")
Back to Journals » OncoTargets and Therapy » Volume 16
Clinical Efficacy and Safety of Immunotherapy Retreatment in Metastatic Cervical Cancer: A Retrospective Study
Authors Li G, Cheng M, Hong K , Jiang Y
Received 6 December 2022
Accepted for publication 27 February 2023
Published 6 March 2023 Volume 2023:16 Pages 157—163
DOI https://doi.org/10.2147/OTT.S400376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Guiling Li,1,* Mingxia Cheng,1,* Kai Hong,2,* Yao Jiang1
1Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Medical Ultrasound, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yao Jiang, Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Tel +86 13797011369, Fax +86-27-85873062, Email [email protected]
Purpose: Metastatic cervical cancer has a poor prognosis, and treatment options are limited. Immunotherapy has been used to achieve disease control in patients with cervical cancer; however, the efficacy of immunotherapy retreatment after disease progression is unclear. This study aimed to explore the efficacy and safety of immunotherapy retreatment in metastatic cervical cancer.
Patients and methods: We retrospectively reviewed the clinical data of patients with metastatic cervical cancer who underwent immunotherapy retreatment after disease progression following previous immunotherapy from June 2019 to April 2021.
Results: Fifteen patients were included in this study. All patients received combination immunotherapy retreatment consisting of camrelizumab, nab-paclitaxel, and apatinib. Four (26.7%) patients achieved partial response while three (20.0%) achieved stable disease. The objective response rate and disease control rate were 26.7% and 46.7%, respectively. The median progression-free survival and overall survival were 3.0 (95% confidence interval: 1.0– 5.0) and 8.0 (95% confidence interval: 3.4– 12.6) months, respectively. None of the patients discontinued treatment because of intolerable toxicity.
Conclusion: Our findings suggest that the triplet combination immunotherapy retreatment could be a therapeutic option for patients with metastatic cervical cancer who failed initial immunotherapy.
Keywords: apatinib, camrelizumab, disease progression, nab-paclitaxel, survival, toxicity
Introduction
Cervical cancer is the fourth most common cancer among women.1 Patients with metastatic cervical cancer have limited treatment options and a poor prognosis.2 In 2014, the GOG240 study3 demonstrated that cisplatin plus paclitaxel and bevacizumab achieved an objective response rate (ORR) of 48% and an overall survival (OS) of 17 months in metastatic cervical cancer. Since then, combination therapy comprising chemotherapy plus bevacizumab has been the standard of care. Furthermore, in the last few years immune checkpoint inhibitors (ICIs) have notably altered the treatment paradigm in cervical cancer. Among these, programmed cell death protein 1 (PD-1) and PD-L1 inhibitors are belonging to the most widely studied class of ICI drugs. A range of Phase II studies have demonstrated clinical benefits of the PD-1 inhibitors pembrolizumab and nivolumab in the second- and later-line treatments of metastatic cervical cancer, with a modest response rate of approximately 15%.4–6 Therefore, the role of combination immunotherapy has been investigated. In a recent phase II study of the PD-1 inhibitor camrelizumab in combination with the antiangiogenic agent apatinib (CLAP study)7 of advanced cervical cancer that progressed after prior lines of systemic treatment, the ORR was 55.6%, and the median progression-free survival (PFS) was 8.8 months. More recently, the Phase III KEYNOTE-826 study8 showed significant survival improvements following the addition of pembrolizumab to standard chemotherapy with or without bevacizumab, and this drug has been approved as first-line treatment for metastatic cervical cancer. Recently, several clinical trials of ICI combination treatments have been conducted with respect to locally advanced and metastatic cervical cancer.9
Under these circumstances, the proportion of patients with metastatic cervical cancer undergoing immunotherapy has been increasing. However, the majority of patients ultimately develop resistance to immunotherapy. For these patients, clinical treatment options are limited. Recently, ICI retreatment has attracted significant attention. A few case series on ICI retreatment in non-small cell lung cancer (NSCLC), renal cell carcinoma, and melanoma have demonstrated promising efficacy and acceptable toxicity profiles.10–15 However, whether ICI retreatment has benefits in cervical cancer is unclear. Furthermore, previous studies mainly included patients who experienced disease progression after ICI monotherapy, while limited data are available on those who progressed after chemo-immunotherapy. Therefore, we conducted this retrospective study to evaluate the efficacy and safety of ICI combination retreatment in patients with metastatic cervical cancer whose disease progressed after initial immunotherapy. We present the following article in accordance with the STROBE reporting checklist.
Methods
Patients
From June 2019 to April 2021, patients with metastatic cervical cancer who received ICI retreatment at the Cancer Center, Union Hospital, Huazhong University of Science and Technology, Wuhan, China, were enrolled in this study. The inclusion criteria were as follows: (1) pathologically confirmed squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix; (2) metastatic cervical cancer; (3) achieved complete response (CR), partial response (PR), or stable disease (SD) as the best clinical response to first-course immunotherapy; (4) received at least two cycles of retreatment with triplet combination therapy including PD-1 inhibitor, chemotherapy, and antiangiogenic agent; (5) had at least one measurable lesion according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1; and (6) Eastern Cooperative Oncology Group performance score of 1 or less. Patients who did not have the follow-up data were excluded from the analyses. Baseline clinicopathological data, including age, histology, initial stage, metastatic sites, primary surgery, lines of prior systemic treatment, and immunotherapy regimens, were retrieved from medical records.
This retrospective study was conducted in accordance with the principles embodied in the 1964 Declaration of Helsinki and was approved by the Ethics Committee of the Union Hospital of the Huazhong University of Science and Technology (20220023). Informed consent was obtained from all the participants or their legal guardians if the participants cannot write.
Treatment
For the initial immunotherapy, patients were treated with 200 mg of intravenous camrelizumab with or without chemotherapy. Camrelizumab is a monoclonal antibody against PD-1 and has been approved for the treatment of a series of solid tumors in China.16 Apatinib is a small-molecule vascular endothelial growth factor receptor 2 inhibitor and has exhibited antitumor efficacy in a range of malignancies. For combination immunotherapy retreatment, all patients received camrelizumab 200 mg with nab-paclitaxel 260 mg/m2 intravenously every 3 weeks and oral apatinib 250 mg once daily until disease progression or intolerable toxicity.
Efficacy and Safety Assessment
Tumor responses included CR, PR, SD, and progressive disease, which were assessed according to the RECIST version 1.1 criteria.17 PFS1 refers to the duration from the first ICI initiation to the date of disease progression. PFS2 refers to the duration from the initiation of ICI retreatment to the date of disease progression or the last follow-up visit, whichever occurred first. OS refers to the duration from the start of ICI retreatment to death or the last follow-up visit. ORR refers to the percentage of patients who exhibited CR or PR. The disease control rate (DCR) refers to the proportion of patients who achieved CR, PR, or SD. Computed tomography or magnetic resonance imaging of the thorax, abdomen, and pelvis was performed at baseline and after completion of every two or three cycles during immunotherapy retreatment. The last follow-up date was October 20, 2021. Treatment-related adverse events (AEs) were graded from 1 to 5 based on the Common Terminology Criteria for Adverse Events version 5.0.18
Statistical Analyses
Statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). Categorical data are presented as percentages. Continuous data are expressed as medians (range). Survival analyses were conducted using the Kaplan–Meier method. Spearman correlation coefficient was used to perform correlation analysis. Two-sided p < 0.05 was regarded as statistically significant.
Results
Characteristics of the Patients
A total of 113 patients with metastatic cervical cancer received immunotherapy, and 15 patients (13.3%) who underwent combination immunotherapy retreatment were included. The median follow-up time was 8.0 months. All patients achieved PR as the best overall response to the first ICI treatment, which was discontinued after disease progression. The median age was 50 years (range: 30–71 years), and 11 (73.3%) patients had squamous cell carcinoma. Six (40.0%) patients had only pelvic recurrence, and 9 (60.0%) had distant metastasis with or without pelvic recurrence. Of the 15 patients included, 11 (73.3%) received two lines of previous systemic treatment before immunotherapy retreatment. Of the prior immunotherapies, 4 (26.7%) patients received camrelizumab monotherapy as a second-line treatment and 11 (73.3%) underwent combination immunotherapy. The patient characteristics are presented in Table 1.
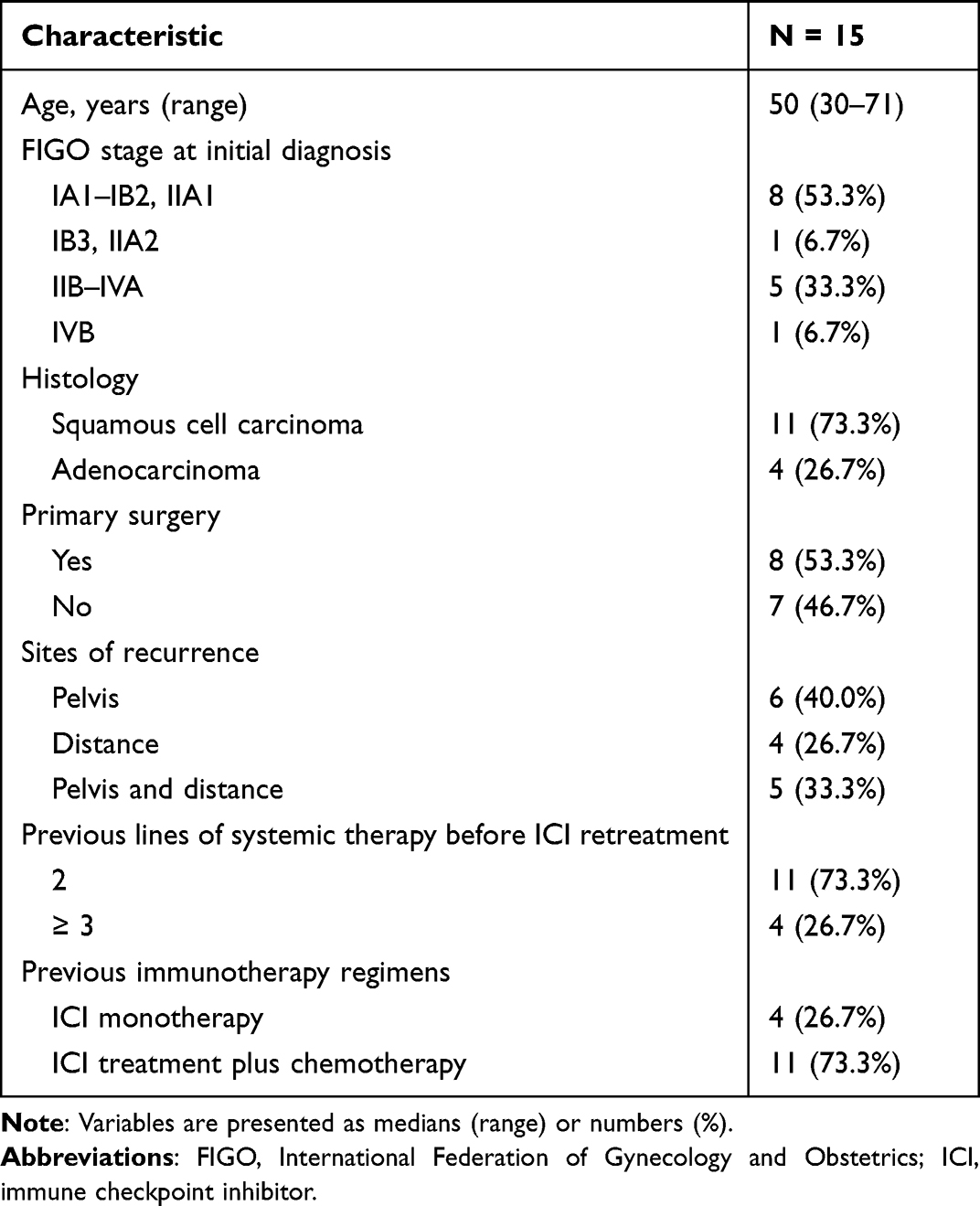 |
Table 1 Patient Characteristics |
Efficacy
All 15 patients received retreatment with the triplet combination immunotherapy consisting of camrelizumab, nab-paclitaxel, and apatinib. Among them, 4 (26.7%) and 3 (20.0%) patients achieved PR and SD, respectively. None of the patients achieved CR. The ORR and DCR were 26.7% and 46.7%, respectively. Of the 11 patients who were previously treated with camrelizumab and chemotherapy, 2 (18.2%) achieved PR and 2 (18.2%) achieved SD after combination immunotherapy retreatment. Of the 15 patients, the median PFS1 was 7.0 (95% confidence interval [CI]: 6.1–7.9) months. The median PFS2 and OS were 3.0 (95% CI: 1.0–5.0) months and 8.0 (95% CI: 3.4–12.6) months, respectively. The duration of clinical responses of initial ICI treatment and ICI combination retreatment are shown in Figure 1. There was no correlation between the duration of PFS1 and PFS2.
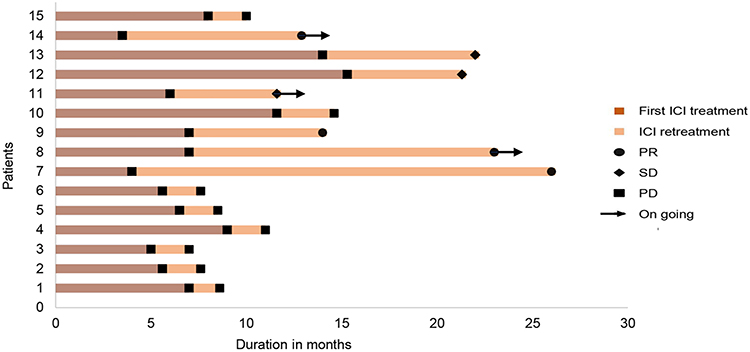 |
Figure 1 Swimmer plot displaying clinical responses to the first ICI treatment and to ICI retreatment in patients with metastatic cervical cancer. Abbreviations: ICI, immune checkpoint inhibitor; PR, partial response; SD, stable disease; PD, progressive disease. |
Safety
Treatment-related AEs are presented in Table 2. Twelve (80.0%) patients experienced an AE after combination immunotherapy retreatment. None of the patients discontinued treatment because of intolerable toxicity, and no treatment-related deaths were documented. The most common AE in this study was anemia (40.0%). Six (40.0%) patients experienced grade 3/4 AEs, with 3 (20.0%) experiencing grade 3 anemia, 2 (13.3%) experiencing grade 3 infection, and 1 (6.7%) experiencing grade 3 elevated transaminase levels, which was resolved with supportive treatment.
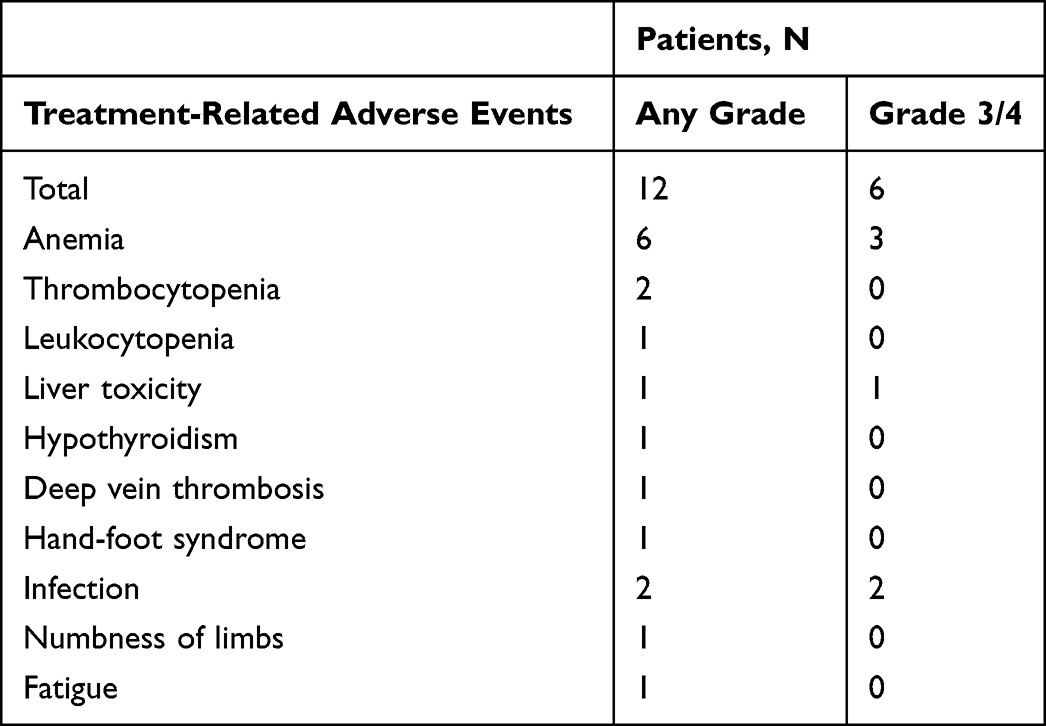 |
Table 2 Treatment-Related Adverse Events Experienced Upon Combination Immunotherapy Retreatment (N = 15) |
Discussion
Metastatic cervical cancer is considered incurable and has limited treatment options. In recent years, immunotherapy has been demonstrated to be a promising treatment for improving the clinical response in metastatic cervical cancer. However, for patients with disease progression after initial immunotherapy, clinical management remains challenging. Recently, immunotherapy retreatment has been suggested as a therapeutic option. However, the efficacy and safety of immunotherapy retreatment for cervical cancer have not been examined. In this study, we demonstrated that ICI combination retreatment was a viable treatment option for patients with metastatic cervical cancer for whom initial immunotherapy has failed.
Several challenges concerning immunotherapy retreatment need to be addressed. The first challenge is to identify patients who would benefit from immunotherapy retreatment. A retrospective study of ICI retreatment in NSCLC reported that ICI retreatment induced longer survival benefits in patients with good performance status.19 Nomura et al20 showed that the efficacy of nivolumab retreatment for metastatic melanoma was associated with the PFS duration after the first nivolumab therapy. In a national database analysis of immunotherapy rechallenge after nivolumab treatment for patients with NSCLC, the median OS was significantly longer in patients with a longer PFS duration after the first nivolumab treatment.21 In contrast, two other studies showed no correlation between the duration of PFS with the first ICIs and the efficacy of the second ICIs.10,22 This may be because patients were treated with different immunotherapy regimens from previous ICIs. In these two studies, most of the enrolled patients were treated with pembrolizumab after the disease progressed despite nivolumab treatment. In our study, patients were previously treated with camrelizumab with or without chemotherapy. After progression, all patients were switched to triplet combination therapy. The median PFS1 was 7.0 months, and there was no association between the duration of PFS1 and the efficacy of immunotherapy retreatment. Previous studies have also suggested that the efficacy of ICI retreatment may depend on the treatment regimen used between the first and second ICI therapies. Patients who received radiotherapy before ICI retreatment achieved a higher response rate.12 However, there are contradictory opinions. In a case series of 12 patients with advanced NSCLC, Fujita et al10 reported that chemotherapy and radiotherapy between the first and second ICI administrations did not affect the efficacy of ICI retreatment.
Notably, the aforementioned studies mainly included patients treated with single-agent ICIs for initial immunotherapy. In clinical practice, an increasing number of patients are being treated with combination immunotherapy. To date, limited data are available on the efficacy of immunotherapy retreatment in these patients. In our study, 11 patients received combination therapy with camrelizumab and chemotherapy as the initial immunotherapy. Among them, the ORR and DCR for immunotherapy retreatment were 18.2% and 36.4%, respectively. Our data suggest that patients treated with combination immunotherapy could achieve clinical benefits from this triplet ICI combination retreatment.
The second challenge is determining the optimal ICI retreatment strategy. Several studies have investigated different retreatment strategies according to the reasons for discontinuation of previous ICIs.23–26 In general, patients who discontinued previous ICIs due to treatment completion often underwent retreatment with the original ICIs. In contrast, patients who experienced disease progression with previous ICIs were usually treated with different ICIs or ICI combination therapy. In our study, all patients experienced disease progression with previous ICI treatment; therefore, combination treatment was considered. Recently, a retrospective study of ICI retreatment in metastatic melanoma after initial ICI failure reported that chemo-immunotherapy demonstrated favorable efficacy compared with ICIs or chemotherapy retreatment alone.27 Chemotherapy has been reported to increase neoantigen release, exert immunostimulatory effects, and, thus, enhance the antitumor effects of immunotherapy.28 Antiangiogenic agents could normalize tumor vasculature, modulate tumor immunosuppressive microenvironment, increase immune cell infiltration, and further boost antitumor efficacy of chemo-immunotherapy.29,30 In the IMpower150 study,31 the combination of atezolizumab plus bevacizumab and chemotherapy significantly improved survival outcomes in patients with advanced non-squamous NSCLC. In our study, 11 patients progressed after chemo-immunotherapy. Thus, combination therapy of camrelizumab with nab-paclitaxel and apatinib was administered as the retreatment regimen. Studies have reported that among patients who failed initial immunotherapy, the ORR of combination immunotherapy retreatment is approximately 20%.15 In our study, the ORR and DCR of the triplet immunotherapy retreatment were 26.7% and 46.7%, respectively; the median PFS and OS were 3.0 and 8.0 months, respectively. Currently, several studies are investigating PD-1/PD-L1 inhibitor retreatment with the addition of CTLA-4 inhibitors, targeted drugs, chemotherapy, or radiotherapy in various cancer types.15
In this analysis, retreatment with combination immunotherapy was well tolerated. The most common treatment-related AE observed during immunotherapy combination retreatment was anemia. None of the patients experienced dose-limiting toxicity. Therefore, the triplet combination strategy showed promising antitumor activity, with manageable AEs, as an ICI retreatment regimen for metastatic cervical cancer.
This study had several limitations. First, it was a single-center, retrospective study with a small sample size, which might have led to selection bias. Therefore, our findings should be interpreted with caution. Second, PD-L1 expression, microsatellite instability, and tumor mutation burden were not routinely examined. Therefore, we could not determine whether these factors could be predictive biomarkers of ICI combination retreatment efficacy.
Conclusion
To our knowledge, this study is the first to provide clinical evidence that ICI combination retreatment consisting of PD-1 inhibitor plus chemotherapy and antiangiogenic agent exhibit clinical efficacy with an acceptable safety profile in patients with metastatic cervical cancer following progression after initial immunotherapy. Further prospective studies are warranted to investigate this immunotherapy retreatment strategy in patients with metastatic cervical cancer.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author on reasonable request.
Ethical Statement
This study was approved by the Ethics Committee of the Union Hospital of Huazhong University of Science and Technology (20220023).
Acknowledgments
We would like to thank Editage for the English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 81902854).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Waggoner SE. Cervical cancer. Lancet. 2003;361(9376):2217–2225. doi:10.1016/S0140-6736(03)13778-6
3. Tewari KS, Sill MW, Long HJ, et al. Improved survival with bevacizumab in advanced cervical cancer. N Engl J Med. 2014;370(8):734–743. doi:10.1056/NEJMoa1309748
4. Frenel JS, Le Tourneau C, O’Neil B, et al. Safety and efficacy of pembrolizumab in advanced, programmed death ligand 1-positive cervical cancer: results from the phase Ib KEYNOTE-028 trial. J Clin Oncol. 2017;35(36):4035–4041. doi:10.1200/JCO.2017.74.5471
5. Chung HC, Ros W, Delord JP, et al. Efficacy and safety of pembrolizumab in previously treated advanced cervical cancer: results from the phase II KEYNOTE-158 study. J Clin Oncol. 2019;37(17):1470–1478. doi:10.1200/JCO.18.01265
6. Naumann RW, Hollebecque A, Meyer T, et al. Safety and efficacy of nivolumab monotherapy in recurrent or metastatic cervical, vaginal, or vulvar carcinoma: results from the phase I/II CheckMate 358 trial. J Clin Oncol. 2019;37(31):2825–2834. doi:10.1200/JCO.19.00739
7. Lan C, Shen J, Wang Y, et al. Camrelizumab plus Apatinib in patients with advanced cervical cancer (CLAP): a multicenter, open-label, single-arm, Phase II trial. J Clin Oncol. 2020;38(34):4095–4106. doi:10.1200/JCO.20.01920
8. Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N Engl J Med. 2021;385(20):1856–1867. doi:10.1056/NEJMoa2112435
9. Wendel Naumann R, Leath CA. Advances in immunotherapy for cervical cancer. Curr Opin Oncol. 2020;32(5):481–487. doi:10.1097/CCO.0000000000000663
10. Fujita K, Uchida N, Kanai O, Okamura M, Nakatani K, Mio T. Retreatment with pembrolizumab in advanced non-small cell lung cancer patients previously treated with nivolumab: emerging reports of 12 cases. Cancer Chemother Pharmacol. 2018;81(6):1105–1109. doi:10.1007/s00280-018-3585-9
11. Fujita K, Uchida N, Yamamoto Y, et al. Retreatment with anti-PD-L1 antibody in advanced non-small cell lung cancer previously treated with anti-PD-1 antibodies. Anticancer Res. 2019;39(7):3917–3921. doi:10.21873/anticanres.13543
12. Watanabe H, Kubo T, Ninomiya K, et al. The effect and safety of immune checkpoint inhibitor rechallenge in non-small cell lung cancer. Jpn J Clin Oncol. 2019;49(8):762–765. doi:10.1093/jjco/hyz066
13. Katayama Y, Shimamoto T, Yamada T, et al. Retrospective efficacy analysis of immune checkpoint inhibitor rechallenge in patients with non-small cell lung cancer. J Clin Med. 2019;9(1):102. doi:10.3390/jcm9010102
14. Abou Alaiwi S, Xie W, Nassar AH, et al. Safety and efficacy of restarting immune checkpoint inhibitors after clinically significant immune-related adverse events in metastatic renal cell carcinoma. J Immunother Cancer. 2020;8(1):e000144. doi:10.1136/jitc-2019-000144
15. Yang K, Li J, Sun Z, Zhao L, Bai C. Retreatment with immune checkpoint inhibitors in solid tumors: a systematic review. Ther Adv Med Oncol. 2020;12:1758835920975353. doi:10.1177/1758835920975353
16. Markham A, Keam SJ. Camrelizumab: first global approval. Drugs. 2019;79(12):1355–1361. doi:10.1007/s40265-019-01167-0
17. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
18. National Cancer Institute. Common terminology criteria for adverse events (CTCAE) common terminology criteria for adverse events (CTCAE) v5,0.; 2017. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm.
19. Gobbini E, Toffart AC, Pérol M, et al. Immune checkpoint inhibitors rechallenge efficacy in non-small-cell lung cancer patients. Clin Lung Cancer. 2020;21(5):e497–e510. doi:10.1016/j.cllc.2020.04.013
20. Nomura M, Otsuka A, Kondo T, et al. Efficacy and safety of retreatment with nivolumab in metastatic melanoma patients previously treated with nivolumab. Cancer Chemother Pharmacol. 2017;80(5):999–1004. doi:10.1007/s00280-017-3444-0
21. Giaj Levra M, Cotté FE, Corre R, et al. Immunotherapy rechallenge after nivolumab treatment in advanced non-small cell lung cancer in the real-world setting: a national data base analysis. Lung Cancer. 2020;140:99–106. doi:10.1016/j.lungcan.2019.12.017
22. Blasig H, Bender C, Hassel JC, et al. Reinduction of PD1-inhibitor therapy: first experience in eight patients with metastatic melanoma. Melanoma Res. 2017;27(4):321–325. doi:10.1097/CMR.0000000000000341
23. Long GV, Schachter J, Arance A, et al. Long-term survival from pembrolizumab (pembro) completion and pembro retreatment: phase III KEYNOTE-006 in advanced melanoma. J Clin Oncol. 2020;38(15_suppl):10013. doi:10.1200/JCO.2020.38.15_suppl.10013
24. Herbst RS, Garon EB, Kim DW, et al. Long-term outcomes and retreatment among patients with previously treated, programmed death-ligand 1‒positive, advanced non‒small-cell lung cancer in the KEYNOTE-010 study. J Clin Oncol. 2020;38(14):1580–1590. doi:10.1200/JCO.19.02446
25. Fernandez AMA, O’Day SJ, Merino LC, et al. LBA44 Lenvatinib (len) plus pembrolizumab (pembro) for advanced melanoma (MEL) that progressed on a PD-1 or PD-L1 Inhibitor: initial results of LEAP-004. Ann Oncol. 2020;31:S1173. doi:10.1016/j.annonc.2020.08.2274
26. Sandhu SK, Atkinson VG, Cao MG, et al. Interim analysis of a phase Ib study of cobimetinib plus atezolizumab in patients with advanced BRAFV600 wild type melanoma progressing on prior anti-PD-L1 therapy. Ann Oncol. 2019;30:V554. doi:10.1093/annonc/mdz255.046
27. Vera Aguilera JV, Paludo J, McWilliams RR, et al. Chemo-immunotherapy combination after PD-1 inhibitor failure improves clinical outcomes in metastatic melanoma patients. Melanoma Res. 2020;30(4):364–375. doi:10.1097/CMR.0000000000000669
28. Galluzzi L, Buqué A, Kepp O, Zitvogel L, Kroemer G. Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell. 2015;28(6):690–714. doi:10.1016/j.ccell.2015.10.012
29. Rebuzzi SE, Facchinetti F, Tiseo M. Anti-angiogenesis boosts chemo-immunotherapy in patients with EGFR mutations or baseline liver metastases: insights from IMpower150 study. Transl Cancer Res. 2019;8(Suppl6):S612–S617. doi:10.21037/tcr.2019.06.21
30. Fukumura D, Kloepper J, Amoozgar Z, Duda DG, Jain RK. Enhancing cancer immunotherapy using antiangiogenics: opportunities and challenges. Nat Rev Clin Oncol. 2018;15(5):325–340. doi:10.1038/nrclinonc.2018.29
31. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.