")
Back to Journals » Clinical Ophthalmology » Volume 14
Clinical Profile of HLA-B27-Associated Uveitis in an Egyptian Cohort
Authors Abd El Latif E , Abdelhalim AS
Received 23 September 2020
Accepted for publication 21 October 2020
Published 10 November 2020 Volume 2020:14 Pages 3821—3828
DOI https://doi.org/10.2147/OPTH.S281860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eiman Abd El Latif,1 Ahmed Shawkat Abdelhalim2
1Department of Ophthalmology, Faculty of Medicine, Alexandria University, Alexandria, Egypt; 2Department of Ophthalmology, Faculty of Medicine, Minia University, Minia, Egypt
Correspondence: Eiman Abd El Latif
Department of Ophthalmology, Faculty of Medicine, Alexandria University, 5 Soliman Mahmoud Street, Cleopatra, Alexandria 12311, Egypt
Tel +20 211 4867-2963
Email [email protected]
Purpose: To describe the clinical profile of patients with HLA-B27-associated uveitis at 2 Egyptian tertiary eye centers.
Methods: A retrospective study reviewing the medical records of all patients with HLA-B27-associated uveitis served at 2 uveitis referral clinics in Egypt between January 2010 and June 2018.
Results: The study included a total of 554 patients. Anterior uveitis was the most common type. Ankylosing spondylitis was an important systemic comorbidity in the present study, affecting 27.4% of our patients. Cataract was the most frequent ocular complication. By the conclusion of the study, 6.1% of the affected eyes had a BSCVA poorer than 20/200.
Conclusion: The clinical profile of HLA-B27-associated uveitis in our cohort of Egyptian patients is similar to that reported from other regions of the world. In our study, a relatively high rate of cataract was observed.
Keywords: Egypt, uveitis, HLA-B27, epidemiology, hypopyon
Introduction
Uveitis, or intraocular inflammation, principally attacks the working-age population (20 to 50 years of age) and may cause major morbidity and economic burdens.1 Anterior uveitis is the most frequent subtype of uveitis, and it has been reported by some studies to represent up to 90% of all uveitis cases.2 The strong association between the genetic marker human leucocyte antigen (HLA)-B27 and anterior uveitis has been repeatedly published, albeit with geographic and ethnic variability in its prevalence. Values as low as 12% and as high as 88% have been reported regarding the positivity of HLA-B27 among patients with acute anterior uveitis (AAU).3–6
To date, the pathophysiology of HLA-B27-associated uveitis is still not completely understood. Moreover, patients have shown considerable variability with respect to the ocular features, the systemic comorbidities, as well as the response to the different treatment modalities.7,8
The aim of the current study is to describe the clinical profile of patients with HLA-B27-associated uveitis at 2 uveitis referral clinics in Egypt between January 2010 and June 2018.
Methods
In the present study, we retrospectively examined the medical records of patients with uveitis referred to 2 uveitis referral clinics in 2 densely populated Egyptian governorates, namely Alexandria and Minia, between January 2010 and June 2018. The study included all patients, of any age or sex, who visited the participating referral clinics between January 2010 and June 2018, and were diagnosed with HLA-B27-positive uveitis and fulfilled a minimum follow-up period of 12 months. Patients with a follow-up period of less than 12 months were excluded from the study. The study protocol was approved by the review boards of the participating institutions (Faculty of Medicine Research Ethics Committee, Minia University, Egypt and Ethics Committee, Faculty of Medicine, Alexandria University, Egypt). All participants provided written informed consent. The confidentiality of the patient’s data was strictly maintained and the study was carried out in compliance with the Declaration of Helsinki.
We followed the concepts published by the SUN Working Group9 in defining and grading intraocular inflammation. All the data in the current study were collected from medical files that were completed during the patients’ visits. The main data retrieved were the age of the patient both at the onset of uveitis and at the time of presentation to the study centers, the patient’s gender, the duration of follow-up at the referral clinics, the type and laterality of uveitis, the best spectacle corrected visual acuity (BSCVA) at both the initial visit and the final follow-up visit, the intraocular pressure, the slit lamp examination findings, the fundus examination findings, the laboratory test results, the imaging procedures performed and their results, and the type of treatment received. All patients had the following tests performed: complete blood count, erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody detection, rheumatoid factor detection, tuberculin test, syphilis serology, as well as X-ray of the chest. At the referral centers, all patients with non-granulomatous uveitis, without a prior test for HLA-B27 positivity were tested for its positivity. All patients were then evaluated by either a rheumatologist or a pediatric rheumatologist.
Topical prednisolone and topical cycloplegic drops were the mainstay of treatment for anterior uveitis. Subconjunctival injection was given in intense anterior segment inflammation not responding or not expected to respond timely to topical treatment, for fear of formation of extensive posterior synechiae. Posterior segment inflammation, cystoid macular edema, as well as ocular hypotony required the use of oral prednisolone. Sub-Tenon injection of triamcinolone acetonide was used in some cases of cystoid macular edema, at the discretion of the provider. Methotrexate was used in some oral prednisolone-resistant cases as well as a steroid-sparing agent. It was also given to patients with active systemic disease. Anti-tumor necrosis factor biological agents were prescribed by the rheumatologist mainly for patients with active systemic disease.
The measurements of the best spectacle corrected visual acuity were expressed as logarithm of the minimum angle of resolution (logMAR). And as previously described in the works of Lange C et al10 and Kwon YH et al,11 a best spectacle corrected visual acuity of counting fingers was expressed as 2.0 logMAR, and a best spectacle corrected visual acuity of hand movements was expressed as 2.3 logMAR. Light perception was converted into 2.6 logMAR, and no light perception into 2.9 logMAR.
The data of the study were tabulated and statistical analysis was performed using the statistical package for social sciences (version 20; SPSS Inc., Chicago, Illinois, USA). Continuous variables in the study were represented using descriptive statistics (mean, SD, and range), whereas categorical variables were expressed as frequencies [number (%)].
Results
Demographics and Clinical Characteristics of Patients
The present study involved a total of 789 eyes (of 554 patients) with HLA-B27-positive uveitis who met the inclusion criteria. Of these, 393 patients (70.9%) were known to be HLA-B27 positive by the time of referral, whereas the remaining 161 patients (29.1%) were diagnosed at the referral clinics. HLA-B27 positive patients represented 7.1% of all the uveitis population and 18.3% of the acute anterior uveitis population at the 2 participating centers during the study period, whereas they contributed to 1.5%, 2.8%, and 1.9% of our patients with intermediate uveitis, posterior uveitis, and panuveitis, respectively. Table 1 summarizes the demographic and clinical characteristics of the study cohort. The age of the patients at the time of their presentation to the referral centers participating in the study ranged from 16 to 77 years (mean 41.6 ± 8.1). Twenty one patients (3.8%) were younger than 18 years at the time of presentation. Males accounted for 68.2% of the study subjects (378 patients) versus 176 females (31.8%). All the patients in the current study were Arab. The mean follow-up period was 25.6 months (range: 12–73 months). At the time of referral, 341 patients (61.6%) had unilateral eye disease, and 213 patients (38.4%) had both eyes involved. During the period of follow-up, 22 patients presenting with unilateral involvement developed uveitis in the other eye, with a total number of patients with bilateral ocular involvement of 235, as per the end of the study period. The majority of those 235 patients with bilateral involvement (192 patients, 81.7%) had not experienced simultaneous bilateral episodes. There was no statistically significant difference in the follow-up time between patients who were referred with unilateral eye disease and patients who had both eyes involved at the time of referral.
 |
Table 1 Demographics and Clinical Characteristics of Patients with HLA-B27-Associated Uveitis |
Presenting Symptoms
In the current study, the authors reviewed the medical charts of the enrolled patients for the presenting symptoms that initially caused them to seek medical advice. The most frequent presenting symptom was pain (171 patients, 30.9%). This was followed by redness (163 patients, 29.4%), blurred vision (151 patients, 27.3%), and photophobia (69 patients 12.5%).
Ocular Findings and Complications
With respect to the anatomic location of intraocular inflammation, the most prevalent type was anterior uveitis, which was detected in 738 eyes (93.5%). Eight eyes had intermediate uveitis (1%), 7 eyes had posterior uveitis (0.9%), whereas 36 eyes suffered from panuveitis (4.6%). The most prevalent clinical anterior segment findings were anterior chamber reaction, which was noted in all eyes that were examined during an acute episode of anterior uveitis, and posterior synechiae, which was noted, with a variable extent, in 511 eyes (64.8%) at the time of presentation to the participating centers and developed de novo in another 68 eyes (8.6%) during the period of the study. With respect to the posterior segment findings, macular edema was observed in 101 eyes (12.8%), and vitreous cells were observed in 51 eyes (6.5%). Three patients in the present report had retinal vasculitis. One of them had bilateral retinal phlebitis with unilateral central retinal vein occlusion, another patient had unilateral retinal phlebitis with branch retinal vein occlusion, and the third patient had unilateral retinal vasculitis that involved both the arteries and the veins and was associated with ipsilateral branch retinal artery occlusion. Evaluation was made both clinically and with fundus fluorescein angiography. Ocular findings and complications encountered in our cohort of patients are summarized in Table 2.
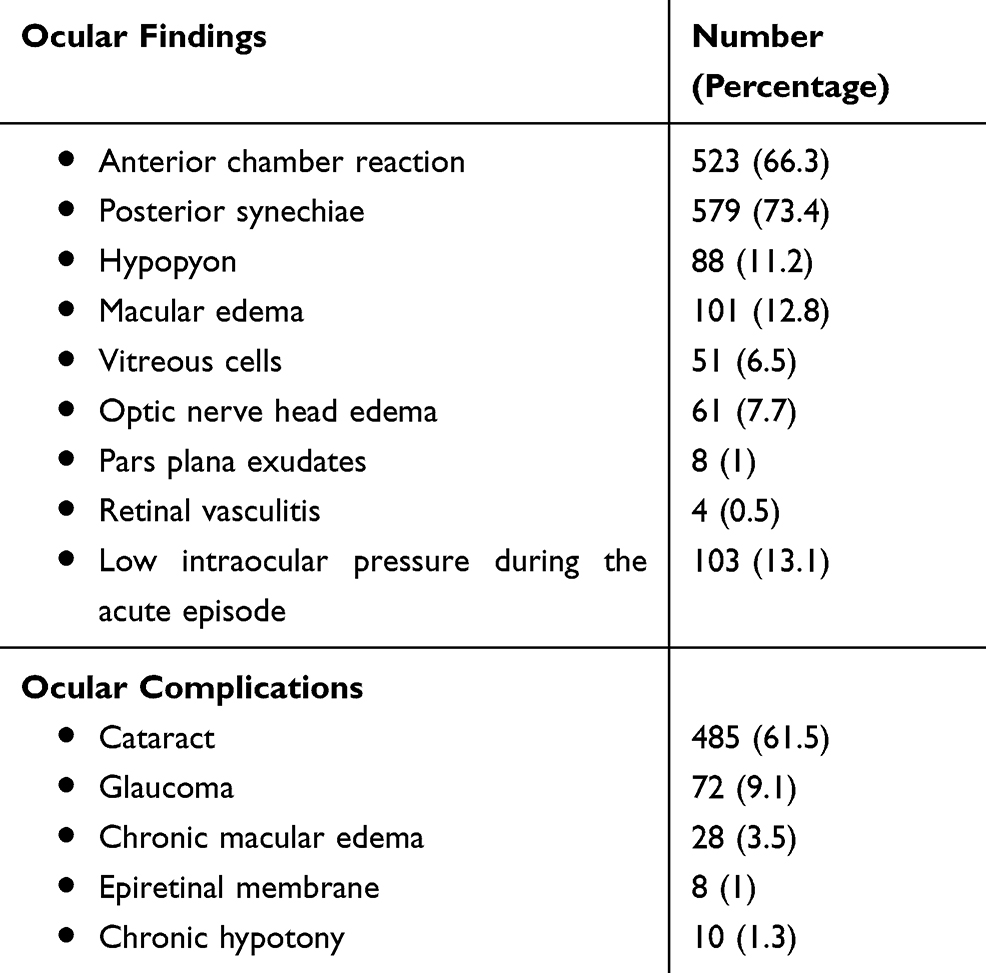 |
Table 2 Ocular Findings and Complications in Patients with HLA-B-27 Associated Uveitis (N = 789 Eyes) |
Systemic Associations
A history of low back pain was given by 257 patients (46.4%), 188 of whom (73.2%), experienced low back pain before the onset of ocular disease. Other systemic symptoms included peripheral (non-axial) joint pain (101 patients, 18.2%), and disturbed bowel habits (23 patients, 4.2%). Ankylosing spondylitis was diagnosed by a rheumatologist in 152 patients (27.4%), Crohn’s disease was diagnosed in 12 patients (2.2%), and 51 patients (9.2%) were diagnosed as undifferentiated spondyloarthropathy. For the remaining 339 patients (61.2%), no relevant systemic comorbidity was diagnosed as per the end of the study. Thirty-one patients in the current report had posterior segment inflammation and specifically among this subgroup of patients, 7 patients were diagnosed as ankylosing spondylitis, 4 patients were diagnosed as Crohn’s disease, and another 4 patients were diagnosed as undifferentiated spondyloarthropathy, whereas no particular systemic disease could be identified among the remaining 16 patients, Table 3.
 |
Table 3 Systemic Associations in Patients with HLA-B27-Associated Uveitis |
Treatment
The mainstay of treatment of acute attacks of anterior uveitis was topical prednisolone and topical cycloplegic drops. The frequency of instillation of eye drops depended upon the severity of inflammation. In conjunction with topical treatment, 49 eyes (6.2%) with intense anterior segment inflammation, received subconjunctival injection. Oral prednisolone was prescribed, for variable durations, to a total of 63 patients (11.4%), for either vision-threatening uveitis, cystoid macular edema, or ocular hypotony, or for systemic disease. Thirteen eyes in our study (1.6%) received sub-Tenon injection of triamcinolone acetonide for cystoid macular edema. In the current retrospective chart review, we found that methotrexate was given to a total of 134 patients (24.2%), by the rheumatologist, at some point of time, mainly for active systemic disease, and less frequently for sight-threatening uveitis in patients not responding adequately to systemic steroids, intolerant to the side effects of steroids, and as steroid-sparing agents. Biological agents in the form of the anti-tumor necrosis factor Infliximab and Adalimumab were administered by the rheumatologist to 14 patients (2.5%), for systemic indications.
The most common ocular complication was cataract, which developed in 485 eyes (61.5%), to a variable density and visual significance (Table 2). About one-fourth of these eyes had undergone cataract extraction by the end of the study period (118 eyes). An elevated intraocular pressure was encountered in 72 eyes (9.1%), 60 of them responded to topical tension-lowering drops alone, another 9 eyes required an additional short course of systemic acetazolamide and 2 eyes required trabeculectomy. Pars plana vitrectomy was performed on 5 eyes with an epiretinal membrane and chronic macular edema.
Visual Outcome
At the time of their presentation to the participating centers, 341 patients had strictly unilateral uveitis and 213 patients had both eyes affected, making a total of 767 eyes. The average visual acuity was 0.66 logMAR±0.47, and 117 eyes (15.3%) had a best-corrected visual acuity >1.00 logMAR (<20/200). Throughout the study, another 22 patients who had initially presented with unilateral involvement, had their sound eye involved, increasing the total number of affected eyes included in the study to 789 eyes. During the period of the study, the average frequency of relapses per year was 1.24±0.8, and the average interval between relapses was 0.85±0.65 years. By the final visit considered in the study, the average final visual acuity of the involved eyes improved to 0.27logMAR ±0.91and only 48 eyes had a best-corrected visual acuity >1.00 logMAR (<20/200), 37 of which had cataract which had not been extracted by the time the current retrospective chart review was concluded.
Discussion
The strong relationship between HLA-B27 positivity and inflammatory diseases such as uveitis, and spondyloarthropathies, particularly ankylosing spondylitis, has been known for more than 4 decades.3,12 One mechanism HLA-B27 can cause uveitis is by disturbing the intestinal microbiome composition, resulting in loss of intestinal tolerance and loss of ocular immune privilege, thereby facilitating uveitis.
In the present report, HLA-B27-positive patients represented 7.1% of the total uveitis population and 18.3% of the acute anterior uveitis population at the 2 centers participating in the study. These findings agree with the results of a previous report from Egypt13 and are similar to the percentages reported from USA14,15 and Southern Europe.16 (The prevalence of HLA-B27 in the Egyptian population was reported to be 4.7%17, slightly lower than an overall prevalence of HLA-B27 of 6.1% reported from the USA18). Lower rates were published by some studies from Lebanon,19 Saudi Arabia,20–22 and Northern Europe,23,24 whereas higher percentages were reported from Japan.25 This variation may in part be explained by the variation in the prevalence of HLA-B27 in the general population in different regions of the world. It is worth noting that HLA-B27-positive patients represented minor subsets of our patients with intermediate uveitis, posterior uveitis, and panuveitis (1.5%, 2.8%, and 1.9%, respectively). Nevertheless, due to relative scarcity of data from Egypt, the authors are not certain whether these values reflect community incidence.
Several studies have shown that the typical HLA-B27-associated uveitis is anterior and either unilateral or showing alternation of activity between both eyes, whereas simultaneous bilateral activity is uncommon.6,26,27 In agreement with these studies, the most prevalent type of uveitis in our study, with respect to its anatomic location, was anterior uveitis, with which 93.5% of the studied eyes were affected. And with respect to the laterality of intraocular inflammation, in more than half of our patients (319 patients, 57.6%), ocular disease remained strictly unilateral and their other eye was not involved at least till the end of the study. In another 34.7% of our cohort, non-simultaneous activity in both eyes was the rule throughout their disease history, and only 7.8% experienced simultaneous bilateral activity at one or more points of time. About two-thirds of our patients (68.2%) were males, in agreement with the larger body of literature on HLA-B27-uveitis that reported male predominance. Few studies, though, reported slight prevalence in females.28
A growing body of literature is describing the incidence and pattern of posterior segment manifestations in patients with HLA-B27-associated uveitis. A wide range of posterior segment findings have been described, including macular edema, optic disc edema, epiretinal membrane and pars plana exudates, vitritis and retinal vasculitis. Our rates of posterior segment findings are not far from those published by other authors.29–31
Macular edema, in particular, could be either a part of a genuine posterior segment inflammation, or a mere complication of moderate to severe anterior uveitis.32 In our study, macular edema was found in 101 eyes with HLA-B27-associated uveitis (12.8%), 73 of which had macular edema in the context of significant anterior segment inflammation, whereas in the remaining 28 eyes, macular edema coexisted with signs of true posterior segment involvement as dense vitritis, pars plana exudates, and retinal vasculitis. Similar rates of macular edema in eyes with HLA-B27-associated uveitis have been reported by other studies.13,33,34.
The prevalence of ankylosing spondylitis among patients with HLA-B27-associated uveitis in the literature ranges from 22% to 39%.13,34,35 In agreement with these data, ankylosing spondylitis was diagnosed in 27.4% of patients in our series, as per the end of the study. The second most commonly diagnosed systemic disease among our patients was undifferentiated spondyloarthropathy (9.2%). However, the fact that in HLA-B27-positive patients, uveitis can precede the onset of spondylitis by an average of about 8 years,3,8,35,36 raises the possibility that a study with a longer follow-up period may reveal a higher prevalence of systemic comorbidity and renders it necessary to periodically review those patients’ systemic symptoms and signs, and particularly in patients with posterior segment inflammation who appeared to be idiopathic by the end of the study period, we could not determine with certainty whether HLA-B27 positivity was incidental or integral to their posterior segment inflammation.
It is also perhaps worth noting that 3 of our patients had retinal vasculitis. In 2 patients, the pattern of vasculitis observed was periphlebitis with manifestations of venous occlusion, and those 2 patients had Crohn’s disease. The association between Crohn’s disease and retinal vasculitis has been published before.37,38 For the third patient, on the other hand, no specific systemic comorbidity was identified by the last visit considered in the current chart review. He had unilateral combined arterial and venous inflammation associated with branch retinal artery occlusion.
Acute episodes of anterior uveitis associated with HLA-B27 positivity generally respond favorably to topical steroids, as have been previously published.6,8 In agreement with the literature in this respect, topical steroids were the principal treatment of acute anterior uveitis in our study. In our series, subconjunctival injection was viewed necessary in only 6.2% of our patients’ eyes, approximately half the percentage reported by a study from turkey,8 and oral steroids were given to 11.4% of our patients, which is nearer to the lower end of the range of values published from other areas of the world (8.8%8 – 48.8%2). About one-fourth of the patients received methotrexate whereas as few as 2.5% of our whole cohort received biologic agents, both of which were prescribed and supervised by the rheumatologists. The relatively scarce prescription of biologic agents in the current study might be attributed in part to, their high cost in relation to the patients’ socioeconomic status, to local cultural barriers against this modality of treatment, as well as to the prevalence of tuberculosis in some areas, and of active infectious hepatitis especially our overwhelming national problem of hepatitis C and its hepatic complications, before the national campaign against hepatitis C launched in 2018.
Cataract was observed in 61.5% of eyes in the present study, but only 24.3% of these eyes had their cataract visually significant in a quiescent eye and warranted surgery, by the last follow-up visit. Majumdar et al2 reported a slightly higher 67.2% prevalence of cataract in their series. They attributed this to the delayed presentation, a relatively higher rate of recurrences, and a relatively higher use of systemic steroids, upon comparison to other studies. On the other hand, lower values of cataract development were published by other authors, where Park et al,39 Rothova et al,26 and Power et al34 published the development of cataract in 5.7%, 12.4%, and 22.7% of eyes with uveitis in HLA-B27-positive patients, respectively. Regarding the intraocular pressure, the percentage of eyes that developed secondary elevation of the intraocular pressure in our series (9.1%) approached those from other studies.2,29,34 At the other end of the spectrum, acute attacks of HLA-B27-associated uveitis could be associated with a temporary decrease of intraocular pressure, as have been previously reported,8 and this was reinforced in 13.1% of eyes in our study. Chronic hypotony in those eyes, however, is much less common,40,41 and in our series, 1.3% of the study eyes had not recovered from hypotony, by the last follow-up visit. The final best corrected visual acuity of eyes with HLA-B27-associated uveitis is generally good,42 and only 6.1% of the affected eyes we studied had a final BCVA < 20/200. It is worth noting that 37 of these eyes suffered from cataract but had not undergone cataract extraction by the time the present retrospective chart review was concluded, which raises the possibility of reporting a better final visual outcome should a longer follow-up be conducted.
Limitations of the current study include those inherent to its retrospective nature as well as the variable follow-up intervals. Moreover, being conducted in referral centers, a referral bias may also affect its results. It is possible that the more complicated cases and the cases of a poorer prognosis were preferentially referred to the participating centers, compared to the less severe cases.
In conclusion, most of the data from this report from Egypt agree with the data published from other parts of the world about HLA-B27-associated uveitis. Uveitis was most commonly anterior and basically unilateral or alternating. Ankylosing spondylitis was diagnosed in over a quarter of our patients. Anterior uveitis responded well to topical treatment in the majority of cases. A relatively low rate of biologic therapy utilization is observed in our country. We had a high prevalence of cataract in the present review, but nevertheless, the final visual results were favorable.
Funding
There is no funding to report.
Disclosure
Neither author has a financial or proprietary interest in any material or method mentioned. The authors report no conflicts of interest for this work.
References
1. Suttorp-Schulten MS, Rothova A. The possible impact of uveitis in blindness: a literature survey. Br J Ophthalmol. 1996;80:844–848. doi:10.1136/bjo.80.9.844
2. Majumdar AK, Kumar A, Roy R, et al. Clinical profile of HLA-B27-associated uveitis patients in a tertiary care eye hospital in eastern India. Ocul Immunol Inflamm. 2018:1–4. doi:10.1080/09273948.2018.1484491
3. Brewerton D, Caftrey M, Nicholls A, Walters D, James DCO. Acute anterior uveitis and HLA B27. Lancet. 1973;2(7836):994–996. doi:10.1016/S0140-6736(73)91090-8
4. McCannel CA, Holland GN, Helm CJ, et al. Causes of uveitis in the general practice of ophthalmology. UCLA Community-Based Uveitis Study Group. Am J Ophthalmol. 1996;121(1):35–46. doi:10.1016/S0002-9394(14)70532-X
5. Chang JH, McCluskey PJ, Wakefield D. Acute anterior uveitis and HLA-B27. Surv Ophthalmol. 2005;50(4):364–388. doi:10.1016/j.survophthal.2005.04.003
6. Accorinti M, Iannetti L, Liverani M, et al. Clinical features and prognosis of HLA B27-associated acute anterior uveitis in an Italian patient population. Ocul Immunol Inflamm. 2010;18(2):91–96. doi:10.3109/09273941003597268
7. Wakefield D, Chang JH, Amjadi S, et al. What is new HLA-B27 acute anterior uveitis? Ocul Immunol Inflamm. 2011;19(2):139–144. doi:10.3109/09273948.2010.542269
8. Inanc M, Şimşek M, Ozdal MPC. Etiological and clinical characteristics of HLA-B27-associated uveitis in a tertiary referral center. Turk J Ophthalmol. 2019;49(1):10–14. doi:10.4274/tjo.galenos.2018.53896
9. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509–516.
10. Lange C, Feltgen N, Junker B, et al. Resolving the clinical acuity categories “hand motion” and “counting fingers” using the Freiburg Visual Acuity Test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):137–142. doi:10.1007/s00417-008-0926-0
11. Kwon YH, Kim CS, Zimmerman MB, et al. Rate of visual field loss and long-term visual outcome in primary open-angle glaucoma. Am J Ophthalmol. 2001;132(1):47–56. doi:10.1016/S0002-9394(01)00912-6
12. Brewerton DA, Hart FD, Nicholls A, et al. Ankylosing spondylitis and HLA B27. Lancet. 1973;301(7809):904–907. doi:10.1016/S0140-6736(73)91360-3
13. Abd El Latif E, Ammar H. Uveitis referral pattern in upper and lower Egypt. Ocul Immunol Inflamm. 2019;27(6):875–882. doi:10.1080/09273948.2017.1410183
14. Chang JH-M, Wakefield D. Uveitis: a global perspective. Ocul Immunol Inflamm. 2002;10:263–279. doi:10.1076/ocii.10.4.263.15592
15. Rodriguez A, Calonge M, Pedroza-Seres M, et al. Referral patterns of uveitis in a tertiary eye care center. Arch Ophthalmol. 1996;114(5):593–599. doi:10.1001/archopht.1996.01100130585016
16. Pivetti-Pezzi P, Accorinti M, La Cava M, et al. Endogenous uveitis: an analysis of 1417 cases. Ophthalmologica. 1996;210(4):234–238. doi:10.1159/000310715
17. Ziade NR. HLA B27 antigen in Middle Eastern and Arab countries: systematic review of the strength of association with axial spondyloarthritis and methodological gaps. BMC Musculoskelet Disord. 2017;18(1):280. doi:10.1186/s12891-017-1639-5
18. Reveille JD, Hirsch R, Dillon CF, et al. The prevalence of HLA-B27 in the US: data from the US National Health and Nutrition Examination Survey, 2009. Arthritis Rheum. 2012;64(5):1407–1411. doi:10.1002/art.33503
19. Abdulaal M, Antonios R, Barikian A, et al. Etiology and clinical features of ocular inflammatory diseases in a tertiary center in Lebanon. Ocul Immunol Inflamm. 2014;9:1–7.
20. Al Dhahri H, Al Rubaie K, Hemachandaran S, et al. Patterns of uveitis in a university-based tertiary referral center in Riyadh, Saudi Arabia. Ocul Immunol Inflamm. 2014;24:1–9.
21. Nizamuddin SH, Bawazeer AM. Causes of uveitis in a tertiary center in Western Saudi Arabia. Saudi Med J. 2013;34:379–387.
22. Bawazeer AM, Joharjy HI. The association of human leukocyte antigen B27 with anterior uveitis in patients from the western region of Saudi Arabia: a retrospective study. Clin Ophthalmol. 2013;7:2107–2111. doi:10.2147/OPTH.S53518
23. Paivonsalo-Hietanen T, Vaahtoranta-Lehtonen H, Tuominen J, et al. Uveitis survey at the University Eye Clinic Turku. Acta Ophthalmol. 1994;72:505–512. doi:10.1111/j.1755-3768.1994.tb02805.x
24. Thean LH, Thompson J, Rosenthal AR. A uveitis register at the Leicester royal infirmary. Ophthal Epidemiol. 1996;3:151–158. doi:10.3109/09286589609080121
25. Kotake S, Furudate N, Sasamoto Y, et al. Characteristics of endogenous uveitis n Hokkaido, Japan. Graefes Arch Clin Exp Ophthalmol. 1997;235(1):5–9. doi:10.1007/BF01007830
26. Rothova A, Van Veenedaal WG, Linssen A, et al. Clinical features of acute anterior uveitis. Am J Ophthalmol. 1987;103(2):137–145. doi:10.1016/S0002-9394(14)74218-7
27. Pathanapitoon K, Suksomboon S, Kunavisarut P, et al. HLA-B27-associated acute anterior uveitis in the university referral centre in North Thailand: clinical presentation and visual prognosis. Br J Ophthalmol. 2006;90(12):1448–1450. doi:10.1136/bjo.2006.099788
28. Kazokoglu H, Onal S, Tugal-Tutkun I, et al. Demographic and clinical features of uveitis in tertiary centers in Turkey. Ophthalmic Epidemiol. 2008;15(5):285–293. doi:10.1080/09286580802262821
29. Rodriguez A, Ya A, Pedroza-Seres M, et al. Posterior segment ocular manifestations in patients with HLA-B27-associated uveitis. Ophthalmology. 1994;101:1267–1274. doi:10.1016/S0161-6420(94)31179-1
30. Sanghvi C, Mercieca K, Jones NP. Very severe HLA-B27-associated panuveitis mimicking endophthalmitis: a case series. Ocul Immunol Inflamm. 2010;18(2):139–141. doi:10.3109/09273940903560236
31. Braakenburg AM, Rothova A. The clinical characteristics of retinal vasculitis in HLA-B27-positive patients. Ocul Immunol Inflamm. 2014;22(3):197–202. doi:10.3109/09273948.2013.835429
32. Pathanapitoon K, Dodds EM, Jr ET C, et al. Clinical spectrum of HLA-B27-associated ocular inflammation. Ocul Immunol Inflamm. 2017;25(4):569–576. doi:10.1080/09273948.2016.1185527
33. Valls Pascual E, Fontanilla Ortega P, Vicens Bernabeu E, et al. Clinical characteristics, treatment and ocular complications of HLA-B27-related anterior uveitis and HLA-B27-non related anterior uveitis. Reumatol Clin. 2016;12(5):244–247. doi:10.1016/j.reuma.2015.11.008
34. Power WJ, Rodriguez A, Pedroza-Seres M, et al. Outcomes in anterior uveitis associated with the HLA-B27 haplotype. Ophthalmology. 1998;105(9):1646–1651. doi:10.1016/S0161-6420(98)99033-9
35. Tay-Kearney M, Schwam BL, Lowder C, et al. Clinical features and associated systemic diseases of HLA-B27 uveitis. Am J Ophthalmol. 1996;121(1):47–56. doi:10.1016/S0002-9394(14)70533-1
36. Wakefield D, Easter J, Penny R. Clinical features of HLA-B27 anterior uveitis. Aust J Ophthalmol. 1984;12(3):191–196. doi:10.1111/j.1442-9071.1984.tb01155.x
37. Duker JS, Brown GC, Brooks L. Retinal vasculitis in Crohn’s disease. Am J Ophthalmol. 1987;103:664–668. doi:10.1016/S0002-9394(14)74326-0
38. Ruby AJ, Jampol LM. Crohn’s disease and retinal vascular disease. Am J Ophthalmol. 1990;110:349–353. doi:10.1016/S0002-9394(14)77013-8
39. Park SC, Ham D-I. Clinical features and prognosis of HLA-B27 positive and negative anterior uveitis in a Korean population. J Korean Med Sci. 2009;24(4):722–728. doi:10.3346/jkms.2009.24.4.722
40. Roe R, Branco BC, Cunningham ET. Hypotony maculopathy in a patient with HLA-B27-associated uveitis. Ocul Immunol Inflamm. 2008;16(3):107–108. doi:10.1080/09273940802023794
41. Van Der Veer EG, Keunen JE, Rothova RA. Severe HLA B27-associated uveitis complicated by hypotony, serous retinal detachment, and ciliochoroidal effusion. Ocul Immunol Inflamm. 2014;22(1):23–26. doi:10.3109/09273948.2013.828081
42. D’Ambrosio EM, La Cava M, Tortorella P, et al. Clinical features and complications of the HLA-B27-associated acute anterior uveitis: a metanalysis. Semin Ophthalmol. 2016. doi:10.3109/08820538.2016.1170158
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.