")
Back to Journals » Infection and Drug Resistance » Volume 12
Clinical Outcomes Of Colistin In Combination With Either 6-G Sulbactam Or Carbapenems For The Treatment Of Extensively Drug-Resistant Acinetobacter Baumannii Pneumonia With High MIC To Sulbactam, A Prospective Cohort Study
Authors Ungthammakhun C , Vasikasin V , Changpradub D
Received 31 July 2019
Accepted for publication 5 September 2019
Published 13 September 2019 Volume 2019:12 Pages 2899—2904
DOI https://doi.org/10.2147/IDR.S225518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Chutchawan Ungthammakhun, Vasin Vasikasin, Dhitiwat Changpradub
Division of Infectious Diseases, Department of Medicine, Phramongkutklao Hospital, Bangkok 10400, Thailand
Correspondence: Dhitiwat Changpradub
Division of Infectious Diseases, Department of Medicine, Phramongkutklao Hospital, Bangkok, 10400, Thailand
Tel +66 81 937 2927
Fax +66 2 644 4420
Email [email protected]
Purpose: Extensively drug-resistant Acinetobacter baumannii (XDRAB) is an important cause of nosocomial pneumonia with limited therapeutic options. Colistin-based regimen is the recommended treatment. Which drugs should be combined with colistin remains uncertain. The aim of this study was to investigate the clinical outcomes of patients with XDRAB pneumonia who were treated with colistin, combined with either 6-g sulbactam or carbapenems, in the setting of high MIC to sulbactam.
Patients and methods: In this prospective cohort study, hospitalized patients diagnosed with XDRAB pneumonia in Phramongkutklao Hospital were enrolled. The primary outcome was 28-day mortality. Secondary outcomes were 7- and 14-day mortality, length of stay, ventilator days and factors associated with mortality.
Results: From 1 July 2016 to 30 September 2017, 182 patients were included; 92 received colistin plus sulbactam and 90 received colistin plus carbapenems. Most of the patients were males diagnosed with ventilator-associated pneumonia in medical intensive care unit. Overall mortality rates at 7, 14, 28 days were 24.2%, 37.4%, and 53.3%, respectively. Mortality rates did not differ between sulbactam group and carbapenem groups at 7 days (19.6% vs 28.9%, p-value 0.424, adjusted HR 1.277; 95% CI = 0.702–2.322), 14 days (34.8% vs 40%, p = 0.658, adjusted HR 1.109; 95% CI = 0.703–1.749) and 28 days (51.1% vs 55.6%, p = 0.857, adjusted HR 1.038; 95% CI = 0.690–1.562). Length of stay, ICU days and ventilator days did not differ. Complications of treatment including acute kidney injury were not statistically different.
Conclusion: In XDRAB pneumonia with high MIC to sulbactam, differences in mortality rates were not statistically significant between colistin plus 6-g sulbactam and colistin plus carbapenems.
Keywords: XDR A. baumannii pneumonia, mortality rate, colistin based, sulbactam, carbapenems
Introduction
Infection with extensively drug-resistant Acinetobacter baumannii (XDRAB) is a serious emerging disease commonly found in hospitals with an increasing global trend.1 The overall mortality rate of XDRAB infection was as high as 64%.2 Pneumonia is among the most common site of infection.3 The current guidelines for the management of XDRAB hospital-acquired pneumonia (HAP) or ventilator-associated pneumonia (VAP) recommend treatment with intravenous colistin.4 However, colistin has poor lung tissue penetration in the animal model that may cause poor clinical outcome for XDRAB pneumonia treated with colistin alone.5 Moreover, synergistic activities between colistin and carbapenems or sulbactam were found in in-vitro studies.6–9 Therefore, colistin combination therapy might improve the clinical outcome of XDRAB pneumonia. Nevertheless, these combinations failed to improve significant mortality outcomes.10–13 Which drugs should be combined with colistin remains uncertain. The previous study found that factors associated with mortality were chronic obstructive pulmonary disease, diabetes,10 higher severity score, old age, and prolonged intensive care unit (ICU) stay before the infections.12
This study aimed to investigate the clinical outcomes of XDRAB pneumonia patients who were treated with colistin, combined with either sulbactam or carbapenems.
Materials And Methods
Study Design, Sites, And Participants
This prospective cohort study included consecutive patients with XDRAB pneumonia in Phramongkutklao Hospital, a 1200-bed tertiary care military hospital in Thailand, from 1 July 2016 to 30 September 2017. After the approval of the protocol, patients aged ≥18 years with XDRAB pneumonia, who received definite treatment with colistin, combined with sulbactam or carbapenems (imipenem or meropenem) were enrolled in the study. XDRAB pneumonia was diagnosed when patients with clinical diagnosis of pneumonia had a single pathogen of XDRAB isolated from their sputum culture, which was collected from tracheal suction or mouth on the date of diagnosis. The sputum collected from the mouth in non-intubate patients and from endotracheal tube suction in intubated patients must have >25 neutrophils and <10 squamous epithelial cells per low power field to be determined as significant. The exclusion criteria included patients who developed a new infection during the treatment, had concurrent diagnosis of another site of infection, had organisms other than XDRAB obtained from blood or sputum culture or received switch regimens between sulbactam and carbapenems. All participants had received information and written informed consent and then study was conducted in accordance with the Declaration of Helsinki.
Eligible patients were categorized into 2 groups as follows: those who received colistin with sulbactam (CL+SB) and those who received colistin with carbapenems (CL+CB). The maximum dosage of 6 g/day of sulbactam was derived from ampicillin/sulbactam and cefoperazone/sulbactam. The maximum dosages of imipenem and meropenem were 2g and 3g/day, respectively. Colistin was used at the maximum dosage of 300 mg/day. These antibiotics were intravenously administered with dosage adjustment according to renal function. The antibiotics prescribed were according to the decision of the attending infectious disease specialists, without clear criteria for the decision.
Ethical Approval
This study was approved by the Institutional Review Board, Royal Thai Army Medical Department, Bangkok, Thailand (www.irbrta.pmk.ac.th reference number R061h/59).
Variables And Definitions
The primary outcome was 28-day mortality rate after initiation of antibiotics. The secondary outcomes were 7-day and 14-day mortality rates, length of hospital stay, length of ICU stay and ventilator days. The baseline demographic data includ sex, age, underlying condition, hospital service, ventilator status, antimicrobial treatment (empirical and definite), intubation and susceptibility data of sputum. Additionally, blood culture samples were collected. The clinical outcomes includ duration of admission, duration of ventilator use, length of hospital stay, length of ICU stay, vital signs, APACHEII severity score,14 kidney functions and complete blood counts.
XDRAB was defined as A. baumannii with all drug resistance except polymyxin or glycylcycline by using automate broth microdilution test. CLSI recommendations were used for susceptibility interpretation.15 Pneumonia and definition of HAP and VAP were defined according to CDC definition.16
Mortality rates were measured regarding the day when sputum culture was collected (considered as day 1). Ventilator day was defined as the duration between the day of intubation (in HAP patients with respiratory failure) or the day when sputum culture was collected (in VAP patients) and the day of extubation or death. Acute kidney injury was defined according to KDIGO 2012 guidelines,17 and disseminated intravascular coagulation (DIC) was defined if ISTH score ≥5,18 and septic shock was defined when patients received vasopressor.
Statistical Analysis
Comparisons between the groups were performed using Pearson’s chi-square test or Fisher’s exact test, as appropriate for proportions and with Student’s T-test or Mann–Whitney U-test, as appropriate for continuous outcomes. Variables with a p-value <0.2 in univariate analysis were introduced into multivariate analyses, which were performed using Cox regression analyses. All p-values were two-tailed with those less than 0.05 considered statistically significant. Power of the study for statistical analysis was at 80%. All statistical analyses were performed using IBM SPSS Statistics for Windows v.22.0 (IBM Corp., Armonk, NY, USA).
Results
Characteristics Of The Study Population
A total of 182 patients with XDRAB pneumonia were included (92 received CL+SB, and 90 received CL+CB). The mean age (SD) was 70 (17.6) years, with 115 (63.2%) male patients. Most common comorbidity was hypertension (61.5%). About 75.2% of patients received colistin-based treatment as empirical therapy, which was defined as an appropriate treatment. Baseline characteristics of patients are shown in Table 1. There were no statistically significant differences in baseline characteristics between the two groups, except for higher cirrhosis in carbapenem group and higher stroke in sulbactam groups. Complication of acute kidney injury after the treatment was not significantly different.
 |
Table 1 Demographic Data |
Treatment Outcomes
The overall 28-day mortality rate was 53.3%. There were no statistically significant differences in mortality between the two groups (Table 2). The mean survival time was not statistically different between the treatment groups. Trends toward higher length of stay, ICU days, and ventilator days were observed in CL+CB group (Table 3). Complication of acute kidney injury after the treatment was not significantly different.
 |
Table 2 Mortality Rate, According To The Treatment |
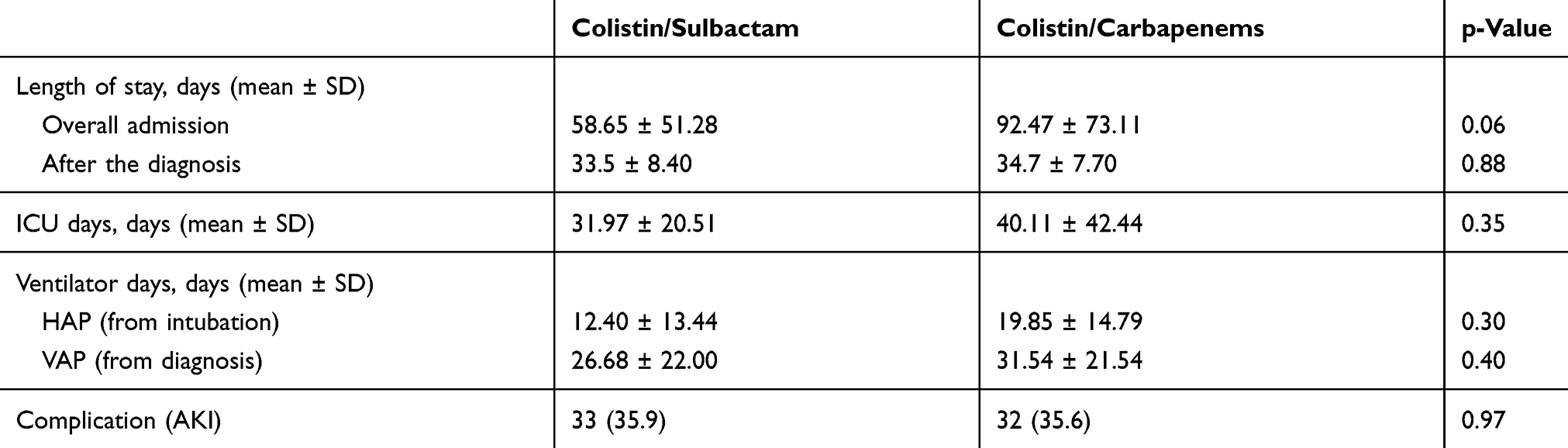 |
Table 3 Length Of Stay, ICU Days And Ventilator Days After Treatment With Colistin Plus Sulbactam Or Colistin Plus Carbapenems |
Risk Factors Associated With Mortality
On multivariate analysis, factors associated with 28-day mortality were gout (adjusted HR, 2.71; 95% CI, 1.15–6.38; p = 0.02), APACHEII score of more than 20 (adjusted HR, 2.5; 95% CI, 1.54–4.07; p < 0.001), and septic shock (adjusted HR, 3.52; 95% CI, 2.06–6; p < 0.001) (Table 4).
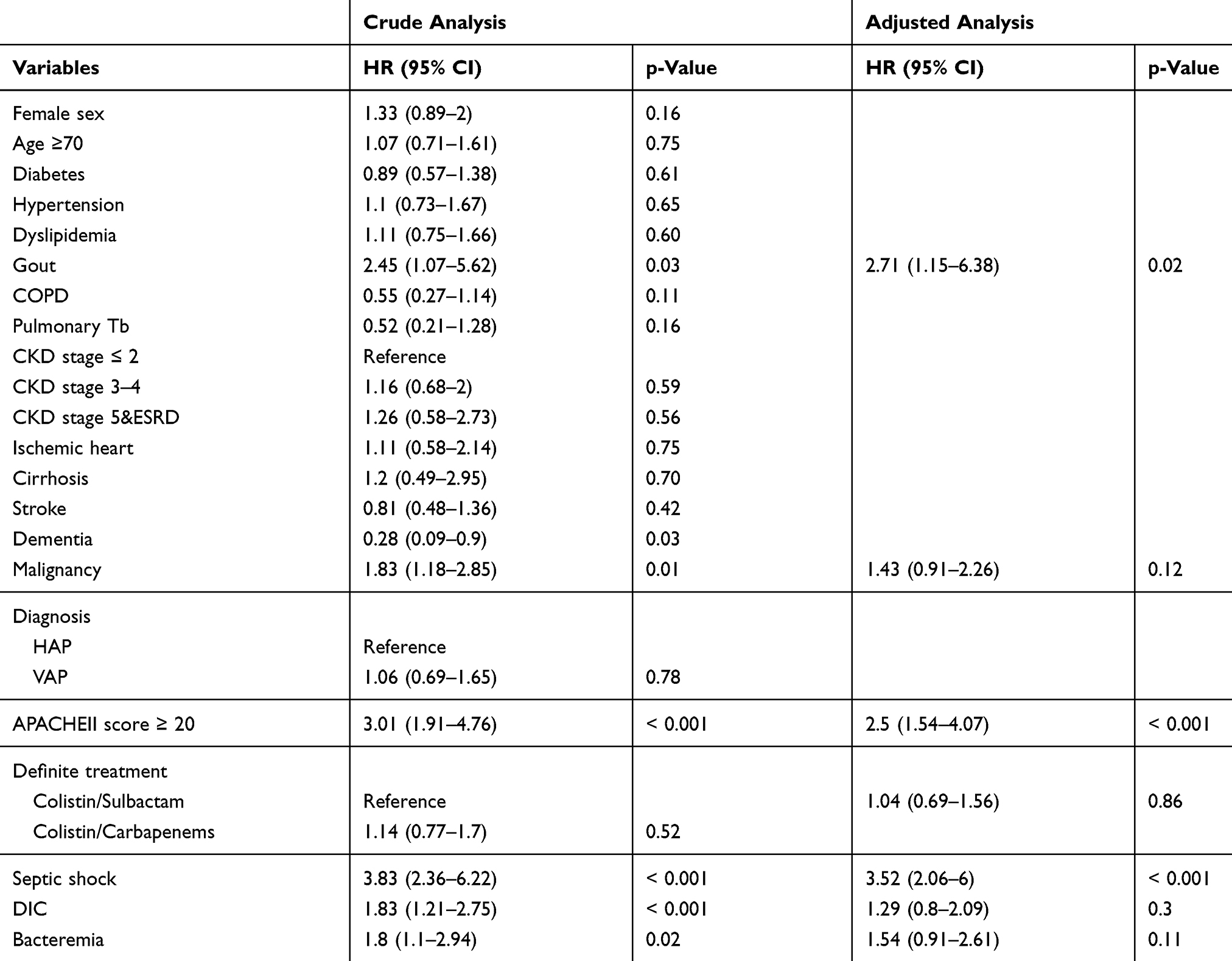 |
Table 4 Univariate And Multivariate Analyses Of Risk Factors Associated With 28 Mortality Using Cox Regression Model |
Discussion
In this prospective cohort study, the treatment with CL+SB and CL+CB had a comparable outcome of mortality at 7, 14, and 28 days. This is consistent with those found in the related studies.10–13 However, trends toward lower morbidities were observed in CL+SB group. From our previous findings,19 minimum inhibitory concentrations (MIC) of sulbactam against XDRAB in Phramongkutklao Hospital were so high that the dosage of sulbactam up to 9–12 g/day with prolonged infusion might be needed to achieve therapeutic targets. Thus, higher dosage and longer infusion might be needed to show the superiority of sulbactam group.
In this study, the 28-day mortality rate of XDRAB pneumonia was comparable to those found in previous studies, despite the slightly different selection criteria. Nevertheless, the 28-day mortality rate of colistin and sulbactam group (51.1%) was lower than a study which used lower sulbactam at a dosage of 3g/day10 (70%) and slightly higher than the one which used higher sulbactam at a dosage of 8g/day (50%)11; the dose of colistin and severity of illness in previous studies are similar to our study. Considering 14-day mortality rate of sulbactam group in this study (34.8%), a study of colistin with the same dosage of sulbactam at 6g/day in XDRAB bacteremia, with VAP diagnosed in the majority of patients, the 14-day mortality rate was comparable to this study (31.9%).12 Surprisingly, a study in VAP patients with 9g/day of sulbactam revealed 14-day mortality at 73%.13 Whether sulbactam dosage contributes to the outcome needs to be explored further.
High APACHEII score and septic shock were also found to still be reliable predictors of mortality. The kidney injury was still a common complication of colistin treatment.
Despite this study being a prospective cohort study with a large sample size, it has certain limitations. First, this is not a randomized study. Other factors affecting the decision of antibiotic regimens were not well-controlled. Second, to control factors resulting in cross-over of treatment regimens, those who received both sulbactam and carbapenems were excluded. Therefore, the mortality rate in this study might not reflect the true rate. Third, the study might be underpowered to exclude the clinical meaningful difference between groups.
Conclusion
Patients with pneumonia caused by XDRAB in Phramongkutklao hospital had a higher mortality rate than previous studies but were not statistically significant between colistin plus 6-g sulbactam and colistin plus carbapenems. Colistin combination with sulbactam had lower ventilator days in patients with HAP.
Acknowledgments
The authors thank the staff of the Department of Medicine, Phramongkutklao Hospital, for their care of the patients, the Division of Infectious disease for their assistance, and the Office of Research Development, Phramongkutklao College of Medicine, for assistance with statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Durante-Mangoni E, Zarrilli R. Global spread of drug-resistant Acinetobacter baumannii: molecular epidemiology and management of antimicrobial resistance. Future Microbiol. 2011;6(4):407–422. doi:10.2217/fmb.11.23
2. Garnacho-Montero J, Ortiz-Leyba C, Jimenez-Jimenez FJ, et al. Treatment of multidrug-resistant Acinetobacter baumannii ventilator-associated pneumonia (VAP) with intravenous colistin: a comparison with imipenem-susceptible VAP. Clin Infect Dis. 2003;36(9):1111–1118. doi:10.1086/374337
3. Kuo LC, Lai CC, Liao CH, et al. Multidrug-resistant Acinetobacter baumannii bacteraemia: clinical features, antimicrobial therapy and outcome. Clin Microbiol Infect. 2007;13(2):196–198. doi:10.1111/j.1469-0691.2006.01601.x
4. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw504
5. Montero A, Ariza J, Corbella X, et al. Efficacy of colistin versus beta-lactams, aminoglycosides, and rifampin as monotherapy in a mouse model of pneumonia caused by multiresistant Acinetobacter baumannii. Antimicrob Agents Chemother. 2002;46(6):1946–1952. doi:10.1128/AAC.46.6.1946-1952.2002
6. Pongpech P, Amornnopparattanakul S, Panapakdee S, et al. Antibacterial activity of carbapenem-based combinations againts multidrug-resistant Acinetobacter baumannii. J Med Assoc Thai. 2010;93(2):161–171.
7. Marie MA, Krishnappa LG, Alzahrani AJ, Mubaraki MA, Alyousef AA. A prospective evaluation of synergistic effect of sulbactam and tazobactam combination with meropenem or colistin against multidrug resistant Acinetobacter baumannii. Bosn J Basic Med Sci. 2015;15(4):24–29.
8. Dong X, Chen F, Zhang Y, Liu H, Liu Y, Ma L. In vitro activities of rifampin, colistin, sulbactam and tigecycline tested alone and in combination against extensively drug-resistant Acinetobacter baumannii. J Antibiot (Tokyo). 2014;67(9):677–680. doi:10.1038/ja.2014.99
9. Thamlikitkul V, Tiengrim S. In vitro activity of colistin plus sulbactam against extensive-drug-resistant Acinetobacter baumannii by checkerboard method. J Med Assoc Thai. 2014;97(Suppl 3):S1–S6.
10. Yilmaz GR, Guven T, Guner R, et al. Colistin alone or combined with sulbactam or carbapenem against A. baumannii in ventilator-associated pneumonia. J Infect Dev Ctries. 2015;9(5):476–485. doi:10.3855/jidc.6195
11. Makris D, Petinaki E, Tsolaki V, et al. Colistin versus colistin combined with ampicillin-sulbactam for multiresistant Acinetobacter baumannii ventilator-associated pneumonia treatment: an open-label prospective study. Indian J Crit Care Med. 2018;22(2):67–77. doi:10.4103/ijccm.IJCCM_302_17
12. Batirel A, Balkan II, Karabay O, et al. Comparison of colistin-carbapenem, colistin-sulbactam, and colistin plus other antibacterial agents for the treatment of extremely drug-resistant Acinetobacter baumannii bloodstream infections. Eur J Clin Microbiol Infect Dis. 2014;33(8):1311–1322. doi:10.1007/s10096-014-2070-6
13. Kalin G, Alp E, Akin A, Coskun R, Doganay M. Comparison of colistin and colistin/sulbactam for the treatment of multidrug resistant Acinetobacter baumannii ventilator-associated pneumonia. Infection. 2014;42(1):37–42. doi:10.1007/s15010-013-0495-y
14. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
15. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 26th Ed. CLSI Supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2016.
16. Centers for Disease Control and Prevention/National Healthcare Safety Network. CDC/NHSN surveillance definitions for specific types of infections. January 2016. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf.
17. Kidney Disease: improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150.
18. Taylor FB
19. Saelim W, Santimaleeworagun W, Thunyaharn S, Changpradub D, Juntanawiwat P. Pharmacodynamic profiling of optimal sulbactam regimens against carbapenem-resistant Acinetobacter baumannii for critically ill patients. Asian Pac J Trop Biomed. 2018;8(1):14–18.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.