")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 10
Clinical potential of aclidinium bromide in chronic obstructive pulmonary disease
Received 16 October 2013
Accepted for publication 17 January 2014
Published 13 June 2014 Volume 2014:10 Pages 449—453
DOI https://doi.org/10.2147/TCRM.S39710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Jun Zhong, Michael Roth
Pneumology and Pulmonary Cell Research, Department of Biomedicine and Internal Medicine, University Hospital Basel, Basel, Switzerland
Abstract: Chronic obstructive pulmonary disease (COPD) is increasing worldwide and is predicted to become the third most frequent cause of death by 2030. Muscarinic receptor antagonists, alone or in combination with long-acting ß2-agonists, are frequently used for COPD therapy. Aclidinium bromide is a novel muscarinic receptor antagonist, and clinical studies indicate that its metabolism is more rapid than that of other muscarinic receptor inhibitors, so systemic side effects are expected to occur less frequently. Aclidinium bromide is well tolerated, and when compared with other muscarinic receptor antagonists, the drug achieves better control of lung function, especially night-time symptoms in COPD patients. This review summarizes the safety profile and side effects reported by recent clinical studies using aclidinium bromide alone.
Keywords: aclidinium, tiotropium, side effects, clinical safety
Introduction
It is estimated that nearly 3 million people worldwide die of chronic obstructive pulmonary disease (COPD) every year and the prevalence is increasing.1 A major pathology of COPD is persistent irreversible constriction of the airways caused by smooth muscle cell activation. Bronchoconstriction in COPD reduces the airway lumen, thus limiting airflow.2 Therefore, smooth muscle cell relaxation is the major target to ease breathing in COPD patients. In the past, bronchodilation has been achieved mainly by inhalation of a long acting β2-agonist, but recent studies have provided evidence that blocking muscarinic receptors is more effective. However, use of the muscarinic receptor antagonists as therapeutics in COPD is not novel, but the previously available drugs had unwanted side effects, especially on the cardiovascular system.3,4 Thus, novel long-acting muscarinic receptor antagonists have been developed in recent years, and have been proven to effectively reduce symptoms in COPD patients with less severe side effects in the cardiovascular system.5,6 Here we provide a summary of the most recent clinical safety studies on the action of aclidinium bromide.
Bronchoconstriction is mainly due to constriction of smooth muscle cells in the airway wall, which can be triggered by activation of M3 receptors.7,8 Therefore, blockade of M3 receptors is assumed to relax the muscle cells and ease breathing. Aclidinium bromide is a novel long-acting muscarinic receptor antagonist, which has been approved for COPD therapy. Preclinical studies showed the preference of aclidinium bromide for the M3 receptor over M2, M1, and M4 receptors.9 Compared with other long-acting muscarinic receptor antagonists, aclidinium bromide has the advantage of being degraded rapidly and cleared from the circulation within 3 hours. Aclidinium bromide is hydrolyzed by butyrylcholinesterase into either carboxylic acid or alcohol metabolites, and thus results in fewer systemic side effects than other muscarinic receptor inhibitors, including tiotropium.9,10 Based on preclinical and Phase I studies, it was concluded that aclidinium bromide would have fewer side effects than other muscarinic receptor antagonists, especially in the cardiovascular system.9–14
This review summarizes the safety profile of aclidinium bromide therapy in COPD patients as reported in recent clinical studies. The selection criterion was reporting of adverse effects in clinical studies, and case reports were not included. However, the available data on the side effects for aclidinium bromide are very limited.
Clinical benefits of rapid aclidinium bromide metabolism
In a comparative study performed in different species, it was demonstrated that the metabolism of aclidinium bromide is most rapid in humans and dogs compared with guinea pigs and rats, while that of tiotropium was similar in all species.15,16 A further study provided evidence that aclidinium bromide was degraded more rapidly than other muscarinic receptor antagonists, supporting the idea that the drug may have a lower incidence of side effects.17 However, neither of these two studies explained on which enzymatic system this rapid turnover is based. When healthy volunteers inhaled 6,000 μg of aclidinium bromide, the compound was rapidly metabolized and not detectable in the circulation 3 hours later.12 In a Phase I trial, 272 healthy volunteers inhaled 800 μg aclidinium bromide daily over a period of 3 days. The drug proved to be very safe with regard to the cardiovascular system and had no significant effect on electrocardiogram readings monitored over 24 hours. Similar to the earlier studies, the plasma concentration of aclidinium bromide was below the detection limit 2 hours after inhalation of the drug.18
In 16 healthy volunteers, the maximum tolerated dose of aclidinium bromide was determined by dry powder inhalation at ascending doses ranging from 600 μg to 6,000 μg, with dose increments separated by a washout period of 7 days.12 The incidence of side effects was identical for aclidinium bromide and placebo, and included mild to moderate cardiac effects, which interestingly were not dose-related. The major side effects of aclidinium bromide were headache, fatigue, and renal pain, while airway obstruction, dry mouth, laryngitis, epistaxis, and acne were reported in two cases each. Like earlier studies, aclidinium bromide was rapidly metabolized and not detectable 3 hours after inhalation. The authors concluded that aclidinium bromide is safe and well tolerated up to a single dose of 6,000 μg.12
In 2012, de la Motte et al11 compared the pharmacokinetics and safety of aclidinium bromide in young and elderly COPD patients. The study included 12 patients aged 40–59 years and 12 patients older than 70 years. All patients inhaled aclidinium bromide 200 μg once daily over 3 days, followed by a second series of inhalations of aclidinium bromide 400 μg over 3 days after a washout period of 7 days. The results of this study showed that aclidinium bromide is rapidly degraded with no difference comparing young with elderly patients, and thereby confirmed the rapid degradation of aclidinium bromide, which had been reported by others.9,13,14,19 The plasma concentration of aclidinium bromide was not detectable at time points later than 3 hours after inhalation and this effect was independent of age. Thus, the dose of aclidinium bromide does not have to be adjusted for age.11
Side effects of aclidinium bromide
In a one-year study, 291 COPD patients inhaled aclidinium bromide 200 μg or 400 μg twice daily, which had very few side effects. In this cohort, less than 5% of patients reported cardiac side effects, and dry mouth was reported by only one patient.19 All reported side effects were independent of dose and duration of treatment. Furthermore, using questionnaires, the patients indicated improved overall quality of life during the 52-week study, which was again independent of aclidinium bromide dose strength. Importantly, aclidinium bromide therapy significantly improved lung function. However, the authors admitted that their study may have been slightly biased by the fact that they selected their long-term study patients from a previous cohort of 467 COPD patients who had been treated with aclidinium bromide over a period of 12 weeks. The authors acknowledged that such selection of their patient cohort, which they assigned as “healthy survivors”, may have improved the safety outcomes for aclidinium bromide. Nevertheless, other studies have also confirmed the good safety profile of aclidinium bromide in long-term treatment.
A similar 52-week, double-blind study including 605 patients with moderate to severe COPD was reported by Gelb et al.20 In this study, patients were randomized to inhalation of aclidinium bromide 200 μg or 400 μg twice daily. The reported side effects included dry mouth in 1.3% and 2.7% of patients and constipation in 2.9% and 1.7% at the respective dosages. Cardiac side effects were reported by less than 2% of patients, and as in the other studies, side effects were not related to drug dosage.
Improved lung function with aclidinium bromide in COPD patients
Following on from the previous section, Gelb et al reported improved breathing capacity over a one-year study period in COPD patients, and the improvement in lung function correlated with the dosage of aclidinium bromide.20 Furthermore, all COPD patients reported improved overall quality of life and better general health status.20 Improvement in lung function as a result of long-term therapy with aclidinium bromide has also been reported by others.21–23
Comparing the clinical benefits of aclidinium bromide 400 μg, (morning and evening) with those of tiotropium (18 μg, morning) in 27 COPD patients, Fuhr et al24 reported a similar bronchodilatory effect for both drugs. Furthermore, a significant reduction in night-time symptoms was achieved with aclidinium bromide but not with tiotropium. In a multicenter study, the effects of twice-daily inhalation of 400 μg aclidinium bromide (morning, evening) were compared with once-daily inhalation of 18 μg tiotropium (morning) or placebo over a period of 6 weeks.25 The authors determined FEV1 AUC0–24 and FEV1 AUC12–24 exacerbation in the different clinical centers and other COPD symptoms by questionnaire. The study comprised 440 patients recruited from 41 different sites, including the Czech Republic, Germany, Hungary, and Poland, who were randomized to treatment. Both drugs significantly increased the forced expiratory volume in one second compared with placebo. Aclidinium bromide showed a greater improvement in lung capacity than tiotropium after 6 weeks; however, the difference between the two drugs was not significant. The reduction of other COPD symptoms was clearly in favor of aclidinium bromide over tiotropium. Furthermore, only aclidinium bromide significantly reduced shortness of breath, wheeze, cough, phlegm, and night-time COPD symptoms. Adverse effects were similar for all treatments, and thus could not be related to the drugs. Drug-related side effects were below 3% and similar for both drugs.25 Finally, the US Food and Drug Administration concluded that the mortality rate under aclidinium bromide treatment does not differ between doses and was the same as with placebo control.26
Conclusion and future perspectives
All published clinical trials indicate that aclidinium bromide is well tolerated and safe for use as long-term COPD therapy. An overview of the studies on aclidinium bromide is provided in Table 1. However, the mechanism(s) by which aclidinium bromide achieves its clinical benefits has to be studied further.27 Studies in animal models and in human cells indicate that the beneficial clinical effect of aclidinium bromide in COPD therapy might involve more than antagonism of muscarinic receptors and muscle relaxation. These studies indicate that aclidinium bromide modifies cell differentiation, which manifests as epithelial–mesenchymal transition, a mechanism that contributes significantly to the pathogenesis of COPD.28–30 Furthermore, when combined with a long-acting β2-agonist, the beneficial effects of aclidinium bromide are increased further. In this regard, it will be interesting to see whether the combination of aclidinium bromide with a long-acting β2 agonist will further improve its benefits in COPD therapy.22,31,32
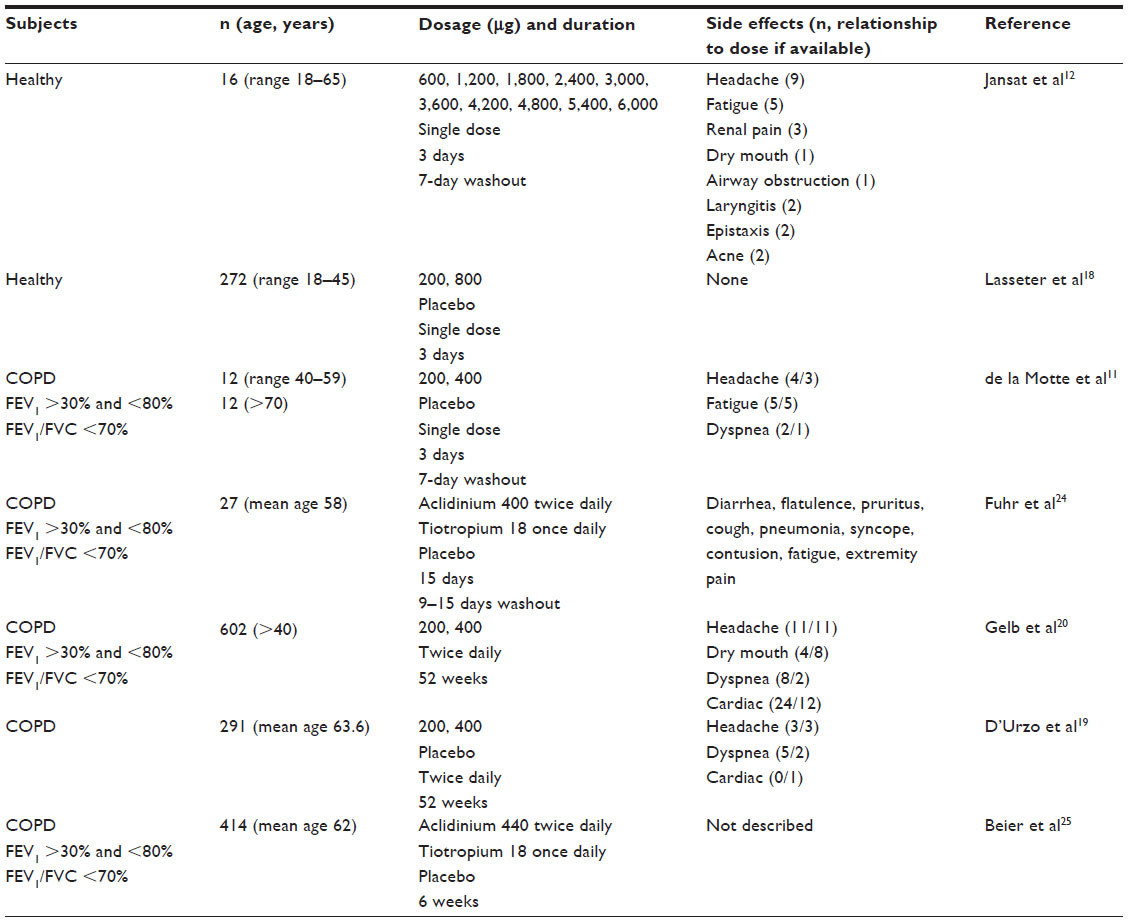 | Table 1 Recent clinical studies on the safety profile of aclidinium bromide |
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Chronic respiratory diseases. Burden of COPD. Available from: http://www.who.int/respiratory/copd/burden/en/. Accessed January 17, 2014. | |
Canning BJ. Reflex regulation of airway smooth muscle tone. J Appl Physiol. 2006;101(3):971–985. | |
Moulton BC, Fryer AD. Muscarinic receptor antagonists, from folklore to pharmacology; finding drugs that actually work in asthma and COPD. Br J Pharmacol. 2011;163(1):44–52. | |
Jacoby DB, Fryer AD. Anticholinergic therapy for airway diseases. Life Sci. 2001;68(22–23):2565–2572. | |
Sharafkhaneh A, Majid H, Gross NJ. Safety and tolerability of inhalational anticholinergics in COPD. Drug Healthc Patient Saf. 2013;5:49–55. | |
Reid DJ, Pham NT. Emerging therapeutic options for the management of COPD. Clin Med Insights Circ Respir Pulm Med. 2013;7:7–15. | |
Eglen RM, Choppin A, Dillon MP, Hegde S. Muscarinic receptor ligands and their therapeutic potential. Curr Opin Chem Biol. 1999;3(4):426–432. | |
Cazzola M, Matera MG, D’Amato G, et al. Evidence of muscarinic receptor subtypes in airway smooth muscle of normal volunteers and of chronic obstructive pulmonary disease patients. Int J Clin Pharmacol Res. 1989;9(1):65–70. | |
Sentellas S, Ramos I, Albertí J, et al. Aclidinium bromide, a new, long-acting, inhaled muscarinic antagonist: in vitro plasma inactivation and pharmacological activity of its main metabolites. Eur J Pharm Sci. 2010;39(5):283–290. | |
Albertí J, Martinet A, Sentellas S, Salvà M. Identification of the human enzymes responsible for the enzymatic hydrolysis of aclidinium bromide. Drug Metab Dispos. 2010;38(7):1202–1210. | |
de la Motte S, Beier J, Schmid K, Pascual S, Jansat JM, Gil EG. Pharmacokinetics and safety of aclidinium bromide in younger and elderly patients with chronic obstructive pulmonary disease. Int J Clin Pharmacol Ther. 2012;50(6):403–412. | |
Jansat JM, Lamarca R, Garcia Gil E, Ferrer P. Safety and pharmacokinetics of single doses of aclidinium bromide, a novel long-acting, inhaled antimuscarinic, in healthy subjects. Int J Clin Pharmacol Ther. 2009;47(7):460–468. | |
Schmid K, Pascual S, Gil EG, Ortiz S, Jansat JM. Pharmacokinetics and safety of aclidinium bromide, a muscarinic antagonist, in adults with normal or impaired renal function: a Phase I, open-label, single-dose clinical trial. Clin Ther. 2010;32(10):1798–1812. | |
Gavaldà A, Gras J, Llupià J, Aubets J, Beleta J, Llenas J. Aclidinium bromide, a novel long-acting muscarinic antagonist for COPD with improved preclinical renal and urinary safety profile. Life Sci. 2012;90(7–8):301–305. | |
Ortiz S, Flach S, Ho J, et al. Mass balance and metabolism of aclidinium bromide following intravenous administration of [14C]-aclidinium bromide in healthy subjects. Biopharm Drug Dispos. 2012;33(1):39–45. | |
Prat M, Fernández D, Buil MA, et al. Discovery of novel quaternary ammonium derivatives of (3R)-quinuclidinol esters as potent and long-acting muscarinic antagonists with potential for minimal systemic exposure after inhaled administration: identification of (3R)-3-{[hydroxy(di-2-thienyl)acetyl]oxy}-1-(3-phenoxypropyl)-1-azoniabicyclo[2.22]octane bromide (aclidinium bromide). J Med Chem. 2009;52(16):5076–5092. | |
Sentellas S, Ramos I, Albertí J, et al. Aclidinium bromide, a new, long-acting, inhaled muscarinic antagonist: in vitro plasma inactivation and pharmacological activity of its main metabolites. Eur J Pharm Sci. 2010;39(5):283–290. | |
Lasseter KC, Aubets J, Chuecos F, Gil EG. Aclidinium bromide, a long-acting antimuscarinic, does not affect QT interval in healthy subjects. J Clin Pharmacol. 2011;51(6):923–932. | |
D’Urzo A, Kerwin E, Rennard S, He T, Gil EG, Caracta C. One-year extension study of ACCORD COPD I: safety and efficacy of two doses of twice-daily aclidinium bromide in patients with COPD. COPD. 2013;10(4):500–510. | |
Gelb AF, Tashkin DP, Make BJ, Zhong X, Garcia Gil E, Caracta C; LAS-MD-35 Study Investigators. Long-term safety and efficacy of twice-daily aclidinium bromide in patients with COPD. Respir Med. 2013;107(12):1957–1965. | |
Jones PW, Singh D, Bateman ED, et al. Efficacy and safety of twice-daily aclidinium bromide in COPD patients: the ATTAIN study. Eur Respir J. 2012;40(4):830–836. | |
Singh D, Magnussen H, Kirsten A, et al. A randomised, placebo- and active-controlled dose-finding study of aclidinium bromide administered twice a day in COPD patients. Pulm Pharmacol Ther. 2012;25(3):248–253. | |
Maltais F, Celli B, Casaburi R, et al. Aclidinium bromide improves exercise endurance and lung hyperinflation in patients with moderate to severe COPD. Respir Med. 2011;105(4):580–587. | |
Fuhr R, Magnussen H, Sarem K, et al. Efficacy of aclidinium bromide 400 μg twice daily compared with placebo and tiotropium in patients with moderate to severe COPD. Chest. 2012;141(3):745–752. | |
Beier J, Kirsten AM, Mrûz R, et al. Efficacy and safety of aclidinium bromide compared with placebo and tiotropium in patients with moderate-to-severe chronic obstructive pulmonary disease: results from a 6-week, randomized, controlled Phase IIIb study. COPD. 2013;10(4):511–522. | |
US Food and Drug Administration. NDA 202-450: aclidinium bromide for the long-term, maintenance treatment of bronchospasm associated with chronic obstructive pulmonary disease (COPD), including chronic bronchitis and emphysema. Paper presented at the Pulmonary Allergy Drugs Advisory Committee Meeting, February 23, 2012, Silver Spring, MD, USA. Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/Pulmonary-AllergyDrugsAdvisoryCommittee/UCM292620.pdf. Accessed August 30, 2012. | |
Cazzola M, Molimard M. The scientific rationale for combining long-acting beta2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23(4):257–267. | |
Milara J, Serrano A, Peiró T, et al. Aclidinium inhibits cigarette smoke-induced lung fibroblast-to-myofibroblast transition. Eur Respir J. 2013;41(6):1264–1274. | |
Milara J, Serrano A, Peiró T, et al. Aclidinium inhibits human lung fibroblast to myofibroblast transition. Thorax. 2012;67(3):229–237. | |
Cortijo J, Mata M, Milara J, et al. Aclidinium inhibits cholinergic and tobacco smoke-induced MUC5AC in human airways. Eur Respir J. 2011;37(2):244–254. | |
Cazzola M, Page C, Matera MG. Long-acting muscarinic receptor antagonists for the treatment of respiratory disease. Pulm Pharmacol Ther. 2013;26(3):307–317. | |
Cazzola M, Rogliani P, Matera MG. Aclidinium bromide/formoterol fumarate fixed-dose combination for the treatment of chronic obstructive pulmonary disease. Expert Opin Pharmacother. 2013;14(6):775–781. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.