")
Back to Journals » Patient Preference and Adherence » Volume 14
Clinical Characteristics and Patient-Reported Outcomes of Primary Care Physiotherapy in Patients with Whiplash-Associated Disorders: A Longitudinal Observational Study
Authors Oostendorp RAB , Elvers JWH , van Trijffel E, Rutten GM, Scholten-Peeters GGM , Heijmans M, Hendriks E, Mikolajewska E , De Kooning M , Laekeman M , Nijs J , Roussel N , Samwel H
Received 13 May 2020
Accepted for publication 22 August 2020
Published 28 September 2020 Volume 2020:14 Pages 1733—1750
DOI https://doi.org/10.2147/PPA.S262578
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Rob AB Oostendorp,1– 4 JW Hans Elvers,5,6 Emiel van Trijffel,7,8 Geert M Rutten,9,10 Gwendolyne GM Scholten-Peeters,11 Marcel Heijmans,4 Erik Hendriks,12,13 Emilia Mikolajewska,14,15 Margot De Kooning,3,16 Marjan Laekeman,17,18 Jo Nijs,3,16,19 Nathalie Roussel,20 Han Samwel21
1Scientific Institute for Quality of Healthcare, Radboud University Nijmegen Medical Centre, Nijmegen, the Netherlands; 2Department of Manual Therapy, Faculty of Medicine and Pharmacy, Vrije Universiteit Brussel, Brussels, Belgium; 3Pain in Motion International Research Group, Department of Physiotherapy, Human Physiology and Anatomy, Faculty of Physical Education and Physiotherapy, Vrije Universiteit Brussel, Brussels, Belgium; 4Practice Physiotherapy and Manual Therapy, Heeswijk-Dinther, the Netherlands; 5Department of Public Health and Research, Radboud University Nijmegen Medical Centre, Nijmegen, the Netherlands; 6Department of Allied Health Care, Methodological Health-Skilled Institute, Beuningen, the Netherlands; 7Department of Master Education, SOMT University of Physiotherapy, Amersfoort, the Netherlands; 8Department of Physiotherapy, Human Physiology and Anatomy, Faculty of Physical Education and Physiotherapy, Vrije Universiteit Brussel, Brussels, Belgium; 9Institute of Health Studies, Faculty of Health and Social Studies, HAN University of Applied Science, Nijmegen, the Netherlands; 10Campus Venlo, Faculty of Science and Engineering, Maastricht University, Maastricht, the Netherlands; 11Department of Human Movement Sciences, Faculty of Behavioral and Movement Sciences, Vrije Universiteit Amsterdam, Amsterdam Movement Sciences, Amsterdam, the Netherlands; 12Department of Epidemiology, Center of Evidence Based Physiotherapy, Maastricht University, Maastricht, the Netherlands; 13Practice Physiotherapy ‘Maasstaete, Druten, the Netherlands; 14Department of Physiotherapy, Ludwik Rydygier Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University, Toruń, Poland; 15Neurocognitive Laboratory, Centre for Modern Interdisciplinary Technologies, Nicolaus Copernicus University, Toruń, Poland; 16Department of Physical Medicine and Physiotherapy, University Hospital Brussels, Brussels, Belgium; 17Department of Nursing Sciences, Ph.D.-Kolleg, Faculty of Health, University Witten/Herdecke, Witten, Germany; 18Department of Physiological Psychology, University of Bamberg, Bamberg, Germany; 19Institute of Neuroscience and Physiology, University of Gothenburg, Gothenburg, Sweden; 20Department of Physiotherapy and Rehabilitation Sciences (MOVANT), Faculty of Medicine and Health Sciences, University of Antwerp, Antwerp, Belgium; 21Revalis Pain Rehabilitation Centre, S Hertogenbosch, the Netherlands
Correspondence: Rob AB Oostendorp
Scientific Institute for Quality of Healthcare, Radboud University Nijmegen Medical Centre, p/a Oude Kleefsebaan 325, AT Berg En Dal 6572, Nijmegen, the Netherlands
Tel +31 246423419
Email [email protected]
Background: Whiplash-associated disorders (WADs) constitute a state of health characterized by a wide diversity of symptoms as a result of impairments of functions, activity limitations, and participation restrictions. Patient-reported outcome measurements (PROMs) and patient-reported outcomes (PROs) seem appropriate when describing and evaluating the health status of patients with WAD.
Aim: To measure the use of PROMs and PROs as quality indicators in clinical reasoning, and to analyze and evaluate pre- and post-treatment ‘pain intensity’ and ‘functioning’, and for ‘perceived improvement’ in patients with WAD in primary care physiotherapy practice by year of referral, with the phase after accident and prognostic health profile embedded in the clinical reasoning process.
Materials and Methods: Data were collected over a period of 10 years. Pain intensity, functioning, and perceived improvement were measured using the Visual Analogue Scale for Pain (VAS-P), the Neck Disability Index (NDI) and the Global Perceived Effect scale (GPE). Pre- and post-treatment mean differences were tested for statistical significance and compared to minimal clinically important differences (MCID). Effect sizes were expressed as Cohen’s d. Multivariable regression analysis was performed to explore independent associations of year of referral, phase after the accident, and the patient’s prognostic health profile with post-treatment pain intensity and functioning.
Results: A consecutive sample of 523 patients was included. Pre- and post-treatment mean differences on VAS-P and NDI were statistically significant (P< 0.000) and clinically relevant, with ‘large’ effect sizes for pain intensity and functioning. MCIDs were achieved by 80% for VAS-P and for 60% for NDI. Year of referral and phase after the accident were independently associated with worse post-treatment functioning. About half of the patients (n=241 [46.1%]) perceived themselves as improved.
Conclusion: The PROMs and PROs pain intensity, functioning and perceived improvement were integrated as quality indicators in the physiotherapy clinical reasoning process for patients with WAD. Significant differences in pain intensity and functioning were found but were unrelated to year of referral, phase after whiplash-related injury or prognostic health profile. The MCID VAS-P scores did not differ depending on experienced pain.
Keywords: whiplash-Associated Disorders, neck pain, physiotherapy, patient-reported outcomes measures, routinely collected data
Introduction
Neck pain constitutes a major health problem in the general population,1–3 and may be associated with many different prognostic factors. One frequently reported cause of (persistent) neck pain is traumatic injury, usually as a result of a motor vehicle accident. Following injury, many patients report a complex of health-related symptoms such as neck pain, arm pain, headache, dizziness, and visual and auditory symptoms, hence the term Whiplash-Associated Disorder (WAD).4,5 This disorder is also characterized by poor coping strategies such as fear avoidance behavior, and by poor outcomes such as activity limitations and restricted participation. Treatment effectiveness and treatment outcomes after whiplash-related injury remain challenging issues, and both show room for improvement.6–8 Due to a range of issues including impairments of sensory functions, pain and neuromusculoskeletal functions, mental functions, activity limitations and participation restrictions, patient-reported outcome measurements (PROMs) are ideally suited to the evaluation of patient-reported outcomes (PROs) in patients with WAD.9,10
PROMs are defined as: ‘… any measurement of the status of a patient’s health condition that comes directly from the patient without interpretation of the patient’s response by a clinician or anyone else,9 while PROs are defined as ‘…. health outcomes directly reported by the patient who experienced it’.11 PROMs and PROs are often used as quality indicators in physiotherapy clinical practice.12,13 Quality indicators have been defined as ‘measurable elements of practice performance for which there is evidence or consensus that they can be used to assess the quality of care provided’.14 In this study, PROMs are used as process indicators and PROs as outcome indicators.
A number of recovery patterns in relation to whiplash-related injury have been reported but little is known concerning the variability of recovery over time. As most studies cease follow-up after one year,15–18 longitudinal studies evaluating the long-term variability of recovery are sparse, although a few studies have evaluated recovery patterns after periods of 5, 15, or 17 years.19–21 Around half of patients report persistent or residual symptoms (such as neck pain, headache, activity limitations and participation problems) a long time after an accident.19–22 High pain intensity and pain-related disability are the most consistent prognostic factors for prolonged activity limitations and participation problems.5,23,24 Prognostic health profiles were introduced in the first publication of Dutch guideline Whiplash and Physiotherapy.25,26 A prognostic health profile can be defined as a complex of positive and negative variables that can be used to estimate the clinical assessment including treatment plan and the chance of recovery,27 specifically the chance of functional recovery in patients with WAD.
Since 1993, the Royal Dutch Association for Physical Therapy has been continuously developing and implementing guidelines, including ‘Physiotherapy Documentation’,28–31 ‘Physiotherapy and Whiplash’25,26 and ‘Neck Pain’,32,33 with the goal of optimizing registration of the clinical reasoning process in patients with WAD based on the phases after whiplash-related accident4 and on prognostic health profiles.34
Use of the PROMs ‘pain intensity’, ‘functioning’ and ‘perceived recovery’ is recommended by and integrated in the Dutch guideline ‘Physiotherapy and Whiplash’.25,26 Recommendations concerning the use of these PROMs as process indicators and PROs as outcome indicators when embedded in the clinical reasoning process have been implemented in Dutch primary care physiotherapy practices.26,34
The primary aim of the present study was to measure the use, in clinical reasoning, of PROMs as process indicators and PROs as outcome indicators. A secondary aim was to analyze and evaluate the routinely collected pre- and post-treatment PROs ‘pain intensity’, ‘functioning’, and ‘perceived recovery’ in WAD patients in primary care physiotherapy practices in relation to the year of referral, phase after whiplash-related injury and prognostic health profile.
Materials and Methods
Design
In 2016, a quality improvement study was launched that focused on the quality of primary care physiotherapy management in patients with WAD. The study was based on an existing dataset (routinely collected dataset whiplash-associated disorders [RCD-WAD]), and details of the design and execution of this retrospective cohort study have been published elsewhere.35,36
The Medical Ethics Committee of Radboud University Medical Centre Nijmegen, The Netherlands waived the requirement for ethical approval. Retrospective research based on anonymized patient files does not fall within the scope of the Medical Research Involving Human Subjects Act because the subject is not physically involved in the research. The data are already available and not collected specifically for this project, and subjects do not have to change their behavior for this project.
Practice Population
Patients were recruited using a consecutive sampling strategy.37 Patients with whiplash-related symptoms were referred by general physicians or medical specialists to two primary care physiotherapy practices in the South of the Netherlands. All patients who met the Quebec Task Force Classification of WAD-1, WAD-2 or WAD-3 were assessed. Following initial screening related to the 5D’s +1 (dizziness, diplopia, drop attacks, dysarthria, dysphagia + nausea), patients with ≥2 Ds were referred back to their general physician. In total, 523 patients were included.
Data Collection
The registration of outcome-related data in the form of PROMs began in 2002. Data on PROMs were collected over a period of 10 years (2002–2011). The current analysis concerns outcome evaluations over this period.
Assessments
Patient assessment was based on a clinical reasoning process consisting of nine steps, including administration, history taking, objectives of examination, clinical examination, conclusion, treatment plan and goals, treatment modalities, evaluation and discharge. Details of the complete clinical reasoning process can be found elsewhere.35 All variables of the clinical reasoning process were operationalized at several different levels of measurement (nominal, ordinal, interval and ratio). See Supplementary file 1.
History taking was used to assess baseline characteristics, including: sociodemographic characteristics (age, gender, educational level and employment status), accident-related characteristics (direction of impact, anticipation of collision, type of trauma, classification WAD, period since accident, and onset of symptoms), pre-existing health status (functioning problems, relevant medication use, previous neck injury, previous neck pain and stiffness, and pain elsewhere), previous diagnostics and treatment (medical imaging diagnostics, use of cervical soft collar, pain medication, [manual] physiotherapy, recovery after treatment), current health status and recovery rate (recovery since accident, functioning problems, pain medication, type and number of symptoms), actual pain behavior and fear avoidance (by means of observation of pain behavior, modified Waddell’s signs, Pain Coping Inventory [PCI], Fear Avoidance Beliefs Questionnaire [FABQ], and prognostic health profile).
The PCI is a 33-item questionnaire measuring active coping (PCI-A: 12 items; total score range 12–48) and passive coping (PCI-P: 21 items; total score range 21–84). Items are scored on a 4-point Likert scale ranging from 1 (hardly ever) to 4 (very often). PCI cutoff scores are ≥24 for active coping, and ≥42 for passive coping.38 The clinimetric properties of the PCI range from acceptable to good.39
The FABQ-Dutch Version (DV) is a 16-item (5 items were not scored) questionnaire measuring fear avoidance beliefs regarding physical activities (FABQ-DV-A: 4 items; total score range: 0 −24) and work-related activities (FABQ-DV-W: 7 items; total score range: 0–42). Items are scored on a 7-point Likert scale ranging from 0 (completely disagree) to 6 (completely agree). FABQ-DV cutoff scores are >15 at risk for pain avoiding behavior, and >34 at risk for not returning to work.40 The clinimetric properties of the FABQ-DV range from acceptable to good.41
Prognostic health profiles were first introduced with the publication of the Dutch guideline ‘Whiplash and Physiotherapy’.25,26 Based on pre-existing symptoms and previous prognostic factors for recovery, patients were classified as Profile A (normal recovery, pain low intensity, decreasing pain, increasing activities, active coping and no fear avoidance), as Profile B (uncertain recovery, medium pain intensity, persistent pain, persistent activity limitations, inconclusive coping and fear avoidance) or as Profile C (delayed recovery, high pain intensity, increasing pain, decreasing activities, passive coping and fear avoidance).
Intervention
Clinical data related to the six phases of the Quebec Task Force WAD4 guided treatment goals and treatment options, combined with the prognostic health profiles (Phase 1: <7 days; acute; normal recovery; Phase 2: 1–3 weeks; acute; normal recovery; phase 3a: 4–6 weeks; sub-acute; uncertain recovery; phase 3b: 4–6 weeks; sub-chronic; delayed recovery; Phase 4a: 7–12 weeks; sub-acute; uncertain recovery; phase 4b: 7–12 weeks; sub-chronic; delayed recovery; Phase 5: 3–6 months; chronic; no recovery; Phase 6: >6 months; chronic; no recovery). A complete flowchart illustrating the clinical reasoning process of physiotherapy management in patients with WAD has been presented elsewhere.35 A summary of treatment goals and physiotherapy modalities per phase 1–6, together with outcomes, is presented in Table 1.
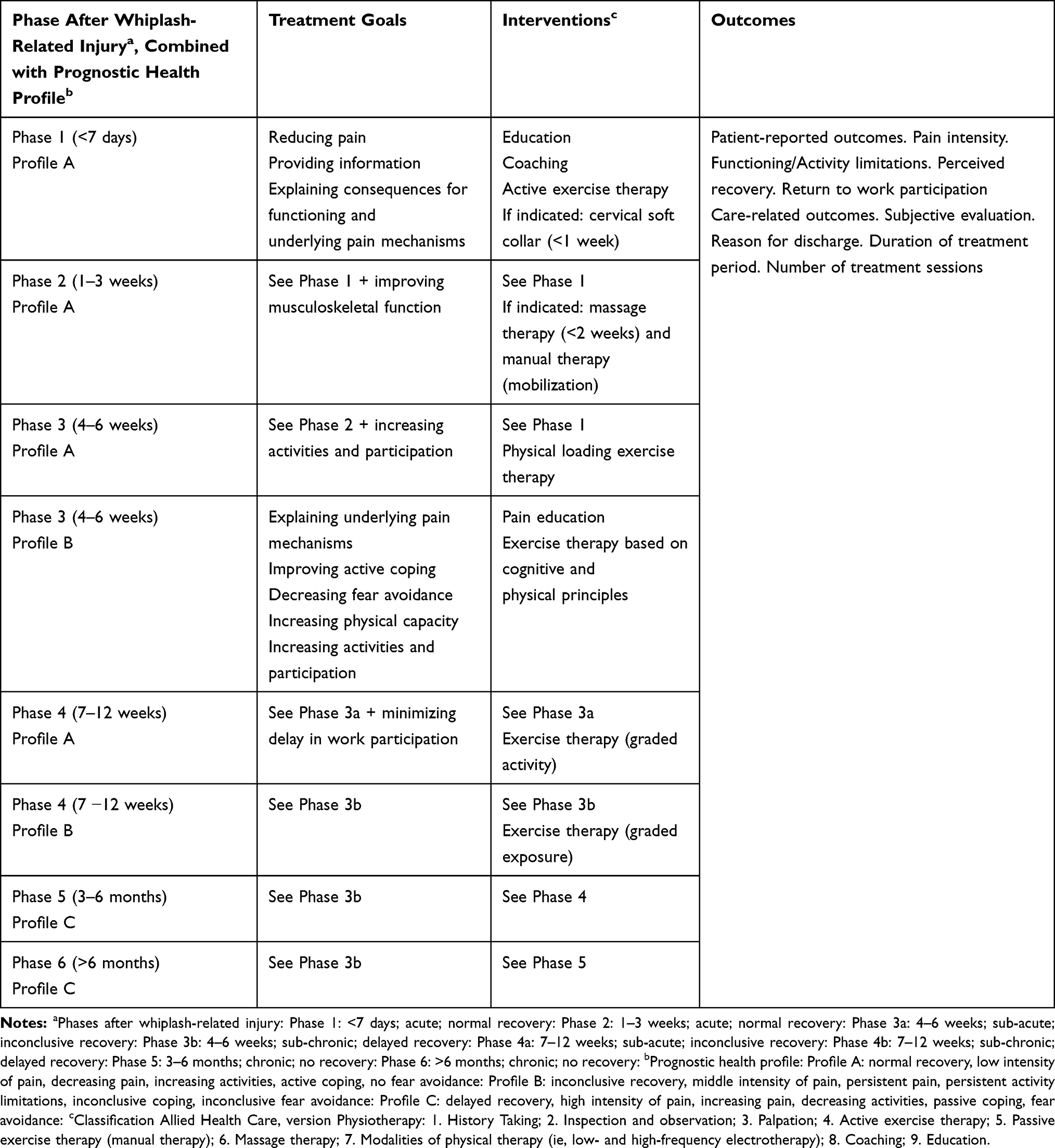 |
Table 1 Phase- and Profile-Based Treatment Goals and Physiotherapy Treatment Modalities, Together with Outcomes for Management in Patients with Whiplash-Associated Disorders (WAD) |
Participating physiotherapists managed patients according to a dynamic protocol consisting of three recovery rate-dependent prognostic health profiles, embedded in the six phases after whiplash-related accident.34 The combined content of treatment modalities was based on the treatment goals per time phase, the prognostic health profiles, and the best available evidence.42–47
Evaluation
In addition to the traditional approach of directly asking a patient about the perceived result of treatment, one of the most rapidly evolving recommendations of the Dutch guideline ‘Physiotherapy and Whiplash’ in 200225,26 involved the introduction of pre- and post-treatment PROMs in clinical practice.
Patient-Reported Outcomes and Patient-Reported Outcome Measurements
The PROs were based on guideline-recommended outcomes and expressed as PROM scores, which included measures of neck pain intensity, functioning, and perceived recovery.48 These recommendations were transformed into quality indicators by phrasing them as the average degree (in %) to which patients were subjected to a methodically performed clinical reasoning process (ie, the average degree [in %] to which pre- and post-treatment pain intensity and functioning were measured and noted). Three newly formulated quality indicators were added to the earlier developed and tested set of quality indicators that were already embedded in the clinical reasoning process for physiotherapy in patients with WAD.35,36
Pain intensity was measured using the Visual Analogue Scale for Pain (VAS-P), which consists of a horizontal 100 mm line scored from 0 (no pain) to 100 (worst imaginable pain).49,50 The minimal clinically important difference (MCID) on VAS-P is 20 mm (≥30% of the initial score).51,52 The VAS-P has proved to be reliable, valid and sensitive to change.53,54 Initial score of ≥55 mm on VAS-P is useful cut-off score to predict poor functional recovery.23
Functioning or activity limitation was measured using the Neck Disability Index (NDI).55,56 The NDI is a self-report questionnaire that measures activity limitations due to neck pain resulting from whiplash-related injuries. The NDI consists of 10 items that address pain intensity, personal care, lifting, reading, headache, concentration, work, driving, sleeping, and recreation. Each item is scored from 0 (no activity limitation) to 5 (major activity limitation). Functioning-related outcome measures (ie, mobility, self-care, domestic life, work and employment) included the Neck Disability Index (NDI). The total score range is 0–50 points, with increasing scores representing increasing impairments and disabilities due to neck pain. The MCID on the NDI is ≥11 points lower than the initial score.52,57-59 The NDI has been translated into Dutch (Dutch version; DV).60 The NDI-DV has proved to be reliable, valid and sensitive to change, and has high internal consistency.61,62 Initial score of >29% from 0–50 points NDI is useful cut-off score to predict poor functional recovery.23
Patients were asked to complete the outcome ‘perceived improvement’, rating the pre- to post-intervention perceived change in improvement from 1 (completely improved) to 6 (much worse).51,63 The Global Perceived Effect (GPE) is a reliable, valid and responsive measure of health status in patients with musculoskeletal pain.63
Participation or participation restrictions in relation to return to work were queried and rated as 1 (no return), 2 (return with adjustments) or 3 (return without adjustments) of patients who were employed before the whiplash-related accident.
Statistical Analysis
Analyses were performed with Statistics 9.0. Descriptive statistics (frequency, means and SDs) were used to characterize the study population’s demographics, accident- and previous and current health-related characteristics, previous diagnostics and treatment, and current functional characteristics. The dataset was checked for missing values. The normality of continuous variables was tested using the Kolmogorov–Smirnov test.
For PROM scores, means and standard deviations (SD) were calculated for pre- and post-treatment scores on pain intensity (VAS-P) and functioning (NDI). The pre- and post-treatment differences in these average scores (including confidence intervals [CI] of 95% [0.05]) were recorded for the total study population (n=523), per year of referral (10-year period [1–10]), per phase (phases 1–6) after whiplash-related injury, and per prognostic health profile (profile A, B and C).
Pre- and post-treatment mean differences were tested for statistical significance with the paired sample t-test (α-value set at 0.05), and for clinical relevance by comparison to established data for the minimal clinically important difference (MCID). Differences ≥30% on the initial score of VAS-P and ≥11 points on NDI51 were considered clinically relevant. Numbers of patients who reached the MCIDs on VAS-P and NDI were calculated and expressed as percentages. Effect size (ES) as magnitude of the difference between the means of pre- and post-treatment scores was expressed in Cohen’s d with 0.21–0.50, 0.51–0.80 and >0.81 considered as small, medium and large effects, respectively.64 Percentage scores were calculated for the three classes of return to work participation.
Percentages scores were also calculated for the perceived improvement. The scores were categorized as ‘improved’ (very good, good, and fairly improved), ‘no change’ (‘same as before’) and ‘worse (worse and much worse).51 A Chi-square test of independence was used to analyze a GPE frequency table constituted of those who did or did not improve (α=0.05).
Finally, multivariable regression analysis was performed to explore independent associations of year of referral, phase after accident, and patients’ prognostic health profile with post-treatment pain intensity and functioning. Beta regression coefficients were estimated with P=0.05, corrected for pre-treatment scores on VAS and NDI, respectively.
Results
The Practice Population
A consecutive sample of 529 patients was originally included, of whom 523 were referred by a GP (n=342; 65.4%) or medical specialist (n=84; 16.1%), and 97 patients visited the practice via self-referral (n=97; 18.5%). Six patients were subsequently referred back to their general physician due to suspicion of serious pathology.
All patients were assessed by one of eight physiotherapists working in two primary care physiotherapy practices. The mean age of the physiotherapists (n=8) at the beginning of the study was 46.2 years (SD 5.6), six were male, and six were manual physiotherapists. The range of experience regarding treatment of patients with whiplash-related injuries varied between 6 and 28 years.
Baseline characteristics of the patients, with no missing values (n=523), are presented in Table 2. Seventy-six percent of patients were female, with a mean age of 43.4 years (SD 13.1). Most patients (n=406; 77.6%) were classified as WAD-2, with a delayed recovery, and were referred 7 weeks to >6 months after an accident (n=293; 56.0%). Fifty-five patients (10.5%) reported a previous whiplash injury and 96 patients (18.4%) previous neck pain and stiffness. Half of the patients had been previously treated with several interventions such as pain medication (n=221; 42.3%), cervical soft collar (n=295; 56.4%), and (manual) physiotherapy (n=234; 44.7%). In 180 patients (34.4%) the results of the earlier treatment were inconclusive, in 104 patients (19.9%) functioning was estimated to have stabilized, and 212 patients (40.5%) showed a deterioration in functioning.
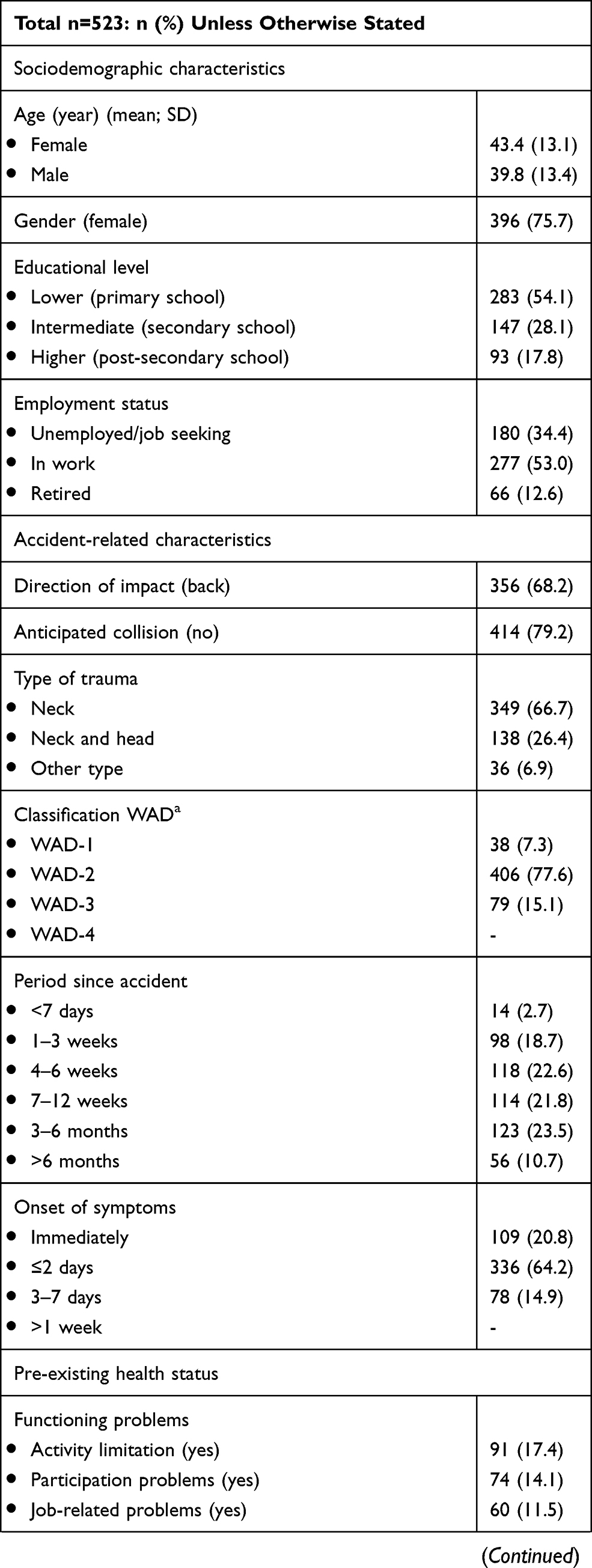 | 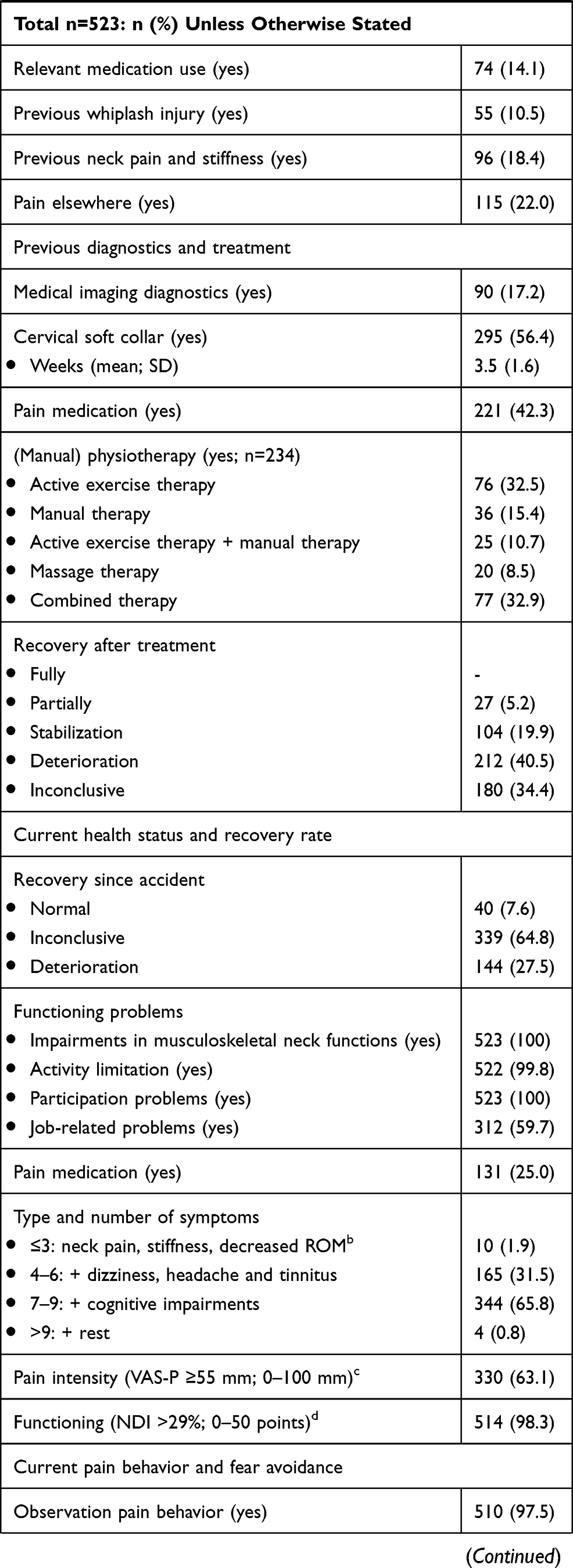 | 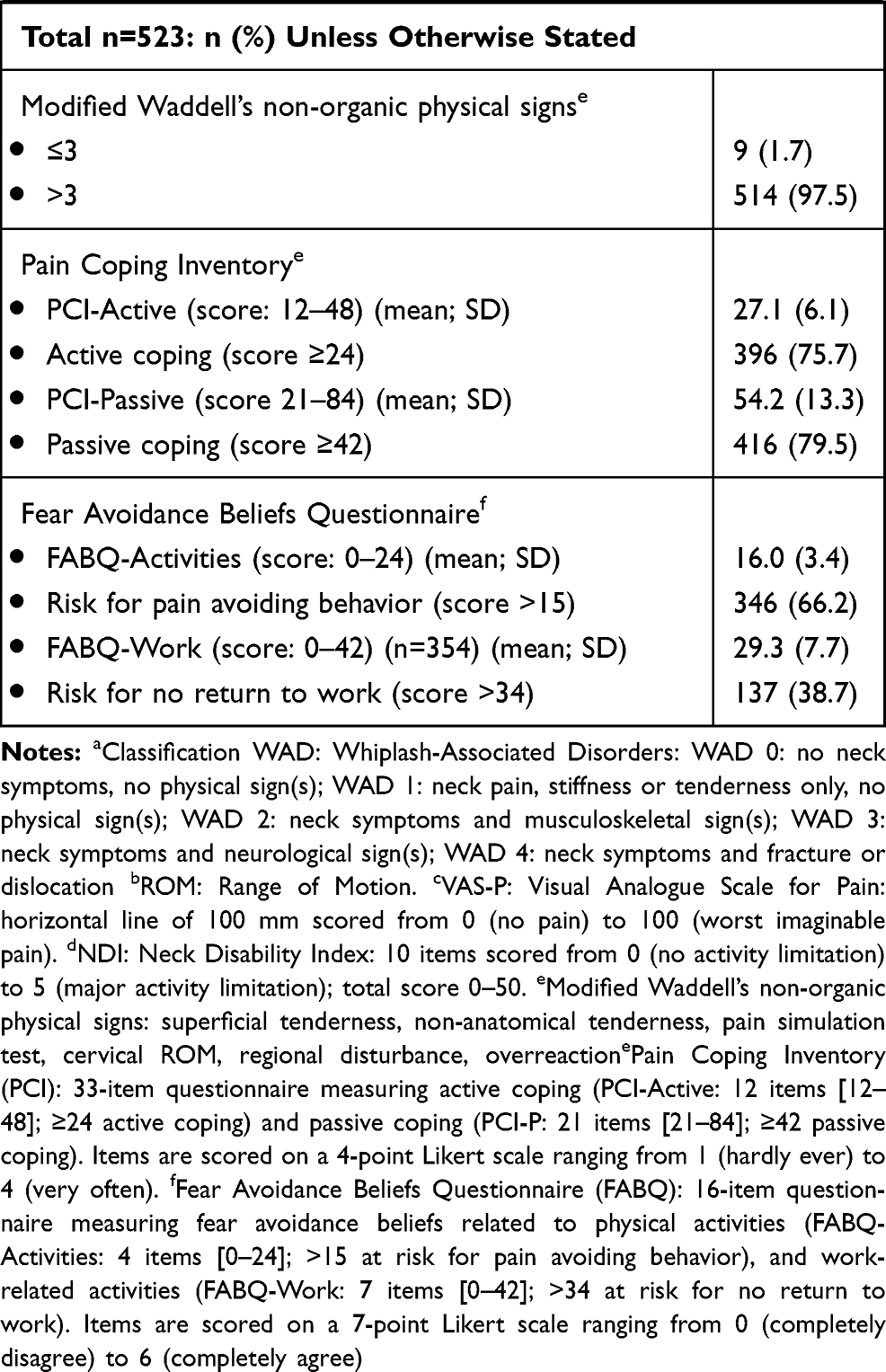 |
Table 2 Baseline Characteristics in Physiotherapy Management in Patients with Whiplash-Associated Disorders |
A number of potentially negative prognostic factors for recovery were reported, including pain intensity, level of functioning, recovery rate since accident (uncertain [n=339; 64.8%] and deterioration [n=144; 27.5%]), modified Waddell’s non-organic physical signs (>3: 514 [97.5%]), risk for poor functional recovery (VAS-P ≥55 mm: n=330 [63.1%]; NDI >29%: n=514 [98.3%]), risk for passive coping (PCI-P ≥42: n=416 [79.5%]), risk for pain avoiding behavior (FABQ-A >15: n=346 [66.2%]), and risk for no return to work (FABQ-W >34: n=137 [38.7%]).
Quality Indicators
Pre-treatment scores for pain intensity (VAS-P) and functioning (NDI) were implemented as process indicators in clinical reasoning (during the treatment plan phase), while post-treatment scores and perceived improvement were implemented as outcome indicators (during the evaluation phase). The new quality indicators met the performance target (≥70%).35
Patient-Reported Outcomes
Outcomes including mean differences between pre- and post-treatment scores on VAS-P and NDI, effect sizes (Cohen’s d), percentage of patients that reached MCIDs, changes in perceived improvement (percentage of “improved”, “no change” or “worse”) in the total group (n=523) and per year of referral are presented in Table 3, per phase 1–6 after whiplash-related injury in Table 4, and per prognostic health profile (profile A (n=40 [7.6%]), profile B (n=339 [64.8%]) or profile C (n=144 [27.5%])) in Table 5.
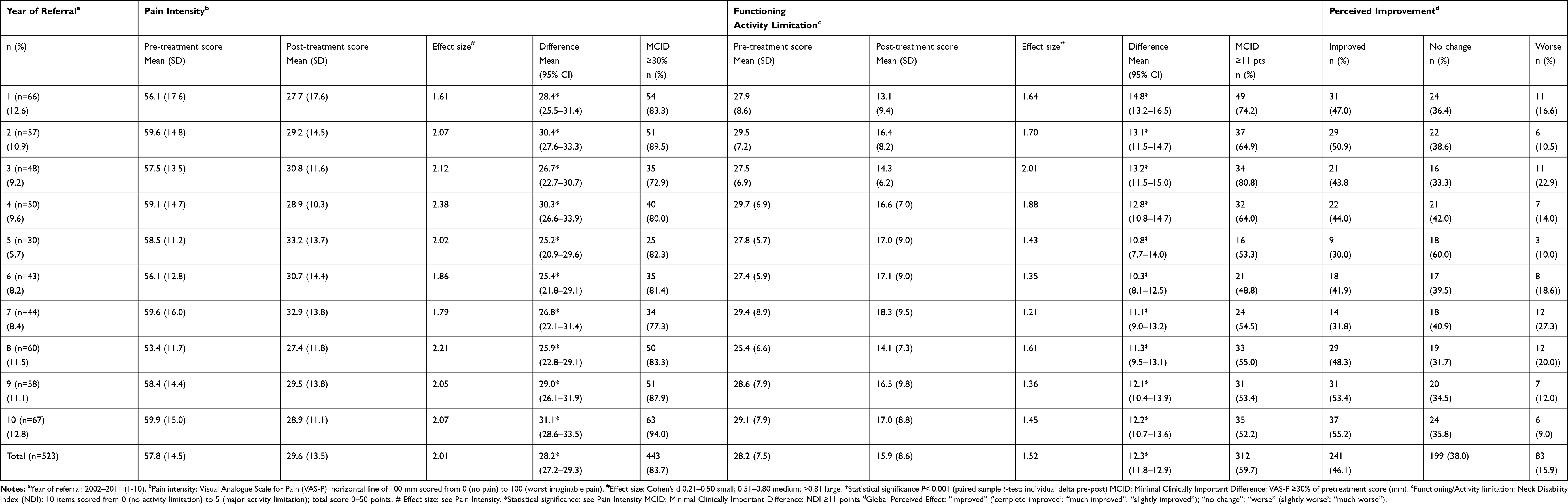 |
Table 3 10 Year Related Outcomes for Physiotherapy Management in Patients with Whiplash-Associated Disorders (WAD) (n=523) |
 |
Table 4 Phase-Related Outcomes for Physiotherapy Management in Patients with Whiplash-Associated Disorders (WAD) (N=523) |
 |
Table 5 Health Profile-Related Outcomes for Physiotherapy Management in Patients with Whiplash-Associated Disorders (WAD) (n=523) |
Year of Referral
Pre- and post-treatment mean differences on VAS-P and NDI were statistically significant (P<0.000) and clinically relevant for the total group and for the groups per year of referral (except for the NDI-MCID at years 5 and 6). The percentage of patients who reached MCIDs was noted for MCID VAS-P (≥30%, ranging from 72.9 to 94.0%) and for MCID NDI (≥11 points, ranging from 48.8 to 80.8%). The MCID for the total group was reached by 83.7% (n=443) for VAS-P and 59.7% (n=312) for NDI. A “large” effect size (Cohen’s d >0.81) was noted for pain intensity, ranging from 1.61 (year 1) to 2.38 (year 4), and for functioning, ranging from 1.21 (year 7) to 2.01 (year 3). The effect size for the total group was also “large”.
About half of the patients were “improved” according to the global perceived improvement scale (n=241; 46.1%), about two fifth “no change” (n=199; 38.0%), and about one fifth “worse” (n=83; 15.9%) for the total group; about the same percentages per year of referral.
Multivariable regression analysis revealed that year of referral was independently associated with post-treatment worse functioning (β 0.27, P<0.00), but not with post-treatment pain intensity (β 0.01, P 0.97).
Phases After Whiplash-Related Injury
Pre- and post-treatment mean differences on VAS-P and NDI were statistically significant (P<0.000) and clinically relevant for the total group (n=523), and for the phases 1–6 after whiplash-related injury separately. The percentage of patients who reached MCIDs was noted for MCID VAS-P (≥30%, ranging from 79.6 to 86.4%) and for MCID NDI (≥11 points, ranging from 53.6 to 68.4%). Effect sizes for pain intensity were “large” (Cohen’s d >0.81), ranging from 1.54 (phase 1) to 2.41 (phase 6), and were also “large” for functioning, ranging from 1.28 (phase 1) to 1.75 (phase 2). The effect size for the total group was “large”. About half of the patients were “improved” according to the global perceived improvement scale (n=241; 46.1%).
Phase after the accident was independently associated with post-treatment worse functioning (β 0.45, P 0.03), but not with post-treatment pain intensity (β 0.20, P 0.57).
Prognostic Health Profiles
Pre- and post-treatment mean differences on VAS-P and NDI were statistically significant (p<0.00) and clinically relevant for the total group (n=523) and for prognostic health profile A, profile B and profile C separately. The percentage of patients who reached MCIDs was noted for MCID VAS-P (≥30%, ranging from 81.3 to 95.0%) and for MCID NDI (≥11 points, ranging from 57.2 to 67.5%). Effect sizes for pain intensity and functioning across the prognostic health profiles were large (pain intensity ranging from 1.89 [profile A] to 2.40 [profile C]; functioning from 1.60 [profile A] to 1.66 [profile B]).
About half of the patients were “improved” according to the GPE (n=241; 46.1%). The difference between “improved” and “worse” on the GPE was statistically significant for all profiles (P<0.00).
Patient prognostic health profiles were not independently associated with post-treatment pain intensity (β 0.80, P 0.40), nor with post-treatment functioning (β 0.82, P 0.15).
Employment
Of the 523 patients, 423 patients (80.9%) were employed at the moment of referral. At the end of their treatment period, 168 patients (39.7%) did not return to work and remained on sick-leave, 123 patients (29.1%) returned with adjustments, and 132 (31.2%) returned without adjustments.
Discussion
In the description of clinical reasoning in patients with WAD, process and outcome indicators for physiotherapy represent an important step forwards in understanding the relationship between process and outcome. Having defined the benefits of using PROMs and PROs as the degree to which VAS-P, NDI and perceived improvement were used and noted in the clinical reasoning process, our analysis suggests that the use of these PROMs and PROs improved the quality of care.
In this study, we found statistically and clinically significant differences in pain intensity and functioning that were unrelated to year of referral, phase after whiplash-related injury or prognostic health profile. MCID values were approximately 80% for VAS-P and 60% for functioning (NDI). Perceived improvement was more likely with a positive (profile A) than with a negative prognostic health profile (profile C).
Patient Population and Specialist Primary Care Physiotherapy Practice
All patients were referred to two primary care physiotherapy practices, both of which were specialized in the assessment and management of patients with neck pain. With the exception of a few patients with red flags, complete data on all included patients were assessed in this retrospective cohort study. The characteristics of our patient sample were comparable to participants in other Dutch studies65–68 and to patients in international studies.,69,70 and the characteristics of the participating physiotherapists were comparable to the national average.71
Patient-Reported Outcomes
As mentioned in the introduction, longitudinal studies were identified that described patient follow-up at 1 year15,18 or at 5, 15 or 17 years19,21 following a motor vehicle accident. Although there are a great number of studies investigating prognostic factors in relation to the course of recovery in patients with WAD, to the best of the authors’ knowledge, no previous study of equivalent duration has described the quality of the clinical reasoning process, including the integration of the PROMs and PROs “pain intensity”, “functioning” and “perceived improvement” as indicators, in patients after WAD-related accident referred to specialist primary care physiotherapy practices.
Year of Referral
The period of time before referral after whiplash-related accident has shifted over the years, becoming longer. Unsurprisingly, referrals in the final years of the study included a higher proportion of chronic cases relative to the early years. This factor presumably explains the outcome of worse functioning as time progressed.
It is clear that over the years of referral most patients reached the MCID value of ≥30% for initial pain intensity score. Although a percentage and not a fixed number of mm was chosen as initial pain intensity threshold, an unanswered question is whether the MCID VAS-P score differs with the intensity of pain experienced. In retrospect, it might have been better to use a reduction in VAS-P of 20% for mild pain (VAS-P ≤30 mm), 30% for moderate pain (VAS-P 31–60 mm) and 40% for severe pain (VAS-P 61–100 mm). This variable “minimal” reduction probably corresponds more closely to patients’ perception of their pain experience than a reduction of ≥30% of all initial scores.72
Phases After Whiplash-Related Injury
The time frame defined by the Quebec Task Force WAD4 guided the clinical management of patients in this study and other studies. The time frame, combined with prognostic factors, defined three profiles in relation to recovery. However, distinguishing between “normal recovery”, “delayed recovery” or “no recovery” at the moment of referral was clinically difficult, and the distinction between “normal recovery” and “delayed recovery” was particularly unclear in the early phases after the whiplash injury. This resulted in the classification of more than half of the patients as ’uncertain recovery’. Nevertheless, the direction of recovery became clearer over the course of the treatment period and treatment sessions.
It was also apparent that the effect sizes for reduction of pain intensity in the later chronic phases were larger than those in the acute phases. A plausible explanation for this observation is that it is “easier” to lower a severe pain intensity score (VAS-P >61 mm) than a mild score (VAS-P <30 mm). Furthermore, patients with chronic pain are more often interested in reducing pain intensity than in increasing functioning.
The phases 4, 5 and 6 had a higher proportion of chronic cases relative to earlier phases. This finding is presumably associated with the outcome of worse functioning.
The percentage of patients showing “improvement”, “no change” or “worse” was approximately equivalent across all phases. This emphasizes the superiority of classifications based on prognostic factors for recovery, which can be influenced by physiotherapy treatment, compared to time-related classifications in relation to whiplash-related injury.
Prognostic Health Profile
A definition of a prognostic health profile is a complex of positive and negative variables that can be used to estimate the chance of functional recovery in patients with WAD.27 The prognostic health profiles used here were based on the recognition of the clinical patterns of positive or negative prognostic factors for recovery. Five prognostic factors were included (course of recovery, pain intensity, functioning, coping, and fear avoidance). However, many other prognostics predict the outcome in patients with whiplash-related injury, such as pain intensity, widespread pain, sensory hypersensitivity, previous activity limitations, frequency of deterioration after previous treatment, history of previous neck injury, and behavioral and psychological factors.18,24,73-77 It is becoming increasingly clear that compensation and legal factors also often contribute to prognostics after whiplash-related injury.78 These factors were not included in the clinical estimation of prognostic patterns in this study.
It is not known how far the participating physiotherapists may have weighed all these prognostic factors when drawing up treatment plans, estimating the length of the treatment period, and determining the number of treatment sessions. Physiotherapists generally show a preference for dealing with mechanical aspects of whiplash injury, despite the growing recognition of psychological and cognitive factors as major contributing factors.79–82 In general, physiotherapists are inclined to overestimate the value of their own clinical assessment in their process of clinical reasoning and decision making, rather than applying guideline-based recommendations and using pre-treatment scores of pain intensity and functioning, and the risk scores of active or passive coping and fear avoidance.
Elements of prognostic health profiles were integrated into treatment goals and the choice of treatment modalities. For instance, positive prognostic factors (ie, low pain intensity, moderate activity limitation and active coping) were integrated into treatment goals for (acute) phases 1–3, and negative prognostic factors (ie, increasing pain intensity, decreasing activities and passive coping) into treatment goals for (chronic) phases 4–6. However, a prognostic profile is often a mix of positive and negative factors, but may sometimes include mainly positive or mainly negative factors. Perceived complete or optimal improvement was reported by around 80% of the patients with mostly positive prognostic factors, about 40% with a mix of positive and negative prognostic factors, and 40% with negative prognostic factors, distributed over all phases.
It might be worthwhile to consider replacing clinical estimations of pain intensity, functioning, coping and fear avoidance in prognostic profiles with individual pre-treatment scores for pain intensity and functioning, together with risk scores for passive coping and fear avoidance. About 80% of the study population was at risk for passive coping and about 66% was at risk for pain avoiding behavior. In contrast to the prognostic profiles used here, scores on the PCI and FABQ were moderately but significantly associated with the PROs “pain intensity”, “functioning” and “perceived improvement” in patients with WAD.36 Integration of these measurement scores into the clinical reasoning process and the treatment plan, goals and modalities in the physiotherapy assessment of patients with WAD would represent a further improvement.
A second consideration is the possible construction of a multicomponent prognostic sum score, analogous to the impairment sum score used in patients with reflex sympathetic dystrophy.83 Scores for pain, range of motion, temperature and volume were transformed into scores ranging from 1 to 10, resulting in a sum score from 4 to 40. The impairment sum score has been shown to be reliable, valid and responsive in patients with reflex sympathetic dystrophy.83 In a similar manner, it should be possible to convert generic (ie, VAS-P, PCI and FABQ) and non-generic (ie, previous history of neck injury, type and number of whiplash-related symptoms, and NDI scores) prognostic factors into a sum score as a tool to steer treatment plans for WAD, and a comparable tool (risk assessment score) has already been developed by the Danish Whiplash Study Group.84 Optimizing physiotherapy treatment based on a sum score of generic and non-generic prognostic factors is a challenge, but will likely improve the process of clinical reasoning, decision making, and outcomes in patients with WAD.
Ceiling Effect of Physiotherapy Treatment
Nearly all patients reached the MCID value for pain intensity and more than half reached the MCID value for functioning in all phases after whiplash-related injury and in all prognostic health profiles. However, only about half of the patients experienced actual improvement. One plausible explanation is a “ceiling effect” in the treatment response.
International data indicate that approximately 50% of people who experience a whiplash accident will not recover but will continue to experience ongoing disability and pain at one year or longer after an accident.15–21 One plausible explanation is a ceiling effect for physiotherapy treatment in patients with WAD. Despite the poor prospects for recovery, treatment response remains an important issue. One of the conclusions of a recently published synthesis of the best available evidence in patients with neck pain, including WAD, was that different physiotherapy modalities or combinations of modalities have only small to moderate effect sizes in the short term, with low to moderate certainty of evidence.8 In the past twenty years, little real progress has been made in the “treatment-response” relationship in patients with WAD. Indeed, many reviews have called for further research in an effort to identify tractable factors associated with an optimal treatment response. However, despite a multitude of studies, treatment effectiveness and treatment outcomes after a whiplash-related injury are still a matter of considerable debate. One possible resolution of this question is the contention that an optimal treatment response relationship has already been achieved.
Limitations
The principal limitations of this retrospective cohort study were involvement of only two primary care physiotherapy practices in the Netherlands, and data were collected by eight physiotherapists in total. These two practices are specialized in the assessment and management of patients with WAD. While the characteristics of the participating physiotherapists were comparable to the national average72 and the patient sample was comparable to participants in other Dutch studies,66–68 the low number of participating practices and physiotherapists may have limited generalizability of the results.
The dataset was checked in 2016 for completeness and actuality. The content of the pen and paper patient record was confirmed on the basis of Dutch guidelines “Physiotherapy Documentation”, as published in 201630 and in 2019.31 Although the pen and paper record has now been replaced by electronic patient documentation,85 the pen and paper record used in this study still meets the requirements of the most recent Dutch CPG Physiotherapy Documentation.31 Despite the limitations of RCD studies generally, including this RCD-WAD study, the expectation was that the results of this study could plausibly represent insights into the PROs and treatment-related outcomes in patients with WAD anno 2020. In order to assess the quality of our study using the RCD-WAD, we compared the text to the criteria of the RECORD statement and found that most criteria were met.86,87
Another limitation of this study was the length of follow-up, which was limited to one or two contacts within a few months of discharge. With regard to primary care physiotherapy, the Dutch health care system sets a maximum number of sessions and does not allow for longer follow-up. The variability in pain and functioning found in patients in long-term studies16,18 can presumably be extrapolated to the patient population in the present study. However, due to an incomplete understanding of the long-term variability of symptoms and functioning beyond the treatment period, it is very difficult to give patients a realistic personal outlook regarding long-term functioning. Nonetheless, electronic tools can be used to define MCIDs for pain intensity and functioning, which in turn provide useful individual information on whether the patient shows a meaningful improvement or a worsening of pain and functioning over time.
In contrast to longitudinal studies,19–21 our study only included data gathered during the treatment episode, without additional follow-up. Within these limitations, about half of the patients improved while the other half were categorized as “no change” or “worse”, without meaningful differences related to year of treatment or phase after whiplash-related injury. Based on the results of longitudinal studies of functional recovery after whiplash-related injury, it seems unlikely that recovery rates will improve substantially in the future. International data also indicate that approximately 50% of people involved in a whiplash accident will not recover and will continue to experience ongoing activity limitations and long-term neck pain.
Conclusion
This study highlighted the integration of PROMs and PROs as quality indicators in the clinical reasoning process in the management of patients with WAD. These recommended measurements were successfully applied in two primary care physiotherapy practices over a period of 10 years, across all phases after whiplash-related accident and with different prognostic health profiles.
Statistically and clinically important differences in pain intensity and functioning were found but were unrelated to year of referral, phase after whiplash-related injury or prognostic health profile.
The MCID VAS-P score did not differ depending on experienced pain.
Finally, improving the integration of the consensus-based PROMs that underpin the process of clinical reasoning in patients with WAD will improve the homogeneity and comparability of data collected in primary care physiotherapy practice.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bovim G, Schrader H, Sand T. Neck pain in the general population. Spine. 1994;19(12):1307–1309. doi:10.1097/00007632-199406000-00001
2. Carroll LJ, Hogg-Johnson S, van der Velde G, et al. Bone and joint decade 2000-2010 task force on neck pain and its associated disorders. Course and prognostic factors for neck pain in the general population: results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. Spine. 2008;33(4Suppl):S75–82. doi:10.1097/BRS.0b013e31816445be
3. Croft PR, Lewis M, Papageorgiou AC, et al. Risk factors for neck pain: a longitudinal study in the general population. Pain. 2001;93(3):317–325. doi:10.1016/S0304-3959(01)00334-7
4. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific monograph of the quebec task force on whiplash-associated disorders: redefining “whiplash” and its management. Spine. 1995;20(8Suppl):1S–73S.
5. Carroll LJ, Holm LW, Hogg-Johnson S, et al. Course and prognostic factors for neck pain in whiplash-associated disorders (WAD): results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. Spine. 2008;33(4Suppl):S83–92. doi:10.1097/BRS.0b013e3181643eb8
6. Hurwitz EL, Carragee EJ, van der Velde G, et al. Bone and joint decade 2000-2010 task force on neck pain and its associated disorders. treatment of neck pain: noninvasive interventions: results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. Spine. 2008;33(4Suppl):S123–152. doi:10.1097/BRS.0b013e3181644b1d
7. Sterling M. Physiotherapy management of whiplash-associated disorders (WAD). J Physiother. 2014;60:5–12. doi:10.1016/j.jphys.2013.12.004
8. Sterling M, de Zoete RMJ, Coppieters I, Farrell SF. Best evidence rehabilitation for chronic pain part 4: neck pain. J Clin Med. 2019;8(8):
9. Kyte DG, Calvert M, van der Wees PJ, Ten Hove R, Tolan S, Hill JC. An introduction to patient-reported outcome measures (PROMs) in physiotherapy. Physiotherapy. 2015;101(2):119–125. doi:10.1016/j.physio.2014.11.003
10. Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353–367. doi:10.2147/PROM.S156279
11. Patient-reported outcome. Available from: https://en.wikipedia.org/wiki/Patient-reported_outcome.
12. Verburg AC, van Dulmen SA, Kiers H, Nijhuis-van der Sanden MWG, van der Wees PJ. Development of a standard set of outcome measures for non-specific low bac pain in Dutch primary care physiotherapy practices: a Delphi study. Eur Spine J. 2019;28(7):1550–1564. doi:10.1007/s00586-019-05962-x
13. van Dulmen SA, van der Wees PJ, Staal JB, Braspenning JCC, Nijhuis-van der Sanden MWG. Patient reported outcome measures (PROMs) for goalsetting and outcome measurement in primary care physiotherapy, an explorative field study. Physiotherapy. 2017;103(1):66–72. doi:10.1016/j.physio.2016.01.001
14. Lawrence M, Olesen F. Indicators of quality health care. Eur J Gen Pract. 1997;3:103–108. doi:10.3109/13814789709160336
15. Kasch H, Qerama E, Kongsted A, Bendix T, Jensen TS, Bach FW. Clinical assessment of prognostic factors for long-term pain and handicap after whiplash injury: a 1-year prospective study. Eur J Neurol. 2008;15(11):1222–1230. doi:10.1111/j.1468-1331.2008.02301.x
16. Myrtveit SM, Carstensen T, Kasch H, Ørnbøl E, Frostholm L. Initial healthcare and coping preferences are associated with outcome 1 year after whiplash trauma: a multicentre 1-year follow-up study. BMJ Open. 2015;5(3):e007239. doi:10.1136/bmjopen-2014-007239
17. Gehrt TB, Wisbech Carstensen TB, Ørnbøl E, Fink PK, Kasch H, Frostholm L. The role of illness perceptions in predicting outcome after acute whiplash trauma: a multicenter 12-month follow-up study. Clin J Pain. 2015;31(1):14–20. doi:10.1097/AJP.0000000000000085
18. Åsenlöf P, Bring A, Söderlund A. The clinical course over the first year of whiplash associated disorders (WAD): pain-related disability predicts outcome in a mildly affected sample. BMC Musculoskelet Disord. 2013;14:361. doi:10.1186/1471-2474-14-361
19. Styrke J, Sojka P, Björnstig U, Stålnacke BM. Symptoms, disabilities, and life satisfaction five years after whiplash injuries. Scand J Pain. 2014;5(4):229–236. doi:10.1016/j.sjpain.2014.06.001
20. Squires B, Gargan MF, Bannister GC. Soft-tissue injuries of the cervical spine. 15-year follow-up. J Bone Joint Surg Br. 1996;78(6):955–957. doi:10.1302/0301-620X.78B6.0780955
21. Bunketorp L, Nordholm L, Carlsson J. A descriptive analysis of disorders in patients 17 years following motor vehicle accidents. Eur Spine J. 2002;11(3):227–234. doi:10.1007/s00586-002-0393-y
22. Carroll LJ, Hogg-Johnson S, Cote P, et al. Course and prognostic factors for neck pain in workers: results of the bone and joint decade 2000-2010 task force on neck pain and lts associated disorders. Spine. 2008;33(4Suppl):S93–S100. doi:10.1097/BRS.0b013e31816445d4
23. Kamper SJ, Rebbeck TJ, Maher CG, McAuley JH, Sterling M. Course and prognostic factors of whiplash: a systematic review and meta-analysis. Pain. 2008;138(3):617–629. doi:10.1016/j.pain.2008.02.019
24. Walton DM, Pretty J, MacDermid JC, Teasell RW. Risk factors for persistent problems following whiplash injury: results of a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2009;39(5):334–350. doi:10.2519/jospt.2009.2765
25. Bekkering GE, Hendriks HJM, Lanser K, et al. KNGF-richtlijn Whiplash (KNGF guideline Whiplash). Ned Tijdschr Fysiother. 2001;111(Supplement):Sl–S25.
26. Scholten-Peeters GGM, Bekkering GE, Verhagen AP, et al. Clinical practice guideline for the physiotherapy of patients with whiplash-associated disorders. Spine. 2002;27(4):412–422. doi:10.1097/00007632-200202150-00018
27. Vaes P, Kerckhofs E, Beckwée D, Oostendorp RAB. Definitie Gezondheidsprofiel (Definition Health Profile). In: Gezondheidsprofiel (Health Profile). Vaes P, Kerckhofs E, Beckwée, Edited by. Antwerpen: Standaard Uitgeverij; 2011:pp42–61.
28. Koninklijk Nederlands Genootschap Fysiotherapie. Richtlijnen Voor De Fysiotherapeutische Verslaglegging (KNGF-Guidelines Physiotherapy Documation). Amersfoort: KNGF; 1993.
29. Heerkens YF, Lakerveld-Heyl K, Verhoeven ALJ, Hendriks HJM. KNGF-richtlijn Fysiotherapeutische Verslaglegging (KNGF-Guidelines Physiotherapy Documation). Ned Tijdschr Fysiother. 2007;117(6):Supplement 1–20.
30. Koninklijk Nederlands Genootschap Fysiotherapie. KNGF-Richtlijn Fysiotherapeutische Dossiervorming (KNGF-Guidelines Physiotherapy Documentation). Amersfoort: KNGF; 2016.
31. Koninklijk Nederlands Genootschap Fysiotherapie. KNGF-Richtlijn Fysiotherapeutische Dossiervorming (KNGF-Guideline Physiotherapy Documentation). Amersfoort: KNGF; 2019.
32. Bier JD, Scholten-Peeters GGM, Staal JB, et al. KNGF-Richtlijn Nekpijn. Amersfoort: KNGF; 2016.
33. Bier JD, Scholten-Peeters GGM, Staal JB, et al. Clinical practice guideline for physical therapy assessment and treatment in patients with nonspecific neck pain. Phys Ther. 2018;98(3):162–171. doi:10.1093/ptj/pzx118
34. Scholten-Peeters GG, Verhagen AP, Neeleman-van der Steen CW, Hurkmans JC, Wams RW, Oostendorp RA. Randomized clinical trial of conservative treatment for patients with whiplash-associated disorders: considerations for the design and dynamic treatment protocol. J Manipulative Physiol Ther. 2003;26(7):412–420. doi:10.1016/S0161-4754(03)00092-7
35. Oostendorp RAB, Elvers JWH, van Trijffel E, et al. Has the quality of physiotherapy care in patients with Whiplash-associated disorders (WAD) improved over time? A retrospective study using routinely collected data and quality indicators. Patient Prefer Adherence. 2018;12:2291–2308. doi:10.2147/PPA.S179808
36. Oostendorp RAB, Elvers JWH, van Trijffel E, et al. Relationships between context, process, and outcome indicators to assess quality of physiotherapy care in patients with whiplash-associated disorders: applying donabedian’s model of care. Patient Prefer Adherence. 2020;14:425–442. doi:10.2147/PPA.S234800
37. Mathieson K. Making sense of biostatistics: making sense of biostatistics: types of nonprobability sampling. J Clin Res Best Pract. 2014;10(10). Available from: https://firstclinical.com/journal.
38. Kraaimaat FW, Bakker A, Evers AMW. Pijncoping-strategieën bij chronische pijnpatiënten. De ontwikkeling van de Pijn-Coping-lnventarisatielijst (PCI). [Pain-coping strategies in chronic pain patients: the development of the Pain Coping lnventory (PCI)]. Gedragstherapie. 1997;30:185–201.
39. Kraaimaat FW, Evers AW. Pain-coping strategies in chronic pain patients: psychometric characteristics of the pain-coping inventory (PCI). Int J Behav Med. 2003;10(4):343–363. doi:10.1207/S15327558IJBM1004_5
40. Waddell G, Newton M, Henderson I, Somerville D, Main CJ, Fear-Avoidance Beliefs A. Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–168. doi:10.1016/0304-3959(93)90127-B
41. Vendrig A, Deutz P, Vink L. Nederlandse vertaling en bewerking van de fear-avoidance beliefs questionnaire. Ned Tijdschr Pijn Pijnbestr. 1998;18(1):11–14.
42. Peeters GG, Verhagen AP, de Bie RA, Oostendorp RA. The efficacy of conservative treatment in patients with whiplash injury: a systematic review of clinical trials. Spine. 2001;26(4):E64–73. doi:10.1097/00007632-200102150-00006
43. Verhagen AP, Scholten-Peeters GG, de Bie RA, Bierma-Zeinstra SM. Conservative treatments for whiplash. Cochrane Database Syst Rev. 2004(1):CD003338.
44. Seferiadis A, Rosenfeld M, Gunnarsson R. A review of treatment interventions in whiplash-associated disorders. Eur Spine J. 2004;13(5):387–397. doi:10.1007/s00586-004-0709-1
45. Kongsted A, Qerama E, Kasch H, et al. Neck collar, “act-as-usual” or active mobilization for whiplash injury? A randomized parallel-group trial. Spine (Phila Pa 1976. 2007;32(6):618–626. doi:10.1097/01.brs.0000257535.77691.bd
46. Goldsmith CH, Gross AR, MacDermid J, Santaguida PL, Miller J. What does the evidence tell us about design of future treatment trials for whiplash-associated disorders? Spine (Phila Pa 1976. 2011;36(25 Suppl):S292–302. doi:10.1097/BRS.0b013e3182388259
47. Rushton A, Wright C, Heneghan N, Eveleigh G, Calvert M, Freemantle N. Physiotherapy rehabilitation for whiplash associated disorder II: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2011;1(2):e000265. doi:10.1136/bmjopen-2011-000265
48. Pietrobon R, Coeytaux RR, Carey TS, Richardson WJ, DeVellis RF. Standard scales for measurement of functional outcome for cervical pain or dysfunction: a systematic review. Spine. 2002;27(5):515–522. doi:10.1097/00007632-200203010-00012
49. Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990;13(4):227–236. doi:10.1002/nur.4770130405
50. Kamper SJ, Grootjans SJ, Michaleff ZA, Maher CG, McAuley JH, Sterling M. Measuring pain intensity in patients with neck pain: does it matter how you do it? Pain Pract. 2015;15(2):159–167. doi:10.1111/papr.12169
51. Ostelo RWJG, De Vet HCW. Clinically important outcomes in low back pain. Best Pract Res Clin Rheumatol. 2005;19(4):593–607. doi:10.1016/j.berh.2005.03.003
52. Pool JJ, Ostelo RW, Hoving JL, Bouter LM, de Vet HC. Minimal clinically important change of the neck disability index and the numerical rating scale for patients with neck pain. Spine. 2007;32(26):3047–3051. doi:10.1097/BRS.0b013e31815cf75b
53. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983;16(1):87–101. doi:10.1016/0304-3959(83)90088-X
54. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–252. doi:10.1002/acr.20543
55. Vernon H, Mior S. The neck disability index: a study of reliability and validity. J Manip Physiol Ther. 1991;14(7):409–415.
56. Vernon H. The neck disability index: state-of-the-art, 1991-2008. J Manip Physiol Ther. 2008;31(7):491–502. doi:10.1016/j.jmpt.2008.08.006
57. Young BA, Walker MJ, Strunce JB, Boyles RE, Whitman JM, Childs JD. Responsiveness of the neck disability index in patients with mechanical neck disorders. Spine J. 2009;9(10):802–808. doi:10.1016/j.spinee.2009.06.002
58. Hoving JL, O’Leary EF, Niere KR, Green S, Buchbinder R. Validity of the neck disability index, Northwick Park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders. Pain. 2003;102(3):273–281. doi:10.1016/S0304-3959(02)00406-2
59. Schellingerhout JM, Verhagen AP, Heymans MW, Koes BW, de Vet HC, Terwee CB. Measurement properties of disease-specific questionnaires in patients with neck pain: a systematic review. Qual Life Res. 2012;21(4):659–670. doi:10.1007/s11136-011-9965-9
60. Koke AJA, Heuts PHTG, Vlaeyen JWS. Neck Disability Index. Pain Knowledge Center, University Medical Center Maastricht, Measurement Instruments Chronic Pain. Maastricht: Pijn Kennis Centrum, Academisch Ziekenhuis Maastricht; 1996.
61. Jorritsma W, de Vries GE, Dijkstra PU, Geertzen JH, Reneman MF. Neck pain and disability scale and neck disability index: validity of dutch language versions. Eur Spine J. 2012;21(1):93–100. doi:10.1007/s00586-011-1920-5
62. Jorritsma W, de Vries GE, Geertzen JH, Dijkstra PU, Reneman MF. Neck pain and disability scale and the neck disability index: reproducibility of the Dutch language versions. Eur Spine J. 2010;19:1695–1701. doi:10.1007/s00586-010-1406-x
63. Kamper SJ, Ostelo RW, Knol DL, Maher CG, de Vet HC, Hancock MJ. Global perceived effect scales provided reliable assessments of health transition in people with musculoskeletal disorders, but ratings are strongly influenced by current status. J Clin Epidemiol. 2010;63(7):760–766. doi:10.1016/j.jclinepi.2009.09.009
64. Portney LG, Watkins. Foundations of Clinical Research. Applications to Practice. Appleton & Lange; Norwalk: Connecticut; 1993:651–657.
65. Scholten-Peeters GG, Neeleman-van der Steen CW, van der Windt DA, Hendriks EJ, Verhagen AP, Oostendorp RA. Education by general practitioners or education and exercises by physiotherapists for patients with whiplash-associated disorders? A randomized clinical trial. Spine. 2006;31(7):723–731. doi:10.1097/01.brs.0000206381.15224.0f
66. Hoving JL, Koes BW, de Vet HC, et al. Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain. A randomized, controlled trial. Ann Intern Med. 2002;136(10):713–722. doi:10.7326/0003-4819-136-10-200205210-00006
67. Pool JJ, Ostelo RW, Knol DL, Vlaeyen JW, Bouter LM, de Vet HC. Is a behavioral graded activity program more effective than manual therapy in patients with subacute neck pain? Results of a randomized clinical trial. Spine. 2010;35(10):1017–1024. doi:10.1097/BRS.0b013e3181c212ee
68. Peters R, Mutsaers B, Verhagen AP, Koes BW, Pool-Goudzwaard AL. Prospective cohort study of patients with neck pain in a manual therapy setting: design and baseline measures. J Manip Physiol Ther. 2019;42(7):471–479. doi:10.1016/j.jmpt.2019.07.001
69. Bunketorp L, Stener-Victorin E, Carlsson J. Neck pain and disability following motor vehicle accidents – a cohort study. Eur Spine J. 2005;14(1):84–89. doi:10.1007/s00586-004-0766-5
70. Meisingset I, Stensdotter AK, Woodhouse A, Vasseljen O. Predictors for global perceived effect after physiotherapy in patients with neck pain: an observational study. Physiotherapy. 2018;104(4):400–407. doi:10.1016/j.physio.2017.01.007
71. Van Hassel DTP, Kenens RJ. Cijfers uit de registratie van fysiotherapeuten. Peiling Januari; 2012. Availabie from: https://www.nivel.nl/nl/publicatie/cijfers-uit-de-registratie-van-fysiotherapeuten-de-eerste-lijn-peiling-1-januari-2012.
72. Kelly AM. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg Med J. 2001;18(3):205–207. doi:10.1136/emj.18.3.205
73. Sterling M, Jull G, Vicenzino B, Kenardy J, Darnell R. Physical and psychological factors predict outcome following whiplash injury. Pain. 2005;114(1–2):141–148. doi:10.1016/j.pain.2004.12.005
74. Scott D, Jull G, Sterling M. Widespread sensory hypersensitivity is a feature of chronic whiplash-associated disorder but not chronic idiopathic neck pain. Clin J Pain. 2005;21(2):175–181. doi:10.1097/00002508-200503000-00009
75. Sterling M, Jull G, Vicenzino B, Kenardy J. Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery. Pain. 2003;104(3):509–517. doi:10.1016/S0304-3959(03)00078-2
76. De Pauw R, Kregel J, De Blaiser C, et al. Identifying prognostic factors predicting outcome in patients with chronic neck pain after multimodal treatment: a retrospective study. Man Ther. 2015;20(4):592–597. doi:10.1016/j.math.2015.02.001
77. Hendriks EJ, Scholten-Peeters GG, van der Windt DA, et al. Prognostic factors for poor recovery in acute whiplash patients. Pain. 2005;114(3):408–416. doi:10.1016/j.pain.2005.01.006
78. Dufton JA, Bruni SG, Kopec JA, Cassidy JD, Quon J. Delayed recovery in patients with whiplash-associated disorders. Injury. 2012;43(7):1141–1147. doi:10.1016/j.injury.2012.03.006
79. Synnott A, O’Keeffe M, Bunzli S, Dankaerts W, O’Sullivan P, O’Sullivan K. Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: a systematic review. J Physiother. 2015;61(2):68–76. doi:10.1016/j.jphys.2015.02.016
80. Zadro J, O’Keeffe M, Maher C. Do physical therapists follow evidence-based guidelines when managing musculoskeletal conditions? Systematic review. BMJ Open. 2019;9(10):e032329. doi:10.1136/bmjopen-2019-032329
81. Sterling M, Kenardy J, Jull G, Vicenzino B. The development of psychological changes following whiplash injury. Pain. 2003;106(3):481–489. doi:10.1016/j.pain.2003.09.013
82. Nijs J, Roussel N, van Wilgen PC, Köke A, Smeets R. Thinking beyond muscles and joints: therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man Ther. 2013;18(2):96–102. doi:10.1016/j.math.2012.11.001
83. Oerlemans HM, Goris RJ, Oostendorp RA. Impairment level sum score in reflex sympathetic dystrophy of one upper extremity. Arch Phys Med Rehabil. 1998;79(8):979–990. doi:10.1016/S0003-9993(98)90098-3
84. Kasch H, Kongsted A, Qerama E, et al. A new stratified risk assessment tool for whiplash injuries developed from a prospective observational study. BMJ Open. 2013;3:e002050. doi:10.1136/bmjopen-2012-002050
85. Coons SJ, Gwaltney CJ, Hays RD, et al. ISPOR ePRO Task Force. Recommendations on evidence needed to support measurement equivalence between electronic and paper-based patient-reported outcome (PRO) measures: ISPOR ePRO Good Research Practices Task Force report. Value Health. 2009;12(4):419–429. doi:10.1111/j.1524-4733.2008.00470.x
86. Benchimol E, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
87. Langan SM, Cook C, Benchimol EI. lmproving the reporting of studies using routinely collected health data in physical therapy. J Orthop Sports Phys Ther. 2016;46(3):126–127. doi:10.2519/jospt.2016.0103
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.