")
Back to Journals » International Journal of General Medicine » Volume 15
Clinical Monitoring of Serum Levels of Vitamins A, D and E in Children with Recurrent Respiratory Tract Infections of Different Ages: A Clinical Controlled Trial
Authors Sun R, Yan Z, Yi W, Tian W, Sun M, Zhang J
Received 12 November 2021
Accepted for publication 2 February 2022
Published 17 August 2022 Volume 2022:15 Pages 6627—6632
DOI https://doi.org/10.2147/IJGM.S347728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rongrong Sun,1 Zhixin Yan,2 Wenxia Yi,2 Wenqiu Tian,2 Mei Sun,2 Jing Zhang1
1Children’s Ward, Cangzhou Central Hospital, Cangzhou, Hebei Province, People’s Republic of China; 2Cangzhou Central Hospital, Cangzhou, Hebei Province, People’s Republic of China
Correspondence: Jing Zhang, Children’s Ward, Cangzhou Central Hospital, Cangzhou City, Hebei Province, 061001, People’s Republic of China, Tel +86 15031730097, Email [email protected]
Objective: To study serum levels of vitamins A, D and E in children with recurrent respiratory tract infections of different ages and the correlation.
Methods: The clinical data of two groups of children of different ages were collected. The serum levels and deficiencies of vitamins A, D and E in children were statistically analyzed.
Results: The proportions of premature infants, low body weight infants, special physique, hospitalization history, hypocalcemia, living in a bungalow, and daily outdoor activities in less than 30 minutes in the case group were higher than those in the control group (χ2=4.507, 5.165, 7.040, 14.907, 4.267, 33.800, 4.507, 8.571, P < 0.05). The serum levels of vitamins A, D and E of children aged 0– 1, 2– 5, and 6– 12 in the case group were lower than those in the control group (P < 0.05). Compared with the control group, the serum vitamin A level of children in the case group was lower (t = 2.631, P < 0.05), and the deficiency rate was higher (χ2=24.200, P < 0.05).
Conclusion: Serum levels of vitamins A, D and E, which are related to birth mode, physical fitness, hospitalization history, hypocalcemia, vitamin deficiency, living environment, and daily outdoor activity time, vary in children with recurrent respiratory tract infections of different ages, and are lower in children with recurrent respiratory tract infections than in healthy children.
Keywords: different age groups, recurrent respiratory tract infections, children, serum vitamins A, D and E levels, correlation
Introduction
Recurrent respiratory tract infections are a repeated disease caused by pathogenic microorganisms invading the respiratory tract and multiplying, and are divided into upper respiratory tract infection and lower respiratory tract infection. They are very common in pediatrics, which are mainly attributed to low immunity in children, deficiencies in local or systemic host defense, pulmonary disorders caused by structural, functional, or environmental factors, with the main clinical manifestations of high fever, throat discomfort, loss of appetite, cough, and sputum,1 leading to serious physical and mental health problems and hindering the growth of children. Additionally, children with the disease are susceptible to pneumonia with a high fatality rate.2–4 Vitamins A, D, and E are multifunctional lipid-soluble compounds that are necessary for human health, and play an essential role in cell function for growth and immunity.1,5 Notwithstanding multiple studies have been reported on the association between vitamins A, D, and E insufficiency and the recurrent respiratory tract infections in children,1,4–6 the results remain inadequate. To fill this gap, this paper statistically analyzed the clinical data of 40 children with recurrent respiratory tract infections of different ages admitted to our hospital from February 2020 to February 2021, and studied its correlation with serum levels of vitamins A, D and E in children.
Materials and Methods
Ethical Statement
The protocol was approved by the Cangzhou Central Hospital. Written informed consent was obtained from each patient. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
Participants’ Characteristics
From February 2020 to February 2021, 40 children with recurrent upper respiratory tract infections treated in our hospital were retrospectively selected as the case group, and 40 children with healthy physical examination were enrolled as the control group. In the case group, children were 0–12 years old, with an average age of (6.25 ± 1.45) years old; there were 18 females (45.00%) and 22 males (55.00%); in terms of age groups, there were 12 cases (30.00%) aged 0–1 year, 20 cases (50.00%) aged 2–5 years, and 8 cases (20.00%) aged 6–12 years. The control group were 0–12 years old, with an average age of (6.42 ± 1.62) years old; there were 19 females (47.50%) and 21 males (52.50%); in terms of age groups, 12 cases (30.00%) were 0 to 1 years old, 19 cases (47.50%) were 2 to 5 years old, and 9 cases (22.50%) were 6 to 12 years old. The baseline information in the two groups of children was well balanced.
The ethics protocol was approved by the Cangzhou Central Hospital. Written informed consent was obtained from each patient. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Inclusion criteria: 1) All the enrolled children had complete medical records including underlying disease, prior hospitalization record and treatment history; 2) All met the diagnostic criteria for recurrent respiratory tract infections.3 Exclusion criteria: 1) Prior use of hormones and gamma globulin, etc.; 2) With supplementation of vitamins A, D and E.
Methods
Data Collection
The general data such as birth mode, physical fitness, feeding history, hospitalization history, hypocalcemia, pet exposure, living environment, and outdoor activity time of children in both groups were collected, and univariate and multivariate analyses were used to determine the risk factors for recurrent respiratory tract infections.
Detection Methods
Fasting venous blood (5 mL) was drawn from the two groups of children, centrifuged for 10 min at a rate of 3000 r/min, and the resultant supernatant was stored in a refrigerator at −20°C. Serum levels of vitamins A, D and E were determined by high performance liquid chromatography with the German Keysys fully automated chromatographic analyzer, with the reference ranges of >1.05 μmol/L (0.30 mg/L), ≥75 nmol/L, and >16.8 μmol/L (7.0 mg/L), respectively.4
Outcome Measures
1) The clinical data were compared between the two groups; 2) Serum levels of vitamins A, D and E of the two groups of children of different ages were detected and compared; 3) Serum vitamins A, D and E levels and deficiencies were compared between the two groups. Values below the reference range were considered to be vitamin deficient.
Statistical Analysis
All data analyses were performed with SPSS20.0 statistical software. Measurement data were represented by (x±s) and verified via t-test; enumeration data were expressed as rate (%), and processed using the chi-square test. The level of the statistical significance was set at P<0.05.
Results
Comparison of Clinical Data Between the Two Groups
The proportions of premature infants, low body weight infants, special physique, history of hospitalization, hypocalcemia, vitamin deficiency, living in a bungalow, and daily outdoor activities less than 30 minutes in the case group were higher than those in the control group (χ2=4.507, 5.165, 7.040, 14.907, 4.267, 33.800, 4.507, 8.571, P<0.05), but the proportions of children born by cesarean section, breastfeeding, and pet exposure were not significantly different between the two groups (χ2=0.050, 0.287, 0.092, P<0.05) Table 1.
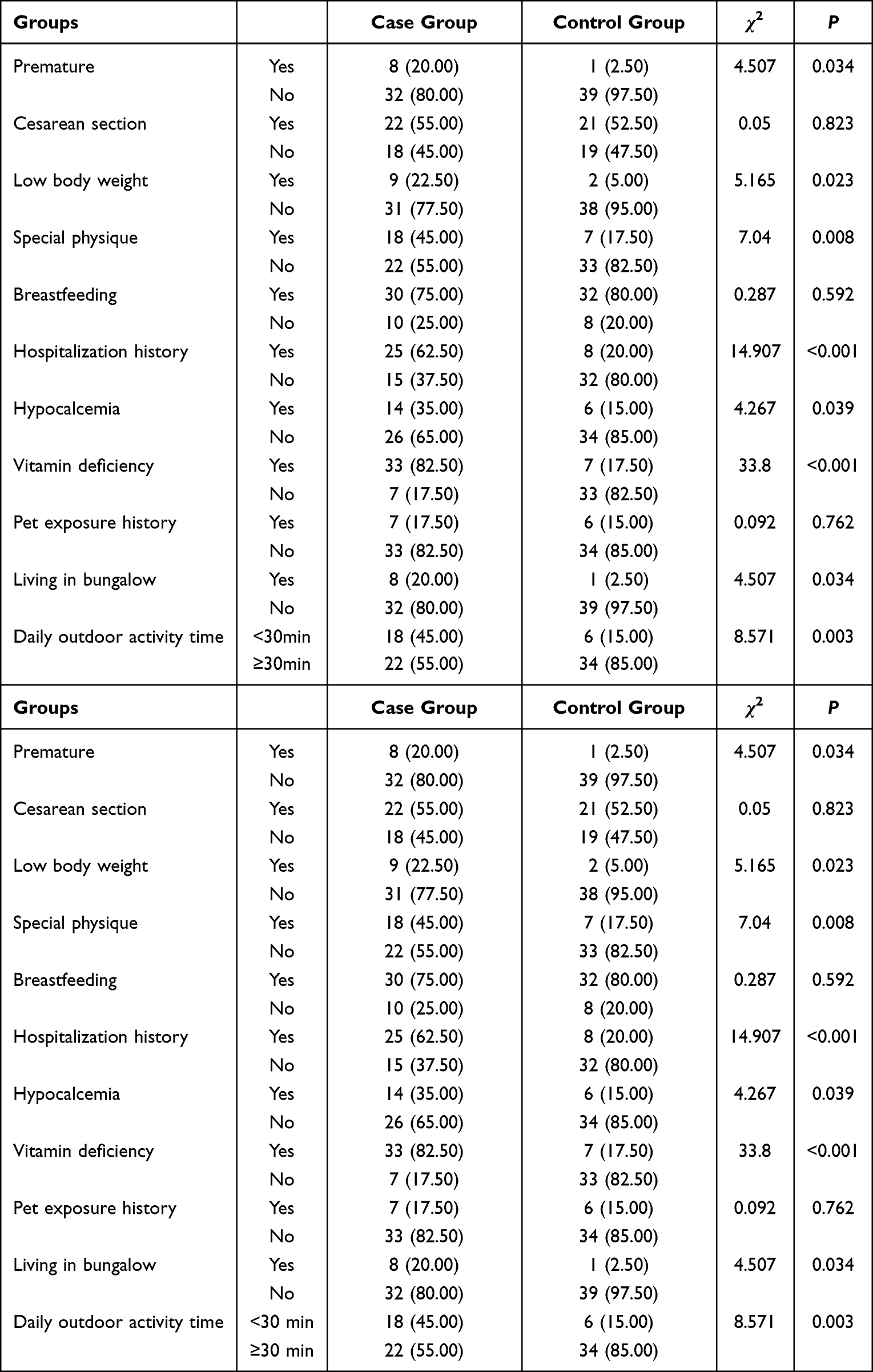 |
Table 1 Comparison of Clinical Data Between the Two Groups of Children [n(%)] |
Comparison of Serum Levels of Vitamins A, D and E Between the Two Groups of Children of Different Ages
In both groups, the level of serum vitamin A in children aged 2–5 years was higher than that in children aged 0–1 and 6–12 (P<0.05), and the level of serum vitamin A in children aged 6–12 was higher than that in children aged 0–1 (P<0.05); serum vitamin D levels in children aged 0–1, 2–5, and 6–12 gradually increased (P<0.05), while serum vitamin E levels gradually decreased (P<0.05). The serum levels of vitamins A, D and E of children aged 0–1, 2–5, and 6–12 in the case group were lower than those in the control group (P<0.05) Table 2.
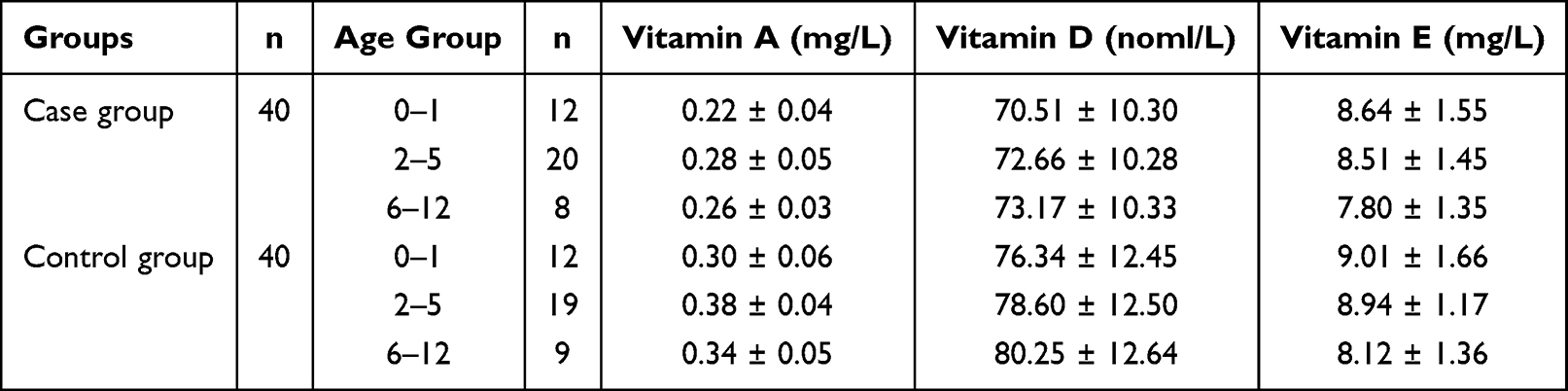 |
Table 2 Comparison of Serum Levels of Vitamins A, D and E Between the Two Groups of Children of Different Ages ( |

Comparison of Serum Vitamins A, D and E Levels and Deficiencies Between the Two Groups
Compared with the control group, the serum vitamin A level of children in the case group was lower (t = 2.631, P < 0.05), and the deficiency rate was higher (χ2=24.200, P<0.05). Serum vitamin D and E levels as well as the deficiency rate were not significantly different between the two groups (t = 0.724, 0.998, χ2=0.949, 0.000, P>0.05) Table 3.
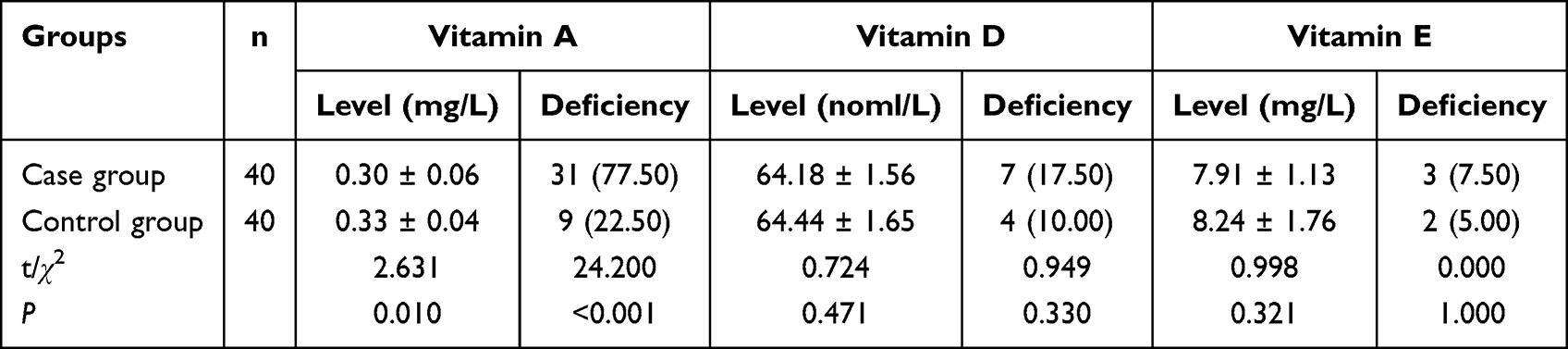 |
Table 3 Comparison of Serum Levels of Vitamins A, D and E and Deficiencies Between the Two Groups of Children |
Discussion
According to the results of this study, the serum levels of vitamins A, D and E of children aged 0–1, 2–5, and 6–12 in the case group were lower than those in the control group. To our knowledge, vitamin A is fat-soluble, also known as retinol. After ingestion by the body, it can not only maintain normal visual function but also maintain the health of epithelial tissue cells and provide favorable conditions for the synthesis of immunoglobulins. On the contrary, vitamin A deficiency can cause infectious diseases in children. Knowingly, vitamin D is also fat-soluble and plays an essential role as a human nutrient, with levels directly affecting recurrent respiratory tract infections and the body’s immune function. As for vitamin E, it is one of the most important antioxidants in the body that can promote the stability of vitamin A.6 Therefore, all these are attributed to the above-mentioned result. Additionally, the serum vitamin A level of children in the case group was lower than that of the control group, and the deficiency rate was higher, which was consistent with the results of the previous studies,7,8 indicating that children with recurrent respiratory tract infections have lower serum vitamins A, D and E levels, and higher deficiency rates compared with healthy children. All these results suggest that children with recurrent respiratory tract infections are directly affected by the body’s deficiencies of vitamins A, D and E, among which the vitamin deficiency symptoms are most obvious in children aged 0–1.
Moreover, the results of this study showed that the proportions of premature infants, low body weight infants, special physique, hospitalization history, hypocalcemia, living in a bungalow, and daily outdoor activities less than 30 minutes in the case group were higher than those in the control group, which was in line with the prior scholars8,9 who argued that children of different ages with recurrent respiratory tract infections are directly affected by the deficiencies of vitamins A, D and E, with those aged 0 to 1 most likely to suffer from deficiencies of there vitamins. The main risk factors for children with recurrent respiratory tract infections are lack of vitamins A, D and E, hypocalcemia, special physique, hospitalization history, living in a bungalow, and daily activity time of less than half an hour. Presumably, because of deficiencies of vitamins A, D and E, multiple hospitalizations, hypocalcemia and special physique would reduce the body’s immunity; bungalows lack adequate basic equipment and have poor air quality; short daily outdoor activities would weaken children’s physical fitness, all of which would predispose children to recurrent respiratory tract infections.
Children are the main victims of respiratory tract infections.10,11 Medical statistics show that the prevalence of recurrent respiratory tract infections in children is as high as 18%, which adversely affects the growth and development as well as the daily life of children.11 In the body’s basal metabolism, vitamins A, D and E and other nutrients play an essential role.12,13 In order to improve the quality of life of children with recurrent respiratory tract infections and avoid the deterioration of their condition, it is imperative to clarify the correlation of the levels of vitamins A, D and E with the pathology of recurrent respiratory tract infections and analyze the risk factors to ensure the physical and mental health of children. Taken together, although our study leads the way in examining the association between recurrent respiratory tract infections and vitamins A, D and E, three limitations merit attention. First, the sample size is small; second, the observation time is shorter; third, the study does not involve a prospective pilot trial. All would possibly bias our results toward the null. Therefore, further studies with larger samples, longer observation time and a prospective intervention are needed.
Overall, serum levels of vitamins A, D and E, being associated with birth mode, physical fitness, hospitalization history, hypocalcemia, vitamin deficiency, living environment, and daily outdoor activity duration, vary in children with recurrent respiratory tract infections of different ages, and are lower in children with recurrent respiratory tract infections compared with healthy children.
Disclosure
All authors declared that they have no conflict of interest.
References
1. Hibbs AM, Ross K, Kerns LA, et al. Effect of vitamin D supplementation on recurrent wheezing in black infants who were born preterm: the D-wheeze randomized clinical trial. JAMA. 2018;319(20):2086–2094. doi:10.1001/jama.2018.5729
2. Principi N, Marchisio P, Terranova L, et al. Impact of vitamin D administration on immunogenicity of trivalent inactivated influenza vaccine in previously unvaccinated children. Hum Vaccin Immunother. 2013;9(5):969–974. doi:10.4161/hv.23540
3. Gong F, Dai Y, Zheng T, et al. Peripheral CD4+ T cell subsets and antibody response in COVID-19 convalescent individuals. J Clin Invest. 2020;130(12):6588–6599. doi:10.1172/JCI141054
4. Wu D, Meydani SN. Age-associated changes in immune function: impact of vitamin E intervention and the underlying mechanisms. Endocr Metab Immune Disord Drug Targets. 2014;14(4):283–289. doi:10.2174/1871530314666140922143950
5. Yang C, Chen J, Guo N, et al. Comparison on the status of vitamin A in 6- to 13- year-old children between 2002 and 2012 in China. Nutr J. 2016;15(1):50. doi:10.1186/s12937-016-0170-0
6. Gupta P, Dewan P, Shah D, et al. Vitamin D supplementation for treatment and prevention of pneumonia in under-five children: a randomized double-blind placebo controlled trial. Indian Pediatr. 2016;53(11):967–976. doi:10.1007/s13312-016-0970-5
7. Tian W, Yi W, Zhang J, Sun M, Sun R, Yan Z. The correlation between the vitamin A, D, and E levels and recurrent respiratory tract infections in children of different ages. Am J Transl Res. 2021;13(5):5665–5671.
8. Zhang X, Ding F, Li H, et al. Low serum levels of vitamins A, D, and E are associated with recurrent respiratory tract infections in children living in Northern China: a case control study. PLoS One. 2016;11(12):e0167689. doi:10.1371/journal.pone.0167689
9. Wang X, Li X, Jin C, et al. Association between serum vitamin A levels and recurrent respiratory tract infections in children. Front Pediatr. 2021;9:756217. doi:10.3389/fped.2021.756217
10. Kwon CY, Lee B, Chang GT. Acupoint herbal patching for long-term immune function in children with recurrent respiratory-tract infections: a systematic review of real-world data. Med Acupunct. 2021;33(2):124–136. doi:10.1089/acu.2020.1444
11. Yin J, Xu B, Zeng X, Shen K. Broncho-Vaxom in pediatric recurrent respiratory tract infections: a systematic review and meta-analysis. Int Immunopharmacol. 2018;54:198–209. doi:10.1016/j.intimp.2017.10.032
12. Niu H, Wang R, Jia YT, Cai Y. Pidotimod, an immunostimulant in pediatric recurrent respiratory tract infections: a meta-analysis of randomized controlled trials. Int Immunopharmacol. 2019;67:35–45. doi:10.1016/j.intimp.2018.11.043
13. Onakpoya IJ, Hayward G, Heneghan CJ. Antibiotics for preventing lower respiratory tract infections in high-risk children aged 12 years and under. Cochrane Database Syst Rev. 2015;(9):CD011530. doi:10.1002/14651858.CD011530.pub2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.