")
Back to Journals » Nature and Science of Sleep » Volume 14
Clinical Predictors of Mixed Apneas in Patients with Obstructive Sleep Apnea (OSA)
Authors Liu P , Chen Q, Yuan F, Zhang Q, Zhang X, Xue C, Wei Y, Wang Y, Wang H
Received 30 November 2021
Accepted for publication 18 February 2022
Published 5 March 2022 Volume 2022:14 Pages 373—380
DOI https://doi.org/10.2147/NSS.S351946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ahmed BaHammam
Pengfei Liu,1,* Quanhui Chen,1,* Fang Yuan,2 Qingru Zhang,1 Xiaoying Zhang,1 Chan Xue,1 Yuqing Wei,1 Yakun Wang,1 Hanqiao Wang1,2
1Department of Sleep Medicine, The Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Physiology, Hebei Key Laboratory of Neurophysiology, Shijiazhuang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hanqiao Wang, Department of Sleep Medicine, The Third Hospital of Hebei Medical University, Shijiazhuang, 050051, Hebei, People’s Republic of China, Tel +86 18533112218, Email [email protected]
Purpose: Mixed events in obstructive sleep apnea (OSA) patients (mixed-OSA) indicate respiratory regulation instability and are essential for OSA pathogenesis and prognosis. It also shows a decreased compliance with continuous positive airway pressure (CPAP). Using predictors to identify mixed-OSA has significant clinical guidance for OSA precise diagnosis and treatment. This study aimed to establish a simple and accessible method for rapid screening of mixed-OSA, thus promoting OSA precise diagnosis.
Patients and Methods: A total of 907 patients with suspected OSA were screened, of which 513 OSA patients, including 344 with pure-OSA and 169 with mixed-OSA, were finally included in the study. The clinical characteristics and polysomnography (PSG) parameters of the two OSA groups were compared. Multivariate logistic regression analysis was used to investigate the factors affecting the morbidity of mixed-OSA. The receiver operating characteristic (ROC) curve was used to explore if some convenient PSG parameters can be used to predict mixed-OSA.
Results: About 33% of OSA patients were identified as mixed-OSA. Multivariate logistic regression analysis showed that apnea hypopnea index (AHI) and lowest oxygen saturation (LSO2) were independently associated with mixed-OSA after adjusting for age, sex, body mass index (BMI), smoking, drinking, hypertension, and Epworth Sleepiness Score (ESS) (AHI: OR=1.046, 95% CI 1.032– 1.060, P < 0.001; LSO2: OR=0.958, 95% CI 0.936– 0.981, P < 0.001). ROC curve analysis showed that AHI > 47 or LSO2 < 77% indicated mixed-OSA. The sensitivity and specificity of AHI> 47 was 0.952 and 0.652, respectively, and 0.822 and 0.675 for LSO2 < 77%, respectively.
Conclusion: Our research found that AHI > 47 or LSO2 < 77% are independently associated with mixed-OSA and can be used to quickly identify the occurrence of mixed-OSA. Therefore, this study can help detect mixed-OSA and precise individual diagnosis of OSA patients.
Keywords: mixed events, apnea hypopnea index, lowest saturation, precise individual diagnosis
Introduction
Obstructive sleep apnea (OSA) significantly impacts human health and has a high and increasing prevalence worldwide.1–5 A previous study found that untreated OSA is related to increased mortality in patients with heart failure.6 Therefore, it is necessary to screen OSA patients for early treatment to improve OSA-related chronic diseases and health levels of the general population. Studies have confirmed that continuous positive airway pressure (CPAP) is among the widely accepted methods for improving OSA symptoms.7–12 Nevertheless, the acceptability and adherence of patients to CPAP have different and unsatisfactory responses, affecting its effectiveness.13–16 Low CPAP compliance and non-individualized diagnosis and treatment cause varying damages to the target organ in OSA patients.17,18 The occurrence of mixed events in OSA patients (mixed-OSA) was related to the stability of the ventilatory control and the severity of the disease. Studies had demonstrated that mixed-OSA was associated with more complex sleep apnea, less optimal therapy, higher titrated CPAP and lower compliance to CPAP.19,20 Therefore, it is necessary to do an early screening of mixed-OSA for precise OSA diagnosis and treatment. Some PSG parameters used to describe OSA can be used as predictors to identify mixed-OSA patients.
This study investigated the clinical features of mixed-OSA and pure-OSA patients. Moreover, the incidence of mixed-OSA was predicted using apnea hypopnea index (AHI) and lowest oxygen saturation (LSO2), which are the main parameters in portable polysomnography (PSG). This study aimed to establish a simple and accessible method for rapid screening of mixed-OSA, thus promoting OSA precise diagnosis.
Materials and Methods
Study Design and Subject
Data from 907 patients were obtained from the Third Hospital of Hebei Medical University between Jan 25, 2017, and Aug 1, 2020. Inclusion criteria were: (1) patients aged ≥ 18 years old; (2) patients completing an overnight PSG; (3) patients with an initial diagnosis of OSA and did not receive any treatment before admission; (4) patients with pure-OSA (no central part of the whole event) or mixed-OSA (the duration of the central part more than 10 seconds and less than 80% of the whole event); (5) patients with mixed sleep apnea index (MAI) ≥ 5. Exclusion criteria were: (1) patients with MAI < 5; (2) patients with central sleep apnea (no obstructive part of the whole event or the duration of the central part more than 80%) index (CAI) >5, or CAI > obstructive sleep apnea index (OAI), or the occurrence of Cheyne-Stokes respiration (CSR); (3) patients with other sleep disorders, such as insomnia, narcolepsy, periodic leg movement, and restless legs syndrome; (4) patients with other diseases or taking drugs that can affect sleep and daytime sleepiness; (5) patients with incomplete data. A total of 223 of 907 patients had a CAI > 5, CAI > OAI, and CSR presence. A total of 171 of the remaining 684 patients had a MAI ranging from 0 to 5 and were excluded from the analysis. Eventually, 513 OSA patients were included in the study. Based on the MAI, the patients were further divided into pure-OSA and mixed-OSA groups (344 and 169, respectively). The Ethics Committee of the Third Hospital of Hebei Medical University approved this study (No. Science2020-037-1), and each patient signed informed consent. The information that could cause privacy disclosure was concealed during data collection.
Definition of Pure-OSA and Mixed-OSA
A generally recognized criterion, AHI ≥5 (which was scored according to the American Academy of Sleep Medicine (AASM), 2007 criteria), was used to define OSA.12,21 OSA patients were further screened based on MAI. OSA patients with an MAI = 0 were classified as a pure-OSA group, and those with MAI ≥ 5 were classified as mixed-OSA group based on the criteria used in previous literature.20,22
Polysomnography
All patients underwent overnight standard PSG (EMBLA S4500, USA), including electroencephalography (the recording electrodes were placed according to the international 10/20 system), submental electromyography, electrooculography, and electrocardiography. Thoracoabdominal movements and airflow were recorded using respiratory inductance plethysmography and an oronasal thermistor. A position sensor was used to monitor the positions of patients. A pulse oximeter (Nonin, USA) fixed on the middle finger was used to detect oxygen saturation continuously during sleep. An infrared video camera was used to record the behaviors of patients throughout the night.
The scoring of sleep stages and respiratory events was conducted based on the AASM Manual for the Scoring of Sleep and Associated Events. A technician with more than ten years of work experience on PSG scoring provided rules, terminologies, and technical specifications. Apnea events were defined as the absence of oronasal airflow that persisted for more than 10 seconds. Mixed apnea was defined as a central event that persisted for more than 10 seconds in the beginning, with an obstructive subsequent event type and the duration of the central part less than 80% of the whole event. Hypopnea events were defined as the occurrence of a more than 50% decrease in airflow from the baseline for more than 10 seconds and simultaneous oxygen saturation decline ≥3% from the baseline.
Data Collection
Clinical data of patients, including age, sex, body mass index (BMI), Epworth Sleepiness Score (ESS), history of smoking and drinking, diabetes, hypertension, hyperlipidemia, coronary heart disease (CHD), cerebrovascular diseases (CVD), were obtained from the medical records. The PSG parameters, including total sleep time (TST), sleep efficiency (SE), sleep latency (SLT), rapid eye movement sleep (REM) latency (RSLT), percentage of non-rapid eye movement (NREM), sleep stage 1, 2 and 3 (N1, N2, and N3), percentage of REM sleep, arousal index (ArI), AHI, CAI, OAI, MAI, mean saturation (MSO2), and LSO2 were recorded and analyzed.
Statistical Analyses
SPSS 22.0 software (IBM Corp., NY, USA) was used for statistical analyses. A normality test was conducted before statistical comparisons. Continuous variables with normal distribution are expressed as mean ± standard deviation. Between-group comparisons were conducted using an independent sample t-test. Non-normally distributed data were expressed as median (first quartile, third quartile) and were compared using the Mann–Whitney U method. Enumeration data were expressed as numbers (proportion) of cases, and the differences in constituent ratios between the two groups were assessed using the chi-square test. Multivariate logistic regression analysis was used to determine the association between AHI and LSO2 and the morbidity of mixed-OSA. Receiver operating characteristic (ROC) curves were used to determine the cut-off values of AHI and LSO2 for predicting the mixed-OSA. P < 0.05 was considered as the statistically significant difference.
Results
A total of 513 of 907 OSA patients were included in this study. The patients were divided into the pure-OSA group (n=344) and the mixed-OSA group (n=169). The average age of patients in the pure-OSA and mixed-OSA groups was 47.8±12.3 and 49.2±10.6 years, respectively. The two groups had no significant difference in age. The proportion of males was significantly higher in mixed-OSA (94.7%) than in pure-OSA (78.2%, P < 0.001, Table 1). Similarly, the percentage of smoking, drinking, and hypertension were higher in the mixed-OSA group (smoking: P < 0.05, drinking: P < 0.001, hypertension: P < 0.01, Table 1) than in pure-OSA. Mixed-OSA Patients also had higher BMI and ESS (BMI: P < 0.001, ESS: P < 0.001, Table 1) than pure-OSA patients. The two groups had no significant differences in the proportion of patients with diabetes, hyperlipidemia, CHD, and CVD.
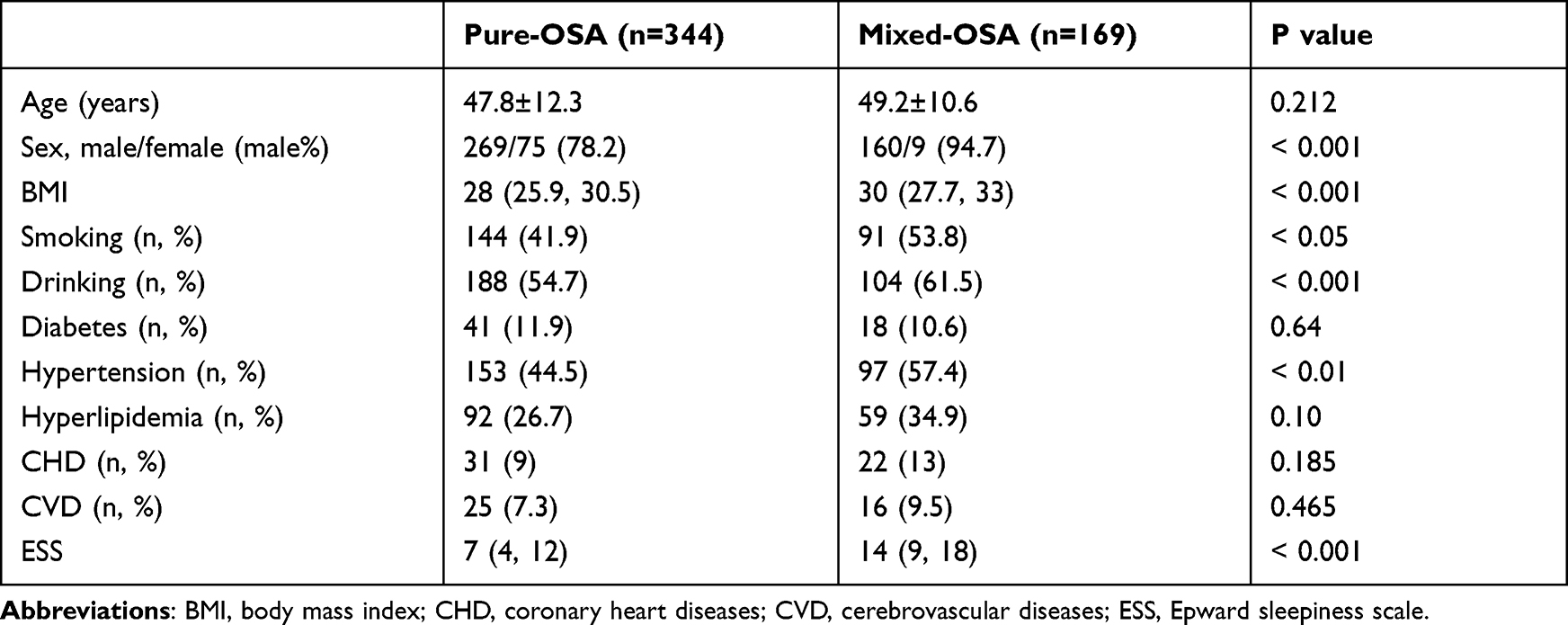 |
Table 1 Clinical Characteristics of Patients with Pure-OSA and Mixed-OSA |
Sleep quality, respiratory events, and oxygen saturation were assessed using the PSG data of the two OSA subgroups to clarify the distinctive characteristics of mixed-OSA patients further. Mixed-OSA patients had a significantly increased AHI and decreased MSO2 and LSO2 compared with pure-OSA patients (P < 0.001, Table 2).
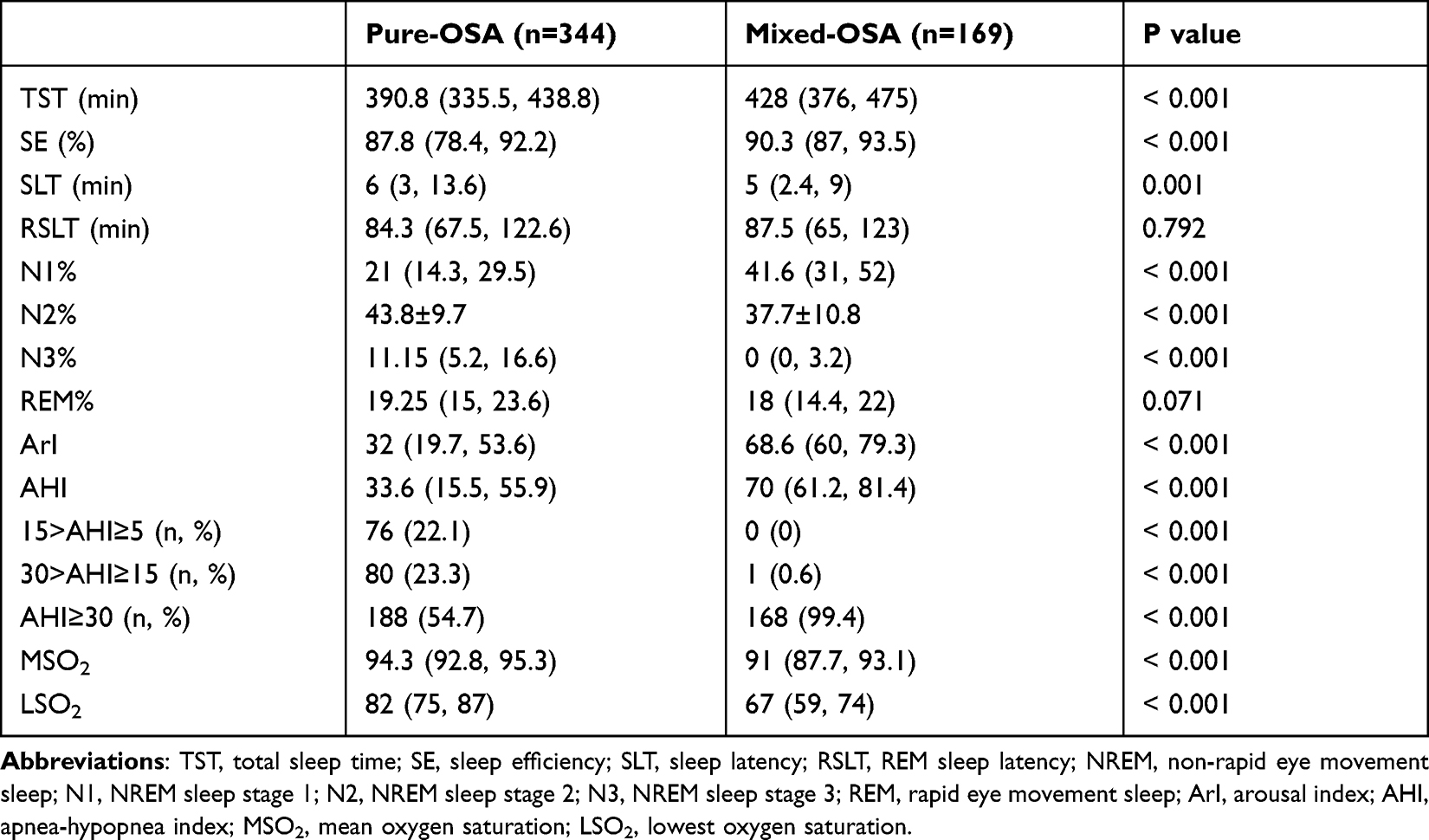 |
Table 2 Sleep Characteristics of OSA Patients with Pure-OSA and Mixed-OSA |
This study further explored the role of AHI and LSO2 in the morbidity of mixed-OSA. This study showed that sex, BMI, and ESS were associated with mixed-OSA, consistent with previous studies (P < 0.01, Table 3).20,23 Multivariate logistic regression analysis also showed that AHI and LSO2 were independently and significantly associated with mixed-OSA after adjusting for age, sex, BMI, smoking, drinking, hypertension, and ESS (AHI: OR=1.046, 95% CI 1.032–1.060, P < 0.001; LSO2: OR=0.958, 95% CI 0.936–0.981, P < 0.001, Table 3). AHI and LSO2 were positively and negatively related to the incidence of mixed-OSA, respectively.
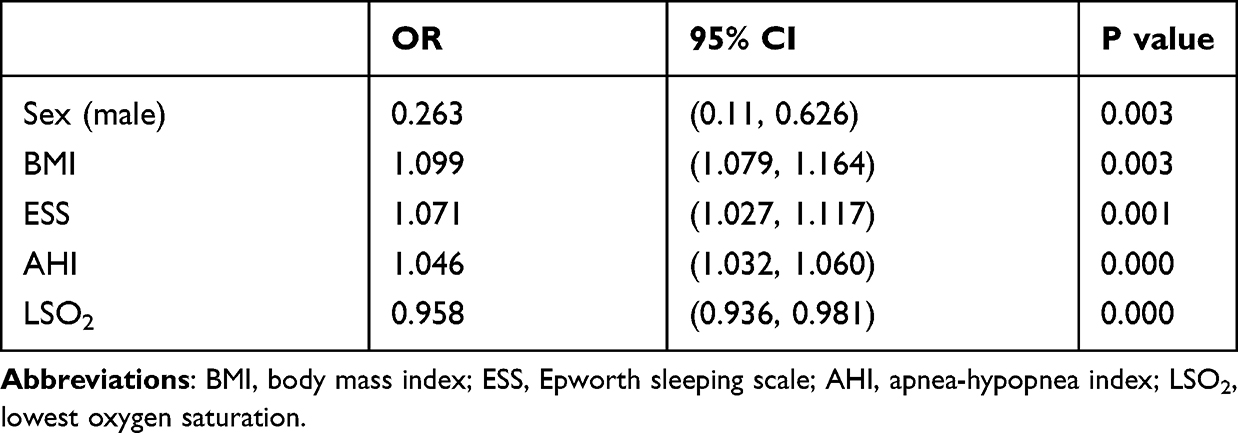 |
Table 3 Multivariate Logistic Regression Analysis of Factors Associated with Mixed-OSA |
This study then investigated if a quantized value of AHI and LSO2 can predict the occurrence of mixed-OSA. ROC curves were used to determine the cut-off values of AHI and LSO2 for predicting mix-OSA. AHI > 47 could predict mixed-OSA at MAI ≥ 5, with a sensitivity and specificity of 0.952 and 0.652, respectively (AUC = 0.822, P < 0.001, Figure 1A and Table 4). Similarly, LSO2 < 77% could also predict mixed-OSA at MAI ≥ 5, with a sensitivity and specificity of 0.822 and 0.675, respectively (AUC = 0.792, P < 0.001, Figure 1B and Table 5). This study used different criteria to further verify the results since previous studies also used the different criteria to define mixed-OSA.19,23 At MAI > 0, the cut-off value for AHI and LSO2 to predict mixed-OSA were 47 and 77%, respectively (AHI: sensitivity = 0.752, specificity = 0.652, AUC = 0.731, P < 0.001, Figure 1C and Table 4; LSO2: sensitivity = 0.652, specificity = 0.675, AUC = 0.696, P < 0.001, Figure 1D and Table 5). Moreover, at MAI > 30%, the cut-off value for AHI and LSO2 to predict mixed-OSA were 48 and 73%, respectively (AHI: sensitivity =0.809, specificity = 0.438, AUC = 0.628, P < 0.001, Figure 1E and Table 4; LSO2: sensitivity =0.642, specificity = 0.643, AUC = 0.636, P < 0.001, Figure 1F and Table 5).
 |
Table 4 Cut-off Value of AHI for Predicting Mixed-OSA with Different MAI Criteria |
 |
Table 5 Cut-off Value of LSO2 for Predicting Mixed-OSA with Different MAI Criteria |
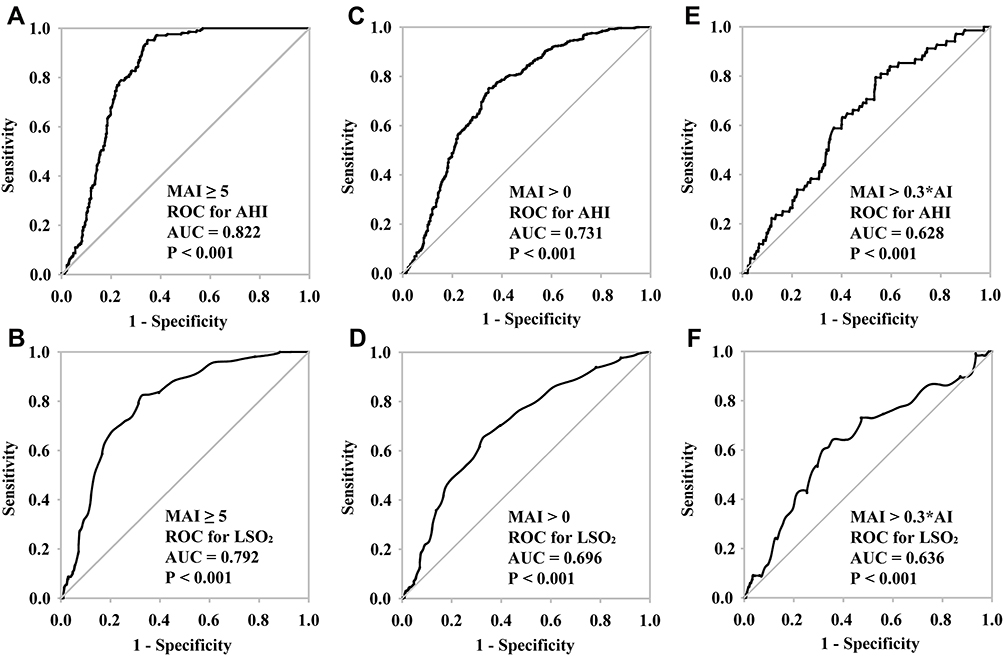 |
Figure 1 ROC curves of the cut-off value for AHI and LSO2 to predict mixed-OSA. (A, C, E) ROC curves of the cut-off values for AHI to predict mixed-OSA with different criteria to define mixed-OSA, which were MAI ≥ 5 (A), MAI > 0 (C), and MAI > 30% AI (E), respectively. (B, D, F) ROC curves of the cut-off values for LSO2 to predict mixed-OSA with different criteria to define mixed-OSA, which were MAI ≥ 5 (B), MAI > 0 (D), and MAI > 30% AI (F), respectively. |
Discussion
A major finding of this study is that AHI and LSO2 can predict occurrence of mixed-OSA. Specifically, AHI > 47 or LSO2 < 77% can be used as clinical predictor of mixed events in patients with OSA. In our view, the most important and clinically useful aspect of the current work is establishment of a novel, simple screening tool for patients with mixed-OSA.
Herein, pure-OSA and mixed-OSA patients had significantly different clinical traits. Unlike previous studies,19,20,22,23 we found that patients with mixed-OSA are more likely to have a history of smoking, drinking, and hypertension. The results also demonstrated that patients with mixed-OSA had a significantly increased percentage of N1 sleep, a reduced percentage of N2 sleep, and an almost complete loss of N3 sleep compared with pure-OSA. Moreover, the increased ArI indicated that sleep fragmentation is significant in mixed-OSA than in pure-OSA. Studies have indicated that more arousal during sleep indicates poor stability of respiratory monitoring,24,25 consistent with this study. Besides, the appearance of mixed events indicates the reduced stability of respiratory regulation, which is related to lower CPAP compliance in some OSA patients.19 In this study, multivariate logistic regression analysis showed that AHI and LSO2 were the risk factors for mixed-OSA. Of note, the AHI ≥ 5 was used to define OSA in this study. However, previous studies on mixed-OSA, such as Lee and colleagues, defined OSA as AHI ≥ 1520 and Yamauchi as AHI > 20.19 However, studies confirmed that mild OSA (5 ≤ AHI ≤ 15) is associated with clinical comorbidities, such as prevalent hypertension,21 poorer sleep quality,26 cognitive impairments, and higher ESS,27 which are significantly correlated with mixed-OSA. Moreover, CPAP can also treat patients with mild OSA, especially when diagnosis and treatment are initiated early.12,28 Therefore, a criterion of AHI ≥ 5 is suitable to define OSA when assessing mixed-OSA. Besides, previous studies have also different definitions of mixed OSA. To examine whether these different definitions influence the prediction of mixed OSA, three different criteria (MAI > 0,23 MAI ≥ 5,20,22 and MAI >30% AI19) were employed to calculate the cut-off values for predicting mixed-OSA based on the definition of mixed-OSA in previous studies. Although MAI >0 and MAI ≥ 5 had the same cut-off values, MAI ≥ 5 had higher sensitivity and AUC. The cut-off values of AHI and LSO2 were higher and lower, respectively, at MAI>30% AI than at MAI >0 and MAI ≥ 5, indicating a more severe OSA. Therefore, MAI ≥ 5 is suitable for defining mixed-OSA.
Collectively, the aforementioned findings indicate that mixed-OSA is related to the demographic data, symptoms, comorbidities, and outcomes of OSA.19,20,22,23 The results obtained here will guide the formulation of specific and individualized diagnostic indicators for OSA patients. As far as we know, the diagnosis of mixed OSA mainly depends on PSG. Although PSG is the gold standard for determining sleep disorder breathing events, including obstructive, central, and mixed events,29 however, it has some disadvantages, such as its expensiveness, inconvenience, complexity, and requirement to operate in a sleep laboratory, which limits its wide application.30,31 In recent years, portable PSG or home sleep apnea test,1,32 have been widely adopted for OSA monitoring due to recognition of the importance of screening OSA (especially during the current COVID-19 period) and the limited number of medical sleep centers to conduct PSG monitoring.33 However, portable devices,34,35 such as Level 3 or 4 diagnostic equipment used to monitor the overnight airflow or oxygen saturation for OSA detection, cannot directly detect mixed-OSA based on the recommendations of the AASM, the American College of Chest Physicians, and the American Thoracic Society.34,36 Therefore, clinically convenient and accurate prediction indicators for mixed-OSA are urgently needed. The results from our study suggest that the commonly used PSG parameters AHI and LSO2, which portable PSG can easily detect, are independently associated with mixed-OSA. Furthermore, for the first time, this study showed that the cut-off values of AHI > 47 and LSO2 < 77% can predict mixed-OSA. Therefore, this study provides faster and more practical indicators for screening mixed-OSA, which marks the instability of the respiratory control system of OSA.19,20
To our knowledge, this is the largest study to investigate mixed-OSA to date. The study comprehensively analyzed several factors such as population information, behavior habits, medical history, and PSG parameters. However, this study had the following limitations: First, it is a retrospective study, and selection bias is inevitable. Further longitudinal studies should be conducted to investigate the dynamic changes of mixed-OSA in OSA patients and analyze the effects of these mixed events on OSA comorbidities. Second, this study only used data from one centre representative of patients in central China. Multi-centre studies with larger populations are needed to further confirm the results. Third, this study has not revealed the underlying mechanisms of the prevalence ratio of mixed-OSA. Further experiments should determine the pathogenesis of mixed-OSA and develop effective treatments.
Conclusion
In summary, mixed-OSA is a common OSA with more severe clinical symptoms than pure-OSA. For instance, Mixed-OSA patients are associated with more severe sleep apnea, lower oxygen supply, poor sleep quality, extreme daytime sleepiness, multiple complications, and harmful living habits, affecting the quality of life and prognosis of OSA. AHI > 47 or LSO2 < 77% can be used as predictor for mixed-OSA and has important clinical significance for refining diagnosis and improving the OSA treatment effectiveness.
Ethics Statement
The Ethics Committee of the Third Hospital of Hebei Medical University approved this study (No. Science2020-037-1), and each patient signed informed consent. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. The information that could cause privacy disclosure was concealed during data collection.
Acknowledgments
This work was supported by Grants from the Key Research and Development Program of Hebei Province (No. 19277706D) and the Natural Science Foundation of Hebei Province (No. H2020206318).
Author Contributions
W.H. is the guarantor of the paper who designed the study, analyzed and interpreted the data, prepared, reviewed and revised the manuscript. L.P. and C.Q. designed the study, collected data, contributed to discussion, wrote the manuscript, and reviewed/edited the manuscript. Y.F., Z.Q., Z.X., X.C., W.Yu., and W.Ya. collected the data, participated in study design, data analysis and interpretation. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council On Cardiovascular Nursing. In collaboration with the national heart, lung, and blood institute national center on sleep disorders research (National Institutes of Health). J Am Coll Cardiol. 2008;52(8):686–717. doi:10.1016/j.jacc.2008.05.002
2. Punjabi NM, Caffo BS, Goodwin JL, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009;6(8):e1000132. doi:10.1371/journal.pmed.1000132
3. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47–112. doi:10.1152/physrev.00043.2008
4. Javaheri S, Barbe F, Campos-Rodriguez F, Dempsey JA, Somers VK. Sleep apnea: types, mechanisms, and clinical cardiovascular consequences. J Am Coll Cardiol. 2017;69(851):841–858. doi:10.1016/j.jacc.2016.11.069
5. Gottlieb DJ, Punjabi NM. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389–1440. doi:10.1001/jama.2020.3514
6. Wang H, Parker JD, Newton GE, et al. Influence of obstructive sleep apnea on mortality in patients with heart failure. J Am Coll Cardiol. 2007;49(15):1632–1633. doi:10.1016/j.jacc.2006.12.046
7. Barbé F, Durán-Cantolla J, Sánchez-de-la-torre M, et al. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;307(20):2161–2168. doi:10.1001/jama.2012.4366
8. McMillan A, Bratton DJ, Faria R, et al. Continuous positive airway pressure in older people with obstructive sleep apnoea syndrome (PREDICT): a 12-month, multicentre, randomised trial. Lancet Respir Med. 2014;2(10):804–812. doi:10.1016/S2213-2600(14)70172-9
9. Bratton DJ, Gaisl T, Wons AM, Kohler M. CPAP vs mandibular advancement devices and blood pressure in patients with obstructive sleep apnea: a systematic review and meta-analysis. JAMA. 2015;314(21):2280–2293. doi:10.1001/jama.2015.16303
10. Shim CY, Kim D, Park S, et al. Effects of continuous positive airway pressure therapy on left ventricular diastolic function: a randomised, sham-controlled clinical trial. Eur Respir J. 2018;51(2):1701774. doi:10.1183/13993003.01774-2017
11. Khan SU, Duran CA, Rahman H, Lekkala M, Saleem MA, Kaluski E. A meta-analysis of continuous positive airway pressure therapy in prevention of cardiovascular events in patients with obstructive sleep apnoea. Eur Heart J. 2018;39(24):2291–2297. doi:10.1093/eurheartj/ehx597
12. Wimms AJ, Kelly JL, Turnbull CD, et al. Continuous positive airway pressure versus standard care for the treatment of people with mild obstructive sleep apnoea (MERGE): a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8(4):349–358. doi:10.1016/S2213-2600(19)30402-3
13. Yoshinaga K, Burwash IG, Leech JA, et al. The effects of continuous positive airway pressure on myocardial energetics in patients with heart failure and obstructive sleep apnea. J Am Coll Cardiol. 2007;49(4):450–458. doi:10.1016/j.jacc.2006.08.059
14. Sánchez-de-la-torre M, Khalyfa A, Sánchez-de-la-torre A, et al. Precision medicine in patients with resistant hypertension and obstructive sleep apnea: blood pressure response to continuous positive airway pressure treatment. J Am Coll Cardiol. 2015;66(9):1023–1032. doi:10.1016/j.jacc.2015.06.1315
15. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919–931. doi:10.1056/NEJMoa1606599
16. Luo K, Zhang L, Zhang X, Han T, Li Y, Wang C. Acceptance of and six-month adherence to continuous positive airway pressure in patients with moderate to severe obstructive sleep apnea. Clin Respir J. 2021;15(1):56–64. doi:10.1111/crj.13269
17. Sánchez-de-la-torre M, Sánchez-de-la-torre A, Bertran S, et al. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): a randomised controlled trial. Lancet Respir Med. 2020;8(4):359–367. doi:10.1016/S2213-2600(19)30271-1
18. Sheth U, Monson RS, Prasad B, et al. Association of continuous positive airway pressure adherence with complications in patients with type 2 diabetes and obstructive sleep apnea. J Clin Sleep Med. 2021;17(8):1563–1569. doi:10.5664/jcsm.9248
19. Yamauchi M, Tamaki S, Yoshikawa M, et al. Differences in breathing patterning during wakefulness in patients with mixed apnea-dominant vs obstructive-dominant sleep apnea. Chest. 2011;140(1):54–61. doi:10.1378/chest.10-1082
20. Lee SA, Lee GH, Chung YS, Kim WS. Clinical, polysomnographic, and CPAP titration features of obstructive sleep apnea: mixed versus purely obstructive type. J Neurol Sci. 2015;355(1–2):150–154. doi:10.1016/j.jns.2015.06.005
21. Bouloukaki I, Grote L, McNicholas WT, et al. Mild obstructive sleep apnea increases hypertension risk, challenging traditional severity classification. J Clin Sleep Med. 2020;16(6):889–898. doi:10.5664/jcsm.8354
22. Lei F, Tan L, Li T, et al. [Association between mixed sleep apnea and treatment-emergent central sleep apnea]. Zhonghua Yi Xue Za Zhi. 2019;99(24):1864–1869. Chinese. doi:10.3760/cma.j.issn.0376-2491.2019.24.006
23. Yang X, Xiao Y, Han B, Lin K, Niu X, Chen X. Implication of mixed sleep apnea events in adult patients with obstructive sleep apnea-hypopnea syndrome. Sleep Breath. 2019;23(2):559–565. doi:10.1007/s11325-018-1745-0
24. Younes M, Ostrowski M, Atkar R, Laprairie J, Siemens A, Hanly P. Mechanisms of breathing instability in patients with obstructive sleep apnea. J Appl Physiol. 2007;103(6):1929–1941. doi:10.1152/japplphysiol.00561.2007
25. Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):144–153. doi:10.1513/pats.200707-114MG
26. Ondze B, Espa F, Dauvilliers Y, Billiard M, Besset A. Sleep architecture, slow wave activity and sleep spindles in mild sleep disordered breathing. Clin Neurophysiol. 2003;114(5):867–874. doi:10.1016/S1388-2457(02)00389-9
27. Kim H, Thomas RJ, Yun CH, et al. Association of mild obstructive sleep apnea with cognitive performance, excessive daytime sleepiness, and quality of life in the general population: the Korean Genome and Epidemiology Study (KoGES). Sleep. 2017;40(5). doi:10.1093/sleep/zsx012.
28. Campos-Rodriguez F, Martinez-Garcia MA, Ines CM, Almeida-Gonzalez C, Catalan-Serra P, Montserrat JM. Cardiovascular mortality in women with obstructive sleep apnea with or without continuous positive airway pressure treatment. Ann Intern Med. 2012;156(2):115–122. doi:10.7326/0003-4819-156-2-201201170-00006
29. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
30. Collop NA, Anderson WM, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Portable monitoring task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2007;3(7):737–747.
31. Chai-Coetzer CL, Antic NA, Hamilton GS, et al. Physician decision making and clinical outcomes with laboratory polysomnography or limited-channel sleep studies for obstructive sleep apnea: a randomized trial. Ann Intern Med. 2017;166(5):332–340. doi:10.7326/M16-1301
32. Malhotra A, Orr JE, Owens RL. On the cutting edge of obstructive sleep apnoea: where next? Lancet Respir Med. 2015;3(5):397–403. doi:10.1016/S2213-2600(15)00051-X
33. Phillips B, Gozal D, Malhotra A. What is the future of sleep medicine in the United States? Am J Respir Crit Care Med. 2015;192(8):915–917. doi:10.1164/rccm.201508-1544ED
34. Flemons WW, Littner MR, Rowley JA, et al. Home diagnosis of sleep apnea: a systematic review of the literature. An evidence review cosponsored by the American Academy of Sleep Medicine, the American College of Chest Physicians, and the American Thoracic Society. Chest. 2003;124(4):1543–1579. doi:10.1378/chest.124.4.1543
35. Jonas DE, Amick HR, Feltner C, et al. Screening for obstructive sleep apnea in adults: evidence report and systematic review for the US preventive services task force. JAMA. 2017;317(4):415–433. doi:10.1001/jama.2016.19635
36. Rosen I, Kirsch D, Carden K, et al. Clinical use of a home sleep apnea test: an updated American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2018;14(12):2075–2077. doi:10.5664/jcsm.7540
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.