")
Back to Journals » Journal of Inflammation Research » Volume 16
Clinical Features of Crohn’s Disease Stratified by Age at Diagnosis According to Montreal Classification
Authors Xiang J, Li J, Liu C, Tian S, Dong W
Received 14 November 2022
Accepted for publication 11 February 2023
Published 21 February 2023 Volume 2023:16 Pages 737—746
DOI https://doi.org/10.2147/JIR.S397483
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Jiankang Xiang,1 Jiao Li,1 Chuan Liu,1 Shan Tian,2 Weiguo Dong1
1Department of Gastroenterology, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 2Department of Infectious Diseases, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
Correspondence: Weiguo Dong, Email [email protected]
Aim: The differences of clinical characteristics stratified by age at diagnosis especially according to Montreal classification were rarely studied in China. This study aimed to evaluate and compare the clinical features in various groups of CD patients stratified by age at diagnosis.
Methods: A cross-sectional study of CD patients was conducted through a stratified sampling according to Montreal classification. Patients were divided into three groups by age at diagnosis: group A1 (< 17 years old), group A2 (17 to 40 years old), and group A3 (> 40 years old). The clinical characteristics, laboratory tests, radiographic, and endoscopic features were analyzed by statistics.
Results: We enrolled 259 CD patients for the study. There was male predominance under 40 years old. Compared to group A1, more female patients were presented in group A3. There were more patients had perianal fistulas in group A1 compared to group A2 and group A3. Compared with group A1, patients in group A2 were associated with lower total protein (TP) levels. The mean TP and platelet count (PC) levels in group A3 were lower than group A1. Patients in group A1 had a lower rate of stricturing (B2) disease behavior than group A2 and group A3, and patients in group A3 who had a B2 disease behavior were higher than group A2. Those differences could guide early treatment or inventions for CD patients who might progress to a more complex disease behavior.
Conclusion: CD patients stratified by age at diagnosis according to Montreal classification had different clinical symptoms, laboratory test results as well as disease locations and behaviors.
Keywords: Crohn’s disease, age at diagnosis, Montreal classification, clinical characteristics
Introduction
Crohn’s disease (CD) is a main type of inflammatory bowel disease (IBD), which can affect any part of the digestive tract, and its major symptoms include abdominal pain, weight loss, chronic diarrhea, and it may have a relapsing and remitting manner.1 The incidence of CD had increased over time.2 From large national databases, a study in the United States3 showed that the overall prevalence of pediatric IBD had increased from 33.0/100,000 in 2007 to 77.0/100,000 in 2016, while from 214.9/100,000 in 2007 to 478.4/100,000 in 2016 for adult IBD patients, and the prevalence of CD in children was 45.9/100,000 and 197.7/100,000 in the adult population in 2016. The incidence and prevalence of CD had increased in China as well.4 The incidence of CD in China was 0.07/100,000 to 3.86/100,000 in 20145. A study had indicated that age at diagnosis could affect the outcome of elderly-onset CD patients.6 It had been found that early-onset CD was different from late-onset CD in clinical outcomes and nutritional status.7 In addition, the lifetime costs of CD patients were associated with their age at diagnosis. A previous study in the United States suggested that lifetime economic burden was particularly high for CD patients diagnosed under 11 years old.8 According to Montreal classification,9 CD patients could be divided into 3 groups by age at diagnosis (age at diagnosis below 16 years old was defined as A1, between 17 and 40 years old was defined as A2, and age at diagnosis above 40 years old was defined as A3). The Montreal classification played an important role in categorizing CD patients. However, there were few studies10,11 that had analyzed the clinical characteristics and laboratory tests according to various ages, hence it is important to clarify what discrepancies exist in different ages. What’s more, it remained unclear what differences existed among Chinese CD patients when they were divided into various groups by age at diagnosis according to Montreal classification. In this study, we aimed to investigate the differences of clinical features and laboratory test results among CD patients stratified by age at diagnosis based on Montreal classification, which could help to provide reference for clinical practice.
Here we collected the different clinical, laboratory and endoscopic features of diverse groups, which were divided by age at diagnosis. From our study, we explored whether there were some differences among diverse age groups for CD patients, such as clinical symptoms, laboratory test results, and disease locations as well as disease behaviors.
Materials and Methods
Study Population
The study was conducted on CD patients in Wuhan, China. We retrospectively collected the CD patients’ clinical manifestations, laboratory examinations, endoscopic, and radiographic features who were hospitalized in Renmin Hospital of Wuhan University (Wuhan, China) from 2018 to 2022. The diagnosis of CD was based on the combination with a medical history, physical examination, laboratory tests, endoscopic, imaging examinations, and histological results according to the Chinese12 and European consensus.13 The inclusion criteria were as following: firstly, patients were diagnosed with CD definitely; secondly, the clinical data or other information such as laboratory test results were relatively complete; thirdly, patients’ informed consent was obtained. The exclusion criteria were as following: patients were diagnosed with ulcerative colitis or IBD-unclassified; the clinical data or information were not complete; patients with others severe diseases such as tumors. All the CD patients were stratified by age at diagnosis according to Montreal classification. Patients under 17 years old were classified into group A1, patients between 17 and 40 years old were defined as group A2, and patients >40 years old were defined as group A3 according to the Montreal classification. Totally, 259 CD patients (22 patients in group A1, 176 patients in group A2, and 60 patients in group A3) were included. We mainly collected the clinical features (such as age, gender, gastrointestinal and other extraintestinal symptoms), laboratory tests (such as complete blood counts, biochemistry tests, and coagulation function results), radiographic, and endoscopic features from the electronic patient record system. The clinical features and laboratory test results among the three age groups were compared using statistical analysis. We assessed disease locations and behaviors among the three groups as well. Then, those clinical features and laboratory tests whose P-value <0.05 were used to perform multivariate logistic regression analysis. This study was approved by the ethics committee of Renmin Hospital of Wuhan University (Wuhan, China) (WDRY2022-K130). Patient informed consent had been obtained.
Statistical Analysis
Categorical variables were shown by numbers (n) and percentages (%), while continuous variables which were normally distributed were demonstrated by mean ± standard deviation (M±SD), and others were displayed by medians and interquartile ranges (IQRs). In this study, statistical analysis was performed using the software SPSS 25.0 (IBM, USA). Chi-square test and one-way ANOVA were used for statistical analysis. A P-value <0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of CD Patients
There were 21 males (95.45%) in the group A1, 132 males (75.00%) in the group A2, 29 males (48.33%) in the group A3, and the differences were statistically significant between group A1 and group A2 (95.45% vs 75.00%, P=0.031), group A1 and group A3 (95.45% vs 48.33%, P<0.001) as well as group A2 and group A3 (75.00% vs 48.33%, P<0.001). Three patients (13.64%) in group A1, 21 patients (11.93%) in group A2, one patient (1.67%) in group A3 presented with perianal abscess, and the difference was statistically significant between group A2 and group A3 (13.64% vs 1.67%, P=0.009). As for fistula formation, 9 patients in group A1 (one intestinal fistula and 8 perianal fistulas), 29 patients in group A2 (2 enterocutaneous fistulas, 2 rectovaginal fistulas, one intestinal fistula, and 24 perianal fistulas), and 7 patients in group A3 (one enterocutaneous fistula, one intestinal fistula, and 5 perianal fistulas) who had fistula formation, and the differences were statistically significant between group A1 and group A2 (40.91% vs 16.48%, P=0.014) as well as group A1 and group A3 (40.91% vs 11.67%, P=0.008). Fourteen patients in group A1, 56 patients in group A2, and 16 patients in group A3 presented with weight loss or growth retardation, and the differences were statistically significant between group A1 and group A2 (63.64% vs 31.82%, P=0.003) as well as group A1 and group A3 (63.64% vs 26.67%, P=0.002). There were none patients in group A1, but 30 patients in group A2, and 4 patients in group A3 had Clostridium difficile infection (CDI), and the difference was statistically significant between group A2 and group A3 (17.05% vs 6.67%, P=0.048). While other clinical features were not statistically significant among the three groups (all P>0.05) (Table 1).
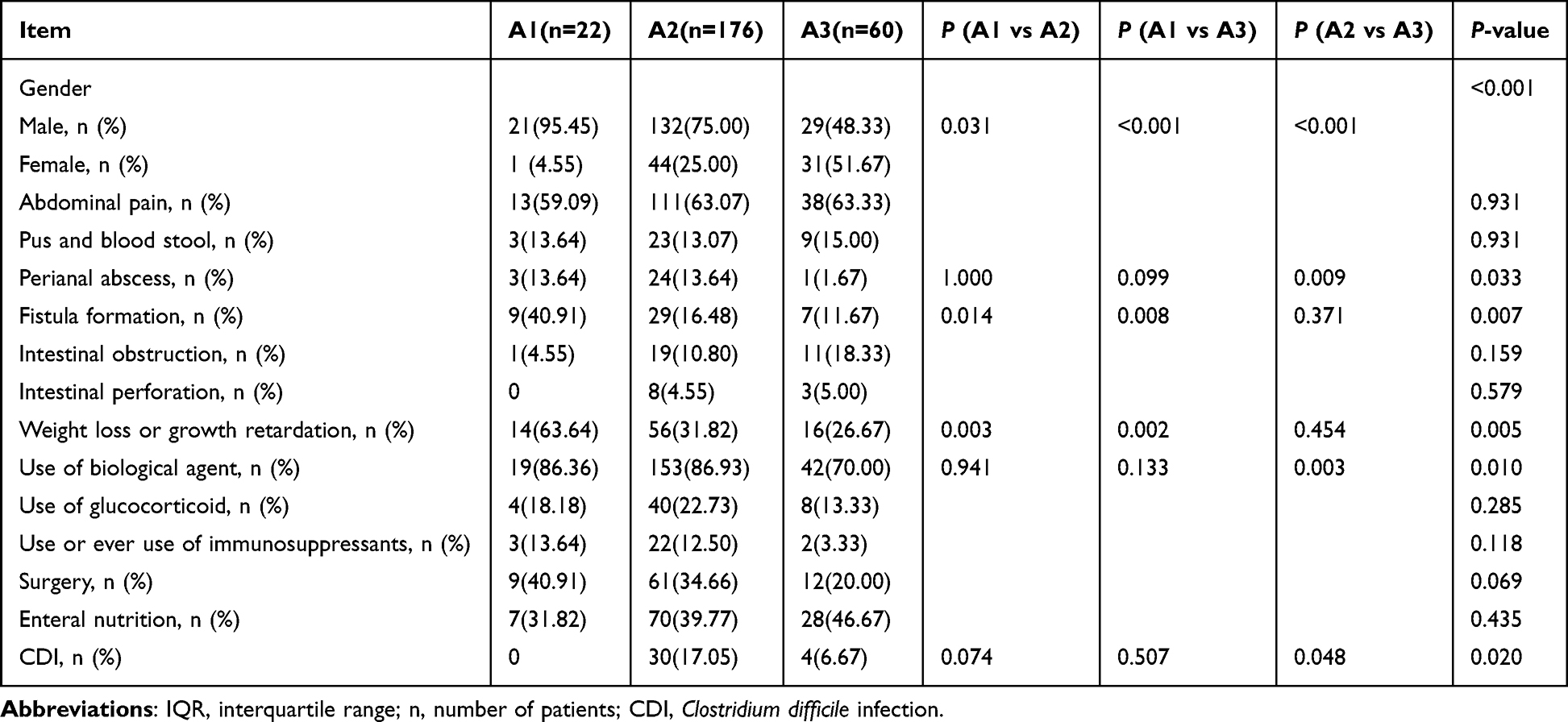 |
Table 1 Clinical Characteristics Comparison Among A1, A2, A3 Groups |
Complete Blood Counts Comparisons Among Different Age Groups
The mean neutrophil counts were higher in group A2 than group A3 [4.02(2.94–5.73) (109/L) vs 2.95(2.21–4.38) (109/L), P=0.001] (Supplementary Table 1). The mean lymphocyte counts were higher in group A1 than group A3 [1.68(1.35–2.21) (109/L) vs 1.27(0.91–1.57) (109/L), P=0.011]. The mean corpuscular volume (MCV) was lower in group A1 than group A2 and group A3 [76.55(67.90–86.75) (fL) vs 84.10(79.55–88.13) (fL), P=0.011; 76.55(67.90–86.75) (fL) vs 86.20(83.80–89.83) (fL), P=0.001, respectively] (Figure 1). The mean corpuscular hemoglobin (MCH) was lower in group A1 than group A2 and group A3 [24.15(21.03–28.85) (pg) vs 27.70(25.00–29.63) (pg), P=0.013; 24.15(21.03–28.85) (pg) vs 28.00(26.70–29.78) (pg), P=0.003, respectively]. The platelet counts (PC) were higher in group A1 and group A2 than group A3 [371.59±117.92 (109/L) vs 244.50(215.25–287.75) (109/L), P=0.002; 308.00(244.00–385.00) (109/L) vs 244.50(215.25–287.75) (109/L), P<0.001, respectively].
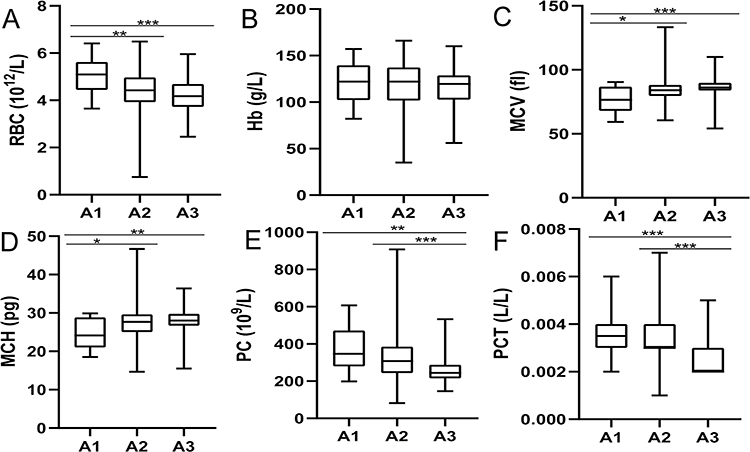 |
Figure 1 (A–D) Boxplot of RBC (A), Hb (B), MCV (C), MCH (D), PC (E) and PCT (F) among A1, A2 and A3 groups. Abbreviations: RBC, red blood cell; Hb, hemoglobin; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; PC, platelet count. |
Biochemistry Laboratory Tests Comparisons Among Different Age Groups
The mean total protein (TP) was higher in group A1 than group A2 and group A3 [75.85(69.68–79.43) (g/L) vs 66.10(60.80–71.60) (g/L), P<0.001; 75.85(69.68–79.43) (g/L) vs 63.95±7.93 (g/L), P<0.001, respectively] (Supplementary Table 2). The mean globulin (G) was higher in group A1 than group A2 and group A3 [30.18(28.68–32.71) (g/L) vs 25.76(22.95–28.90) (g/L), P=0.008; 30.18(28.68–32.71) (g/L) vs 24.95(21.93–27.29) (g/L), P=0.001, respectively]. The mean calcium (Ca) was higher in group A1 than group A2 and group A3 [2.29±0.12 (mmol/L) vs 2.21(2.10–2.31) (mmol/L), P=0.007; 2.29±0.12 (mmol/L) vs 2.17±0.17 (mmol/L), P=0.001, respectively]. The mean levels of high-sensitivity C-reactive protein (hs-CRP) and erythrocyte sedimentation rate (ESR) were not statistically significant among the three groups (both P>0.05) (Figure 2).
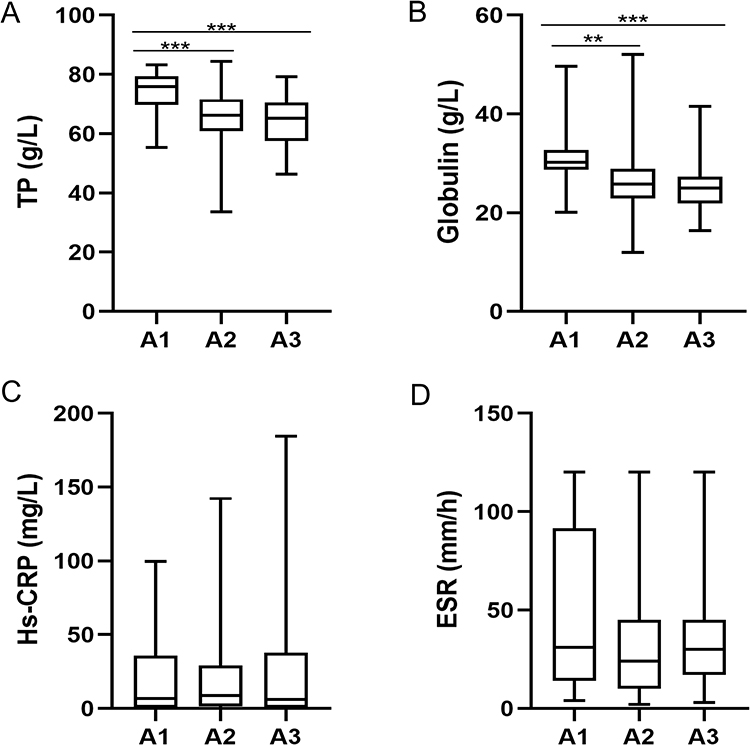 |
Figure 2 (A–D) Boxplot of TP (A), Globulin (B), Hs-CRP (C), ESR (D) among A1, A2 and A3 groups. Abbreviations: TP, total protein; Hs-CRP, High-sensitivity C-reactive protein; ESR, erythrocyte sedimentation rate. |
Coagulation Function Tests Comparisons Among Different Age Groups
From the coagulation function results, we showed that the mean prothrombin time (PT) international normalized ratio (INR) was higher in group A2 than group A3 [1.00(0.93–1.05) vs 0.94(0.91–1.01), P=0.015]. The differences for mean activated partial thromboplastin time (APTT), thrombin time (TT), fibrinogen (Fg), D-dimer, fibrinogen degradation products (FDPs), and antithrombin III activity among the three groups were not statistically significant (all P>0.05) (Table 2).
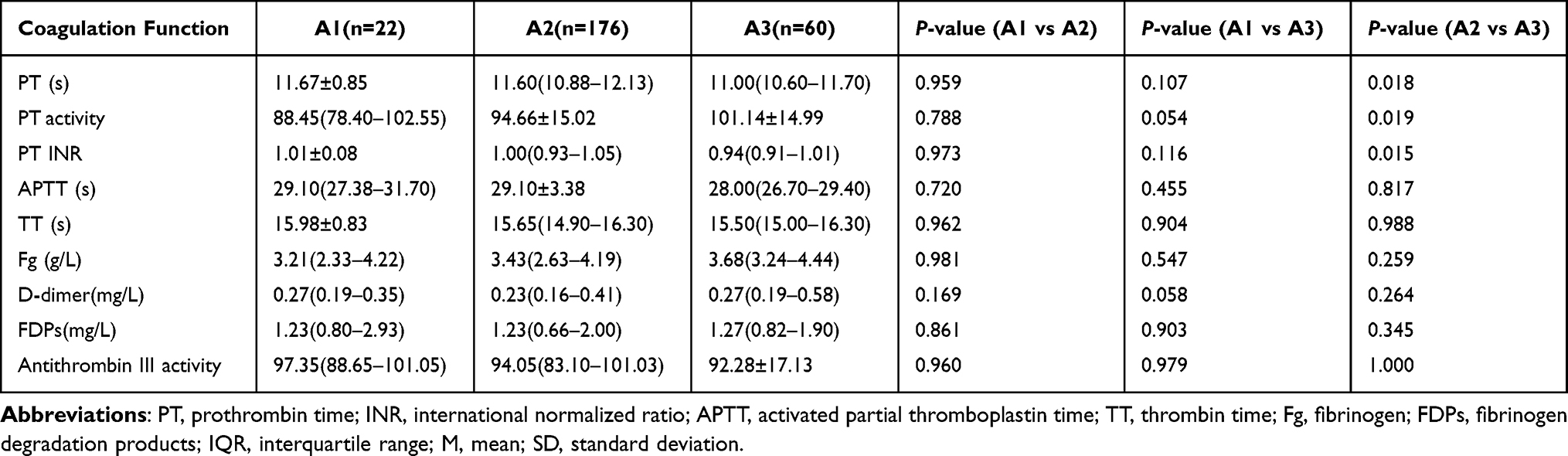 |
Table 2 Coagulation Function Results Comparison Among A1, A2, A3 Groups (M±SD or IQR) |
Comparisons of Disease Locations and Behaviors Among Different Age Groups
There were fewer patients in group A1 than group A2 whose disease locations were at terminal ileal ± limited cecal disease (L1) (13.64% vs 41.48%, P=0.011). Patients in group A2 whose disease locations were involved in colonic (L2) were less than group A3 (8.52% vs 18.33%, P=0.036). More patients in group A2 presented with non-stricturing and non-penetrating (B1) disease behavior than group A3 (43.75% vs 28.33%, P=0.035). Patients in group A3 who had stricturing (B2) disease behavior were more than group A1 and group A2 (56.67% vs 18.18%, P=0.002; 56.67% vs 40.91%, P=0.034, respectively). Patients in group A2 who had B2 type were higher than group A1 (40.91% vs 18.18%, P=0.039). More patients in group A1 presented with a penetrating (B3) disease behavior than group A2 and group A3 (36.36% vs 10.80%, P=0.001; 36.36% vs 5.00%, P<0.001, respectively). The differences of disease location at ileocolonic (L3), isolated upper disease (L4), and perianal disease modifier (P) were not statistically significant among the three groups (all P>0.05) (Table 3).
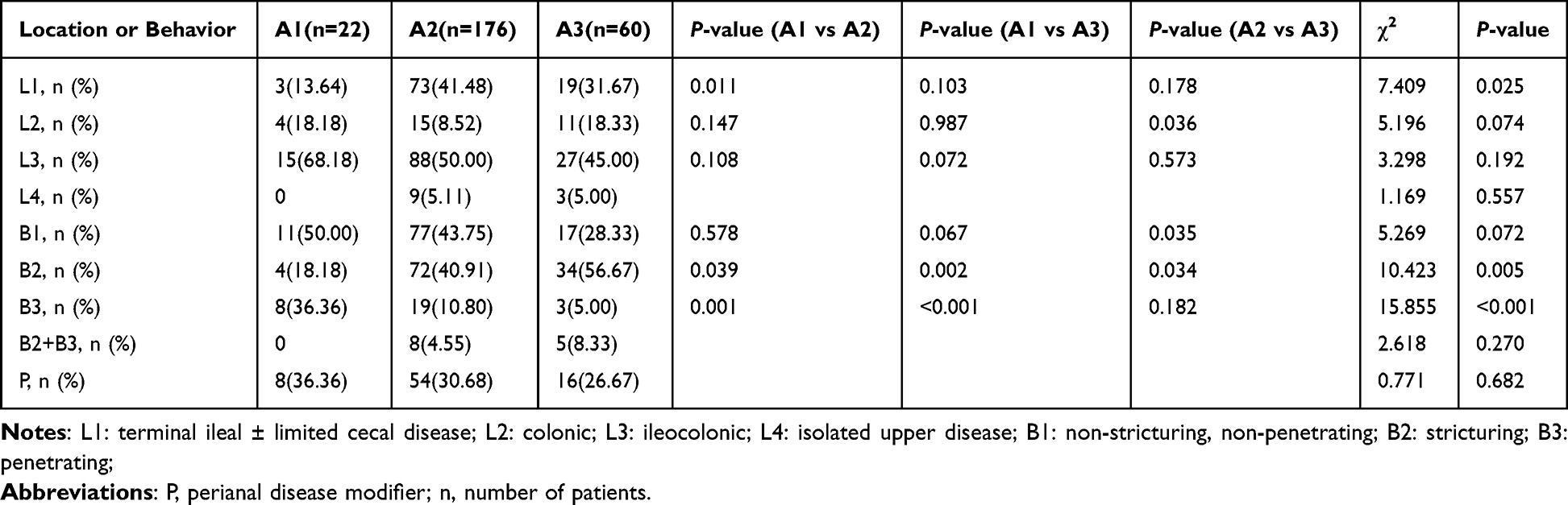 |
Table 3 Disease Locations or Behaviors Comparison Among A1, A2, A3 Groups |
Multivariate Logistic Regression Analysis
Parts of the clinical characteristics and laboratory tests whose P-value <0.05 were selected for multivariate logistic regression analysis further. Based on the multivariate logistic regression analysis, we found that compared with group A1, patients in group A2 were associated with lower TP levels [hazard ratios (HR)=0.915, 95% confidence interval (CI)=0.839~0.998, P=0.044]. Fewer patients in group A2 had a fistula formation than group A1 [HR (95% CI) =0.241(0.059–0.983), P=0.047]. The rates of CDI in group A2 were higher than group A1 (P<0.001). Compared to group A1, more female patients were presented in group A3 [HR (95% CI) =0.079 (0.008–0.800), P=0.032]. More patients in group A3 had a B2 disease behavior than group A1 [HR (95% CI) =4.570 (1.109–18.830), P=0.035]. In addition, the mean TP and PC levels in group A3 were lower than group A1 [HR (95% CI) =0.883 (0.801–0.972), P=0.011; HR (95% CI) =0.991 (0.985–0.997), P=0.004, respectively] (Table 4).
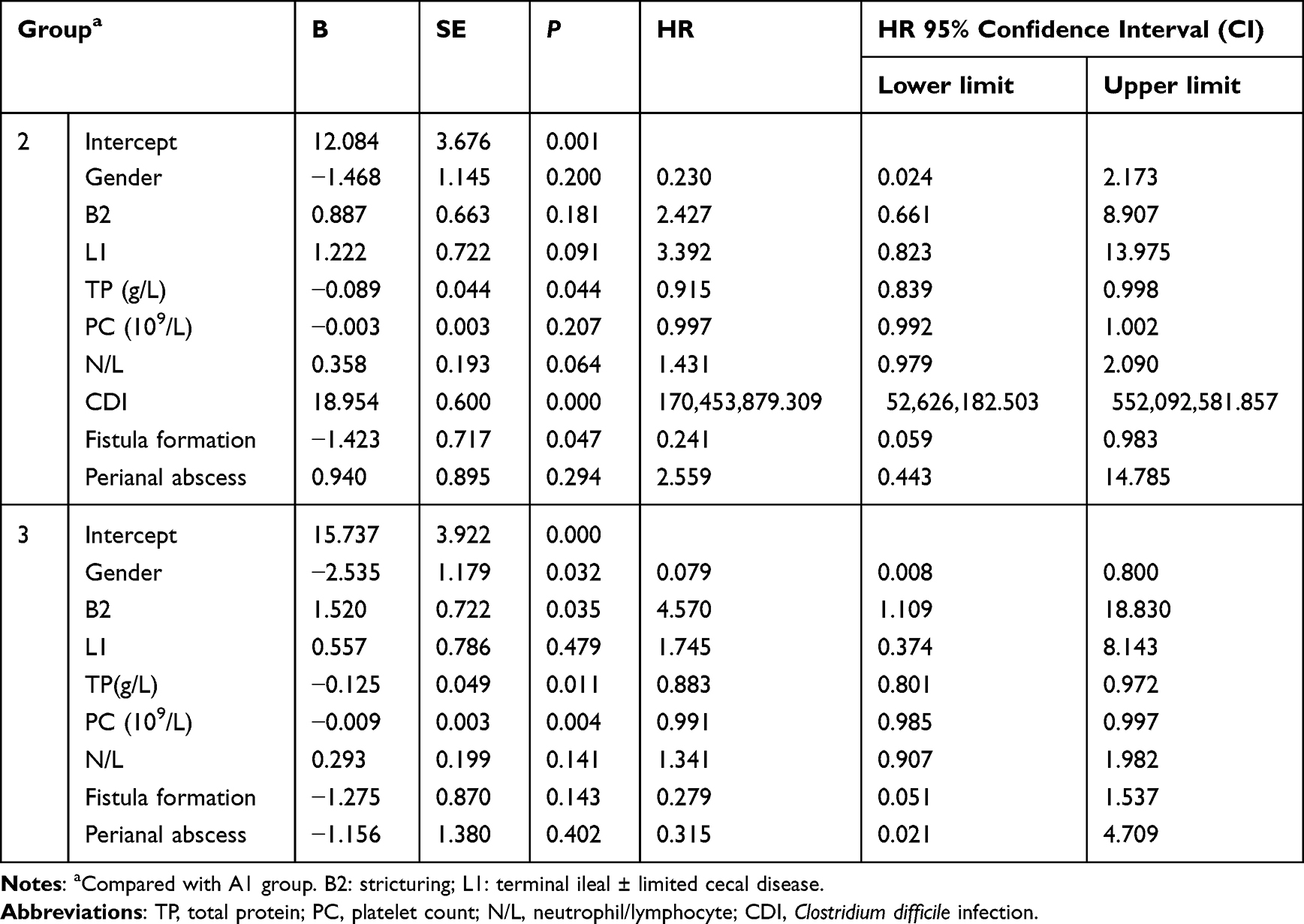 |
Table 4 Multivariate Logistic Regression Analysis Among A1, A2 and A3 Groups |
Discussion
To our knowledge, there had been limited studies which directly compared the different clinical characteristics and laboratory tests among various age groups in CD patients according to the Montreal classification. Here in this study, we investigated the differences of clinical presentations, laboratory tests, and disease behaviors among various age groups at diagnosis based on Montreal classification. The male predominance had been reported in pediatric CD.14 A nationwide cohort study in South Korea showed that the risk of developing CD in the middle-aged group (40–64 years old) was higher in men than women, but the difference disappeared when patients were above 64 years old, and the possible risk factors for developing CD included history of smoking, anemia, chronic kidney disease and low body mass index in Asians who were more than 40 years old.15 From our study, we showed that the gender discrepancy existed in different age groups, the group A1 had the highest male ratio which consisted of 95.45%, while in the group A2 and group A3, they were 75.00% and 48.33%, respectively, which suggested that CD was more likely to happen in male when patients were less than 40 years old, but as individuals growing older, the females could have more chance to be a CD patient.
The clinical presentations among CD patients stratified by age at diagnosis according to Montreal classification were distinct. From the clinical features, we demonstrated that CD patients in group A1 were more likely to have weight loss or growth retardation than patients in group A2 and group A3. The risk of developing a more complicated disease with perianal involvement was higher (40% vs 10%) in early-onset CD (≤17 years old) than late-onset CD (≥60 years old).16 A previous study in China10 showed that in perianal CD patients more complicated local manifestations were presented in early-onset CD patients, but adult-onset perianal CD patients were more likely to progress to severe luminal damage and increase the rate of intestinal resection, and the disease onset age could help to guide individual treatment of CD patients. We found that CD patients in group A2 had a higher risk for a perianal abscess than group A3. From our study, we revealed that patients in group A1 were more likely to have a perianal fistula formation than group A2 and group A3, but the difference disappeared between group A2 and group A3. Biologics plays an important role in the treatment of CD, and CD patients could benefit from them. It had been revealed that in CD patients the use of biologic agent varied inversely with age at diagnosis.17 Compared with patients in group A3, we found that patients in group A2 were more likely to use biological agents. The Italian group for the study of IBD found that when CD patients were classified by young adult-onset (16–39 years), adult-onset (40–64 years), and late-onset (≥65 years), the three age groups had an equal need for surgery and using of steroids.18 Another cohort study16 showed that compared to late-onset CD (≥60 years old), early-onset CD (≤17 years old) patients had a greater chance for using medical therapy, while the need for surgery did not increase. From our study, we displayed that the rates of surgery among the three groups were not statistically different, which was consistent with previous studies. A retrospective analysis in Greece showed that compared with patients without IBD, hospitalized IBD had a higher CDI rate.19 We found that CD patients in group A2 were more likely to have CDI than group A3, the occurrence rates were 17.05% and 6.67%, respectively. CDI could increase the health care burden and 90-day CDI-specific readmission rate of IBD,20 and it could increase the risk of surgery by depleting the beneficial fecal microbiome and methionine biosynthesis.21
We then investigated the differences of blood cell counts and some biochemistry results among the three groups based on Montreal classification. Researchers had found that active CD patients had higher values of neutrophils, monocytes, and neutrophil-to-lymphocyte ratio (NLR), but had lower values of lymphocyte-to-monocyte ratio (LMR) compared with inactive CD.22 From the complete blood counts, we showed that the neutrophil counts were higher in group A2 than those in group A3. The lymphocyte counts of group A1 were higher than group A3. Preoperative NLR had prognostic value in CD.23 CD patients who presented with abscesses, an acute indication for surgery, inflammatory masses and a colorectal cancer in the resected specimen had a higher NLR.23 In addition, a significant decrease in MCV levels and a significant increase in PC could be detectable prior to diagnosis in patients with CD, which might help reduce diagnostic delay, acquire earlier therapy and improve clinical outcomes.24 We found that the MCV and MCH in group A1 were lower than those of group A2 and group A3, which suggested that children or adolescent CD patients were more likely to suffer from iron deficiency anemia or malnutrition than adult CD patients. What’s more, PC could be significant higher in pediatric CD patients.25 From our study, we showed that the PC and platelet-crit (PCT) of group A1 and group A2 were higher than group A3. CD patients could suffer from malnourishment.26 We observed that TP among the three age groups was different, which suggested that we should pay attention to the nutritional status for CD patients.
Coagulation function tests were assessed among various age groups according to Montreal classification as well. The mean levels of PT were higher in IBD patients compared with healthy controls, and PT could predict disease activity and inflammation in female patients with CD.27 In addition, coagulation status was impaired in the CD patients who had intestinal fistula, and PT in patients with intestinal fistula was longer than CD patients without intestinal fistula.28 From the coagulation function, we found that PT and PT INR in group A2 patients were higher than that of patients in group A3, which might be explained by the differences of fistula formation in various age groups.
We next explored the differences of disease locations and behaviors among the three groups. The late adult onset and elderly onset CD patients had a lower rate of L3 disease location than other groups in Korea.29 We demonstrated that compared with patients in group A1, patients in group A2 were more like to have a disease location at L1. In addition, there were more patients in group A3 whose disease locations were at L2 than those in group A2. A Canadian cohort study showed that the proportion of L3 location was 53% in overall, and L1 location increased with age until 10 years old in pediatric CD.30 Those findings suggested that the extent of the lesions among different age groups was diverse. As for disease behaviors, the predominance in B1 was found to be more evident in pediatric-onset CD than adult-onset CD.31 A population-based cohort study in Denmark showed that 18% of patients progressed from B1 to B2 or B3, which increased the risk of surgical resection.32 The Italian study mentioned previously had also found that compared with adult-onset (40 to 64 years old) CD, late-onset (≥65 years old) CD were more likely to present with stenosing behavior.18 We revealed that the disease behavior of B1 in group A2 was more likely to be seen than those in group A3, and the B2 behavior was more common in group A2 and group A3 than group A1. In addition, more patients in group A3 had a B2 behavior than group A1 and group A2, which suggested that more CD patients could become stricturing in their disease courses. As more CD patients could have a complex disease behavior, such as stricturing behavior, those patients might be benefited from initiating or optimizing the treatment early. Biologics could reduce the overall rate of CD-related surgery.33 In addition, de-escalation of biologic therapy provides a treatment choice for CD patients.34 Long-term outcome in CD patients could be improved by early initiation of anti-TNF.35 Further studies should focus on how to optimize the treatment plan for older CD patients so as to prevent the disease progress and improve their prognosis.
In this study, we explored the differential clinical presentations, laboratory tests, and disease locations as well as disease behaviors among various age groups according to the Montreal classification. Based on different ages at diagnosis, we found that CD patients had different clinical features, which could help us predict the disease progress and initiate appropriate treatments to improve the prognosis of CD patients. However, there were some limitations of the current study. First, this study was a single-center retrospective analyzation. Second, the sample size in group A1 was relatively small. So prospective multi-center studies are needed in the future.
Conclusions
In summary, there had some differences in CD patients when they were stratified by age at diagnosis according to Montreal classification. More female patients were presented in group A3. Patients in group A2 was associated with lower TP levels compared to group A1. The mean TP and PC levels in group A3 were lower than group A1. What’s more, fewer patients in group A2 had a perianal fistula formation than group A1. In addition, more patients in group A3 had a B2 disease behavior than group A1. Based on those different clinical features, we could infer the disease behavior or other information according to the age at diagnosis. What’s more, we could also take early interventions to improve the prognosis for CD patients.
Abbreviations
RBC, red blood cell; Hb, hemoglobin; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; PC, platelet count; TP, total protein; Alb, albumin; Na, sodium; Ca, calcium; P, phosphorus; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IQR, interquartile range; n, number of patients; CDI, Clostridium difficile infection; PT, prothrombin time; INR, international normalized ratio; APTT, activated partial thromboplastin time; TT, thrombin time; Fg, fibrinogen; FDPs, fibrinogen degradation products; M, mean; SD, standard deviation; L1, terminal ileal ± limited cecal disease; L2, colonic; L3, ileocolonic; L4, isolated upper disease; B1, non-stricturing, non-penetrating; B2, stricturing; B3, penetrating; P, perianal disease modifier; n, number of patients.
Data Sharing Statement
All data generated or analysed during this study are included in this article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by ethics committee of the Renmin Hospital of Wuhan University. All subjects signed a document of informed consent.
Acknowledgments
The authors thank the patients involved in this study. In addition, the authors thank suggestions of Dr Zhengru Liu for this research.
Disclosure
The authors declare that they have no competing interests in this study.
References
1. Joana Torres SMJC, Mehandru S, Colombel J-F, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389:1741–1755. doi:10.1016/S0140-6736(16)31711-1
2. Zhulina Y, Udumyan R, Henriksson I, et al. Temporal trends in non-stricturing and non-penetrating behaviour at diagnosis of Crohn’s disease in Örebro, Sweden: a population-based retrospective study. J Crohn’s Colitis. 2014;8(12):1653–1660. doi:10.1016/j.crohns.2014.07.006
3. Ye Y, Manne S, Treem WR, et al. Prevalence of inflammatory bowel disease in pediatric and adult populations: recent estimates from large national databases in the United States, 2007–2016. Inflamm Bowel Dis. 2019. doi:10.1093/ibd/izz182
4. Lv H, Jin M, Zhang H, et al. Increasing newly diagnosed inflammatory bowel disease and improving prognosis in China: a 30-year retrospective study from a single centre. BMC Gastroenterol. 2020;20(1). doi:10.1186/s12876-020-01527-1
5. Bai X, Zhang H, Ruan G, et al. Long-term disease behavior and surgical intervention analysis in hospitalized patients with Crohn’s disease in china: a retrospective cohort study. Inflamm Bowel Dis. 2022;28(Supplement_2):S35–41. doi:10.1093/ibd/izab295
6. Ministro P, Dias CC, Portela F, et al. Age at diagnosis is determinant for the outcome of inflammatory bowel disease: is it a Myth? Clin Transl Gastroenterol. 2021;12(2):e309. doi:10.14309/ctg.0000000000000309
7. Tang WJ, Shi P, Zheng CF, et al. Special clinical characteristics and outcomes in Chinese pediatric patients with early‐onset Crohn’s disease. J Digest Dis. 2019;20(10):539–546. doi:10.1111/1751-2980.12803
8. Lichtenstein GR, Shahabi A, Seabury SA, et al. Lifetime economic burden of Crohn’s disease and ulcerative colitis by age at diagnosis. Clin Gastroenterol H. 2020;18(4):889–897. doi:10.1016/j.cgh.2019.07.022
9. Satsangi J. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. GUT. 2006;55(6):749–753. doi:10.1136/gut.2005.082909
10. Wang H, Wu Y, Ye C, et al. Perianal disease onset age is associated with distinct disease features and need for intestinal resection in perianal Crohn’s disease: a ten-year hospital-based observational study in China. Bmc Gastroenterol. 2021;21(1). doi:10.1186/s12876-021-01961-9
11. Day AS. Crohn’s and colitis in children and adolescents. World J Gastroentero. 2012;18(41):5862. doi:10.3748/wjg.v18.i41.5862
12. Inflammatory Bowel Disease Group CSOG, Association. Chinese consensus on diagnosis and treatment in inflammatory bowel disease (2018), Beijing. J Digest Dis. 2021;22(6):298–317. doi:10.1111/1751-2980.12994
13. Gomollón F, Dignass A, Annese V, et al. European evidence-based consensus on the diagnosis and management of Crohn’s Disease 2016: part 1: diagnosis and medical management. J Crohn’s Colitis. 2016;11(1):3–25. doi:10.1093/ecco-jcc/jjw168
14. Kim HJ, Oh SH, Kim DY, et al. Clinical characteristics and long-term outcomes of paediatric Crohn’s disease: a single-centre experience. J Crohn’s Colitis. 2017;11(2):157–164. doi:10.1093/ecco-jcc/jjw146
15. Moon JM, Kang EA, Han K, et al. Trends and risk factors of elderly-onset Crohn’s disease: a nationwide cohort study. World J Gastroentero. 2020;26(4):404–415. doi:10.3748/wjg.v26.i4.404
16. Cantoro L, Lenti MV, Monterubbianesi R, et al. Early‐onset versus late‐onset Crohn’s disease: an Italian cohort study. United Eur Gastroent. 2020;8(1):52–58. doi:10.1177/2050640619860661
17. Feagins LA, Spechler SJ. Biologic agent use varies inversely with age at diagnosis in Crohn’s disease. Digest Dis Sci. 2010;55(11):3164–3170. doi:10.1007/s10620-010-1397-9
18. Viola A, Monterubbianesi R, Scalisi G, et al. Late-onset Crohn’s disease: a comparison of disease behaviour and therapy with younger adult patients: the Italian Group for the Study of Inflammatory Bowel Disease ‘AGED’ study. Eur J Gastroen Hepat. 2019;31(11):1361–1369. doi:10.1097/MEG.0000000000001546.
19. Viazis N, Pontas C, Karmiris K, et al. Prevalence of Clostridium difficile infection among hospitalized inflammatory bowel disease patients in Greece. Eur J Gastroen Hepat. 2019;31(7):773–776. doi:10.1097/MEG.0000000000001414
20. Palacios Argueta P, Salazar M, Attar B, et al. 90-Day specific readmission for clostridium difficile infection after hospitalization with an inflammatory bowel disease flare: outcomes and risk factors. Inflamm Bowel Dis. 2021;27(4):530–537. doi:10.1093/ibd/izaa224
21. Hellmann J, Andersen H, Fei L, et al. Microbial shifts and shorter time to bowel resection surgery associated with C. difficile in pediatric Crohn’s disease. Inflamm Bowel Dis. 2019. doi:10.1093/ibd/izz263
22. Mengque X. Correlation between serological biomarkers and disease activity in patients with inflammatory bowel disease. Biomed Res Int. 2019;2019:1–7. doi:10.1155/2019/6517549.
23. Argeny S, Stift A, Bergmann M, et al. Prognostic value of preoperative neutrophil-to-lymphocyte ratio in Crohn’s disease. Wien Klin Wochenschr. 2018;130(11–12):398–403. doi:10.1007/s00508-018-1322-3
24. Irwin JR, Ferguson E, Simms LA, et al. Detectable laboratory abnormality is present up to 12 months prior to diagnosis in patients with crohn’s disease. Digest Dis Sci. 2019;64(2):503–517. doi:10.1007/s10620-018-5357-0
25. Ashton JJ, Borca F, Mossotto E, et al. Analysis and hierarchical clustering of blood results before diagnosis in pediatric inflammatory bowel disease. Inflamm Bowel Dis. 2018. doi:10.1093/ibd/izy369
26. Ferreiro B, Llopis-Salinero S, Lardies B, et al. Clinical and nutritional impact of a semi-elemental hydrolyzed whey protein diet in patients with active Crohn’s disease: a prospective observational study. Nutrients. 2021;13(10):3623. doi:10.3390/nu13103623
27. Shen J, Ran ZH, Zhang Y, et al. Biomarkers of altered coagulation and fibrinolysis as measures of disease activity in active inflammatory bowel disease: a gender-stratified, cohort analysis. Thromb Res. 2009;123(4):604–611. doi:10.1016/j.thromres.2008.04.004
28. Li Y, Jian AR, Ge FW, et al. Impaired coagulation status in the Crohn’ s disease patients complicated with intestinal fistula. Chinese Med J-Peking. 2018;131(5). doi:10.4103/0366-6999.226072
29. Hwang SW, Kim JH, Im JP, et al. Influence of age at diagnosis on the clinical characteristics of Crohn’s disease in Korea: results from the CONNECT study. J Gastroen Hepatol. 2017;32(10):1716–1722. doi:10.1111/jgh.13775
30. Dhaliwal J, Walters TD, Mack DR, et al. Phenotypic variation in paediatric inflammatory bowel disease by age: a multicentre prospective inception cohort study of the Canadian children IBD network. J Crohn’s Colitis. 2020;14(4):445–454. doi:10.1093/ecco-jcc/jjz106
31. Park SH, Im JP, Park H, et al. Clinical features and long-term outcomes of paediatric-onset inflammatory bowel disease in a population-based cohort in the Songpa-Kangdong District of Seoul, Korea. J Crohn’s Colitis. 2022;16(2):207–215. doi:10.1093/ecco-jcc/jjab132
32. Lo B, Vester-Andersen MK, Vind I, et al. Changes in disease behaviour and location in patients With Crohn’s disease after seven years of follow-up: a Danish population-based inception cohort. J Crohn’s Colitis. 2018;12(3):265–272. doi:10.1093/ecco-jcc/jjx138
33. Kurowski JA, Milinovich A, Ji X, et al. Differences in biologic utilization and surgery rates in pediatric and adult Crohn’s Disease: results from a large electronic medical record-derived cohort. Inflamm Bowel Dis. 2021;27(7):1035–1044. doi:10.1093/ibd/izaa239
34. Hirten RP, Lakatos PL, Halfvarson J, et al. A user’s guide to de-escalating immunomodulator and biologic therapy in inflammatory bowel disease. Clin Gastroenterol H. 2020;18(6):1336–1345. doi:10.1016/j.cgh.2019.12.019
35. Frei R, Fournier N, Zeitz J, et al. Early Initiation of Anti-TNF is associated with favourable long-term outcome in crohn’s disease: 10-year-follow-up data from the Swiss IBD cohort study. J Crohn’sColitis. 2019;13(10):1292–1301. doi:10.1093/ecco-jcc/jjz057
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.