")
Back to Journals » Cancer Management and Research » Volume 6
Clinical implications of recent studies using mTOR inhibitors to treat advanced hormone receptor-positive breast cancer
Authors Arena F
Received 30 October 2013
Accepted for publication 3 March 2014
Published 6 October 2014 Volume 2014:6 Pages 389—395
DOI https://doi.org/10.2147/CMAR.S56802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Francis Arena
Clinical Research Alliance, Lake Success, New York, NY, USA
Abstract: Breast cancer is a leading cause of cancer-related death worldwide. Approximately 75% of breast cancer is hormone receptor-positive (HR+) and is managed with endocrine therapies. However, relapse or disease progression caused by primary or acquired endocrine resistance is frequent. Phosphatidylinositol-3-kinase (PI3K)/protein kinase B (Akt)/mammalian target of rapamycin (mTOR)-mediated signaling is one of the molecular mechanisms leading to endocrine resistance. mTOR inhibitors that target the PI3K/Akt/mTOR pathway are the first of the targeted therapies to be evaluated in clinical trials to overcome endocrine resistance. Although the clinical trial with temsirolimus, an mTOR inhibitor, did not show any benefit when compared with endocrine therapy alone, a Phase II clinical trial with sirolimus has been promising. Recently, everolimus was approved in combination with exemestane by the US Food and Drug Administration for treating postmenopausal women with advanced HR+ breast cancer, based on the results of a Phase III trial. Therefore, everolimus represents the first and only targeted agent approved for combating endocrine resistance.
Keywords: advanced breast cancer, hormone receptor-positive, endocrine resistance, mTOR inhibitors
Introduction
Breast cancer is one of the most frequently diagnosed cancers and a leading cause of death among women worldwide. In 2008, the worldwide incidence of female breast cancer was approximately 1.4 million, and the estimated number of deaths as a result of breast cancer was more than 450,000.1 Breast cancer is the second most common cancer diagnosed in US women.2 Approximately 75% of primary breast cancers test positive for a hormone (estrogen or progesterone) receptor protein.3,4 Endocrine therapies such as tamoxifen, fulvestrant, and aromatase inhibitors that interfere with signaling through the estrogen receptor have revolutionized the treatment of hormone receptor-positive (HR+) breast cancer. Despite significant advances in the treatment of HR+ breast cancer, primary or acquired resistance to endocrine therapy is a major obstacle in this treatment and a frequent cause of disease recurrence.
Deregulation or aberrant signaling in the phosphatidylinositol-3-kinase (PI3K)/protein kinase B (Akt)/mammalian target of rapamycin (mTOR) signal transduction pathway through activation of mutations in PI3K or inactivation of mutations in protein tyrosine phosphatase is thought to contribute to the development of breast cancer.5–7 mTOR is a serine/threonine protein kinase located immediately downstream of the PI3K/Akt pathway and upstream of several key mediators of cell growth, proliferation, survival, metabolism, and angiogenesis (Figure 1).8–10 Activation of the mTOR pathway results in the phosphorylation of two downstream targets, the ribosomal p70 S6 kinase and the eukaryotic translation initiation factor 4E-binding protein, which mediate the translation of proteins involved in regulation of cell growth and proliferation.8,9 In addition, activation of mTOR may result in phosphorylation of several downstream effectors and transcription factors that regulate survival, metabolism, and angiogenesis.8,9 Therefore, mTOR is the central nexus in a series of signaling pathways that integrate intracellular nutrient, energy, and redox needs with extracellular amino acid, nutrient, growth factor, and cytokine availability.8
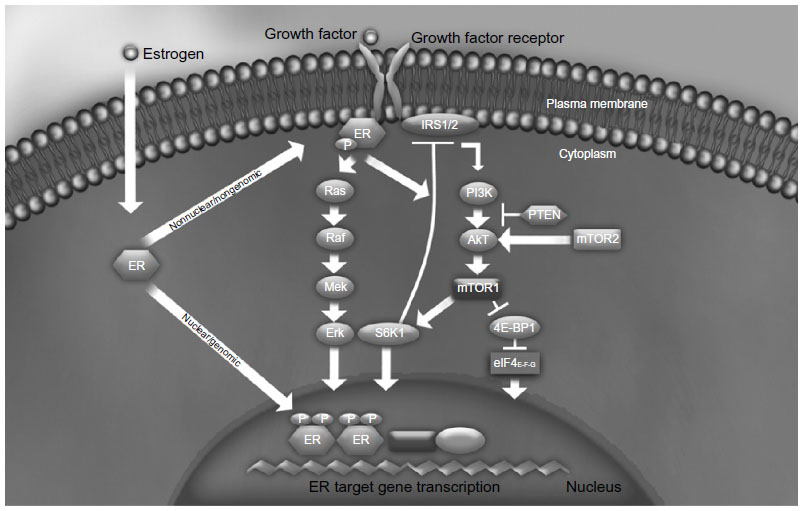 | Figure 1 PI3K/Akt/mTOR signaling pathway. |
Hormone-independent breast cancer cell growth is associated with increased PI3K/mTOR signaling and inhibition of PI3K and mTOR-induced apoptosis.11 Additionally, activation of the PI3K pathway after endocrine therapy was shown to be predictive of poor disease outcome.11 mTOR inhibition restores sensitivity to endocrine therapy in resistant breast cancer cells expressing aberrant Akt activity.12,13 Altogether, these preclinical observations suggest that mTOR plays a central role in endocrine resistance. As a strategy to overcome endocrine resistance, mTOR inhibitors have been studied in several clinical trials in combination with endocrine therapies, and recent evidence from these trials will be discussed here.
Temsirolimus
A Phase II study (NCT00062751)14 of temsirolimus in postmenopausal women with locally advanced or metastatic breast cancer showed that intermittent dosing of temsirolimus (30 mg daily for 5 days, every 2 weeks) plus daily letrozole (2.5 mg) improved the clinical benefit rate (80% versus 69%) and median progression-free survival (13.2 months versus 11.6 months), compared with daily letrozole alone.15 Based on this finding, intermittent dosing of temsirolimus was studied in combination with letrozole as first-line therapy in the Phase III HORIZON trial (NCT00083993)16 in postmenopausal women with aromatase inhibitor-naïve, HR+, locally advanced or metastatic breast cancer.17 Data from an interim analysis showed that the objective response rate (27% each) and median progression-free survival (hazard ratio [HR] 0.90; 95% confidence interval [CI] 0.76–1.07; P=0.25) were similar between the temsirolimus plus letrozole arm (n=556) and the letrozole alone (n=556) arm. No difference in overall survival (HR 0.89; 95% CI 0.65–1.23) was noted between the two arms.17 Therefore, lack of efficacy led to the early termination of this trial. The most frequently reported grade 3–4 adverse events in the Phase III trial were consistent with those observed in the Phase II trial with temsirolimus.17 Despite the lack of efficacy observed in the main trial, an exploratory subgroup analysis showed that, in patients ≤65 years of age, but not in those >65 years, temsirolimus plus letrozole improved median progression-free survival from 5.6 months to 9.0 months (HR 0.75; 95% CI 0.60–0.93; P=0.009),17 suggesting that temsirolimus plus letrozole might be beneficial in younger women; however, larger trials are necessary to confirm this finding.
Sirolimus
A Phase II trial in patients with HR+, human epidermal receptor 2-negative (HER2−) metastatic breast cancer evaluated the efficacy and safety of sirolimus in combination with tamoxifen.18 In patients whose disease progressed while they were receiving prior tamoxifen or an aromatase inhibitor, treatment with sirolimus plus tamoxifen significantly improved median progression-free survival from 3.3 months to 11.7 months (HR 0.43; 95% CI 0.25–0.92; P=0.0023).18 Sirolimus plus tamoxifen improved median progression-free survival by 7.0 months in the second part of this Phase II trial, in which patients with HR+, HER2− metastatic breast cancer who could not afford aromatase inhibitor therapy were randomly assigned to receive sirolimus plus tamoxifen and compared with those randomly assigned to receive tamoxifen alone (HR 0.48; 95% CI 0.25–0.93; P=0.0028).18 Respectively, anemia (21% versus 18%), hyperglycemia (16% versus 8%), hypercholesterolemia (11% versus 1%), hypertriglyceridemia (11% versus 1%), stomatitis (8% versus 0%), rash (7% versus 1%), anorexia (7% versus 2%), and fatigue (6% versus 8%) were the most frequently reported grade 3–4 adverse events with sirolimus plus tamoxifen or tamoxifen alone in this trial.18 Although the results of this small Phase II trial are promising, larger trials are necessary before sirolimus can be used to treat patients with advanced breast cancer.
Everolimus
Phase I studies suggested that treatment with everolimus in combination with endocrine therapy was feasible for patients with HR+ breast cancer.19 TAMRAD (NCT01298713),20 a randomized, open-label, Phase II study, evaluated the efficacy and safety of everolimus 10 mg/day plus tamoxifen 20 mg/day (n=54) versus tamoxifen 20 mg/day alone (n=57) in postmenopausal women with HR+, HER2−, aromatase inhibitor-resistant metastatic breast cancer.21 Randomization was stratified by primary (relapsing during or within 6 months of stopping adjuvant aromatase inhibitor treatment or progressing within 6 months of starting aromatase inhibitor treatment in the metastatic setting) and secondary resistance relapsing >6 months after stopping adjuvant aromatase inhibitors or responding for ≥6 months to aromatase inhibitors in the metastatic setting.21 The primary end point of clinical benefit rate was 61% (95% CI 47–74) among patients in the everolimus/tamoxifen arm, compared with 42% (95% CI 29–56) for patients in the tamoxifen only arm (exploratory P=0.045, Table 1).21 Time to progression was significantly longer in the combination group (8.6 months versus 4.5 months; exploratory P=0.002), and a 55% reduction in risk of death was associated with combination therapy (HR 0.45; 95% CI 0.24–0.81; exploratory P=0.007).21 The clinical benefit rate and time to progression were higher in patients receiving everolimus who had secondary hormone resistance (Table 1), suggesting a potential compensatory adaptive response to long-term estrogen depletion and a potential clinical benefit from adding everolimus to hormone therapy in this subpopulation of patients.21 The safety profile of everolimus was consistent with those of previous reports; the severity of most adverse events were grade 1 or 2, and the adverse events could be managed without treatment interruption.21 Adverse events more common in the combination group were stomatitis, rash, diarrhea, anorexia, and infection.21 The overall incidence of serious adverse events was similar in the two treatment groups.21
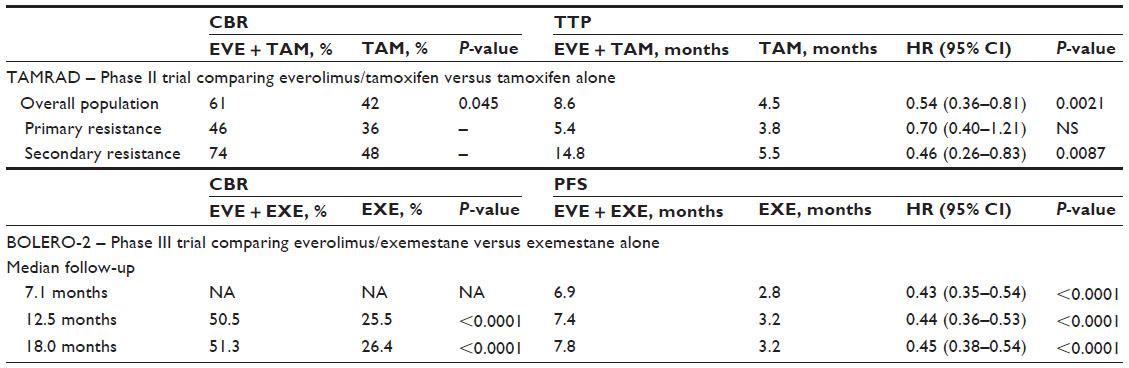 | Table 1 Efficacy of mTOR inhibitors in combination with endocrine therapy in HR+/HER2− patients with advanced breast cancer |
BOLERO-2 (NCT00863655),25 a randomized, international, double-blind, placebo-controlled Phase III study, evaluated the safety and efficacy of everolimus 10 mg/day plus exemestane 25 mg/day compared with exemestane 25 mg/day alone in postmenopausal women with HR+, HER2− advanced breast cancer with recurrence or progression after previous therapy with letrozole or anastrozole.22 Patients were randomly assigned 2:1 to receive everolimus (n=485) or placebo (n=239), in addition to open-label exemestane, in a blinded manner.22 Randomization was stratified according to the presence of visceral metastasis (yes or no) and sensitivity to previous hormonal therapy (yes or no).22 The primary efficacy analysis, reported at a median follow-up of 7.1 months, resulted in an estimated 57% risk reduction for progression-free survival (HR 0.43; 95% CI 0.35–0.54; P<0.001, local assessment, Table 1).22 This corresponded to a clinically meaningful 4.1-month prolongation in median progression-free survival from 2.8 months to 6.9 months.22 At a median follow-up of 12.5 months, a 56% reduction in risk of progression was identified (HR 0.44; 95% CI 0.36–0.53; P<0.0001, local assessment), corresponding to a 4.2-month prolongation in median progression-free survival from 3.2 months to 7.4 months (Table 1).23 Recently, at a median follow-up of 18 months, the median progression-free survival was 7.8 months compared with 3.2 months (HR 0.45; 95% CI 0.38–0.54, P<0.001, local assessment), for the combination therapy versus exemestane only therapy (P<0.001).24 Central assessment of median progression-free survival at 7.1 months, 12.5 months, and 18.0 months was consistent with local assessments.22–24 In addition, the objective response rate was significantly higher with combination therapy that with exemestane only therapy after 18 months of follow-up (12.6% versus 1.7%; P<0.0001).26 Respectively, the most common grade 3 or 4 adverse events were stomatitis (8% versus 1%), anemia (6% versus <1% ), dyspnea (4% versus 1%), hyperglycemia (4% versus <1%), fatigue (4% versus 1%), and pneumonitis (3% versus 0%) for everolimus plus exemestane compared with exemestane alone.22
There has been a series of exploratory subanalyses of different patient populations in the BOLERO-2 study. In patients younger than 65 years of age, everolimus plus exemestane was found to lower the risk of progression by 62% (HR 0.38; 95% CI 0.30–0.47) compared with exemestane alone.27 In patients ≥65 years of age, the risk of progression was reduced by 41% (HR 0.59; 95% CI 0.43–0.80).27 The improvement in median progression-free survival with everolimus plus exemestane in patients <65 years of age and ≥65 years of age was 6.83 months and 8.31 months, respectively.27 Also, an analysis of patients with visceral metastases showed that treatment with everolimus plus exemestane reduced the risk of progression by 53% in patients with visceral metastasis at baseline (HR 0.47; 95% CI 0.37–0.60), whereas the risk reduction was 59% in those without baseline visceral metastasis (HR 0.41; 95% CI 0.31–0.55).28 Everolimus plus exemestane also reduced the risk of progression by 61% (HR 0.39; 95% CI 0.25–0.62) in patients who had recurrence after neoadjuvant or adjuvant therapy.29 Additionally, using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 scale to evaluate patients’ health-related quality of life, the time to deterioration (ie, worsening) was longer with everolimus plus exemestane than with exemestane alone (8.3 months versus 5.8 months, P=0.0084).30
A recent randomized, double-blind, placebo-controlled Phase II study demonstrated that continuation with everolimus 10 mg/day was beneficial in patients with HER2− breast cancer and bone metastases.31 An exploratory analysis of the BOLERO-2 study showed that everolimus plus exemestane significantly lowered bone turnover marker levels at 6 and 12 weeks relative to baseline, irrespective of the presence or absence of baseline bone metastasis, whereas treatment with exemestane alone increased the levels of these markers.32 Even though progression of disease in bone was more severe in patients with baseline bone metastasis than in the overall population, progression in bone was significantly less severe in patients treated with everolimus plus exemestane than in those treated with exemestane alone.32 Patients with bone-only metastasis had a significant improvement in median progression-free survival with everolimus plus exemestane than with exemestane alone (12.88 months versus 5.29 months).28 Following these analyses, the long-term effects of mTOR inhibition with everolimus plus exemestane on bone health in postmenopausal women with HR+ locally advanced or metastatic breast cancer were assessed in the Phase IIIb, multicenter, open-label 4EVER study (NCT01626222).33 The preliminary results of 4EVER supported the findings of BOLERO-2, suggesting that everolimus provides a bone-protective effect that includes reduction of bone turnover and a reversal in the increased bone resorption associated with exemestane therapy.33
Two additional ongoing Phase II studies investigating the efficacy and safety of everolimus combined with endocrine therapy in postmenopausal women with HR+ advanced or metastatic breast cancer are currently being conducted. The multicenter, open-label BOLERO-4 (NCT01698918)34 trial will assess the safety and efficacy of first-line therapy with everolimus 10 mg/day plus letrozole 2.5 mg/day in postmenopausal women with ER+, HER2− metastatic breast cancer, and the beneficial effects of continuing everolimus plus endocrine therapy (exemestane 25 mg/day) beyond initial disease progression.35 The multicenter, open-label, randomized BOLERO-6 (NCT01783444)36 trial is also underway and will compare the efficacy and safety of everolimus plus exemestane and everolimus or capecitabine monotherapy in postmenopausal women with HR+, HER2− advanced breast cancer who progressed on prior anastrozole or letrozole therapy.37 These studies are expected to be completed in 2015, and their results should provide further evidence supporting the use of mTOR inhibitors, such as everolimus, in combination with endocrine therapy to improve outcomes in postmenopausal women with HR+, HER2− breast cancer.
Conclusion and future directions
Although the clinical trial with temsirolimus did not show any benefit, potentially because of issues related to dosing or patient selection, the clinical trials with everolimus and sirolimus provide important insight into the clinical usefulness of targeting the mTOR pathway to enhance the efficacy of available hormonal therapies and to overcome or minimize endocrine resistance in breast cancer. Therefore, use of mTOR inhibitors might delay the need for chemotherapy.
Despite clinical evidence demonstrating the clinical usefulness of mTOR inhibitors in the treatment of patients with breast cancer, limited research has been done on identification of biomarkers that can be used to identify patients who are most likely to benefit from these agents. Recent results from a translational study of the TAMRAD trial indicated that the benefit derived from everolimus therapy was greater in patients with low PI3K, low liver kinase B1, or high phosphorylated 4E binding protein 1 expression.38 Additionally, a retrospective exploratory biomarker analysis of the BOLERO-2 trial used next-generation sequencing to analyze numerous cancer-related genes and to determine if there were correlations between exon sequence or gene copy number variations and the efficacy of everolimus (ie, improvement in progression-free survival).39 The four most frequently altered genes/pathways were not predictive of everolimus efficacy when assessed individually, but a greater benefit from everolimus was seen in patients with minimal genetic alterations in the PIK3CA/phosphatase and tensin homolog/cyclin D1 or fibroblast growth factor receptor 1/2 genes combined (76% of the next-generation sequencing population).39 The findings of TAMRAD and BOLERO-2 provide useful information that may have important implications for the future clinical management of patients with breast cancer (ie, patient selection and identification of combinations of novel targeted therapies). However, these results will need to be validated in prospective studies of independent patient cohorts.
First-generation mTOR inhibitors, such as everolimus, appear to exert their inhibitory effects on the mTOR pathway by specifically targeting mTOR complex 1 (mTORC1) without binding to mTOR complex 2 (mTORC2).10 However, specific inhibition of mTORC1 by these agents may result in induction of prosurvival feedback loops, such as the PI3K-Akt pathway; this may explain why the antitumor activity of first-generation mTOR inhibitors is modest when administered alone.10 This limitation of first-generation mTOR inhibitors has led to development of the second generation of mTOR inhibitors, which includes adenosine triphosphate-competitive inhibitors that block both mTORC1 and mTORC2, as well as dual PI3K/mTOR inhibitors. Dual mTORC1/2 inhibitors currently in the early stages of clinical development include INK128, CC-223, OSI-027, AZD8055, AZD2014, and Palomid 529. However, caution should be taken with the use of second-generation mTOR inhibitors, because global inhibition of the PI3K/Akt/mTOR pathway may result in greater toxicity.
With the US Food and Drug Administration approval of everolimus to treat postmenopausal women with advanced HR+, HER2− breast cancer in combination with exemestane after failure of treatment with letrozole or anastrozole, everolimus is the first and only targeted agent approved for combating endocrine resistance. Inhibiting mTOR when treating patients with HR+, HER2− breast cancer is expected to improve treatment outcomes and might help to maintain quality of life.
Acknowledgments
The author thanks Lauren D’Angelo, Janardhan Sampath, Matthew Grzywacz, and ApotheCom, Yardley, PA for their editorial and technical support (funded by Novartis Pharmaceuticals Corporation) in the development of this manuscript.
Disclosure
FA has received grant support from and is a member of the scientific advisory board for Novartis Pharmaceuticals Corporation. The author reports no other conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics, 2011. CA Cancer J Clin. 2011;61(2):69–90. | |
American Cancer Society. Cancer facts and figures, 2013. Atlanta, GA, USA: American Cancer Society; 2013. Available from: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-036845.pdf. Accessed March 5, 2014. | |
Setiawan VW, Monroe KR, Wilkens LR, Kolonel LN, Pike MC, Henderson BE. Breast cancer risk factors defined by estrogen and progesterone receptor status: the Multiethnic Cohort Study. Am J Epidemiol. 2009;169(10):1251–1259. | |
Anderson WF, Chatterjee N, Ershler WB, Brawley OW. Estrogen receptor breast cancer phenotypes in the Surveillance, Epidemiology, and End Results database. Breast Cancer Res Treat. 2002;76(1):27–36. | |
Bachman KE, Argani P, Samuels Y, et al. The PIK3CA gene is mutated with high frequency in human breast cancers. Cancer Biol Ther. 2004;3(8):772–775. | |
Saal LH, Holm K, Maurer M, et al. PIK3CA mutations correlate with hormone receptors, node metastasis, and ERBB2, and are mutually exclusive with PTEN loss in human breast carcinoma. Cancer Res. 2005;65(7):2554–2559. | |
Perez-Tenorio G, Alkhori L, Olsson B, et al. PIK3CA mutations and PTEN loss correlate with similar prognostic factors and are not mutually exclusive in breast cancer. Clin Cancer Res. 2007;13(12):3577–3584. | |
Huang J, Manning BD. The TSC1-TSC2 complex: a molecular switchboard controlling cell growth. Biochem J. 2008;412(2):179–190. | |
Margariti N, Fox SB, Bottini A, Generali D. Overcoming breast cancer drug resistance with mTOR inhibitors. Could it be a myth or a real possibility in the short-term future? Breast Cancer Res Treat. 2011;128(3):599–606. | |
Villarreal-Garza C, Cortes J, Andre F, et al. mTOR inhibitors in the management of hormone receptor-positive breast cancer: the latest evidence and future directions. Ann Oncol. 2012;23(10):2526–2535. | |
Miller TW, Hennessy BT, Gonzalez-Angulo AM, et al. Hyperactivation of phosphatidylinositol-3 kinase promotes escape from hormone dependence in estrogen receptor-positive human breast cancer. J Clin Invest. 2010;120(7):2406–2413. | |
Beeram M, Tan QT, Tekmal RR, Russell D, Middleton A, deGraffenried LA. Akt-induced endocrine therapy resistance is reversed by inhibition of mTOR signaling. Ann Oncol. 2007;18(8):1323–1328. | |
deGraffenried LA, Friedrichs WE, Russell DH, et al. Inhibition of mTOR activity restores tamoxifen response in breast cancer cells with aberrant Akt activity. Clin Cancer Res. 2004;10(23):8059–8067. | |
Wyeth/Pfizer. Study Evaluating Temsirolimus (CCI-779) In Breast Neoplasms. In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2003 [updated April 13, 2011]. Available from http://clinicaltrials.gov/ct2/show/NCT00062751. NLM identifier: NCT00062751. Accessed March 11, 2014. | |
Carpenter J, Roche H, Campone M, et al. Randomized 3-arm, phase 2 study of temsirolimus (CCI-779) in combination with letrozole in postmenopausal women with locally advanced or metastatic breast cancer. Abstract 564 presented at the American Society of Clinical Oncology Annual Meeting, May 13–17, 2005, Orlando, FL, USA. | |
Wyeth/Pfizer. Study Evaluating CCI-779 and Letrozole in Post-menopausal Women With Breast Cancer. In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2004 [updated November 7, 2011]. Available from http://clinicaltrials.gov/ct2/show/NCT00083993?term=NCT00083993&rank=1. NLM identifier: NCT00083993. Accessed March 11, 2014. | |
Wolff AC, Lazar AA, Bondarenko I, et al. Randomized phase III placebo-controlled trial of letrozole plus oral tmsirolimus as first-line endocrine therapy in postmenopausal women with locally advanced or metastatic breast cancer. J Clin Oncol. 2013;31(2):195–202. | |
Bhattacharyya GN, Biswas J, Singh JH, et al. Reversal of tamoxifen resistance (hormone resistance) by addition of sirolimus (mTOR inhibitor) in metastatic breast. Abstract 16LBA presented at the 2011 European Multidisciplinary Cancer Congress, September 23–27, 2011, Stockholm, Sweden. | |
Awada A, Cardoso F, Fontaine C, et al. The oral mTOR inhibitor RAD001 (everolimus) in combination with letrozole in patients with advanced breast cancer: results of a phase I study with pharmacokinetics. Eur J Cancer. 2008;44(1):84–91. | |
ARCAGY/GINECO Group. Tamoxifen-RAD001 Versus Tamoxifen Alone in Patients With Anti-aromatase Resistant Breast Metastatic Cancer. In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2011. Available from http://clinicaltrials.gov/ct2/show/NCT01298713?term=NCT01298713&rank=1. NLM identifier: NCT01298713. Accessed March 11, 2014. | |
Bachelot T, Bourgier C, Cropet C, et al. Randomized Phase II trial of everolimus in combination with tamoxifen in patients with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer with prior exposure to aromatase inhibitors: a GINECO study. J Clin Oncol. 2012;30(22):2718–2724. | |
Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone receptor-positive advanced breast cancer. N Engl J Med. 2012;366(6):520–529. | |
Hortobagyi GN, Piccart M, Rugo H, et al. Everolimus for postmenopausal women with advanced breast cancer: updated results of the BOLERO 2 Phase III trial. Abstract S3-7 presented at the CTRC-AACR San Antonio Breast Cancer Symposium, December 6–10, 2011, San Antonio, TX, USA. | |
Yardley DA, Noguchi S, Pritchard KI, et al. Everolimus plus exemestane in postmenopausal patients with HR(+) breast cancer: BOLERO-2 final progression-free survival analysis. Adv Ther. 2013;30(10):870–884. | |
Novartis Pharmaceuticals. Everolimus in Combination With Exemestane in the Treatment of Postmenopausal Women With Estrogen Receptor Positive Locally Advanced or Metastatic Breast Cancer Who Are Refractory to Letrozole or Anastrozole (BOLERO2). In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2009 [updated October 18, 2013]. Available from http://clinicaltrials.gov/ct2/show/NCT00863655?term=NCT00863655&rank=1. NLM identifier: NCT00863655. Accessed March 11, 2014. | |
Burris H, Gnant M, Hortobagyi G, et al. Characterization of response to everolimus (EVE) in BOLERO-2: a phase 3 trial of EVE plus exemestane (EXE) in postmenopausal women with HR+, HER2− advanced breast cancer. Abstract P2-16-17 presented at the San Antonio Breast Cancer Symposium, December 10–14, 2013, San Antonio, TX, USA. | |
Pritchard KI, Burris HA 3rd, Ito Y, et al. Safety and efficacy of everolimus with exemestane vs exemestane alone in elderly patients with HER2-negative, hormone receptor-positive breast cancer in BOLERO-2. Clin Breast Cancer. 2013;13(6):421–432. | |
Campone M, Bachelot T, Gnant M, et al. Effect of visceral metastases on the efficacy and safety of everolimus in postmenopausal women with advanced breast cancer: subgroup analysis from the BOLERO-2 study. Eur J Cancer. 2013;49(12):2621–2632. | |
Beck JT, Hortobagyi GN, Campone M, et al. Everolimus plus exemestane as first-line therapy in HR+ HER2− advanced breast cancer in BOLERO-2. Breast Cancer Res Treat. 2014;144(3):459–467. | |
Burris HA III, Lebrun F, Rugo HS, et al. Health-related quality of life of patients with advanced breast cancer treated with everolimus plus exemestane versus placebo plus exemestane in the phase 3, randomized, controlled, BOLERO-2 trial. Cancer. 2013;119(10):1908–1915. | |
Maass N, Harbeck N, Mundhenke C, et al. Everolimus as treatment for breast cancer patients with bone metastases only: results of the phase II RADAR study. J Cancer Res Clin Oncol. 2013;139(12):2047–2056. | |
Gnant M, Baselga J, Rugo HS, et al. Effect of everolimus on bone marker levels and progressive disease in bone in BOLERO-2. J Natl Cancer Inst. 2013;105(9):654–663. | |
Hadji P, Lüftner D, Fasching PA, et al. 4EVER: Does mTOR inhibition have a major clinical impact on bone health in postmenopausal women with hormone receptor positive (HR+) locally advanced breast cancer treated with everolimus (EVE) in combination with exemestane (EXE)? Abstract P6-06-32 presented at the San Antonio Breast Cancer Symposium, December 10–14, 2013, San Antonio, TX, USA. | |
Novartis Pharmaceuticals. Open-label, Phase II, Study of Everolimus Plus Letrozole in Postmenopausal Women With ER+, HER2- Metastatic or Locally Advanced Breast Cancer (Bolero-4). In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2012 [updated February 6, 2014]. Available from http://clinicaltrials.gov/ct2/show/NCT01698918?term=NCT01698918&rank=1. NLM identifier: NCT01698918. Accessed February 6, 2014. | |
Gradishar WJ, Bachelot TD, Saletan S, et al. BOLERO-4: multicenter, open-label, phase II study of everolimus plus letrozole as first-line therapy in ER+, HER2− metastatic breast cancer. Abstract TPS661 presented at the American Society of Clinical Oncology Annual Meeting, May 31 to June 4, 2013, Chicago, IL, USA. | |
Novartis Pharmaceuticals. A Phase II Study of Everolimus in Combination With Exemestane Versus Everolimus Alone Versus Capecitabine in Advance Breast Cancer. (BOLERO-6). In: ClinicalTrials.gov [website on the Internet]. Bethesda, MD: US National Library of Medicine; 2013 [updated February 28, 2014]. Available from http://clinicaltrials.gov/ct2/show/NCT01783444?term=NCT01783444&rank=1. NLM identifier: NCT01783444. Accessed February 28, 2014. | |
Ejlertsen B, Jerusalem GHM, Hurvitz SA, et al. BOLERO-6: Phase II study of everolimus plus exemestane versus everolimus or capecitabine monotherapy in HR+, HER2− advanced breast cancer. Abstract TPS660 presented at the American Society of Clinical Oncology Annual Meeting, May 31 to June 4, 2013, Chicago, IL, USA. | |
Treilleuz I, Arnedos M, Cropet C, et al. Predictive markers of everolimus efficacy in hormone receptor positive (HR+) metastatic breast cancer (MBC): final results of the TAMRAD trial translational study. Abstract 510 presented at the American Society of Clinical Oncology Annual Meeting, May 31 to June 4, 2013, Chicago, IL, USA. | |
Hortobagyi GN, Piccart-Gebhart MJ, Rugo HS, et al. Correlation of molecular alterations with efficacy of everolimus in hormone receptor–positive, HER2-negative advanced breast cancer: results from BOLERO-2. Abstract LBA509 presented at the American Society of Clinical Oncology Annual Meeting; May 31 to June 4, 2013, Chicago, IL, USA. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.