")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Clinical evaluation of dacomitinib for the treatment of metastatic non-small cell lung cancer (NSCLC): current perspectives
Authors Lavacchi D, Mazzoni F, Giaccone G
Received 6 June 2019
Accepted for publication 23 August 2019
Published 6 September 2019 Volume 2019:13 Pages 3187—3198
DOI https://doi.org/10.2147/DDDT.S194231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Georgios Panos
Video abstract presented by Daniele Lavacchi.
Views: 395
Daniele Lavacchi1, Francesca Mazzoni1, Giuseppe Giaccone1,2
1Department of Oncology, Careggi Hospital and University of Florence, Florence, Italy; 2Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC, USA
Correspondence: Giuseppe Giaccone
Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC, USA
Tel +1 202 687 7072
Email [email protected]
Abstract: Systemic treatment of advanced non-small cell lung cancer (NSCLC) has undergone remarkable changes in the last decade, with the introduction of targeted therapies and immunotherapy. The identification of activating mutations in the epidermal growth factor receptor (EGFR) gene (deletions in exon 19 [Del19] and point mutation L858R in exon 21) has been the first important step toward molecularly guided precision therapy in lung cancer. Several randomized trials comparing EGFR tyrosine kinase inhibitors (TKIs) (gefitinib, erlotinib, and afatinib) to standard chemotherapy in first-line treatment of advanced EGFR-mutant NSCLC showed significant improvement in progression-free survival (PFS) and in response rate, with lower rates of adverse events (AEs) and better symptom control. However, none of these trials showed significant improvement in overall survival (OS). Despite impressive responses with EGFR-TKI, disease invariably progresses after 9 to 13 months, due to acquired resistance. Dacomitinib is a potent, irreversible, highly selective, second-generation EGFR-TKI, which inhibits the signaling from both heterodimers and homodimers of all the members of the human epidermal growth factor receptor (HER) family. Here, we review the clinical development of dacomitinib from phase I to phase III, with particular attention to its toxicity and on its activity on T790M mutation. Then, we critically examine the results of ARCHER 1050, a study that was crucial for Food and Drug Administration (FDA) approval. ARCHER 1050 was the first randomized phase III study comparing dacomitinib with gefitinib, in first-line treatment of patients with advanced EGFR-mutated NSCLC. Dacomitinib was superior to gefitinib in terms of primary end-point (14.7 vs 9.2 months) and OS (34.1 vs 26.8 months). The incidence of diarrhea, skin rash, mucositis and, consequently, dose reductions was higher with dacomitinib, while hepatic toxicity was higher with gefitinib. Dacomitinib constitutes one of the standard first-line options in patients with advanced EGFR-mutated NSCLC.
Keywords: dacomitinib, non-small cell lung cancer, NSCLC, epidermal growth factor receptor, EGFR, pan-HER inhibitor, second-generation TKI
Introduction
Lung cancer is the leading cause of cancer-related death, with 1.6 million tumor-related deaths annually worldwide. Non-small cell lung cancer (NSCLC) accounts for nearly 85% of all newly diagnosed cases. Survival has not significantly improved in the past decades, and most patients are diagnosed at late-stage disease, when surgery is no longer feasible and consequently have poor prognosis. Cytotoxic chemotherapy developed over the past few decades has produced only modest improvements in survival in metastatic NSCLC. Undoubtedly, one of the major advancement in the treatment of NSCLC came with the discovery of specific genetic alterations driving the development and progression. Systemic treatment has recently undergone remarkable changes, first with targeted therapies and, in the last few years, with the introduction of immunotherapy with immune checkpoint inhibitors.1
The identification of activating mutations in the gene encoding the epidermal growth factor receptor (EGFR) (deletion in exon 19 [Del19] and point mutation L858R in exon 21) has been the first important step toward molecularly guided precision therapy.2,3 Several randomized trials comparing EGFR tyrosine kinase inhibitors (TKIs) (gefitinib, erlotinib, and afatinib) to standard chemotherapy in first-line treatment of advanced EGFR-mutant NSCLC showed significant improvements in progression-free survival (PFS) (9.6 to 13.1 months vs 4.6 to 6.9 months) and in response rate (50–70% vs 15–35%), with lower rates of adverse events and better symptom control. None of these trials, however, showed significant differences in overall survival (OS). Despite high and rapid tumor responses with first-line EGFR tyrosine kinase inhibitors, disease invariably progresses after 9 to 13 months of treatment, due to acquired resistance.4–11
On September 27, 2018, the Food and Drug Administration (FDA) approved dacomitinib, a second-generation EGFR-targeted TKI agent. The indication includes the first-line treatment of patients with metastatic NSCLC harboring EGFR Del19 or exon 21 L858R mutations. Dacomitinib is a potent and irreversible pan-human epidermal growth factor receptor (HER) family inhibitor.
The HER family, with its four tyrosine kinases receptors (HER1/EGFR/ErbB1, HER2/ErbB2, HER3/ErbB3, and HER4/ErbB4), is involved in several cell processes, including proliferation, differentiation, and migration. Many ligands specifically bind at least one of these receptors: EGF, TGF-α, EPG, and amphiregulin bind EGFR; BTC, HB-EGF, and EPR bind EGFR and HER4; neuregulins bind HER3 and HER4. Not having a specific ligand, HER2 acts as a dimerization partner, forming dimers with other members of the HER family.12
After ligand binding to the EGFR, the formation of both homodimers and heterodimers occurs. EGFR heterodimerization can occur with any other receptor of the HER family (ie, HER2, HER3, and HER4). Consequently, a cascade of events, that includes activation of kinase activity and autophosphorylation on multiple tyrosine residues, takes place. The kinase activity is implemented through an asymmetric dimerization particularly for L858R mutation, in which EGFR mutants predominantly play an acceptor role in the presence of wild-type (WT) EGFR or HER2. This results in the activation of multiple intracellular signaling pathways involved in promoting cell growth, protein synthesis, and cell survival. AKT, STAT 3 and 6, PI3K through Gab1, and RAS/RAF/MEK/ERK are the key protein kinases involved in these signaling cascades.13–15
Three generations of EGFR-TKIs have been developed in order to prevent the activation of HER-driven oncogenic pathway [Tables 1 and 2]. The first generation includes gefitinib and erlotinib, which target a single member of the HER family (EGFR). They inhibit EGFR tyrosine kinase by reversibly binding to the ATP-binding site. Although particularly active in inhibiting the most common EGFR mutations (Del19 and point mutation L858R in exon 21), first-generation inhibitors do not have similar efficacy for rare mutations, which are less studied due to the small size of the population within clinical trials.14
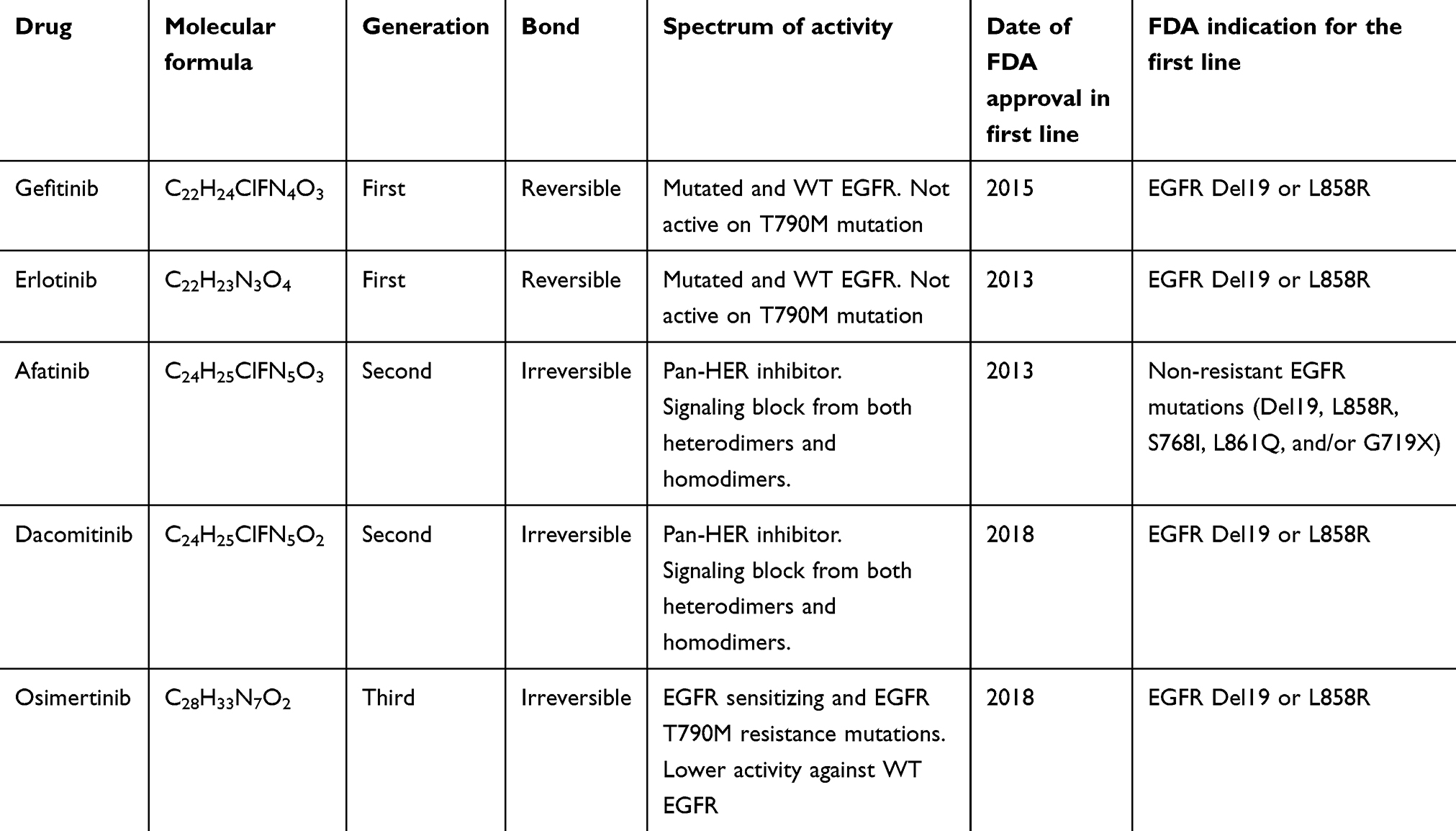 |
Table 1 EGFR-TKIs currently available for the treatment of EGFR-mutated NSCLC |
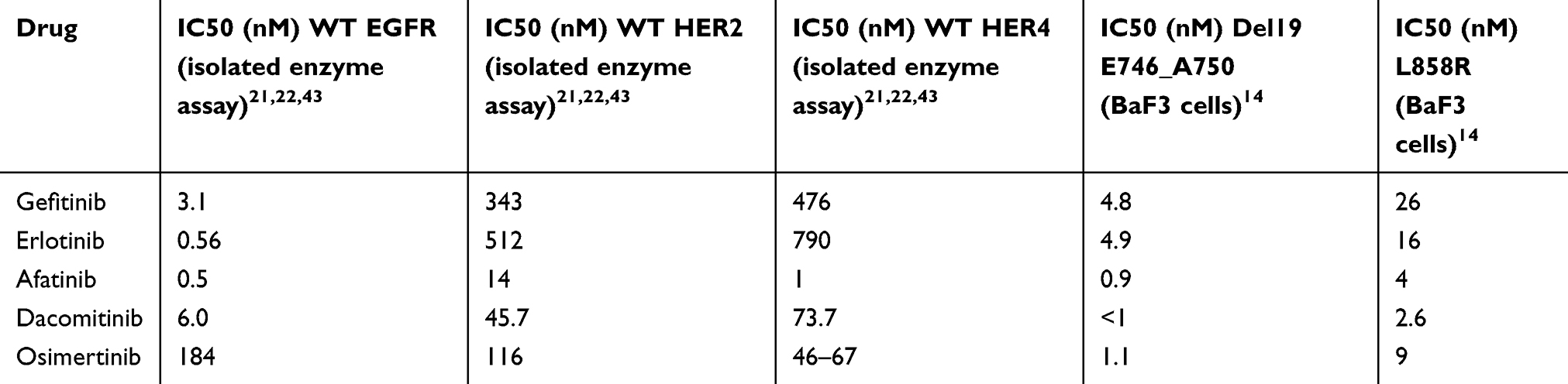 |
Table 2 IC50 values for EGFR, HER2, HER4, Del19, and L858R |
The mechanism of acquired resistance that most frequently (50–60%) occurs in patients treated with first-generation EGFR-TKIs is the development of T790M point mutation in exon 20. This mutation is due to a substitution of threonine with methionine at position 790 of the ATP-binding pocket and results in an increase of the affinity of receptors for ATP.16
Several other EGFR-dependent and EGFR-independent mechanisms of acquired resistance have been described, including other rare EGFR mutations, MET amplification, HER2 amplification, PIK3CA mutations or amplification, PTEN loss, RAS/MAPK pathway activation, BRAF mutation, IGF-1R of FGFR activation, SCLC transformation, and others.17,18
Afatinib and dacomitinib are second-generation EGFR-TKIs approved by FDA. These drugs are irreversible inhibitors forming covalent bonds with the kinase domains of EGFR and other HER family receptors. As a consequence, the signaling from both heterodimers and homodimers is blocked.12,14,19 Analyzing in vitro the activity of afatinib on Ba/F3 cells, sensitivity was high for some uncommon mutations such as G719A, E709K, Del18, K745_E746insTPVAIK, S768I, and L861Q.14 In addition, afatinib has been shown to be effective in a subset of patients harboring rare mutations (G719X, L861Q, and S768I).20
Binding an unpaired cysteine at the ATP-binding pocket site, dacomitinib strongly inhibits EGFR, ErbB2, and ErbB4, both in vitro and in xenograft models.19,21 Using cell lines with L858R/T790M mutations (H1975, H3255 GR, Ba/F3) resistant to gefitinib (IC50>10 μmol/L), dacomitinib proved to be an effective inhibitor, having IC50 0.44 μmol/L for H1975, 0.119 μmol/L for H3255 GR, and 300 nmol/L for Ba/F3. Dacomitinib was also able to inhibit the proliferation of Ba/F3 cells expressing T790M in cis to different deletions in exon 19, with IC50s between 140 and 330 nmol/L. Similar results were obtained in HCC827 Del/T790M xenograft models resistant to gefitinib. The activity of dacomitinib was also observed in cell lines (H1781 and NIH-3T3) with ErbB2 mutations (Ins G776V,C and Ins774YVMA, respectively) or amplification (Calu-3 and H1819 cell lines).22
Being an irreversible inhibitor, dacomitinib has longer pharmacodynamic effects than those observed with first-generation TKIs. Dacomitinib has also favorable pharmacokinetic properties, including high oral bioavailability (>50%), high volume of distribution (>17 L/kg), and long half-life (>12 hrs).19
Third-generation EGFR-TKIs were developed with the aim to target common EGFR mutations and T790M point mutation as primary or secondary resistance mechanism. In addition, they have a lower activity against WT EGFR. Osimertinib, which is the only drug that received FDA approval for the treatment of EGFR-mutated NSCLC, has IC50 values of 184 nM, 12 nM, and 1 nM against WT EGFR, L858R mutation, and L858R/T790M mutations, respectively. In cell lines, osimertinib was characterized by low activity against WT-EGFR cells (IC50 480–1865 nM) and high against L858/T790M (IC50 15 nM) and ex/19del/T790M (IC50 6 nM).22
Here, we review the clinical development of dacomitinib, with a special attention to its toxicity. We will examine the results of ARCHER 1050, the phase III study that was responsible for FDA approval, and put them into perspective.
Clinical development
Phase I trials
The largest phase I trial, ARCHER 1001, was conducted in the US by Jänne and colleagues; 121 patients were treated with dacomitinib, 57 of whom had a NSCLC, mainly pre-treated with first-generation TKIs. The starting dose was 0.5 mg and an accelerated dose escalation method was used with 100% dose escalation up to 60 mg, when grade (G) 3 stomatitis, palmar–plantar erythema and dehydration were observed in 3 out of 6 patients. After an expansion of the 30 mg dose level (the next lower dose), a 45 mg dose escalation was performed. At this dose level, a G3 rash was observed in 1 out of 6 patients. The maximum tolerated dose (MTD) was therefore determined at 45 mg daily. Finally, 4 (6%) out of 71 patients experienced unacceptable AEs at this dose, including rash (n=2), acneiform dermatitis (n=1), and mucositis (n=1). Although the study was not designed to evaluate the efficacy, an encouraging activity was observed in a subset of patients pre-treated with a first-generation TKI. Notably, no partial response (PR) was obtained in patients (n=4) harboring the T790M secondary mutation. The half-life was 59 to 85 hrs at dose levels between 30 and 60 mg. There was no apparent food effect (n=4) on absorption of oral dacomitinib: average maximum concentration achieved was similar with (22.5 ng/mL) or without (25.6 ng/mL) food. In addition, no significant variation was observed with antacid coadministration.23
Another phase I trial of dacomitinib explored dose levels from 15 mg to 45 mg in 13 Japanese patients with advanced cancers of whom 9 NSCLC (ARCHER 1005). Overall, rash was the most commonly reported adverse event (AE), affecting 13 patients out of 13 (G1 in 4 patients, G2 in 6, and G3 in 2). Eight dacomitinib-related G3 AEs were observed: rash (n = 2), decreased appetite, transaminase elevation (n=2), elevation of blood bilirubin, device-related infection, and transient ischemic attack. Systemic exposure parameters had a dose proportional trend, with linear kinetics between 15 and 45 mg.24
Similar results were observed in a phase I/II trial conducted in Korea (ARCHER 1003). The study population consisted of 12 patients in the phase I part and 43 patients in the phase II part, with KRAS WT advanced NSCLC previously treated with at least one chemotherapy line and a first-generation EGFR-TKI. In the dose-finding part of the trial, the dose level of 45 mg was established as adequate for the phase II. Overall, skin toxicity and diarrhea were the most frequently observed AEs. All treatment-related G3 AEs occurred in the phase II, including diarrhea (14%), paronychia (9.3%), dermatitis (4.7%), stomatitis (2.4%), pruritus (2.4%), fatigue (2.4%), and decrease in hemoglobin or lymphocyte values (7.2%). However, no AE led to treatment discontinuation after adequate management, including dose reductions or short-term interruptions. Interestingly, one patient harboring the T790M mutation attained a partial response that was however not confirmed on a subsequent scan and was classified as stable disease (SD).25
Phase II trials
The recommended phase II dose established from phase I studies was 45 mg daily. Three phase II trials assessed the activity of dacomitinib in patients with NSCLC [Table 3].
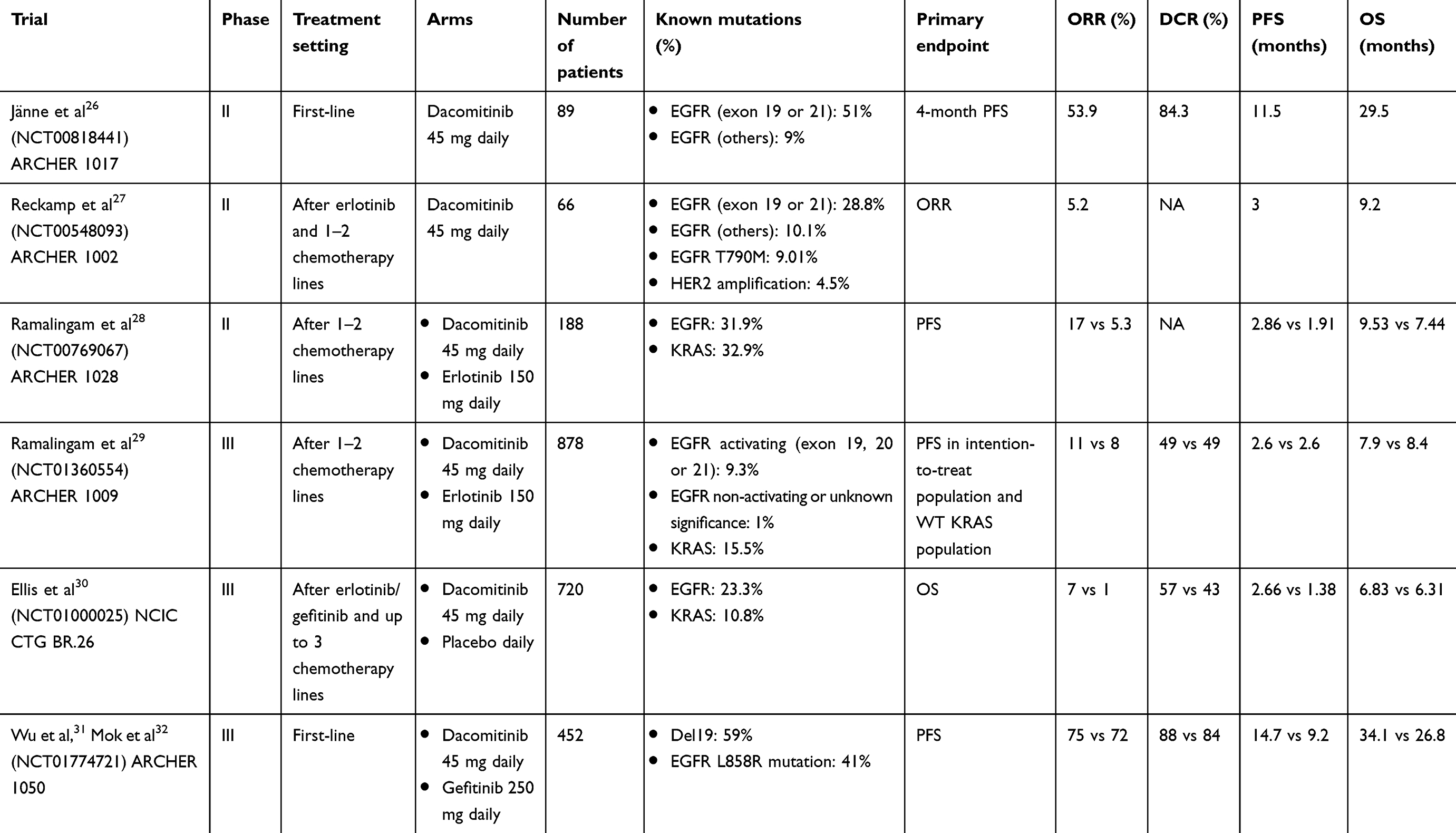 |
Table 3 Summary of the main phase II and III trials of dacomitinib |
ARCHER 1017 enrolled 89 stage IIIB/IV treatment-naïve NSCLC patients, from 25 centers in Hong Kong, Japan, South Korea, Taiwan, and USA. Initially, only never-smokers or former light smokers (clinically selected patients) were enrolled, with KRAS WT if non-Asian. This single-arm trial was subsequently amended to also include patients with EGFR mutations (molecularly selected patients), regardless of smoking status. Furthermore, the EGFR mutation was retrospectively tested in all patients with available tissue and unknown status at the time of enrolment. Since many patients needed early dose reduction, a starting dose of 30 mg was allowed, escalating to 45 mg if well tolerated. The study met the primary endpoint, which was 4-month PFS (76.8%; 95% CI: 66.4 to 84.4). ORR was 53.9% (95% CI: 43.0 to 64.6) and one patient obtained complete response (CR). Median PFS and OS were 11.5 (95% CI: 9.0 to 12.9) and 29.5 months (95% CI: 22.8 to 35.6), respectively.
Among patients harboring Del19 or exon 21 L858R mutation, a remarkable activity of dacomitinib was observed in all efficacy outcomes. In particular, ORR was 75.6%, disease control rate (DCR) was 97.8%, and median PFS and OS were 18.2 and 40.2 months, respectively. In patients with WT EGFR, estimated median OS and PFS, ORR, and DCR were 19.7 and 2.1 months, 7.1%, and 42.9%, respectively. Discontinuation rate due to treatment-related AE was 6%. In addition, dose reductions and short-term interruptions were reported in 32% and 56%, respectively. Diarrhea, acneiform dermatitis, and paronychia were the most frequently reported G≥2 AEs with rates of 44%, 53%, and 29%, respectively. Notably, diarrhea was experienced by 93% of the patients. Despite the toxicity profile, even in patients who had started treatment at a dose of 30 mg, the patient-reported outcomes (PROs) showed significant and clinically meaningful improvement in terms of dyspnea, chest pain, and cough.26
A second multicenter, open-label, single-arm phase II trial (66 patients) was conducted by Reckamp and colleagues. Eligibility criteria included KRAS WT or known EGFR Del19 or EGFR exon 21 mutation NSCLC, after 1 or 2 chemotherapy regimens and erlotinib failure; also non-adenocarcinomas were allowed. T790M mutation as secondary resistance to erlotinib was detected in 9.1% of the patients, while in 81.8% it was unknown.
Overall, PRs were observed in 5.2% of the patients. Focusing on EGFR-mutant patients, 8% obtained PR and 68% SD. Among 6 patients harboring the T790M mutation, 3 experienced progressive disease (PD) and 3 achieved SD, although the maximum duration of SD was only 12 weeks. The results of this study confirmed the greater efficacy of dacomitinib in patients with EGFR mutations compared to the overall population, both in terms of PFS (18 vs 12 weeks) and OS (57 vs 37 weeks). In terms of safety, G3 AEs were commonly reported, including diarrhea (12.1%), acneiform dermatitis (6.1%), pruritus (4.5%), and lymphopenia (18.2%). Treatment-related AEs required dose reductions or discontinuation in 33% and 9.1% of the patients, respectively; improvements in PROs were observed with regard to dyspnea, cough, chest pain, and pain in arm/shoulder.27
ARCHER 1028 was a multicenter, open-label randomized phase II trial comparing dacomitinib to erlotinib in unselected advanced NSCLC treated with one or two prior chemotherapies. The primary endpoint was PFS. A total of 188 patients were randomly assigned (1:1) to receive dacomitinib or erlotinib. Despite the randomization, patients who received dacomitinib were, on average, more frequently ECOG PS 2 (10.1% vs 1.6%), EGFR-mutant (10.1% vs 5.8%), and heavily pretreated (22.8% vs 16.4%) than patients who received erlotinib. The primary endpoint was met, with a PFS of 2.86 months in the dacomitinib arm compared to 1.91 months in the erlotinib arm (HR 0.66, 95% CI: 0.47 to 0.91, P=0.012). In the subgroup analysis, the advantage of dacomitinib was evidenced among patients with KRAS WT/EGFR any status (HR 0.55), KRAS WT/EGFR WT (HR 0.61), but was not statistically significant among patients harboring EGFR mutations (p=0.098). Overall, dacomitinib provided higher overall response rate (ORR) (17% including one CR vs 5.3%; P=0.011) and median duration of response (16.56 months vs 9.23). In contrast, OS was not statistically significantly different (HR 0.80, 95% CI: 0.56 to 1.13, P=0.205). Dacomitinib was associated with a worse safety profile than erlotinib. The rate of dose reductions for dacomitinib-related AEs was more than double in one of the patients receiving erlotinib. Moreover, among patients treated with dacomitinib a higher incidence of G≥2 diarrhea (40.8% vs 10.7%), acneiform dermatitis (32.3% vs 29.8%), paronychia (14% vs 3.1%), stomatitis (14% vs 5.4%), mucosal inflammation (13% vs 4%), and a lower rate of G≥2 fatigue (6.5% vs 7.5%) were observed.28
Recently, two additional phase II studies evaluated a different schedule of administration of dacomitinib, in order to obtain a better safety profile or to overcome the T790M resistance. These studies will be described later in this review.
Phase III trials
ARCHER 1009 was a randomized, multicentre (134 centers in 23 countries, both Asian and non-Asian), double-blind trial, comparing dacomitinib to erlotinib in patients with advanced NSCLC previously treated with one or two chemotherapy regimens (drugs targeting EGFR were not allowed). The primary endpoint was PFS in the whole population and in WT KRAS patients. Among 878 patients enrolled, 82 patients (9.3%) harbored an EGFR activating mutation and 136 (15.5%) had a KRAS mutant status. Overall, median PFS, confirmed by independent review, was 2.6 months in both treatment arms (HR 0.941, 95% CI: 0.802 to 1.104, P=0.229), and median OS was 7.9 months in the dacomitinib group and 8.4 months in the erlotinib group (HR 1.079, 95% CI: 0.914 to 1.274; P=0.817). In WT KRAS patients, median PFS was 2.6 months in both treatment arms (HR 1.022, 95% CI: 0.834 to 1.25, P=0.587) and median OS was 8.1 and 8.5 months (HR 1.095, 95% Cl: 0.882 to 1.360, P=0.796), respectively. As expected, patients harboring EGFR mutations achieved a longer PFS (11.0 months with dacomitinib and 10.9 with erlotinib) and OS (26.6 months with dacomitinib and not reached with erlotinib) in comparison with WT EGFR patients (PFS 1.9 months with dacomitinib or erlotinib and OS 6.8 with dacomitinib and 7.6 with erlotinib). Safety profile was similar to the one reported in previous studies, confirming a higher rates of G≥2 AEs in the dacomitinib group than in the erlotinib group: 39% versus 12% for diarrhea, 24% versus 21% for rash, 12% versus 13% for acneiform dermatitis, 12% versus 6% for paronychia, and 16% versus 4% for stomatitis. Discontinuation due to treatment-related AEs was observed in 7% of the patients receiving dacomitinib and 5% of the patients receiving erlotinib, with a dose reduction rate of 30% and 13%, respectively.29
NCIC CTG BR.26 was a double-blind phase III where 720 unselected NSCLC patients were randomly assigned 2:1 to receive dacomitinib or placebo, from 75 centers in 12 countries. Eligibility criteria included up to three chemotherapy lines and a first-generation EGFR-TKI. The primary endpoint of this study was OS. The trial did not show superiority for dacomitinib compared to placebo in terms of OS. Median OS was 6.83 months in the dacomitinib group versus 6.31 in the placebo group (HR 1.00, 95% CI: 0.83 to 1.21, P=0.506). In addition, there were no significant differences according to EGFR or KRAS mutational status. However, patients treated with dacomitinib obtained an improvement in PFS (2.66 months vs 1.38; HR 0.66, 95%, CI: 0.55 to 0.79, p<0.0001) and ORR (7% vs 1%, P=0·001). Safety profile was comparable with that reported in previous studies, with 9% of the patients who discontinued dacomitinib versus 1% who discontinued placebo; in addition, dose reduction rates were 35% and 3%, respectively, and 39% of the patients in the dacomitinib group experienced serious AEs. The most commonly reported G≥3 AEs due to dacomitinib were: diarrhea (12%), acneiform rash (10%), paronychia (3%), oral mucositis (3%), and fatigue (3%).30
ARCHER 1050 was a multicentre (71 centers in Asia, Europe, and North America), randomized, open-label, phase III study, where patients were assigned (1:1) to receive dacomitinib 45 mg or gefitinib 250 mg, orally daily. Eligibility included stage IIIB/IV or recurrent NSCLC (452 patients) with activating EGFR mutations (Del19 or L858R mutation). Exclusion criteria included brain metastases and atypical EGFR mutations. The trial met its primary endpoint (PFS), without meaningful differences between patients harboring Del19 and L858R mutation. As assessed by an independent radiological central review, PFS was 14.7 months in the dacomitinib arm and 9.2 in the gefitinib arm (HR 0. 59, 95% CI: 0.47 to 0.74, P<0.001). Similar proportion of patients in both groups obtained ORR (75% vs 72%), with CR in 5% and 2%, respectively. Patients treated with dacomitinib experienced more G≥3 AEs (63%) compared with patients treated with gefitinib (41%). In particular, G≥3 diarrhea was observed in 8% versus 1%, acneiform rash in 14% versus 0%, paronychia in 7% versus 1%, oral mucositis in 4% versus <1% and hypokalemia in 5% versus 2%. In contrast, G≥3 increases in alanine and aspartate aminotransferases were more represented in the gefitinib group. Nine percent of patients receiving dacomitinib experienced a serious treatment-related AE, including gastrointestinal, skin, subcutaneous, respiratory, hepatobiliary disorders, or others. Permanent discontinuation rate due to toxic effect was 10% with dacomitinib and 7% with gefitinib, while AEs requiring dose reduction were observed in 66% and 8% (as every-other-day dosing), respectively.31
In a further analysis, the OS data, secondary endpoint of the ARCHER 1050 study, were presented, with 31 months median follow-up time. Dacomitinib confirmed its superiority over gefitinib, showing a median OS of 34.1 months versus 26.8 months (HR 0.760, 95% CI: 0.582 to 0.993, P=0.0438). In addition, only one patient in the dacomitinib group developed brain metastases versus 11 patients in the gefitinib group. First subsequent treatments were represented by chemotherapy in 27.8% of dacomitinib arm and 35.6% of gefitinib arm and a third-generation TKI in 9.7% and 11.1%, respectively [Table 3].32
A special issue: safety profile
Since patients receive this treatment for over 1 year on average, the topic of safety deserves special attention [Table 4]. AEs developed under treatment with dacomitinib are believed to have an EGFR blockade etiology consistent with its mechanism of action. Phase II–III clinical trials have shown a dose reduction rate of 30–66% and a discontinuation rate due to treatment-related AEs of 6–10%.
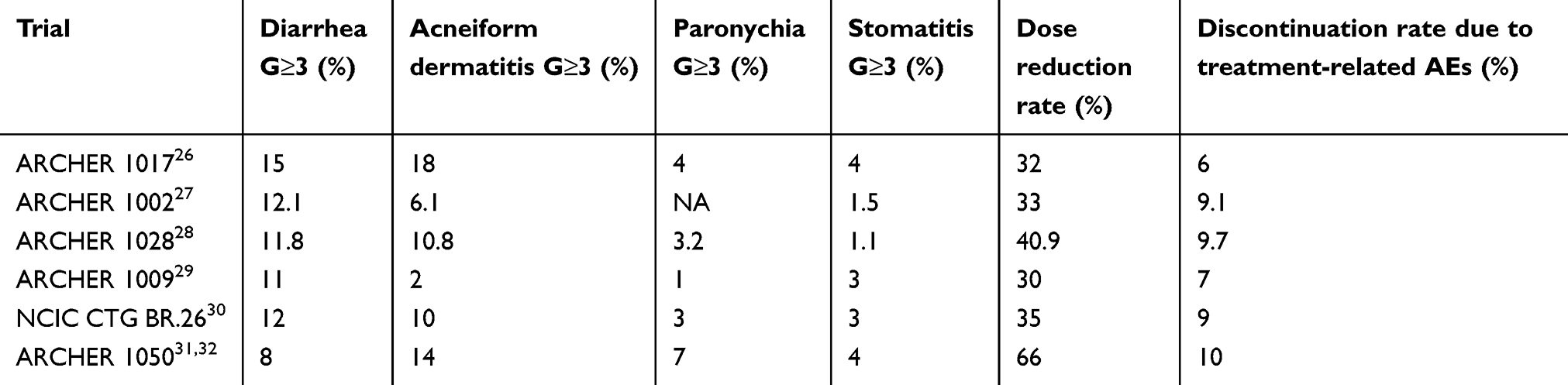 |
Table 4 Adverse events of dacomitinib in the main phase II and III trials |
The vast majority of G 3–4 AEs occurred during treatment with dacomitinib included diarrhea (8–15%), acneiform rash (2–18%), paronychia (1–7%), and stomatitis (1.1–4%).26,27,28,29,30,31,32 The frequency of these G 3–4 treatment-related AEs reported in the pivotal trial, ARCHER 1050, was significantly higher with dacomitinib than gefitinib.31 On the other hand, dacomitinib AEs are manageable with dose modifications and concomitant symptom treatment.
Although some toxicities, such as skin toxicity, improved considerably after appropriate management, early treatment of skin toxicity has been proposed to improve the safety profile of dacomitinib. ARCHER 1042 trial was conducted to overcome the limitation of skin toxicity with a preventive therapeutic intervention. It was a multicenter (in USA and Korea), phase II trial, conducted by Lacouture et al. The study design included three cohorts. In cohort I, patients randomly received 1:1 oral doxycycline 100 mg bid for 4 weeks or placebo. In cohort II, patients received oral VSL#3 probiotic up to 5 weeks. In addition, a topical cortisone-based (alclometasone dipropionate 0.05%) cream was provided for daily use in the evening. The trial met its primary endpoint. Doxycycline provided a remarkable reduction in the onset of G≥2 skin AEs compared with placebo (23.2% vs 46.6%, P=0.016) and a slight but not significant reduction in G≥2 diarrhea. In contrast, topical cream provided only a trend for reduction of dermatologic AEs, albeit not statistically significant. The probiotic did not bring any benefit in reducing diarrhea.33 In cohort III, 25 patients received dacomitinib at the dose of 45 mg with a planned interruption from day 11 to day 14 of cycle 1. On the days when treatment interruption was planned, a progressive decrease in dacomitinib plasma concentration was observed, from 66.8 ng/mL to 26.3 ng/mL. A similar trend was also observed for its metabolite PF-05199265. The comparison between the safety data of this study and the other studies that did not foresee the planned dose interruption is indirect and therefore inconclusive. However, in ARCHER 1042, a non-negligible incidence of G≥2 AEs was reported, including diarrhea in 40%, paronychia in 36%, stomatitis in 24%, and acneiform dermatitis in 20%. Moreover, concomitant medications for diarrhea were prescribed to more than three-quarters of patients in the first 8 weeks of treatment.34
A special topic: dacomitinib for T790M-positive NSCLC
Irreversible pan-HER TKI was also developed to overcome the T790M mutation. Despite the promising preclinical data and based on clinical development studies, a modest efficacy of dacomitinib in patients with NSCLC harboring T790M mutation was observed.19,21,23,25,27 However, the relatively small size of the T790M-positive population within the dacomitinib clinical trials precludes a precise estimate of the real benefit provided by dacomitinib in this group of patients. The study of Yu and colleagues was designed to understand whether dacomitinib is active in this population. Starting from the preclinical assumption that the pulsatile administration of dacomitinib would overcome the T790M resistance, a two-cohort, multicenter, phase II study was conducted. In this trial, EGFR T790M-positive patients (cohort A, n=16) and molecularly unselected T790M-negative patients (cohort B, n=22) were enrolled. Dacomitinib was administered at a dose of 45 mg every 12 hrs for 6 doses; the following week, patients received dacomitinib at 60 mg every 12 hrs for 6 doses with cycles repeated every 2 weeks. In cohort A, dose escalation with 15 mg levels was added if no major AEs were reported. The maximum dose reached was 105 mg every 12 hrs. Among patients assigned to cohort A, only 1 PR, of 2.8 months duration, and 7 SD were achieved (ORR 6.3%, DCR 50%). In contrast, ORR in cohort B was 0%. Median PFS was 2.3 months in cohort A and 1.6 months in cohort B. In terms of toxicity, 21% of the patients required a dose reduction, but no patients discontinued treatment due to specific AE. Safety profile was similar to that reported with usual dacomitinib dose (45 mg daily), with no unacceptable toxicity reported for patients undergoing a dose escalation. Despite the pulsatile dacomitinib administration, the efficacy parameters did not show an improvement from this treatment schedule, both in T790M-positive and in unselected patients.35
Interestingly, the AURA3 trial showed a remarkable benefit offered by the use of osimertinib among T790M-positive patients after progressive disease during first-line EGFR-TKI therapy. Clear advantages were obtained in PFS (10.1 months vs 4.4; HR 0.30; P<0.001) and ORR (71% vs 31%) compared to chemotherapy, across all pre-specified subgroups, even in patients with brain metastases.36
Current perspectives and future directions
Although results from ARCHER 1050 have shown a clear survival benefit from dacomitinib in first-line treatment, the field has undergone significant changes. This benefit must, indeed, be interpreted and compared with the results of two recent trials, LUX-Lung 7 and FLAURA, conducted in the same setting of patients.37–39
LUX-Lung 7, a phase IIb trial, demonstrated a PFS benefit of afatinib, another second-generation irreversible TKI, over gefitinib, with a median of 11.0 months vs 10.9 (HR 0.73, P=0.017); additionally, median time-to-treatment failure was significantly longer with afatinib than with gefitinib (13.7 months vs 11.5; HR 0.73, P=0.0073).37 On the contrary, OS did not differ significantly between the two treatments (27.9 vs 24.5 months; HR 0.86, P=0.2580). Being an irreversible HER inhibitor, afatinib showed a safety profile more similar to dacomitinib than to gefitinib, with an increase in treatment-related G≥3 (31.3% vs 19.5%) and in particular diarrhea (13.1% vs 1.3%), acneiform dermatitis (9.4% vs 3.1%), and fatigue (5.6% vs 0%).38
The results of the FLAURA study have demonstrated an important benefit of osimertinib compared to gefitinib or erlotinib in the first-line treatment. Patients treated with osimertinib obtained a median PFS of 18.9 months versus 10.2 of the control arm (HR 0.46, P<0.001). Although the survival data were immature, 83% of the patients treated with osimertinib and 71% of the patients treated with a first-generation EGFR-TKI were alive at 18 months (HR 0.63, P=0.007). The study has some worthy distinctive features. First of all, patients with brain metastases were not excluded from the study. Even in these patients, usually associated with a poor prognosis, osimertinib offered a consistent benefit in PFS. Another strength of this study is the lower incidence of AEs related to osimertinib compared to erlotinib or gefitinib. G≥3 AEs occurred in 34% of the patients receiving osimertinib and in 45% of the patients receiving first-generation TKI. The EGFR-TKI class toxicities had very low incidence with osimertinib treatment: G≥3 rash in 1%, diarrhea in 2%, paronychia in <1%, stomatitis in <1%. Additionally, few AEs led to treatment interruption (13%). The only G≥3 AE that deserves attention was the prolongation of the QT interval, which was observed in 2% of the patients receiving osimertinib.39
While awaiting the final OS results of the FLAURA trial, dacomitinib remains the only TKI to have shown a survival advantage over a first-generation EGFR inhibitor. However, the favorable results obtained in terms of improvement in PFS, associated with remarkable evidence of benefit in patients with brain metastases and the more favorable safety profile, make osimertinib the preferred first-line treatment.
Nevertheless, several aspects of dacomitinib are currently little explored and could be promising for future development.
As suggested by preclinical data, dacomitinib might have activity in patients whose tumors harbor HER2 mutations or amplification. Among 30 patients treated with dacomitinib in a phase II study, 3 patients with exon 20 mutation (p. M774delinsWLV and p. P780_Y781insGSP) achieved PR, while no patients with HER2 amplification obtained objective response.40 Although dacomitinib inhibits both EGFR, HER2, and HER4 tyrosine kinases, these results suggest that the HER2-mutant population is widely heterogeneous and only a limited group of patients may benefit from this treatment. Further clinical trials are expected to define which group of molecularly selected patients could have a considerable advantage from dacomitinib.12,21,40
Another additional propriety of dacomitinib is the synergistic effect with cytotoxic chemotherapy, which has recently been studied. Preclinical studies show that dacomitinib enhances the effect of ATP-binding cassette subfamily G member 2 (ABCG2) substrate drugs (eg, topotecan and methotrexate) in vitro, particularly in the case of multi-drug resistance due to ABCG2 overexpression. This specific property was also observed in murine xenograft models, where dacomitinib significantly increased the antitumor efficacy of topotecan.41
An open question is the activity of dacomitinib on rare mutations. There is no conclusive evidence of efficacy of dacomitinib on rare mutations, mainly because this population was poorly represented in clinical trials. However, in ARCHER 1001 study, among 5 patients with exon 20 insertion, a DCR of 60% was reported.23 Moreover, in the phase 2 study by Reckamp and colleagues, 1 patient with G719C (exon 18) and S768I (exon 20) mutations obtained an objective response.27 In addition, analyzing in vitro the activity of dacomitinib on Ba/F3 cells an IC50 value <10 nM for G719X mutation was reported.14
Another key issue is the incidence of the T790M mutation as secondary resistance to dacomitinib. As suggested by preclinical data, Ba/F3 cells harboring Del19, L858R, or G719A mutations can develop T790M and C797S mutations after prolonged dacomitinib exposure.42 Although there are no clinical studies that provide a precise estimate of the incidence of the T790M mutation as secondary resistance to dacomitinib, the analysis of serum samples from ARCHER 1017 study showed that about half of the patients were T790M mutation-positive at the time of progression.26
Several clinical trials are currently investigating new perspectives on the use of dacomitinib in NSCLC. A phase I trial is evaluating the safety of the combination of dacomitinib and osimertinib, at increasing doses, in patients with NSCLC harboring activating mutations in EGFR, never treated with an EGFR-TKI (NCT03810807). Another phase I trial is studying the efficacy of dacomitinib after osimertinib failure in patients with or without C797S mutation (NCT03755102). The pharmacokinetic parameters after a single dose of dacomitinib in patients with severe hepatic impairment (cohort 1) or normal hepatic function (cohort 2) are the primary endpoints of another ongoing phase I trial (NCT03865446). A phase I/II trial is investigating the combination of dacomitinib and PD-0325901 (MEK inhibitor) in patients with KRAS mutant NSCLC (NCT02039336). Finally, an international, multicenter, phase II trial is assessing the safety and efficacy of dacomitinib, with or without dose titration, as first line for advanced NSCLC with EGFR activating mutations (NCT04027647).
In conclusion, the initial studies of dacomitinib, which included EGFR WT patients yielded negative results; however, the advantage of EGFR-TKIs is provided in patients with EGFR activating mutations. In this population, ARCHER 1050 trial confirmed the efficacy of dacomitinib, demonstrating for the first time an OS gain compared to the first-generation TKI gefitinib. Although burdened by greater toxicity than osimertinib, dacomitinib can be considered as a standard first-line option in patients with advanced EGFR-mutated NSCLC.
Abbreviations
ABCG2, ATP-binding cassette subfamily G member 2; AE, adverse event; CR, complete response; DCR, disease control rate; Del19, deletions in exon 19; EGFR, epidermal growth factor receptor; FDA, Food and Drug Administration; G, grade; HER, human epidermal growth factor receptor; MTD, maximum tolerated dose; NSCLC, non-small cell lung cancer; OS, overall survival; ORR, overall response rate; PROs, patient-reported outcomes; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease; TKI, tyrosine kinase inhibitor; WT, wild-type.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Herbst RS, Morgensztern D, Boshoff C, et al. The biology and management of non-small cell lung cancer. Nature. 2018;553(7689):446–454. doi:10.1038/nature25183
2. Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(21):2129–2139. doi:10.1056/NEJMoa040938
3. Paez JG, Jänne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5676):1497–1500. doi:10.1126/science.1099314
4. Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–957. doi:10.1056/NEJMoa0810699
5. Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362(25):2380–2388. doi:10.1056/NEJMoa0909530
6. Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–128. doi:10.1016/S1470-2045(09)70364-X
7. Yoshioka H, Mitsudomi T, Morita S, et al. Final overall survival results of WJTOG 3405, a randomized phase 3 trial comparing gefitinib (G) with cisplatin plus docetaxel (CD) as the first-line treatment for patients with non-small cell lung cancer (NSCLC) harboring mutations of the epidermal growth factor receptor (EGFR). J Clin Oncol. 2014;32(15_suppl):8117.
8. Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12(8):735–742. doi:10.1016/S1470-2045(11)70184-X
9. Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13(3):239–246. doi:10.1016/S1470-2045(11)70393-X
10. Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31(27):3327–3334. doi:10.1200/JCO.2012.44.2806
11. Yang JC, Wu YL, Schuler M, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015;16(2):141–151. doi:10.1016/S1470-2045(14)71173-8
12. Liu X, Wang P, Zhang C, et al. Epidermal growth factor receptor (EGFR): A rising star in the era of precision medicine of lung cancer. Oncotarget. 2017;8(30):50209–50220.
13. Yoshida T, Zhang G, Haura EB. Targeting epidermal growth factor receptor: central signaling kinase in lung cancer. Biochem Pharmacol. 2010;80(5):613–623. doi:10.1016/j.bcp.2010.05.014
14. Kobayashi Y, Mitsudomi T. Not all epidermal growth factor receptor mutations in lung cancer are created equal: perspectives for individualized treatment strategy. Cancer Sci. 2016;107(9):1179–1186. doi:10.1111/cas.12996
15. Red Brewer M, Yun CH, Lai D, et al. Mechanism for activation of mutated epidermal growth factor receptors in lung cancer. Proc Natl Acad Sci U S A. 2013;110(38):E3595–E3604. doi:10.1073/pnas.1220050110
16. Yun CH, Mengwasser KE, Toms AV, et al. The T790M mutation in EGFR kinase causes drug resistance by increasing the affinity for ATP. Proc Natl Acad Sci U S A. 2008;105(6):2070–2075. doi:10.1073/pnas.0709662105
17. Morgillo F, Della Corte CM, Fasano M, et al. Mechanisms of resistance to EGFR-targeted drugs: lung cancer. ESMO Open. 2016;1(3):e000060. doi:10.1136/esmoopen-2016-000060
18. Engelman JA, Zejnullahu K, Mitsudomi T, et al. MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science. 2007;316(5827):1039–1043. doi:10.1126/science.1141478
19. Gonzales AJ, Hook KE, Althaus IW, et al. Antitumor activity and pharmacokinetic properties of PF–00299804, a second-generation irreversible pan-erbB receptor tyrosine kinase inhibitor. Mol Cancer Ther. 2008;7:1880–1889. doi:10.1158/1535-7163.MCT-07-2370
20. Yang JC, Sequist LV, Geater SL. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: a combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015;16(7):830–838. doi:10.1016/S1470-2045(15)00026-1
21. Engelman JA, Zejnullahu K, Gale CM, et al. PF00299804, an irreversible pan-ERBB inhibitor, is effective in lung cancer models with EGFR and ERBB2 mutations that are resistant to gefitinib. Cancer Res. 2007;67(24):11924–11932. doi:10.1158/0008-5472.CAN-07-1885
22. Cross DA, Ashton SE, Ghiorghiu S, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4(9):1046–1061. doi:10.1158/2159-8290.CD-14-0337
23. Jänne PA, Boss DS, Camidge DR, et al. Phase I dose-escalation study of the pan-HER inhibitor, PF299804, in patients with advanced malignant solid tumors. Clin Cancer Res. 2011;17:1131–1139. doi:10.1158/1078-0432.CCR-10-1220
24. Takahashi T, Boku N, Murakami H, et al. Phase I and pharmacokinetic study of dacomitinib (PF-00299804), an oral irreversible, small molecule inhibitor of human epidermal growth factor receptor-1, −2, and −4 tyrosine kinases, in Japanese patients with advanced solid tumors. Invest New Drugs. 2012;30(6):2352–2363. doi:10.1007/s10637-011-9789-z
25. Park K, Cho BC, Kim DW, et al. Safety and efficacy of dacomitinib in korean patients with KRAS wild-type advanced non-small-cell lung cancer refractory to chemotherapy and erlotinib or gefitinib: a phase I/II trial. J Thorac Oncol. 2014;9(10):1523–1531. doi:10.1097/JTO.0000000000000275
26. Jänne PA, Ou SH, Kim DW, et al. Dacomitinib as first-line treatment in patients with clinically or molecularly selected advanced non-small-cell lung cancer: a multicentre, open-label, phase 2 trial. Lancet Oncol. 2014;15(13):1433–1441. doi:10.1016/S1470-2045(14)70461-9
27. Reckamp KL, Giaccone G, Camidge DR, et al. A phase 2 trial of dacomitinib (PF‐00299804), an oral, irreversible pan‐HER (human epidermal growth factor receptor) inhibitor, in patients with advanced non–small cell lung cancer after failure of prior chemotherapy and erlotinib. Cancer. 2014;120(8):1145–1154. doi:10.1002/cncr.28561
28. Ramalingam SS, Blackhall F, Krzakowski M, et al. Randomized phase II study of dacomitinib (PF-00299804), an irreversible pan-human epidermal growth factor receptor inhibitor, versus erlotinib in patients with advanced non-small-cell lung cancer. J Clin Oncol. 2012;30(27):3337–3344. doi:10.1200/JCO.2011.40.9433
29. Ramalingam SS, Jänne PA, Mok T, et al. Dacomitinib versus erlotinib in patients with advanced-stage, previously treated non-small-cell lung cancer (ARCHER 1009): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(12):1369–1378. doi:10.1016/S1470-2045(14)70452-8
30. Ellis PM, Shepherd FA, Millward M, et al. Dacomitinib compared with placebo in pretreated patients with advanced or metastatic non-small-cell lung cancer (NCIC CTG BR.26): a double-blind, randomised, phase 3 trial. Lancet Oncol. 2014;15(12):1379–1388. doi:10.1016/S1470-2045(14)70472-3
31. Wu YL, Cheng Y, Zhou X, et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18(11):1454–1466. doi:10.1016/S1470-2045(17)30608-3
32. Mok TS, Cheng Y, Zhou X, et al. Improvement in overall survival in a randomized study that compared dacomitinib with gefitinib in patients with advanced non-small-cell lung cancer and EGFR-activating mutations. J Clin Oncol. 2018;36(22):2244–2250. doi:10.1200/JCO.2018.78.7994
33. Lacouture ME, Keefe DM, Sonis S, et al. A phase II study (ARCHER 1042) to evaluate prophylactic treatment of dacomitinib-induced dermatologic and gastrointestinal adverse events in advanced non-small-cell lung cancer. Ann Oncol. 2016;27(9):1712–1718. doi:10.1093/annonc/mdw227
34. Kim DW, Garon EB, Jatoi A, et al. Impact of a planned dose interruption of dacomitinib in the treatment of advanced non-small-cell lung cancer (ARCHER 1042). Lung Cancer. 2017;106:76–82. doi:10.1016/j.lungcan.2017.01.021
35. Yu HA, Ahn MJ, Cho BC, et al. Phase 2 study of intermittent pulse dacomitinib in patients with advanced non-small cell lung cancers. Lung Cancer. 2017;112:195–199. doi:10.1016/j.lungcan.2017.08.017
36. Mok TS, Wu Y-L, Ahn M-J, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. 2017;376(7):629–640. doi:10.1056/NEJMoa1612674
37. Park K, Tan EH, O’Byrne K, et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016;17(5):577–589. doi:10.1016/S1470-2045(16)30033-X
38. Paz-Ares L, Tan EH, O’Byrne K, et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: overall survival data from the phase IIb LUX-Lung 7 trial. Ann Oncol. 2017;28(2):270–277. doi:10.1093/annonc/mdx075
39. Soria J-C, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
40. Kris MG, Camidge DR, Giaccone G, et al. Targeting HER2 aberrations as actionable drivers in lung cancers: phase II trial of the pan-HER tyrosine kinase inhibitor dacomitinib in patients with HER2-mutant or amplified tumors. Ann Oncol. 2015;26(7):1421–1427. doi:10.1093/annonc/mdv383
41. Guo X, To KKW, Chen Z, et al. Dacomitinib potentiates the efficacy of conventional chemotherapeutic agents via inhibiting the drug efflux function of ABCG2 in vitro and in vivo. J Exp Clin Cancer Res. 2018;37(1):31. doi:10.1186/s13046-018-0690-x
42. Kobayashi Y, Fujino T, Nishino M, et al. EGFR T790M and C797S mutations as mechanisms of acquired resistance to dacomitinib. J Thorac Oncol. 2018;13(5):727–731. doi:10.1016/j.jtho.2018.01.009
43. Li D, Ambrogio L, Shimamura T, et al. BIBW2992, an irreversible EGFR/HER2 inhibitor highly effective in preclinical lung cancer models. Oncogene. 2008;27(34):4702–4711. doi:10.1038/onc.2008.109
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.