiwi (Table 4).
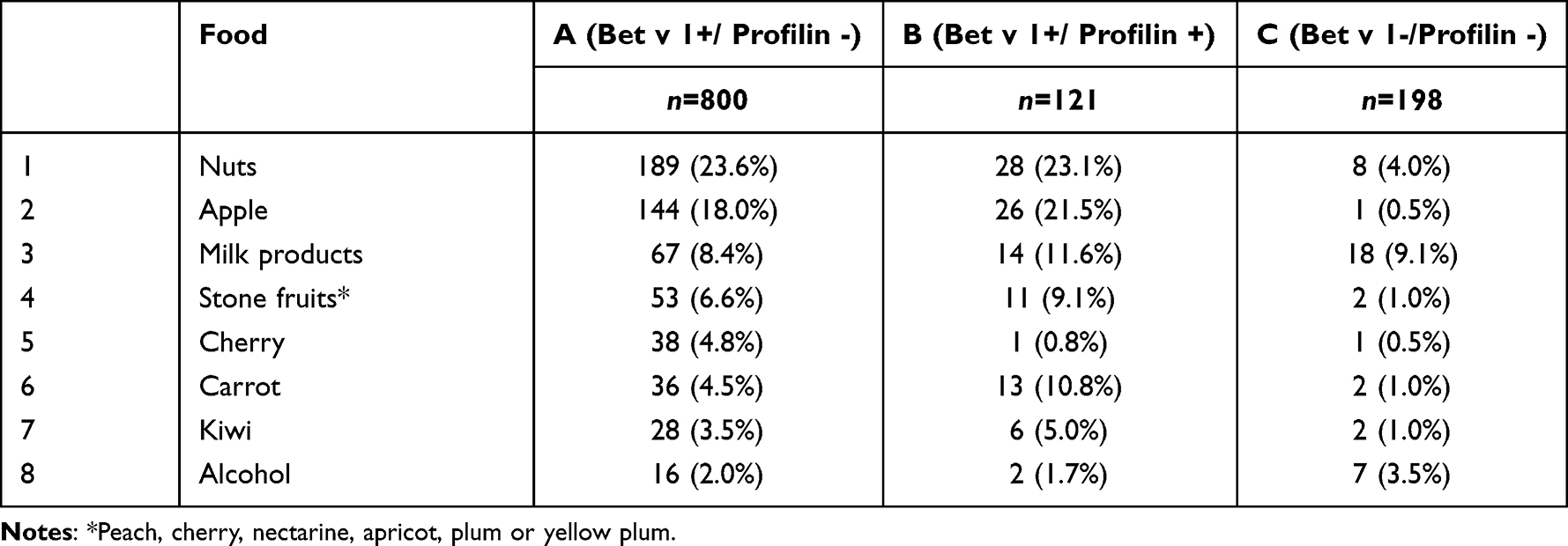 |
Table 4 Ranked Triggers of Oral Allergy Syndrome in This Cohort |
Discussion
Profilin sensitization seems to be on the rise, as shown by a more recent study that found a prevalence of 30% among an unselected population of pollen-allergic adults, and as suggested also by the markedly increasing prevalence of patients showing multiple pollen sensitization in in vivo or in vitro routine diagnostic tests.15,16 Overall, these recent findings highlight the importance of testing for profilin in patients showing pollen sensitization in order to understand more about its clinical relevance.15,16 Although there are several studies comparing the serological pattern of patients in regard to Bet v 1 and profilin, to the best of our knowledge there are no specific studies about the effect of an additional profilin sensitization concerning OAS symptoms.17–19
Patients sensitized to birch with specific IgE to the allergen components Bet v 1 and profilin were more frequently affected by mucosal reactions through foods in terms of local (oral itching and oral swelling) and intestinal reactions. To evaluate the patient's individual risk of a severe reaction in terms of a systemic anaphylaxis we analyzed the incidence of systemic reactions. Systemic anaphylactic reactions, however, did not occur more often in this group. This result leads to new knowledge that in our opinion is important in terms of consulting patients after having diagnosed a birch pollen sensitization with positive Bet v 1 and profilin.
Further, these patients suffered more frequently and severely from rhinitis symptoms and showed a higher tendency of developing asthma compared to birch-sensitized patients without IgE reactivity towards profilin. This is congruent to other recent studies eg from Ruiz-Hornillos et al who found in a prospective case-control study that sensitization to profilin seems to be a marker of severity in patients with rhinoconjunctivitis and asthma mediated by pollen.20 Previous observations also have suggested the importance of profilin as a marker of evolution and early marker of asthma severity which is in accordance to our results with a higher rate of self-reported asthma among patients sensitized to profilin.16,21,22
In order to give an even more detailed recommendation to our patients, we also took an explicit look into the food categories that provoked an oral allergy syndrome. Patients belonging to groups A and B reported as the three main food triggers nuts, apple and stone fruit. In group C food triggers were reported rarely; mentioned were mainly nuts followed by stone fruit, carrot and kiwi. This finding is in accordance to the molecular association concerning cross-reactivity to homologous proteins described by Worm et al.23
With regard to allergen-specific immunotherapy, the panallergen-positive group had a significantly higher hyposensitization rate and higher success rate, which proves acceptable to us because of their higher psychological strain, having more frequent and more severe symptoms.
Although our data do not allow a conclusion whether profilin sensitization is a marker for a more severe and complex allergic disease or a causal factor by itself, it appears probable that profilin sensitization might play a more important role in the severity of allergic symptoms, especially in OAS caused by birch sensitization, than generally supposed. Consequently, component-resolved diagnostics might be a helpful diagnostic tool in terms of oral allergy syndrome to better advise birch-sensitized patients concerning their expected perspectives and limitations of their allergy and potential treatment options.
However, there are certain limitations to our study. It is retrospective, and information on clinical manifestations of allergic symptoms in the study population were based on a questionnaire and, therefore, exposed to potential recall bias and over-reporting. In addition, asthma and OAS could not be confirmed by lung tests and double-blind, placebo controlled food challenges because data used in this study had been collected during the routine practice in our outpatient clinic. Furthermore, it did not take into consideration the profile of sensitization to the most relevant foods.
Conclusion
Since the first case report, OAS has been a challenging diagnosis to the practicing allergologists because of its many clinical, diagnostic and therapeutic considerations. Our data show that patients with birch allergy recognizing the allergens Bet v 1 and profilin have greater probability of suffering from an oral allergy syndrome, and allergologists should be aware of this in order to give better advice to their patients.
Abbreviations
OAS, oral allergy syndrome; SPT, skin prick test; HDM, house dust mite; FEIA, fluorimetric enzyme-linked immunoassay.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank the medical technician staff of the Department of Otorhinolaryngology of the Ludwig-Maximilians-University in Munich, Gabriele Bärr and Elisabeth Pfrogner, and also Dominik Steubl for statistical analysis support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
No potential conflict of interest was reported by the authors. There was no financial support for this study.
References
1. Salén EB, Juhlin-Dannfelt C. Über das Vorkommen von sogen. latenter Allergie; Gleichzeitig einige Gesichtspunkte über gewisse prinzipiell bedeutungsvolle Allergieprobleme. [About the occurrence of so-called latent allergies; at the same time, some aspects about certain allergy problems that are important in principle]. J Intern Med. 1935;86(5–6):505–569.
2. Thompson JC, Kroker GF. The role of component-resolved testing in food allergy and oral allergy syndrome. Ann Allergy Asthma Immunol. 2010;104(6):
3. Webber CM, England RW. Oral allergy syndrome: a clinical, diagnostic, and therapeutic challenge. Ann Allergy Asthma Immunol. 2010;104(2):101–108. doi:10.1016/j.anai.2009.11.007
4. Kondo Y, Urisu A. Oral allergy syndrome. Allergol Int. 2009;58(4):485–491. PMID: 19847095. doi:10.2332/allergolint.09-RAI-0136
5. Ma S, Sicherer SH, Nowak-Wegrzyn A. A survey on the management of pollen-food allergy syndrome in allergy practices. J Allergy Clin Immunol. 2003;112(4):784–788. PMID: 14564362. doi:10.1016/s0091-6749(03)02008-6
6. Valenta R, Duchêne M, Pettenburger K, et al. Identification of profilin as a novel pollen allergen; IgE autoreactivity in sensitized individuals. Science. 1991;253(5019):557–560. doi:10.1126/science.1857985
7. Wensing M, Akkerdaas JH, van Leeuwen WA, et al. IgE to Bet v 1 and profilin: cross-reactivity patterns and clinical relevance. J Allergy Clin Immunol. 2002;110(3):435–442. doi:10.1067/mai.2002.126380
8. Thorn KS, Christensen HE, Shigeta R, et al. The crystal structure of a major allergen from plants. Structure. 1997;5(1):19–32. PMID: 9016723. doi:10.1016/s0969-2126(97)00163-9
9. Fedorov AA, Ball T, Mahoney NM, et al. The molecular basis for allergen cross-reactivity: crystal structure and IgE-epitope mapping of birch pollen profilin. Structure. 1997;5(1):33–45. PMID: 9016715. doi:10.1016/s0969-2126(97)00164-0
10. Biedermann T, Winther L, Till SJ, et al. Birch pollen allergy in Europe. Allergy. 2019;74(7):1237–1248. PMID: 30829410. doi:10.1111/all.13758
11. Geroldinger-Simic M, Zelniker T, Aberer W, et al. Birch pollen-related food allergy: clinical aspects and the role of allergen-specific IgE and IgG4 antibodies. J Allergy Clin Immunol. 2011;127(3):616–22.e1. PMID: 21251701. doi:10.1016/j.jaci.2010.10.027
12. Matricardi PM, Kleine-Tebbe J, Hoffmann HJ, et al. EAACI molecular allergology user’s guide. Pediatr Allergy Immunol. 2016;27(Suppl 23):1–250. PMID: 27288833. doi:10.1111/pai.12563
13. Bousquet PJ, Burbach G, Heinzerling LM, et al. GA2LEN skin test study III: minimum battery of test inhalent allergens needed in epidemiological studies in patients. Allergy. 2009;64(11):1656–1662. PMID: 19824887. doi:10.1111/j.1398-9995.2009.02169.x
14. Dreborg S. The skin prick test in the diagnosis of atopic allergy. J Am Acad Dermatol. 1989;21(4):820–821. PMID: 2689475. doi:10.1016/s0190-9622(89)70256-5
15. Asero R, Monsalve R, Barber D. Profilin sensitization detected in the office by skin prick test: a study of prevalence and clinical relevance of profilin as a plant food allergen. Clin Exp Allergy. 2008;38(6):1033–1037. doi:10.1111/j.1365-2222.2008.02980.x
16. Asero R, Tripodi S, Dondi A, et al. Prevalence and clinical relevance of IgE sensitization to profilin in childhood: a Multicenter Study. Int Arch Allergy Immunol. 2015;168(1):25–31. doi:10.1159/000441222
17. Ortolani C, Ispano M, Pastorello EA, et al. Comparison of results of skin prick tests (with fresh foods and commercial food extracts) and RAST in 100 patients with oral allergy syndrome. J Allergy Clin Immunol. 1989;83(3):683–690. doi:10.1016/0091-6749(89)90083-3
18. Ebner C, Hirschwehr R, Bauer L, et al. Identification of allergens in fruits and vegetables: igE cross-reactivities with the important birch pollen allergens Bet v 1 and Bet v 2 (birch profilin). J Allergy Clin Immunol. 1995;95(5):962–969. doi:10.1016/S0091-6749(95)70096-X
19. Pauli G, Oster JP, Deviller P, et al. Skin testing with recombinant allergens rBet v 1 and birch profilin, rBet v 2: diagnostic value for birch pollen and associated allergies. J Allergy Clin Immunol. 1996;97(5):1100–1109. doi:10.1016/S0091-6749(96)70264-6
20. Ruiz-Hornillos J, López-Matas MA, Berges Jimeno P, et al. Profilin is a marker of severity in allergic respiratory diseases. Allergy. 2020;75(4):853–861. doi:10.1111/all.14140
21. Barber D, de la Torre F, Feo F, et al. Understanding patient sensitization profiles in complex pollen areas: a molecular epidemiological study. Allergy. 2008;63(11):1550–1558. doi:10.1111/j.1398-9995.2008.01807.x
22. Alvarado MI, Jimeno L, De La Torre F, et al. Profilin as a severe food allergen in allergic patients overexposed to grass pollen. Allergy. 2014;69(12):1610–1616. doi:10.1111/all.12509
23. Worm M, Jappe U, Klein-Tebbe J, et al. Food allergies resulting from immunological cross-reactivity with inhalant allergens: guidelines from the German Society for Allergology and Clinical Immunology (DGAKI), the German Dermatology Society (DDG), the Association of German Allergologists (AeDA) and the Society for Pediatric Allergology and Environmental Medicine (GPA). Allergo J Int. 2014;23(1):1–16. doi:10.1007/s40629-014-0004-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.