")
Back to Journals » Infection and Drug Resistance » Volume 15
Clinical Characteristics of Acute Pancreatitis Patients with Multidrug-Resistant Bacterial Infection
Authors Cheng G, Wang D, Zhu P, Lin Z, Zhu S, Li J, Li L, Zhang Y, Li G
Received 16 December 2021
Accepted for publication 21 March 2022
Published 31 March 2022 Volume 2022:15 Pages 1439—1447
DOI https://doi.org/10.2147/IDR.S354347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Guilan Cheng,1,* Dingxi Wang,1,* Ping Zhu,2 Ziqi Lin,2 Shichao Zhu,3 Juan Li,1 Linqian Li,1 Yipeng Zhang,4 Guixiang Li1
1Department of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu, People’s Republic of China; 2Department of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Department of Infection Control, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 4Department of Information Centre, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guixiang Li, Department of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, No. 37 Wainan Guoxue Alley, Chengdu, 610041, People’s Republic of China, Tel +86 18980601726, Email [email protected]
Background: There are few published reports describing the clinical characteristics of acute pancreatitis (AP) patients with multidrug-resistant organism (MDRO) infection.
Methods: This was a retrospective analysis of AP patients with MDRO infection in West China Hospital between July 2015 and June 2020. Basic clinical data, disease progression states, and prognoses of the MDRO and non-MDRO infection groups were compared and analyzed. Logistic regression analysis was performed to explore the related risk factors for MDRO infection. The prognoses of different MDRO infection types were compared.
Results: In total, 9812 AP patients were included, 2436 (24.83%) of whom had healthcare-associated infections (641 [26.31%] MDRO infections and 1795 [73.69%] non-MDRO infections). The main MDRO strain was carbapenem-resistant Acinetobacter baumannii (CRAB) (400/62.40%). The rate of discharge against doctor’s advice, mortality, hospitalization expenses, and hospitalization days was higher in the MDRO infection group than in the noninfection group. By logistic regression analysis, the independent risk factors associated with MDRO infection included male sex (OR 1.36, 95% CI 1.09∼ 1.70), severity (OR 1.40, 95% CI 1.10∼ 1.78), ICU referral (OR 2.48, 95% CI 1.79∼ 3.44), abdominal puncture (OR 2.78, 95% CI 1.93∼ 4.02), fiberoptic bronchoscopy (OR 1.95, CI 1.35∼ 2.81), and PICC/CVC placement (OR 1.48, CI 1.06∼ 2.06). Compared with biliary and hypertriglyceridemia (HTG) (OR 0.94, 95% CI 0.73∼ 1.23), alcohol (OR 0.30, 95% CI 0.19∼ 0.47) and other etiologies (OR 0.58, 95% CI 0.41∼ 0.81) conferred a lower risk of MDRO infection. The carbapenem-resistant Klebsiella pneumoniae (CRKP) infection rate was highest in the patients who died.
Conclusion: The CRAB proportion was highest in AP patients with MDRO infection. MDRO infection is related to many factors, has a poor prognosis, and increases the patient burden. CRKP infection is directly related to poor prognosis.
Keywords: acute pancreatitis, multidrug-resistant organisms, infection
Introduction
Acute pancreatitis (AP) is a common critical disease of the digestive system, and its incidence is increasing yearly.1 Mild AP is usually relieved spontaneously within 1–2 weeks. Approximately 20% of patients develop moderate to severe AP, with a mortality rate of 20–40%.2–4 Organ failure and infection secondary to peripancreatic necrosis may be two independent risk factors for a poor AP prognosis.5,6 In the past 10 years, the treatment concept changed from early surgery to conservative treatment with internal medicine, minimally invasive surgery, and endoscopic surgery, which improved the cure rate of AP.7 Changes in surgical methods have reduced the need for invasive operations, but the infection caused by multidrug-resistant organisms (MDROs) shows an upward trend and affects the prognosis of AP patients.8–10 Therefore, it is necessary to conduct a large-sample survey of AP patients with MDRO infection and summarize the clinical characteristics of such patients to provide a basis for the prevention and identification of early infections and treatment and prevention measures.
Scholars have performed some studies on the clinical progress and prognoses of patients with partial infectious pancreatic necrosis (IPN) and walled-off pancreatic necrosis (WOPN) combined with MDRO infection.8–11 However, due to the small sample size, there are certain limitations in comprehensively describing the clinical characteristics, influencing factors, and disease prognosis of MDRO infection in AP. Therefore, this study aimed to further expand the sample size and retrospectively analyze the clinical data of AP patients with MDRO infection admitted to West China Hospital of Sichuan University over the past five years to explore the effect of MDRO infection on the progression and prognosis of AP.
Methods
Study Design and Data Collection
We retrospectively analyzed the clinical data of AP patients admitted to West China Hospital of Sichuan University (including multiple hospitalized patients, counted by cases) between July 2015 and June 2020 (in a total of five years). AP patients were mostly admitted to the following departments: integrated traditional Chinese and Western Medicine, pancreatic surgery, gastroenterology, and the ICU. The inclusion criteria were as follows: patients diagnosed with AP and hospitalized at West China Hospital, Sichuan University between July 2015 and June 2020. The exclusion criteria were as follows: ① age < 18 years, ② hospital stay < 24 hours, and ③ incomplete main research indicators. The members of this study group included clinicians, information center engineers, hospital infection management department researchers, statisticians, research nurses, hospital infection prevention and control nurses, and clinical nurses. The diagnoses and classifications of all patients were conducted by recognized international guidelines.12 This study protocol was approved by the institutional review committee of West China Hospital, Sichuan University (Approval number: 20201245). The ethics committee waived informed consent because this was a retrospective study. Patient data came from the medical record system, no names or identifying information were indicated on the checklists, and confidentiality was assured throughout the study. The methods were carried out following the relevant guidelines and regulations of the West China Hospital, Sichuan University. Our study was conducted in accordance with the Declaration of Helsinki.13
Definition
The diagnoses and severity classifications of AP patients were based on the 2012 Atlanta International Consensus.12 Regarding the etiologies, biliary AP was defined as choledocholithiasis or other biliary-related factors associated with AP. HTG-AP was defined as serum triglyceride (TG) level ≥1000 mg/dl on admission after ruling out common etiologies.14 Alcoholic AP was defined as a drinking history >35 standard drinks per week, especially with a pattern of binge drinking.15 Other causes included autoimmune diseases, endoscopic retrograde cholangiopancreatography (ERCP), drug-induced diseases, and trauma.16,17 The measures of the prognoses included discharge against doctor’s advice, mortality, hospitalization expenses, and hospitalization days. These were recorded during the index hospitalization or during 3 months of follow-up. The diagnostic criteria for hospital infection management issued in China in 200118 and the relevant provisions of the United States Centers for Disease Control and Prevention19 were used to classify the specimen sources and sites of drug-resistant bacterial infections. MDROs are defined as bacteria that are resistant to commonly used antibiotics of three or more categories.20 In this study, different types of drug-resistant bacteria in the same infected patient were statistically analyzed separately and counted as individual cases. When the same type of drug-resistant bacteria was detected in specimens from different tissues of the same patient, statistical analysis was carried out on only the first specimen sent for inspection. AP was treated by medical treatment strategies and surgical treatment strategies. The commonly used surgical methods included percutaneous catheter drainage (PCD), minimally invasive retroperitoneal pancreatic necrosis removal (MARPN), and open pancreatic necrosis removal (OPN).8,9,16 The commonly performed invasive operations mainly included abdominal puncture, chest puncture, fiberoptic bronchoscopy, deep vein catheterization (peripherally inserted central catheters [PICCs] and central venous catheters [CVCs]), arterial catheter insertion, continuous renal replacement therapy (CRRT), and tracheal intubation.
Statistical Analysis
The entered data were checked for accuracy and normality using the Kolmogorov–Smirnov test. Continuous variables are expressed as the mean and standard deviation (normally distributed) or as the median and interquartile range (nonnormally distributed). Qualitative variables are expressed as the number and percentage, while quantitative variables are expressed as the mean and standard deviation. The t test or Mann–Whitney test was chosen to compare continuous variables, and the chi-squared test or Fisher’s exact test was used to compare categorical variables. Factors associated with MDRO infection were identified using multivariate logistic regression analysis. The odds ratio (OR) and 95% confidence interval (CI) were calculated. Results with a two-sided p value less than 0.05 were deemed statistically significant. All analyses were completed with Microsoft Excel 2016 and IBM SPSS (version 22.0).
Results
Patient Infections
This study analyzed the medical records of patients with AP who were first diagnosed at West China Hospital of Sichuan University between July 2015 and June 2020. A total of 9812 patients with AP were admitted within 5 years. There were 2436 patients with healthcare-associated infections (including nosocomial infection and out-of-hospital entry), including 641 cases of nosocomial MDRO infection (26.31%) and 1795 cases of non-MDRO infection (73.69%). A total of 53.20% of specimens were collected from sputum, followed by peritoneal drainage fluid (32.92%) and blood (9.67%). The main MDRO strain was carbapenem-resistant Acinetobacter baumannii (CRAB) (400/62.40%), followed by carbapenem-resistant Klebsiella pneumoniae (CRKP) (121/18.88%) and carbapenem-resistant Pseudomonas aeruginosa (CRPA) (65/10.14%). There were 436 cases of nosocomial MDRO infection (68.02%) and 205 cases of external hospital infection (31.98%).A total of 364 patients (83.49%) had used antibiotics before MDRO infection (Supplemental Table 1).
Basic Clinical Data, States of Disease Progression, and Prognoses of Patients
The basic clinical data, states of disease progression, and prognoses of the MDRO infection group and non-MDRO infection group were analyzed by single-factor analysis. The results showed that the proportion of male and severe AP in the MDRO infection group was higher. Biliary and HTG-AP were apparently higher than alcohol in the MDRO infection group. The proportions of patients who underwent invasive procedures and operations and ICU referrals in the MDRO infection group were significantly higher than those in the non-MDRO infection group. In terms of prognosis, the rate of discharge against doctor’s advice, mortality, hospitalization expenses, and hospitalization days was worse than those in the non-MDRO infection group (P < 0.05) (Table 1).
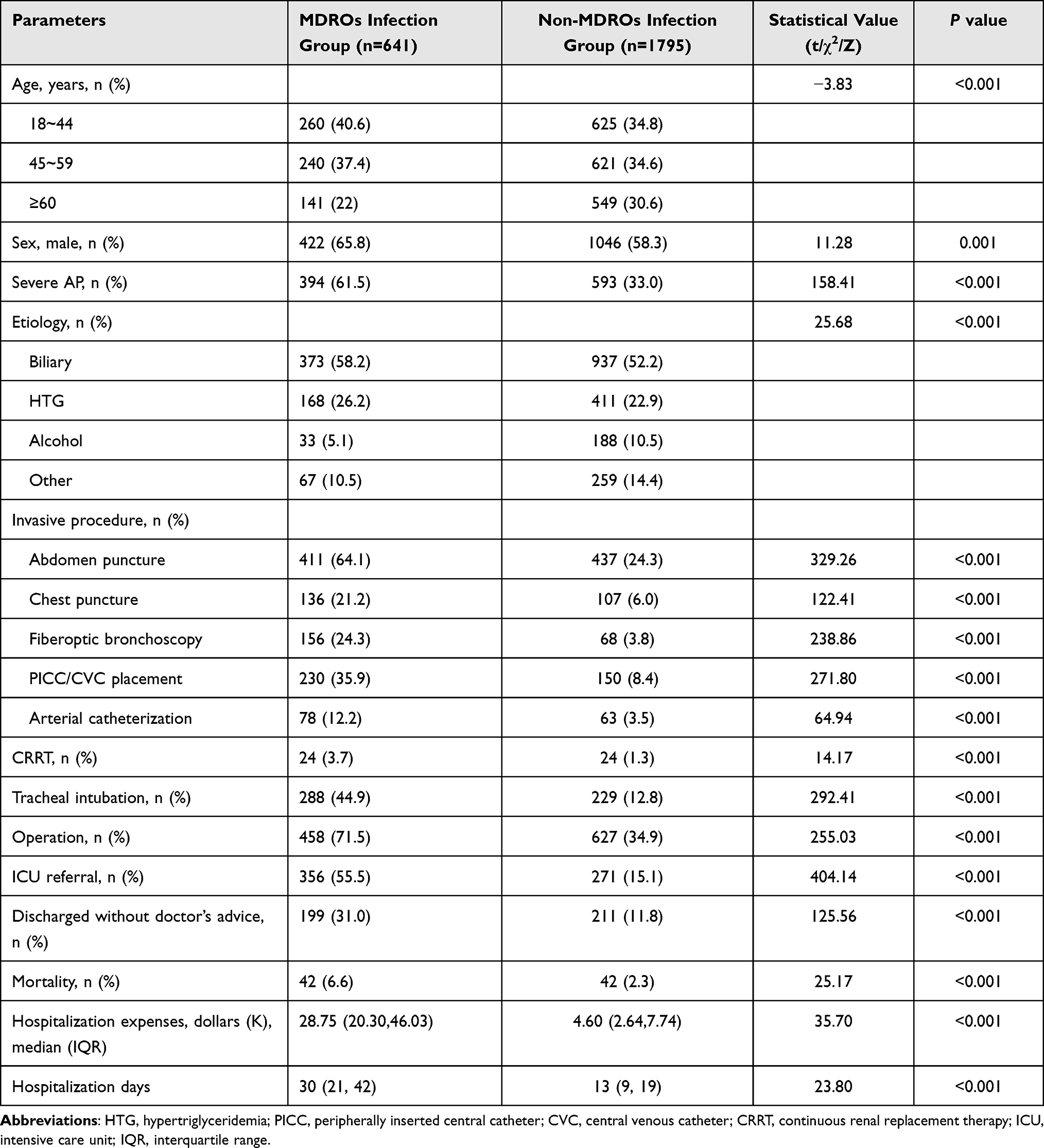 |
Table 1 Comparison of Baseline Characteristics and Outcomes Between Patients with and without MDROs |
Logistic Regression Analysis of Influencing Factors of MDRO Infection in AP Patients
By logistic regression analysis, the independent risk factors associated with MDRO infection included male sex (OR 1.36, 95% CI 1.09~1.70), severity (OR 1.40, 95% CI 1.10~1.78), ICU referral (OR 2.48, 95% CI 1.79~3.44), abdominal puncture (OR 2.78, 95% CI 1.93~4.02), fiberoptic bronchoscopy (OR 1.95, CI 1.35~2.81), and PICC/CVC placement (OR 1.48, CI 1.06~2.06). Compared with biliary and hypertriglyceridemia (HTG) (OR 0.94, 95% CI 0.73~1.23), alcohol (OR 0.30, 95% CI 0.19~0.47) and other etiologies (OR 0.58, 95% CI 0.41~0.81) conferred a lower risk of MDRO infection (Table 2).
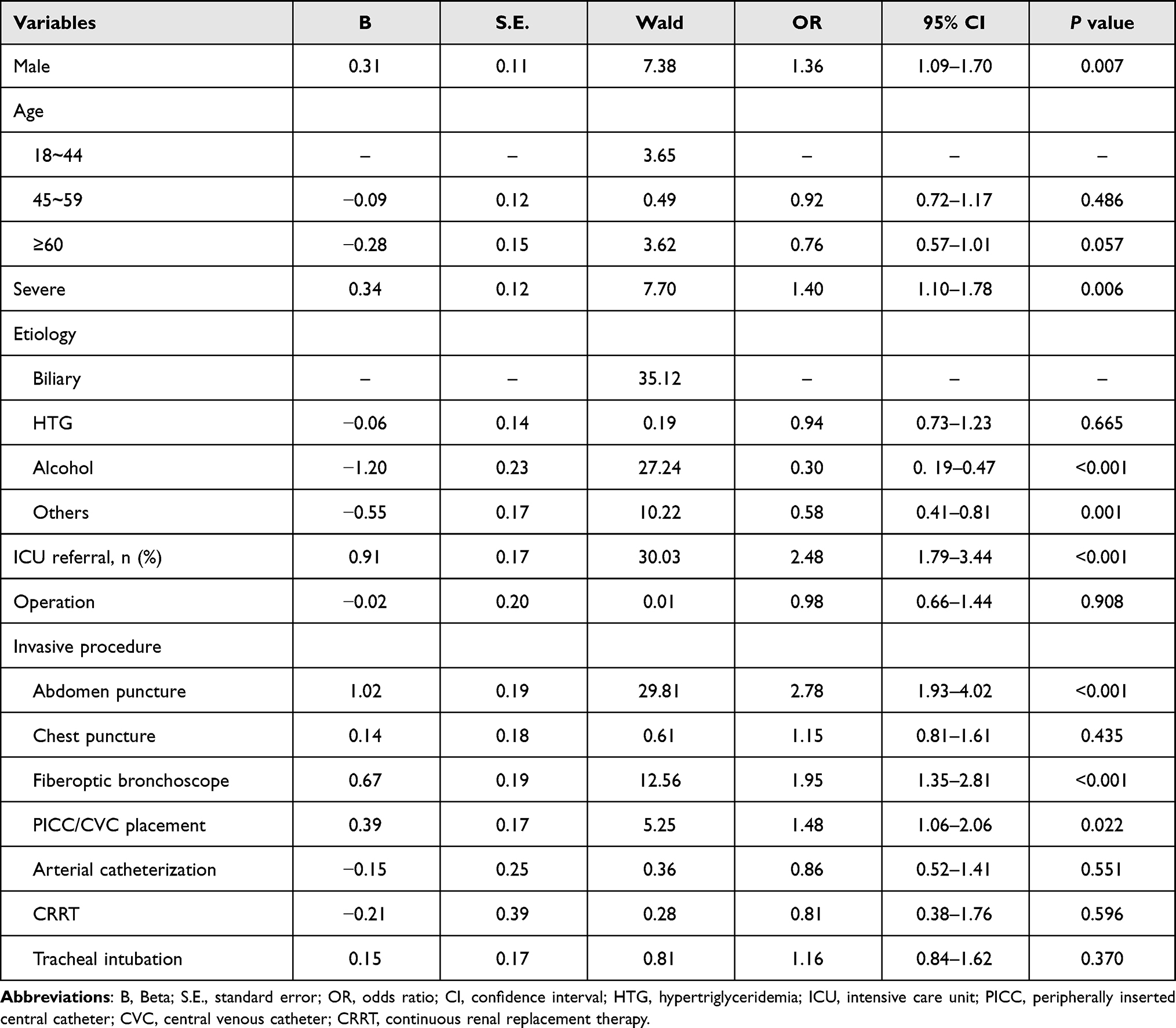 |
Table 2 Logistic Regression Analysis of AP Patients with MDRO Infection |
Effects of Different Drug-Resistant Bacteria on Patient Prognosis
By analyzing the effects of different drug-resistant bacterial infections on patient prognosis, we found that the mortality rate of patients with CRKP infection was the highest among the patients who died (Table 3).
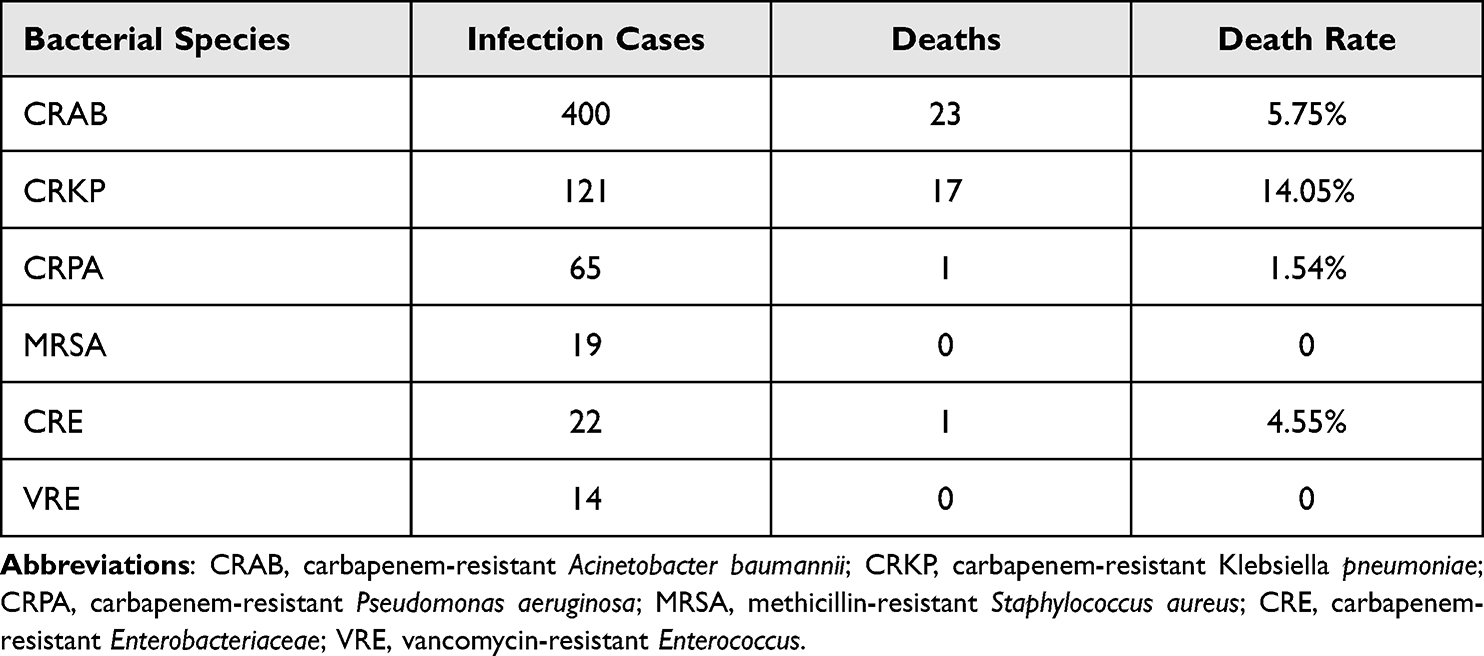 |
Table 3 Effects of Different Drug-Resistant Bacteria on Prognosis |
Discussion
This study was a large-scale investigation of the status of AP combined with MDRO infection in tertiary hospitals in China and was performed to evaluate the drug-resistant bacterial status, clinical characteristics, and prognosis of patients with infection. We found that MDRO infection was associated with adverse clinical outcomes, including a high rate of discharge against doctor’s advice, high mortality, high hospitalization expenses, and long hospitalization days. Thus, MDRO infection may be one of the main obstacles in preventing and treating the complications of AP infection in China.11 MDRO infection in AP patients is related to sex. Males were significantly more often infected with MDROs than females, which may be related to the slightly higher incidence of AP in males than in females.21 Among the AP patients with MDRO infection in this study, 55.5% had been previously admitted to the ICU, which again suggests to some extent that ICU hospitalization is a risk factor for cross-infection of multidrug-resistant bacteria.22–24 On the one hand, because of the critical conditions of such patients, a large number of invasive operations destroy the functions of the original mucosa and vascular barrier and increase the risk of nosocomial infection. On the other hand, the lack of strict implementation of hospital infection prevention and control measures by medical personnel affects the ICU.
The sources and locations of drug-resistant bacteria in this study were classified according to the diagnostic criteria of nosocomial infection in China and the relevant provisions of the United States Centers for Disease Control and Prevention.17–19 The results showed that more than half of the specimens were collected from the sputum of patients with lower respiratory tract infection, and 44.9% of all patients with infection had received tracheal intubation. Moreover, the multivariate analysis showed that bronchoscopy was one of the risk factors for MDRO infection, which suggests that drug-resistant bacteria easily invade the respiratory tract, and it is necessary to prevent the occurrence of in-hospital cross-infection when performing invasive respiratory operations such as tracheal intubation and bronchoscopy. In this study, since the same drug-resistant bacteria were detected in specimens from different parts of the same patient, statistical analyses were carried out on the first specimen. Since sputum was the first source of specimens, this was also the reason why the largest proportion of specimens was obtained from sputum.
CRAB accounted for the largest proportion of MDROs infected with AP, followed by CRKP and CRPA. It is a matter of national and international concern, as they are emerging causes of hospital-acquired infection (HAI) that pose a significant threat to public health.25 These bacterial infections are difficult to treat due to high levels of antimicrobial resistance (AMR) and are associated with high mortality rates. Importantly, they have the potential for the widespread transmission of resistance via mobile genetic elements.26 This will also allow the earlier introduction of infection prevention and control (IPC) measures in health care settings to prevent pathogen transmission to other patients in the hospital environment, with particular attention to patients infected with CRKP. This study found that the risk of MDRO infection in biliary AP and HTG-AP was significantly higher than that in alcoholic AP and other causes (autoimmune disorders, ERCP, drug-induced, traumatic, etc.). Whether alcohol can increase antibacterial activity in a patient needs further research.
At present, antibiotic resistance has become a major public health threat worldwide.27 In this study, 83.49% of patients who used antibiotics before the MDRO infection became infected in the hospital. In the 2020 Guidelines for the Treatment of AP, it was pointed out that early related infections in AP patients, such as pneumonia or bacteremia, and secondary pancreatic or peripancreatic necrosis can lead to sepsis and have a significant impact on clinical prognosis.28 Nevertheless, the prophylactic use of antibiotics does not reduce the risk of secondary infection,29,30 and the use of prophylactic antibiotics is related to the development of overlapping infections of multidrug-resistant bacteria and fungi. Therefore, antibiotics can be selected when a secondary infection is diagnosed or clinically suspected, and antibiotics can be used under the guidance of clear evidence of infection and drug sensitivity tests. Once infection control needs to be discontinued as soon as possible, it is not recommended to use antibiotics routinely.8,31
In this survey, 71.5% of AP patients with MDROs underwent different degrees of surgery. Multivariate analysis showed that abdominal puncture, fiberoptic bronchoscopy, and PICC/CVC increased the risk of MDRO infection. There are some disputes about whether AP patients need surgery and the method of surgery. For most AP patients with aseptic inflammation or peripancreatic necrosis, conservative treatment can be performed regardless of the amount and scope of exudation.14,32 Over time, most of the exudation can be absorbed by itself,33 and blind drainage can cause iatrogenic infection.5,34,35 At the same time, some doctors who advocate active surgery believe that, for some patients who ultimately need surgical intervention, the Traditional “step-up” sequential treatment procedure should be crossed, and the “step-jump” treatment strategy should be adopted for early surgical intervention.36 In summary, regardless of which surgical method is adopted, strict infection control measures, including hand hygiene, contact isolation, active screening, environmental surface disinfection, and the management of restrictive antibiotic use, are the key to preventing MDROs in AP.
Of the AP patients surveyed, 31.98% of MDROs were imported from outside the hospital, and these patients had a poor prognosis. If AP cannot be treated in large hospitals in a timely manner after onset, it will directly affect the prognosis of patients. An Indian scholar found that patients with AP who were referred to tertiary hospitals in the second and third weeks had worse outcomes than those who were referred within the first week.37 This finding may be related to timely fluid resuscitation, organ system support, nutritional support and antibiotic use for patients in tertiary hospitals, and timely radiation, endoscopic or surgical intervention.
Conclusion
In summary, the CRAB proportion was highest in AP patients with MDRO infection. MDRO infection is related to many factors, has a poor prognosis, and increases the patient burden. CRKP infection is directly related to poor prognosis.
Limitations of the Study
This study has several limitations. First, this was a retrospective study; hence, bias in the documentation was unavoidable. Second, this study included only patients with an initial diagnosis of AP, and patients with diagnoses other than AP were not included. Third, the results of this study were obtained from a single center and cannot be generalized to other hospitals. Further multicenter and prospective original research will provide more accurate data to clarify potentially confusing results.
Acknowledgments
The authors wish to thank all staff of the Department of Infection Control Center, the Department of Information Center, and the Department of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was supported by the Science and Technological Supports Project of Sichuan Province, China (No. 2019YFS0389, GL and 2020YFS0268, DW).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xiao AY, Tan ML, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi:10.1016/S2468-1253(16)30004-8
2. Crockett SD, Wani S, Gardner TB, et al.; American Gastroenterological Association Institute Clinical Guidelines Committee. American gastroenterological association institute guideline on initial management of acute pancreatitis. Gastroenterology. 2018;154(4):1096–1101. doi:10.1053/j.gastro.2018.01.032.
3. Schepers NJ, Bakker OJ, Besselink MG, et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2019;68(6):1044–1051. doi:10.1136/gutjnl-2017-314657
4. Bang JY, Wilcox CM, Arnoletti JP, et al. Superiority of endoscopic interventions over minimally invasive surgery for infected necrotizing pancreatitis: meta-analysis of randomized trials. Dig Endosc. 2019;32(3):298–308. doi:10.1111/den.13470
5. Kadiyala V, Suleiman SL, McNabb-Baltar J, et al. Atlanta classification, revised Atlanta classification, and determinant based classification of acute pancreatitis: which is best at stratifying outcomes? Pancreas. 2016;45(4):510–515. doi:10.1097/MPA.0000000000000477
6. Choi JH, Kim MH, Cho DH, et al. Revised Atlanta classification and determinant-based classification: Which one better at stratifying outcomes of patients with acute pancreatitis? Pancreatology. 2017;17(2):194–200. doi:10.1016/j.pan.2017.01.004
7. Van Brunschot S, Hollemans RA, Bakker OJ, et al. Minimally invasive and endoscopic versus open necrosectomy for necrotising pancreatitis: a pooled analysis of individual data for 1980 patients. Gut. 2018;67(4):697–706. doi:10.1136/gutjnl-2016-313341
8. Lee HS, Lee SK, Park DH, et al. Emergence of multidrug resistant infection in patients with severe acute pancreatitis. Pancreatology. 2014;14(6):450–453. doi:10.1016/j.pan.2014.10.003
9. Jain S, Mahapatra SJ, Gupta S, et al. Infected pancreatic necrosis due to multidrug-resistant organisms and persistent organ failure predict mortality in acute pancreatitis. Clin Transl Gastroenterol. 2018;9(10):190. doi:10.1038/s41424-018-0056-x
10. Tugal D, Lynch M, Hujer AM, et al. Multi-drug-resistant Klebsiella pneumoniae pancreatitis: a new challenge in a serious surgical infection. Surg Infect. 2015;16(2):188–193. doi:10.1089/sur.2012.175
11. Ning C, Huang G, Shen D, et al. Adverse clinical outcomes associated with multidrug-resistant organisms in patients with infected pancreatic necrosis. Pancreatology. 2019;19(7):935–940. doi:10.1016/j.pan.2019.09.008
12. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
13. Shrestha B, Dunn L. The Declaration of Helsinki on medical research involving human subjects: a review of seventh revision. J Nepal Health Res Counc. 2020;17(4):548–552. doi:10.33314/jnhrc.v17i4.1042
14. Tenner S, Baillie J, DeWitt J, et al. American college of gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108(9):
15. Yadav D, Whitcomb DC. The role of alcohol and smoking in pancreatitis. Nat Rev Gastroenterol Hepatol. 2010;7(3):131–145. doi:10.1038/nrgastro.2010.6
16. Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–734. doi:10.1016/S0140-6736(20)31310-6
17. Carr RA, Rejowski BJ, Cote GA, et al. Systematic review of hypertriglyceridemia-induced acute pancreatitis: a more virulent etiology? Pancreatology. 2016;16(4):469–476. doi:10.1016/j.pan.2016.02.011
18. Ministry of Health of the People’s Republic of China. Diagnostic criteria for nosocomial infections(proposed). Chin Med J. 2001;81:314–320. doi:10.3760/j:
19. Centers for Disease Control and Prevention/ National Healthcare Safety Network. Identifying Healthcare-associated Infections (HAI) for NHSN Surveillance; January, 2017. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/2psc_identifyinghais_nhsncurrent.pdf.
20. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
21. Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, et al. Impact on morbidity, mortality, and length of stay of hospital-acquired infections by resistant microorganisms. Clin Infect Dis. 2017;65(4):644–652. doi:10.1093/cid/cix411
22. Su LX, Wang XT, Pan P, et al.; China Critical Infection and Infection Control Alliance (CCICA). Infection management strategy based on prevention and control of nosocomial infections in intensive care units. Chin Med J. 2019;132(1):115–119. doi:10.1097/CM9.0000000000000029.
23. Kostakoğlu U, Saylan S, Karataş M, et al. Cost analysis and evaluation of nosocomial infections in intensive care units. Turk J Med Sci. 2016;46:1385–1392. doi:10.3906/sag-1504-106
24. Rasslan O, Seliem ZS, Ghazi IA, et al. Device-associated infection rates in adult and pediatric intensive care units of hospitals in Egypt. International Nosocomial Infection Control Consortium (INICC) findings. J Infect Public Health. 2012;5(6):394–402. doi:10.1016/j.jiph.2012.07.002
25. Chen X, Liu Q, Liu W, et al. Risk factors for subsequential carbapenem-resistant Klebsiella pneumoniae clinical infection among rectal carriers with carbapenem-resistant Klebsiella pneumoniae. Infect Drug Resist. 2020;13:1299–1305. doi:10.2147/IDR.S247101
26. Dickstein Y, Lellouche J, Ben Dalak Amar M, et al. Treatment Outcomes of Colistin- and Carbapenem-resistant Acinetobacter baumannii infections: an exploratory subgroup analysis of a randomized clinical trial. Clin Infect Dis. 2019;69:769–776. doi:10.1093/cid/ciy988
27. Menz BD, Charani E, Gordon DL, et al. Surgical antibiotic prophylaxis in an era of antibiotic resistance: common resistant bacteria and wider considerations for practice. Infect Drug Resist. 2021;14:5235–5252. doi:10.2147/IDR.S319780
28. Besselink MG, van Santvoort HC, Boermeester MA, et al. Timing and impact of infections in acute pancreatitis. Br J Surg. 2009;96(3):267–273. doi:10.1002/bjs.6447
29. Lim CL, Lee W, Liew YX, et al. Role of antibiotic prophylaxis in necrotizing pancreatitis: a meta analysis. J Gastrointest Surg. 2015;19(3):480–491. doi:10.1007/s11605-014-2662-6
30. Vege SS, DiMagno MJ, Forsmark CE, et al. Initial medical treatment of acute pancreatitis: American gastroenterological association institute technical review. Gastroenterology. 2018;154(4):1103–1139. doi:10.1053/j.gastro.2018.01.031
31. Baron TH, DiMaio CJ, Wang AY, et al. American gastroenterological association clinical practice update: management of pancreatic necrosis. Gastroenterology. 2020;158(1):67–75. doi:10.1053/j.gastro.2019.07.064
32. Working Group IAP/APA acute pancreatitis guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4):e1–15. doi:10.1016/j.pan.2013.07.063.
33. Freeman ML, Werner J, van Santvoort HC, et al. Interventions for necrotizing pancreatitis: summary of a multidisciplinary consensus conference. Pancreas. 2012;41(8):1176–1194. doi:10.1097/MPA.0b013e318269c660
34. Walser EM, Nealon WH, Marroquin S, et al. Sterile fluid collections in acute pancreatitis: catheter drainage versus simple aspiration. Cardiovasc Intervent Radiol. 2006;29(1):102–107. doi:10.1007/s00270-004-0220-4
35. Zerem E, Imamovic G, Omerović S, et al. Randomized controlled trial on sterile fluid collections management in acute pancreatitis: should they be removed? Surg Endosc. 2009;23(12):2770–2777. doi:10.1007/s00464-009-0487-2
36. Yi MIAO, Dong-ya HUANG, Qiang LI, et al. From “step-up” to “step-jump”: leapfrog therapy of infected necrotizing pancreatitis. Chin J Pract Surg. 2020;40:1251–1254. doi:10.19538/j.cjps.issn1005-2208.2020.11.06
37. Mallick B, Dhaka N, Sharma V, et al. Impact of timing of presentation of acute pancreatitis to a tertiary care centre on the outcome. Pancreatology. 2019;19(1):143–148. doi:10.1016/j.pan.2018.10.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.