")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Clinical relevance of paliperidone palmitate 3-monthly in treating schizophrenia
Authors Mathews M, Gopal S , Nuamah I, Hargarter L , Savitz AJ, Kim E , Tan W , Soares B, Correll CU
Received 6 December 2018
Accepted for publication 2 April 2019
Published 21 May 2019 Volume 2019:15 Pages 1365—1379
DOI https://doi.org/10.2147/NDT.S197225
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Maju Mathews,1 Srihari Gopal,1 Isaac Nuamah,1 Ludger Hargarter,2 Adam J Savitz,1 Edward Kim,3 Wilson Tan,4 Bernardo Soares,5 Christoph U Correll6–8
1Department of Neuroscience, Janssen Research & Development, LLC, Raritan, NJ, USA; 2Department of Neuroscience, Janssen-Cilag EMEA, Neuss, Deutschland; 3Janssen Scientific Affairs, LLC, Hopewell, NJ, USA; 4Regional Medical Affairs, Janssen Pharmaceutical Companies of Johnson and Johnson, Singapore; 5Neuroscience Medical Affairs, Janssen-Cilag, High Wycombe, Buckinghamshire, UK; 6The Zucker Hillside Hospital, Psychiatry Research, Glen Oaks, NY, USA; 7Department of Psychiatry and Molecular Medicine, Hofstra Northwell School of Medicine, East Garden City, NY, USA; 8Department of Child and Adolescent Psychiatry, Charité Universitätsmedizin, Berlin, Germany
Abstract: Antipsychotics are the mainstay in schizophrenia management, and long-acting injectable (LAI) antipsychotics contribute to the successful maintenance of treatment by improving non-adherence and preventing relapses. Paliperidone palmitate 3-monthly (PP3M) formulation is the only available LAI antipsychotic that offers an extended 3-month window of stable plasma drug concentration, enabling only four injections per year. This paper summarizes clinically relevant endpoints from available evidence for PP3M to bridge translational research gaps and provide measurable outcomes that can be interpreted in clinical practice. Low number-needed-to-treat (NNT) for relapse prevention (NNT [95% CI] 6-month estimate: 4.8 [3.2; 10.0]; 12-month estimate: 3.4 [2.2; 7.0]), and high number-needed-to-harm (NNH [95% CI] akathisia, 27.1 [12.3; −667.1]; tremor, 80.0 [22.5; 67.3]; dyskinesia, −132.6 [44.5; −23.2]; parkinsonism, 160.0 [28.9; −49.8]) quantify the relative benefits and low propensity for adverse events with PP3M. Symptom remission and reductions in positive and negative symptoms indicate treatment stability. Additionally, meaningful functional remission, reduced dosing frequency, and freedom from daily negotiations favorably impact patient preference and attenuate burdensome aspects of caregiving, representing important healthcare determinants that enhance prospects of treatment continuity in schizophrenia. This information can potentially improve clinicians’ judgment of treatment choices, clinical response, and patient selection in routine care. Taken together, PP3M is a valuable antipsychotic treatment option, meriting consideration for a broader role in the long-term management of schizophrenia; its utility should not be limited to patients with poor adherence or when oral antipsychotics have failed.
Keywords: number-needed-to-harm, number-needed-to-treat, paliperidone palmitate 3-monthly, remission
Introduction
Schizophrenia is a complex psychiatric disorder with a variable trajectory of symptomatic status that may include stabilization, remission, relapse, deterioration, or total incapacitation.1,2 Clinical studies evaluating antipsychotics for schizophrenia are replete with data; however, discerning the data in a clinically useful way is often difficult.3 Assessment of antipsychotics using valid indicators of treatment effects would assist clinicians and psychiatrists with robust, reliable, and comparative data for making treatment decisions.4 Such indicators would include perceptible symptomatic and functional improvements or treatment differences, risk–benefit balance, and factors influencing patient’s and caregiver’s well-being that are not merely based on statistical significance and would reinforce the utility of antipsychotics in routine clinical practice.5
Non-adherence or gaps in antipsychotic use increase the odds of relapse, hospitalization, and suicidal attempts, and restrict translation of putative treatment benefits of antipsychotics in real-world clinical practice.6–10 Partial adherence (<80%) has been directly correlated with risk of hospitalization, and a gap of 1–10 days in oral antipsychotic (OAP) treatment coverage has been shown to increase the odds of hospitalization (odds ratio [OR]=1.98).11,12 Long-acting injectable (LAI) antipsychotics facilitate adherence by reducing dosing frequency, offering reliable medication delivery, stable pharmacokinetics, and allowing regular monitoring of dose administration.13
Paliperidone, the major active metabolite of the second-generation antipsychotic (SGA) risperidone, is a centrally-active antagonist of the D2 and 5HT2A receptors.14 Paliperidone extended-release (ER), the oral formulation (approved in 2006), has demonstrated efficacy with improvements in symptom control, patient functioning, and relapse prevention in several randomized-controlled trials (RCTs) conducted to date.15–18 Its first LAI formulation, paliperidone palmitate once-monthly (PP1M), allows once-monthly administration, thereby improving prospects for medication adherence, and is approved (in 2009) for the treatment of schizophrenia.19 PP1M as deltoid or gluteal injections is available in multiple dosing strengths (25, 50, 75, 100, or 150 mg eq. [corresponding doses in mg paliperidone palmitate: 39 mg, 78 mg, 117 mg, 156 mg, and 234 mg]) for ease of dose titration.14,20 PP1M has shown robust efficacy in attenuating psychotic symptoms, improving functional status, and relapse prevention, along with meaningful reductions in hospitalizations, meriting consideration as a viable choice for schizophrenia management at different stages of illness.21–27 PP1M has also shown efficacy in delaying time-to-relapse for psychotic, depressive, and manic symptoms and improvements in the level of functioning in schizoaffective disorder, and is approved for this indication in some countries.28,29
Pharmacological prospects and clinical experience from the PP1M formulation supported the use of model-based pharmacometric analysis to develop a modified, extended-release LAI formulation of PP, paliperidone palmitate 3-monthly (PP3M), for the maintenance treatment of schizophrenia with only four injections per year.30 The PP3M formulation (approved by the US FDA in 2015 and by the European Medicines Agency in 2016) is indicated for the treatment of schizophrenia; initiation requires clinical stability with at least 4 months of PP1M treatment that allows clinicians to optimize the dose and derive the equivalent PP3M dose (3.5-fold dose multiplier of PP1M) adequate to maintain stable paliperidone exposure.30,31 The available doses for PP3M administered as either deltoid or gluteal injection are 175, 263, 350, and 525 mg eq. (corresponding doses in mg: 273, 410, 546, and 819 mg).31,32 Efficacy and safety data for PP3M have been largely accrued from two phase 3 studies (a placebo-controlled relapse prevention study and a non-inferiority [vs PP1M] study), wherein PP3M has shown favorable clinical outcomes in relapse prevention, symptom remission, and functional recovery.33,34
The purpose of the current paper is to summarize and interpret data for PP3M from the two large controlled trials, focusing on the evaluation of clinically meaningful endpoints and results.33,34 The paper also summarizes empirical evidence for paliperidone ER and PP1M within the context of findings for PP3M.
Studies, evaluations, and definitions
The majority of clinical data for PP3M were derived from the final analyses and multiple post hoc and subgroup analyses of two large RCTs of PP3M.33,34 The first RCT comparing the efficacy and safety of PP3M vs placebo was conducted across 64 centers in eight countries.33 Patients received PP1M during a 17-week open-label (OL) transition phase, received a single dose of PP3M in a 12-week OL maintenance phase, and were randomized (n=305) to PP3M or placebo in the double-blind (DB) treatment phase.33 The second RCT demonstrating the non-inferiority of PP3M vs PP1M was conducted across 199 centers in 26 countries.34 Patients received PP1M during a 17-week OL stabilization phase and were randomized (n=1,016) to PP3M or PP1M in the double-blind (DB) treatment phase.34 A fixed dosing regimen was implemented for PP3M and PP1M in both studies, and the patients did not require any dose adjustments during the span of these studies.33,34 In addition to the findings from these studies, the data were analyzed in the following ways to examine the clinical relevance of PP3M treatment.
Measures of effect sizes (to quantify a clinical response) such as number-needed-to-treat (NNT) and number-needed-to-harm (NNH) were used to indicate the number of patients who will likely need to be treated with the study treatment to benefit, or result in harm, in a single patient more than with placebo, respectively.35–37 NNT was calculated for response of positive and negative symptoms, as well as symptomatic and functional remission; NNH was calculated for overall extrapyramidal symptoms (EPS), headache, weight gain, nasopharyngitis, and use of anticholinergic medications during the DB phase of the study as the reciprocal of the absolute difference in event rates.37 The proportion of patients using anticholinergic medications was used as an indirect measure of clinically relevant EPS-related events.37 To support the NNT calculation for time-to-relapse, the survival probability (based on Kaplan-Meier method) at fixed time points (6 and 12 months) was also calculated. The confidence interval (CI) for NNT for relapse prevention was calculated based on the Altman and Andersen38 method. CIs for NNH were derived based on the Wilson score method using SAS 9.2 (Cary, NC, USA).39 Other measures, such as standardized mean differences (SMD) along with their CIs, were also presented.40
Symptomatic remission was interpreted using the Andreasen et al41 remission criteria, and improvements in functional status were assessed using the validated Personal and Social Performance (PSP) scale.42,43 The Andreasen et al41 remission criteria for schizophrenia exclusively include the symptomatic component and do not necessitate complete absence of symptoms, considering the chronic and relapsing nature of the illness.44 The criteria define symptomatic remission as a rating of no more than mild in four core positive and four core negative symptoms on the Positive and Negative Syndrome Scale (PANSS)45 (P1, G9, P3, P2, G5, N1, N4, N6) that is sustained for ≥6 months.41
The consequences of PP1M and PP3M treatment on caregiver burden were analyzed using pooled data from the two phase 3 studies of PP3M.46 The Involvement Evaluation Questionnaire (IEQ) was used to measure overall caregiver burden and important domains of care.47 The Medication Preference Questionnaire (MPQ) was used to assess the attitude and preference of patients towards PP3M.48
Efficacy and outcomes for PP3M treatment in schizophrenia
Relapse prevention
PP3M significantly delayed the time to first relapse vs placebo (hazard ratio=3.81 [95% CI=2.08; 6.99]; P<0.001).33 As assessed by relapse rates, PP3M was significantly more efficacious than placebo (incidence of relapse: PP3M, 8.8% [14/160]; placebo, 29.0% [42/145]).33 In addition, PP3M was non-inferior to PP1M in terms of relapse rates and relapse-free percentage (incidence of relapse: PP3M, 8.1% [37/458]; PP1M, 9.2% [45/490]; percentage relapse-free: PP3M, 91.2%; PP1M, 90%; difference in relapse-free rate: 1.2% [95% CI=−2.7%; 5.1%]).34
In the placebo-controlled studies, the median time-to-relapse was not estimable for all three paliperidone formulations (Table 1). In an additional assessment, the estimated time point when 15% patients experience a relapse event was longer in paliperidone ER and PP1M vs the respective placebo groups, and non-estimable in the PP3M group. In an indirect comparison of three similarly-designed relapse prevention studies conducted with different formulations of paliperidone, post-withdrawal median time-to-impending-relapse (Table 1) was increased with longer half-life formulations.23 The median time until half of the respective sample had relapsed was 58 days for patients discontinuing paliperidone ER, compared to 172 days after discontinuing PP1M, and 395 days after discontinuing PP3M. Having been on PP3M prior to discontinuation and placebo-substitution showed significant advantages (P<0.0001, pair-wise comparison) compared to PP1M and oral formulations.23 These differences underscore clinical benefits, as the relapse-risk was significantly lower (P<0.001) in patients discontinuing PP LAIs as compared with paliperidone ER, and lower (P<0.001) in patients discontinuing PP3M vs those discontinuing PP1M.23
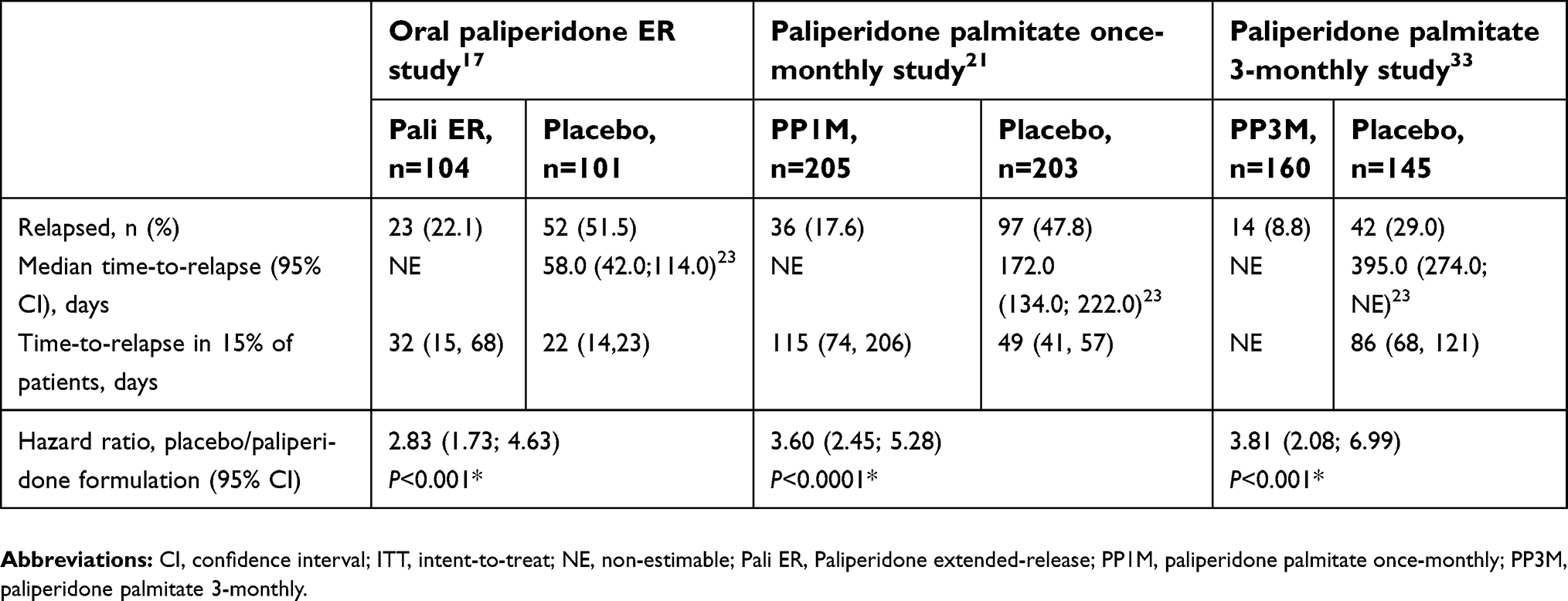 | Table 1 Relapse rates in placebo controlled studies with three formulations of paliperidone (ITT final analysis set) |
PP1M had low NNT (2 to 3), suggesting favorable efficacy for relapse prevention, consistent with the reported relapse prevention efficacy.21,37 The NNT (95% CI) with PP3M for relapse prevention was calculated at two time points (6 and 12 months). At both time points, the NNTs to prevent relapse relative to placebo were low (NNT [95% CI]: 6-month, final analysis=4.8 [3.2; 10.0]; 12-month, final analysis=3.4 [2.2; 7.0]), thus supporting the relapse prevention efficacy from the primary phase 3 study.33,39 The NNTs for PP3M were comparable to PP1M (Table 2).37 Overall, the NNT data imply low risk of relapse with PP3M maintenance treatment in schizophrenia.39
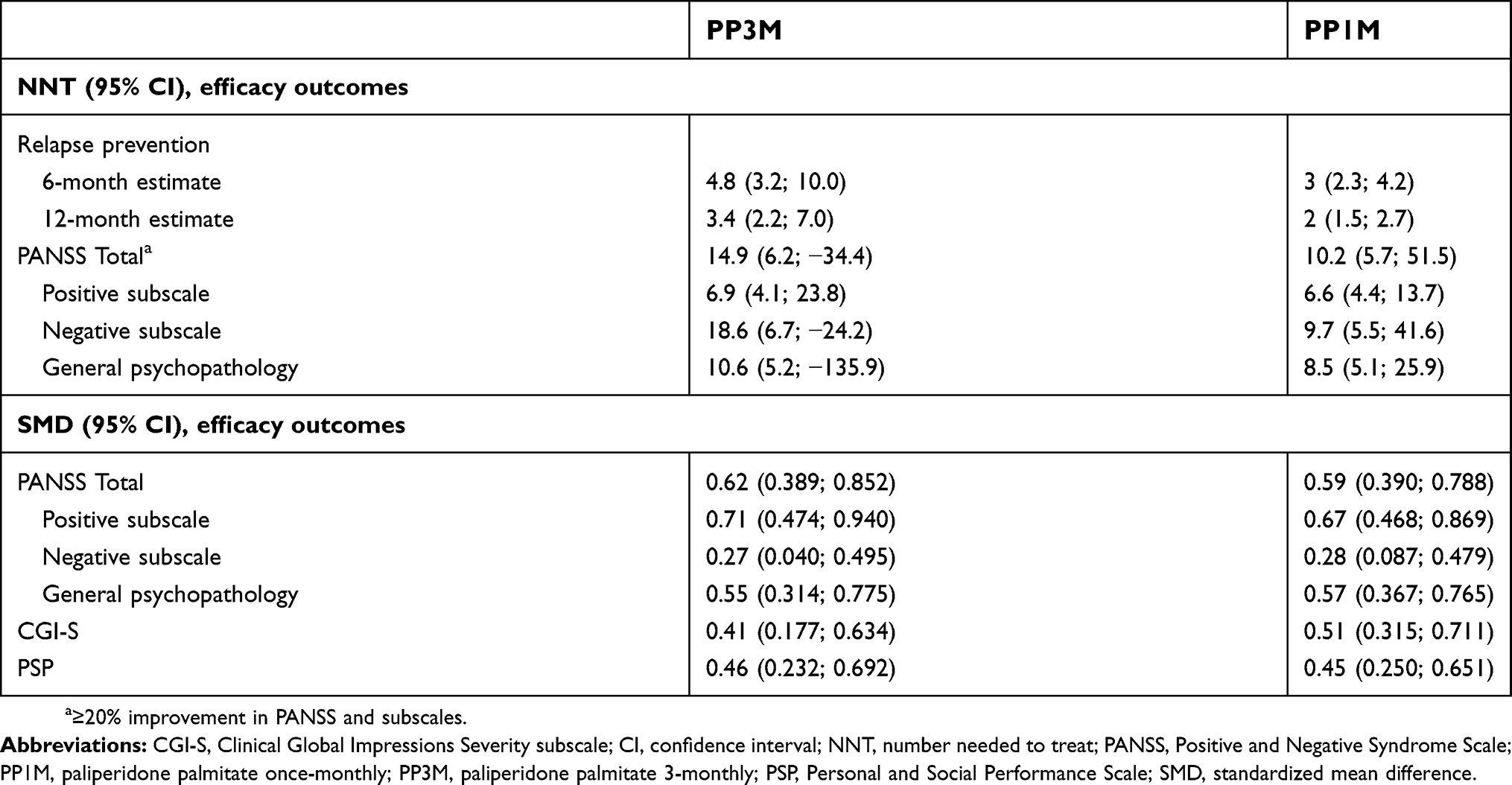 | Table 2 Number needed to treat and standardized mean difference for selected clinical outcomes with different formulations of paliperidone palmitate |
Positive symptoms
In the phase 3 non-inferiority study, improvements in positive and negative symptoms were observed with PP1M treatment during the OL phase that were sustained through the DB phase for both PP1M and PP3M groups (Table 3).34 In the OL phase of the placebo-controlled study, PP1M and PP3M treatment improved positive symptoms. At DB endpoint, PP3M treatment significantly improved (P<0.001) positive symptoms vs placebo.33 Treatment with PP1M has also shown improvements in positive symptoms in patients with recent-onset or chronic schizophrenia, acute schizophrenia, as well as hospitalized patients with exacerbated symptoms.49–53 NNT (95% CI) with PP3M treatment for a minimally important change (percent reduction based on ≥20% improvement) in PANSS positive sub-scale was also low (6.9 [4.1, 23.8]; PP1M: 6.6 [4.4, 13.7]) and the SMD (95% CI) was 0.71 (0.474; 0.940); PP1M: 0.67 (0.468; 0.869) suggesting favorable improvements (Table 2). Overall, these results suggest meaningful improvements in typical psychotic behavior of schizophrenia and potential for clinically meaningful outcomes with PP3M treatment.
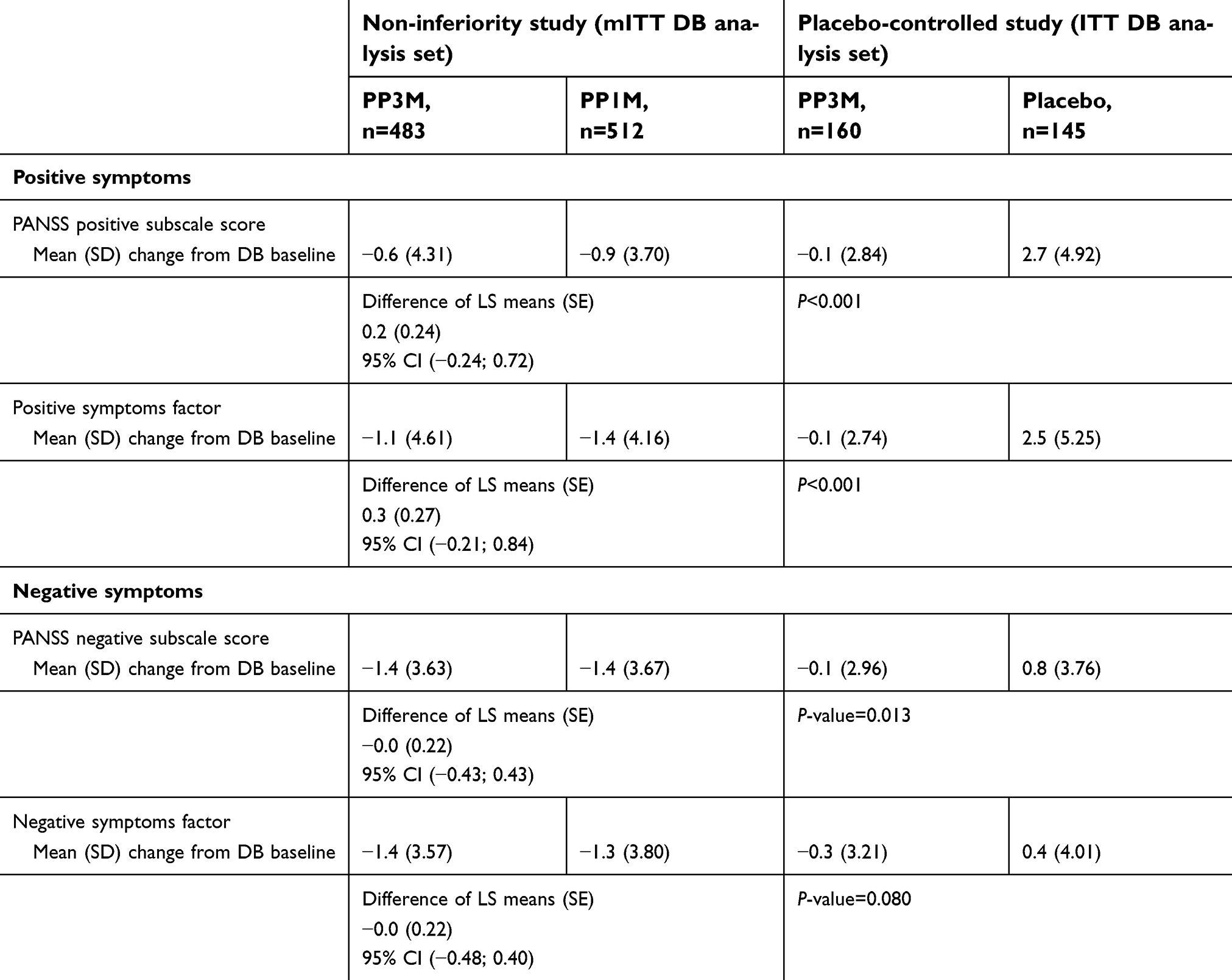 | Table 3 Improvements in positive and negative symptoms from double-blind baseline to double-blind endpoint of phase 3 PP3M studies |
Negative symptoms
In a post-hoc analysis of the phase 3 non-inferiority study of PP3M vs PP1M, the negative subscale and negative symptoms factor scores showed continuous improvements throughout the OL and DB phases of the study.54 The mean (SD) change from baseline in PANSS negative subscale score for PP1M vs PP3M were similar over time (DB baseline to DB endpoint: −1.4 [3.67], R2=0.06 vs −1.4 [3.63], R2=0.05).54 In addition, the NNT (95% CI) values for achieving ≥20% improvements in PANSS negative symptoms subscale were low for PP3M (18.6 [6.7; −24.2]) and PP1M (9.7 [5.5; 41.6]), and the SMD (95% CI) was 0.27 (0.040; 0.495) for PP3M comparable with PP1M (0.28 [0.087; 0.479]) (Table 2). Thus, PP3M treatment has clinical benefits in the improvement of negative symptoms that are relevant for the ultimate goal of functional recovery.55
Symptomatic remission
Post hoc analysis of data from the non-inferiority study demonstrated that the proportion of patients achieving the Andreasen et al criteria of 6-month remission based on the PANSS items was similar between PP1M and PP3M (~50% in both treatments) (Table 4).34,56 A majority of these patients maintained their remission status throughout the 48-week DB phase in both treatment arms.56 In a retrospective analysis of an observational study, PP1M treatment was associated with clinically meaningful symptomatic remission (using the Structured Clinical Interview for Symptoms of Remission [SCI-SR]) in concordance with the rates for PP3M.57 A significantly higher proportion of patients on PP1M (new user of PP1M: 45.0%; continuous user of PP1M: 39.0%) relative to OAPs (23.0%) achieved remission (P<0.001). At the 12-month follow-up, PP1M users were more likely to achieve remission vs users of OAPs (new user of PP1M vs OAP: OR=2.65 [1.39; 5.05]; continuous user of PP1M vs OAP: OR=1.83 [1.03; 3.25]).57 As the majority of patients with schizophrenia continue to be symptomatic, despite having reductions in symptoms, the high rates of remission obtained with PP3M treatment suggest maintenance of clinically relevant stability, rather than only symptom improvement.
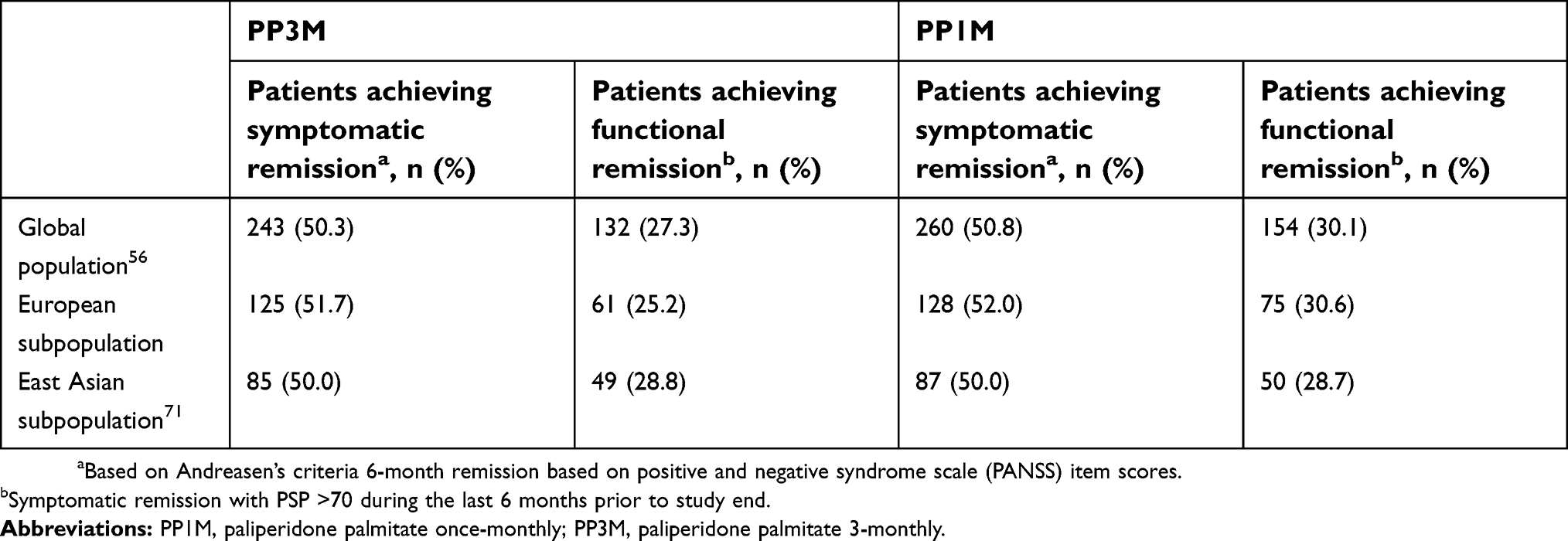 | Table 4 Remission status from double-blind randomized studies of PP3M |
Functional status
In the non-inferiority study, stable PSP scores in patients treated with PP3M (27.3%) and PP1M (30.1%) suggest a sustained effect on functioning from DB baseline to DB endpoint (Table 4). Nearly 25% of patients on PP3M and 27% on PP1M maintained both symptomatic and functional remission during the last 6 months of DB phase.56 A greater proportion of patients in both PP3M and PP1M groups had “good PSP scores” (>70) at DB baseline (PP3M: 28.8%; PP1M: 27.1%), as compared with OL baseline (PP3M: 5.2%; PPIM: 5.1%), and a similar proportion of patients maintained this “good PSP score” in the last 6 months before the end of study across both treatment arms (PP3M: 42.5%; PP1M: 43.9%). Additionally, most patients who achieved remission at DB baseline maintained their remission status throughout the DB phase. Patients’ clinical improvement was associated with greater improvements in other PSP domains, such as social activities, personal and social relationships, self-care, disturbing and aggressive behaviors, along with improvements in insight, and social and occupational functioning domains.56 Evaluation of functional remission based on the duration of illness (subgroups: ≤5 years, 6–10 years, and >10 years since diagnosis) suggested that more patients with a recent onset (≤5 years and 6–10 years) achieved functional remission (PSP >70) than patients with chronic illness (>10 years) during the OL and DB phases.58 Significant improvements were observed in PSP scores in the ≤5 years and 6–10 years subgroup vs the >10 years subgroup at DB baseline and DB end point (P≤0.003), supporting early initiation of PP3M for better functional outcomes.58
Evaluation of work functioning and productivity based on occupational status at OL baseline in phase 3 studies of PP3M revealed that most patients were either unemployed, not seeking work, or retired; however, a general trend of improvement in occupational status was observed in the PP3M groups through the span of both studies.59 While interpreting these findings, it should be acknowledged that a patient’s occupational status depends on several clinical (illness severity, symptomatic status, etc.) and social (level of education, social support, etc.) variables, including employment barrier and support.59 Overall, these data suggest that PP3M treatment has wide-ranging efficacy, including improvements in functional impairment that commonly tend to persist even after symptom reduction.
Caregiver burden
The overall caregiver burden gradually improved with PP1M and PP3M treatment throughout the phase 3 studies (pooled IEQ total scores change from OL baseline to DB endpoint: −8.9 [14.73] points, n=756). Treatment with PP1M or PP3M LAI formulation was associated with improvements in urging, worrying, tension, and supervision domains, thus helping alleviate the burden on caregivers and improving their quality-of-life (QoL). Improvement in caregiver burden was significantly greater in patients without relapse (P<0.001) vs patients who experienced relapse. In addition, switching from OAPs to PP1M or PP3M significantly eased the caregiver burden and had a positive impact on the stress conditions of caregivers (mean IEQ total score: pre-switch [at OL baseline] 28.0 points vs post-switch [at DB endpoint] 19.3 points, P<0.001).46 Reductions in caregiver burden with PP3M treatment were also observed across regions from post hoc analysis of pooled data.60 It was also noted that the perceived caregiver burden improvement was significant in patients switching from OAPs to LAI with less leisure days impacted and less hours spent in caregiving (P<0.001).60
Patients’ attitude and preference
In the placebo-controlled study, most patients (PP3M: 108/150 [72.0%]; placebo: 90/135 [66.7%]) preferred to receive the medication every 3 months based on the MPQ analysis. The main reasons stated for this preference were “less pain due to fewer injections” and “reduced commuting hassles due to fewer appointments.” In the non-inferiority study, the proportion of patients who “preferred pills” in both PP3M (23% and 21%) and PP1M (18% and 19%) groups was similar and comparable between OL baseline and DB endpoint. Of note however, patients randomized to the PP3M group in this study received an injection once a month to maintain the study blind. Thus, the influence of once-monthly vs three-monthly injections on patient preference remains unclear in this study. In other studies of PP1M, patients have recorded greater preference for LAIs over OAPs, owing to monthly dosing flexibility as opposed to daily dosing with oral medications.48,61 From a preference survey of the two phase 3 studies of PP3M, patients and physicians showed greater preference for PP3M and PP1M than OAPs (P<0.05), regardless of treatment or adherence history.62 Patient preference was attributed to improvements in positive symptoms, whereas physicians based their choice on overall improvement (negative and positive symptoms). Physicians also showed greater preference for PP3M over PP1M in patients with a history of missing 20% (P=0.02) and 50% (P=0.003) of doses.62
Selection of patients for PP3M use
In a retrospective analysis of the non-inferiority study, there were no notable differences in demographic and baseline disease characteristics between patients on PP3M achieving and not achieving remission.63 Overall, remitters had a robust symptomatic profile during the 17-week PP1M treatment OL phase. Early improvements observed from week 5 and sustained through week 17 were associated with better prospects for remission. Remitters had greater improvement on the PANSS, PSP, and CGI-S (Clinical Global Impression–Severity)64 scores, and a higher proportion of patients achieved improvements in CGI-S (score ≥1) and PANSS change (≥30%) than non-remitters. In an analysis of predictors of remission using univariate and multivariate logistic regression models, CGI-S, PSP, and PANSS negative factor scores at week 17, change in PANSS uncontrolled hostility/excitement factor score, and change in PANSS anxiety/depression factor score were identified as significant variables influencing remission.63
Due to the slow drug release profile of the formulation, PP3M is not intended in patients experiencing acute exacerbation of schizophrenia and those who are currently on oral risperidone or paliperidone ER, or those not currently receiving PP1M.31 Maintenance treatment with PP3M should be initiated after the patient has adequately responded and tolerated a flexible dose range of PP1M for at least 4 months. The last two doses of PP1M prior to switching to PP3M is recommended to be the same, and the patient should be clinically stable (based on clinical judgment) and adequately tolerating PP1M before transitioning to PP3M.31 The evaluation of adequate response should reflect a high degree of symptomatic remission and clinical stability at steady state of PP1M to determine the correct dose of PP3M during transitioning to maintain the desired exposure with no or minimal dose adjustment in the future. Clinicians should be careful not to initiate PP3M as a last resort in patients not responding to current antipsychotic therapy.32
Safety and tolerability
The safety and tolerability profile of PP1M has been extensively described. Treatment-emergent adverse events (TEAEs) of clinical interest are weight gain (13–27%), EPS-related TEAEs (6–25%), potentially prolactin-related TEAEs (2–29%), and glucose-related TEAEs (0–4%).21,25,26,65–67 Suicidality, tachycardia, and QT prolongation were among the other TEAEs reported with PP1M use with sporadic incidences. The high NNH (16 to ∞) reported for selected risk outcomes support the favorable safety profile of PP1M.37
Overall, 62% of patients in the placebo-controlled study (placebo group: 58%) and 68% of patients in the non-inferiority study (PP1M group: 66%) experienced TEAEs with PP3M treatment.33,34 The nature and frequency of TEAEs were generally comparable between PP1M and PP3M groups, and corroborate earlier reports of PP1M.33,34 The NNH reported for overall EPS, akathisia, headache, weight gain, nasopharyngitis, and use of anticholinergic medications during the DB phase of the study was high relative to placebo (160 to −132.6), suggesting a low incidence of these TEAEs with PP3M. The highest risks were reported for weight gain (NNH=18.9, 95% CI=9.1, 362.6) and akathisia (NNH=27.1, 95% CI=12.3, −667.1) and lowest for dyskinesia (NNH= −132.6, 95% CI=44.5, −23.2), with the negative NNH values indicating that PP3M-treated patients had reduced risk of dyskinesia events vs placebo.39 The likelihood of being helped or harmed (LHH=NNH/NNT) ranged from 5.6–47.2 for relapse prevention vs each selected safety outcome of PP3M relative to placebo, suggesting overall therapeutic gain.39 Overall, NNHs for adverse events associated with PP3M were comparable to PP1M (Table 5).37
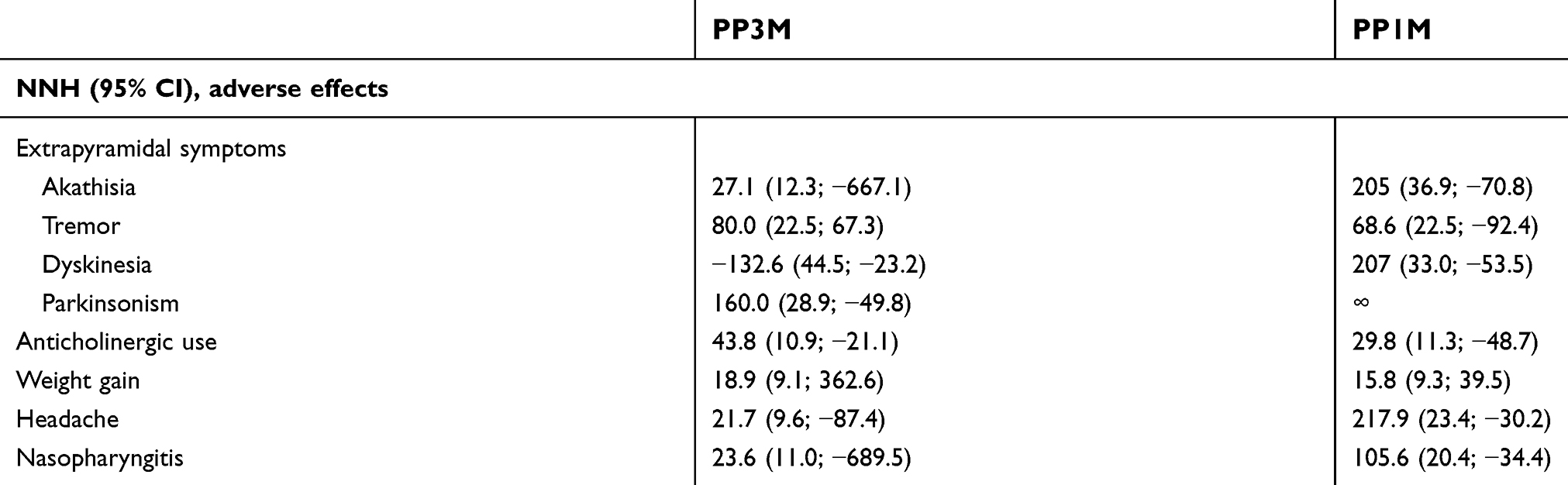 | Table 5 Number needed to harm for selected adverse events with different formulations of paliperidone palmitate |
The incidences of EPS-related TEAEs and time-to-onset (TTO) and time-to-resolution (TTR) of these events were similar between PP3M and PP1M.68 The reported median TTO was 115 days (PP3M) and 98.5 days (PP1M), and the median TTR was 36.5 days (PP1M) in OL, 91 days (PP3M) and 85.5 days (PP1M) in the DB phase of the non-inferiority study.68 Despite the higher dose strength and longer half-life of PP3M, no meaningful differences were reported in the EPS-profile of PP3M vs PP1M. Reduced dosing frequency and low rate of EPS-related TEAEs with PP3M implicate a positive impact on adherence and overall QoL of patients and their caregivers.68 Similar results were observed for injection-site reaction and pain, an important concern pertinent to LAIs from a healthcare perspective.69 Low visual analog scale scores suggested mild injection-site pain and reduction from DB baseline to endpoint without notable differences between PP3M (Mean [SD]=19.5 [20.7] to 15.6 [17.9]) and PP1M (18.4 [20.4] to 15.5 [18.3]). Severity of injection-site induration, redness, and swelling were mild, with low frequency in both treatment groups, without any significant influence of the formulation difference.70 Overall, the safety profile of PP3M in the global patient population was consistent with findings in the East Asian,71 European, and Latin American sub-groups, suggesting an absence of regional or ethnic influences.
Review of evidence
Increasing awareness of antipsychotic treatment efficacy for schizophrenia has led to broadening of treatment goals to encompass specific clinical dimensions of the disease, such as cognitive deficits, negative symptoms, mood symptoms, and, most importantly, relapses.72,73 Relapses in schizophrenia are the leading causes of hospitalization and worsening of social and occupational functioning, and often lead to loss of progress when patients are participating in recovery-oriented programs.74 In this context, SGA-LAI antipsychotics have been developed and examined with regard to their potential benefits.75 Evidence from RCTs of available LAIs have shown mixed results for the advantages of LAIs over OAPs for relapse prevention in schizophrenia.76–82 However, mirror image and cohort studies have supported the superiority of LAIs over OAPs for prevention of rehospitalizations,83,84 generally without risk of greater or additional adverse effects in RCTs79,85 and, even with some indication of lower mortality than with OAPs.86
By virtue of longer plasma half-lives and continuous antipsychotic exposure, LAI formulations are likely to provide protracted relapse-free periods, even after treatment interruption or discontinuation.87,88 In three similarly-designed relapse prevention studies with different formulations of paliperidone, patients in the placebo group were first stabilized on the corresponding paliperidone formulation (oral, PP1M, PP3M) before being withdrawn.23 Discontinuation in these studies reflects a situation that is common in real-world treatment settings, where patients may interrupt or completely discontinue their medication without notifying their physician. Thus, findings of longer post-discontinuation time-to-relapse bring improved clarity about clinical benefits and efficacy for long-term treatment of schizophrenia with LAI formulations having extended half-lives. However, clinicians may have concerns that the longer half-life of PP3M may not allow intermittent dose titrations or therapeutic changes during the 3-month window to manage any potential adverse events.89 It is, therefore, critical to adequately stabilize patients on PP1M before initiating PP3M to minimize the chances of unknown or uncontrolled adverse events. Also, a paradoxical decrease in adherence due to the longer gap between physician visits that could delay detection of worsening symptoms or signs of adverse events has been postulated as a possible disadvantage of longer-acting formulations such as PP3M.90
Benefit–risk assessments drive clinical decision-making, and quantitative analyses using effect size measurements are reliable methods for evidence-based research that offer a more objective approach.62 Measures of effect size, such as NNT, help establish therapeutic benefit. NNH refers to the magnitude of adverse effects, and SMD suggest the magnitude of effect for continuous efficacy outcomes, adjusted for differences in scale of measurement and measuring inaccuracies.35,36,40 For interpretation of efficacy data, the SMD values are defined as small (0.2), medium (0.5), and large (0.8) effect sizes.91 In the absence of sufficient head-to-head comparisons between available LAI antipsychotics, effect sizes are interpretable measures that allow comparison of observed clinical effects and risks across distinct studies.92 Overall, low NNT for relapse prevention and achieving minimally important change (≥20%) in PANSS total scores suggest meaningful efficacy with a lower relapse risk and comparable benefits of PP3M and PP1M treatment. The SMDs for all efficacy outcomes also supported the comparative efficacy of the two PP LAIs, suggesting that the probability of patients improving was comparable between PP3M and PP1M treatment.
Diagnostic classification of schizophrenia into discrete subtypes based on predominance of positive or negative symptoms serves as a useful predictor of prognosis and treatment response.93 This strategy supports efforts to establish clinical and pathophysiological correlations that help in patient selection for improved outcomes, longitudinal approaches for better care, and judgment of symptom relief.93,94 Prominence of positive symptoms reflects a relatively routine course of disease with better premorbid adjustment, superior treatment outcomes with antipsychotic treatment, and a neurochemical pathophysiology with minimal atrophy; in contrast, negative symptoms represent a more malignant disease course with poor pre-morbid adjustment, compromised functioning and characteristic structural brain changes.94 Negative symptoms tend to linger during periods of clinical stability, and can interfere with normal functioning.95 There is consistent evidence that available antipsychotics predominantly treat positive symptoms with modest effects on other domains of schizophrenia.96 A limited number of antipsychotics are available for specific treatment of negative symptoms of schizophrenia and in most cases improvements are perceived as a consequence of their effects on positive symptoms.95,97 Among available evidence for antipsychotic monotherapy, clozapine and aripiprazole did not show satisfactory efficacy for improving negative symptoms, whereas olanzapine showed significant (P≤0.05) improvements in PANSS negative subscale vs haloperidol.98–100 In acutely ill patients with schizophrenia and predominantly negative symptoms, paliperidone ER significantly improved negative symptoms when compared with placebo.101 Clinically relevant improvements in negative, depressive, and anxiety symptoms and disorganized thoughts have also been observed in patients with schizophrenia treated with PP1M in a real-world setting.102 Sustained improvements in positive and negative subscale and symptoms factor scores indicate the efficacy of PP3M across the spectrum of schizophrenia comprising major domains. PP3M treatment could potentially be useful in treating negative symptoms in schizophrenia, a symptom domain with few therapeutic options.55
Remission is an important component of recovery in patients with schizophrenia, and consolidated outcome measures of remission can aid interpretation of symptomatic outcomes in clinical studies.41,44 The observed remission rates for both PP3M and PP1M were high; however, it should be noted that both PP3M studies were of longer duration and implemented an enrichment design, allowing clinically stable patients to enter the DB treatment phase.33,34,103 Overall, the achievement of symptomatic remission on severity and duration indicate that the reductions in symptoms are robust and sustained, underscoring the clinical utility of PP3M.
Functional disability in schizophrenia is a major obstacle in everyday activities. Among several other factors, neurocognitive deficits (attention, memory, processing speed, executive functioning, vigilance, and reasoning) and severity of negative symptoms contribute to impaired functionality in schizophrenia.104 Difficulty in succeeding at school or maintaining a job, managing social relationships, living independently, and the struggle to handle basic daily needs are common challenges reported in patients with schizophrenia.105 Functional remission is defined as a separate domain from clinical remission and is assessed using performance-based scales to measure adequate levels of psychosocial functioning.106,107 Therefore, functional recovery (in addition to symptom control, delaying progression and relapse) is regarded an essential goal in the management of schizophrenia, and broadly emphasizes the capacity of a person to resume normal levels of social and occupational function, independent life, and remission in overt behavioral symptoms.3,107 Collectively, parallel improvements in symptomatic and functional domains by PP3M can be an important consideration for use in the comprehensive management of schizophrenia, including enabling enhanced efficacy of adjunctive psychosocial interventions.
Schizophrenia is still all too frequently an incapacitating psychiatric disorder that can lead to a “burden of care”: a complex concept that exerts emotional, psychological, physical, and economic impacts on the lives of caregivers for patients with schizophrenia.108,109 Although there is a lack of consensus regarding any specific cluster of psychotic symptoms maximally impacting the caregiver’s burden, severity of symptoms would in all likelihood escalate the burden.108 The functional status of patients and relapses are also thought to directly impact caregiver burden by hampering the patient’s psychosocial competency and ability to live an independent life, and increasing the risk of rehospitalization.109,110 Additionally, it is established that the increasing number of hospitalizations and severity of illness in these patients will heighten caregiver burden.111 Although substantial evidence comparing the effectiveness of SGA-LAIs and their effects on functioning and symptom alleviation are available, data on caregiver burden assessments are limited. A Spanish epidemiological study demonstrated significant benefits (P=0.0018) on caregiver burden among caregivers of patients using risperidone-LAI compared with those on oral atypical antipsychotics based on the Zarit caregiver burden scale.112 Overall, PP3M and PP1M treatment correlated with positive reduction in the caregiver burden, as well as an improved ability to cope with the burden, potentially by addressing the refractory nature and non-adherence associated with schizophrenia. Formulation benefits of LAIs may be the major reasons for reductions in urging and worrying domains among caregivers of patients on PP1M/PP3M treatment. Taken together, caregivers benefit from the patient’s use of LAI therapy, as it dispels the need to negotiate daily for medication adherence, reducing caregiver’s struggle, and eventually de-stressing the patient–caregiver relationship. With a longer half-life, negotiations during PP3M treatment are needed just 4-times a year. From a patient’s perspective, a formulation like PP3M is advantageous, as they need to visit clinics less frequently for injections, especially benefiting patients who are away from home or traveling, etc. As studies have shown a lack of any significant adherence advantage with monthly injected LAIs, it is important to investigate correlations between observed patient preference and positive attitudes on measurement of actual medication adherence in patients using PP3M.113
The safety profile of SGA-LAIs, such as olanzapine, aripiprazole, risperidone, and PP, are generally analogous to OAPs,79 except for the post-injection delirium/sedation syndrome with olanzapine LAI.114 Other side-effects include variable incidences of psychotic symptoms, EPS events, and metabolic/endocrine-related TEAEs (weight gain, hyperprolactinemia, and impaired glucose metabolism).115 The higher NNH for EPS and weight gain relative to placebo reflect lower incidences of these TEAEs with PP3M.37 The safety profile of PP3M, especially with regard to EPS-related events and weight gain, could potentially mediate improvements in QoL.116
Although this paper endeavors to reconcile research findings for PP3M and bridge the gap between trial-based outcomes and clinical applicability, the results described here represent a well-characterized clinical study population with schizophrenia, without distinct identification of symptom predominance or risk factors. Some limitations are noted in the primary outcome reports, such as exclusion of patients with a history of recent substance dependence and patients with treatment-resistant illness, particularly those that require clozapine. Since patients need to first tolerate and respond to PPIM before they switch to PP3M, patients are enriched for tolerability to PP, and this may lead to higher NNH levels for EPS and similar adverse events.33,34 Also, the efficacy and safety of PP3M were determined in patients who were already responsive to PP1M, thus limiting the generalizability of these findings to a treatment-naïve population.117 However, it should be noted that PP3M administration is prescribed only in patients who have been clinically stabilized on PP1M, and that clinically, long-term treatment is not provided to unselected populations, but rather to enriched populations who responded to and tolerated the medication acutely. Interpretations of measurement-based outcomes should be placed within a context to individual patient requirements with a careful assessment of disease course, risk factors, patient/caregiver outlook, and individual adverse event profile.3 Thus, large real-world trials of PP3M in an unselected patient population, assessing more pragmatic outcomes, are needed to eliminate the risk of selection bias, improve external validity of findings, and provide more exhaustive safety data for PP3M.90,118 Additionally, approaches to identify and address common patient and clinician-related barriers to LAI use in general, such as social stigma, increased direct costs, limited clinical experience, and lack of control over medication, would ultimately help improve treatment outcomes.119
Conclusion
Available evidence supports a prominent position for PP3M in the current therapeutic armamentarium for schizophrenia. High remission rates substantiate the differences in scores reported in clinical studies of PP3M, and help to elucidate the magnitude of symptomatic improvement and level of patient functioning, supporting the use of PP3M in the maintenance treatment of schizophrenia. Robust effect sizes for treatment effects and harm could help clinicians in patient management and advising patients about potential outcomes with PP3M. Improvements in clinically important domains of schizophrenia, such as negative symptoms and caregiver burden, can be expected to benefit patients, clinicians, and caregivers alike. Future studies to further delineate potential beneficial outcomes with PP3M treatment in terms of long-term effects, cost-effectiveness, and real-world experiences would substantiate these findings.
Acknowledgments
The authors thank Priya Ganpathy, MPharm, ISMPP CMPP™ (SIRO Clinpharm Pvt. Ltd, India) for writing assistance, and Ellen Baum, PhD (Janssen Global Services, LLC) for additional editorial assistance. The development of this review article was supported by funding from Janssen Research & Development, LLC.
Author contributions
MM and AJS were responsible for initial conceptualization of the scope, focus, analysis, and interpretation. LH, EK, WT, BS, SG, and CUC were responsible for analysis and interpretation. IN was the statistician and conducted and directed data analysis and interpretation. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
MM, SG, IN, and AJS are employees and shareholders of Janssen Research & Development, LLC, USA (parent company Johnson and Johnson). LH is an employee and shareholder of Janssen-Cilag EMEA, Neuss, Deutschland. EK is an employee of Janssen Scientific Affairs, LLC, USA. WT is an employee and shareholder of Janssen Pharmaceutical Companies of Johnson and Johnson, Singapore. BS is an employee and shareholder of Jan-Cil, Brazil. CUC has been a consultant and/or advisor to or has received honoraria from: Alkermes, Allergan, Angelini, Boehringer-Ingelheim, Gerson Lehrman Group, Indivior, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, Medavante-ProPhase, Medscape, Merck, Neurocrine, Noven, Otsuka, Pfizer, Rovi, Servier, Sunovion, Takeda, and Teva. He has provided expert testimony for Bristol-Myers Squibb, Janssen, and Otsuka. He also served on a Data Safety Monitoring Board for Lundbeck, Rovi, and Teva. He received royalties from UpToDate® and grant support from Janssen and Takeda. The authors report no other conflicts of interest in this work.
References
1. Rabinowitz J, Levine SZ, Haim R, Hafner H. The course of schizophrenia: progressive deterioration, amelioration or both? Schizophr Res. 2007;91(1–3):254–258. doi:10.1016/j.schres.2006.12.013
2. Kahn RS, Sommer IE, Murray RM, et al. Schizophrenia. Nat Rev Dis Primers. 2015;1:15067. doi:10.1038/nrdp.2015.67
3. Correll CU, Kishimoto T, Nielsen J, Kane JM. Quantifying clinical relevance in the treatment of schizophrenia. Clin Ther. 2011;33(12):B16–39. doi:10.1016/j.clinthera.2011.11.016
4. Citrome L, Ketter TA. When does a difference make a difference? Interpretation of number needed to treat, number needed to harm, and likelihood to be helped or harmed. Int J Clin Pract. 2013;67(5):407–411. doi:10.1111/ijcp.12142
5. Carbon M, Correll CU. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin Neurosci. 2014;16(4):505–524.
6. Ascher-Svanum H, Faries DE, Zhu B, Ernst FR, Swartz MS, Swanson JW. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry. 2006;67(3):453–460.
7. Citrome L. New second-generation long-acting injectable antipsychotics for the treatment of schizophrenia. Expert Rev Neurother. 2013;13(7):767–783. doi:10.1586/14737175.2013.811984
8. Herings RM, Erkens JA. Increased suicide attempt rate among patients interrupting use of atypical antipsychotics. Pharmacoepidemiol Drug Saf. 2003;12(5):423–424.
9. Morken G, Widen JH, Grawe RW. Non-adherence to antipsychotic medication, relapse and rehospitalisation in recent-onset schizophrenia. BMC Psychiatry. 2008;8:32.
10. Kane JM, Kishimoto T, Correll CU. Non-adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry. 2013;12(3):216–226. doi:10.1002/wps.20060
11. Ascher-Svanum H, Zhu B, Faries DE, Furiak NM, Montgomery W. Medication adherence levels and differential use of mental-health services in the treatment of schizophrenia. BMC Res Notes. 2009;2:6. doi:10.1186/1756-0500-2-6
12. Weiden PJ, Kozma C, Grogg A, Locklear J. Partial compliance and risk of rehospitalization among California Medicaid patients with schizophrenia. Psychiatr Serv. 2004;55(8):886–891. doi:10.1176/appi.ps.55.8.886
13. Park EJ, Amatya S, Kim MS, et al. Long-acting injectable formulations of antipsychotic drugs for the treatment of schizophrenia. Arch Pharm Res. 2013;36(6):651–659. doi:10.1007/s12272-013-0105-7
14. Gopal S, Gassmann-Mayer C, Palumbo J, Samtani MN, Shiwach R, Alphs L. Practical guidance for dosing and switching paliperidone palmitate treatment in patients with schizophrenia. Curr Med Res Opin. 2010;26(2):377–387. doi:10.1185/03007990903482772
15. Davidson M, Emsley R, Kramer M, et al. Efficacy, safety and early response of paliperidone extended-release tablets (paliperidone ER): results of a 6-week, randomized, placebo-controlled study. Schizophr Res. 2007;93(1–3):117–130. doi:10.1016/j.schres.2007.03.003
16. Kane J, Canas F, Kramer M, et al. Treatment of schizophrenia with paliperidone extended-release tablets: a 6-week placebo-controlled trial. Schizophr Res. 2007;90(1–3):147–161. doi:10.1016/j.schres.2006.09.012
17. Kramer M, Simpson G, Maciulis V, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2007;27(1):6–14. doi:10.1097/JCP.0b013e31802dda4a
18. Schreiner A, Hargarter L, Hitschfield K, et al. Clinical effectiveness and resource utilization of paliperidone ER for schizophrenia: pharmacoepidemiologic International Longitudinal Antipsychotic Registry (PILAR). Curr Med Res Opin. 2014;30(7):1279–1289. doi:10.1185/03007995.2014.898630
19.
20. Newton R, Hustig H, Lakshmana R, et al. Practical guidelines on the use of paliperidone palmitate in schizophrenia. Curr Med Res Opin. 2012;28(4):559–567. doi:10.1185/03007995.2012.665362
21. Hough D, Gopal S, Vijapurkar U, Lim P, Morozova M, Eerdekens M. Paliperidone palmitate maintenance treatment in delaying the time-to-relapse in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. Schizophr Res. 2010;116(2–3):107–117. doi:10.1016/j.schres.2009.10.026
22. Marcus SC, Zummo J, Pettit AR, Stoddard J, Doshi JA. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J Manag Care Spec Pharm. 2015;21(9):754–768. doi:10.18553/jmcp.2015.21.9.754
23. Weiden PJ, Kim E, Bermak J, Turkoz I, Gopal S, Berwaerts J. Does half-life matter after antipsychotic discontinuation? A relapse comparison in schizophrenia with 3 different formulations of paliperidone. J Clin Psychiatry. 2017;78(7):e813–e820. doi:10.4088/JCP.16m11308
24. Zhang F, Si T, Chiou CF, et al. Efficacy, safety, and impact on hospitalizations of paliperidone palmitate in recent-onset schizophrenia. Neuropsychiatr Dis Treat. 2015;11:657–668. doi:10.2147/NDT.S77778
25. Gopal S, Vijapurkar U, Lim P, Morozova M, Eerdekens M, Hough D. A 52-week open-label study of the safety and tolerability of paliperidone palmitate in patients with schizophrenia. J Psychopharmacol. 2011;25(5):685–697. doi:10.1177/0269881110372817
26. Pandina GJ, Lindenmayer JP, Lull J, et al. A randomized, placebo-controlled study to assess the efficacy and safety of 3 doses of paliperidone palmitate in adults with acutely exacerbated schizophrenia. J Clin Psychopharmacol. 2010;30(3):235–244. doi:10.1097/JCP.0b013e3181dd3103
27. Emsley R, Parellada E, Bioque M, Herrera B, Hernando T, Garcia-Dorado M. Real-world data on paliperidone palmitate for the treatment of schizophrenia and other psychotic disorders: a systematic review of randomized and nonrandomized studies. Int Clin Psychopharmacol. 2018;33(1):15–33. doi:10.1097/YIC.0000000000000195
28. Fu DJ, Turkoz I, Simonson RB, et al. Paliperidone palmitate once-monthly reduces risk of relapse of psychotic, depressive, and manic symptoms and maintains functioning in a double-blind, randomized study of schizoaffective disorder. J Clin Psychiatry. 2015;76(3):253–262. doi:10.4088/JCP.14m09416
29. Fu DJ, Turkoz I, Walling D, Lindenmayer JP, Schooler NR, Alphs L. Paliperidone palmitate once-monthly maintains improvement in functioning domains of the personal and social performance scale compared with placebo in subjects with schizoaffective disorder. Schizophr Res. 2018;192:185–193. doi:10.1016/j.schres.2017.04.004
30. Samtani MN, Nandy P, Ravenstijn P, et al. Prospective dose selection and acceleration of paliperidone palmitate 3-month formulation development using a pharmacometric bridging strategy. Br J Clin Pharmacol. 2016;82(5):1364–1370. doi:10.1111/bcp.13050
31. Gopal S, Vermeulen A, Nandy P, et al. Practical guidance for dosing and switching from paliperidone palmitate 1 monthly to 3 monthly formulation in schizophrenia. Curr Med Res Opin. 2015;31(11):2043–2054. doi:10.1185/03007995.2015.1085849
32.
33. Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):830–839. doi:10.1001/jamapsychiatry.2015.0241
34. Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. 2016;19:7. doi:10.1093/ijnp/pyw018
35. Citrome L, Ketter TA. NNT and NNH remain helpful in evidence-based medicine. Br J Psychiatry. 2016;209(3):262–263. doi:10.1192/bjp.209.3.262b
36. Citrome L, Ketter TA, Cucchiaro J, Loebel A. Clinical assessment of lurasidone benefit and risk in the treatment of bipolar I depression using number needed to treat, number needed to harm, and likelihood to be helped or harmed. J Affect Disord. 2014;155:20–27. doi:10.1016/j.jad.2013.10.040
37. Gopal S, Berwaerts J, Nuamah I, et al. Number needed to treat and number needed to harm with paliperidone palmitate relative to long-acting haloperidol, bromperidol, and fluphenazine decanoate for treatment of patients with schizophrenia. Neuropsychiatr Dis Treat. 2011;7:93–101. doi:10.2147/NDT.S17177
38. Altman DG, Andersen PK. Calculating the number needed to treat for trials where the outcome is time to an event. BMJ. 1999;319(7223):1492–1495.
39. Mathews M, Nuamah I, Savitz A, Gopal S. Efficacy and safety of paliperidone palmitate 3-month formulation vs placebo for relapse prevention of schizophrenia: treatment effect using a number needed to treat analysis. Biol Psychiatry. 2017;81(10):S350–S351. doi:10.1016/j.biopsych.2017.02.592
40. Faraone SV. Interpreting estimates of treatment effects: implications for managed care. P T. 2008;33(12):700–711.
41. Andreasen NC, Carpenter WT
42. Kawata AK, Revicki DA. Psychometric properties of the personal and social performance scale (PSP) among individuals with schizophrenia living in the community. Qual Life Res. 2008;17(10):1247–1256. doi:10.1007/s11136-008-9400-z
43. Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and occupational functioning assessment scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323–329.
44. van Os J, Burns T, Cavallaro R, et al. Standardized remission criteria in schizophrenia. Acta Psychiatr Scand. 2006;113(2):91–95. doi:10.1111/j.1600-0447.2005.00659.x
45. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276.
46. Gopal S, Xu H, McQuarrie K, et al. Caregiver burden in schizophrenia following paliperidone palmitate long acting injectables treatment: pooled analysis of two double-blind randomized phase three studies. NPJ Schizophr. 2017;3(1):23. doi:10.1038/s41537-017-0025-5
47. van Wijngaarden B, Schene AH, Koeter M, et al.Caregiving in schizophrenia: development, internal consistency and reliability of the involvement evaluation questionnaire–European version. EPSILON study 4. European psychiatric services: inputs linked to outcome domains and needs. Br J Psychiatry Suppl. 2000;(39):s21–27. doi:10.1192/bjp.177.39.s21
48. Si T, Zhang K, Tang J, et al. Efficacy and safety of flexibly dosed paliperidone palmitate in Chinese patients with acute schizophrenia: an open-label, single-arm, prospective, interventional study. Neuropsychiatr Dis Treat. 2015;11:1483–1492. doi:10.2147/NDT.S81760
49. Hargarter L, Bergmans P, Cherubin P, et al. Once-monthly paliperidone palmitate in recently diagnosed and chronic non-acute patients with schizophrenia. Expert Opin Pharmacother. 2016;17(8):1043–1053. doi:10.1080/14656566.2016.1174692
50. Li H, Li Y, Feng Y, et al. Impact of time of initiation of once-monthly paliperidone palmitate in hospitalized Asian patients with acute exacerbation of schizophrenia: a post hoc analysis from the PREVAIL study. Neuropsychiatr Dis Treat. 2018;14:1107–1117. doi:10.2147/NDT.S157399
51. Li H, Turkoz I, Zhang F. Efficacy and safety of once-monthly injection of paliperidone palmitate in hospitalized Asian patients with acute exacerbated schizophrenia: an open-label, prospective, noncomparative study. Neuropsychiatr Dis Treat. 2016;12:15–24. doi:10.2147/NDT.S83651
52. Nasrallah HA, Gopal S, Gassmann-Mayer C, et al. A controlled, evidence-based trial of paliperidone palmitate, a long-acting injectable antipsychotic, in schizophrenia. Neuropsychopharmacology. 2010;35(10):2072–2082. doi:10.1038/npp.2010.79
53. Pandina G, Lane R, Gopal S, et al. A double-blind study of paliperidone palmitate and risperidone long-acting injectable in adults with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):218–226. doi:10.1016/j.pnpbp.2010.11.008
54. Mathews M, Gopal S, Singh A, Gogate J, Edward Kim PK. Comparison of paliperidone palmitate 3-month and paliperidone palmitate 1-month formulation for negative symptoms in schizophrenia: A phase 3 non-inferiority study. Schizophr Bull. 2018;44(Suppl 1):S311. doi:10.1093/schbul/sby017.761
55. Remington G, Foussias G, Fervaha G, et al. Treating negative symptoms in schizophrenia: an update. Curr Treat Options Psychiatry. 2016;3:133–150. doi:10.1007/s40501-016-0075-8
56. Savitz AJ, Xu H, Gopal S, Nuamah I, Hough D, Mathews M. Paliperidone palmitate 3-month treatment results in symptomatic remission in patients with schizophrenia: a randomized, multicenter, double-blind, and noninferiority study. Int Clin Psychopharmacol. 2017;32(6):329–336. doi:10.1097/YIC.0000000000000190
57. Anderson JP, Icten Z, Alas V, Benson C, Joshi K. Comparison and predictors of treatment adherence and remission among patients with schizophrenia treated with paliperidone palmitate or atypical oral antipsychotics in community behavioral health organizations. BMC Psychiatry. 2017;17(1):346. doi:10.1186/s12888-017-1489-6
58. Brown B, Turkoz I, Mancevski B, Mathews M. PM411. evaluation of paliperidone palmitate long-acting injectable therapy by duration of illness in patients with schizophrenia. Int J Neuropsychopharmacol. 2016;19(Suppl 1):49. doi:10.1093/ijnp/pyw041.411
59. Chirila C, Nuamah I, Woodruff K. Health care resource use analysis of paliperidone palmitate 3 month injection from two phase 3 clinical trials. Curr Med Res Opin. 2017;33(6):1083–1090. doi:10.1080/03007995.2017.1300144
60. Srihari G, Haiyan X, Adam S, et al. PM511. determinants of caregiver burden in family carers of asian patients with schizophrenia treated with paliperidone palmitate 3-monthly injectable. Int J Neuropsychopharmacol. 2016;19(Suppl_1):85–86. doi:10.1093/ijnp/pyw041.511
61. Zhao J, Li L, Shi J, et al. Safety and efficacy of paliperidone palmitate 1-month formulation in Chinese patients with schizophrenia: a 25-week, open-label, multicenter, Phase IV study. Neuropsychiatr Dis Treat. 2017;13:2045–2056. doi:10.2147/NDT.S131224
62. Katz EG, Hauber B, Gopal S, et al. Physician and patient benefit-risk preferences from two randomized long-acting injectable antipsychotic trials. Patient Prefer Adherence. 2016;10:2127–2139. doi:10.2147/PPA.S114172
63. Nash A, Turkoz I, Savitz A, Maju Mathews KE. Predictors of Achieving Remission in Schizophrenia Patients Treated with Paliperidone Palmitate 3-Month Formulation.
64. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4(7):28–37.
65. Bossie CA, Fu DJ, Sliwa JK, Ma YW, Alphs L. Tolerability of initiation doses of once-monthly paliperidone palmitate in patients with recently diagnosed schizophrenia in an acute treatment trial. Ther Adv Psychopharmacol. 2011;1(4):111–124. doi:10.1177/2045125311413006
66. Kramer M, Litman R, Hough D, et al. Paliperidone palmitate, a potential long-acting treatment for patients with schizophrenia. Results of a randomized, double-blind, placebo-controlled efficacy and safety study. Int J Neuropsychopharmacol. 2010;13(5):635–647. doi:10.1017/S1461145709990988
67. Alphs L, Bossie CA, Sliwa JK, Ma YW, Turner N. Onset of efficacy with acute long-acting injectable paliperidone palmitate treatment in markedly to severely ill patients with schizophrenia: post hoc analysis of a randomized, double-blind clinical trial. Ann Gen Psychiatry. 2011;10(1):12. doi:10.1186/1744-859X-10-12
68. Mathews M, Nuamah I, Savitz A, et al. PM410. comparison of 3-monthly versus 1-monthly paliperidone palmitate for time to onset and time to resolution of extrapyramidal symptoms in patients with exacerbated schizophrenia. Int J Neuropsychopharmacol. 2016;19(Suppl 1):49. doi:10.1093/ijnp/pyw041.410
69. Elefant E, Sliwa JK, Savitz A, et al. PM386. an assessment of injection site reactions and injection site pain of once-every one month and three-month long-acting injectable formulations of paliperidone palmitate. Int J Neuropsychopharmacol. 2016;19(Suppl 1):41. doi:10.1093/ijnp/pyw041.386
70. Kern Sliwa J, Savitz A, Nuamah I, et al. An assessment of injection site reaction and injection site pain of 1-month and 3-month long-acting injectable formulations of paliperidone palmitate. Perspect Psychiatr Care. 2018. doi:10.1111/ppc.12267
71. Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate three-monthly formulation in East Asian patients with schizophrenia: subgroup analysis of a global, randomized, double-blind, Phase III, noninferiority study. Neuropsychiatr Dis Treat. 2017;13:2193–2207. doi:10.2147/NDT.S134287
72. Bruijnzeel D, Suryadevara U, Tandon R. Antipsychotic treatment of schizophrenia: an update. Asian J Psychiatr. 2014;11:3–7.
73. Carbon M, Correll CU. Thinking and acting beyond the positive: the role of the cognitive and negative symptoms in schizophrenia. CNS Spectr. 2014;19(Suppl 1):
74. Kane JM. Improving patient outcomes in schizophrenia: achieving remission, preventing relapse, and measuring success. J Clin Psychiatry. 2013;74(9):e18.
75. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(suppl 3):1–24.
76. Rauch AS, Fleischhacker WW. Long-acting injectable formulations of new-generation antipsychotics: a review from a clinical perspective. CNS Drugs. 2013;27(8):637–652.
77. Haddad PM, Kishimoto T, Correll CU, Kane JM. Ambiguous findings concerning potential advantages of depot antipsychotics: in search of clinical relevance. Curr Opin Psychiatry. 2015;28(3):216–221.
78. Kane JM, Kishimoto T, Correll CU. Assessing the comparative effectiveness of long-acting injectable vs. oral antipsychotic medications in the prevention of relapse provides a case study in comparative effectiveness research in psychiatry. J Clin Epidemiol. 2013;66(8 Suppl):S37–41.
79. Kishi T, Matsunaga S, Iwata N. Mortality risk associated with long-acting injectable antipsychotics: a systematic review and meta-analyses of randomized controlled trials. Schizophr Bull. 2016;42(6):1438–1445.
80. Kishi T, Oya K, Iwata N. Long-acting injectable antipsychotics for the prevention of relapse in patients with recent-onset psychotic disorders: A systematic review and meta-analysis of randomized controlled trials. Psychiatry Res. 2016;246:750–755.
81. Kishimoto T, Robenzadeh A, Leucht C, et al. Long-acting injectable vs oral antipsychotics for relapse prevention in schizophrenia: a meta-analysis of randomized trials. Schizophr Bull. 2014;40(1):192–213.
82. Leucht C, Heres S, Kane JM, Kissling W, Davis JM, Leucht S. Oral versus depot antipsychotic drugs for schizophrenia–a critical systematic review and meta-analysis of randomised long-term trials. Schizophr Res. 2011;127(1–3):83–92.
83. Kishimoto T, Hagi K, Nitta M, et al. Effectiveness of long-acting injectable vs oral antipsychotics in patients with schizophrenia: a meta-analysis of prospective and retrospective cohort studies. Schizophr Bull. 2018;44(3):603–619.
84. Kishimoto T, Nitta M, Borenstein M, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. 2013;74(10):957–965.
85. Misawa F, Kishimoto T, Hagi K, Kane JM, Correll CU. Safety and tolerability of long-acting injectable versus oral antipsychotics: A meta-analysis of randomized controlled studies comparing the same antipsychotics. Schizophr Res. 2016;176(2–3):220–230.
86. Taipale H, Mittendorfer-Rutz E, Alexanderson K, et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr Res. 2017;197:271–280.
87. De Hert M, Sermon J, Geerts P, Vansteelandt K, Peuskens J, Detraux J. The use of continuous treatment versus placebo or intermittent treatment strategies in stabilized patients with schizophrenia: a systematic review and meta-analysis of randomized controlled trials with first- and second-generation antipsychotics. CNS Drugs. 2015;29(8):637–658.
88. Zhornitsky S, Stip E. Oral versus long-acting injectable antipsychotics in the treatment of schizophrenia and special populations at risk for treatment nonadherence: a systematic review. Schizophr Res Treatment. 2012;2012:407171.
89. Bioque M, Bernardo M. The current data on the 3-month paliperidone palmitate formulation for the treatment of schizophrenia. Expert Opin Pharmacother. 2018;19(14):1623–1629.
90. Ostuzzi G, Papola D, Gastaldon C, Barbui C. New EMA report on paliperidone 3-month injections: taking clinical and policy decisions without an adequate evidence base. Epidemiol Psychiatr Sci. 2017;26(3):231–233.
91. J C. Statistical Power Analysis for the Behavioral Sciences.
92. Kraemer HC, Kupfer DJ. Size of treatment effects and their importance to clinical research and practice. Biol Psychiatry. 2006;59(11):990–996.
93. Andreasen NC, Flaum M, Swayze VW
94. Andreasen NC, Olsen S. Negative v positive schizophrenia. Definition and validation. Arch Gen Psychiatry. 1982;39(7):789–794.
95. Buchanan RW. Persistent negative symptoms in schizophrenia: an overview. Schizophr Bull. 2007;33(4):1013–1022.
96. Lee J, Takeuchi H, Fervaha G, et al. Subtyping schizophrenia by treatment response: antipsychotic development and the central role of positive symptoms. Can J Psychiatry. 2015;60(11):515–522.
97. Arango C, Garibaldi G, Marder SR. Pharmacological approaches to treating negative symptoms: a review of clinical trials. Schizophr Res. 2013;150(2–3):346–352.
98. Lindenmayer JP, Khan A, Iskander A, Abad MT, Parker B. A randomized controlled trial of olanzapine versus haloperidol in the treatment of primary negative symptoms and neurocognitive deficits in schizophrenia. J Clin Psychiatry. 2007;68(3):368–379.
99. Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31–41.
100. Mossaheb N, Kaufmann RM. Role of aripiprazole in treatment-resistant schizophrenia. Neuropsychiatr Dis Treat. 2012;8:235–244. doi:10.2147/NDT.S13830
101. Canuso CM, Bossie CA, Turkoz I, Alphs L. Paliperidone extended-release for schizophrenia: effects on symptoms and functioning in acutely ill patients with negative symptoms. Schizophr Res. 2009;113(1):56–64. doi:10.1016/j.schres.2009.05.021
102. Schreiner A, Bergmans P, Cherubin P, Hargarter L. The effect of long-acting paliperidone palmitate once-monthly on negative and depressive symptoms in patients with schizophrenia switched from previous unsuccessful treatment with oral aripiprazole. Ther Adv Psychopharmacol. 2017;7(2):59–65. doi:10.1177/2045125316673012
103. Beitinger R, Lin J, Kissling W, Leucht S. Comparative remission rates of schizophrenic patients using various remission criteria. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(7):1643–1651. doi:10.1016/j.pnpbp.2008.06.008
104. Shamsi S, Lau A, Lencz T, et al. Cognitive and symptomatic predictors of functional disability in schizophrenia. Schizophr Res. 2011;126(1–3):257–264. doi:10.1016/j.schres.2010.08.007
105. Rajji TK, Miranda D, Bh M. Cognition, function, and disability in patients with schizophrenia: a review of longitudinal studies. Can J Psychiatry Revue Canadienne De Psychiatr. 2014;59(1):13–17. doi:10.1177/070674371405900104
106. Harvey PD, Bellack AS. Toward a terminology for functional recovery in schizophrenia: is functional remission a viable concept? Schizophr Bull. 2009;35(2):300–306. doi:10.1093/schbul/sbn171
107. Valencia M, Fresan A, Barak Y, Juarez F, Escamilla R, Saracco R. Predicting functional remission in patients with schizophrenia: a cross-sectional study of symptomatic remission, psychosocial remission, functioning, and clinical outcome. Neuropsychiatr Dis Treat. 2015;11:2339–2348. doi:10.2147/NDT.S87335
108. Awad AG, Voruganti LN. The burden of schizophrenia on caregivers: a review. PharmacoEconomics. 2008;26(2):149–162. doi:10.2165/00019053-200826020-00005
109. Yazici E, Karabulut Ü, Yildiz M, et al. Burden on caregivers of patients with schizophrenia and related factors. Nöro Psikiyatri Arsivi. 2016;53(2):96–101. doi:10.5152/npa.2015.9963
110. Biagi E, Capuzzi E, Colmegna F, et al. Long-acting injectable antipsychotics in schizophrenia: literature review and practical perspective, with a focus on aripiprazole once-monthly. Adv Ther. 2017;34(5):1036–1048. doi:10.1007/s12325-017-0507-x
111. Mancevski B, Gogate J, Ashcroft K, Tardieu K, Kim E. Correlation of Caregiver Burden and Baseline Characteristics of Caregivers and Patients in Their Care with Recent-Onset Psychosis: the FIRST Study. Psychopharmacol Bull. 2017;47(3):17–25.
112. Fe Bravo-Ortiz M, Gutierrez-Casares JR, Rodriguez-Morales A, Garcia MA, Hidalgo-Borrajo R. Influence of type of treatment on the well-being of Spanish patients with schizophrenia and their caregivers. Int J Psychiatry Clin Pract. 2011;15(4):286–295. doi:10.3109/13651501.2011.608469
113. Carr CN, Hall CP, Roche-Desilets JE, Burant CJ, Fuller MA. Evaluation of adherence in patients prescribed long-acting injectable antipsychotics: A comparison of biweekly versus monthly administered neuroleptics. Ment Health Clin. 2016;6(5):248–253. doi:10.9740/mhc.2016.09.248
114. Meyers KJ, Upadhyaya HP, Landry JL, et al. Postinjection delirium/sedation syndrome in patients with schizophrenia receiving olanzapine long-acting injection: results from a large observational study. BJPsych Open. 2017;3(4):186–192. doi:10.1192/bjpo.bp.116.004382
115. Gentile S. Adverse effects associated with second-generation antipsychotic long-acting injection treatment: a comprehensive systematic review. Pharmacotherapy. 2013;33(10):1087–1106. doi:10.1002/phar.1313
116. Leucht S, Davis JM. Second-generation antipsychotics and quality of life in schizophrenia. Lancet Psychiatry. 2016;3(8):694–695. doi:10.1016/S2215-0366(16)30093-1
117. Ho C, Jones S. Three-Month Injectable Paliperidone Palmitate for the Treatment of Adults with Schizophrenia: A Review of Clinical Effectiveness, Safety, and Guidelines. Ottawa (ON); Canadian Agency for Drugs and Technologies in Health2017.
118. Gentile S. Safety concerns associated with second-generation antipsychotic long-acting injection treatment. A systematic update. Horm Mol Biol Clin Investig. 2017. doi:10.1515/hmbci-2017-0004
119. Parellada E, Bioque M. Barriers to the Use of long-acting injectable antipsychotics in the management of schizophrenia. CNS Drugs. 2016;30(8):689–701. doi:10.1007/s40263-016-0350-7
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.