")
Back to Journals » International Journal of General Medicine » Volume 13
Clinical Characteristics of Acalypha indica Poisoning
Authors Pradoo A , Sriapha C , Trakulsrichai S , Tongpoo A, Kheiawsawang M, Wananukul W
Received 19 May 2020
Accepted for publication 27 July 2020
Published 25 August 2020 Volume 2020:13 Pages 539—545
DOI https://doi.org/10.2147/IJGM.S263199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aimon Pradoo,1 Charuwan Sriapha,1 Satariya Trakulsrichai,1,2 Achara Tongpoo,1 Metta Kheiawsawang,3 Winai Wananukul1,4
1Ramathibodi Poison Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 2Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 3Nursing Service Department, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 4Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Correspondence: Charuwan Sriapha
Ramathibodi Poison Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Tel +66-2-201-1084-5
Fax +66-2-2011084-5#1
Email [email protected]
Background: Acalypha indica is a tropical plant used as a herbal medicine in various parts of the world, including Thailand. In glucose-6-phosphate dehydrogenase (G6PD)-deficient patients, acute hemolysis has been reported following the ingestion of this plant. Methemoglobinemia was reported in the present study.
Patients and Methods: Descriptive data of patients who suffered from Acalypha indica toxicity reported from different hospitals to the Ramathibodi Poison Center were retrieved from 2011 to 2019.
Results: Eight patients were included, mostly male with a median age of 61.5 years. The plant was ground for fresh juice or boiled before consuming as herbal medicine. All patients presented with dark urine. Most had jaundice and fever, and all reported hemolysis. Seven out of eight patients were diagnosed as methemoglobinemia. Methemoglobin level was confirmed in five patients with the highest level of 23.9%. Early symptoms occurred within 24 hours of the last ingested dose.
Discussion: In previous case reports of Acalypha indica ingestion, acute hemolysis was mostly observed in G6PD-deficient patients, consistent with the current findings. However, our patients also demonstrated methemoglobinemia, with some constituents in this plant (quinine, 2-methyl anthraquinone and tectoquinone) implicated as the cause in previous studies. Further studies are crucial to validate these findings.
Conclusion: We report a case series in which acute hemolysis and methemoglobinemia after Acalypha indica ingestion were observed. This study presents methemoglobinemia as the other toxicity caused by this plant.
Keywords: acute hemolysis, methemoglobinemia, G6PD deficiency, plant-induced methemoglobinemia
Introduction
Herbal medicine plays an important role as alternative medicine among Asian countries. Acalypha indica, a tropical plant that grows in various parts of the world including Thailand,1 is used in herbal medicines and as local food. Although toxicity has not been documented in animal studies even at high doses,2,3 intravascular hemolysis has been reported in humans with glucose-6-phosphate dehydrogenase enzyme (G6PD) deficiency after ingesting this plant.4–6 One case report also described methemoglobinemia.7 Studies of Acalypha indica poisoning in Southeast Asia that include Thailand are limited. Therefore, the objective of this study was to characterize the clinical manifestations and the clinical outcomes of Acalypha indica poisoning in Thailand.
Patients and Methods
We conducted a cross-sectional retrospective study of all human exposures to Acalypha indica reported to the Ramathibodi Poison Center (RPC), Bangkok, Thailand from January 2011 to December 2019. The RPC is a poison center based in a tertiary teaching hospital, serves the whole country, both healthcare professionals and the general public 24 hours a day, 7 days a week. Most calls to the RPC are from medical personnel. There are approximately 20,000 calls annually. Follow-up calls are periodically made to collect and monitor case progress, to provide ongoing treatment recommendations, and to determine the medical outcomes of cases. All cases are recorded in the RPC Toxic Surveillance System database.
Acalypha indica was determined by 1) description of plant or plant name given by the patient or relative, 2) pictures of plant that were sent to the RPC’s application Line or an email, 3) identification using botany textbooks, and 4) identification by a botanist at the Medicinal Plant Information Center, Faculty of Pharmacy, Mahidol University. This verification process was conducted by a team of information scientists and medical toxicologists.
All circumstances of human exposures to Acalypha indica were retrieved. We collected each patient’s demographic data, reason for exposure, amount of exposure, plant preparation for consumption, duration from exposure to arrival at a healthcare facility, medical history, laboratory findings, treatment modalities, follow-up details, final diagnosis, and outcome. A case with the history of co-exposures to other drugs, chemicals, herbs, or pesticides which cause hemolysis or methemoglobinemia were excluded. In this study, a heart rate greater than 100 beats per minute was defined as tachycardia, and a heart rate less than 60 beats per minute was defined as bradycardia.8 Fever was defined as an oral temperature at the morning reading above 37.2°C or an afternoon temperature of above 37.7°C.9 Jaundice is often used interchangeably with hyperbilirubinemia when serum bilirubin is greater than 2 mg/dL, twice the normal upper limit.10 Hemolysis was defined by the presence of dark urine, decreased hematocrit from the baseline results and increased indirect bilirubin. Methemoglobinemia was an abnormal elevation of the methemoglobin level above 1%,11 or defined by the presence of oxygen saturation gap (between pulse oximetry and arterial blood gas) and desaturation not well responded to oxygen therapy or cyanosis. Acute kidney injury was diagnosed based on the patient’s clinical history and laboratory data using the Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines.12
The RPC data were obtained and managed using Microsoft Excel, and then analyzed with IBM SPSS Statistics for Windows, version 18 (IBM Corp., Armonk, NY, USA). Descriptive statistics were performed to characterize the data. The median, minimum, maximum, and interquartile range (IQR) were analyzed for continuous data, while the frequency and percentage were assessed for categorical data.
This study was approved by the Institutional Ethics Committee Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University (Reference Number: 10–61-30) and performed in accordance with the principles of the Declaration of Helsinki. Patient consent was not required by the ethics committee board because this study was retrospective in nature and used the preexisting confidential database from RPC. All results were reported anonymously.
Results
A total of nine patients with a definite history of Acalypha indica ingestion reported from different hospitals between 2011–2019 were retrieved from the database system of the Ramathibodi Poison Center (RPC), Thailand. One case was excluded due to incomplete information; eight patients were included. Table 1 summarizes the demographic and exposure characteristics of patients with Acalypha indica ingestion. Most patients (7/8) were male, with a median age of 61.5 years (range 38–70 years). Leaves (75%) were commonly used, followed by the whole plant (25%). For ingestion, the plant was ground for fresh juice or boiled as a decoction. Four individuals drank this herbal decoction one time. The median time from ingestion to arrival at healthcare facility was 2.5 days (range, 2–4 days). After ingestion of the first dose, the median onset of symptoms was 18 hours (range, 4–24 hours) for single ingestion and 3 days (range, 2–4 days) for multiple ingestions. In the latter group, the symptom onset occurred within 24 hours after a last dose of ingestion. All patients presented with dark urine, most had jaundice and fever (Figure 1). Hemolysis was diagnosed in all patients. Details of each patient are shown in Table 2. The lowest hematocrit (Hct) was 10.5%; the highest indirect bilirubin level was 14.5 mg/dL. G6PD deficiency was confirmed in 2 patients; remaining patients demonstrated normal G6PD activity at presentation but were lost to follow-up G6PD activity at 3 months after discharge. Seven patients had desaturation and oxygen saturation gaps, failing to adequately respond to oxygen therapy. Some had cyanosis. Methemoglobin levels were confirmed in 5 patients, with a median level of 5.6% (range, 1–23%). All patients presented no prior personal or family history of unexplained cyanosis or low oxygen saturation. Prior to discharge, oxygen saturation returned to normal. The median duration from symptom initiation to the disappearance of dark urine, hemolysis, and methemoglobinemia was 4.5, 5, and 5 days for single, and 3.5, 5.5, and 4.5 days for multiple ingestions, respectively. Four patients developed acute kidney injury, with three requiring hemodialysis. Treatment was mainly supportive (Table 2). One patient died due to cardiovascular disease (Patient 3). He was a 70-year-old man with underlying asthma, chronic obstructive pulmonary disease, and coronary artery disease and had ingested a glass of fresh juice daily for 3 days. He developed dyspnea, central cyanosis, dark urine, tachycardia (HR 122 bpm), fever (38.5°C), low oxygen saturation by pulse oximetry (SpO2 49–52%), and anemia (Hct 32%, his baseline Hct was 40%) on the 3rd day. He was mechanically ventilated with 100% oxygen but his SpO2 was 60–62%. Laboratory tests indicated methemoglobinemia (his methemoglobin level of 23.9%) with normal G6PD. Treatment included blood transfusion, two doses of methylene blue 1% (1, 0.5 mg/kg) and supportive treatment. His condition improved until he was weaned off the ventilator. Later, he suddenly had tachypnea, SpO2 levels decreased to 65%, and acute myocardial infarction was suspected; death occurred on the 2nd day of admission.
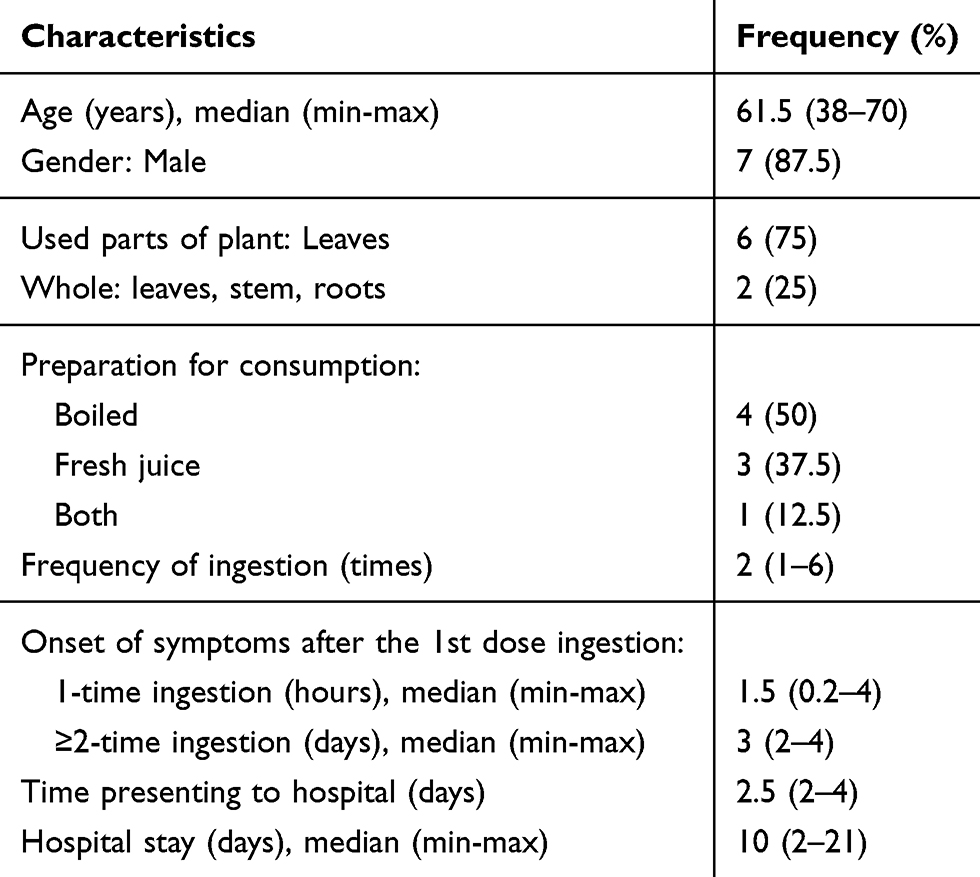 |
Table 1 Demographic and Exposure Characteristics of Patients with Acalypha indica Ingestion |
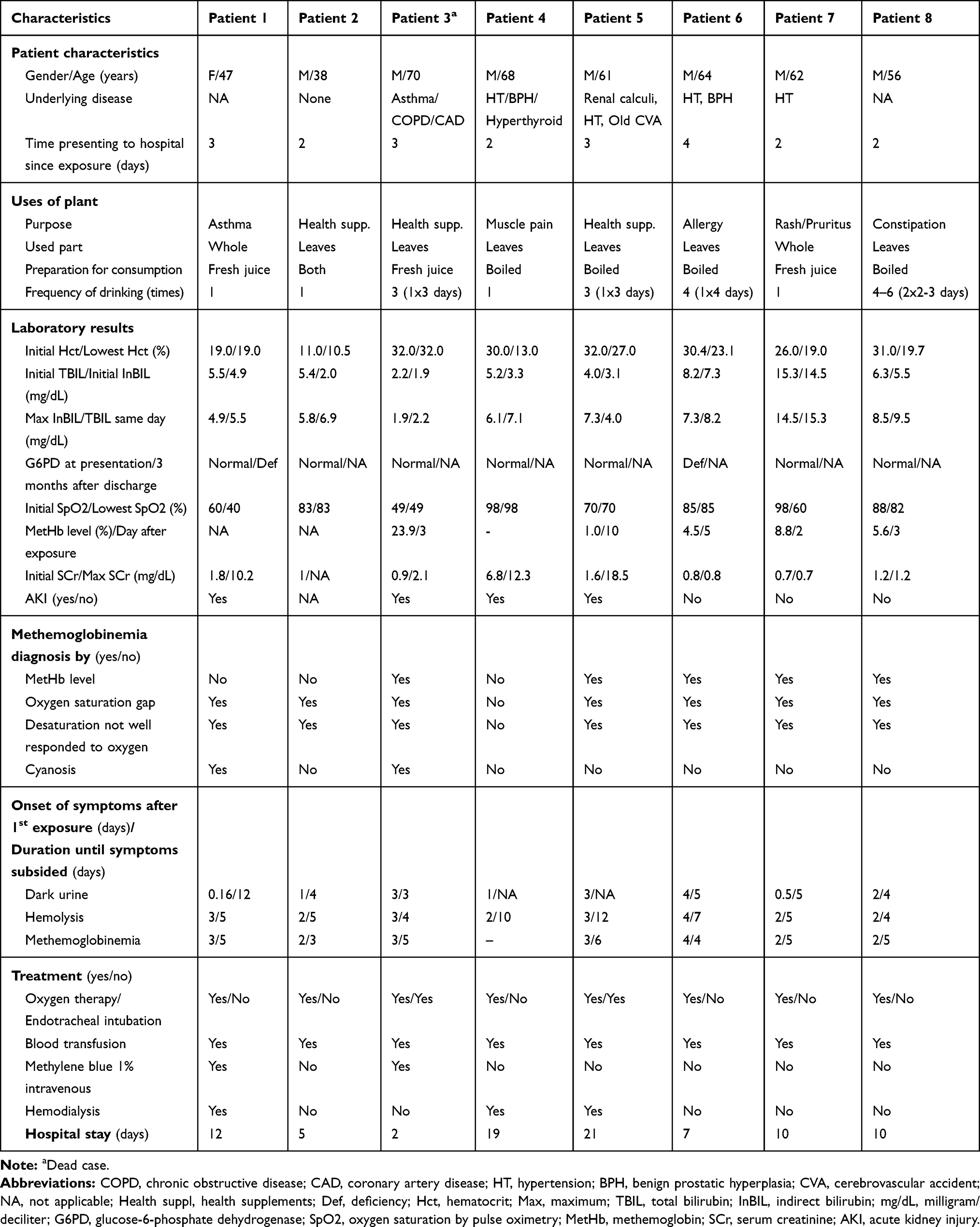 |
Table 2 Demographic Data, Clinical Manifestations, Laboratory Results and Treatment in Each Patient Who Exposed to Acalyha Indica |
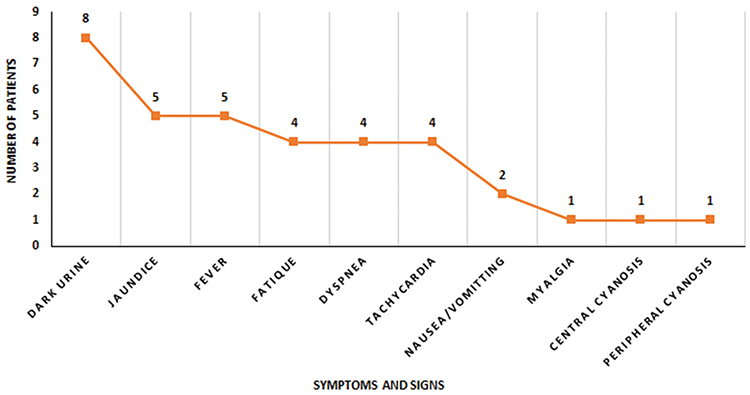 |
Figure 1 Clinical signs and symptoms at first presentation. |
Discussion
Acute hemolysis has been primarily reported in G6PD-deficient patients after ingesting Acalypha indica,4–6 with only one case in normal G6PD status.13 In this study, all patients had acute hemolysis. At presentation, most patients had normal G6PD status except two patients had G6PD deficiency. The measurement of G6PD activity can be normal during hemolysis. Phenotypic test for G6PD deficiency is best done 2–3 months after hemolytic crisis.14 Therefore, we cannot elucidate the G6PD status in six patients who lost to follow-up after discharge.
Seven patients (88%) in our study presented symptoms suggesting methemoglobinemia, with five confirmed by methemoglobin levels ranging from 1–23.9%. The level of 1% was low because it was monitored on the 10th day after ingestion when methemoglobinemia symptom recovered. Methemoglobinemia is commonly an acquired condition, although it can rarely be hereditary. Our patients were not screened for hereditary methemoglobinemia but the presence of normal oxygen saturation on pulse oximetry at discharge could demonstrate the improbability of an altered hemoglobin form, such as Hemoglobin M, or the absence of an essential enzyme, such as homozygotes of NADH-cytochrome b5 reductase deficiencies. Owing to a lack of in-depth investigation, some limitations include the heterozygosity in the patients, necessitating future validation studies.
To date, methemoglobinemia due to Acalypha indica has been previously presented in one case report.7 This report describes “acute hemolysis and methemoglobinemia in G6PD deficiency” in a 59-year-old patient, with no additional information of plant part used or implementation, laboratory results, methemoglobin level and treatment. Acalypha indica is composed of various phytochemicals (Table 3) and nutrients which most of them play a role in human therapeutic property.1 On the other hand, previous studies have implicated three constituents found in leaf and the whole parts of this plant; quinine,15 2-methyl anthraquinone and tectoquinone16 resulting in methemoglobinemia (Table 3). These constituents might have oxidative potentials. Oxidative chemicals may cause both acute hemolysis and methemoglobinemia.15–17 Although this plant contains cyanogenic glycosides and hydrogen cyanide, no patient developed or demonstrated any signs/symptoms of cyanide poisoning.
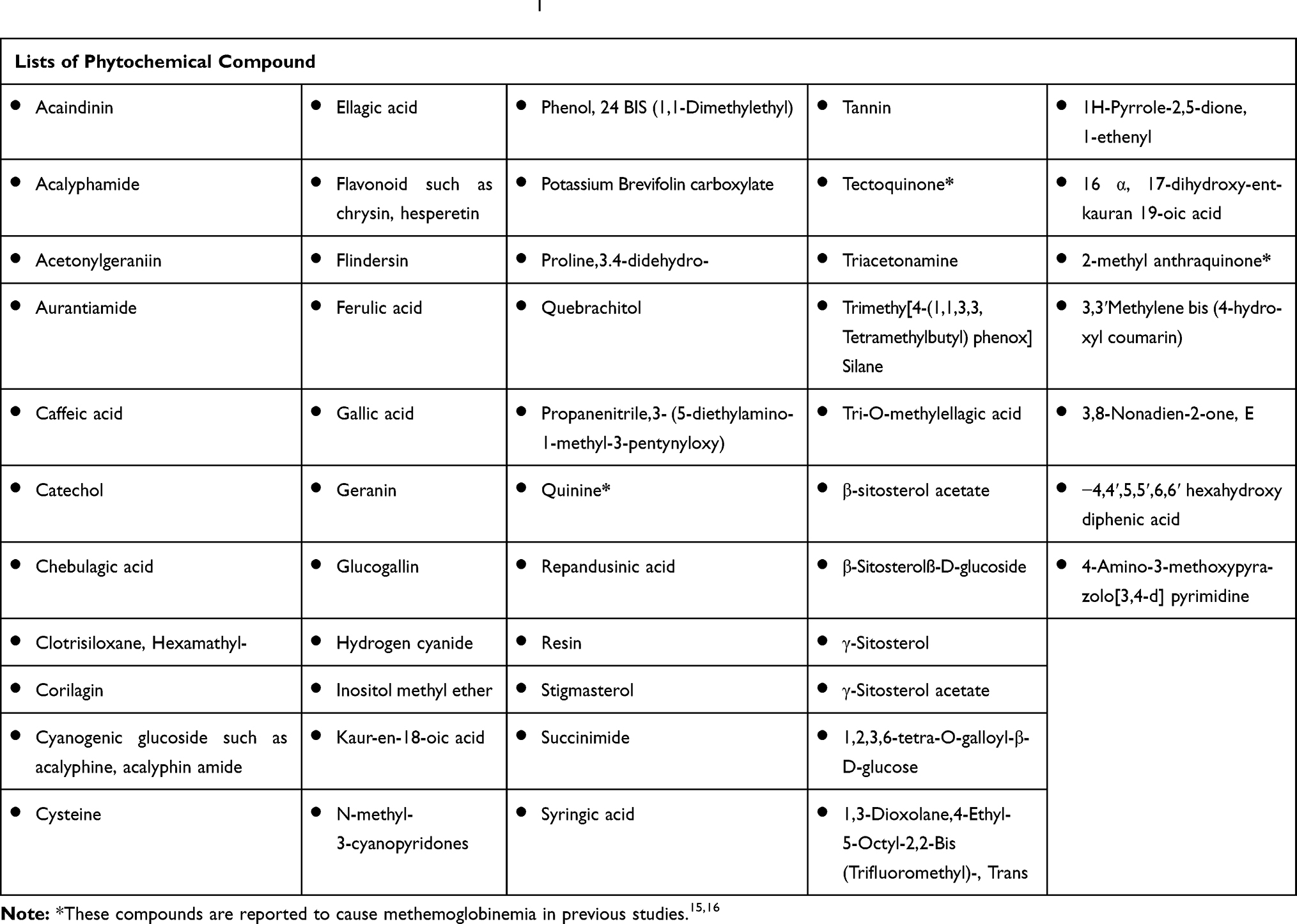 |
Table 3 Phytochemical Compounds in Acalypha Indica.1 |
Reportedly, most patients ingested cooked leaves,4–6 except for one patient who ingested uncooked leaves.13 In this study, patients consumed either a decoction or fresh juice. Hence, these phytochemicals might be heat stable. Moreover, ingestion patterns among countries, preparation methods, phytochemical contents, and concentrations in the Acalypha indica cultivars might contribute to the distinct findings. As doses were inadequately documented, no distinction was observed between the onset and duration of symptoms between single and multiple ingestions, failing to support a dose–response relationship. Symptoms usually occurred within 24 hours of the last ingested dose.
Here, one out of eight patients died. The cause of death might be contributed by hemolysis, severe methemoglobinemia and his preexisting diseases. Hemolysis and methemoglobinemia could be a susceptibility factor that resulted in death, especially in elderly patients with pre-existing medical conditions. The main treatment of Acalypha indica toxicity was supportive care, while methylene blue might be considered in the patient who developed severe methemoglobinemia. To our knowledge, this is the first case series of patients with methemoglobinemia attributed to Acalypha indica.
This study had some limitations which can be listed as follows. First, it is not mandatory to report potentially adverse exposures from Acalypha indica to our poison center. Thus, not all exposures are reported, especially the negligible and mild cases. Second, this study was retrospective in nature together with data obtained from telephone consultations, such that it might have contained some incomplete data. Third, methemoglobin level was not measured and confirmed in all patients, especially during the patient had signs of methemoglobinemia. Therefore, we needed to rely on the saturation gap, response to oxygen therapy and/or cyanosis for diagnosis in these patients. Finally, there was no laboratory test performed to confirm the exact dose of ingestion or to exclude the adulterants causing these adverse events. In addition, we did not retrieve and analyse the biological samples from these patients.
Conclusion
Acalypha indica is used as a herbal medicine in several countries, including Thailand, and can induce adverse effects, such as acute hemolysis. This study presents methemoglobinemia as the other toxicity caused by this plant. The responsible oxidizer might be heat stable. Further studies are needed to elucidate the etiology. Elderly patients with preexisting medical conditions might demonstrate poor outcomes. Public education could help prevent Acalypha indica poisoning cases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zahidin NS, Saidin S, Zulkifli RM, Muhamad II, Ya’akob H, Nur H. A review of Acalypha indica L. (Euphorbiaceae) as traditional medicinal plant and its therapeutic potential. J Ethnopharmacol. 2017;207:146–173. doi:10.1016/j.jep.2017.06.019
2. Priya CL, Rao KVB. Acute and sub-chronic toxicological studies on methanolic stem extract to Acalypha indica Linn in albino wistar rats. Int J Pharm Pharm Sci. 2014;6(9):560–563.
3. Hazali N, Nazri N, Ibrahim M, Masri M. Subchronic toxicity of Malaysian acalypha indica: biochemistry and haematology analysis of rat. Jurnal Teknologi. 2016;78.
4. Lamabadusuriya SP, Jayantha UK. Acalypha indica induced haemolysis in G6PD deficiency. Ceylon Med J. 1994;39(1):46–47.
5. Senanayake N, Sanmuganathan PS. Acute intravascular haemolysis in glucose-6-phosphate dehydrogenase deficient patients following ingestion of herbal broth containing Acalypha indica. Trop Doct. 1996;26(1):32. doi:10.1177/004947559602600113
6. Ehelepola NDB, Abayagunawardana AN, Sudusinghe TN. A vegetable-induced hemolytic crisis in a G6PD deficient person: a case report. BMC Res Notes. 2018;11(1):179. doi:10.1186/s13104-018-3286-9
7. Rattanasunya P. (2015, December 1-5). Acute hemolysis and methemoglobinemia in G6PD deficiency after Acalypha indica ingestion [Abstract Poster Presentation no 48].. 14th International Conference Asia Pacific Association of Medical Toxicology, Perth, Western Australia. Available from: http://www.apamt.org/14th-apamt-poster-presentations/
8. Michaud GF, Stevenson WG. Physiologic and Nonphysiologic Sinus Tachycardia. Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine.
9. Dinarello CA, Porat R. Chapter 15: fever. Jameson L, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine.
10. Roy-Chowdhury N, Roy-Chowdhury J. Classification and causes of jaundice or asymptomatic hyperbilirubinemia. Available from: https://www.uptodate.com/contents/pathophysiology-and-treatment-of-fever-in-adults. Accessed July 4, 2020.
11. Price DP. Methemoglobin inducers. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, editors. Goldfrank’s Toxicologic Emergencies.
12. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Inter Suppl. 2012;2:1–138.
13. Mekavuthikul P, Phuditshinnapatra J. North American Congress of Clinical Toxicology (NACCT) Abstracts 2019. Clin Toxicol. 2019;57(10):870–1052.
14. Marco LAS. Hematologic principle. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, editors. Goldfrank’s Toxicologic Emergencies.
15. Alanazi MQ. Drugs may be induced methemoglobinemia. J Hematol Thrombo Dis. 2017;6:154.
16. Kusumoto S, Nakajima T. Methemoglobin formation by aminophenol and diphenol in rabbits. Ind Health. 1964;2(3–4):133–138. doi:10.2486/indhealth.2.133
17. Rehman A, Shehadeh M, Khirfan D, Jones A. Severe acute haemolytic anaemia associated with severe methaemoglobinaemia in a G6PD-deficient man. BMJ Case Rep. 2018;2018:254.http://iwmsfs:9028/login
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.