")
Back to Journals » Psychology Research and Behavior Management » Volume 10
Clinical impact of early diagnosis of autism on the prognosis and parent-child relationships
Authors Elder JH, Kreider CM , Brasher SN, Ansell M
Received 15 April 2017
Accepted for publication 19 June 2017
Published 24 August 2017 Volume 2017:10 Pages 283—292
DOI https://doi.org/10.2147/PRBM.S117499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Video abstract presented by Jennifer Harrison Elder.
Views: 635
Jennifer Harrison Elder,1 Consuelo Maun Kreider,2 Susan N Brasher,3 Margaret Ansell4
1Department of Family and Community Health Nursing Science, 2Department of Occupational Therapy, University of Florida, Gainesville, FL, 3Nell Hodgson Woodruff School of Nursing, Emory University, Atlanta, GA, 4Health Science Center Libraries, University of Florida, Gainesville, FL, USA
Abstract: Autism spectrum disorder (ASD) refers to a lifelong condition that usually appears in late infancy or early childhood, and is characterized by social and communication deficits that impede optimal functioning. Despite widespread research and greater public awareness, ASD has an unclear etiology and no known cure, making it difficult to acquire accurate and timely diagnoses. In addition, once an ASD diagnosis is made, parents find it challenging to navigate the healthcare system and determine which interventions are most effective and appropriate for their child. A growing body of evidence supports the value of early diagnosis and treatment with evidence-based interventions, which can significantly improve the quality of life of individuals with ASD as well as of their carers and families. Particularly noteworthy are early interventions that occur in natural surroundings and can be modified to address age-related goals throughout the lifespan. Therefore, the purpose of this review is to: 1) provide readers with a brief background related to ASD; 2) describe commonly used screening instruments and tools for early diagnosis; 3) describe early interventions that have empirical support; and 4) discuss how the parent–child and family relationships can be affected through this process. This information can provide professionals with information they can use to assist families who make critical and potentially life-changing decisions for children with ASD.
Keywords: autism spectrum disorder, ASD, early diagnosis, early intervention, parent–child relationship
Introduction
Autism spectrum disorder (ASD) refers to a group of neurodevelopmental conditions characterized by a wide range of symptoms, skills, and levels of disability. First described in the 1940s by Leo Kanner,1 autism was once considered to be a rare condition. Despite the consensus that ASD diagnoses occur more frequently today, researchers continue to debate whether this is a result of new cases or simply the availability of better diagnostic measures, or even a combination of both. Regardless, one cannot dismiss the fact that the Centers for Disease Control and Prevention (CDC) notes that ASD is a prevalent condition, with 1 in 68 children identified with some form of ASD.2 Symptoms appear in the first 2 years of life and affect the individual’s ability to function socially, at school, at work, or in other areas of life. Although current treatments vary, most interventions focus on managing behavior and improving social and communication skills to enable optimal social functioning and independence.3–8
When determining the presence of ASD, clinician appraisal of ASD symptoms remains the current standard for diagnosis. Diagnostic criteria were revised in 2013 with the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), which delineates two core ASD symptoms: persistent social and communication deficits and the presence of restricted, repetitive patterns of behaviors and/or interests, and sensory differences.9 Additionally, ASD severity, which categorizes the impact of symptoms on the individual’s adaptive functioning, is now considered in the diagnostic process.9 Advances in ASD science challenge traditional conceptualizations of ASD as a discrete phenotype10 and, instead, posit that ASD exists along a continuum of neurodiversity.11 Indeed, multiple studies have applied quantitative measurements to ASD symptoms and traits and demonstrated the continuous distribution of ASD traits across human populations.12–14 As a result, some researchers now support the use of standardized, percentile-based descriptions of ASD symptom manifestation.15,16 These percentile-based methods have been used successfully in the characterization of other quantifiable clinical conditions, such as anorexia nervosa and hypertension.16 At present, expert clinical judgment is required to evaluate the presence of significant impairment in the core symptom areas, thus determining the presence (or absence) of ASD.
Some individuals with ASD are mildly impaired by their symptoms, whereas others are profoundly impaired.9,17 Although the heterogeneity in ASD is well-accepted, the range of ASD symptoms can be classified into broad categories of core symptoms and secondary symptoms. Secondary symptoms can include conditions such as intellectual impairment, which occurs in approximately 50% of patients with ASD,18 self-injury, aggressiveness toward others, sleeping disorders, eating disturbances, and seizures. Additionally, for individuals with ASD, symptom manifestation can change throughout the lifespan. For instance, language difficulties and hyperactivity that is often seen in younger children can shift to relational problems, mood dysregulation, and hypo-activity in adolescence and young adulthood.19–21 In summary, characterizing ASD can be challenging, but progress has been made in refining diagnostic processes that can be addressed over the lifespan.
Search methodology
In recognition of how rapidly the field of ASD has changed, a state-of-the-art science review was conducted, as described by Grant and Booth,22 whereby the purpose is to provide broad and up-to-date information related to the early diagnosis and treatment of ASD. This included a PubMed search for literature related to three major concepts: parent–child relationships, autism, and diagnosis. The search for the parent–child relationships concept was conducted using the exploded major MeSH term “Parent-Child Relations” or any one of these phrases in the title or abstract: “parent-child relationship”, “mother-child relationship”, or “father-child relationship”. Similarly, we searched for the autism concept using the MeSH terms “Autistic Disorder” or “Autism Spectrum Disorder”, or the presence of the truncated word autis* in the title. Finally, the concept of diagnosis was searched for very broadly with the term “diagnosis” in the title, abstract, or MeSH terms. In order to ensure a thorough review of the literature, a secondary search was also run; in this search, 1) the criteria for the parent–child relationships concept was broadened to include non-major MeSH terms, and 2) emphasis was placed on early diagnosis and interventions, which led to searches for the terms “early” and “diagnosis” in the title, abstract, or MeSH terms of the records.
The search was conducted on March 16, 2017, with a narrower scope for early diagnosis and then a broader scope for parent–child relationship. This yielded an initial result set of 53 records, which was narrowed down to 31 after a review of the title/abstract. The second search, which included broader search terms related to diagnosis, but narrower terms related to the parent–child relationship, retrieved 98 records, 60 of which were included after a review of the title/abstract. No filters were used in either search strategy. Inclusion criteria used to conduct the title/abstract review were: 1) English-language observational or interventional studies, 2) examining children with ASD, 3) including data/information about time/age of diagnosis, and 4) including data/information about the quality of the parent–child relationship. Studies that focused on the well-being of parents of children with ASD or examined parent–child relationships as the cause of specific ASD characteristics were excluded. The following discussion and concluding recommendations are based on results of this search.
The ASD screening and diagnostic instruments described in Table 1 were selected from an extensive search of ASD screening literature. The most recent search for screening/diagnostic instruments for ASDs was performed on May 15, 2017. The authors searched PubMed for literature related to the concepts of autism, diagnosis, and survey instruments. The autism concept was searched for using the MeSH terms “Autistic Disorder” or “Autism Spectrum Disorder”, or the presence of the truncated word autis* in the title. The concept of diagnosis was searched for very broadly using the MeSH term “Diagnosis”, the term “screening”, or the truncated word diagnos* in the title, abstract, or MeSH terms of the records. The survey instruments concept was searched using the exploded MeSH term “Surveys and Questionnaires” or the truncated word instrument* or the word tool in the title or abstract.
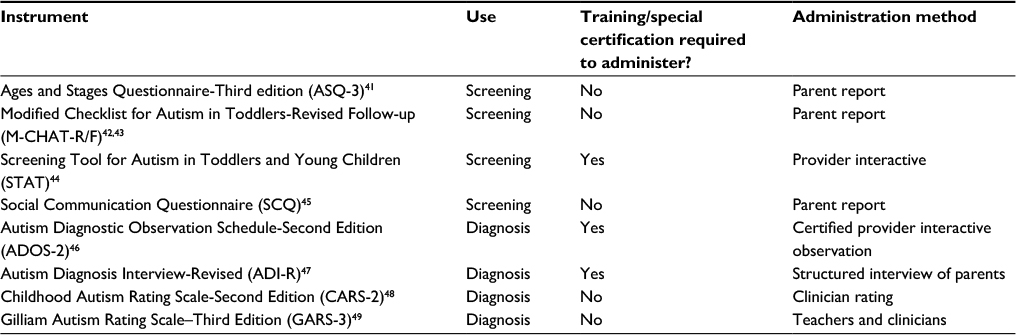 | Table 1 Examples of commonly used ASD screening and diagnostic instruments Abbreviation: ASD, autism spectrum disorder. |
No date restrictions were used. The search was intentionally broad, with a high number of irrelevant results, in order to capture as many unique screening instruments as possible: the initial result set included 970 records; 125 records remained after title/abstract review. As this was an instrument search, the inclusion criterion was simply the presence of a unique instrument used for diagnosis/screening of ASDs. Preference was given to studies that included a complete description or full text of the instrument, such as validation studies. Furthermore, literature reviews related to autism screening were included for full-text review. From these results, the authors created a list of ASD screening and diagnostic instruments, which were then assessed for their relevance and quality. The final list of screening instruments includes high-quality, validated instruments that are commonly used today.
Impact of early diagnosis on ASD prognosis
The importance of receiving an early diagnosis of ASD and subsequent early intervention is well-established in the literature.3,23,24 However, in surveying 1,420 parents of children with ASD, Oswald et al found that, despite early parental concerns, children in the ASD group were diagnosed later than children in the developmentally delayed group.25 Late diagnosis is associated with increased parental stress and delays early intervention, which is critical to positive outcomes over time.26,27 This is particularly important because studies have found that interventions implemented before age 4 (eg, 12–48 months) are associated with significant gains in cognition, language, and adaptive behavior.28,29 Similarly, researchers have linked the implementation of early interventions in ASD with improvements in daily living skills and social behavior.30 Collectively, this evidence suggests that early diagnosis and intervention are imperative in the long-term trajectories and quality of life for children with ASD.
Barriers to early diagnosis
Although some parents report a suspicion of ASD in the first 12 months,31,32 many are told by healthcare providers to “not worry about” common features, such as slow language development or isolative behavior, that can be misinterpreted as shyness.5 However, clinicians are able to recognize the subtler signs of ASD (eg, language deficits, impaired social relatedness, gaze aversion) and know that a reliable diagnosis can be made by age 2.33,34 In fact, ASD can be detected before age 2 using standard screening methods for ASD, such as the Modified Checklist for Autism in Toddlers (MCHAT),35 and later confirmed using gold standard diagnostic methods, such as the Autism Diagnostic Interview – Revised and Autism Diagnostic Observational Schedule-2.17,32 Despite the availability of reliable methods for early diagnosis, the average age at which a child receives a diagnosis of ASD is currently between 4 and 5 years.27 Thus, there is a great need to minimize the time between when children can receive a diagnosis of ASD and when they are actually diagnosed. Indeed, reducing this gap is vital to improving long-term outcomes related to cognition, language, adaptive behavior, daily living skills, and social behavior.
Empirically validated screening and assessment
To facilitate early diagnosis, it is important to raise provider awareness of the current best practice recommendations, which calls for all children to be screened using ASD-sensitive and -specific tools.36 Table 1 includes screening and diagnostic tools that are well-known in the ASD field and have established sensitivity and specificity; conversely, the table excludes tools that are primarily for treatment planning (eg, the Social Responsive Scale,37 Vineland Adaptive Behavior,38 Differential Ability Scale,39 Mullen Scales of Early Learning40).
In summary, early identification of ASD is critical to ensuring that children with ASD are able to access evidence-based interventions that mitigate their levels of disability.4,27,28,50 Furthermore, providers must be aware of, and trained to use, tools that can accurately detect and diagnose ASD. Additional information regarding ASD instruments can be found in other reviews published from 2014 to 2016.36,51–53 It is important for providers to have a strong understanding of ASD in order to appropriately diagnose and link families to appropriate services.54,55
Parental role in ASD interventions and shifts with development
Although interventions for preschool age children are common, researchers in the field of ASD need to develop interventions that target the unique needs of infants and children younger than 24 months of age.56 Currently, interventions for children under 2 years teach parents specific procedures and strategies to use during daily routines to enrich the child’s experiences and interactions.56 Similarly, interventions for infants under 12 months of age focus on parent skills and responsiveness6,57,58 in order to enhance the young child’s first relationships (ie, interactions) with others. Emerging evidence shows that very early interventions may exert a strong positive effect on the developmental trajectories of infants at high-risk of ASD,59 as well as provide benefit for the parents.56 An expert panel convened by the American Academy of Pediatrics recommends that clinicians refer infants or children at risk for ASD as early as possible so that they can benefit from early interventions.60 Children at risk for ASD may have a family history of ASD (eg, sibling with ASD), experience unusual medical events (eg, seizures, gastrointestinal [GI] concerns, sleep problems), and/or exhibit behavioral risk factors that inspire the concern of parents or physicians.61 Recommendation for early intervention to occur even before a definitive diagnosis of ASD is made speaks to the urgency of the need for further development of interventions for infants and children with ASD.
Building social and communication abilities
For children who receive early childhood ASD services, intervention focuses heavily on building and fostering social–relational and communication abilities. An additional cornerstone of childhood ASD interventions includes developmental or habilitative therapies.60,61 These therapies not only aim to minimize any existing delays in communication and social–relational abilities, but also work to enhance developmental skill progression across the broad developmental domains of communication, adaptive functioning (eg, toileting), gross- and fine-motor skills, and cognitive–perceptual abilities (Table 2). After developmental delays are minimized, efforts can be shifted to focus on optimizing developmental trajectories. Therapies begun early can also focus heavily on shaping development of desired daily routines, such as learning how to engage with the family at mealtime. For children with difficult behaviors, undesired behaviors are often easier to physically redirect in younger, smaller children. Thus, current best practice recommendations call for combined developmental and behavioral early intervention approaches for young children with suspected and confirmed ASD.60,61
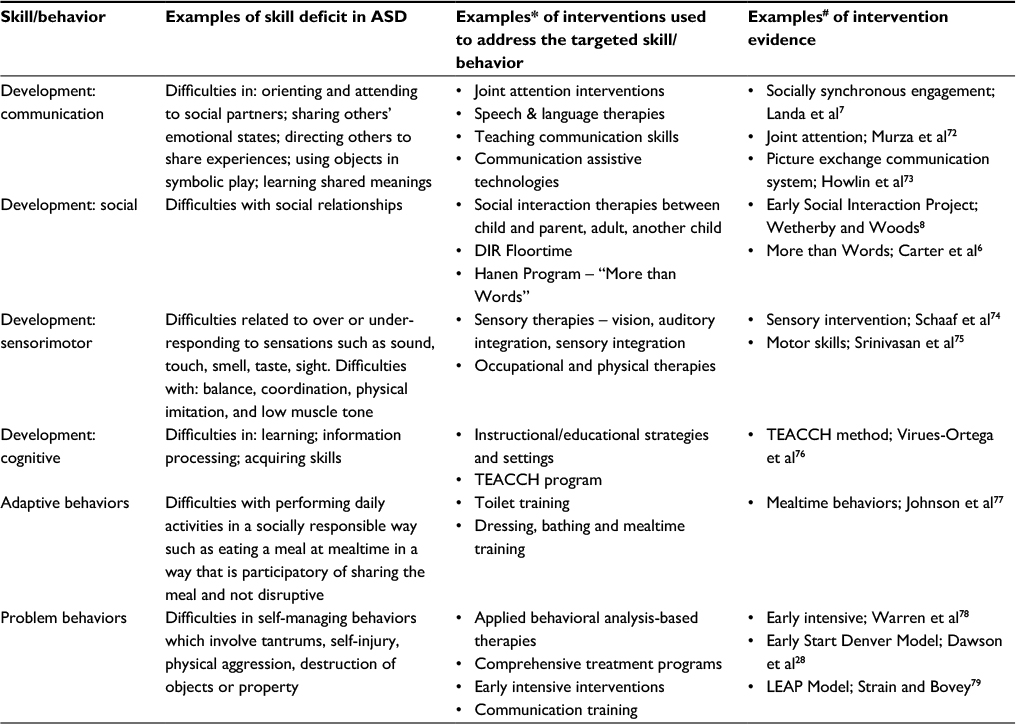 | Table 2 Skills and behaviors targeted in early intervention and childhood ASD therapies Notes: *Interventions included can be used to address the behavior/skill indicated, but may also be used to address the development and/or shaping of other behaviors/skills. #Studies included are examples of existing evidence and are not indicative of the strength of the evidence. Abbreviations: ASD, autism spectrum disorder; LEAP, Learning Experiences and Alternative Program for Preschoolers and their Parents. |
Interventional setting
Whether the intervention offered is comprehensive (ie, addresses multiple developmental areas and/or multiple core ASD features), or has a specific focus (eg, relational, communication, behavioral), one common setting is the naturalistic setting, which is the child’s day-to-day environment such as the home, daycare, or preschool.62 Interventions within naturalistic settings provide the child with ASD multiple contexts and opportunities for learning and practicing targeted skills, behaviors, and routines.62 Naturalistic settings, moreover, enable the interventionist to harness parental skills while optimizing parent–child interactions within the context of the child’s daily routines.62 For example, consider the scenario of a young child who is identified at risk of developing ASD with excessive irritability and hyper-reactivity to sounds or busy environments. For this child, the interventionist could work with the parents to identify overstimulating situations or routines within the child’s natural environments and then teach the parent ways to prevent overstimulation and facilitate the child’s recovery from irritating stimuli. Similarly, clinicians can train parents at home to ameliorate symptoms and promote the child’s communication skills, social development, sensory processing abilities, and/or behavioral control within the child’s everyday life situations.63,64 Indeed, current practice recommendations regarding interventions for children younger than 3 years include active parental, caregiver, and family involvement to achieve optimal functioning of the affected child.60,61
Addressing comorbidities
Regardless of the child’s age, ASD interventions should address related difficulties60 and challenges brought about or exacerbated by existing comorbid conditions, such as emotional dysregulation, GI disturbances,65 attention-deficit hyperactivity disorder,66 learning disability,67 anxiety and depression,68,69 sleep disturbances,65 sensory sensitivities,21 and motor difficulties.70 Moreover, interventions may need to address the child’s challenging behaviors that can be aggravated by the presence of inflexible behaviors and/or thinking. The impacts of co-occurring conditions and behavioral difficulties may increase the stress of both the child and families, especially as the child grows older and is expected to engage with others within the classroom and community (eg, sports leagues, clubs).
Tailoring interventions over the life course
Because ASD is a neurobiological disorder, symptoms persist and change throughout the life span. In order to effectively address these changes, the focus of interventions shifts over time. For example, interventions for young children focus on developmental skill enhancement, whereas interventions for adolescents focus on the attainment of, and engagement in, functional activities such as regularly cleaning their living space and living independently. With progression into young adulthood, the focus of interventions again shifts toward engagement in young adult social roles and attainment of independence, such as participating in post-secondary educational or work settings.71 As a result, roles of parents and families in facilitating and engaging within the interventions also change over time. For example, when the child is very young, parents play a central role in implementing recommended therapeutic strategies. However, as the child matures through adolescence and adulthood, parents shift to facilitating the youths’ and young adults’ strategic use of supportive environments, routines, and services. Clinical providers can better help families anticipate and prepare for these shifts when they adopt a life-course perspective for treatment of ASD.
Effects of ASD on the parent–child relationship and implications of early diagnosis
Sources of stress
Reports indicate that parents and family members without adequate support and direction can experience extreme stress, especially around the tumultuous time of diagnosis.5 Research has shown that families of children with ASD report more stress than families of children with other disabilities,80 perhaps because hallmarks of ASD – unpredictable behavior, disinterest in affection, and aloofness – present unique challenges to parents. Parents may feel ill-equipped to deal with these challenges, and may not know where to turn for support. In addition, treatment costs are high, and many parents may drop out of the workforce to care full-time for their child with ASD, leading to a significant financial burden on families. To date, there have been few evidence-based options for parents and families to alleviate the stress related to having a child with ASD.
Value of the parent–professional relationship
However, there is some evidence that a good parent–professional relationship can help mitigate this stress.81 For example, in a qualitative study of 10 Chinese families, Ho et al82 found that the quality of the parent–professional partnership determined how well families reacted to a diagnosis of ASD. Similar findings about the importance of the parent–professional relationship were noted in an earlier Scottish study,83 where 126 participants responded to a “questionnaire package”, as well as in an exploratory Dutch study of 77 parents who completed a Reaction to Diagnosis Interview.84 Collectively, these findings suggest that, while acquiring and accepting an ASD diagnosis can be difficult for families, a key to successfully navigating through this time is a positive parent–professional relationship.
Navigators and acquiring social support
Another way that parents may relieve stress related to caring for a child with ASD is to find a “navigator” who can assist them from the time of diagnosis until they secure appropriate services for their child. This concept was a dominant theme in the authors’ recently conducted focus groups with families of individuals with ASD.5 Indeed, one mother reported experiencing significant stress because she expended a considerable amount of time and money on treatments that had no positive effect on her child with ASD. She stated that an informed navigator along with centralized, dependable resources would have helped her through this stressful phase and toward the use of evidence-based interventions with her child.
The literature provides evidence that social support is vital to helping families relieve stress associated with caregiving for a child with ASD. Indeed, Ingersoll and Hambrick85 note that acquiring informal social support is especially important at the time of diagnosis. Brobst et al report that both fathers and mothers of children with ASD are affected by stress, especially if the child exhibits severe behaviors (eg, tantrums, aggression), and that this stress can negatively affect the marital relationship.86 To counteract this stress, Twoy et al87 recommend “external family coping strategies”, including community, social, and spiritual support, as well as the informal support and respite care provided by friends and family. In 2007, Mandell and Salzer88 found that two-thirds of a group of 1,005 caregivers of children with ASD had participated in support groups and, in 2013, Clifford and Minnes89 reported similar results in their study of 149 parents of children with ASD. In both of these studies, there was evidence that parents who currently attended support groups had more adaptive coping strategies than non-attenders. Currently, online support groups are gaining popularity, perhaps because they are more practical than in-person meetings for families with demanding schedules.
Addressing differences in stress reactions
Intervening early with children at risk for ASD and tailoring interventions to parents and families are critical ways to protect child and family wellbeing. Intervening professionals may find it helpful to examine how parents react to receiving and accepting an ASD diagnosis. Although there appear to be some patterns in how families react to a diagnosis, there are some individual variations. For example, some parents express relief at finally receiving a conclusive diagnosis after prolonged periods of uncertainty.81 In other cases, parents experience the well-documented grieving process: denial, anger, depression, and acceptance.55,90 Eventually, parents must accept that, although their child appears similar to other children in many respects, he/she has limitations that may require revised expectations and future plans. For example, a parent may have envisioned his/her child as a famous orator but realizes that goals may need to be adapted due to the ASD features. Parents may also express anger and ask, “Why us? Why our child?”, and this anger may be intensified if professionals have been inattentive to their concerns. Although parental anger may be challenging for service providers to handle, these professionals should recognize that anger is part of the grieving process and try to empathize with parents to ensure healthy coping and adaptation.26
Clinicians should note, however, that once parents have accepted a diagnosis, it is common for them to set out frantically in search of “a cure”.5 During this phase, parents and families are particularly vulnerable and can fall prey to false claims of “cures” from a variety of sources, many of which are on the Internet. Service providers must recognize this potential danger, and direct families to credible information sources while correcting inaccurate information and “myths” of a cure.26,80
Helping families adapt
Familial perceptions of the ASD diagnosis play an important role in how they ultimately adapt as a family unit. For example, Cappe et al91 found that perceiving experiences as a loss or threat significantly predicts poor adaptation, whereas Ekas et al54 assert that optimism and the maintenance of hope improve adaptation. While some families are naturally more optimistic than others, such an outlook can be cultivated by supportive professionals.
Studies have also shown that successful families are creative, flexible, and willing to try new things.92 For example, in the first author’s experience, one family developed a creative means of promoting appropriate eye contact by rewarding the young girl when she could recall the color of visitors’ eyes after they had been in the home. Research also shows that knowledgeable professionals can improve adaptation to diagnosis, which can lead to stronger family units and feelings of hope for the future.26
Limitations
The field of ASD research is rapidly changing with the addition of many new diagnostic and screening instruments and interventions. This review describes commonly used instruments that are, to date, frequently cited in the literature. We sought to illustrate a broad range of ASD symptoms and experiences that are reflective of the heterogeneity in both ASD symptomatology and co-occurring conditions. We highlighted a limited range of skills and behaviors that are targeted in ASD early intervention and, thus, narrowed our focus on a sample of behavioral, educational/developmental, and psychosocial ASD approaches. However, it is important to note that ASD interventions can also include pharmacological, medical, dietary, and technological options, which were not included in this review. Furthermore, it is noteworthy that, within the range of ASD interventions and approaches in our review, several can be used to address multiple symptoms and/or targeted behaviors and skills. For example, behavioral interventions are not restricted to the treatment of problem behaviors; they can also be used to target communication and/or adaptive functioning. There are other instruments and interventions being developed with much potential for improving outcomes for individuals with ASD and their families.
Conclusion
This article highlights the importance of early diagnosis and intervention as well as family support for individuals with ASD. While major advances have been made in the field, it is clear that more provider education is needed, together with timely, empathetic, and ongoing support to families of children with ASD. As previously mentioned, ASD is a lifelong condition and families must learn to shift their focus on therapies as their child grows into adulthood. Effective communication between providers and families is the key to building supportive relationships that can positively affect not only the individual with ASD but also the family over a lifetime.
Acknowledgments
The authors thank Debra McDonald, MA, UF College of Nursing, for her editorial assistance. This work was supported in part by the National Institutes of Health – National Center for Medical and Rehabilitation Research (NICHD) and National Institute for Neurological Disorders & Stroke (grant no. K12 HD055929). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217–250. | ||
Centers for Disease Control and Prevention. Autism spectrum disorder (ASD) data & statistics. 2016. Available from: https://www.cdc.gov/ncbddd/autism/data.html. Accessed April 11, 2017. | ||
Volkmar FR. Editorial: the importance of early intervention. J Autism Dev Disord. 2014;44(12):2979–2980. | ||
Lovaas OI. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol. 1987;55(1):3–9. | ||
Elder JH, Brasher S, Alexander B. Identifying the barriers to early diagnosis and treatment in underserved individuals with autism spectrum disorders (ASD) and their families: a qualitative study. Issues Ment Health Nurs. 2016;37(6):412–420. | ||
Carter AS, Messinger DS, Stone WL, Celimli S, Nahmias AS, Yoder P. A randomized controlled trial of Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. J Child Psychol Psychiatry. 2011;52(7):741–752. | ||
Landa RJ, Holman KC, O’Neill AH, Stuart EA. Intervention targeting development of socially synchronous engagement in toddlers with autism spectrum disorder: a randomized controlled trial. J Child Psychol Psychiatry. 2011;52(1):13–21. | ||
Wetherby AM, Woods JJ. Early social interaction project for children with autism spectrum disorders beginning in the second year of life. Topics Early Child Spec Educ. 2006;26(2):67–82. | ||
American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013. | ||
Lyall K, Croen L, Daniels J, et al. The changing epidemiology of autism spectrum disorders. Annu Rev Public Health. 2017;38:81–102. | ||
Kapp SK, Gillespie-Lynch K, Sherman LE, Hutman T. Deficit, difference, or both? Autism and neurodiversity. Dev Psychol. 2013;49(1):59–71. | ||
Constantino JN. The quantitative nature of autistic social impairment. Pediatr Res. 2011;69(5 Pt 2):55R–62R. | ||
Ronald A, Larsson H, Anckarsäter H, Lichtenstein P. Symptoms of autism and ADHD: a Swedish twin study examining their overlap. J Abnorm Psychol. 2014;123(2):440–451. | ||
Kamio Y, Inada N, Moriwaki A, et al. Quantitative autistic traits ascertained in a national survey of 22 529 Japanese schoolchildren. Acta Psychiatr Scand. 2013;128(1):45–53. | ||
Geschwind DH. Advances in autism. Annual review of medicine. 2009;60:367–80. | ||
Constantino JN, Charman T. Diagnosis of autism spectrum disorder: reconciling the syndrome, its diverse origins, and variation in expression. Lancet Neurol. 2016;15(3):279–291. | ||
Centers for Disease Control and Prevention. Autism spectrum disorder (ASD) screening and diagnosis for healthcare providers. 2016. Available from: https://www.cdc.gov/ncbddd/autism/hcp-screening.html. Accessed April 11, 2017. | ||
Matson JL, Shoemaker M. Intellectual disability and its relationship to autism spectrum disorders. Res Dev Disabil. 2009;30(6):1107–1114. | ||
Solomon M, Miller M, Taylor SL, Hinshaw SP, Carter CS. Autism symptoms and internalizing psychopathology in girls and boys with autism spectrum disorders. J Autism Dev Disord. 2012;42(1):48–59. | ||
Hofvander B, Delorme R, Chaste P, et al. Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry. 2009;9:35. | ||
Burke L, Stoddart KP. Medical and health problems in adults with high-functioning autism and asperger syndrome. In: Volkmar FR, Reichow B, McPartland JC, editors. Adolescents and Adults with Autism Spectrum Disorders. New York, NY: Springer New York; 2014:239–267. | ||
Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009;26(2):91–108. | ||
Rotholz DA, Kinsman AM, Lacy KK, Charles J. Improving early identification and intervention for children at risk for autism spectrum disorder. Pediatrics. 2017;139(2). pii e20161061. | ||
Swanson AR, Warren ZE, Stone WL, Vehorn AC, Dohrmann E, Humberd Q. The diagnosis of autism in community pediatric settings: does advanced training facilitate practice change? Autism. 2014;18(5):555–561. | ||
Oswald DP, Haworth SM, Mackenzie BK, Willis JH. Parental report of the diagnostic process and outcome: ASD compared with other developmental disabilities. Focus Autism Other Dev Disabil. 2017;32(2):152–160. | ||
Elder JH. Assisting parents in adapting and making decisions regarding the most efficacious treatment options. In: Giarelli E, Fisher KM, editors. Integrated Health Care for People with Autism Spectrum Disorders: Interdisciplinary Planning and Delivery of Care. Springfield, IL: Charles C. Thomas, Publishers Ltd.; 2016:173–192. | ||
Zwaigenbaum L, Bauman ML, Stone WL, et al. Early identification of autism spectrum disorder: recommendations for practice and research. Pediatrics. 2015;136(Suppl 1):S10–S40. | ||
Dawson G, Rogers S, Munson J, et al. Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model. Pediatrics. 2010;125(1):e17–e23. | ||
Vivanti G, Dissanayake C; Victorian ASELCC Team. Outcome for children receiving the Early Start Denver Model before and after 48 months. J Autism Dev Disord. 2016;46(7):2441–2449. | ||
Remington B, Hastings RP, Kovshoff H, et al. Early intensive behavioral intervention: outcomes for children with autism and their parents after two years. Am J Ment Retard. 2007;112(6):418–438. | ||
De Giacomo A, Fombonne E. Parental recognition of developmental abnormalities in autism. Eur Child Adolesc Psychiatry. 1998;7(3):131–136. | ||
Lord C, Risi S, DiLavore PS, Shulman C, Thurm A, Pickles A. Autism from 2 to 9 years of age. Arch Gen Psychiatry. 2006;63(6):694–701. | ||
Moriuchi JM, Klin A, Jones W. Mechanisms of diminished attention to eyes in autism. Am J Psychiatry. 2017;174(1):26–35. | ||
Chawarska K, Paul R, Klin A, Hannigen S, Dichtel LE, Volkmar F. Parental recognition of developmental problems in toddlers with autism spectrum disorders. J Autism Dev Disord. 2007;37(1):62–72. | ||
Baron-Cohen S, Allen J, Gillberg C. Can autism be detected at 18 months? The needle, the haystack, and the CHAT. Br J Psychiatry. 1992;161:839–843. | ||
Zwaigenbaum L, Bauman ML, Fein D, et al. Early Screening of autism spectrum disorder: recommendations for practice and research. Pediatrics. 2015;136(Suppl 1):S41–S59. | ||
Constantino JN, Gruber CP. Social Responsiveness Scale-Second Edition (SRS-2) Manual. Torrance, CA: Western Psychological Services; 2012. | ||
Sparrow SS, Balla DA, Cicchetti DV. Vineland Adaptive Behavior Scales. Circle Pines, MN: American Guidance Service, Inc.; 1984. | ||
Elliott CD. Differential Ability Scales. New York, NY: The Psychological Corporation; 1990. | ||
Mullen EM. Mullen Scales of Early Learning (AGS ed). Circle Pines, MN: American Guidance Service Inc.; 1985. | ||
Squires J, Bricker D, Potter L. Ages and Stages Questionnaires (ASQ-3). 3rd ed. Baltimore, MD: Paul H. Brookes Publishing; 2009. | ||
Robins DL, Fein D, Barton ML, Green JA. The Modified Checklist for Autism in Toddlers: an initial study investigating the early detection of autism and pervasive developmental disorders. J Autism Dev Disord. 2001;31(2):131–144. | ||
Robins DL, Casagrande K, Barton M, Chen CM, Dumont-Mathieu T, Fein D. Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics. 2014;133(1):37–45. | ||
Stone WL, Coonrod EE, Ousley OY. Brief report: screening tool for autism in two-year-olds (STAT): development and preliminary data. J Autism Dev Disord. 2000;30(6):607–612. | ||
Rutter M, Bailey A, Lord C, Berument SK. Social Communication Questionnaire. Los Angeles, CA: Western Psychological Association; 2003. | ||
Lord C, Rutter M, DiLavore PC, Risi S, Gotham K, Bishop S. Autism Diagnostic Schedule. 2nd ed. Torrance, CA: Western Psychological Services; 2010. | ||
Rutter M, Le Couteur A, Lord C. Autism Diagnostic Interview–Revised (ADI–R) Manual. Los Angeles, CA: Western Psychological Services; 2003. | ||
Schopler E, Van Bourgondien ME, Wellman GJ, Love SR. Childhood Autism Rating Scale. 2nd ed. Los Angeles, CA: Western Psychological Services; 2010. | ||
Gilliam JE. Gilliam Autism Rating Scale. 3rd ed. Austin, TX: Pro-Ed; 2014. | ||
Rogers SJ, Vismara L, Wagner AL, McCormick C, Young G, Ozonoff S. Autism treatment in the first year of life: a pilot study of infant start, a parent-implemented intervention for symptomatic infants. J Autism Dev Disord. 2014;44(12):2981–2995. | ||
Lai MC, Lombardo MV, Baron-Cohen S. Autism. Lancet. 2014;383(9920):896–910. | ||
Soleimani F, Khakshour A, Abbasi Z, Khayat S, Ghaemi SZ, Hajikhani Golchin NA. Review of autism screening tests. Int J Pediatr. 2014;2(4.1):319–329. | ||
McPheeters ML, Weitlauf A, Vehorn A, et al. Screening for Autism Spectrum Disorder in Young Children: A Systematic Evidence Review for the U.S. Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality (US); 2016. | ||
Ekas NV, Lickenbrock DM, Whitman TL. Optimism, social support, and well-being in mothers of children with autism spectrum disorder. J Autism Dev Disord. 2010;40(10):1274–1284. | ||
Elder JH, D’Alessandro T. Supporting families of children with autism spectrum disorders: questions parents ask and what nurses need to know. Pediatr Nurs. 2009;35(4):240–245, 253. | ||
Bradshaw J, Steiner AM, Gengoux G, Koegel LK. Feasibility and effectiveness of very early intervention for infants at-risk for autism spectrum disorder: a systematic review. J Autism Dev Disord. 2015;45(3):778–794. | ||
McConkey R, Truesdale-Kennedy M, Crawford H, McGreevy E, Reavey M, Cassidy A. Preschoolers with autism spectrum disorders: evaluating the impact of a home-based intervention to promote their communication. Early Child Dev Care. 2010;180(3):299–315. | ||
Wong VC, Kwan QK. Randomized controlled trial for early intervention for autism: a pilot study of the Autism 1-2-3 Project. J Autism Dev Disord. 2010;40(6):677–688. | ||
Webb SJ, Jones EJ, Kelly J, Dawson G. The motivation for very early intervention for infants at high risk for autism spectrum disorders. Int J Speech Lang Pathol. 2014;16(1):36–42. | ||
Zwaigenbaum L, Bauman ML, Choueiri R, et al. Early intervention for children with autism spectrum disorder under 3 years of age: recommendations for practice and research. Pediatrics. 2015;136(Suppl 1):S60–S81. | ||
Myers SM, Johnson CP. Management of children with autism spectrum disorders. Pediatrics. 2007;120(5):1162–1182. | ||
Schreibman L, Dawson G, Stahmer AC, et al. Naturalistic developmental behavioral interventions: empirically validated treatments for autism spectrum disorder. J Autism Dev Disord. 2015;45(8):2411–2428. | ||
Oono IP, Honey EJ, McConachie H. Parent-mediated early intervention for young children with autism spectrum disorders (ASD). Evid Based Child Health. 2013;8(6):2380–2479. | ||
Roberts J, Williams K, Carter M, et al. A randomised controlled trial of two early intervention programs for young children with autism: centre-based with parent program and home-based. Res Autism Spectr Disord. 2011;5(4):1553–1566. | ||
Mannion A, Leader G. Comorbidity in autism spectrum disorder: a literature review. Res Autism Spectr Disord. 2013;7(12):1595–1616. | ||
Antshel KM, Hier BO. Attention deficit hyperactivity disorder (ADHD) in children with autism spectrum disorders. In: Patel BV, Preedy RV, Martin RC, editors. Comprehensive Guide to Autism. New York, NY: Springer New York; 2014:1013–1029. | ||
Boulet SL, Boyle CA, Schieve LA. Health care use and health and functional impact of developmental disabilities among us children, 1997–2005. Arch Pediatr Adolesc Med. 2009;163(1):19–26. | ||
Doyle CA, McDougle CJ, Stigler KA. Pharmacotherapy of behavioral symptoms and psychiatric comorbidities in adolescents and adults with autism spectrum disorders. In: Volkmar FR, Reichow B, McPartland JC, editors. Adolescents and Adults with Autism Spectrum Disorders. New York, NY: Springer New York; 2014:161–191. | ||
Sofronoff K, Attwood T, Hinton S. A randomised controlled trial of a CBT intervention for anxiety in children with Asperger syndrome. J Child Psychol Psychiatry. 2005;46(11):1152–1160. | ||
Bhat AN, Landa RJ, Galloway JC. Current perspectives on motor functioning in infants, children, and adults with autism spectrum isorders. Phys Ther. 2011;91(7):1116–1129. | ||
Taylor JL, Dove D, Veenstra-VanderWeele J, et al. Interventions for Adolescents and Young Adults With Autism Spectrum Disorders. Rockville, MD: Agency for Healthcare Research and Quality; 2012. Report No.: 12-EHC063-EF. | ||
Murza KA, Schwartz JB, Hahs-Vaughn DL, Nye C. Joint attention interventions for children with autism spectrum disorder: a systematic review and meta-analysis. Int J Lang Commun Disord. 2016;51(3):236–251. | ||
Howlin P, Gordon RK, Pasco G, Wade A, Charman T. The effectiveness of Picture Exchange Communication System (PECS) training for teachers of children with autism: a pragmatic, group randomised controlled trial. J Child Psychol Psychiatry. 2007;48(5):473–481. | ||
Schaaf RC, Benevides T, Mailloux Z, et al. An intervention for sensory difficulties in children with autism: a randomized trial. J Autism Dev Disord. 2014;44(7):1493–1506. | ||
Srinivasan SM, Kaur M, Park IK, Gifford TD, Marsh KL, Bhat AN. The effects of rhythm and robotic interventions on the imitation/praxis, interpersonal synchrony, and motor performance of children with autism spectrum disorder (ASD): a pilot randomized controlled trial. Autism Res Treat. 2015;2015:736516. | ||
Virues-Ortega J, Julio FM, Pastor-Barriuso R. The TEACCH program for children and adults with autism: a meta-analysis of intervention studies. Clin Psychol Rev. 2013;33(8):940–953. | ||
Johnson CR, Foldes E, DeMand A, Brooks MM. Behavioral parent training to address feeding problems in children with autism spectrum disorder: a pilot trial. J Dev Phys Disabil. 2015;27(5):591–607. | ||
Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glasser A, Veenstra-Vanderweele J. A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics. 2011;127(5):e1303–e1311. | ||
Strain PS, Bovey EH. Randomized, controlled trial of the LEAP model of early intervention for young children with autism spectrum disorders. Topics Early Child Spec Educ. 2011;31(3):133–154. | ||
Hayes SA, Watson SL. The impact of parenting stress: a meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J Autism Dev Disord. 2013;43(3):629–642. | ||
Abbott M, Bernard P, Forge J. Communicating a diagnosis of Autism Spectrum Disorder – a qualitative study of parents’ experiences. Clin Child Psychol Psychiatry. 2013;18(3):370–382. | ||
Ho HS, Yi H, Griffiths S, Chan DF, Murray S. ‘Do It Yourself’ in the parent–professional partnership for the assessment and diagnosis of children with autism spectrum conditions in Hong Kong: a qualitative study. Autism. 2014;18(7):832–844. | ||
Brogan CA, Knussen C. The disclosure of a diagnosis of an autistic spectrum disorder: determinants of satisfaction in a sample of Scottish parents. Autism. 2003;7(1):31–46. | ||
Poslawsky IE, Naber FB, Van Daalen E, Van Engeland H. Parental reaction to early diagnosis of their children’s autism spectrum disorder: an exploratory study. Child Psychiatry Hum Dev. 2014;45(3):294–305. | ||
Ingersoll B, Hambrick DZ. The relationship between the broader autism phenotype, child severity, and stress and depression in parents of children with autism spectrum disorders. Res Autism Spectr Disord. 2011;5(1):337–344. | ||
Brobst JB, Clopton JR, Hendrick SS. Parenting children with autism spectrum disorders. Focus Autism Other Dev Disabil. 2009;24(1):38–49. | ||
Twoy R, Connolly PM, Novak JM. Coping strategies used by parents of children with autism. J Am Acad Nurse Pract. 2007;19(5):251–260. | ||
Mandell DS, Salzer MS. Who joins support groups among parents of children with autism? Autism. 2007;11(2):111–122. | ||
Clifford T, Minnes P. Who participates in support groups for parents of children with autism spectrum disorders? The role of beliefs and coping style. J Autism Dev Disord. 2013;43(1):179–187. | ||
Ross EKR, Kessler D. Finding the Meaning of Grief Through the Five Stages of Loss. New York: Scribner; 2007. | ||
Cappe E, Wolff M, Bobet R, Adrien JL. Quality of life: a key variable to consider in the evaluation of adjustment in parents of children with autism spectrum disorders and in the development of relevant support and assistance programmes. Qual Life Res. 2011;20(8):1279–1294. | ||
Greeff AP, van der Walt KJ. Resilience in families with an autistic child. Educ Train Autism Dev Disabil. 2010;45(3):347–355. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.