")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Clinical Characteristics of Women with ADHD in Japan
Authors Hayashi W , Suzuki H, Saga N, Arai G, Igarashi R, Tokumasu T, Ota H, Yamada H, Takashio O, Iwanami A
Received 12 October 2019
Accepted for publication 23 November 2019
Published 4 December 2019 Volume 2019:15 Pages 3367—3374
DOI https://doi.org/10.2147/NDT.S232565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Wakaho Hayashi,1,2 Hirohisa Suzuki,3 Nobuyuki Saga,1,2 Gosuke Arai,1,2 Reiko Igarashi,1,2 Takahiro Tokumasu,3 Haruhisa Ota,1,2 Hiroki Yamada,1,2 Osamu Takashio,1,2 Akira Iwanami1,2
1Department of Psychiatry, Showa University School of Medicine, Setagaya-ku, Tokyo 157-8577, Japan; 2Department of Psychiatry, Showa University Karasuyama Hospital, Setagaya-ku, Tokyo 157-8577, Japan; 3Department of Psychiatry, Showa University Northern Yokohama Hospital, Yokohama-shi, Kanagawa 224-8503, Japan
Correspondence: Wakaho Hayashi
Department of Psychiatry, Showa University Karasuyama Hospital, 6-11-11 Kitakarasuyama, Setagaya-ku, Tokyo 157-8577, Japan
Tel +81-3-3300-5231
Fax +81-3-3308-9710
Email [email protected]
Purpose: Although gender differences have been reported in various aspects of adult attention-deficit hyperactivity disorder (ADHD), such as prevalence, comorbidities, and social functioning, there have been few such studies conducted in Japan. Our research investigated gender differences in sociodemographic and clinical characteristics of adults with ADHD in a Japanese clinical sample. Due to unique Japanese cultural ideals and expectations of women’s behavior that are in opposition to ADHD symptoms, we hypothesized that women with ADHD experience more difficulties and present more dysfunctions than men. We tested the following hypotheses: first, women with ADHD have more comorbidities than men with ADHD; second, women with ADHD experience more social hardships than men, such as having less full-time employment and being more likely to be divorced.
Patients and methods: The subjects were 335 outpatients with a DSM-5 ADHD diagnosis, who visited our ADHD specialty clinic at Showa University Karasuyama Hospital in central Tokyo between April 2015 and March 2016. Sociodemographic and clinical characteristics were collected, and gender differences were compared.
Results: Results fully supported our hypotheses: women had a significantly higher psychiatric comorbidity rate, were significantly less likely to be a full-time employee, and were significantly more likely to be divorced than men with ADHD.
Conclusion: Consistent with research in other countries, women with ADHD have greater impairments than men with ADHD in Japan. The importance of understanding gender differences of ADHD-diagnosed adults within a sociocultural context is highlighted.
Keywords: ADHD, adults, gender difference, Japan
Introduction
Although gender difference is one of the crucial factors in understanding mental disorders,1,2 few studies of adult ADHD exist; in particular, research focusing on women with ADHD is lacking globally and in individual contexts. Historically, ADHD has been thought of as a childhood and male-dominant disorder;3,4 however, research over the past few years has found that ADHD symptoms persist well into adulthood5–8 and that prevalence in adults is similar between genders.9,10 Some researchers have argued that girls have fewer externalizing and overt symptoms of ADHD11,12 and that, as a result, they are likely to remain undiagnosed,11,13–15 and indeed, later diagnosis of women makes the prevalence similar between genders in adults.16,17 Thus, with an approximately 2.5% prevalence worldwide18,19 and a sizable group of affected women, it is important to investigate their clinical characteristics in adulthood in comparison to those of men with ADHD.
ADHD in adults is associated with significant functional impairments across multiple domains of life, including work, home, school, and social relations.20 Although findings remain inconclusive regarding gender differences, women with ADHD may face greater difficulties than their male counterparts in several areas. For example, Fedele and colleagues21 found that female college students with ADHD experience higher levels of impairment than male college students with ADHD in home life, social life, education, money management, and daily life activities. In terms of work, Fredriksen and colleagues22 found that compared to men, significantly more women with ADHD were long-term work-disabled (either unemployed but looking for work or completely out of work). They suggested the possibility that women are more prone to working in an ADHD-incompatible work environment or more subject to the disabling consequences of ADHD in a vocational context. Regarding social relations, Robin and Payson23 studied couples in which one spouse had ADHD and found significantly more problems reported by non-ADHD partners if the affected spouses were women. They also discussed the burden of gender roles and expectations placed on women, which may increase the hardships faced by women with ADHD in marriage when compared to their male counterparts.
While frequent psychiatric comorbidities in adults with ADHD are well documented,3,14,24–28 findings on gender differences are scarce and heterogeneous. In a double-blinded, placebo-controlled study, Robison et al29 found that women with ADHD had higher levels of internalizing problems, such as depression, anxiety, sleep problems, and emotional dysregulation, than men with ADHD. Rasmussen and Levander30 similarly reported a higher prevalence of affective, eating, and somatization disorders among women with ADHD. However, in Biederman et al,16 there were no gender differences in comorbidity rates of mood and anxiety disorders in adults with ADHD. Concerning substance use disorders, the authors found a higher prevalence in men than women,16 as corroborated by Rasmussen and Levander,30 who found that substance abuse and criminality were more common among men than women with ADHD.
Japanese society is often described as a “high-context” society in which “homogeneity, collectivism, and group harmony are highly valued.”31,32 People are often required to read between the lines and follow certain sets of norms and expectations. Yamatonadeshiko refers to a woman who is gentle, polite, modest, reserved, delicate, quiet, attentive, organized, and patient;33 these remain the ideal, expected female characteristics, and such women are generally perceived as more appealing to men and society.33–35 Being in some ways almost the opposite of yamatonadeshiko, women with ADHD—inattentive or/and hyperactive-impulsive—may face greater vulnerability to secondary disorders or impairments due to experience of conflict with social ideals or of being perceived more negatively.
In the present study, we investigated clinical characteristics and gender differences in adults with ADHD in a Japanese clinical sample. Given the possible cultural impact on women with ADHD, we established two hypotheses: first, women with ADHD have more comorbidities than men with ADHD; second, compared to men, women with ADHD experience more social hardships, such as having less full-time employment and being divorced. We tested the hypotheses by collecting clinical and social data from outpatients who visited our ADHD specialty clinic at Showa University Karasuyama Hospital.
Materials and Methods
Participants
Showa University Karasuyama Hospital, located in central Tokyo, has an ADHD specialty clinic that focuses on diagnosis and treatments for adults with ADHD. Individuals who are suspected of having ADHD visit or are referred to the clinic from across Japan. Patients who visited our clinic between April 2015 and March 2016 were recruited consecutively, and only those fulfilling the DSM-5 criteria for ADHD were included. The exclusion criteria were people with an intelligence quotient (IQ) under 85 based on the Japanese Adult Reading Test (JART),36 those who were aged under 18 years, and those with other psychiatric and medical conditions requiring urgent treatment. During the aforementioned period, 470 patients were assessed for eligibility, and 335 people (71%) were ultimately included in the study.
Assessments and Diagnosis
During the assessment interview that each patient received, the following information was collected: current chief complaints and problems, developmental and medical history, daily living and social situations (including work, marital status, and typical daily activity), physical illnesses, family history, history of psychiatric consultations, past psychiatric diagnoses, history of alcohol abuse and illicit drug use, and current medications. Behavioral and developmental history from infancy was also collected from suitable informants for each patient, who had known the patient from early childhood to adulthood, and from school reports if available. The Japanese edition of Conners’s Adult ADHD Diagnostic Interview for the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; CAADID)37,38 was used to assist the diagnosis of ADHD. Current ADHD symptoms were evaluated using the Japanese version of Conners’s Adult ADHD Rating Scale Self-Report Screening Version (CAARS-S:SV-J).39,40 IQ was estimated by the Japanese Adult Reading Test (JART), which has been standardized and shown to yield adequate IQ estimates of Japanese adults.36 The final diagnosis of ADHD and comorbid psychiatric disorders, if any, was made based on DSM-5 criteria with consensus between at least two psychiatrists involved in the assessment and CAADID interview.
Ethics
This study was evaluated and approved by the Medical Ethics Committee of Showa University School of Medicine, and the protocols were in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants included in the study after the study description was provided.
Statistical Analysis
All statistical analyses were carried out using SPSS version 20.0 (IBM, Chicago, IL, USA). Between-gender comparisons were made using the chi-squared test for categorical variables and Student’s t-test for continuous variables by setting gender as the independent variable and each of the other demographic and clinical items as dependent variables: age, years of education, marital and employment status, family history, consultation history, past diagnoses, comorbidities, medications, and CAARS-S:SV-J Inattentive, Hyperactive-Impulsive, and Total (the sum of Inattentive and Hyperactive-Impulsive subscale) scores. A logistic regression analysis was performed for employment status, marital status, and comorbidity to evaluate the independent effects of gender on these dependent variables. Candidates for other explanatory variables were chosen from items that were statistically significant in the univariate analyses. Odds ratios (ORs) with corresponding 95% confidence intervals (95% CIs) were estimated. The level of significance was set at p < 0.05, and all tests were two-sided.
Results
Data of 335 participants were analyzed, namely those of 156 women (46.6%) and 179 men (53.4%). Their demographics and clinical characteristics are shown in Table 1. No gender difference was found for age or years of education. The mean age was 32.0 (SD = 9.2) years, with most participants (94.3%) being in their 20s to 40s. The educational level was high, as 83.3% of participants had more than 12 years of education, with an average of 14.8 (SD = 1.8) years.
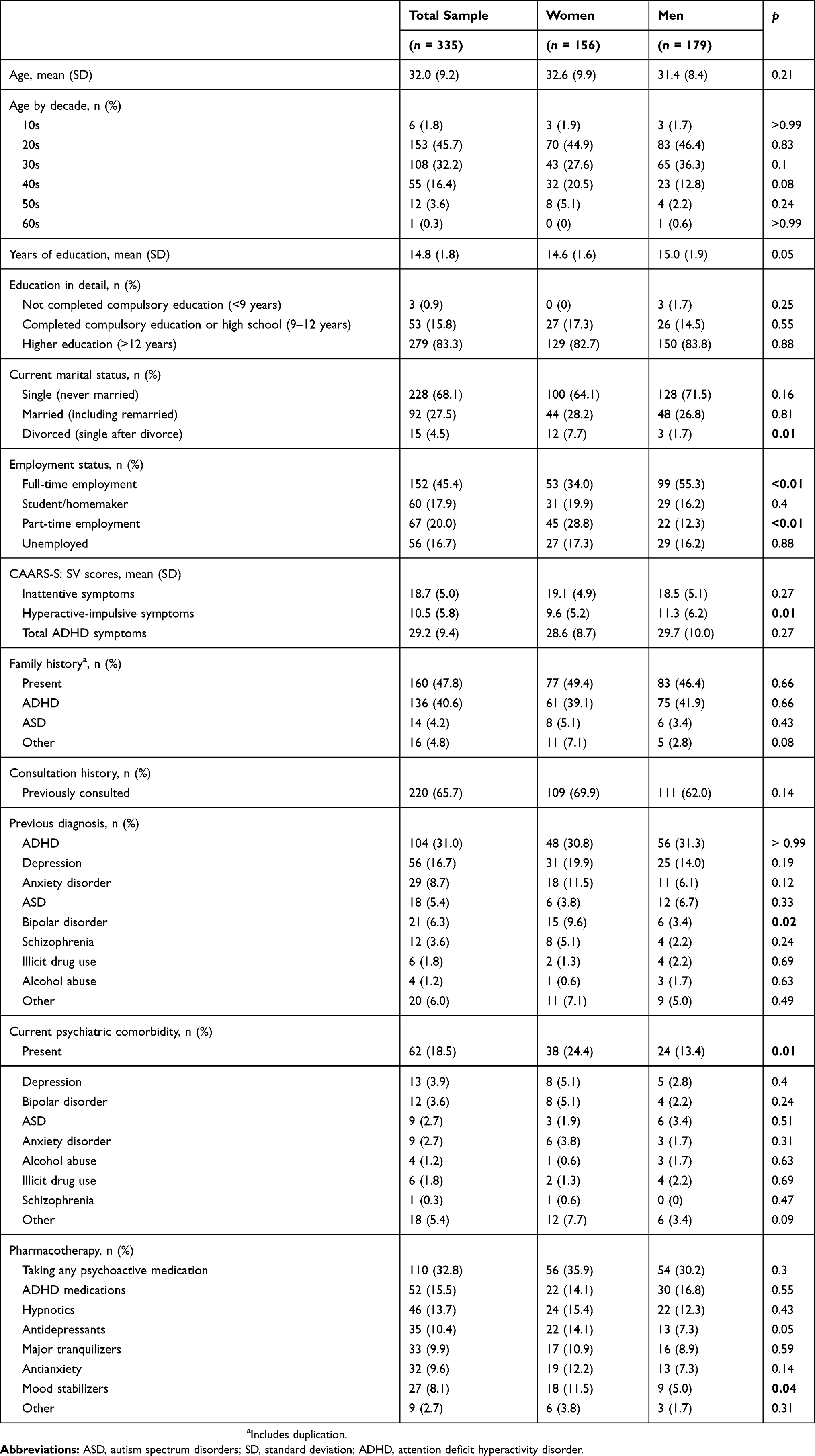 |
Table 1 Demographics and Clinical Characteristics by Gender |
As expected, the mean CAARS-S: SV-J scores were high: total ADHD symptoms of 29.2 (SD = 9.4), inattentive symptoms of 18.7 (SD = 5.0), and hyperactive-impulsive symptoms of 10.5 (SD = 5.8). While inattentive and total ADHD symptom scores were similar across genders, hyperactive-impulsive symptoms score was significantly higher in men than in women (11.3 vs. 9.6, t[333] = 2.79, p = 0.01).
Although only 31.9% of participants had experienced marriage, significantly more women than men were divorced (7.7% vs. 1.7%, χ2 = 7.05, df = 1, p = 0.014). Occupational status also showed significant gender differences: women were less likely to have full-time employment than men (34.0% vs. 55.3%, χ2 = 15.31, df = 1, p < 0.001) and more likely to have part-time jobs (28.8% vs. 12.3%, χ2 = 14.28, df = 1, p <0.001). The unemployment rate was 16.7% with no gender difference.
Nearly half of the participants had a family history of either ADHD (40.6%) or ASD (4.2%). Of those who had sought previous psychiatric consultation, one in two had received an ADHD diagnosis, and depression was the second most common diagnosis for both genders. Women were more likely to be previously diagnosed with bipolar disorder than men (9.6% vs. 3.4%, χ2 = 5.57, df = 1, p = 0.023).
Approximately one-fifth (18.5%) of the participants had comorbid psychiatric disorders, and the gender difference was significant: women had a higher overall comorbidity rate than men (24.4% vs. 13.4%, χ2 = 6.63, df = 1, p = 0.011). Mood disorders were the most common comorbidities (depression 3.9%, bipolar disorder 3.6%), although no disorder-specific difference was found by gender. Rates of both alcohol abuse (1.2%) and illicit drug abuse (1.8%) were low, with no gender difference. Approximately one-third (32.8%) of the participants were taking psychiatric medication; of these, only half were taking drugs for ADHD (16.0%). Significantly more women than men were prescribed mood stabilizers (11.5% vs. 5.0%, χ2 = 4.77, df = 1, p = 0.043).
As shown in Table 2, logistic regression analyses revealed that being female significantly increased the likelihood of being out of full-time employment (adjusted odds ratio [aOR], 2.99; 95% confidence interval [CI]: 1.79–4.98), being divorced (aOR, 5.79; 95% CI: 1.17–28.58), and having any psychiatric comorbidity (aOR, 2.81; 95% CI: 1.51–5.25).
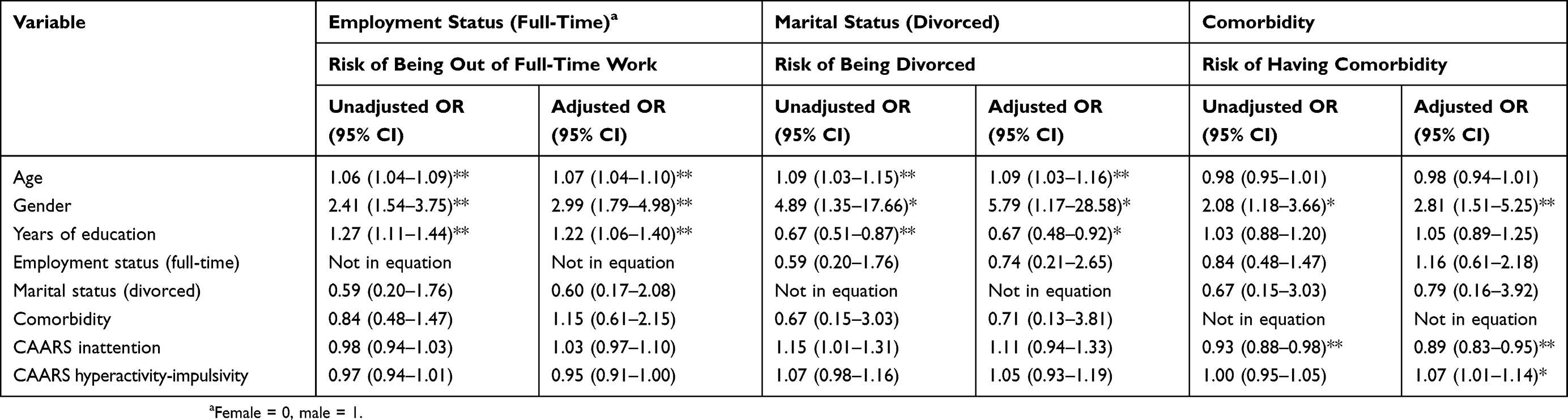 |
Table 2 Logistic Regression Analyses of Employment Status, Marital status, And Comorbidity |
Discussion
We studied gender differences in sociodemographic and clinical characteristics in a clinical sample of Japanese adults with ADHD. The results fully supported our hypotheses that women with ADHD have more comorbidities and are more socially disadvantaged (ie, less likely to be in full-time employment, more likely to be divorced) than men. The gender ratio of our sample was almost equal (men:women = 1.1:1), consistent with previous findings in other countries9,10 that the gender gap in prevalence declines in adult ADHD. Notably, nearly 70% of participants had not received an ADHD diagnosis until participating in the study, indicating that, for both genders, a large proportion of individuals with ADHD are left undiagnosed until adulthood. In accordance with previous studies,12,41 men had more hyperactive-impulsive symptoms than women.
As predicted, women with ADHD experienced greater difficulties than men in several social domains, particularly work and marriage. Our results that significantly fewer women were in full-time employment and more in part-time jobs and divorced are consistent with studies in other countries showing that more women than men with ADHD are long-term work-disabled22 and that ADHD in women is less tolerated in marriage.23 With gender inequality still existing in Japan, firms are inclined to hire and assign men to more active and creative positions, while women are placed in more routine clerical work, such as general administration, reception, and window service.35,42 Similarly in marriage, women are expected to take the main role in household management.33,35,43 Yamatonadeshiko characteristics are highly valued in such roles so that women with ADHD—with symptoms of inattention or/and hyperactivity and impulsivity—could be highly prone to negative evaluations, intolerance, and low self-esteem. Viewing the results in this sociocultural context, general Japanese population statistics for people with similar demographic characteristics to our participants (university graduates and persons in their 20s to 40s) indicate full-time employment rate of 84.2% and 60.3%, part-time employment of 2.65% and 13.8%, and unemployment of 3.27% and 1.72% for men and women, respectively.44–46 For both genders, full-time employment rates are smaller and those of part-time and unemployment larger in our ADHD sample. Importantly, the proportion of people in full-time employment in our ADHD sample as compared to the general population is 66% for men and 56% for women; the smaller ratio in women indicates the particular burden on females with ADHD in getting or maintaining full-time work. In addition, although the part-time work ratio between our ADHD sample and the general population was greater in men (4.6 to 1) than in women (2.1 to 1), the ratio for unemployment was greater in women (10.1 to 1) than in men (5.0 to 1), possibly demonstrating a tendency for females with ADHD to become unemployed while male counterparts find part-time work. Similarly, the proportion of divorced individuals in the general population is 2.92% for men and 5.66% for women.47 These values were 0.6 times smaller in men and 1.4 times larger in women with ADHD in the sample. Although this cannot be an exact comparison, the gender differences in work and marriage in our ADHD sample are not a mere reflection of the background population trends but show the possible additional burden on women with ADHD, in association with the gender inequality and unique cultural attitudes in Japan. However, some caution is required when interpreting the divorce results, due to the small number of divorced individuals in our sample.
Unsurprisingly, women with ADHD had more comorbidities than men. Women with ADHD may experience increased proneness to develop secondary psychiatric disorders due to lower self-esteem and symptom internalization. Lower self-esteem has been found in women with ADHD48 and in turn, is related to the onset of various mental disorders.49 The relative lack of externalized or overt symptoms of ADHD11,12 may also delay diagnosis in women,11,13,15,16 leading to additional comorbid problems. The constant failure of women with ADHD to conform to social ideals and expectations of Japanese culture may exacerbate this process. No disorder-specific gender difference was found, in contrast to some studies that reported greater internalizing of problems in women than in men.29,30,50 We attribute this to bias in our sample, as only adults exhibiting ADHD symptoms (and not those of other psychiatric disorders) are likely to visit or be referred to our ADHD specialty clinic. Indeed, the comorbidity rates for all observed disorders were strikingly lower than those reported in previous studies.3,14,24–28,51,52 The results that women were more likely to have a past diagnosis of bipolar disorder and to be prescribed mood stabilizers may support the higher prevalence of affective problems in women, as reported in previous studies.29,30
Our findings must be viewed in the context of several limitations. First, the study lacked a normal control population, such that we could provide only an approximate comparison to national demographic statistics. Second, the total sample size was only 335, making conclusions less precise than ideal. Third, the data were based on a clinical sample of outpatients who visited our ADHD specialty clinic and might not accurately represent the whole ADHD population in Japan. Only participants with serious and obvious symptoms of ADHD and without other urgent psychiatric conditions are likely to self-refer or be referred. Third, we did not exclude participants who were already taking ADHD medications. Although only 16% were prescribed such medications, with no gender difference in the proportion, this could still possibly have confounded the results regarding social functioning in both genders. A further multi-center study with a normal control group is planned for the future.
Conclusion
In this clinical sample-based study, Japanese women with ADHD were found to have a higher psychiatric comorbidity rate and more functional impairments in marital and vocational domains than men with ADHD. Cultural ideals and expectations of women in Japan may contribute to greater difficulties faced by women with ADHD. Further larger, multi-center studies are planned to explore symptom manifestations and self-esteem.
Acknowledgments
We thank the doctors in the Department of Psychiatry at Showa University for their helpful advice and support in the present study. We would also like to thank Editage for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gelder MG, Andreasen NC, Lopez-Ibor JJ
2. Riecher-Rossler A. Sex and gender differences in mental disorders. Lancet Psychiatry. 2016;4(1):8–9. doi:10.1016/S2215-0366(16)30348-0
3. Angold A, Costello EJ, Erkanli A. Comorbidity. J Child Psychol Psychiatry. 1999;40(1):57–87. doi:10.1111/1469-7610.00424
4. Hill J, Schoener E. Age-dependent decline of attention deficit hyperactivity disorder. Am J Psychiatry. 1996;153(9):1143–1146. doi:10.1176/ajp.153.9.1143
5. Biederman J, Mick E, Faraone SV. Age-dependent decline of symptoms of attention-deficit-hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry. 2000;157(5):816–818. doi:10.1176/appi.ajp.157.5.816
6. Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159–165. doi:10.1017/S003329170500471X
7. Rasmussen P, Gillberg C. Natural outcome of ADHD with developmental coordination disorder at age 22 years: a controlled, longitude, community-based study. J Am Acad Child Adolesc Psychiatry. 2000;39(11):1424–1431. doi:10.1097/00004583-200011000-00017
8. Weiss G, Hechtman L. Hyperactive Children Grown Up: ADHD in children, Adolescents, and Adults. New York: Guildford Press; 1993.
9. Faraone SV, Biederman J. What is the prevalence of adult ADHD? Results of a population screen of 966 adults. J Atten Disord. 2005;9(2):384–391. doi:10.1177/1087054705281478
10. Vingilis E, Erickson PG, Toplak ME, Kolla NJ, Mann RE. Attention deficit hyperactivity disorder symptoms, comorbidities, substance use, and social outcomes among men and women in a Canadian sample. Biomed Res Int. 2015;2015:982072. doi:10.1155/2015/982072
11. Biederman J, Mick E, Faraone SV, et al. Influence of gender on attention deficit hyperactivity disorder in children referred to psychiatric clinic. Am J Psychiatry. 2002;159(1):36–42. doi:10.1176/appi.ajp.159.1.36
12. Gershon J, Gershon J. A meta-analytic review of gender differences in ADHD. J Atten Disord. 2002;5(3):143–154. doi:10.1177/108705470200500302
13. Groenwald C, Emond A, Sayal K. Recognition and referral of girls with attention deficit hyperactivity disorder: case vignette study. Child Care Health Dev. 2009;35(6):767–772. doi:10.1111/j.1365-2214.2009.00984.x
14. Kooij JJ, Huss M, Asherson P, Akehurst R, Beusterien K, French A. Distinguishing comorbidity and successful management of adult ADHD. J Atten Disord. 2012;16(5_suppl):3S–19S. doi:10.1177/1087054711435361
15. Quinn PO. Treating adolescent girls and women with ADHD: gender-specific issues. J Clin Psychol. 2005;61(5):579–587. doi:10.1002/jclp.20121
16. Biederman J, Faraone SV, Monuteaux MC, Bober M, Cadogen E. Gender effects on attention-deficit/hyperactivity disorder in adults, revisited. Biol Psychiatry. 2004;55(7):692–700. doi:10.1016/j.biopsych.2003.12.003
17. Kooij SJ, Bejerot S, Blackwell A, et al. European consensus statement on diagnosis and treatment of adult ADHD: the European Network Adult ADHD. BMC Psychiatry. 2010;10(1):67. doi:10.1186/1471-244X-10-67
18. Simon V, Czobor P, Balint S, Meszaros A, Bitter I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: meta-analysis. Br J Psychiatry. 2009;194(3):204–211. doi:10.1192/bjp.bp.107.048827
19. Michielsen M, Semeijn E, Comijs HC, et al. Prevalence of attention-deficit hyperactivity disorder in older adults in The Netherlands. Br J Psychiatry. 2012;201(4):298–305. doi:10.1192/bjp.bp.111.101196
20. Spencer TJ, Biederman J, Mick E. Attention-deficit/hyperactivity disorder: diagnosis, lifespan, comorbidities, and neurobiology. Ambul Pediatr. 2007;7(suppl 1):73–81. doi:10.1016/j.ambp.2006.07.006
21. Fedele DA, Lefler EK, Hartung CM, Canu WH. Sex differences in the manifestation of ADHD in emerging adults. J Atten Disord. 2012;16(2):109–117. doi:10.1177/1087054710374596
22. Fredriksen M, Dahl AA, Martinsen EW, Klungsoyr O, Faraone SV, Peleikis DE. Childhood and persistent ADHD symptoms associated with educational failure and long-term occupant disability in adult ADHD. ADHD. 2014;6:87–99. doi:10.1007/s12402-014-0126-1
23. Robin AL, Payson E. The impact of ADHD on marriage. ADHD Rep. 2002;10(3):9–14. doi:10.1521/adhd.10.3.9.20553
24. Arias AJ, Gelernter J, Chan G, et al. Correlates of co-occurring ADHD in drug-dependent subjects: prevalence and features of substance dependence and psychiatric disorders. Addict Behav. 2008;33(9):1199–1207. doi:10.1016/j.addbeh.2008.05.003
25. Barkley RA, Murphy K, Kwasnik D. Psychological adjustment and adaptive impairments in young adults with ADHD. J Atten Disord. 1996;1(1):41–54. doi:10.1177/108705479600100104
26. de Zwaan M, Gruss B, Müller A, et al. The estimated prevalence and correlates of adult ADHD in a German community sample. Eur Arch Psychiatry Clin Neurosci. 2012;262(1):79–86. doi:10.1007/s00406-011-0211-9
27. Fayyad J, De Graaf R, Kessler R, et al. Cross-national prevalence and correlates of adult attention-deficit/hyperactivity disorder. Br J Psychiatry. 2007;190(5):402–409. doi:10.1192/bjp.bp.106.034389
28. Sobanski E, Brüggemann D, Alm B, et al. Psychiatric comorbidity and functional impairment in a clinically referred sample of adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neurosci. 2007;257(7):371–377. doi:10.1007/s00406-007-0712-8
29. Robison RJ, Reimherr FW, Marchant BK, Faraone SV, Adler LA, West SA. Gender differences in 2 clinical trials of adults with attention-deficit/hyperactivity disorder: a retrospective data analysis. J Clin Psychiatry. 2008;69(2):213–221. doi:10.4088/JCP.v69n0207
30. Rasmussen K, Levander S. Untreated ADHD in adults: are there sex differences in symptoms, comorbidity, and impairment? J Atten Disord. 2009;12(4):353–360. doi:10.1177/1087054708314621
31. Japanology. Japan’s “high context” society-tips on reading between the lines [webpage on the Internet]. Barton, DW; 2016. Available from: http://japanology.org/2016/10/japans-high-context-society-tips-on-reading-between-the-lines/.
32. Roger JD, Ikeno O. The Japanese Mind: Understanding Contemporary Japanese Culture. Clarendon, VT: Tuttle Publishing; 2011.
33. Nadeshiko—adorable till they die [webpage on the Internet]. Shoji, K; 2013. The Japan Times. Available from: https://www.japantimes.co.jp/life/2013/09/15/language/nadeshiko-adorable-till-they-die/#.WyP3Wzf7S1s.
34. Azuma K. Social Psychology of Gender. Dainippon Tosho: Tokyo; 1979.
35. Ogasawara Y. Office Ladies and Salaried Men: Power, Gender, and Work in Japanese Companies. Berkeley: University of California Press; 1998.
36. Matsuoka K, Kin Y. Chitekikinounokannihyoka: Japanese Adult Reading Test (JART). Shinkoigakusyuppansya: Tokyo; 2006.
37. Epstein JN, Johnson DE, Conners CK. Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID): Technical Manual. Toronto: Multi-Health Systems; 2001.
38. Nakamura K. CAADID. KanekoShobo: Japanese edition manual. Tokyo; 2012.
39. Conners CK, Erhardt D, Sparrow E. Conners’ Adult ADHD Rating Scales (CAARS) Technical Manual. North Tonawanda, NY: Multi-Health Systems; 1999.
40. Takahashi M, Takita Y, Ichikawa H, et al. Reliability and validity of the Japanese version of CAARS-screening version (CAARS-SV), adult ADHD symptom rating scale. Seishin Igaku. 2011;53(1):23–34.
41. Williamson D, Johnston C. Gender differences in adults with attention-deficit/hyperactivity disorder: A narrative review. Clin Psychol Rev. 2015;40:15–27. doi:10.1016/j.cpr.2015.05.005
42. Sugihara Y, Katsurada E. Gender-role personality traits in Japanese culture. Psychol Women Q. 2000;24(4):309–318. doi:10.1111/j.1471-6402.2000.tb00213.x
43. Zhou Y. Career interruption of Japanese women: why is it so hard to balance work and childcare? Jpn Labor Rev. 2015;12(2):106–123.
44. e-Stat Portal Site of Official Statistics of Japan Table 01200 [webpage on the Internet]. Tokyo: Statistics of Japan; 2018. Available from: https://www.e-stats.go.jp/dbview?sid=0003222442.
45. e-Stat Portal Site of Official Statistics of Japan Table 21001 [webpage on the Internet]. Tokyo: Statistics of Japan; 2018. Available from: https://www.e-stats.go.jp/dbview?sid=0003222648..
46. e-Stat Portal Site of Official Statistics of Japan Table 09900 [webpage on the Internet]. Tokyo: Statistics of Japan; 2018. Available from: https://www.e-stats.go.jp/dbview?sid=0003222527.
47. Table 6.20 Population by Marital Status, Age and Sex: 2015 [webpage on the Internet]. Tokyo: Population Statistics of Japan; 2017. Available from: http://www.ipss.go.jp/p-info/e/psj2017/PSJ2017-06.xls.
48. Rucklidge JJ. Gender differences in attention-deficit/hyperactivity disorder. Psychiatr Clin North Am. 2010;33(2):357–373. doi:10.1016/j.psc.2010.01.006
49. Silverstone PH, Salsali M. Low self-esteem and psychiatric patients: part I - The relationship between low self-esteem and psychiatric diagnosis. Ann Gen Hosp Psychiatry. 2003;2(2):2. doi:10.1186/1475-2832-2-2
50. Jensen CM, Steinhausen HC. Comorbid mental disorders in children and adolescents with attention-deficit/hyperactivity disorder in a large nationwide study. ADHD. 2015;7(1):27–38. doi:10.1007/s12402-014-0142-1
51. Biederman J, Monuteaux MC, Mick E, Spencer T. Young adult outcome of attention deficit hyperactivity disorder: a controlled 10-year follow-up study. Psychol Med. 2006;36(2):167–179. doi:10.1017/S0033291705006410
52. Biederman J, Wilens T, Mick E, Milberger S, Spencer TJ, Faraone SV. Psychoactive substance use disorders in adults with attention deficit hyperactivity disorder (ADHD): effects of ADHD and psychiatric comorbidity. Am J Psychiatry. 1995;152(11):1652–1658. doi:10.1176/ajp.152.11.1652
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.