")
Back to Journals » International Journal of General Medicine » Volume 14
Clinical, Echocardiographic, and Therapeutic Characteristics of Heart Failure in Patients with Preserved, Mid-Range, and Reduced Ejection Fraction: Future Directions
Authors Alem MM
Received 26 October 2020
Accepted for publication 21 January 2021
Published 16 February 2021 Volume 2021:14 Pages 459—467
DOI https://doi.org/10.2147/IJGM.S288733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Manal M Alem
Department of Pharmacology, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Manal M Alem
Department of Pharmacology, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University, PO Box 1982, Dammam, 31441, Saudi Arabia
Email [email protected]
Background: Heart failure (HF) is recognized as a worldwide epidemic. Definitions and risk stratification are usually based upon measurements of left ventricular ejection fraction (LVEF) but such classifications reflect an underlying spectrum of different pathologic, phenotypic, and therapeutic patterns.
Methods: This was a retrospective cohort study of HF patients in Saudi Arabia. Patients were divided into three categories based on LVEF: those with preserved ejection fraction (EF) (EF≥ 50%, HFpEF); those with mid-range EF (EF 40– 49%, HFmrEF); and those with reduced EF (EF < 40%, HFrEF). Their demographics, co-morbid conditions, echocardiographic findings, pharmacological treatments and all-cause mortality (ACS) after a follow-up period of 24 months were compared.
Results: A total of 293 HF patients were identified (mean age: 63 years). In total, 65% were males, 79% were Saudi nationals, and 70% had type 2 diabetes mellitus (DM). Classification based on EF was established in 288 patients: HFpEF (105 patients, 36.5%), HFmrEF (49, 17.0%), and HFrEF (134, 46.5%). The 3 groups differed in sex distribution: 51% females in the HFpEF group and 78% males in the HFrEF group (P< 0.001). Body mass index (BMI) was highest in the HFpEF group and lowest in the HFrEF group (31.5 vs 26.6; P< 0.001). Although systolic blood pressure (SBP in mmHg) was highest in patients with HFpEF, left ventricular mass index (LVMI in g/cm2) was highest in patients with HFrEF 121.00 (94.50, 151.50), and eccentric hypertrophy was the dominant LV geometrical characteristic (54.6%). HFrEF patients had the highest use of ACE inhibitors (60.5%), loop diuretics (79.9%), and aldosterone receptor antagonists (56.7%) (P values; 0.009, 0.007, and < 0.001, respectively). A total of 42 deaths occurred during follow-up: HFpEF (17 events), HFmrEF (3 events) and HFrEF (22 events) (Logrank test P=0.189).
Conclusion: This Saudi HF population shows similarities to other populations: EF category distribution, sex distribution, therapeutic trends, and survival outcomes. However, findings related to the underlying risk factors, namely type 2 DM and obesity, have identified HFpEF as an emerging threat in this (relatively) young population.
Keywords: HFpEF, HFmrEF, HFrEF, Saudi Arabia, left ventricular mass, left ventricular geometry, survival
Introduction
For more than twenty years, heart failure (HF) has been recognized as a pandemic1 and up-to-date, evidence-based management guidelines have been established. In addition, the importance of early detection and the need for prevention strategies are also recognized. Traditionally, the classification of heart failure has been based upon the patient’s clinical or echocardiographic characteristics, particularly left ventricular systolic function. However, it is known that heart failure involves a variety of patient sub-types: symptomatic vs asymptomatic left ventricular dysfunction; left-sided vs right-sided HF; acute vs chronic HF; and systolic vs diastolic HF. Based on the American College of Cardiology/American Heart Association,2 and the European Society of Cardiology guidelines,3 terminologies related to ejection fraction (EF) have formed the basis for the latest classification of HF patients: thus, reduced EF (EF <40%, HFrEF); preserved EF (EF≥50%, HFpEF); and mid-range EF (EF 40–49%, HFmrEF). The Framingham Heart Study, although with outdated definitions, emphasized that there was a distinction between the two distinct entities: HFpEF (defined with EF >45%) and HFrEF (defined with EF≤45%).4 Systolic blood pressure (SBP), atrial fibrillation, and female sex were found to be associated with HFpEF, whereas prior myocardial infarction, left bundle branch block, higher serum potassium, and male sex were risk factors for HFrEF. However, surprisingly, there was no significant difference in survival between the two categories.4
In Saudi Arabia, there is a paucity of data on the detailed characteristics of HF patients. Data from 3 earlier studies that enrolled a total of 3077 patients from the cities of Riyadh (Riyadh province) and Jeddah (Makkah province) identified that the HF population of Saudi Arabia is younger than other populations and has a higher prevalence of type 2 DM.5–7 The male sex dominated in patients with reduced EF, while the female sex dominated in patients with preserved EF. In terms of the total number of enrolled HF patients, two studies reported a dominance of patients with reduced EF over those with preserved EF,5,6 while the third reported the opposite.7 Therefore, this present observational study seeks not only to report the clinical, echocardiographic, and therapeutic characteristics of HF using another representative sample of the Saudi HF population (Eastern province), but also to identify characteristics that may be relevant elsewhere.
Methods
Study Design
This retrospective, observational, cohort study was based on secondary analysis of existing data of patients with chronic heart failure with New York Heart Association (NYHA) class I–IV to assess the clinical features, echocardiographic findings, therapeutic trends, and mortality during a 24-month follow-up period based on EF categories. The diagnosis of heart failure in the enrolled patients was in accordance with the American College of Cardiology/American Heart Association.8 The reporting system of this study was in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.9
Study Setting
Patients’ data were extracted from two studies, the first was based in King Fahd Hospital of the University (KFHU), Al-Khobar, Saudi Arabia, from Jan 1st, 2005 to Dec 31st, 2016, and the second was based in the Heart Center, King Faisal Specialist Hospital and Research Center (KFSH-RC), Riyadh, Saudi Arabia, from Jan 1st, 2010 to Dec 31st, 2017.
Ethical Approval
The first study protocol and the consent process were approved by the Institutional Review Board (IRB-2020-306-Pharm), Deanship of Scientific Research, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. Verbal informed consent was obtained from the patients or their next of kin by telephone conversation because survival data was required at 24 months. The second study protocol was approved by the Research Ethics Committee at KFSH-RC (Project 2181034), Riyadh, Saudi Arabia. A waiver of informed consent was obtained based on study design, lack of intervention, and lack of survival status checks. Both studies were conducted in accordance with the Declaration of Helsinki (2013), the ICH Harmonized Tripartite Good Clinical Practice Guidelines, and the laws of Saudi Arabia.
Inclusion and Exclusion Criteria
The following inclusion and exclusion criteria applied at time of baseline data collection or study entry.
Inclusion Criteria
- Age > 18 years
- Chronic heart failure (of any aetiology) with New York Heart Association NYHA functional class I–IV.
Exclusion Criteria
- Acute heart failure
- Serum Hb ˂ 9 gr/dl and hematocrit ˂ 30% due to anemia of any etiology
- Malignancy
Recruitment and Variables
Recruitment of eligible patients in both studies was described elsewhere.10,11 The variables collected were: patient’s demographic information, NYHA functional class, etiology of heart failure, and co-morbidities (systemic hypertension, diabetes mellitus (DM), dyslipidemia, arrhythmias (including atrial fibrillation (AF)), transient ischemic attacks (TIA), and stroke. Patients’ cardiac medications, anti-diabetic drugs and other relevant drugs were also documented. Echocardiographic parameters were extracted to calculate left ventricular mass (LVM; in grams) according to the guidelines of the American Society of Echocardiography and the European Association of Cardiovascular Imaging, using linear measurements derived from transthoracic echocardiogram 2-D images. LVM along with LV relative wall thickness allowed derivation of LV geometry. LVM was indexed to body surface area and referred to left ventricular mass index (LVMI; in g/m2)12
Statistical Analysis
Baseline data are reported as mean ± Standard Deviation (SD) for continuous variables and as number and percentages for categorical variables. Median and interquartile ranges were used for non-normally distributed data. Comparison of means between the three patient groups was by one-way analysis of variance, Kruskal–Wallis test, and chi-square test depending on the type of data. Kaplan–Meier survival analysis with Logrank test was used to compare survival curves for the three patients groups based on LVEF. All statistical analyses were performed using Minitab statistical software (version18, Minitab Inc., State College, PA, USA) and MedCalc statistical software (version 19.1.13, MedCalc software, Ostend, Belgium). A two-sided P value of ˂0.05 was considered statistically significant.
Results
Clinical and Echocardiographic Characteristics
A total of 293 patients were initially identified; mean age 62.75 ± 13.30 years, 64.85% male and 79.18% Saudi nationals but there was no record of EF in 5 patients. Therefore, from the records of 288 patients, the main findings were as follows: the rank order of frequency was HFrEF, HFpEF and HFmrEF. Patients were matched for age across the three categories but there were more males with HFrEF and HFmrEF whereas females were more prevalent in the HFpEF category, which also recorded a significantly higher body weight and body mass index than the other two (Table 1 and Figure 1). Regarding clinical co-morbidities, higher percentages of patients in the HFrEF and HFmrEF categories had underlying ischemic heart disease (IHD) (compared to HFpEF), however, such trend did not reach statistical significance. Although the three groups were matched for a history of systemic hypertension, the patients with HFpEF were found to have a significantly higher systolic blood pressure: in turn, those with HFrEF had higher LVM, LVMI, and worse LV geometry, ie, higher percentage of eccentric hypertrophy/concentric hypertrophy in comparison to normal geometry/concentric remodeling (Table 1). The prevalence of chronic kidney disease (defined as eGFR of less than 60 mL/min/1.73 m2) in HFpEF, HFmrEF, and HFrEF were 40.0%, 26.5%, and 36.1%, respectively (P=0.267), while that of dyslipidemia (reported in 236 patients) was 56.0%, 63.2%, and 54.2%, respectively (P=0.631), and history of smoking (reported in 202 patients) was 37.9%, 37.8%, and 51.5%, respectively (P=0.406). The prevalence of atrial fibrillation in the 3 categories did not show a significant difference.
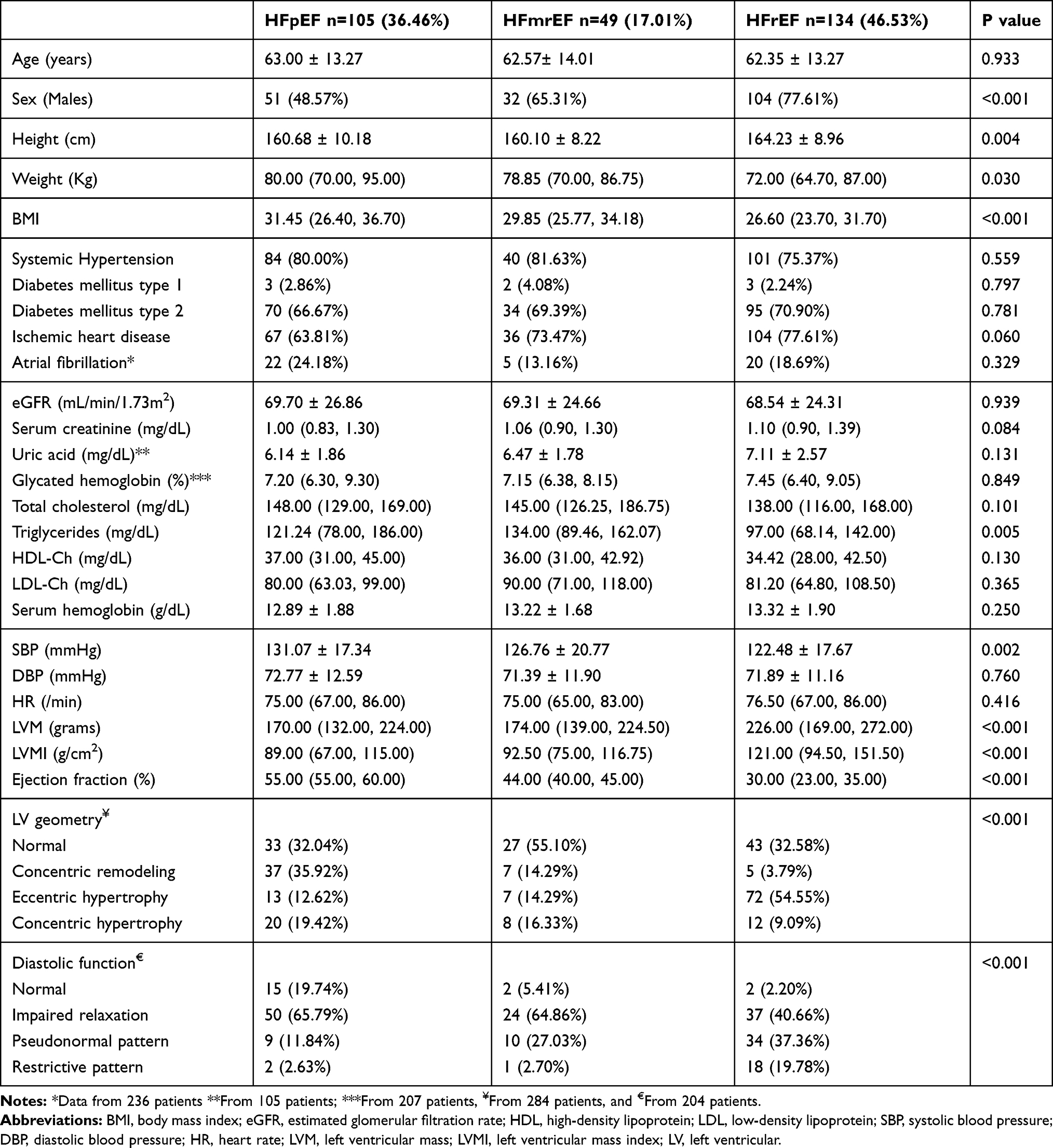 |
Table 1 Clinical and Echocardiographic Characteristics of Study Population |
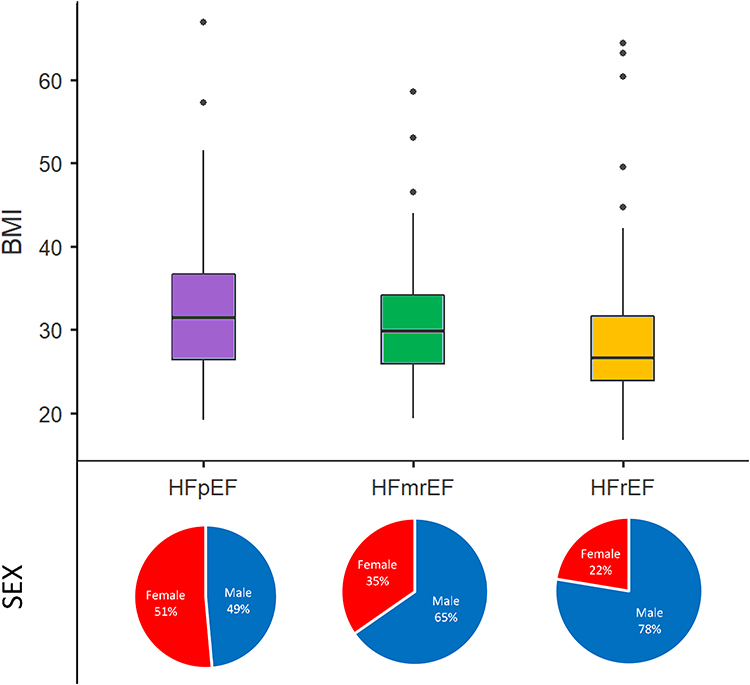 |
Figure 1 Body mass index and sex distribution among the 3 categories of heart failure. BMI comparison – Kruskal–Wallis test (P<0.001). Sex comparison – Chi-square test (P<0.001). |
Diastolic Function
Data on diastolic function was available for 204 patients: 76 patients in HFpEF, 37 patients in HFmrEF, and 91 patients in HFrEF. HFpEF patients had the highest percentage of normal diastolic function (19.74%). The pattern of diastolic dysfunction severity was more pronounced in HFrEF, followed by HFmrEF, and HFpEF (Table 1).
Pharmacological Management
Patients were treated with conventional HF medications (see Table 2); however, the use of ACE inhibitors was significantly less in patients with HFpEF patients as compared with HFmrEF and HFrEF. In addition, patients in the HFrEF group had significantly higher prescription rates for loop diuretics, aldosterone receptor antagonists, and organic nitrates, while those in HFmrEF had higher prescription rates for statins, as compared with the other groups (Table 2).
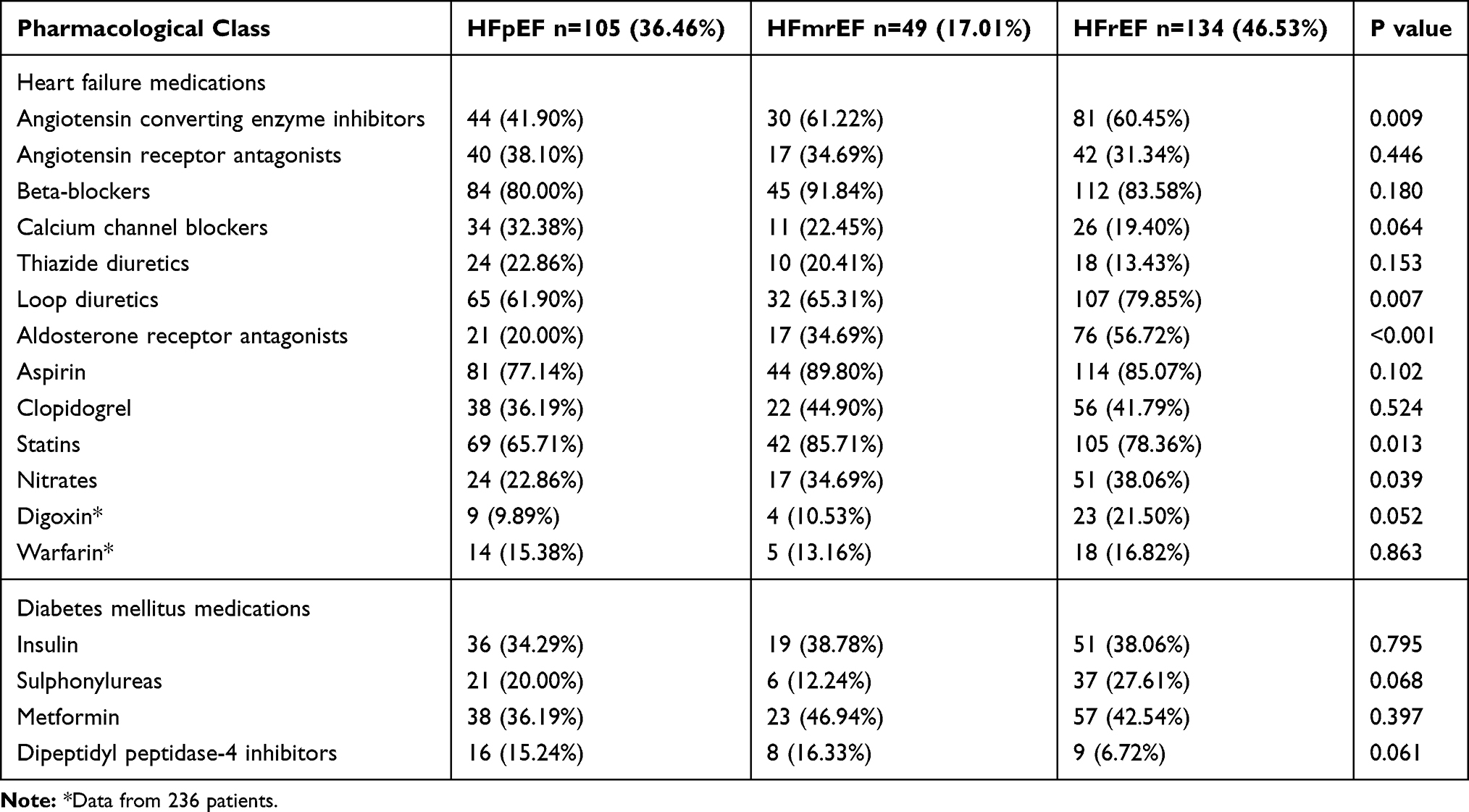 |
Table 2 Pharmacological Management of Study Population |
Survival Analysis
Mortality data was available for 241 patients (236 of which had been classified according to their EF) for 24 months after study entry.
- 1-year mortality was 6.8%, based on 16 fatalities – HFpEF (9 events), HFmrEF (1 event), and HFrEF (6 events) (P=0.264).
- 2-year mortality was 17.8%, based on 42 fatalities – HFpEF (17 events), HFmrEF (3 events), HFrEF (22 events) (P=0.207).
The survival curves of the 3 patient groups over 24 months suggests that the poorest survival was found in HFpEF patients, followed by HFrEF and then HFmrEF, but this comparison was not found to be statistically significant (Figure 2). Disease severity in the 3 categories was known for 230 patients and confirmed that the number of patients in NYHA class III–IV was highest in the HFrEF category (58.1%), in comparison with HFmrEF (39.5%), and HFpEF (37.9%) (P=0.012).
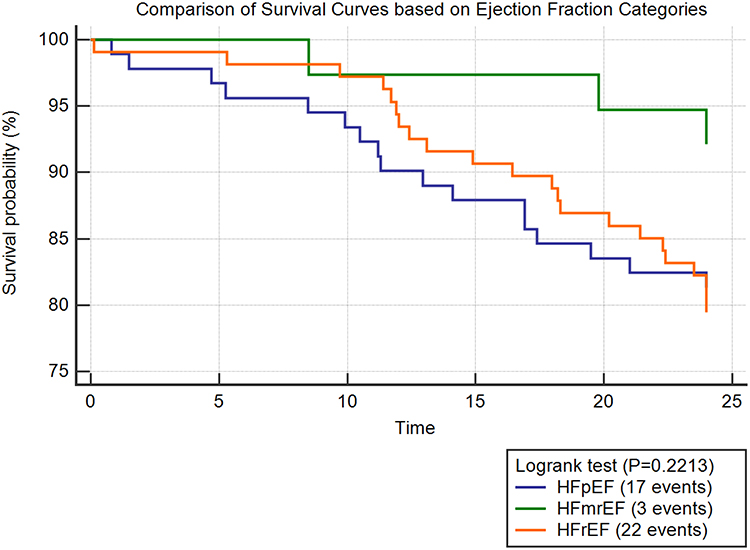 |
Figure 2 Kaplan–Meier survival analysis in patient’s population based on ejection fraction. Abbreviations: HFpEF, heart failure with preserved ejection fraction; HFmrEF, heart failure with mid-range ejection fraction; HFrEF, heart failure with reduced ejection fraction. |
Discussion
We had two principal objectives for embarking on this study: a) Clarification of local issues relating directly to HF patients in Saudi Arabia. b) Identification of additional factors/considerations which may be applicable worldwide.
Local Issues
To the best of our knowledge, only a few studies from Saudi Arabia5–7 have addressed risk stratification for HF patients. The following are the salient points:
- Based on LVEF: HFrEF is more frequent than HFpEF.
- Males are more likely to have reduced EF and IHD is more likely to be a factor.
- BMI was highest in the HFpEF category.
- Despite a history of higher SBP in HFpEF, LVM and LVMI were highest in HFrEF, along with worse LV geometry and more severe diastolic dysfunction.
- Not surprisingly, patients with HFpEF had significantly less use of ACE inhibitors than those with HFrEF, with the latter group having significantly higher use of loop diuretics, aldosterone receptor antagonists, nitrates, and digoxin.
- Considering survival, there was no significant difference in mortality across the 3 categories: presumably an issue of statistical power.
Comparing the Current Results with Other studies at a National Level
With regard to the dominance of LV reduced EF (despite different cut-off values) and male sex, over those with preserved EF and female sex, these present findings are in agreement with two national studies,5,6 whereas a third study reported an opposite pattern,7 with Saudi nationals constituting 43.5% of the participants. With respect to BMI, disease severity (NYHA III–IV), underlying IHD, hypertension, therapeutic trends and mortality, there are general similarities. However, the prevalence of type 2 DM is highest in our cohort (69.6%) as compared with 52.7%,6 and 61.7%.5
International Comparisons
Despite different designs and sample size, the major international studies (CHARM Program,13,14 Framingham Heart study,15 ESC HF long-term registry,16 Swedish Heart Failure registry,17 China Heart Failure Center Registry,18 and others19 have demonstrated similar findings. Overall, however, the Saudi patients were younger with a mean age of 62.7 years, as compared with other studies that had a cumulative age range of 65–82 years.13–21 Our cohort also had a higher BMI of 30.3, as compared with other studies that had a cumulative BMI range of 22–28.6%.14–16,19 In addition, they had a significantly higher prevalence of DM of 69.6%, as compared with other studies that had a cumulative prevalence range of 18–41%,13–20 and a higher prevalence of hypertension of 78.5%, as compared with other studies that had a cumulative prevalence range of 53.3–58.5%.14,16,18,19,21 The proportion of HFpEF in our population (36.5%) was higher than others with a cumulative range of 16–26%.14,16,17 Despite the strong association of atrial fibrillation with HFpEF in the literature,14–17 lack of such association in our cohort was comparable to other populations.19,21 Mortality outcomes and therapeutic approaches were broadly similar to other studies.
Overall, it can be concluded that the Saudi HF population is a high-risk population compared with others. HFpEF, in particular, was associated with obesity, with 80% of patients being overweight/obese (compared, for example, with 71% in the I-PRESERVE trial).20 This strong association is well supported in the literature as a risk factor rather than a comorbid condition.22 Visceral fat, which is a marker of central obesity, was independently associated with LV concentric remodeling.23 Such geometric pattern is the predominant form in HFpEF in our study.
At a molecular level, there are substantial differences related to systemic inflammation and cardiac remodeling depending on the EF category. While HFpEF patients have low-grade chronic and systemic inflammation described as metabolic risk-induced inflammation caused by obesity, DM, hypertension, chronic obstructive pulmonary disease, and others, the inflammatory response in HFrEF is described as sterile inflammation resulting from myocardial ischemic damage.24 These differing inflammatory patterns lead to concentric remodeling in HFpEF25 and to eccentric hypertrophy in HFrEF26: these are the dominant patterns seen in the corresponding groups in our cohort. Further interpretation of high BMI, and left ventricular hypertrophy showed that they are predictors for new onset HFpEF and HFrEF, respectively.15,27 Thus, obesity in the former and LVH in the latter might be risk factors for developing HFpEF and HFrEF, rather than simple co-morbidities.
According to an epidemiological study, the prevalence of HFpEF, relative to HFrEF is reported to be increasing at a rate of 1% per year.28 However, a sub-study of the Global Burden of Disease study in Saudi Arabia reported that the top two risk factors for all-cause years lived with disability were high BMI (41.9% rise between 1990 and 2017) and high fasting blood glucose (18.3% rise between 1990 and 2017).29 Thus, with increasing life expectancy and aging of the population, HFpEF would be expected to increase at a higher rate in Saudi Arabia than other countries.28,30 Finally, the category less studied in the literature, HFmrEF, does exhibit some similarities with the other two categories. While in our population it showed similarities to HFrEF with regard to sex predominance, and underlying IHD, it ranked in the middle with regard to BMI, SBP, LVM, LVMI, and LV diastolic dysfunction. Therefore, HFmrEF in our study showed similarities to other studies in the literature with regard to clinical and therapeutic characteristics13,14,16,17,19,31 but differed in echocardiographic findings.31
Limitations
This study has a number of limitations, with the relatively small sample size being the most important, especially since mortality data was missing for some patients. Additionally, there was insufficient data on brain natriuretic peptide concentrations for comparisons based on EF. Furthermore, there was no information in the patients’ records on non-pharmacological treatments eg exercise therapy or vaccination.
Conclusion
This study confirms the inter-relationships between HFpEF, relatively young age, obesity, and type 2 DM in Saudi Arabia. Whilst, at present, this may be a peculiar problem to the Saudi HF population, requiring preventive strategies at a national level (involving weight loss and physical exercise), similar considerations will obviously apply worldwide. There is a clear need to implement strategies to combat the progressive increase in the new epidemic of HFpEF. For future considerations, there is also the HFmrEF category which requires further epidemiological studies.
Abbreviations
HF, Heart Failure; LVEF, Left Ventricular Ejection Fraction; HFpEF, Heart Failure with preserved Ejection Fraction; HFmrEF, Heart Failure with mid-range Ejection Fraction; HFrEF, Heart Failure with reduced Ejection Fraction; ACM, All-cause mortality; DM, Diabetes Mellitus; BMI, Body Mass Index; SBP, Systolic Blood Pressure; NYHA, New York Heart Association; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; KFHU, King Fahd Hospital of the University; KFSH-RC, King Faisal Specialist Hospital and Research Center; ICH, International Conference on Harmonization; AF, Atrial Fibrillation; LVM, Left Ventricular Mass; LVMI, Left Ventricular Mass Index; SD, Standard Deviation; EF, Ejection Fraction; IHD, Ischemic Heart Disease; ACE, Angiotensin Converting Enzyme; CHARM, Candesartan in Heart failure: Assessment of Reduction in Mortality and Morbidity; I-PRESERVE, Irbesartan in Patients with Heart Failure and Preserved Ejection Fraction.
Data Sharing Statement
The data that support the findings of this study is available on request from the corresponding author (M.M. Alem).
Ethics Approval and Informed Consent
The first study protocol was approved by the institutional review board (IRB-2020-306-Pharm), Deanship of Scientific Research, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia. Verbal informed consents were obtained from the patients included or their next of kin by telephone conversation. The second study was approved by the Research Ethics Committee at KFSH-RC (Project 2181034), Riyadh, Saudi Arabia. A waiver of informed consent was obtained based on study design, lack of intervention, and lack of survival status checks.
Consent for Publication
The author grants Dove Press and International Journal of General Medicine the license of publishing this study.
Funding
This research has not been funded by any source.
Disclosure
The author declares no conflicts of interest for this work.
References
1. Braunwald E. Shattuck lecture–cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337(19):1360–1369. doi:10.1056/NEJM199711063371906
2. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart failure society of America. Circulation. 2017;136(6):e137–e161. doi:10.1161/CIR.0000000000000509
3. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
4. Lee DS, Gona P, Vasan RS, et al. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framingham heart study of the national heart, lung, and blood institute. Circulation. 2009;119(24):3070–3077. doi:10.1161/CIRCULATIONAHA.108.815944
5. Alqahtani M, Alanazi T, Binsalih S, et al. Characteristics of Saudi patients with congestive heart failure and adherence to management guidelines in a tertiary hospital in Riyadh. Ann Saudi Med. 2012;32(6):583–587. doi:10.5144/0256-4947.2012.583
6. Alhabeeb W, Elasfar A, AlBackr H, et al. Clinical characteristics, management and outcomes of patients with chronic heart failure: results from the heart function assessment registry trial in Saudi Arabia (HEARTS-chronic). Int J Cardiol. 2017;235(235):94–99. doi:10.1016/j.ijcard.2017.02.087
7. Subki AH, Almalki MA, Butt NS, et al. Echocardiographic and clinical correlates of ejection fraction among 2000 patients with heart failure in Western Saudi Arabia. Int J Gen Med. 2020;13:281–288. doi:10.2147/IJGM.S251924
8. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239.
9. Vandenbroucke JP, von EE, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):e297. doi:10.1371/journal.pmed.0040297
10. Alem MM. Predictors of mortality in patients with chronic heart failure: is hyponatremia a useful clinical biomarker? Int J Gen Med. 2020;13:407–417. doi:10.2147/IJGM.S260256
11. Alem MM, Aldosari SR, Alkahmous AA, Obad AS, Fagir NM, Al-Ghamdi BS. Effect of long-term allopurinol therapy on left ventricular mass index in patients with ischemic heart disease; a cross-sectional study. Vasc Health Risk Manag. 2019;15:539–550. doi:10.2147/VHRM.S226009
12. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39. doi:10.1016/j.echo.2014.10.003
13. Hillege HL, Nitsch D, Pfeffer MA, et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation. 2006;113(5):671–678. doi:10.1161/CIRCULATIONAHA.105.580506
14. Lund LH, Claggett B, Liu J, et al. Heart failure with mid-range ejection fraction in CHARM: characteristics, outcomes and effect of candesartan across the entire ejection fraction spectrum. Eur J Heart Fail. 2018;20(8):1230–1239. doi:10.1002/ejhf.1149
15. Ho JE, Lyass A, Lee DS, et al. Predictors of new-onset heart failure: differences in preserved versus reduced ejection fraction. Circ Heart Fail. 2013;6(2):279–286. doi:10.1161/CIRCHEARTFAILURE.112.972828
16. Chioncel O, Lainscak M, Seferovic PM, et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC heart failure long-term registry. Eur J Heart Fail. 2017;19(12):1574–1585. doi:10.1002/ejhf.813
17. Lofman I, Szummer K, Dahlstrom U, Jernberg T, Lund LH. Associations with and prognostic impact of chronic kidney disease in heart failure with preserved, mid-range, and reduced ejection fraction. Eur J Heart Fail. 2017;19(12):1606–1614. doi:10.1002/ejhf.821
18. Wang H, Li YY, Chai K, et al. [Contemporary epidemiology and treatment of hospitalized heart failure patients in real clinical practice in China]. Zhonghua Xin Xue Guan Bing Za Zhi. 2019;47(11):865–874. Chinese. doi:10.3760/cma.j.issn.0253-3758.2019.11.004
19. Shiga T, Suzuki A, Haruta S, et al. Clinical characteristics of hospitalized heart failure patients with preserved, mid-range, and reduced ejection fractions in Japan. ESC Heart Fail. 2019;6(3):475–486. doi:10.1002/ehf2.12418
20. Haass M, Kitzman DW, Anand IS, et al. Body mass index and adverse cardiovascular outcomes in heart failure patients with preserved ejection fraction: results from the Irbesartan in heart failure with preserved ejection fraction (I-PRESERVE) trial. Circ Heart Fail. 2011;4(3):324–331. doi:10.1161/CIRCHEARTFAILURE.110.959890
21. Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the community: a study of all incident cases in Olmsted County, Minnesota, in 1991. Circulation. 1998;98(21):2282–2289. doi:10.1161/01.CIR.98.21.2282
22. Tadic M, Cuspidi C. Obesity and heart failure with preserved ejection fraction: a paradox or something else? Heart Fail Rev. 2019;24(3):379–385. doi:10.1007/s10741-018-09766-x
23. Neeland IJ, Gupta S, Ayers CR, et al. Relation of regional fat distribution to left ventricular structure and function. Circ Cardiovasc Imaging. 2013;6(5):800–807. doi:10.1161/CIRCIMAGING.113.000532
24. Simmonds SJ, Cuijpers I, Heymans S, Jones EAV. Cellular and molecular differences between HFpEF and HFrEF: a step ahead in an improved pathological understanding. Cells. 2020;9(1):242. doi:10.3390/cells9010242
25. Zile MR, Gottdiener JS, Hetzel SJ, et al. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation. 2011;124(23):2491–2501. doi:10.1161/CIRCULATIONAHA.110.011031
26. Nauta JF, Hummel YM, Tromp J, et al. Concentric vs. eccentric remodelling in heart failure with reduced ejection fraction: clinical characteristics, pathophysiology and response to treatment. Eur J Heart Fail. 2020;22(7):1147–1155. doi:10.1002/ejhf.1632
27. Savji N, Meijers WC, Bartz TM, et al. The association of obesity and cardiometabolic traits with incident HFpEF and HFrEF. JACC Heart Fail. 2018;6(8):701–709. doi:10.1016/j.jchf.2018.05.018
28. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251–259. doi:10.1056/NEJMoa052256
29. Tyrovolas S, El Bcheraoui C, Alghnam SA. The burden of disease in Saudi Arabia 1990–2017: results from the global burden of disease study 2017. Lancet Planet Health. 2020;4(5):e195–e208. doi:10.1016/S2542-5196(20)30075-9
30. Oktay AA, Rich JD, Shah SJ. The emerging epidemic of heart failure with preserved ejection fraction. Curr Heart Fail Rep. 2013;10(4):401–410. doi:10.1007/s11897-013-0155-7
31. Ozlek B, Ozlek E, Agus HZ, et al. Patients with HFpEF and HFmrEF have different clinical characteristics in Turkey: a multicenter observational study. Eur J Intern Med. 2019;61:88–95. doi:10.1016/j.ejim.2018.11.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.