")
Back to Journals » Infection and Drug Resistance » Volume 13
Clinical Features and Co-Infections in Invasive Pulmonary Aspergillosis in Elderly Patients
Authors Lao M , Zhang K, Zhang M, Wang Q, Li J, Su L, Ding M , He W, Gong Y
Received 26 July 2020
Accepted for publication 19 September 2020
Published 12 October 2020 Volume 2020:13 Pages 3525—3534
DOI https://doi.org/10.2147/IDR.S273946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Minxi Lao,1,* Kaicong Zhang,1,* Meng Zhang,2,* Qian Wang,1 Jin Li,1 Lei Su,1 Meilin Ding,1 Wen He,1 Yingying Gong1
1Department of Geriatrics, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Pathology, Shenzhen Second People’s Hospital/The First Affiliated Hospital of Shenzhen University Health Science Center, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingying Gong Email [email protected]
Introduction: Invasive pulmonary aspergillosis (IPA) is a potentially lethal opportunistic infection. Old age is one of the important risk factors of IPA. However, data regarding the clinical characteristics and prognostic factors of elderly patients with IPA are limited, with data regarding co-infection of other bacteria or fungi even scarcer.
Methods: We performed a retrospective study of elderly patients (aged≥ 60) with IPA diagnosed in the First Affiliated Hospital of Sun Yat-sen University from January 2000 to December 2019. Data collection included demographic characteristics, premorbid conditions, underlying diseases, clinical manifestations, therapeutic procedures, and pathogenic detection. Associated factors were analyzed by logistic regression analysis.
Results: A total of 97 elderly patients (75 males, 22 females) with IPA were included. The all-cause mortality rate was 36.1% (35/97). Body mass index (BMI) (adjusted odds ratio (OR) 1.27, 95% confidence interval (CI) 1.08– 1.50, P=0.01), solid organ malignancy (adjusted OR 5.37, 95% CI 1.35– 21.33, P=0.02), and co-infections (adjusted OR 5.73, 95% CI 1.40– 23.51, P=0.02) were associated with mortality in the elderly patients with IPA. Nearly, 76.3% (74/97) of the patients developed co-infections. Most of the infections (55/74, 74.3%) involved the lung. A total of 77 strains of bacteria were isolated, and Gram-negative bacteria (63/77, 81.3%) were predominant. Patients with co-infections are older (72.3± 7.6 vs 67.4± 7.4, P=0.04), prone to admit to the intensive care unit (ICU) (59.5% vs 26.1%, P=0.01), and present lymphopenia (60.8% vs 26.1%, P=0.004). In multivariate analysis, ICU admission (adjusted OR 4.57, 95% CI 1.53– 13.67, P=0.01), and lymphopenia (adjusted OR 4.82, 95% CI 1.62– 14.38, P=0.01) were significantly associated with co-infection in the elderly patients with IPA.
Conclusion: IPA is a fatal disease in the elderly population. Co-infection is closely associated with mortality. Lymphopenia could be an indicator for co-infection in the elderly patients with IPA.
Keywords: pulmonary aspergillosis, elderly, co-infection, mortality
Introduction
Invasive pulmonary aspergillosis (IPA) is an invasive fungal disease (IFD) with high mortality. Patients with neutropenia, treated with a long course of glucocorticoids (GC) or immunosuppressants, are extremely risky for IPA.1 Increasing evidence suggests that patients with various comorbidities such as diabetes mellitus (DM), malnutrition, and chronic pulmonary disease are potential hosts for IPA.2,3 Elderly patients are usually complicated with but not limited to the chronic medical conditions. They display some characteristics different from their younger counterparts. The cleaning function of respiratory epithelial cells degenerates with age, leading to impaired defense against air-transmitting pathogens.4 Besides, the biological function of lymphocytes alters with aging. A skew towards memory T cells due to immunosenescence is observed in the elderly population.5 In other words, elderly patients bearing a wide range of risk factors of IPA and need attentions.
The mortality of IPA increases with age.6 Many factors contribute to the high mortality of IPA. Of note, co-infections with other pathogens are remarkable. In patients with invasive mold infection and connective tissue disease (CTD), the co-infection rate is significantly higher in non-survivors than survivors (70% vs 18.7%).7 Co-infections increase the difficulty in treating IPA. However, until recently, few studies report the situation of co-infections in patients with IPA.
In our previous study, we demonstrated that aspergillosis accounts for a growing proportion of invasive fungal diseases in the elderly population during the last two decades.8 However, much is left to know due to the constraints of space. In the current study, we reported the clinical features of IPA in the elderly population, focusing on co-infections, aiming to provide an in-depth investigation of IPA in the specific population.
Patients and Methods
Study Design
A retrospective study was performed on the inpatients age ≥60 years from the First Affiliated Hospital of Sun Yat-sen University from January 1st, 2000 to December 31st, 2019. The International Classification of Diseases-10 (ICD-10) coding of discharged diagnoses was used to identify patients with IPA. One episode of IPA from each patient was collected. Patients without complete clinical data or developing IPA at the age <60 were excluded. This work was conducted according to the provisions of the Declaration of Helsinki.
Case Definition
IPA was designated as proven, probable, or possible according to the EORTC/MSG Guidelines.9 Patients with histopathological evidence of aspergillosis obtained by lung biopsy or surgery were considering having proven IPA. Patients presenting classical chest radiographic imaging (dense, well-circumscribed lesions with or without a halo sign, air-crescent sign, cavity, or bronchoscopy found tracheobronchial ulceration, nodule, pseudomembrane, plaque, or eschar) and having Aspergillus spp. isolated from sputum, bronchoalveolar lavage fluid (BALF), or bronchial brush, or showing galactomannan (GM) antigen detection positive in plasma, serum, or BALF were considered having probable IPA. Possible IPA was diagnosed based on the aforementioned clinical criteria but without mycological evidence.
Co-infection was considered in two cases: (i) If IPA occurred during the treatment against bacteria, virus or superficial fungi, the advanced infections were considered as co-infection. (ii) Infection with bacteria, virus or superficial fungi was considered as co-infection if it occurred from the diagnosis of IPA till discharge. Co-infected agents can be isolated from any body fluid samples obtained from the suspected sites, not limited to the culture yielding Aspergillus spp. Bacterial infection was diagnosed proven if responsible pathogens were identified by microscopy or culturing. Otherwise, bacterial infections were considered probable based on the clinical symptoms, laboratory test results, radiographic findings, and response to antibiotic therapy. Drug susceptibility test was performed on the isolated bacteria. Multidrug resistance (MDR) bacteria were defined as resistance to at least one agent in three or more antimicrobial categories. Pandrug resistance (PDR) bacteria were determined if the bacteria were resistant to all agents in all antimicrobial categories.10 Inappropriate antibacterial therapy is defined as non-compliance with at least one of the following rules: (i) documented antibiotic indication, (ii) appropriate collection of microbiological samples, (iii) appropriate dose, (iv) appropriate de-escalation strategy and duration of treatment.11 Acute viral infections were diagnosed based on a combination of: (i) clinical features (e.g., prolonged fever, arthralgia, or cutaneous rash) and/or specific imaging (e.g., interstitial pneumonia); (ii) suggestive of acute viral infections in response to antiviral treatment; and (iii) positive results of antiviral immunoglobulin (Ig) M antibodies and subsequent specific IgG antibodies. A diagnosis of herpes zoster was clinically established by the presence of a typical vesicular eruption developing in a dermatomal distribution. Considering the clinical manifestations of herpes zoster are relatively specific, virology examination is not necessarily needed in this case. Superficial fungal infections were defined as fungal infections that occurred in the oral cavity, skin/mucosa, or genitalia based on direct examination and culture methods.
Clinical Data
Clinical data were collected from the medical records. Clinical characteristics of IPA included symptoms and signs, sites of infection, and anti-fungi treatment. Underlying diseases were recorded. Laboratory data included routine blood tests and blood biochemistry. Neutropenia was defined as an absolute neutrophil count of less than 2.0×109/L.12 Lymphopenia was defined as peripheral blood lymphocyte count<1.0×109/L.12 Anemia was defined as hemoglobin <120 g/L in males and hemoglobin <110 g/L in females at sea level.13 Hypoalbuminemia was defined as serum albumin level <3.5 g/dl. Microbial culture and biopsy findings were recorded if available. The cut-off value for GM antigen in blood and respiratory samples was 0.9 according to the manufacturer’s recommendation. Aspergillus spp. were distinguished according to the color of cultured colonies and morphology in direct microscopical analysis. Prolonged hospitalization was defined as hospital stay longer than 10 days. Prolonged use of GC was defined as a mean minimum dose of 0.3 mg/kg/day of prednisone equivalent for >3 weeks.9 The all-cause mortality was estimated at hospital discharge.
Statistical Analysis
Normally distributed quantitative variables were expressed as mean ± SD, while non-normal variables were expressed as median (interquartile range, IQR). Qualitative variables were expressed as absolute numbers and percentages. Proportions were compared using Fisher’s exact test or Pearson χ2 test. Between-group comparison was evaluated using Student’s t-test for continuous variables with normal distribution. Odds ratio (OR) and corresponding 95% confidence interval (CI) of clinically significant variables with a P<0.05 in univariate regression analysis was adjusted by multivariate logistic regression analysis, applying forward procedure. The two-sided level of significance was set at P < 0.05. All statistical analysis was performed with the SPSS 19 statistical package (IBM).
Results
Patient Characteristics
A total of 233,471 patients were screened, and 114 potential patients were selected. Seventeen patients were excluded for data incompleteness. Finally, 97 elderly patients (75 males, 22 females) with IPA were included. The mean (SD) age was 71.1±7.7 years (range, 60–89). Eighteen (18.6%) cases were proven IPA, 78 (80.4%) cases were probable, and 1 (1.0%) case was possible. One (1.0%) patient was infected with human immunodeficiency virus (HIV). No patient received hematopoietic stem cell transplant (HSCT).
Clinical symptoms of IPA included expectoration (62/97, 63.9%), dry coughing (57/97, 58.8%), fever (56/97, 57.7%), dyspnea (31/97, 32.0%), and hemoptysis (18/97, 18.6%). The radiographic features included patchy infiltrates (52/97, 53.6%), nodules (40/97, 41.2), cavitary lesions (27/97, 27.8%), and ground glass opacity (12/97, 12.4%). Air-crescent sign was found in 3 (3.1%) patients.
The positivity of GM test in serum sample and BALF was 30.1% (22/73) and 32/39 (82.1%), respectively. A total of 72 strains of Aspergillus spp. were isolated. A. fumigatus (52/72, 72.2%) accounted for most of the cases, followed by A. flavus (15/72, 20.8%), A. niger (4/72, 5.6%) and A. terreus (1/72, 1.4%). Pathological evidence of IPA was obtained by fiberoptic bronchoscopy in eight patients and surgery in nine patients.
Ninety-one (93.8%) patients received antifungal medications. Triazoles (67/91, 73.6%) remained the cornerstone in IPA treatment, even in the elderly population, followed by echinocandins (13/91, 14.3%). Among 67 patients on triazoles monotherapy, 58 patients (86.6%) were treated with voriconazole, 8 patients (11.9%) with itraconazole, and 1 patient (1.5%) with posaconazole. Among 13 patients on echinocandins monotherapy, 9 patients (69.2%) were treated with caspofungin and 4 patients (30.8%) with micafungin. Anti-fungal treatment was initiated in 17 (18.7%) patients when IPA was suspected and in 74 (81.3%) patients with microbiological support.
The all-cause mortality rate estimated at discharge was 36.1% (35/97). The oldest old (age ≥80 years) had the highest mortality (7/14, 50.0%), followed by patients aged between 70 and 79 (15/38, 39.5%), and patients aged between 60 and 69 (13/45, 28.9%). The mortality in patients admitted to the intensive care unit (ICU) was 64.0% (32/50). Causes of death are summarized in Table S1. Nearly half of the patients (16/35, 45.7%) died of septic shock. The mortality in patients receiving triazoles monotherapy (17/67, 25.4%) was lower than that in patients receiving echinocandins monotherapy (10/13, 76.9%) (P=0.001). No differences in age (75.7 ± 8.2 vs 71.2 ± 8.7, P=0.20), ICU admission (82.4% vs 100%, P=0.23), or co-infections (88.2% vs 100%, P=0.39) between groups were detected.
Associated Factors for Mortality in Elderly Patients with IPA
A comparison between survivors and non-survivors is shown in Table 1. The average (SD) age of the non-survivors was older than the survivors (73.6±14.8 vs 69.4±7.2, P<0.03). The prevalence of neutropenia increased in non-survivors (11.4% vs 1.6%, P=0.04). A large proportion of deceased patients were complicated with co-infections (91.4% vs 67.7%, P=0.01). Among survived patients, 10 out of 58 (17.2%) received antifungal therapy when IPA was suspected, while the number in non-survivor group was 21.2% (7/33). The impact of antifungal therapy timing on mortality was not significant (P=0.78)
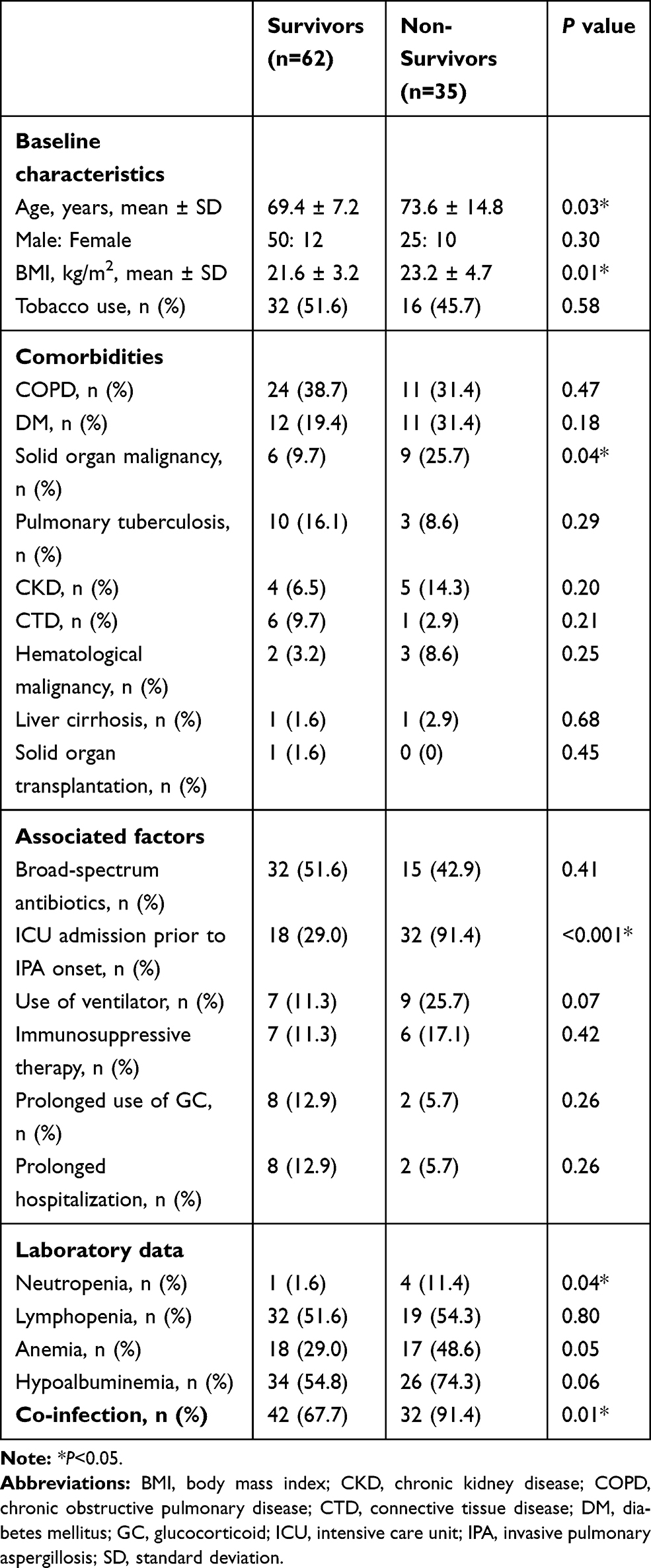 |
Table 1 Comparison Between Survivors and Non-Survivors |
Several variables were identified as associated factors for mortality in univariate logistic regression analysis. We constructed two models with or without ICU admission in multivariate regression analysis. In model 1, ICU admission appeared to be associated with mortality exclusively (adjusted OR 26.07, 95% CI 7.08–96.09, P<0.001). Considering 95% CI was relatively wide, we excluded ICU admission in model 2, and found that BMI (adjusted OR 1.27, 95% CI 1.08–1.50, P=0.01), solid organ malignancy (adjusted OR 5.37, 95% CI 1.35–21.33, P=0.02), and co-infections (adjusted OR 5.73, 95% CI 1.40–23.51, P=0.02) were associated with mortality in the elderly patients with IPA (Table 2).
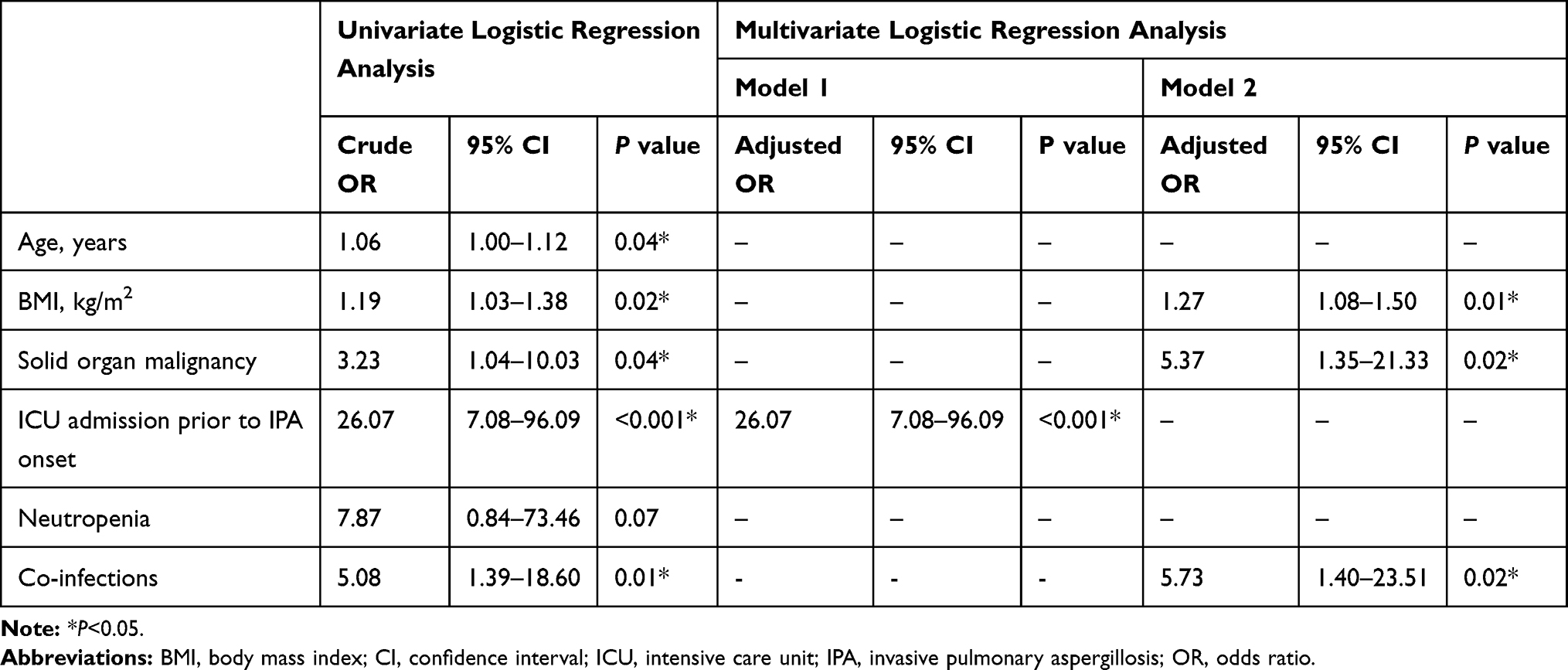 |
Table 2 Associated Factors for Mortality |
Characteristics of Co-Infections in Elderly Patients with IPA
Since co-infection is a common complication and the most critical factor for mortality, we further analyzed the characteristics of co-infections in the elderly patients with IPA.
Nearly 76.3% (74/97) of the patients developed co-infections. Nearly 70.3% (52/74) of the infections occurred after IFD diagnosis. Most of the infections (55/74, 74.3%) presented as pneumonia, and 21.6% (16/74) were disseminated (Table 3). Fifty-nine patients were infected with bacteria (59/74, 79.7%), and the rest of them (15/74, 20.3%) were infected with multiple agents simultaneously. In particularly, 7 (46.6%) patients were infected with bacteria and Candida spp., 1 (6.7%) was infected with bacteria and Cryptococcus spp., 6 (40.0%) were infected with bacteria and virus, and 1 (6.7%) was infected with bacteria, Candida spp. and virus. Viral infections included cytomegalovirus pneumonia (n=3), influenza virus pneumonia (n=2), herpes zoster (n=2), and herpes simplex infection (n=1).
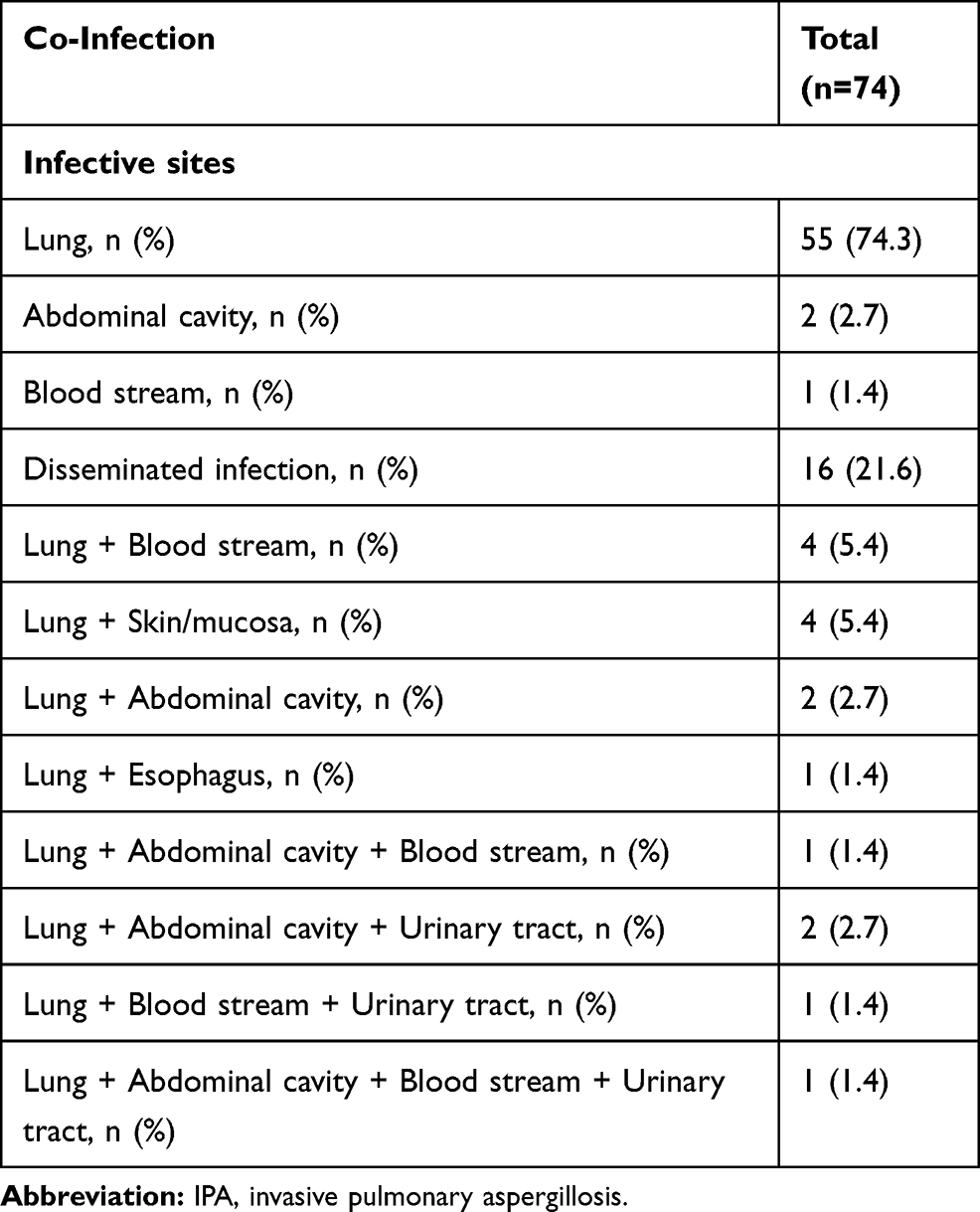 |
Table 3 Sites of Co-Infections |
A total of 77 strains of bacteria were isolated (Table 4), and Gram-negative bacteria (63/77, 81.8%) were predominant. A. baumannii (21/77, 27.3%), P. aeruginosa (10/77, 13.0%) and S. maltophilia (7/77, 9.1%) were the leading agents. Infections caused by Gram-positive bacteria were less common (14/77, 18.2%). E. faecium (5/77, 6.5%), E. faecalis (3/77, 3.9%), and S. haemolyticus (3/77, 3.9%) were the leading pathogens. One strain of E. coli was positive for extended-spectrum beta-lactamase (ESBL). Of note, 5 (6.5%) strains of the bacteria were MDR, including 3 strains of P. aeruginosa, 1 strain of A. baumannii, and 1 strain of E. aerogenes. Eleven (14.3%) strains of A. baumannii were PDR.
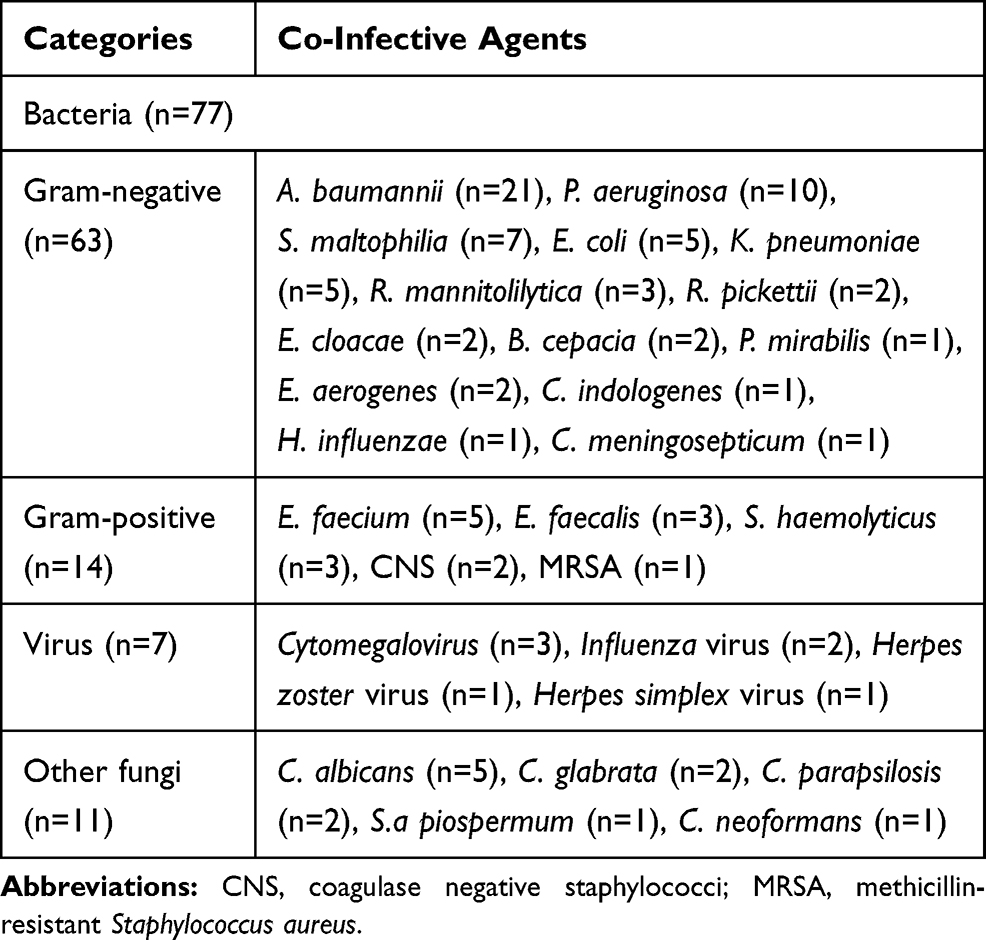 |
Table 4 Distributions of Co-Infected Agents |
Antibiotics were prescribed to 74 patients prior to the diagnosis of IPA, and the median (IQR) duration of antibiotics intake was 10 (14.5) days. Among them, 52 (70.3%) patients received antibiotics before IPA without indication. The mortality rate in this group was 42.3% (22/52). In contrast, 22 (29.7%) patients received antibiotics before IPA with etiological support, and 10 of them died (45.4%). All patients with bacterial infections occurred after the diagnosis of IPA received appropriate antibiotic treatment. The relation between inappropriate antibacterial therapy before IPA and mortality is not statistically significant (P=0.80).
Associated Factors for Co-Infection in Elderly Patients with IPA
A comparison between patients with and without co-infections is shown in Table 5. Patients with co-infections are older (72.3±7.6 vs 67.4±7.4, P=0.04), prone to admit to ICU (59.5% vs 26.1%, P=0.01), and present lymphopenia (60.8% vs 26.1%, P=0.004).
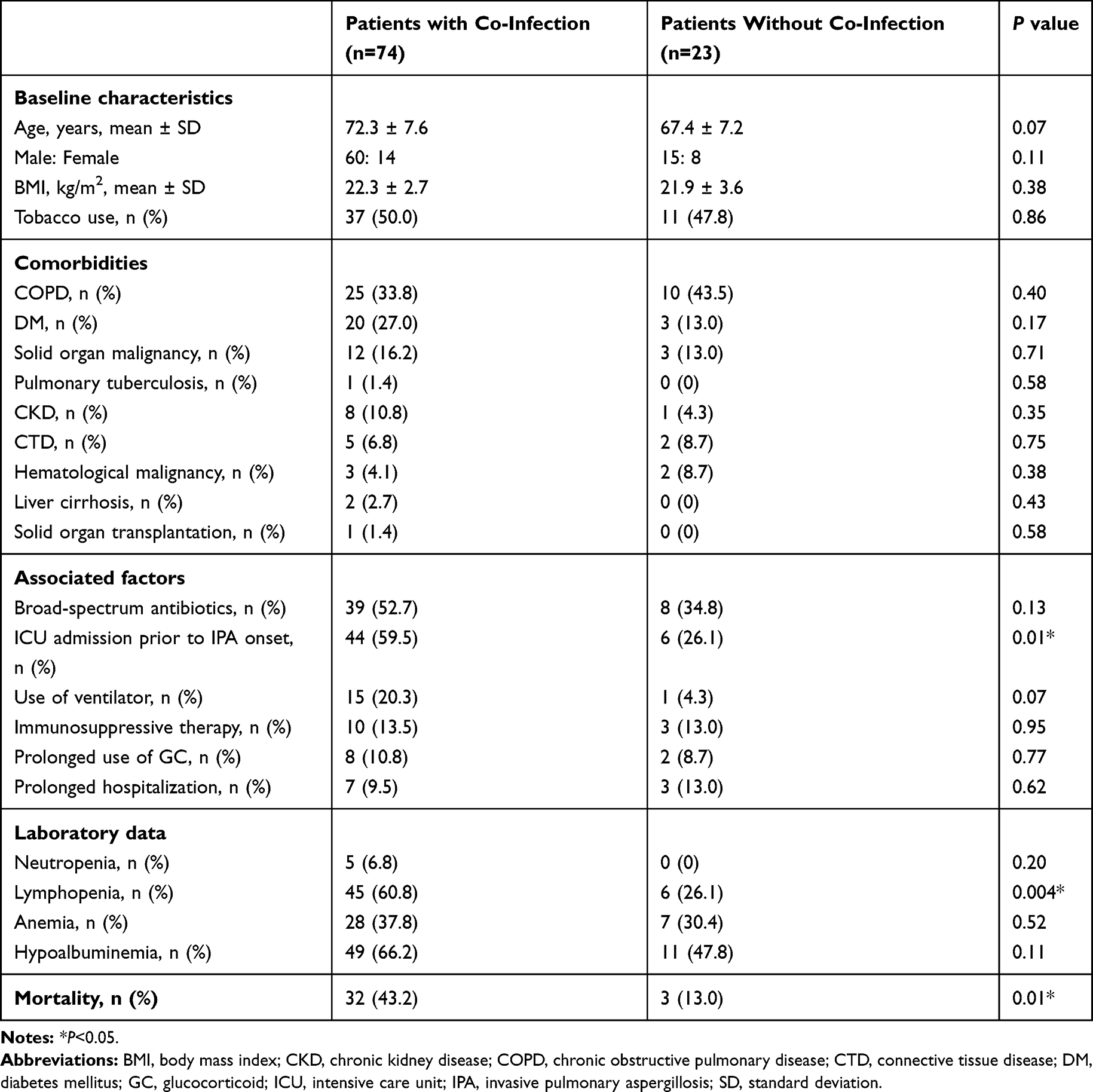 |
Table 5 Comparison Between Patients with and without Co-Infection |
Variables identified as associated factors for co-infection in univariate logistic regression analysis were analyzed in multivariate regression analysis. ICU admission (adjusted OR 4.57, 95% CI 1.53–13.67, P=0.01), and lymphopenia (adjusted OR 4.82, 95% CI 1.62–14.38, P=0.01) were associated with co-infection in the elderly patients with IPA (Table 6).
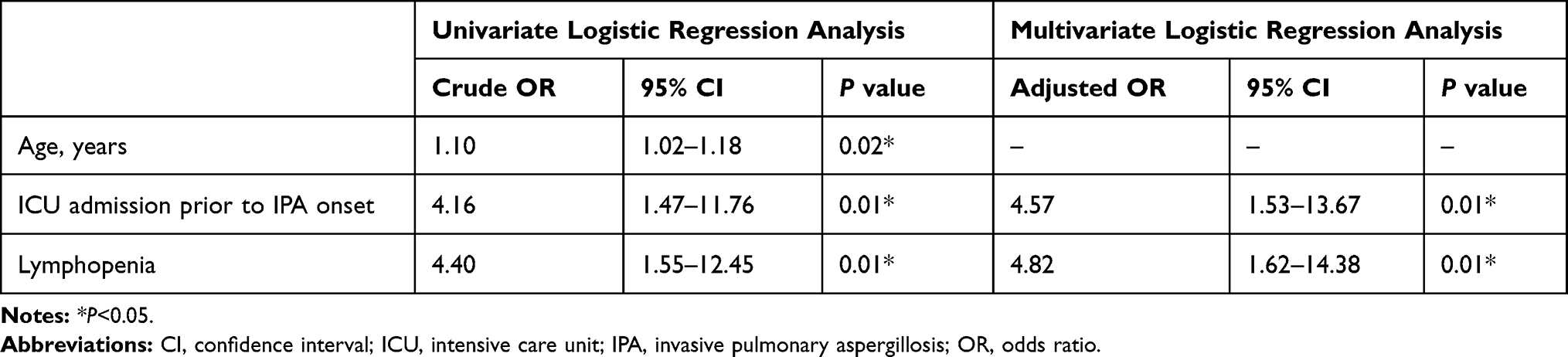 |
Table 6 Associated Factors for Co-Infections |
Discussion
The mortality of IPA in the elderly is extremely high and increased with age. Co-infection is a great contributor to mortality, mainly presenting as pneumonia caused by Gram-negative bacteria. Elderly patients with lymphopenia are prone to develop co-infections. Surveillance of lymphocyte count and effective control of co-infection could improve the clinical outcomes of IPA in the elderly.
IPA is a fatal disease in the elderly patients. In patients with hematological malignancy, the overall mortality within 12 weeks after IPA diagnosis is reported to be 40.1%.14 In the current study, the mortality of IPA in the elderly patients is close to that in the severe immunocompromised population. The overall mortality in critically ill elderly patients with IPA is extremely high (82.9%), exceeding that in the general population (77%).15 Previous findings and our results re-enforce the lethality of IPA in the elderly patients. Triazoles are the preferred agents for IPA.16 In our study, patients receiving triazoles treatment were more likely to survive than those receiving echinocandins, while the other potential risk factors such as age, ICU admission, and co-infections were comparable. Our findings imply that triazoles continue to be the first-line agents for IPA in the elderly populations.
Many factors are considered as risk factors of mortality and discussed widely.17 BMI is a simple biochemical parameter related to nutritional status. Generally, lower BMI, suggesting sarcopenia and malnutrition, is associated with higher mortality in the elderly population.18,19 In contrast, obese patients might have a survival benefit.20 However, in our study, higher BMI was demonstrated to have an unfavorable effect on the elderly patients with IPA. This paradoxical association between BMI and mortality has been observed in various chronic diseases.21,22 The reason why higher BMI is associated with poorer outcome in the elderly is yet not clear. One probable explanation is that overweight and obesity are found to reduce pulmonary function longitudinally and may relate to systemic inflammation that contributes to the development of comorbidities and exacerbations in chronic diseases.23,24 Moreover, Asians usually have a higher percentage of body fat than non-Asians with a similar BMI.25 In other words, high BMIs in the elderly patients do not insure favorable prognosis. Future studies with a greater number of subjects will allow for a more meaningful analysis of the relationship between an increased BMI and mortality in elderly patients with IPA.
So far, data on the clinical relevance of co-infection in IPA are relatively limited. Previous studies reported that the mixed bacteria and Candida spp. infections occur in about 23–57% of the candidemia cases.26,27 Similarly, a high proportion (76.3%) of the patients infecting with mixed pathogens was observed in our study, suggesting that co-infection is an outstanding issue in the elderly patients with IPA. It is not yet clear whether co-infections lead to poor clinical outcomes. One study identified that the survival rate in patients with bacteria-Candida spp. bloodstream infections is lower than that in patients with Candida spp. infection alone.28 Moreover, bacterial-fungal co-infections seem to exert more deleterious effects in the context of cystic fibrosis compared to single pathogen infection.29,30 In consistence, we provide the evidence that co-infections are associated with increased mortality in the elderly patients with IPA. We further analyzed the distribution of co-infected agents. Our results showed that most of the cases were infected with Gram-negative bacteria. One of the possible reasons is that most of the co-infected cases occurred after the diagnosis of IFD, and these cases were usually nosocomial infections. Thus, the distribution of the co-infected agents is consistent with that in nosocomial infections.31 Of note, the inappropriate use of antibiotics before IPA seems to be irrelevant to all-cause mortality. One reason could be that antibiotics were applied for a short period of time in our study. Data regarding the misuse of antibiotics and mortality in patients with IPA are scarce. A previous study showed that short-term intake of antibiotics (<30 days) is not related to aspergillosis in non-neutropenic, non-transplant patients.32 Our results did not contradict the conception that long-term use of antibiotics might increase the susceptibility of fungal infection.33 Our findings indicate that co-infections in elderly patients with IPA are common. Gram-negative bacteria are the major co-infected agents. Empirical coverage of Gram-negative bacteria is necessary when choosing appropriate antibiotics.
Lymphopenia is an important associated factor with elderly patients with co-infection. Except for neutropenia, lymphopenia is found to be associated with invasive fungal disease in many medical backgrounds.7 Age-related remodeling of the immune system is considered as a major contributor to the increasing possibility of infections in the elderly.34,35 T cells are critical defenders against invasive fungi.36 However, both the output of naïve T cells from thymus and the activation of CD4+T cells decreased during aging physiologically.37,38 Besides, comorbidities such as DM contribute to the exhaustion of lymphocytes, let alone chemotherapy.39 The decreasing number of lymphocytes predicts impairing immune defense. Our results suggest that elderly patients with lymphopenia are extremely vulnerable to mixed infections. Lymphocyte counts are informative to predict the possibility of co-infection in the elderly patients with IPA.
Our study has certain drawbacks. Data were generated from one tertiary hospital from Southern China. The interpretation of the results to the general elderly population needs cautious. The retrospective nature is not able to establish a causal relationship between co-infection and mortality or lymphopenia and co-infection. Molecular methods are recommended for the diagnosis of IFD since 2019,40 however, most of the patients (78/97) included in our study were diagnosed with IFD before 2019. Among the rest of the 19 patients, only one received DNA sequencing in blood sample. No mold was detected. Therefore, molecular methods are not included regularly in the diagnostic criteria in the current study.
Conclusion
IPA is a fatal disease in the elderly population. Co-infection is an important contributor to mortality, and most of them are caused by Gram-negative bacteria. Complicating with lymphopenia increases the risk of co-infection in the elderly and needs close monitoring.
Abbreviations
BALF, bronchoalveolar lavage fluid; BMI, body mass index; CI, confidential interval; CKD, chronic kidney disease; CNS, coagulase negative staphylococci; COPD, chronic obstructive pulmonary disease; CTD, connective tissue disease; DM, diabetes mellitus; GC, glucocorticoid; GM, galactomannan; HSCT, high-resolution computed tomography; ICD-10, International Classification of Diseases; ICU, intensive care unit; IFD, invasive fungal disease; IPA, invasive pulmonary aspergillosis; IQR, interquartile range; MDR, multidrug resistance; MRSA, methicillin-resistant Staphylococcus aureus; OR, odds ratio; PDR, pandrug resistance; SD, standard deviation.
Data Sharing Statement
The datasets generated and analyzed in the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethics committee of the First Affiliated Hospital of Sun Yat-sen University approved the research (Approval number: 2,019,422), waiving written informed consent for deidentified patient data.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. M. Lao, K. Zhang and M. Zhang contributed equally to this work.
Funding
This project was supported by a grant from the National Natural Science Foundation of China (81701367).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Ledoux P, Guffroy B, Nivoix Y, et al. Invasive Pulmonary aspergillosis. Semin Respir Crit Care Med. 2020;41(1):80–98. doi:10.1055/s-0039-3401990
2. Kousha M, Tadi R, Soubani A. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011;20(121):156–174. doi:10.1183/09059180.00001011
3. Perfect J, Cox G, Lee J, et al. The impact of culture isolation of Aspergillus species: a hospital-based survey of aspergillosis. Clin Infect Dis. 2001;33(11):1824–1833. doi:10.1086/323900
4. Daniel J, Chun H. Mechanisms of dysfunction in senescent pulmonary endothelium. J Gerontol a Biol Sci Med Sci. 2012;67(3):236–241. doi:10.1093/gerona/glr248
5. Webster R. Immunity to influenza in the elderly. Vaccine. 2000;18(16):1686–1689. doi:10.1016/s0264-410x(99)00507-1
6. Peng L, Xu Z, Huo Z, et al. New insights into the clinical characteristics and prognostic factors of pulmonary fungal infections from a retrospective study in Southwestern China. Infect Drug Resist. 2018;11:307–315. doi:10.2147/IDR.S157030
7. Lao M, Zhan Z, Su F, et al. Invasive mycoses in patients with connective tissue disease from Southern China: clinical features and associated factors. Arthritis Res Ther. 2019;21(1):71. doi:10.1186/s13075-019-1851-9
8. Gong Y, Li C, Wang C, et al. Epidemiology and mortality-associated factors of invasive fungal disease in elderly patients: a 20-year retrospective study from Southern China. Infect Drug Resist. 2020;13:711–723. doi:10.2147/IDR.S242187
9. Pauw B, Walsh T, Donnelly J, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008;46(12):1813–1821. doi:10.1086/588660
10. Magiorakos A, Srinivasan A, Carey R, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
11. Germán P, Fernández-Urrusuno R, María J, et al. Long-term impact of an educational antimicrobial stewardship programme in primary care on infections caused by extended-spectrum β-lactamase-producing Escherichia coli in the community: an interrupted time-series analysis. Lancet Infect Dis. 2020;20(2):199–207. doi:10.1016/S1473-3099(19)30573-0
12. National Cancer Institute. Common terminology criteria for adverse events version 3.0. 2003. Available from: https://ctepcancergov/protocoldevelopment/electronic_applications/docs/ctcaev3pdf.
13. Zhang Z, Shen T. Diagnosis and Treatment of Blood Diseases.
14. Dib R, Khalil M, Fares J, et al. Invasive pulmonary aspergillosis: comparative analysis in cancer patients with underlying haematologic malignancies versus solid tumours. J Hosp Infect. 2020;104(3):358–364. doi:10.1016/j.jhin.2019.09.020
15. Stevens D, Melikian G. Aspergillosis in the ‘nonimmunocompromised’ host. Immunol Invest. 2011;40(7–8):751–766. doi:10.3109/08820139.2011.614307
16. Patterson T, Thompson G
17. Kosmidis C, Denning D. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015;70(3):270–277. doi:10.1136/thoraxjnl-2014-206291
18. Bartolome C, Claudia C, Jose M, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
19. Emanuele A, Shilpa B, David W, et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776–786. doi:10.1016/S0140-6736(16)30175-1
20. Amundson D, Djurkovic S, Matwiyoff G. The obesity paradox. Crit Care Clin. 2010;26(4):583–596. doi:10.1016/j.ccc.2010.06.004
21. Zafrir B, Adir Y, Shehadeh W, et al. The association between obesity, mortality and filling pressures in pulmonary hypertension patients; the “obesity paradox”. Respir Med. 2013;107(1):139–146. doi:10.1016/j.rmed.2012.10.019
22. Carnethon M, De Chavez P, Biggs M, et al. Association of weight status with mortality in adults with incident diabetes. JAMA. 2012;308(6):581–590. doi:10.1001/jama.2012.9282
23. Bottai M, Pistelli F, Di Pede F, et al. Longitudinal changes of body mass index, spirometry and diffusion in a general population. Eur Respir J. 2002;20(3):665–673. doi:10.1183/09031936.02.01282001
24. Franssen F, O’Donnell D, Goossens G, et al. Obesity and the lung: 5. Obesity and COPD. Thorax. 2008;63(12):1110–1117. doi:10.1136/thx.2007.086827
25. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
26. Kim S, Yoon Y, Kim M, et al. Risk factors for and clinical implications of mixed Candida/bacterial bloodstream infections. Clin Microbiol Infect. 2013;19(1):62–68. doi:10.1111/j.1469-0691.2012.03906.x
27. Abi‐Said D, Anaissie E, Uzun O, et al. The epidemiology of hematogenous candidiasis caused by different Candida species. Clin Infect Dis. 1997;24(6):1122–1128. doi:10.1086/513663
28. Dyess D, Garrison R, Fry D. Candida sepsis. Implications of polymicrobial blood-borne infection. Arch Surg. 1985;120(3):345–348. doi:10.1001/archsurg.1985.01390270083014
29. Leclair L, Hogan D. Mixed bacterial-fungal infections in the CF respiratory tract. Med Mycol. 2010;48(Suppl 1):S125–S132. doi:10.3109/13693786.2010.521522
30. Reece E, Segurado R, Jackson A, et al. Co-colonisation with Aspergillus fumigatus and Pseudomonas aeruginosa is associated with poorer health in cystic fibrosis patients: an Irish registry analysis. BMC Pulm Med. 2017;17(1):70. doi:10.1186/s12890-017-0416-4
31. Ho J, Tambyah P, Paterson D. Multiresistant gram-negative infections: a global perspective. Curr Opin Infect Dis. 2010;23(6):546–553. doi:10.1097/QCO.0b013e32833f0d3e
32. Barberán J, García-Pérez FJ, Villena V, et al. Development of Aspergillosis in a cohort of non-neutropenic, non-transplant patients colonised by Aspergillus spp. BMC Infect Dis. 2017;17:34. doi:10.1186/s12879-016-2143-5
33. Delsuc C, Cottereau A, Frealle E, et al. Putative invasive pulmonary aspergillosis in critically ill patients with chronic obstructive pulmonary disease: a matched cohort study. Crit Care. 2015;19:421. doi:10.1186/s13054-015-1140-1
34. Bueno V, Sant’Anna O, Lord J. Ageing and myeloid-derived suppressor cells: possible involvement in immunosenescence and age-related disease. Age (Dordr). 2014;36(6):9729. doi:10.1007/s11357-014-9729-x
35. Sharma R, Kapila R, Haq M, et al. Age-associated aberrations in mouse cellular and humoral immune responses. Aging Clin Exp Res. 2014;26(4):353–362. doi:10.1007/s40520-013-0190-y
36. Wüthrich M, George SD
37. Moro-García M, Alonso-Arias R, López-Larrea C. Molecular mechanisms involved in the aging of the T-cell immune response. Curr Genomics. 2012;13(8):589–602. doi:10.2174/138920212803759749
38. Chou J, Effros R. T cell replicative senescence in human aging. Curr Pharm Des. 2013;19(9):1680–1698. doi:10.2174/138161213805219711
39. Renata K, Elżbieta M, Wojciech K. The etiology of lower respiratory tract infections in people with diabetes. Pneumonol Alergol Pol. 2015;83(5):401–408. doi:10.5603/PiAP.2015.0065
40. Donnelly J, Sharon C, Carol K, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2019:ciz1008. doi:10.1093/cid/ciz1008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.