")
Back to Journals » Patient Preference and Adherence » Volume 10
Clinical factors affecting quality of life of patients with asthma
Authors Uchmanowicz B, Panaszek B, Uchmanowicz I , Rosinczuk J
Received 23 December 2015
Accepted for publication 23 February 2016
Published 19 April 2016 Volume 2016:10 Pages 579—589
DOI https://doi.org/10.2147/PPA.S103043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Bartosz Uchmanowicz,1 Bernard Panaszek,2 Izabella Uchmanowicz,1 Joanna Rosińczuk3
1Division of Nursing in Internal Medicine Procedures, Department of Clinical Nursing, Wroclaw Medical University, Wroclaw, Poland; 2Department and Clinic of Internal Diseases, Geriatrics and Allergology, Wroclaw Medical University, Wroclaw, Poland; 3Department of Nervous System Diseases, Department of Clinical Nursing, Wroclaw Medical University, Wroclaw, Poland
Background: In recent years, there has been increased interest in the subjective quality of life (QoL) of patients with bronchial asthma. QoL is a significant indicator guiding the efforts of professionals caring for patients, especially chronically ill ones. The identification of factors affecting the QoL reported by patients, despite their existing condition, is important and useful to provide multidisciplinary care for these patients.
Aim: To investigate the clinical factors affecting asthma patients’ QoL.
Methods: The study comprised 100 patients (73 female, 27 male) aged 18–84 years (mean age was 45.7) treated in the Allergy Clinic of the Wroclaw Medical University Department and Clinic of Internal Diseases, Geriatrics and Allergology. All asthma patients meeting the inclusion criteria were invited to participate. Data on sociodemographic and clinical variables were collected. In this study, we used medical record analysis and two questionnaires: the Asthma Quality of Life Questionnaire (AQLQ) to assess the QoL of patients with asthma and the Asthma Control Test to measure asthma control.
Results: Active smokers were shown to have a significantly lower QoL in the “Symptoms” domain than nonsmokers (P=0.006). QoL was also demonstrated to decrease significantly as the frequency of asthma exacerbations increased (R=−0.231, P=0.022). QoL in the domain “Activity limitation” was shown to increase significantly along with the number of years of smoking (R=0.404; P=0.004). Time from onset and the dominant symptom of asthma significantly negatively affected QoL in the “Activity limitation” domain of the AQLQ (R=−0.316, P=0.001; P=0.029, respectively). QoL scores in the “Emotional function” and “Environmental stimuli” subscale of the AQLQ decreased significantly as time from onset increased (R=−0.200, P=0.046; R=−0.328, P=0.001, respectively).
Conclusion: Patients exhibiting better symptom control have higher QoL scores. Asthma patients’ QoL decreases as time from onset increases. A lower QoL is reported by patients who visit allergy clinics more often, and those often hospitalized due to asthma. Smoking also contributes to a lower QoL in asthma patients.
Keywords: clinical factors, bronchial asthma, quality of life
Introduction
The prevalence of bronchial asthma makes it a global public health issue. Estimates put the worldwide number of asthma patients at ~300 million, and the number of deaths at ~250,000 per year.1 Due to the chronic nature of asthma, the primary focus of treatment is symptom management, aiming to achieve the highest degree of control possible.2 Recent years have shown significant developments in research on health-related quality of life (HRQoL). This is a consequence of adopting the “holistic” medicine model, which, contrary to the “biotechnical” model, assumes a comprehensive approach to the patient. Many clinical studies on chronic illness outcomes depart from reporting only the medical measures of health and adopt a multifaceted perspective, paying special attention to all QoL aspects, which are related to the patient’s social status and psychophysical condition. The World Health Organization defines QoL as “an individual’s subjective view of their life situation in the context of their culture, values, goals, expectations, standards, and interests”. It is a concept involving a comprehensive perspective on the human being in terms of physical health, psychological condition, sense of autonomy, social relationships, and personal beliefs, also considering the characteristics of the individual’s living environment.3–6 Changes in HRQoL resulting from illness and treatment can be either positive or negative.3–6
The objective evaluation of QoL is based on objective variables that can be assessed by the researcher (eg, physical and psychological health, test results, symptoms, diagnoses). The subjective evaluation is based on objective and subjective variables assessed by the patients themselves, and filtered through their subjective views and experiences (their knowledge and beliefs regarding their illness, their fitness and functioning, as well as their emotional attitude toward the illness and its treatment).7 The originators of the holistic approach to medicine mainly intended this approach to yield better treatment outcomes8 in chronic diseases, including asthma. However, the aims of holistic care should also include engaging the patient in the therapeutic process.9 The results of studies performed to date, using both generic and specific questionnaires, enabled the identification of numerous factors that may affect HRQoL in asthma patients. These include the patient’s demographic, clinical, and personality characteristics. The most important clinical parameter affecting the QoL of patients with bronchial asthma is disease severity, defined both in terms of objective spirometry results and in terms of other variables, for example, the frequencies of unscheduled clinic visits and of hospitalizations due to exacerbations.9 Therefore, the purpose of the study was to investigate the clinical factors affecting asthma patients’ QoL.
Study design
We performed a descriptive correlation study, which was conducted from September 2014 until January 2015. Data on sociodemographic and clinical variables, asthma control, and QoL were collected. Patients were required to give written informed consent before inclusion in the study. All asthma patients meeting the inclusion criteria were invited to participate. Inclusion criteria were as follows: 1) age: 18 years or older; 2) a diagnosis of bronchial asthma, made at least 6 months before the study, according to the Global Initiative for Asthma 2012 criteria; 3) informed consent expressed in writing. Exclusion criteria were as follows: 1) lack of consent; 2) psychological disorders; 3) other disorders preventing survey completion.
The study protocol was approved by the Bioethics Committee of the Wrocław Medical University (approval number 40/2014).
Materials and methods
The study comprised 100 patients (73 females, 27 males) aged 18–84 years (mean age: 45.7) treated in the Allergy Clinic of the Wrocław Medical University Department and Clinic of Internal Diseases, Geriatrics and Allergology in Wrocław, Poland; and in the Allergy Clinic at the “Kosmonautów” nonpublic health center in Wrocław, Poland.
The study incorporated the following methods and instruments: 1) medical record analysis and questionnaires: the Asthma Quality of Life Questionnaire (AQLQ) and 2) the Asthma Control Test (ACT). All participants received surveys and an information sheet stating that participation was voluntary and completely anonymous. The surveys were completed in the researcher’s presence.
All patients received the following questionnaires.
Adult AQLQ
An instrument comprising 32 items for adult asthma patients. It aims to identify the areas of functioning that are impaired by asthma in adult patients. The survey can be administered by a researcher or self-administered by the patient. It measures four domains: “Activity limitation” (eleven items), “Emotional function” (five items), “Exposure to environmental stimuli” (four items), and “Symptoms” (12 items). The patients describe their experience with the condition in the previous 2 weeks, using a 7-point scale (1= severely impaired, 7= not impaired at all). The higher the score, the better the QoL. Cultural adaptation and linguistic validation of AQLQ questionnaire in Polish have been done by the MAPI Research Institute.10,11
ACT
ACT comprises five questions regarding the frequency of dyspnea, waking due to the symptoms, the need for rescue medication, and control of the condition as perceived by the patient. The maximum score is 25 and indicates perfect control. Scores at 20–24 points indicate well, but not fully controlled asthma, while scores <20 points indicate uncontrolled asthma.11,12 The first four questions of the questionnaire relate to the symptoms of the disease. They concern limitation of daily activity, dyspnea, nocturnal symptoms, and the utilization of rescue medications. The fifth question refers to the patient’s self-assessment of the degree of asthma control in the past 4 weeks. The patient determines the degree of control as complete (five points), good (four points), moderate (three points), poor (two points), or states that in the recent 4 weeks the disease has not been controlled (one point). Cultural adaptation and linguistic validation of ACT questionnaire in Polish have been done by the MAPI Research Institute.11,12
Statistical analysis
Statistical analysis for quantitative characteristics (measurable variables) involved the calculation of basic statistics: mean, standard deviations, medians, and extreme values – minimum and maximum. The normality of quantitative variable distribution was verified using the Shapiro–Wilk test at a significance level of P=0.05.
The significance of differences between quantitative variables with normal distributions in two groups (sex) was verified using Student’s t-test for independent variables. If the distribution of a given variable significantly differed from normal or differed by variance, the nonparametric Mann–Whitney U-test was used. Hypotheses on equality of means in more than two groups (education or professional activity) were verified using either analysis of variance (if variable distributions in all groups were not significantly different from normal) or the nonparametric Kruskal–Wallis test (for skewed distributions).
The strength of correlations between two quantitative variables was determined using Spearman’s or Pearson’s linear correlation coefficient (R or r). When correlation coefficients r were significantly different from zero, regression analysis was performed, with linear correlation model parameter values determined for the two variables (a and b) and correlation diagrams created, illustrating the dispersion of the variables against the mathematical model. The correlation of the quantitative variable (AQLA) with several other variables was described using multiple regression analysis. For qualitative variables (nominal or categorical), numbers and percentages were calculated. The independence of qualitative variables was verified using the chi-squared test. For all statistical tests, P<0.05 was used as a statistical significance criterion.
Calculations were made using the STATISTICA 10 software and MS EXCEL spreadsheets.
Results
The study included 100 patients (73 females, 23 males) aged 18–84 years (mean age: 45.7) treated at the Allergy Clinic of the Wrocław Medical University Department and Clinic of Internal Diseases, Geriatrics and Allergology in Wrocław, Poland; and at the Allergy Clinic at the “Kosmonautów” non-public health center in Wrocław, Poland. The patients’ sociodemographic and clinical characteristics are shown in Tables 1 and 2.
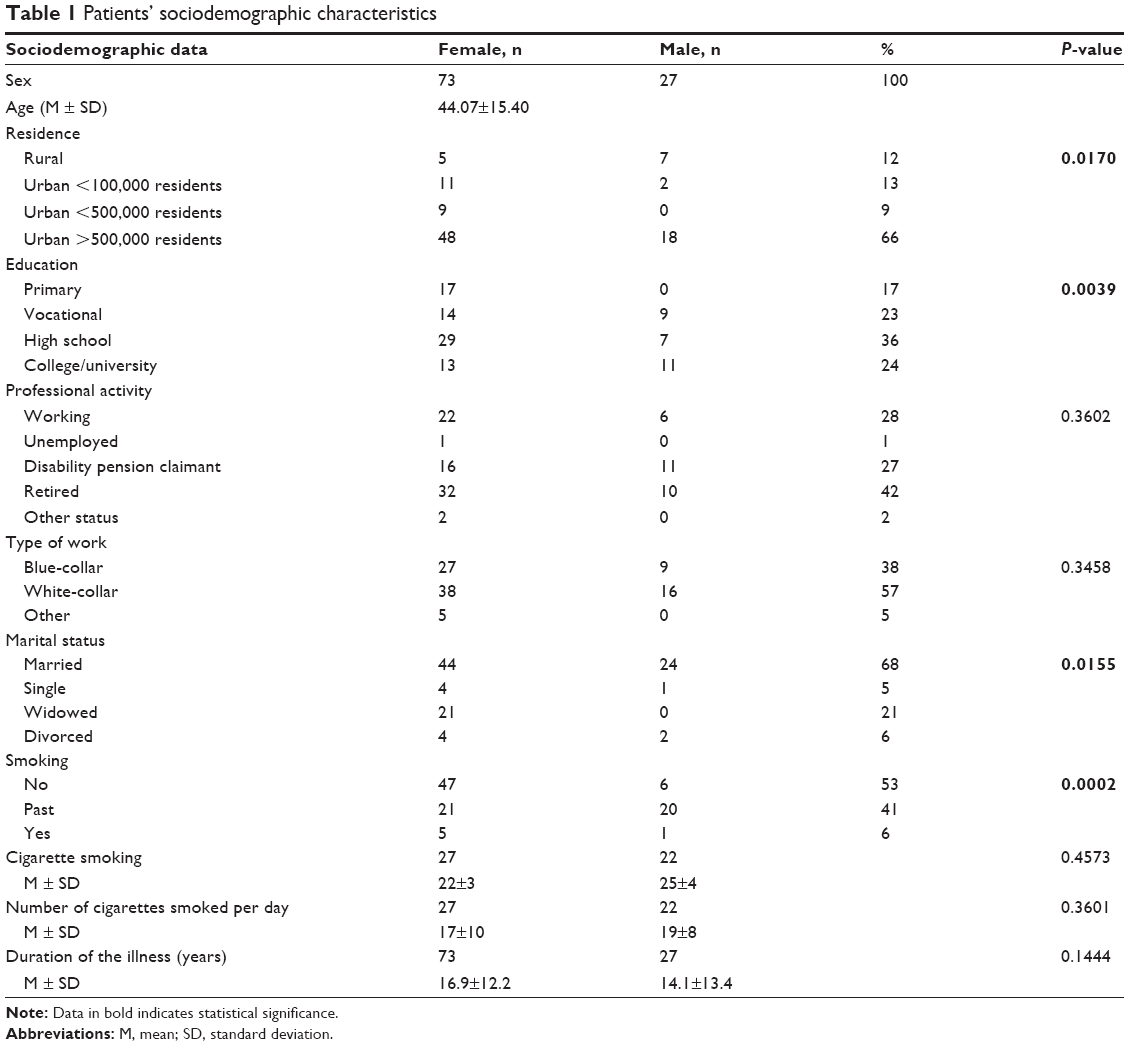 | Table 1 Patients’ sociodemographic characteristics |
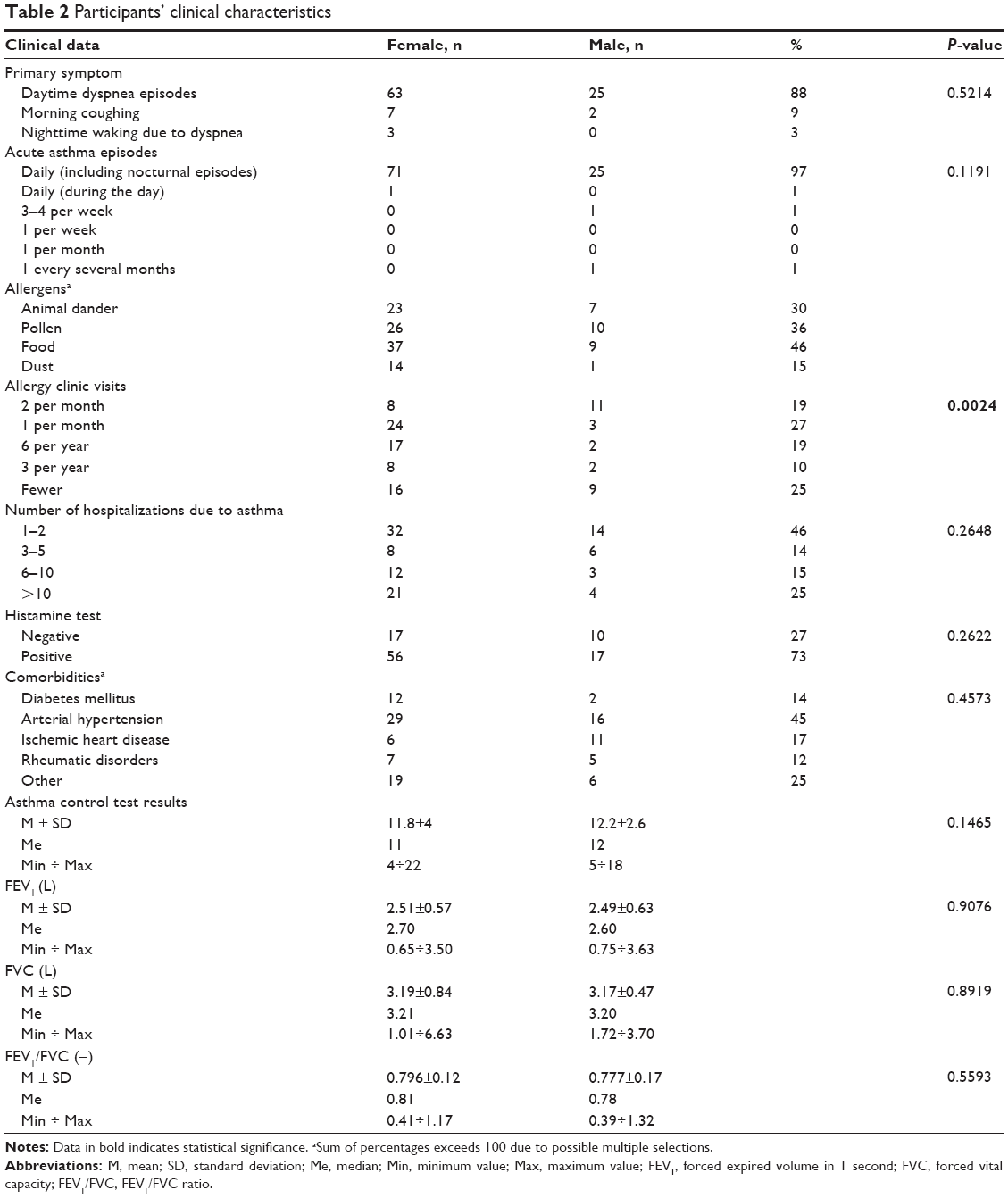 | Table 2 Participants’ clinical characteristics |
Clinical factors affecting QoL in the “Symptoms” domain of the AQLQ
Active smokers were shown to have a significantly lower QoL in the “Symptoms” domain than nonsmokers (P=0.006; Table 3). Interestingly, QoL in the domain was shown to increase significantly along with the number of years of smoking (R=0.501, P<0.001). No significant correlation was found, however, between QoL in the “Symptoms” domain of the AQLQ and the mean number of cigarettes smoked per day (R=0.075, P=0.608). Time from illness onset did not significantly affect QoL in the domain either (R=−0.122, P=0.225). In turn, the dominant symptom of asthma did significantly affect QoL in the “Symptoms” domain. Patients whose disease was mainly manifested with daytime dyspnea experienced a significantly lower QoL in the domain than those whose primary symptom was morning coughing (P=0.006; Table 3). QoL was also demonstrated to decrease significantly as the frequency of asthma exacerbations increased (R=−0.231, P=0.022; Table 3). The correlation between QoL in the “Symptoms” domain and allergies was close to statistical significance; allergic patients had a lower QoL in the domain than those with no allergies (P=0.050; Table 3). QoL in the “Symptoms” domain of the AQLQ decreased significantly as the frequency of allergy clinic visits (R=−0.323, P=0.001; Table 3) and the number of hospitalizations due to exacerbations increased (R=−0.322, P=0.001; Table 3).
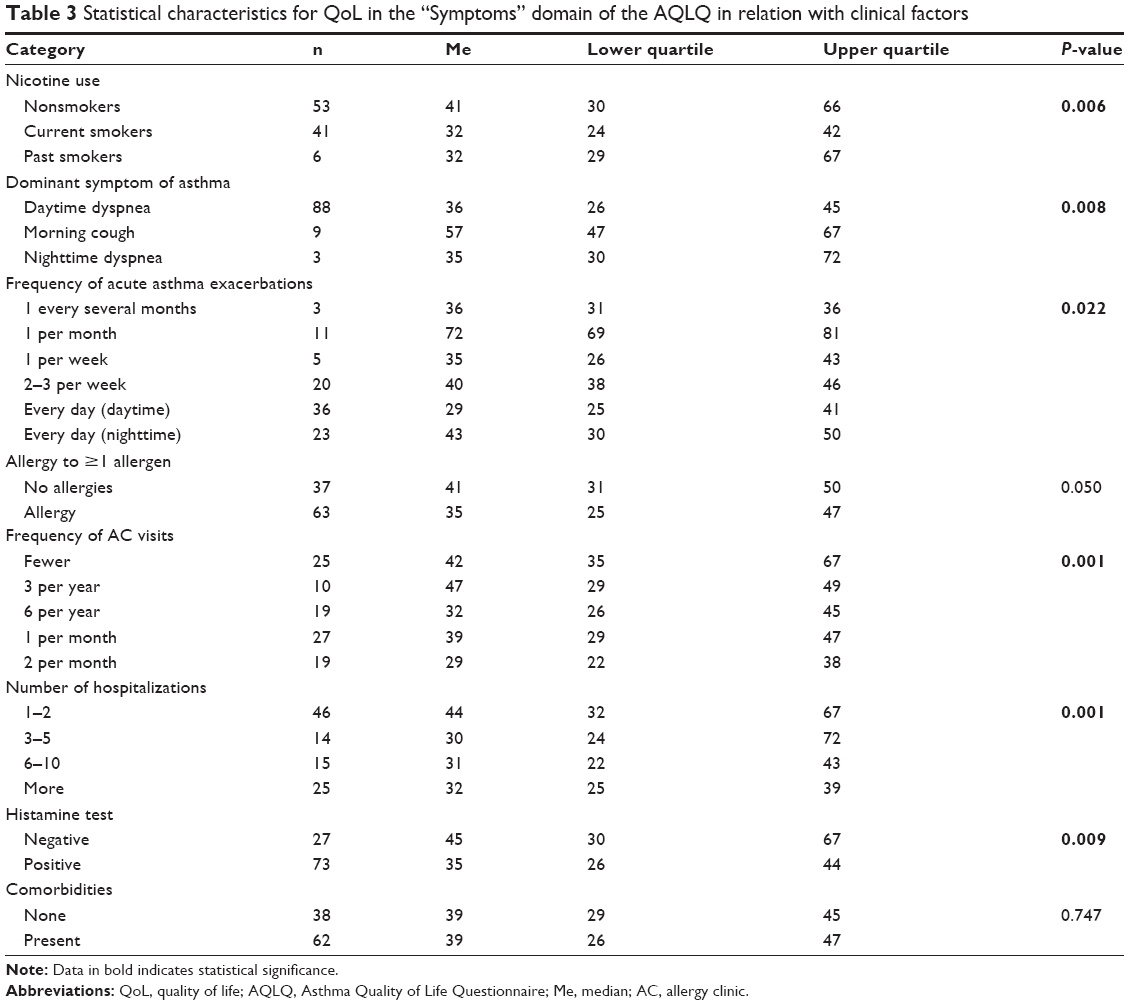 | Table 3 Statistical characteristics for QoL in the “Symptoms” domain of the AQLQ in relation with clinical factors |
Significantly higher scores in the “Symptoms” domain of the AQLQ were noted among patients whose histamine test was negative (P=0.009; Table 3). QoL in the domain also increased in proportion to ACT scores (R=0.285, P=0.004). As to comorbidities, no significant impact on QoL in the “Symptoms” domain of the AQLQ was shown (P=0.747; Table 3). Nor were any statistically significant correlations found between QoL in the domain and spirometry parameters: forced expired volume in 1 second (FEV1) (R=0.163, P=0.105), forced vital capacity (FVC) (R=0.017, P=0.863), and FEV1/FVC (R=0.131, P=0.193).
Clinical factors affecting QoL in the “Activity limitation” domain of the AQLQ
Current and past smokers were not significantly different from nonsmokers in terms of the “Activity limitation” QoL subscale score (P=0.176; Table 4). Nor was any significant correlation found between QoL in this domain of the AQLQ and the mean number of cigarettes smoked per day (R=−0.011, P=0.938). QoL in the domain was, however, shown to increase significantly along with the number of years of smoking (R=0.404, P=0.004). Time from onset significantly negatively affected QoL in the “Activity limitation” domain of the AQLQ (R=−0.316, P=0.001). Another factor that significantly affected QoL in the “Activity limitation” domain was the dominant symptom of asthma. Patients whose disease was mainly manifested with daytime dyspnea experienced a significantly lower QoL in the domain than those whose primary symptom was morning coughing (P=0.029; Table 4). As to the frequency of asthma exacerbations, it did not significantly affect QoL in the “Activity limitation” domain (R=−0.175, P=0.086; Table 4). However, a statistically significant correlation was found between QoL in the domain and allergy (to any allergen); allergic patients had a significantly lower QoL than those with no allergies (P=0.007; Table 4). QoL in the “Activity limitation” domain of the AQLQ also decreased significantly as the frequency of allergy clinic visits (R=−0.323, P=0.001; Table 4) and the number of hospitalizations due to asthma exacerbations (R=−0.340, P=0.001; Table 4) increased.
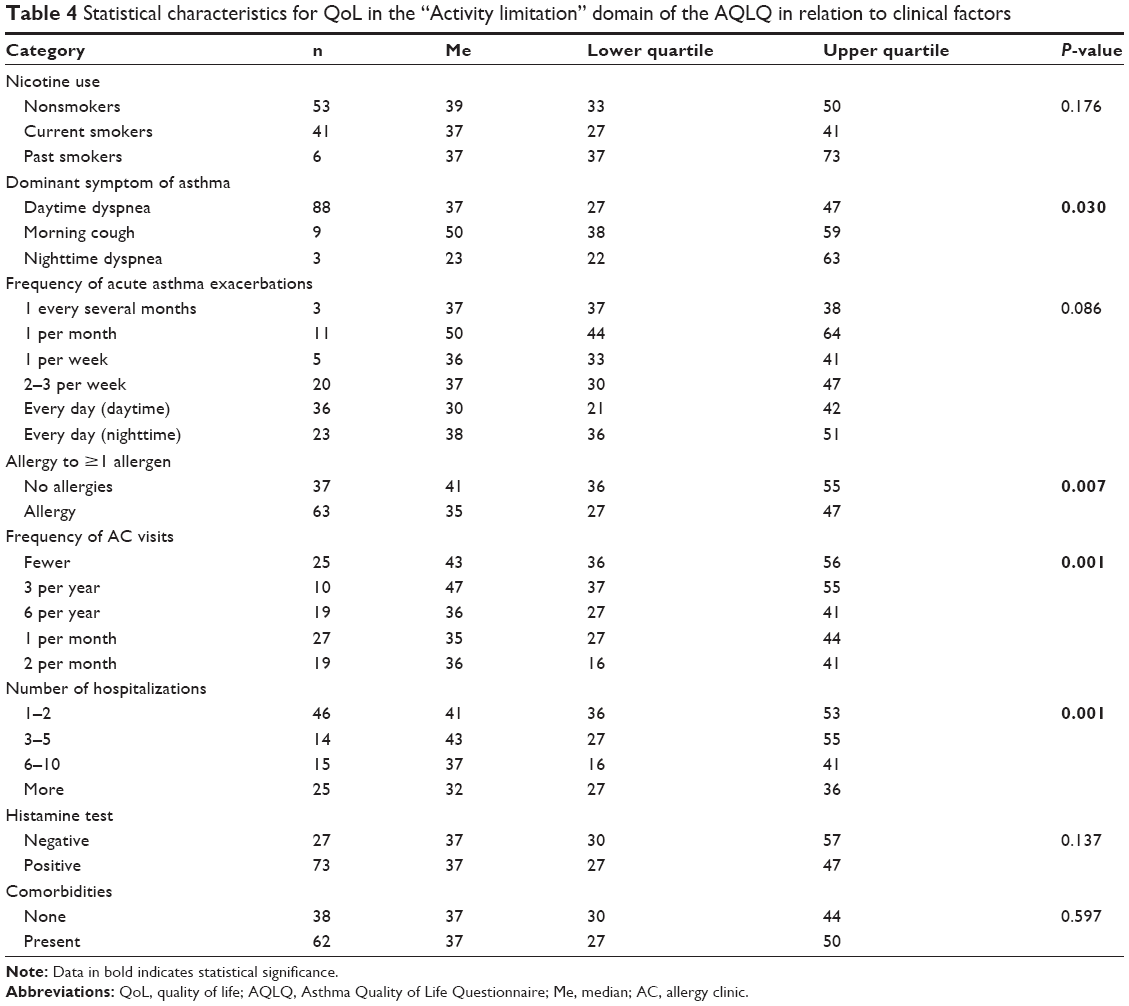 | Table 4 Statistical characteristics for QoL in the “Activity limitation” domain of the AQLQ in relation to clinical factors |
The result of the histamine challenge test had no significant impact on QoL in the “Activity limitation” domain of the AQLQ (P=0.137; Table 4). QoL in the domain did, however, increase in proportion to ACT scores (R=0.290, P=0.003). As to comorbidities, no significant impact on QoL in the “Activity limitation” domain of the AQLQ was shown (P=0.597; Table 4). Nor were any statistically significant correlations found between QoL in the domain and spirometry parameters: FEV1 (R=0.137, P=0.175), FVC (R=0.092, P=0.365), and FEV1/FVC (R=0.062, P=0.542).
Clinical factors affecting QoL in the “Emotional function” domain of the AQLQ
Current and past smokers were not significantly different from nonsmokers in terms of their “Emotional function” QoL subscale score (P=0.062; Table 5). Nor was any significant correlation found between QoL in this domain of the AQLQ and the mean number of cigarettes smoked per day (R=0.089, P=0.545). QoL in the domain was, however, shown to increase significantly along with the number of years of smoking (R=0.299, P=0.037). QoL scores in the “Emotional function” subscale of the AQLQ decreased significantly as time from onset increased (R=−0.200, P=0.046). No significant correlation with QoL in this domain was found for the dominant symptom (P=0.108; Table 5). QoL in the domain did, however, decrease significantly as the frequency of exacerbations increased (R=−0.247, P=0.014; Table 5). No significant correlation was shown between QoL in the “Emotional function” domain and allergies (P=0.055; Table 5) or the number of hospitalizations due to asthma exacerbations (R=−0.161, P=0.110; Table 5). QoL in the AQLQ “Emotional function” domain did, however, decrease significantly as the frequency of allergy clinic visits increased (R=−0.203, P=0.043; Table 5).
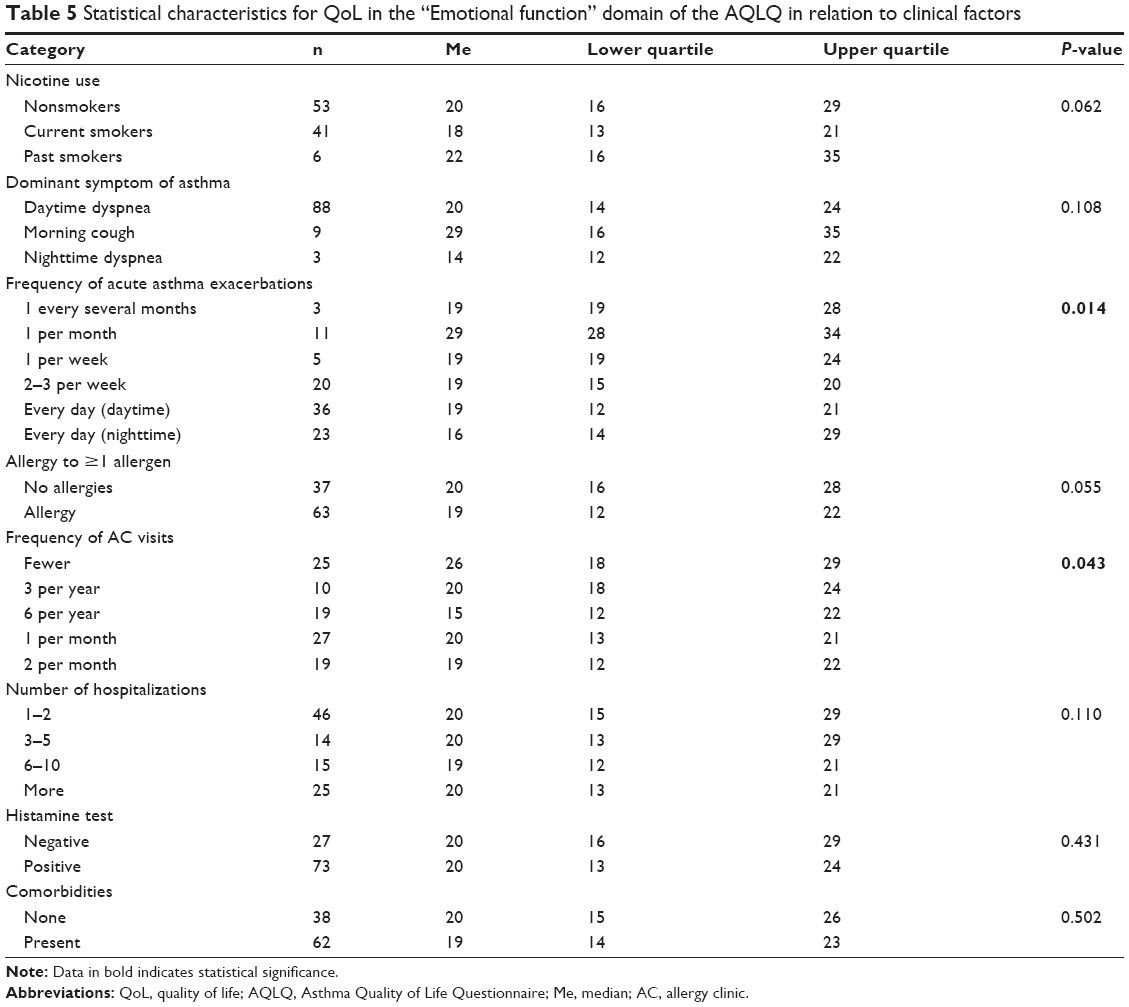 | Table 5 Statistical characteristics for QoL in the “Emotional function” domain of the AQLQ in relation to clinical factors |
The results of the histamine challenge test (P=0.431; Table 5), ACT scores (R=0.185, P=0.065), and comorbidities (P=0.502; Table 5) had no significant impact on the “Emotional function” domain of the AQLQ. Nor were any statistically significant correlations found between QoL in the domain and spirometry parameters: FEV1 (R=0.181, P=0.072), FVC (R=0.194, P=0.053), and FEV1/FVC (R=0.039, P=0.697).
Clinical factors affecting QoL in the “Environmental stimuli” domain of the AQLQ
Current and past smokers were not significantly different from nonsmokers in terms of the “Environmental stimuli” QoL subscale score (P=0.645; Table 6). Similarly, no significant correlations were found between QoL in the domain and the number of years of smoking (R=0.183, P=0.207) or the mean number of cigarettes smoked per day (R=0.053, P=0.717). However, QoL scores in the “Environmental stimuli” subscale of the AQLQ decreased significantly as time from onset increased (R=−0.328, P=0.001). The dominant asthma symptom (P=0.558; Table 6) or the frequency of asthma exacerbations (R=0.076, P=0.460; Table 6) did not have any significant impact on QoL in the domain. However, a statistically significant correlation was found between QoL in the “Environmental stimuli” domain and allergy (to any allergen); allergic patients had a significantly lower QoL in the domain than those with no allergies (P=0.001; Table 6). QoL in this AQLQ domain also decreased significantly as the frequency of allergy clinic visits increased (R=−0.206, P=0.040; Table 6). With regard to the number of hospitalizations due to asthma exacerbations, this did not significantly affect QoL in the “Environmental stimuli” domain (R=−0.158, P=0.116; Table 6).
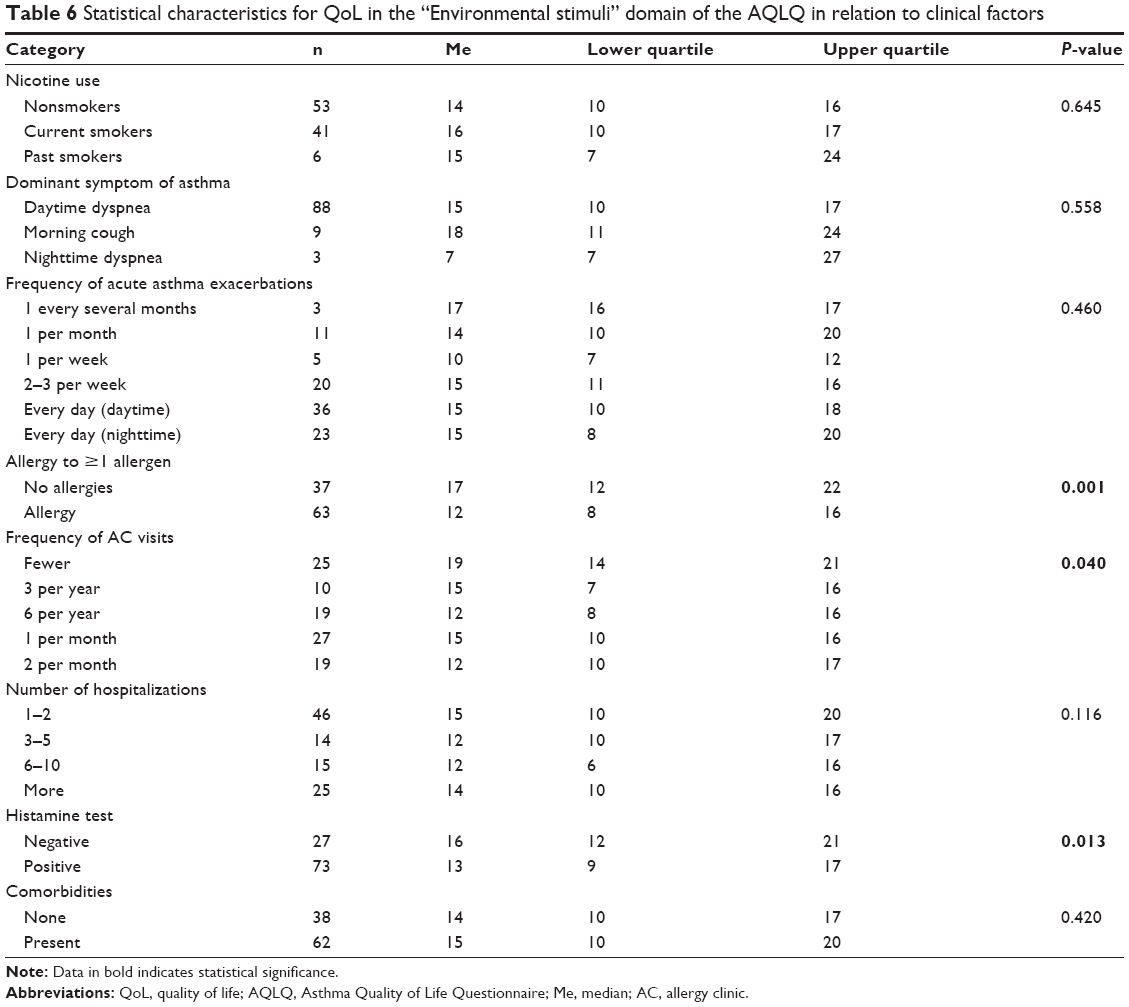 | Table 6 Statistical characteristics for QoL in the “Environmental stimuli” domain of the AQLQ in relation to clinical factors |
Significantly higher QoL scores in the “Environmental stimuli” domain of the AQLQ were noted among patients whose histamine test was negative (P=0.013; Table 6). QoL in the domain also increased in proportion to the ACT scores (R=0.238, P=0.017).
With regard to comorbidities, no significant impact on QoL in the “Environmental stimuli” domain of the AQLQ (P=0.420) was shown (Table 6).
Discussion
QoL is a significant indicator guiding the efforts of professionals caring for patients, especially chronically ill ones. The identification and confirmation of factors affecting the QoL reported by patients, despite their existing condition, are important and useful for health science and for medical professionals providing day-to-day care and treatment for these patients.
This paper attempted to answer questions about the relationship between clinical factors and the QoL of asthma patients. It presented the clinical determinants of subjective QoL. The results of studies performed to date, using both generic and specific questionnaires, enabled the identification of numerous factors that may affect HRQoL in asthma patients. The authors’ study identified a number of determinants affecting the QoL of patients with bronchial asthma.
The discussion of particular AQLQ domains focused on clinical variables, such as asthma control level, dominant symptom, acute asthma attack frequency, allergies, allergy clinic visit frequency, hospitalization frequency, and comorbidities, all of which may affect QoL in asthma patients. In the “Symptoms” domain, smoking was a factor lowering the QoL. Other researchers also reported decreases in QoL related to smoking. Tan et al,13 in their study of asthma patients using AQLQ, confirmed the negative impact of smoking on QoL in the “Symptoms” domain. Results showing a lower QoL due to active smoking are consistent with studies on symptom aggravation resulting from smoking.14 Moreover, studies by Lange et al15 and Jang et al16 indicate impaired pulmonary function in actively smoking asthma patients. This could further reduce the QoL of patients who smoke.
Importantly, results showed that daytime dyspnea also affected QoL in the “Symptoms” domain of the AQLQ. Patients whose dominant symptom was daytime dyspnea had a significantly lower QoL. QoL was also demonstrated to decrease significantly as the frequency of asthma exacerbations, the frequency of allergy clinic visits, and the number of hospitalizations due to exacerbations increased. Better asthma control (as measured by the ACT) contributed to higher QoL scores. The issue of proper asthma control is extremely important. Due to the chronic nature of asthma, the primary focus of treatment is symptom management, aimed at achieving the highest possible degree of control. Apart from objective clinical parameters (spirometry results), commonly applied asthma control indicators also include semiobjective (the frequencies of unscheduled clinic visits and of hospitalizations due to exacerbations, additional doses of antiasthmatic drugs) and subjective variables (eg, the asthma control score in the ACT).11
The results obtained by Bateman et al17 indicate that despite modern treatments, not all patients can achieve full control of asthma symptoms. Therefore, it can be suspected that poorer symptom control adversely affects asthma patients’ QoL. The results of numerous international studies also confirm the fact that asthma control remains unsatisfactory, despite the treatment standards introduced.18–20 In the current study, as many as 62% of patients were found to have unsatisfactory control of symptoms. Polish and European studies point to the issue of inadequate asthma control, with as many as 50% of patients experiencing sudden asthma attacks. The American aspirin induced asthma study also found insufficient control, with 30% of patients reporting nighttime symptoms, and nearly half experiencing activity limitations.20 Worse asthma control entails a lower HRQoL.21
Factors negatively affecting QoL in the “Activity limitation” domain included longer time from illness onset, daytime dyspnea, more frequent allergy clinic visits, and more hospitalizations; while better asthma control improved the QoL. Asthma is a chronic disease with a variable course, requiring constant treatment; and thus, it affects all aspects of an individual’s activity. QoL seems to deteriorate especially when symptoms are not well-controlled. As reported by Chełmińska et al,22 QoL scoring in patients with well- and poorly-controlled asthma omits several aspects important to the patients. The authors state that aspects such as the maintenance of full activity, the adverse effects of chronic treatment, or the need for emergency care are disregarded. QoL in this domain deteriorated in proportion to time from onset, frequency of asthma attacks, and frequency of allergy clinic visits.
As in the previously discussed AQLQ subscales, the QoL decreased significantly as time from onset and allergy clinic visit frequency increased. Once again, in this subscale, QoL increased with ACT scores. These findings were confirmed in the study done by Martínez-Moragón et al where they stated that good asthma control affects QoL positively in this group of patients.23 Thus, asthma control proved to be a significant determinant of better QoL scores. In summary, it can be said that the most important clinical parameter affecting the QoL of patients with bronchial asthma is disease severity, defined both in terms of objective spirometry results and of quasiobjective variables, eg, the frequencies of unscheduled clinic visits and of hospitalizations due to exacerbations. To date, the results of all studies using the AQLQ and St George’s Respiratory Questionnaire show unambiguously that QoL is inversely correlated with asthma severity and positively correlated with the degree of asthma control.24,25 This correlation was confirmed in the current study. Patients with higher frequencies of hospitalizations and clinic visits scored their subjective QoL lower. Simultaneously, poor control of asthma is correlated with a higher severity of the disease and a lower HRQoL.
The present study demonstrates that the proper therapeutic interventions and patient education are key to increasing asthma patients’ QoL, as these factors may promote better compliance with treatment, contributing to better objective health.
Conclusion
In conclusion, only some factors have an effect on patients’ QOL. Patients exhibiting better symptom control have higher QoL scores. Asthma patients’ QoL decreases as time from onset increases. A lower QoL is reported by patients who visit allergy clinics more often and those often hospitalized due to asthma. Smoking also contributes to a lower QoL in asthma patients.
Disclosure
The authors report no conflicts of interest in this work.
References
Masoli M, Fabian D, Holt S, Beasley R; Global Initiative for Asthma (GINA) Program. The global burden of asthma: executive summary of the GINA Dissemination Committee Report. Allergy. 2004;59(5):469–478. | ||
Gajewski P. Światowa strategia rozpoznawania, leczenia i prewencji astmy. Aktualizacja 2006 [Global Strategy for Asthma Management and Prevention. Update 2006]. Medycyna Praktyczna: Kraków; 2007. | ||
The WHOQOL Group. Development of the WHOQOL: Rationale and current status. Int J Ment Health. 1994;23(3):24–56. | ||
No authors listed. The World Health Organization Quality of Life Assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403–1409. | ||
Storstein L. Lifestyle changes in cardiovascular patients – measuring their effect. In: Birdwood GF, editor. Quality of life – how it can be assessed and improved. Cardiovascular problems in everyday practice. A service to the medical profession. Basel, Switzerland: CIBA-GEIGY, Medical and Pharmaceutical Information; 1987:3–6. | ||
Ostrzyżek A. Jakość życia w chorobach przewlekłych [Quality of life in chronic diseases]. Probl Hig Epidemiol. 2008;89(4):467–470. Polish. | ||
De Walden-Gałuszko K, Majkowicz M. Jakość życia w chorobie nowotworowej. [Quality of life in cancer]. Uniwersytetu Gdańskiego (Gdańsk); 1994. | ||
Schipper H. Quality of life: principles of the clinical paradigm. J Psychosoc Oncol. 1990;8(2):171–185. | ||
Higginson IJ, Carr AJ. Measuring quality of life: Using quality of life measures in the clinical setting. BMJ. 2001;322(7297):1297–1300. | ||
Juniper EF, Guyatt GH, Ferrie PJ, Griffith LE. Measuring quality of life in asthma. Am Rev Respir Dis. 1993;147(4):832–838. | ||
Acquadro C, Conway K, Giroudet C, Mear I. Linguistic validation manual for patient-reported outcomes (PRO) instruments. Lyon, France: MAPI Research Institute; 2004. | ||
Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. | ||
Tan WC, Tan JW, Wee EW, Niti M, Ng TP. Validation of the English version of the Asthma Quality of Life Questionnaire in a multi-ethnic Asian population. Qual Life Res. 2004;13(2):551–556. | ||
Thomson NC, Chaudhuri R, Livingston E. Asthma and cigarette smoking. Eur Respir J. 2004;24(5):822–833. | ||
Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med. 1998;339(17):1194–1200. | ||
Jang AS, Park SW, Kim DJ, et al. Effects of smoking cessation on airflow obstruction and quality of life in asthmatic smokers. Allergy Asthma Immunol Res. 2010;2(4):254–259. | ||
Bateman ED, Bousquet J, Keech ML, Busse WW, Clark TJ, Pedersen SE. The correlation between asthma control and health status: the GOAL study. Eur Respir J. 2007;29(1):56–62. | ||
Rabe KF, Vermeire PA, Soriano JB, Maier WC. Clinical management of asthma in 1999: the Asthma Insights and Reality in Europe (AIRE) study. Eur Respir J. 2000;16(5):802–807. | ||
Micheletto C, Visconti M, Tognella S, Facchini FM, Dal Negro RW. Aspirin induced asthma (AIA) with nasal polyps has the highest basal LTE4 excretion: a study vs AIA without polyps, mild topic asthma, and normal controls. Eur Ann Allergy Clin Immunol. 2006;38(1):20–23. | ||
Kowalski ML, Jędrzejczak M, Cirlić M. The efficacy of bronchial asthma treatment in Poland as assessed by patients – results of AIRCEE (Asthma Insights & Reality in Central and Eastern Europe) survey. Alerg Astma Immun. 2004;9(4):187–195. | ||
Apfelbacher CJ, Hankins M, Stenner P, Frew AJ, Smith HE. Measuring asthma-specific quality of life: structured review. Allergy. 2010;66(4):437–457. | ||
Chełmińska M, Werachowska L, Niedoszytko M, et al. Jakość życia chorych na astmę dobrze i źle kontrolowaną. [Quality of life of patients with asthma which has been well and poorly controlled]. Pneumonol Alergol Pol. 2007;75(1):70–75. Polish. | ||
Martínez-Moragón E, Palop M, de Diego A, et al. Factors affecting quality of life of asthma patients in Spain: the importance of patient education. Allergol Immunopathol (Madr). 2014;42(5):476–484. | ||
Wang KY, Wu CP, Tang YY, Yang ML. Health-related quality of life in Taiwanese patients with bronchial asthma. J Formos Med Assoc. 2004;103(3):205–211. | ||
Koskela J, Kupiainen H, Kilpeläinen M, et al. Longitudinal HRQoL shows divergent trends and identifies constant decliners in asthma and COPD. Respir Med. 2014;108(3):463–471. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.