")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Clinical Outcomes And Risk Factors In Patients Circumcised By Chinese Shang Ring: A Prospective Study Based On Age And Types Of Penile Disease
Authors Wang H , Huang Z, Zhou J, Zhang X, Liang C
Received 12 May 2019
Accepted for publication 25 September 2019
Published 21 October 2019 Volume 2019:15 Pages 1233—1241
DOI https://doi.org/10.2147/TCRM.S215471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Hui Wang,1–3 Zhenyu Huang,1–3 Jun Zhou,1–3 Xiansheng Zhang,1–3 Chaozhao Liang1–3
1Department of Urology, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2The Institute of Urology, Anhui Medical University, Hefei, People’s Republic of China; 3Anhui Province Key Laboratory of Genitourinary Diseases, Anhui Medical University, Hefei, People’s Republic of China
Correspondence: Chaozhao Liang
Department of Urology, The First Affiliated Hospital of Anhui Medical University, Hefei 230022, People’s Republic of China
Tel +86 551 6292 3440
Fax +86 551 6363 3742
Email [email protected]
Purposes: To explore the efficacy of circumcision with Chinese Shang Ring (CSR) in the different cohorts so that can obtain the best applicable population and manage complications better.
Methods: This study consisted of 657 patients who were circumcised with CSR in our institute between August 2017 and August 2018. All cases were followed up at post-operation for 3 to 15 months. The surgery time (ST), wound healing time (WHT), satisfaction with the appearance of postoperative penis and complications were collected and comparatively analyzed. Multivariate analysis was used to determine the independent risk factors associated with efficacy, which were presented by odd ratios and its 95% confidence index.
Results: All cases wore the CSR successfully. The ST and WHT respectively were 5.75 ± 2.27 mins and 21.15 ± 5.05 days. The long-term complications, total complications (TC), satisfaction and successful circumcision (SC) respectively were 5.30%, 11.70%, 97.70% and 94.70%. For TC and SC, there was a difference between phimosis and redundant foreskin (21.30% vs 6.20%, P<0.001 and 89.20% vs 97.8%, P<0.001, respectively). In terms of satisfaction and SC, adolescents were higher than children (98.70% vs 94.70%, P=0.035 and 96.80% vs 90.10%, P=0.024, respectively) but was similar to adults (98.70% vs 100.00%, P=0.071 and 96.80% vs 98.00%, P=0.257, respectively). The degree of pain and the incidence of wound dehiscence in adults was higher than adolescents (P<0.05). The phimosis (OR= 1.47, 95% CI=1.26–1.79, P<0.001) and childhood (OR= 1.13, 95% CI =1.06–1.36, P<0.001) were associated with poor efficacy.
Conclusion: The curative effect of circumcision by CSR in adolescents was similar to adults, both higher than that of children. However, adults have more severe pain and a higher probability of wound dehiscence in the later stage than adolescents. So, adolescence is probably the best time to be circumcised with CSR.
Keywords: redundant foreskin, phimosis, age, sizes, Chinese Shang Ring
Introduction
Chinese Shang Ring (CSR) is a novel disposable device of circumcision, which eliminates the need for suturing and has been on the Chinese market since 2005. Lots of previous studies had demonstrated that CSR is safe and easy to apply.1–4 The CSR for circumcision has been carried out in many areas, including Kenya, Zambia and other African countries, which also are one of the measures recommended by the World Health Organization (WHO) for circumcision.5
A crowd of researchers from China and other countries certified that CSR has many advantages compared to conventional surgical approaches.1,2,4,6 Firstly, the CSR has an excellent safety profile and is relatively easy to teach and learn for the doctors. Second, the operative time of circumcision by CSR takes about 4–6 mins, rarely more than 10 mins, which is much less than the time of conventional surgical approaches. Third, the type of complications is similar to conventional surgical approaches, but the incidence of complication is lower than conventional surgical approaches. Besides, the patients greatly satisfied with the cosmetic appearance of their circumcised penis. Finally, most important is that few problems and little disruption are involved in daily life after they are circumcised by CSR. Therefore, the above merits have the potential to promote the safe and effective scale-up of circumcision services in settings where circumcision is not widely utilized.
Even if the CSR is better than conventional approaches to adult circumcision, is it good for every male? There are few types of research about the efficacy and safety of CSR for the child whose penis is undeveloped or for men with phimosis.7,8 Therefore, our study aims at getting the feasibility and effect of CSR for the undeveloped penis and phimosis.
Materials And Methods
Patients
A total of 657 patients who were circumcised with CSR between August 2017 and August 2018, including 417 (63%) cases of the redundant foreskin and 240 (37%) cases of phimosis, were involved in the study. All of the patients are willing to circumcise by CSR after the detailed introduction of CSR. Their ages ranged from 7 to 65 years (mean ± SD, 17.6 ± 7.7 years). Included criteria are as the following: (1) phimosis, (2) a history of balanoposthitis, (3) unsatisfying penile hygiene. Excluded criteria are as the following: (1) the foreskin or glans is in the inflammatory phase, (2) the primary or secondary concealed penis, (3) patient cannot cooperate with the doctor during the operation.
This study was approved by Ethics committees regarding Human Research of the First Affiliated Hospital of Anhui Medical University. All experiments were performed following the relevant guidelines and regulations of the Institutional Ethics Committee and the Declaration of Helsinki, 1975. All patients provided written informed consent. For patients under the age of 18 years, the written informed consent was signed simultaneously by patients and their parents.
Disease Types And Observation Indicators
Many factors prevent the foreskin from retracting smoothly from the glans, such as an abnormal tightness of the foreskin, the adhesion between foreskin and glans and so on, which is called phimosis. In brief, the foreskin cannot voluntarily retract and leak out the glans, or retraction does not automatically and smoothly return to the original position covering the glans. For redundant foreskin, the foreskin merely wraps around the glans and retracts smoothly and automatically to expose the glans. A penis that has normal size appears small either because it is buried in prepubic tissues or enclosed in scrotal tissue, which named concealed penis.
If the complication lasts longer than 90 days (3 months), we consider this to be a long-term complication, such as edema near the back of the penis or frenulum, scar hyperplasia and the uncomfortable feeling when touching the healed scar. The complete healing time is from the removal of the ring to the exfoliation of scab. Surgery time is from anesthesia to the end of the operation (excluding the anesthesia time). Patients are not only satisfied with the aesthetic appearance of the penis (generally satisfied or higher) but also have no long-term complications, which named successful circumcision (SC).
If the wound with redness, tenderness and swelling or with abscess and pus, this wound infected. After circumcision by CSR, the outer prepuce and inner prepuce were connected by scab. However, this scab connection is unstable in the early postoperative period. The tension between the outer prepuce and inner prepuce were increasing with the penile erecting, leading to the wound dehiscence. Therefore, this scab connection between the outer prepuce and inner prepuce were separated easily by erection and so on, which named wound dehiscence.
Follow-Up
Patients were followed up for 3 to 15 months after surgery (mean ± SD, 10.45 ± 5.83 months) through the out-patient review or other social software (such as QQ and WeChat designed by Tencent). The surgery time, wound healing time, satisfaction with the cosmetic appearance of the postoperative penis and the complications was observed by an investigator, and these indexes were used to assess the efficacy and safety in different groups. In addition, the collected data were checked and re-examined by another independent investigator.
Grouping
The patients were divided into three groups based on the age and the types of foreskin disease. The study also was evaluated through the subgroups that were grouping depended on the previous researches about the investigation on the development of the penis in Chinese.9,10 For the age, the subgroups consisted of childhood (n=243, age from 7 to 11 years or diameter from to 1.10 to 1.40 centimeter), adolescence (n=158, age from 12 to 16 years or diameter from to 1.46 to 1.94 centimeter) and adulthood (n=256, aged 17 or higher years or diameter from 2.14 or bigger centimeters). The types of foreskin diseases included two subgroups, phimosis (n=240) and redundant foreskin (n=417).
Circumcision Device (Chinese Shang Ring [CSR])
The CSR was produced by Wu Hu Snnda Medical Treatment Appliance Technology Co., Ltd., Wu Hu City, China, which had had the domestic patent. An inner, an outer ring, a silicon rubber gasket and a fastener constitute the CSR. The inner ring is a complete seamless circle, which has lots of sizes based on its inside diameter. This study involved in 16 sizes, including E (2.86 cm), F (2.77cm), G (2.71cm), H (2.64cm), I (2.51cm), K (2.32cm), M (2.13cm), O (1.94cm), Q (1.78cm), S (1.59cm), U (1.46cm), V (1.4cm), W (1.34cm), X (1.27cm), Y (1.18cm), Z (1.08cm).
Steps Of Operation
Preoperative preparation: the doctor introduces the surgical procedures and potential complications to patients, and lets patients sign the informed consent form. Besides, the doctor urges patients to clean the perineum on the scheduled surgery morning.
Operation
the standard surgical scrub with 0.1% polyvinyl pyrrolidone (PVP-I) and the local anesthesia with 1% lidocaine respectively are the preparatory work before surgery. Then, the procedure of circumcision was according to the standard methods described by Masson P4 and Cheng Y.11 Patients needed to remain this ring for seven days, and then the ring was removed. Besides, patients also required to disinfect the ring 2 to 3 times a day during these seven days.
Post-Operation
after seven days, the ring was removed by the special measures described by Masson P and Cheng Y.4,11 The wound should be covered with a bandage that should be removed after 24 hrs and should be keeping the wound clean and disinfecting the wound 2 to 3 times a day until the scab covered the wound.
Statistical Analysis
A closed questionnaire including five levels (1 to 5 scores) was used to evaluated satisfaction with the cosmetic appearance of the postoperative penis, extreme dissatisfaction (1 point), dissatisfaction (2 points), general satisfaction (3 points), satisfaction (4 points) and great satisfaction (5 points). The visual analog scale (VAS) (0 to 10 points) was used to assess the pain, which was obtained through the out-patient review or other social software, such as QQ and WeChat. A score of 0 indicates no pain, and a score of 10 indicates the most severe pain. When patients need to evaluate the degree of pain, the VAS was provided to them, and they used the scores as feedback for pain. The categorical variables and continuous variables were tested respectively by the Chi-square test and 2-tailed T-test, Mann–Whitney test or the analysis of variance (ANOVA). Univariate and multivariate logistic regression analysis are used to determine the independent risk factors associated with efficacy. The statistical analysis was performed with SPSS version 23.0 and statistical significance was considered at P<0. 05.
Results
Patient Demographics
A total of 657 cases were circumcised with CSR, including 240 cases with phimosis and 417 cases with redundant foreskin. All cases were wearing CSR successfully (Figure 1). Besides, the distribution of ages and sizes of the penis also was exhibited in Table 1. Some indexes were used to evaluate the safety and efficacy of CSR, including long-term complications, total complications, satisfaction with the cosmetic appearance of the postoperative penis (general satisfaction or higher), successful circumcision, surgery time and wound healing time. The above indexes in different subgroups were shown in Table 1.
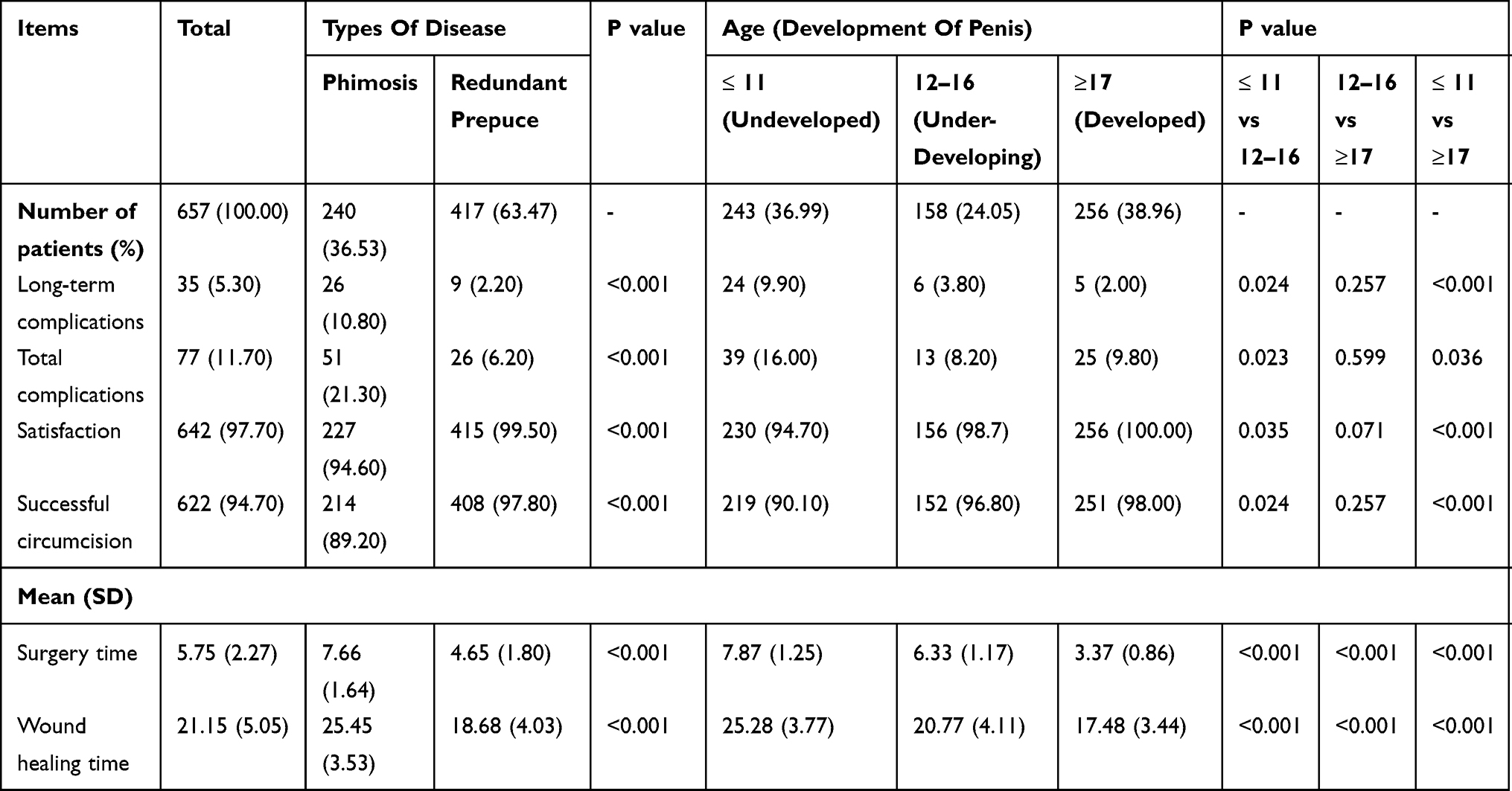 |
Table 1 Distribution Of Complications And Prognostic Indicators For Different Disease And Age Groups |
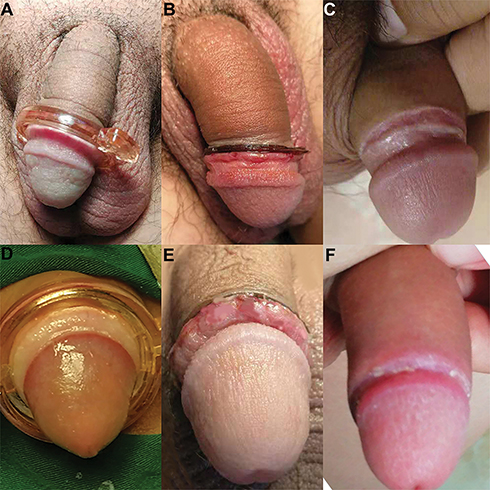 |
Figure 1 Normal process of circumcision with CSR. Wearing the CSR: adults (A) and children (D), the CSR removal: adults (B) and children (E) and wound healed: adults (C) and children (F). |
Comparison Of Indicators
Multivariate logistic regression analysis revealed that the phimosis (OR= 1.47, 95% CI=1.26–1.79, P<0.001) and childhood (OR= 1.13, 95% CI =1.06–1.36, P<0.001) were associated with poor efficacy. Besides, we compared the above indexes in different subgroups to understand whether the effect of CSR is the same in the population with different characteristics. For the surgery time and wound healing time, any two subgroups of age between the three subgroups had a statistically significant (P<0.001). For the long-term complications, total complications, satisfaction and successful circumcision, there were statistically significant between the subgroup of the undeveloped penis and under-developing penis in the group of the redundant foreskin (P = 0.024, etc. Details in Table 2). But the under-developing penis and the developed penis were not statistically significant (P>0.05). Beyond that, these indicators were compared in different groups, details in Table 2. Promoting the use of the CSR in areas with high HIV prevalence, such as Africa, the study also analyzed the effects at different ages segments (10–14, 15–29 and 30–49 years), which is recommended by the WHO (Table 3).
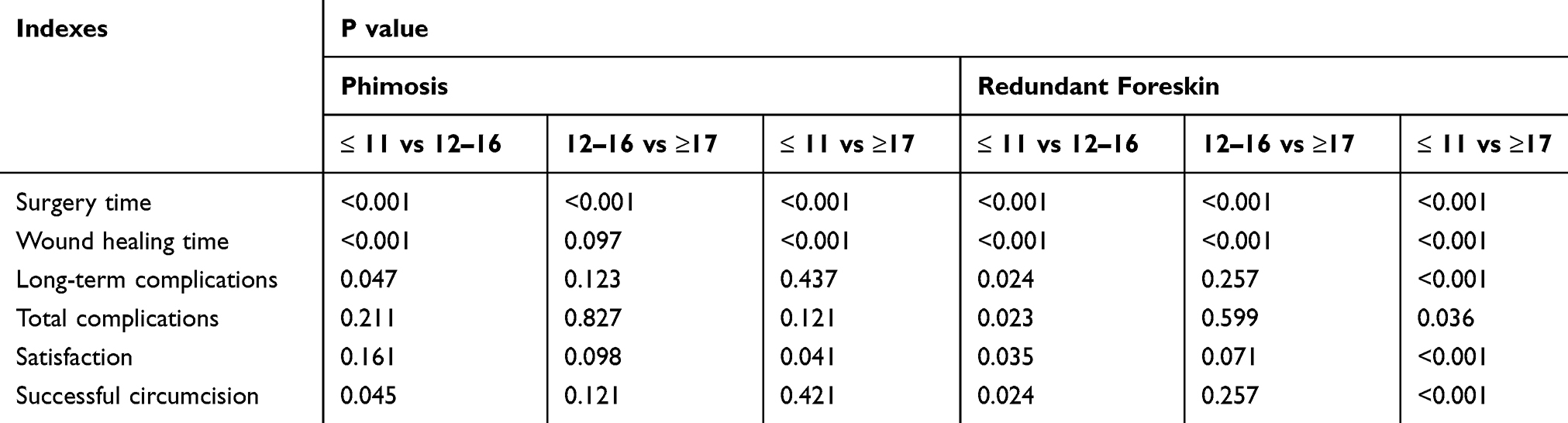 |
Table 2 Comparison Of Complications And Prognostic Indicators In Different Subgroups |
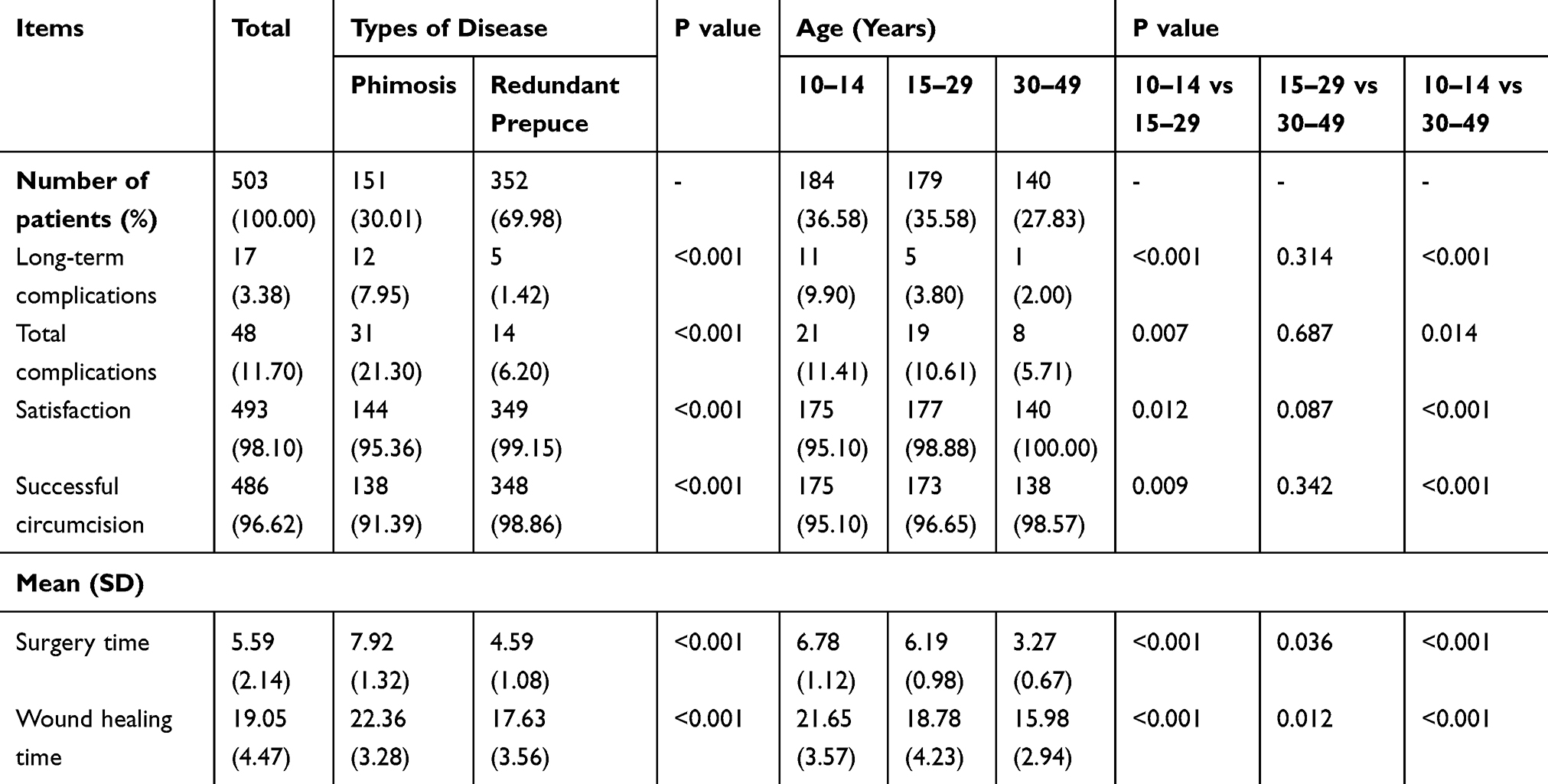 |
Table 3 Distribution Of Complications And Prognostic Indicators For Different Disease (phimosis And Redundant Prepuce) And Age Segments (10–14, 15–29 And 30–49 Years) |
Types And Distribution Of Complications
There were several complications, but most of the complication relieved without any special treatment. Most notably, changes in complications were dynamically observed in this study. Types and degree of complications varied with different groups and different follow-up time, as shown in Table 4. Fortunately, there were no incidents of injury to the frenulum in all cases. But there were 12 patients with wound dehiscence, and the wound was sutured by 3–0 absorbable line. From our results, we can know that the different penile sizes and phimosis may be contributed to the types and incidence of complications (shown in Table 4 and Figure 2). Although there was no statistically significant difference between adolescents and adults in terms of the long-term complications, total complications, satisfaction and successful circumcision, the incidence of postoperative pain and wound dehiscence in adults were higher than that in adolescents (P<0.05). Besides, postoperative pain changes at different stages were shown in Figure 3.
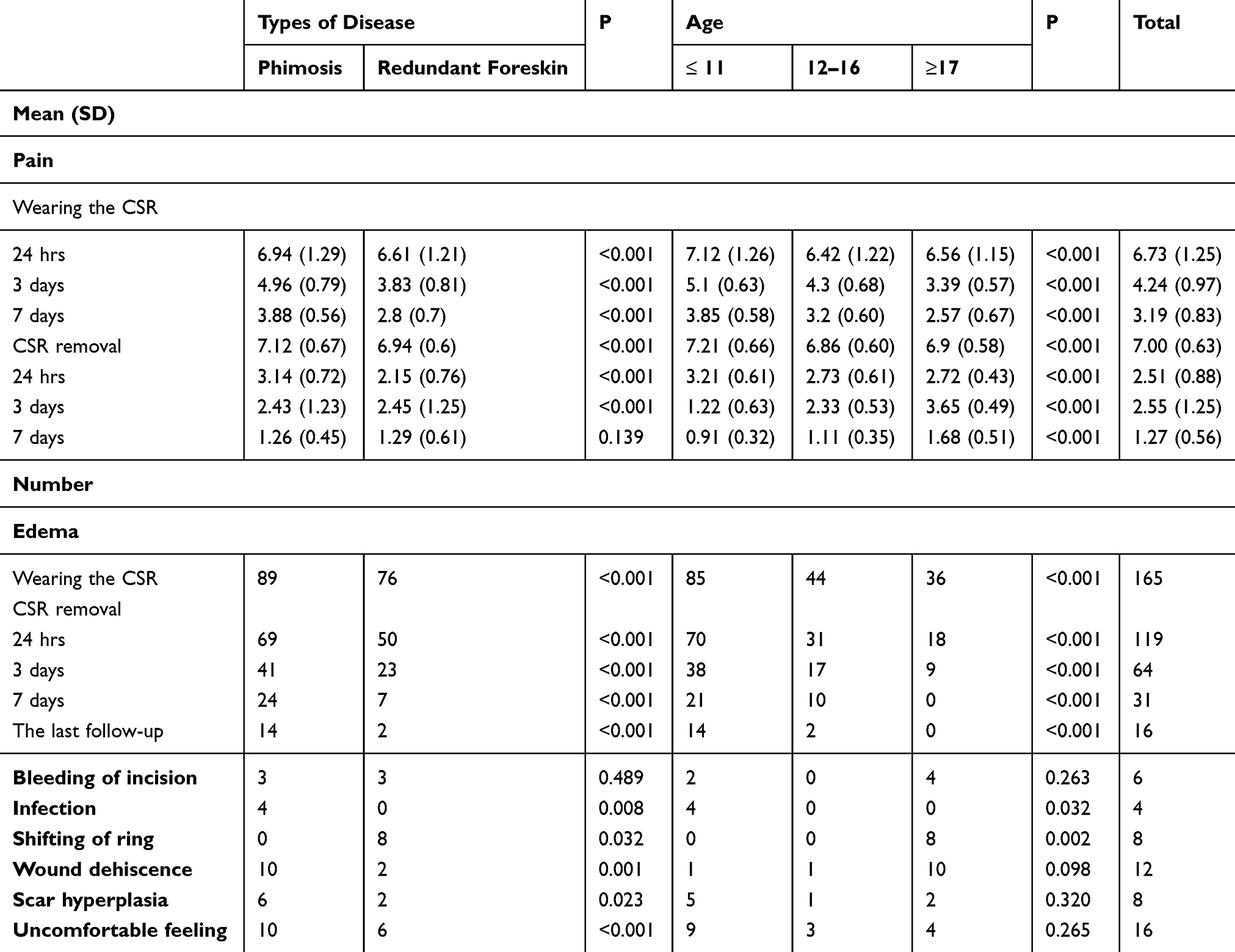 |
Table 4 The Types And Distribution Of Complications In Different Subgroups |
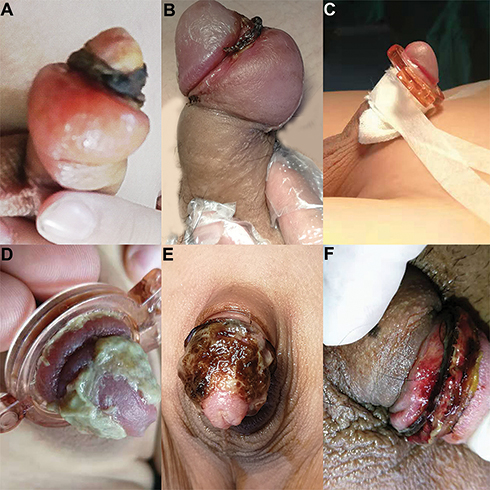 |
Figure 2 The types of complication. Edema and scar (A), edema in the back side of penis (B), pressure dressing (C), effusion of yellowish fluid caused by phimosis when wearing CSR (D) and CSR removal (E) and wound dehiscence (F). |
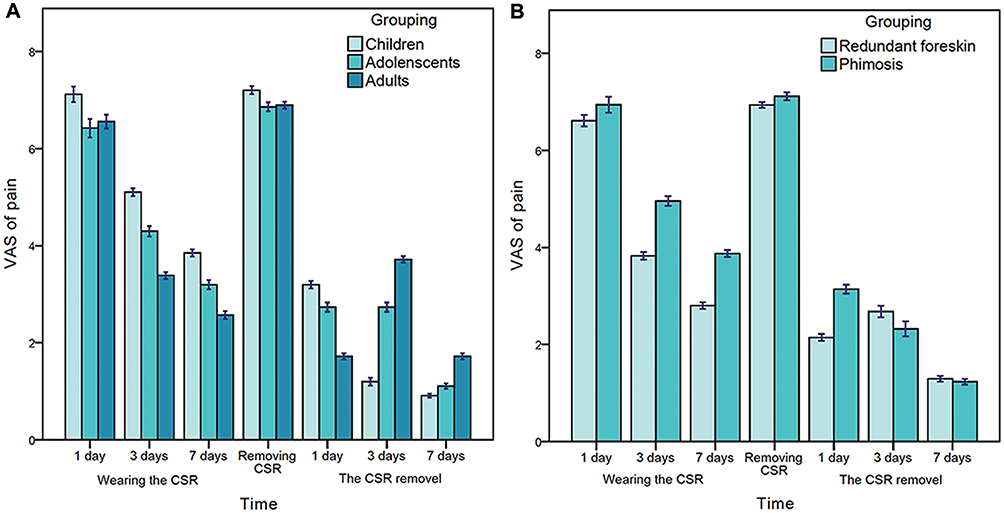 |
Figure 3 The degree of pain for different age (A) and types of disease (B) in different phase of post-operation. |
Discussion
Conventional circumcision was a classical surgery and was the most common method to circumcise before the invention and widespread use of CSR.11 With the great advantages of CSR was reported by many studies in China and Africa, CSR has gradually replaced conventional circumcision as the most used tool in China.2 Compared with the conventional circumcision, lots of advantages from CSR, including a lower incidence of complication, shorter operative time, more comfortable use and teaching, make it one of the circumcision measures recommended by WHO.5 Even so, are the CSR safe and suitable for everyone? At present, lots of studies focused on the efficacy of CSR in adults,3,4,12,13 because the use of CSR had a significant effect on reducing the risk of HIV and other sexually transmitted infections. Few prospective studies have compared the efficacy among adults, adolescents and children. Therefore, our research can add evidence for the efficacy of CSR in different ages.
Although the benefits of circumcision have been reported and promoted, including improving penile hygiene, increasing sexual pleasure and reducing the risk of HIV, the attitudes towards the need for male circumcision vary significantly from region to region, especially for children. In China, the prevalence of circumcision is still very low, and some urologists do not think that the redundant foreskin must be treated, and they does not suggest children who are the population with low risk of HIV play circumcision. As health awareness grows, more and more parents take their children to do circumcision to keep their penises clean. Notably, is the CSR suitable for the children? XiaoJun W et al and YiFeng P et al had reported the complication and other observation indexes for children.7,8 However, XiaoJun W et al classified the men aged from 7 to 17 years into children, which were unreasonable and may result in the bias of conclusion.8 Although YiFeng P et al respectively summarized the complications in the groups of children, adolescents and adults,7 the complications were not dynamically observed and just were described generally. Our research has some advantages that the above previous studies have not addressed. First, this study dynamically observed the types and degree of complications at the different postoperative time. Second, we reported in detail the incidence and types of complications in cohorts with different age and sizes of penis.
From the results, we can see that using CSR to do circumcision was safe and effective in total. Total complications, healing time, satisfaction and other prognostic indicators were consistent with previous studies. For the incidence of total complications, satisfaction and success rate, there was statistical significance between children and adolescents and between children and adults. However, these discrepancies between adolescents and adults did not exist. In addition, patients with phimosis had lower satisfaction and higher incidence of complications than patients with redundant foreskin. For example, the incidence of total complications in phimosis was three times that of the redundant foreskin. Besides, the logistic regression results showed that age and sizes of the penis were the independent risk factors for the efficacy of circumcision with CSR. Therefore, children owing undeveloped penis or patients with phimosis may not be suitable for circumcision with CSR. We suggest that, if there are no alternative measures, adolescents are the best fit population to circumcise with CSR. Phimosis could result in infection and affect the development of the penis, which must be treated immediately. But our research demonstrated that the prognosis of patients with phimosis was not as good as patients with redundant foreskin. For patients with phimosis, the adhesion between the foreskin and glans needs to be lysis before circumcision, which might cause the glans surface mucosa damage, leading to the continuous effusion of slight yellowish fluid from the damaged surface of the glans andmaking the process of wound healing slow. So, for these patients, we recommend that circumcision with CSR could be carried out after recovery of the glans surface damage caused by the lysis of adhesion between foreskin and glans. Because there wasn’t the effusion from the glans’ damaged surface affecting the wound healing so that the healed time will reduce and the incidence of complications also may decrease.
Of course, our medical center, at present, also has another sutureless technique, circumcision anastomat (CA). In general, CA is another device to circumcision. However, CA also has some disadvantages compared to CSR. First, the price of the CA is five times that of the CSR. Secondly, in our early observation of the efficacy, the incidence of CA complications, such as bleeding and pain, was relatively high. The incision bleeding resulted by CA is quite violent, which often need suturing wound to stop bleeding. Besides, anastomotic nail that was difficult to fall off automatically and required a second intervention to take out the nail. So, CSR is more economical and safer, and it is worth promoting.
For children with phimosis, urologists might recommend them to circumcise immediately. If we use CSR to do circumcision for these children, we may not get all the results we expected. If we don’t deal with phimosis, it can increase the risk of infection and affect penis development. How can we balance this conflict? For these children, urologists can first solve phimosis in childhood. Second, when these children enter puberty, they can receive circumcision if necessary, because it not only can solve the phimosis that must be resolved as early as possible but also can reduce the incidence of complications and increase the success rate.
The types and incidence of complication varied among children and adults, but pain and edema were the common focus issues. The procedure of circumcision with CSR was a continuous process, from wearing the CSR to the CSR removal. Therefore, the pain should be evaluated dynamically. Pain duration at removal and placement was different. During the removal process, the pain was transient and usually relieved within three minutes. During wearing the ring, the degree of pain was dynamic. The pain was very mild during normal life, and the pain was aggravated during exercise or erection. In addition, patients received the most unbearable pain in the first 24 hrs at post-circumcision and in the period of removing CSR. While wearing the CSR, the main objective of pain was children. On the contrary, after the CSR was removed, the pain that adults underwent was higher than children and adolescents, which was mainly caused by the erection that adults were more prone to having. In view this, we should pay more attention to pain management in the periods of wearing the CSR for children and after the removal of CSR for adults.
Besides, edema was the other most common complication. The incidence of edema varied with age and sizes of penis. Due to incomplete lymphatic and capillary circulation, the proportion of edema in children was the highest. For some children with edema, the lack of perfect lymphatic and capillary circulation, scab and scar hyperplasia led to slow relief of edema, which had a greater impact on wound healing. Eventually, some edema became the “meatball” that much like the elephantiasis caused by the lymph accumulation, so it required traditional surgery to cut off the meatball and suture the wound. According to our follow-up observation, if the edema cannot be eliminated within three months, this edema will be difficult to disappear automatically. For these patients, we adopted a series of interventions to promote the absorption and circulation of edema, including pressure dressing, sticking penis to the lower abdomen, hip bath by warm water and using Chinese traditional medicine. Unfortunately, there were still 16 patients with penile edema (2.4%) in our research, and most of them (87.5%) were children. So, it is more powerful evidence that the undeveloped penis lacking perfect lymphatic and capillary circulation maybe not suitable for circumcision with CSR.
In this study, there were 35 cases with unsuccessful circumcision (35/657, 5.3%). Most of the complications were unpredictable. But the wound dehiscence can be prevented if some necessary interventions are taken. The number of patients with wound dehiscence achieved 12 (1.82%), the majority of which (83.3%) were adults, which may be associated with the erection. Compared to children and adolescents, adults have more frequent and greater erection during sleeping or in the morning. So, the probability of wound dehiscence was higher than them. Besides, Most of the wound dehiscence occurred within three days of the CSR removal, rarely over seven days. So, preventing erection for adults also is a notable thing within three days of the CSR removal. In the processing of investigation, there were the incision bleeding and ring displacement (8/657, 1.21%), and participants reported that they had not tampered with the devices and that the slipping was spontaneous. However, before the ring slipped, all the men took part in the exercise. So, the friction between CSR and underwear may be the reason why the ring slipped. Therefore, patients should take a rest or slight activity in the period of wearing CSR and within three to seven days after the CSR removal. Last but not least, incision infection and long-term edema may result in the scar hyperplasia (8/657, 1.21%), and it also might be related to the individual differences. Fortunately, the scar hyperplasia has no effect on its function. Feeling discomfort (16/657, 2.44%) when they were touching the healed wound may be caused by the destruction of nerve endings. However,this discomfort does not affect life or penis function. Most of the discomfort was occurring when the patient was sleeping, and the patient could not detect the uncomfortable feeling when they were busy, such as working and studying. So, psychological factors cannot be ruled out.
Finally, our study also has several limitations. First, the statistical sample size is too small. We need to enlarge the sample to verify the conclusions. Second, the pain for children was evaluated by VAS, which may overestimate the degree of pain, because the subjective feeling of children is susceptible to patients in order to receive more parental attention and comfort.
Conclusion
In general, circumcision with CSR is a safe and efficacious method. But compared to patients with redundant foreskin, patients with phimosis had a higher incidence of complication and lower satisfaction. Besides, in terms of the whole efficacy, adolescents and adults were better than children. Therefore, circumcision with CSR is more suitable for adolescents and adults with redundant foreskin. Notably, adolescents have more advantages over adults in reducing the incidence of wound dehiscence and pain at the post-circumcision.
Data Sharing Statement
All data involved in this study are accessible from the authors on reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sokal D, Barone M, Simba R, et al. 925 randomized controlled trial of the shang ring versus conventional techniques for adult male circumcision in kenya and zambia. J Urol. 2012;187(4):e376–e377.2.
2. Yan B, You H, Zhang K. Circumcision with the Chinese Shang Ring in children: outcomesof 824 cases. Zhonghua Nan Ke Xue. 2010;16(3):250–3.3.
3. Barone MA, Ndede F, Li PS, et al. The Shang Ring device for adult male circumcision: a proof of concept study in Kenya. J Acquir Immune Defic Syndr. 2011;57(1):e7–e12. doi:10.1097/QAI.0b013e3182158967
4. Puneet M, Li PS, Barone MA. The Shang Ring device for simplified adult circumcision. Nat Rev Urol. 2010;7(11):638–642. doi:10.1038/nrurol.2010.167
5. January. WHO Technical Advisory Group on Innovations in Male Circumcision: Evaluation of Two Adult Devices. World Health Organization; 2013.
6. Huang C, Song P, Xu C, et al. Comparative efficacy and safety of different circumcisions for patients with redundant prepuce or phimosis: a network meta-analysis. Int J Surg. 2017;43:17–25.
7. Peng Y-F, Cheng Y, Wang G-Y, et al. Clinical application of a new device for minimally invasive circumcision. Asian J Androl. 2008;10(3):447–454. doi:10.1111/j.1745-7262.2008.00411.x
8. Xiaojun W, Yongquan W, Ji Z, et al. A report of 918 cases of circumcision with the Shang Ring: comparison between children and adults. Urology. 2013;81(5):1058–1063. doi:10.1016/j.urology.2012.11.046
9. Liu XQ, Zheng W, Zhao YW. Retrospective analysis for determinative value and size of penis and testicles in 4854 juveniles. J Clini Pediatr Surg. 2003;2(2):95–98.
10. Fu C, Pan F, Liu XL. Normal penile growth amongst Chinese. Chin J Pediatr Surg. 2010;31(6):432–434.
11. Cheng Y, Li PS, eds. Male Circumcision Using the Shang Ring. Beijing, China: People’s Medical Publishing House; 2012.
12. Feldblum PJ, Mwambula C, Selemani M, et al. Prospective observational study of the shang ring device for adult medical male circumcision in a routine clinical setting in Malawi. Afr J Reprod Health. 2016;20(4):60–66.
13. Sokal DC, Li PS, Zulu R, et al. Randomized controlled trial of the shang ring versus conventional surgical techniques for adultmale circumcision: safety and acceptability. J Acquir Immune Defic Syndr. 2014;65(4):447–455. doi:10.1097/QAI.0000000000000061
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.