")
Back to Journals » International Medical Case Reports Journal » Volume 15
Clinical Course of Two Patients with COVID-19 Respiratory Failure After Administration of the Anticancer Small Molecule, RRx-001
Authors Hammond TC, Lee RC, Oronsky B , Reid TR, Caroen S, Juarez TM, Gill J, Heng A, Kesari S
Received 23 September 2022
Accepted for publication 13 December 2022
Published 15 December 2022 Volume 2022:15 Pages 735—738
DOI https://doi.org/10.2147/IMCRJ.S389690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Terese Catherine Hammond,1,2 Raymond C Lee,1,3 Bryan Oronsky,4 Tony R Reid,4 Scott Caroen,4 Tiffany M Juarez,2 Jaya Gill,5 Annie Heng,2 Santosh Kesari1,2,5
1Providence St. Johns Health Center, Santa Monica, CA, USA; 2John Wayne Cancer Institute, Santa Monica, CA, USA; 3Cardiovascular Thoracic Institute, Keck School of Medicine of USC, Los Angeles, CA, USA; 4EpicentRx, Inc., La Jolla, CA, USA; 5Pacific Neuroscience Institute, Santa Monica, CA, USA
Correspondence: Bryan Oronsky, EpicentRx, Inc, 11099 North Torrey Pines Road, La Jolla, CA, 92037, USA, Tel +1 858 947-6635, Fax +1 858 724-3080, Email [email protected]
Abstract: Two critically ill COVID-19 infected patients, who had exhausted all available treatment options, were treated with the small-molecule RRx-001 with subsequent improvement. RRx-001, a first-in-class small molecule with anti-inflammatory, vascular normalizing and macrophage-repolarizing properties, has been safely administered 300+ patients in clinical trials. This is the first report of RRx-001 treatment of COVID-19.
Keywords: COVID-19, SARS-CoV-2, critical care, ARDS, RRx-001, nitric oxide, viral diseases
Background
RRx-001 (N-(bromoacetyl)-3,3-dinitroazetidine) is a hypoxia-activated, small-molecule nitric oxide (NO) donating immunotherapeutic with minimal toxicity, which also mediates NLRP3 inhibition,1 Nrf2 and p53 upregulation, NFκB inhibition and platelet deaggregation.2–4 The main impetuses to evaluate RRx-001 in COVID-19 cases and more generally in patients with cardiorespiratory disease are 1) its favorable safety profile in over 300 patients with cancer,5 many of whom have been and are highly comorbid due to older age and tobacco use, 2) evidence of anti-inflammatory properties mediated through NLRP3 inflammasome inhibition based on evidence that an overactivation of inflammasome signaling is a driver of severe cases of COVID-19,6 3) its preclinical alleviation of some of the cardiopulmonary complications endemic to severe COVID-19 such as pulmonary artery hypertension, heart failure,7 vasospasm,8 thromboembolism, and shock,9 4) evidence of antiviral properties in the form of activity against Ebola and 5) hypoxia-mediated generation of nitric oxide,10 a free radical species that induces vasodilatory, bronchodilatory and antimicrobial effects. This case report summarizes the clinical courses of 2 severe COVID-19 patients treated under compassionate use protocols with RRx-001.
Case Reports
Case 1
The first patient is a 59-year-old severely ill COVID-19 male patient comorbid for hypothyroidism, diabetes mellitus type II and hypertension with acute respiratory distress syndrome (ARDS) on VV-ECMO who received four 4 mg doses of RRx-001 given twice weekly intravenously for two weeks. Previous treatments included hydroxychloroquine, azithromycin, convalescent plasma, tocilizumab, meropenem and vancomycin. The CT result showed bilateral ground glass dense opacities (GGOs). Following his initial treatment with RRx-001, for which no adverse events or drug–drug interactions were observed, hemodynamic parameters stabilized, and interstitial GGOs decreased. He was able to wean from VV-ECMO, although he continued to require mechanical ventilation via tracheostomy and was ultimately discharged forty-six days later to a tertiary center for lung transplant evaluation due to clinical signs of pulmonary fibrosis. There he underwent surgical intervention for a gangrenous gallbladder and was discharged to a subacute nursing facility to recuperate.
Case 2
The second patient is a 36-year-old severely ill morbidly obese male with COVID-19 pneumonia, who was transferred from an outside hospital for VV-ECMO initiation. On day 24 of hospitalization, he continued to be profoundly hypoxemic despite 100% oxygen supplementation, maximal VV-ECMO and high-pressure control ventilation. His course was also complicated by bilateral pneumothoraces. Given his grave condition, he was treated with four 4 mg doses of RRx-001 given twice weekly intravenously over two weeks. Previous treatments included plasma exchange, corticosteroids and tocilizumab. At the time of treatment with RRx-001, he was three weeks into his hospitalization and remained severely hypoxemic despite prone positioning, maximal VV-ECMO, tracheostomy and ventilatory support and had received treatment with multiple courses of antibiotics including Vancomycin, levofloxacin, ganciclovir, meropenem, piperacillin/tazobactam, linezolid and ceftazidime and therapeutic anticoagulation. Following his initial treatment with RRx-001, for which no adverse events or drug–drug interactions were observed, the patient clinically and radiographically improved to the point of VV-ECMO decannulation after 45 days on pump and was successfully discharged back to his original institution 59 days after admission. His chest tubes and tracheostomy were subsequently discontinued, and he was discharged home 109 days after his initial admission for COVID-19 on 2 liters nasal cannula oxygen.
Conclusion
In an attempt to keep pace with the rapid spread of the pandemic and the near daily revelations about the complex, protean and system-wide clinical manifestations of SARS-CoV-2, over 300 trials have been launched with repurposed antivirals like hydroxychloroquine and chloroquine, immunomodulators like tocilizumab, experimental agents like RRx-001 and vitamin C in what has been described as a “tsunami” and a “torrent”.11,12 Whether this inundation with 300+ trials is counterproductive, because it spreads resources (and patients) thin and actually renders clinical investigation less conclusive, or whether it is an ethical and moral imperative to evaluate as many therapies as possible, in the event that one or more of them provides evidence of benefit, is a matter of debate.
In the case of RRx-001, it was administered, in desperation, under an FDA emergency compassionate use as a “Hail Mary” due to the lack of any remaining known adequate therapies, all other potential ones having already been deployed in the ICU, failure to qualify for existing clinical trials nearby, and because the probable risk from RRx-001, as a minimally toxic anticancer agent in a Phase 3 clinical trial13 with anti-inflammatory properties was deemed to be much less than the risk of imminent death from COVID-19 and acute respiratory distress syndrome (ARDS).14 Compassionate use, which is also known as expanded access, refers to the use of an unapproved drug like RRx-001 for individual patients in an “n-of-1” setting outside of a clinical trial.15
Much has been written about the pros and cons of “n-of-1” treatment.16 While it is certainly true that generalizability to a broader population is impossible, especially in this case given the marked heterogeneity of COVID-19 and ARDS in terms of presentation, course, and outcomes,17 it is equally true that the more granular data on individual patients, which they provide, may identify unintended/unexpected effects that are less evident and discoverable in an entire patient population where the law of averages operate.18 The clinical improvement of these two RRx-001-treated patients that a priori were deemed likely to die from COVID-19 and ARDS potentially lends support to the hypothesis that the anti-inflammatory and NO-donating effects19 of RRx-001 increased blood flow to ischemic tissues and ameliorated inflammatory and oxidative damage through NLRP3 inhibition since RRx-001 has been found in in vitro and in vivo experiments to bind directly to and block the NLRP3 inflammasome1 as well as Nrf2 and p53 upregulation. RRx-001 consists of a highly strained four-membered ring, an azetidine, which is substituted with two strongly electron-withdrawing nitro groups. Under conditions of severe hypoxia and acidosis, the ring fragments and liberates the vasodilatory antiviral agent, nitric oxide.2,20 A table, which demonstrates clinical characteristics of the two patients is shown in Table 1.
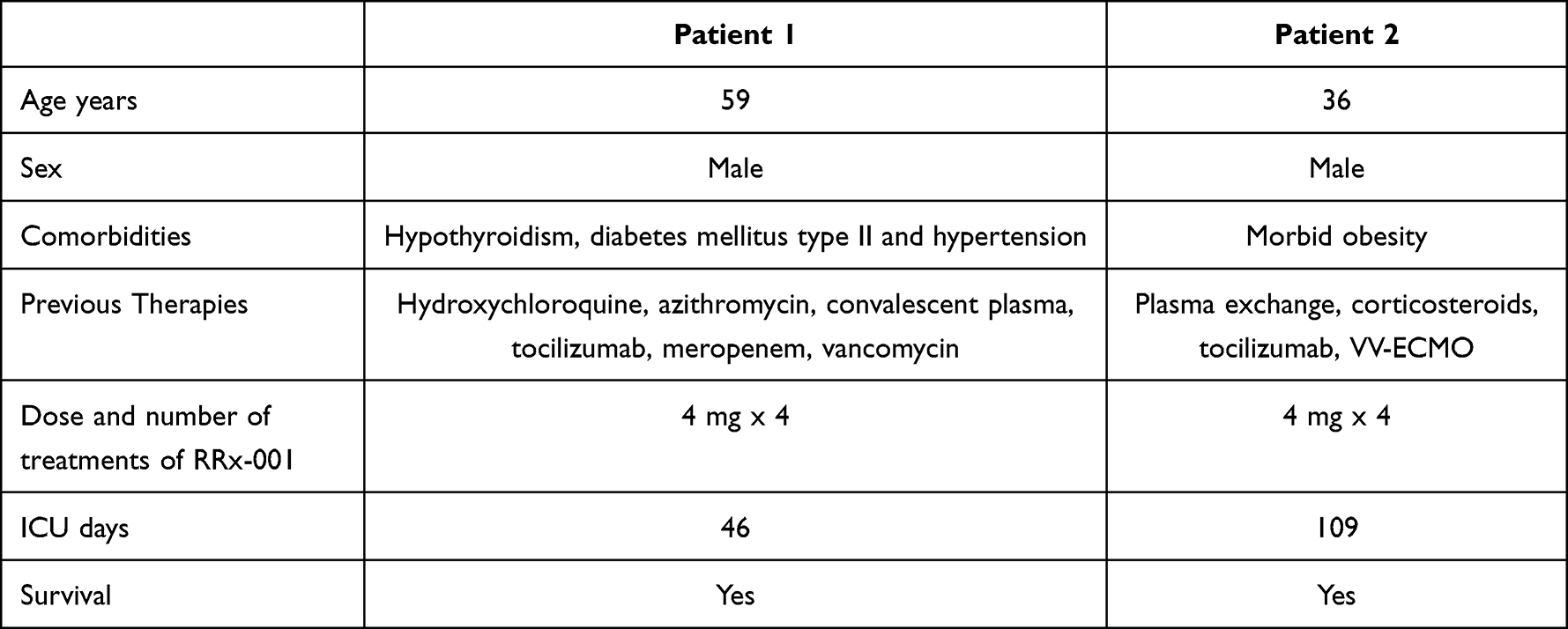 |
Table 1 Characteristics of Two Patients |
It is possible that the clinical improvement that was documented after treatment with RRx-001 was not due to RRx-001; rather these patients experienced an inflammatory lung process, which coincidentally may have peaked in severity around the time of enrollment or that a confounding effect from one or more of the other prior treatment regimens was present. Nevertheless, given the lack of any documented adverse effects or drug–drug interactions with RRx-001, further controlled trials enrolling larger sample of patients with COVID-19 and/or severe cardiopulmonary failure are warranted, especially with the current rampant infectivity of the Omicron subtype of the coronavirus, which is increasingly immune to vaccines and monoclonal antibodies.
Abbreviations
ARDS, acute respiratory distress syndrome; COVID-19, novel coronavirus disease 2019; NO, nitric oxide; NRF2, nuclear factor erythroid 2-related factor 2; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; VV-ECMO, venovenous extracorporeal membrane oxygenation.
Ethical Approval
The study was approved by the institutional review board at the treating medical centers.
Consent to Publish
Informed consent to publish was obtained from the patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
BO, SC, TRR are employed by EpicentRx, Inc. TCH, RCL, TMJ, JG, AH, SK have no conflicts to disclose in this work.
References
1. Chen Y, He H, Lin B, et al. RRx-001 ameliorates inflammatory diseases by acting as a potent covalent NLRP3 inhibitor. Cell Mol Immunol. 2021;18:1425–1436. doi:10.1038/s41423-021-00683-y
2. Oronsky B, Guo X, Wang X, et al. Discovery of RRx-001, a Myc and CD47 downregulating small molecule with tumor targeted cytotoxicity and healthy tissue cytoprotective properties in clinical development. J Med Chem. 2021;64(11):7261–7271. doi:10.1021/acs.jmedchem.1c00599
3. Oronsky B, Knox S, Cabrales P, Oronsky A, Reid TR. Desperate times, desperate measures: the case for RRx-001 in the Treatment of COVID-19. Semin Oncol. 2020;47(5):305–308. doi:10.1053/j.seminoncol.2020.07.002
4. Oronsky B, Oronsky N, Cabrales P. Platelet inhibitory effects of the phase 3 anticancer and normal tissue cytoprotective agent, RRx-001. J Cell Mol Med. 2018;22(10):5076–5082. doi:10.1111/jcmm.13791
5. Reid T, Oronsky B, Scicinski J. Safety and activity of RRx-001 in patients with advanced cancer: a first-in-human, open-label, dose-escalation Phase 1 study. Lancet Oncol. 2015;16(9):1133–1142. doi:10.1016/S1470-2045(15)00089-3
6. Vora SM, Lieberman J, Wu H. Inflammasome activation at the crux of severe COVID-19. Nat Rev Immunol. 2021;21(11):694–703. doi:10.1038/s41577-021-00588-x
7. Oronsky B, Ao-Ieong ESY, Yalcin O, Carter CA, Cabrales P. Cardioprotective effect of phase 3 clinical anticancer agent, RRx-001, in doxorubicin-induced acute cardiotoxicity in mice. Mol Pharm. 2019;16(7):2929–2934. doi:10.1021/acs.molpharmaceut.9b00150
8. Yalcin O, Oronsky B, Carvalho LJ, Kuypers FA, Scicinski J, Cabrales P. From METS to malaria: RRx-001, a multi-faceted anticancer agent with activity in cerebral malaria. Malar J. 2015;14:218. doi:10.1186/s12936-015-0720-5
9. Brouse C, Ortiz D, Su Y, Oronsky B, Scicinski J, Cabrales P. Impact of hemoglobin nitrite to nitric oxide reductase on blood transfusion for resuscitation from hemorrhagic shock. Asian J Transfus Sci. 2015;9(1):55–60. doi:10.4103/0973-6247.150952
10. Fens MH, Cabrales P, Scicinski J, et al. Targeting tumor hypoxia with the epigenetic anticancer agent, RRx-001: a superagonist of nitric oxide generation. Med Oncol. 2016;33(8):85. doi:10.1007/s12032-016-0798-9
11. Mucke HAM. COVID-19 and the drug repurposing tsunami. Assay Drug Dev Technol. 2020;18(5):211–214. doi:10.1089/adt.2020.996
12. Mullard A. Flooded by the torrent: the COVID-19 drug pipeline. Lancet. 2020;395(10232):1245–1246. doi:10.1016/S0140-6736(20)30894-1
13. Oronsky B, Reid TR, Larson C, et al. REPLATINUM phase III randomized study: rRx-001 + platinum doublet versus platinum doublet in third-line small cell lung cancer. Future Oncol. 2019;15(30):3427–3433. doi:10.2217/fon-2019-0317
14. FDA. Expanded access (compassionate use); 2016. Available from: http://www.fda.gov/NewsEvents/PublicHealthFocus/ExpandedAccessCompassionateUse/default.htm.
15. Borysowski J, Ehni HJ, Górski A. Ethics review in compassionate use. BMC Med. 2017;15(1):136. doi:10.1186/s12916-017-0910-9
16. Lillie EO, Patay B, Diamant J, Issell B, Topol EJ, Schork NJ. The n-of-1 clinical trial: the ultimate strategy for individualizing medicine? Per Med. 2011;8(2):161–173. doi:10.2217/pme.11.7
17. Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi:10.1001/jama.2016.0291
18. Kravitz RL, Duan N, Braslow J. Evidence-based medicine, heterogeneity of treatment effects, and the trouble with averages. Milbank Q. 2004;82(4):661–687. doi:10.1111/j.0887-378X.2004.00327.x
19. Mir JM, Maurya RC. Nitric oxide as a therapeutic option for COVID-19 treatment: a concise perspective. New J Chem. 2020;45:1774–1784. doi:10.1039/D0NJ03823G
20. Zamanian RT, Pollack CV, Gentile MA, et al. Outpatient inhaled nitric oxide in a patient with vasoreactive idiopathic pulmonary arterial hypertension and COVID-19 infection. Am J Respir Crit Care Med. 2020;202:130–132. doi:10.1164/rccm.202004-0937LE
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.