")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Clinical Benefits of Neoadjuvant Radiotherapy on the Postoperative Recurrence of Centrally Located Hepatocellular Carcinoma: A Real-World Evidence Based on Phase II Clinical Trial
Authors Tao C, Wu F, Wang H, Wang L, Liu Y, Wu A, Zheng L, Wang Y, Chen B, Rong W , Wu J
Received 31 December 2022
Accepted for publication 8 May 2023
Published 16 May 2023 Volume 2023:10 Pages 753—764
DOI https://doi.org/10.2147/JHC.S403287
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Changcheng Tao,1,* Fan Wu,1,* Hongwei Wang,1,* Liming Wang,1 Yue Liu,1 Anke Wu,1 Linlin Zheng,1 Yaru Wang,1 Bo Chen,2 Weiqi Rong,1 Jianxiong Wu1
1Department of Hepatobiliary Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China; 2Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianxiong Wu; Weiqi Rong, Email [email protected]; [email protected]
Objective: Although surgical resection is one of the most effective way to treat liver cancer, its efficacy and safety in treatment of centrally located hepatocellular carcinoma (HCC) remains elusive. Therefore, it is very important to find a comprehensive treatment mode, such as radical resection combined with neoadjuvant radiotherapy (neoRT).
Methods: The centrally located HCC patients who underwent radical resection from July 2015 to April 2021 were enrolled. According to whether the neoRT was implemented or not, these patients were allocated into neoadjuvant radiotherapy combined with liver resection (neoRT+LR) and liver resection alone (LR) group. The research method used propensity-score analysis and Cox proportional-hazards regression models. We generated an E-value to assess the sensitivity to unmeasured confounding. This study is a real-world, retrospective study based on phase II clinical trial.
Results: A total of 168 patients were enrolled, including 38 patients treating with neoRT+LR and 130 patients with LR. The 1-, 3-, 5-year disease free survival (DFS) rates were 74%, 55% and 39% in the neoRT+LR group, and 44%, 28%, and 24% in the LR group, respectively. Neoadjuvant radiotherapy was an independent prognostic factor for postoperative recurrence ([HR]0.42, 95% CI [0.25, 0.69]). There was significant association between neoRT+LR and longer disease-free survival (Match, [HR] 0.43, 95% CI [0.24, 0.76]; GenMatch, [HR] 0.32, 95% CI [0.23, 0.43]; Adjusted for propensity score, [HR] 0.41, 95% CI [0.23, 0.73]; Inverse probability weighting, [HR] 0.38, 95% CI [0.22, 0.65], respectively). DFS before and after matching analysis was statistically different in two groups (p-value=0.005, p-value=0.0024, respectively). Neoadjuvant radiotherapy can significantly reduce the postoperative early recurrence (p-value < 0.05). E-value analysis suggested robustness to unmeasured confounding.
Conclusion: Liver resection combined with neoadjuvant radiotherapy was effective and safe for treatment of centrally located HCC patients, which improved the prognosis of patients and reduced the incidence of early recurrence.
Keywords: centrally located hepatocellular carcinoma, neoadjuvant radiotherapy, radical resection, recurrence
Introduction
Malignant tumor of liver is one of the most common tumor in the world. An estimated 19.3 million new cancer cases and 10 million cancer-related deaths occurred globally in 2020. Liver cancer represents 4.7% of all new malignancies and 8.3% of cancer deaths in the world.1 Primary liver cancer (PLC) is a lethal disease associated with high morbidity and poor prognosis and always a prerequisite question to be solved in clinical applications.2 Hepatocellular carcinoma (HCC) accounts for approximately 90% of all cases of PLC.3 The treatment strategies for liver cancer include surgical resection, liver transplantation, radiofrequency ablation (RFA) and transcatheter arterial chemoembolization (TACE), of which, surgical resection is the most important and effective treatment.4 However, 70% patients develop a tumor relapse in 5 years after surgical resection.5
Centrally located HCC is a tumor located at the bifurcation of the portal vein, the confluence of the three main hepatic veins, the inferior vena cava or within 1 centimeter (cm) of the posterior inferior vena cava trunk, usually located in Couinaud segments I, IV, V, VIII, or at the junction of the central segments.6,7 Due to its proximity to important blood vessels and bile ducts, the treatment of centrally located HCC still faces big challenges in the clinic, which is raising concerns over the world. It is reported that the recurrence rate of centrally located HCC after five years is more than 90%, and the five-year DFS is 15–30%.8 Narrower resection margins (<1 cm) and even null margins after surgery greatly increase the possibility of recurrence after surgery. Such narrow margins tend to result in microscopic residual lesions that can diffuse through intrahepatic vessels causing relapses.9 Thus, exploring effective comprehensive treatment mainly based on surgery for centrally located HCC patients to improve prognosis is crucial, and a research hotspot.
Until now, radical resection is still the most effective option for patients with resectable HCC patients and adjuvant therapies can be performed according to the results of postoperative pathological examinations. Previous research results have shown that radiofrequency ablation can achieve similar therapeutic effects as surgical resection for liver cancer with a diameter of ≤3 cm.10 Patients with centrally located HCC usually have larger tumors and surgical treatment is more recommended.11 In recent years, the emergence of radiotherapy technique, such as three-dimensional conformal radiotherapy (3D-CRT), intensity modulated radiation therapy (IMRT) and stereotactic body radiation therapy (SBRT), which make precise radiotherapy possible for patients. Radiotherapy (RT) is an important adjuvant treatment and has shown the safety and efficacy for centrally located HCC in multiple previous studies.12–14 RT is effective treatment modalities; however, this does not translate into an improvement in surgical safety. At the same time, the deviation of radiation target area may be caused by surgical resection. Thus, we investigate the role of neoadjuvant radiotherapy combined with liver resection address the above question.
To the best of our knowledge, this is the first cohort study investigating the potential clinical benefit of neoadjuvant radiotherapy combined with liver radical resection for centrally located HCC. Aiming to promote the comprehensive treatment mainly based on surgery for centrally located HCC.
Materials and Methods
Selection of Patients
The patients undergoing surgical resection for liver cancer from July 2015 to April 2021 in our hospital were collected. Patients were enrolled according the following inclusion and exclusion criteria. Inclusion criteria: (1) Age ≥18 years old; (2) No extrahepatic metastasis; (3) Centrally located liver cancer adhesion to or with a distance of <1 cm from hepatic vein, portal vein, the main hepatic brunch of the biliary system or retrohepatic inferior vena cava confirmed by the preoperative imaging; (4) Complete clinical and pathological data; (5) Child-Pugh class A; (6) Surgical operation is feasible. Exclusion criteria: (1) non-HCC by postoperative pathological examination; (2) Radiotherapy after the surgical resection. The enrollment of all subjects (such as inclusion/exclusion) was judged by the multidisciplinary team (MDT) consisting of surgeon, physician, radiologist, pathologist, etc. who were all involved in the decision how to treat the patient.
Treatment
Neoadjuvant Radiotherapy
Liver-directed neoadjuvant intensity modulated radiation therapy (IMRT) was performed in all neoRT+LR patients. Liver tissue biopsies were performed under ultrasound guidance to determine that the pathology is HCC. Gross tumor volume (GTV), including primary tumor (GTVp) and tumor thrombosis (GTVt), was delineated on planning CT scan, referring to pretreatment multiphasic contrast MRI through an image fusion approach. Clinical target volume (CTV) included the GTVp plus a 0.5 cm margin in all directions15 and GTVt without a margin. The planning target volume (PTV) included CTV plus a 0.5 cm margin in the anterior-posterior and left-right directions and a 1.0 cm margin in the cranial-caudal direction.16 The prescription dose to 95% of the PTV was 50–60 Gy in 25–30 fractions over 5–6 weeks, depending on the dose constraints of organs at risk (OARs).
Surgical Treatment
An MDT discussion was held before surgery for all patients. Surgery was usually performed 4–12 weeks after IMRT. The same surgical team completed all operations to standardize operative quality and safety. All surgeries were radical resections, with a negative surgical margin and no residual tumor. As the first step of surgery, exploratory laparotomy was performed on abdomen and pelvis to confirm the status of extrahepatic metastasis; when necessary, intraoperative ultrasound was utilized to examine the liver tumor. The surgical resection range was determined by overall considering the tumor and liver cirrhosis. During the surgery, individualized precise liver resection was implemented using the selective and dynamic region-specific vascular occlusion (SDRVO) technique.6 Surgical options for treating HCC were anatomic hepatectomy and non-anatomical hepatectomy. The liver resection without incision margin that was tumor being stripped off the surface of large blood vessels or biliary tract was performed for those patients having a tumor adhesion to important tracts by using a Cavitron Ultrasonic Surgical Aspirator (CUSA) to avoid cutting the major vessels.
Follow-Up
A relapse was defined as follows: fast-in and fast-out characteristics shown in imaging of hepatocellular nodular (≥2 cm) or HCC confirmed by cytological/histological results.17 Serum AFP level, liver function tests, kidney function tests, routine blood tests, abdominal enhanced magnetic resonance imaging (MRI) or enhanced computed tomography (CT) scans and chest X-ray were regularly examined. The patients were reviewed every 3 months in 2 years after surgical resection, every 4–6 months in 2–5 years, and every 6–12 months after 5 years. Patients should be reviewed when undergoing a physical discomfort during follow-up. All subjects were followed up until February 2022. The median follow-up was 50 months.
This study had been approved by the Ethics Committee of Cancer Hospital of Chinese Academy of Medical Science. All reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.18 This was a non-intervention cohort study, which did not interfere the diagnosis or treatment. The results of this study would be published in the form of statistical analysis data, which did not contain any information that can make patient identifiable. According to the Helsinki’s Declaration, relevant data of patients were fully kept secret informed consent was exempted by Ethics Committee from all subjects.
Treatment for Recurrence
The treatment strategy employed for recurrent HCC was based on the characteristics of tumor, liver function, general condition and choice of the patient, along with advice from the multidisciplinary team, such as reoperationhepatectomy, RFA, TACE, molecular targeted therapy and immunotherapy.
Definition and Analysis
Disease-free survival (DFS) was defined as the time from the date of surgery to the date of HCC recurrence. Besides neo-RT, the variables with a potential influence on survival were selected to generate propensity score.19 The complications during the hospitalization were evaluated as follows using the Clavien grading system: Grade I: the intervention with drug, surgery, endoscopy and radiotherapy was not required after surgery, but antiemetics, antipyretics, analgesics, diuretics, electrolyte and physiotherapy were allowed; Grade II: the drugs other than those for Grade I were required, including blood transfusion and parenteral nutrition; Grade III: the intervention with surgery, endoscopy and radiotherapy was required; Grade IV: the life-threatening complications, such as central nervous system (CNS) complications (cerebral hemorrhage and subarachnoid hemorrhage), and admission to ICU was required; Grade V: death during the hospitalization. The Grade I or II complications were considered as mild, and the Grade III, IV, V complications were considered as severe.
Statistical Methods
We conducted the analysis with the following steps: (1) Comparison of baseline data between the two groups using SMD; (2) A priori identification of confounders that could confound outcomes (these confounders on the basis of their associations with the outcomes of interest or a change in effect estimate of more than 10%); (3) Cox proportional-hazards regression models were used to estimate the association between exposure factors and prognosis, including Crude analysis and Multivariable analysis; (4) Associations between exposure factors and prognosis were estimated by Cox regression models with the use of four propensity-score methods, including Propensity-score Match (PSM), GenMatch (Diamond and Sekhon 2005 and Sekhon and Grieve 2011), Covariate adjustment using propensity score (CAPS) and Inverse Probability Weighting (IPTW); (5) DFS was estimated using the Kaplan–Meier method and the difference between two groups was assessed using the Log rank test; (6) Subgroup analysis to study the clinical benefits of neo-RT on early recurrence; (7) We explored the potential for unmeasured confounding between two groups by calculating E-values.20 The E-value quantifies the required magnitude of an unmeasured confounder that could negate the observed association between neo-RT and DFS.
To generate a matched population among two groups, we used a 1:1 matching algorithm. We used calipers of 0.02 on the propensity score scale and 1:1 sampling without replacement. All patient characteristics included in generating and distributing the propensity scores were compared before and after propensity score-matching using a standardized mean difference (SMD). A threshold less than 0.1 was considered acceptable.21 The statistical analyses were performed with the use of R software, version 4.2.0 (http://www.R-project.org) and IBM SPSS Statistics 23.
Results
Patients
A total of 208 patients were enrolled according to the inclusion criteria. Forty patients were then excluded according to the exclusion criteria. A total of 168 patients were eventually selected. According to whether the neoRT was implemented or not, these patients were allocated into neoadjuvant radiotherapy combined with liver resection (neoRT+LR, 38 patients) and liver resection alone (LR, 130 patients) group. The median follow-up was 50 months. The 1-, 3-, 5-year DFS rates were 74%, 55% and 39% for patients in the neoRT+LR group, and 44%, 28%, and 24% for patients in the LR group, respectively. The tumor size decreased significantly after neoRT (p-value <0.01). Flow chart for patient screening is shown in Figure 1. Baseline demographics and clinicopathological characteristics are shown in Table 1. According to standardized mean difference, there was significant difference (SMD > 0.1) between the two groups before matching.
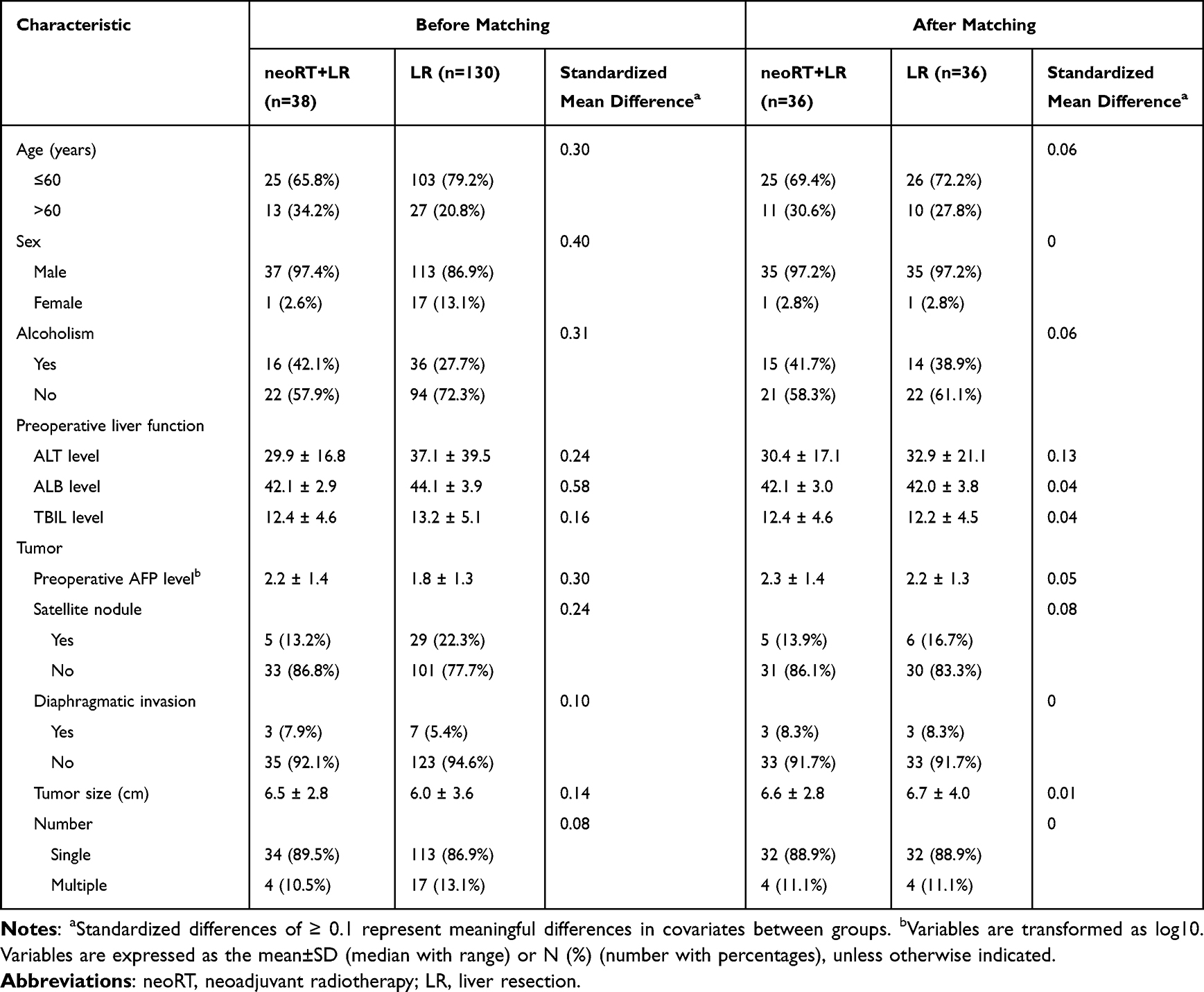 |
Table 1 Comparisons of Baseline Demographics and Clinicopathological Characteristics in Patients Undergoing neoRT + LR or LR Alone Before and After Propensity Score Matching Analysis |
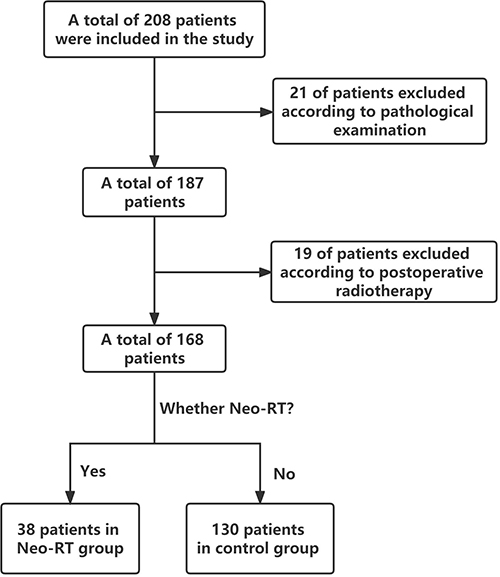 |
Figure 1 Flow chart for patient screening. |
Cox Regression
As shown by forest plot Figure 2 in crude analysis, there was significant association between neoRT+LR and better DFS (HR 0.52, 95% CI [0.32, 0.84], Table 2 and Figure 2). Subsequently, we screened out confounding factors according to the above methods, including Sex, ALB, Tumor number, Tumor size and Satellite nodule. The above confounding factors were included in the multiple regression equation for adjustment. Then, multivariate Cox analysis showed that neo-RT was the independent prognostic factors for centrally located HCC (HR 0.42, 95% CI [0.25, 0.69], Table 2 and Figure 2).
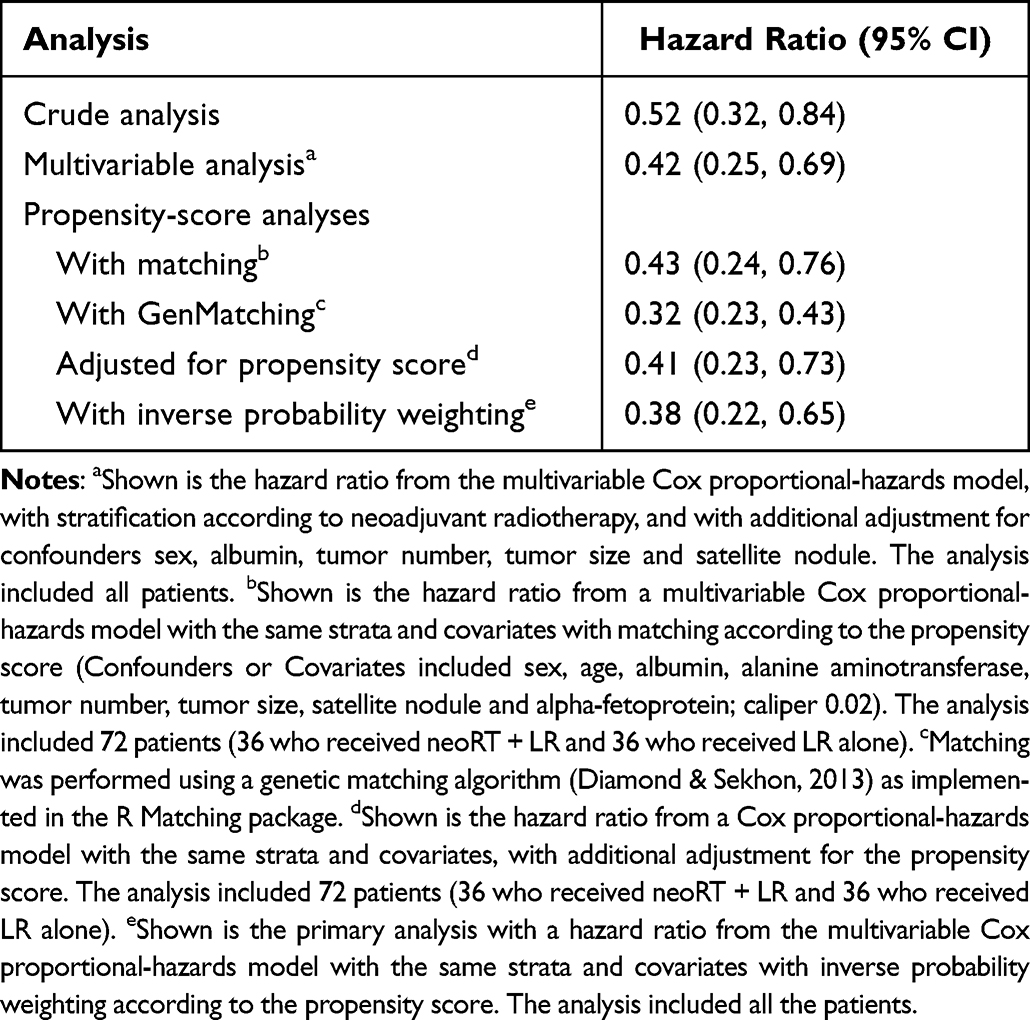 |
Table 2 Associations Between neoRT + LR and LR Alone Group in the Crude Analysis, Multivariable Analysis and Propensity-Score Analysis |
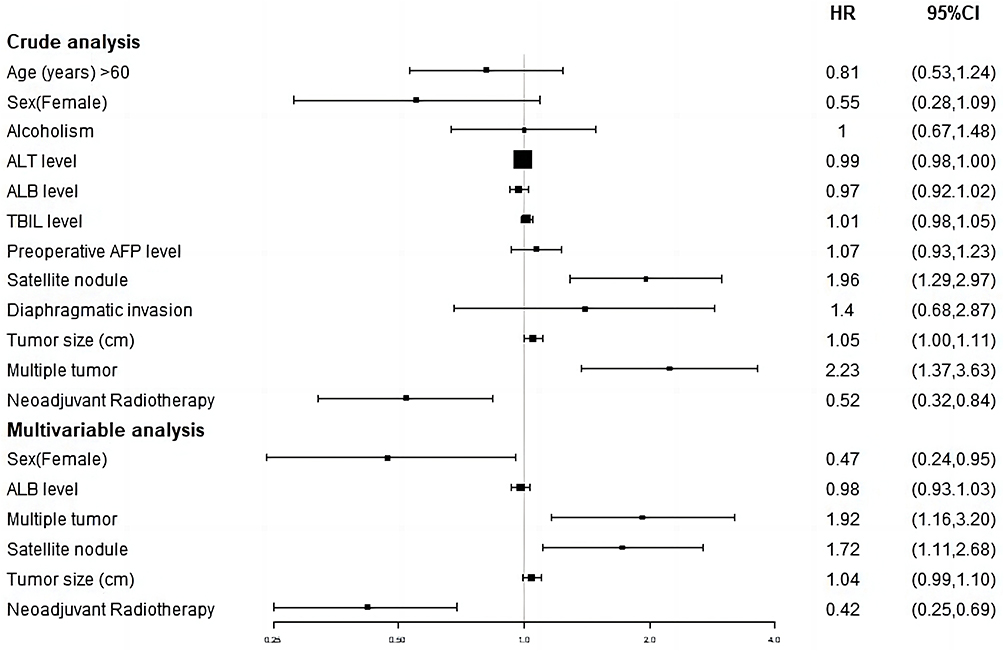 |
Figure 2 Cox proportional-hazards regression in DFS. Abbreviations: NeoRT, neoadjuvant radiotherapy; LR, liver resection; Cm, centimetre; AFP, Alpha-fetoprotein; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; TBIL, Total bilirubin. |
Propensity-Score Analyses
First, because of the imbalance of baseline information, we used propensity-score matching (PSM) analysis to reduce the difference between the two groups. Matching factors included baseline information and confounders, such as Age, Sex, AFP, ALB, ALT, Tumor size, Satellite nodule and Tumor number. A total of 36 patients were matched successfully. The baseline characteristics after matching analysis was not statistically different (SMD < 0.1) between two groups in Table 1. There was significant association between neoRT+LR and longer disease-free survival after PSM (HR 0.43, 95% CI [0.24, 0.76], Table 2). Then, we used GenMatching22 in order to match all patients as much as possible, which can be matched repeatedly, that is, one observation object can be matched to multiple cases or treatments, and the matching goal is to maximize the balance of covariates between matched groups. There was significant association between neoRT+LR and longer disease-free survival after GenMatch (HR 0.32, 95% CI [0.23, 0.43], Table 2). Subsequently, we used covariate adjustment using propensity score (CAPS)23 in order to control confounding. If PSM is used for matching, the matched pairs may have similar total scores. However, if a single variable is different, the confounding cannot be completely controlled. If the regression equation is used to adjust propensity-score based on PSM, the confounding can be further controlled. There was significant association between neoRT+LR and longer disease-free survival after CAPS (HR 0.41, 95% CI [0.23, 0.73], Table 2). Finally, we used inverse probability weighting (IPTW). In the inverse-probability weighted analysis, the predicted probabilities from the propensity-score model were used to calculate the stabilized inverse-probability weight.24 There was significant association between neoRT+LR and longer disease-free survival after IPTW (HR 0.38, 95% CI [0.22, 0.65], Table 2). The above statistical methods based on real-world data show that statistically better DFS was observed in the combination group compared to the control group.
Survival Analysis
As shown by Kaplan–Meier curves (Figure 3), DFS before matching analysis was significantly different between the two groups (p-value=0.005). Subsequently, 36 patients were matched by 1:1 using matching analysis. The baseline data after matching analysis was not statistically different. Kaplan–Meier curve of DFS after matching analysis is shown in Figure 4. DFS after matching analysis was improved and significantly different in neoRT+LR group compared with that in LR group (p-value=0.0024).
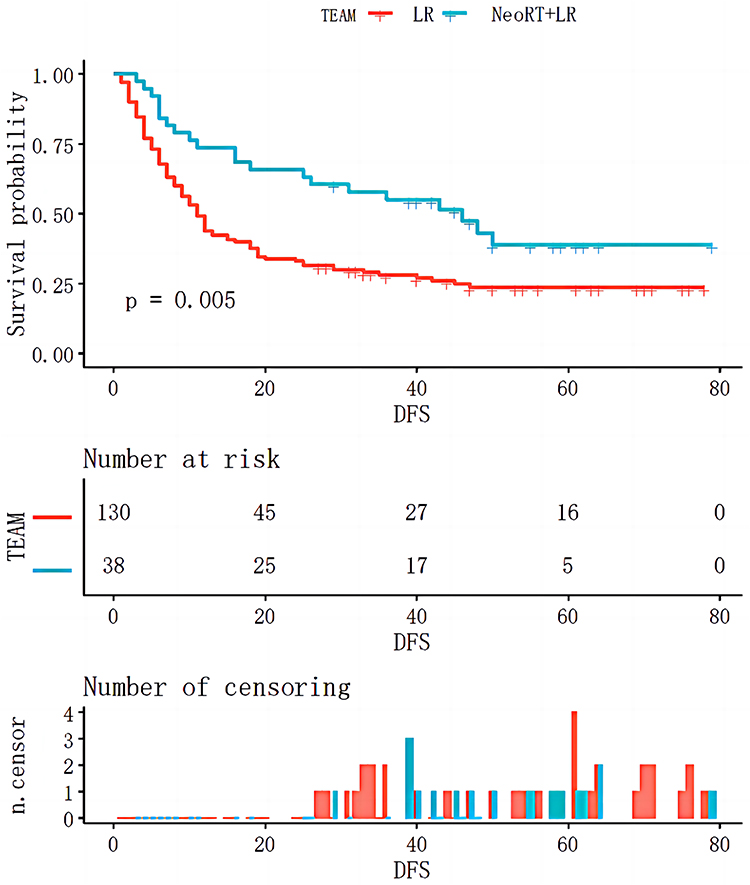 |
Figure 3 Kaplan–Meier curve of DFS before matching in neoRT+LR and LR groups. Abbreviations: NeoRT, neoadjuvant Radiotherapy; LR, liver resection. |
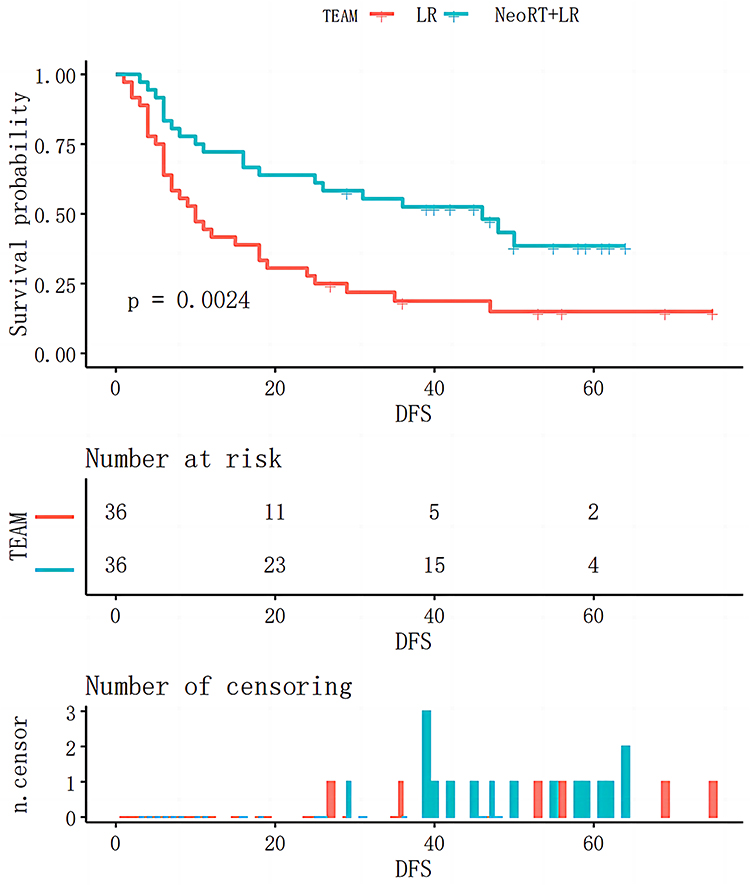 |
Figure 4 Kaplan–Meier curve of DFS after matching in neoRT+LR and LR groups. Abbreviations: NeoRT, neoadjuvant Radiotherapy; LR, liver resection. |
Recurrence Pattern and Subgroup Analysis
A total of 72 patients were included after matching analysis in this study, of which 50 patients developed recurrence, including 20 patients in the neoRT+LR group and 30 patients in the LR group. Among the recurrent patients, 5 received liver surgical treatment, 18 received TACE, 15 received molecular targeted therapy, 3 received RFA, 7 received immunotherapy, and 2 did not receive treatment. The incidence of intrahepatic recurrence and extrahepatic metastasis was 16 and 4 in neoRT group, 26 and 4 in LR group, respectively. As everyone knows, the high recurrence rate after hepatectomy is the most important reason to affect its prognosis. According to the recurrence time, the recurrence can be divided into early recurrence and late recurrence.25,26 A large number of studies have shown that the prognosis of patients with early recurrence is worse than that of patients with late recurrence.27–29 At present, most scholars believe that it is feasible to set 12 months and 24 months as the time point of early recurrence.25,30–32 Therefore, we conducted subgroup analysis to explore the effect of neoRT on early recurrence. The incidence of early recurrence and late recurrence was 10 and 26 in neoRT group, 21 and 15 in LR group according to 12 months, and 13 and 23 in neoRT group, 26 and 10 in LR group according to 24 months, respectively (Table 3). Our study had shown that neoRT could reduce the incidence of early recurrence no matter whether the time point of early recurrence was 12 months or 24 months (p-value=0.009, p-value=0.002, respectively. Table 3).
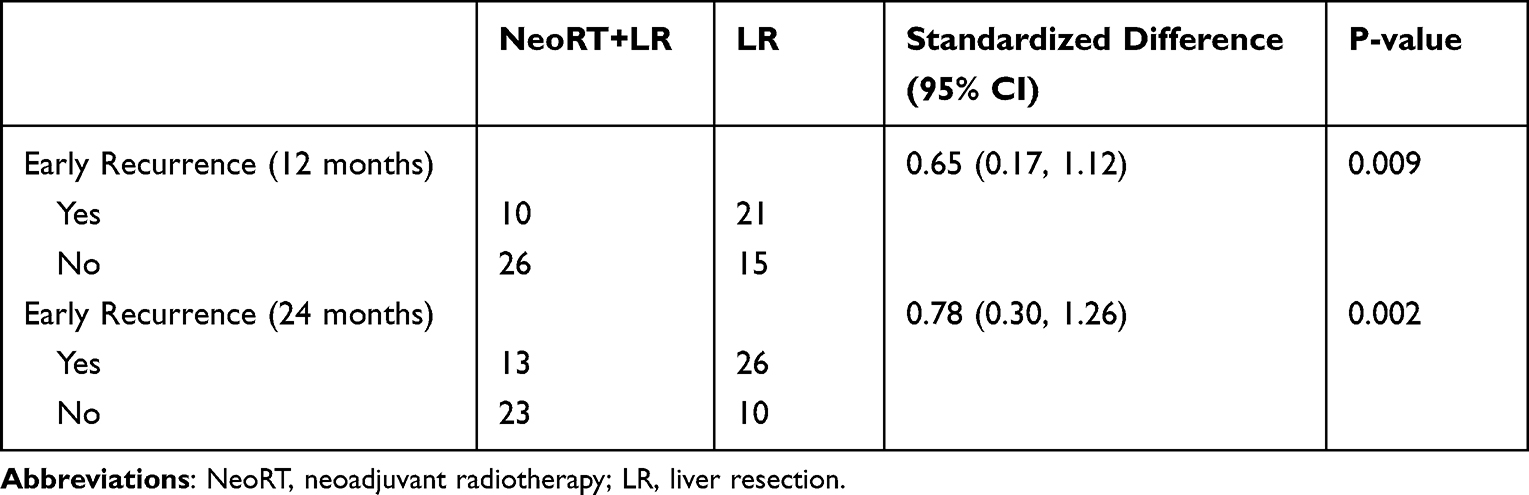 |
Table 3 Comparisons of Early Recurrence in Patients Undergoing LR+neoRT or LR |
Sensitivity Analysis
We generated an E-value to assess the sensitivity to unmeasured confounding. The primary findings were robust, unless an unmeasured confounder existed with a higher relative risk of HR, with an HR higher than 2.97. E-value analysis suggested robustness to unmeasured confounding.
Complications
In terms of safety, all 36 patients underwent surgery successfully in both groups. Intraoperative bleeding and operation duration were not significantly different between the two groups (p-value=0.139, p-value=0.284, respectively). The patients in both groups received successful surgical treatment without serious complications.
Discussion
According to traditional definition, centrally located HCC refers to the tumor sited in Couinaud segments IV, V and VIII of the liver.33 We propose a revised definition that centrally located HCC refers to liver tumor adhesion to or with a distance of <1 cm from hepatic vein, portal vein, the main hepatic brunch of the biliary system or retrohepatic inferior vena cava confirmed by the preoperative imaging, intraoperative macroscopic examination and postoperative pathological examination, that is usually located in Couinaud segments I, IV, V, VIII, or at the junction of the central segments.7,34 How to safely remove centrally located HCC and improve the postoperative survival rate is one of the important challenges in the field of liver cancer treatment. Our team has carried out long-term research on the comprehensive treatment of centrally located liver cancer based on surgery.12,14,34,35
This study is the first study investigating the potential clinical benefit of neoadjuvant radiotherapy combined with liver resection for centrally located HCC. The results suggest that the combined treatment has a significant effect and significantly improves the prognosis of patients.
Radiotherapy, as an important treatment option, has been extensively applied for clinical treatment of patients with malignant tumors. In recent years, the radiotherapy has become one of the treatment strategies for HCC due to the improvement of precision radiotherapy that high dose radiation ray can directly reach the target area without radioactive injuries in normal tissues around target area and other tissues/organs around the liver. As demonstrated by the recent relevant studies, the prognosis of patients could be improved after receiving the neoRT. Wu et al7 conducted a phase II clinical trial and confirmed that neoadjuvant IMRT plus surgery is effective and well tolerated in patients with centrally located HCC. Lin et al36 report that preoperative radiotherapy could improve survival outcome of HCC patients, compared with postoperative radiotherapy in a retrospective study by using SEER database. Wei et al37 indicate that the survival of HCC patients with portal vein tumor thrombus (PVTT) after receiving preoperative radiotherapy combined with surgical resection is longer than those patients after receiving only surgical resection. Our study has the following advantages over other studies, first of all, all enrolled patients were treated by the same group of doctors in the center, so the treatment level and management ensure high quality. Secondly, this study applies the statistical method of real world to minimize the selection bias and make the results more authentic and reliable. Thirdly, our study has a long follow-up time, which can better reflect the long-term prognosis and has better guiding significance.
In terms of prognosis, neoRT for the treatment of centrally located HCC is feasible and has the following potential advantages. On the one hand, neoRT can significantly reduce the size of tumors, it can keep the tumor away from important blood vessels and reduce the difficulty of operation; on the other hand, it can make tumor tissue necrosis and replace it with normal liver tissue. This has significant advantages for the improvement of surgical safety and prognosis.
According to guideline consensus, a conservative minimum surrogate threshold effect of HR ≤ 0.6 for DFS is highly predictive of a significant improvement in overall survival (OS).38 All our results meet the above criteria (Table 2), so neo-RT is of great significance to improve the overall survival time of patients with liver cancer after operation.
The improvement in survival may be explained from the following aspects. Firstly, neoRT decreased tumor burden and size, making some of the lesions resectable with wide margins (≥1 cm). It has been reported that wide margin resection produced better OS than narrow margin resection (<1 cm).39,40 Secondly, neoRT significantly reduced the recurrence rate, which is a surprising result. It may be that neoRT destroyed the minimal residual disease (MRD) that led to postoperative recurrence.41,42 The reduction of recurrence rate ensures the improvement of survival rate. There are some limitations in this study. This study is a cohort study. Our conclusions are needed to be confirmed in a large randomized controlled study.
Conclusion
Liver resection combined with neoadjuvant radiotherapy was effective and safe for treatment of centrally located HCC patients, which improved the prognosis of patients and reduce the incidence of early recurrence.
Abbreviations
HCC, Hepatocellular carcinoma; NeoRT, neoadjuvant radiotherapy; LR, liver resection; SMD, Standardized mean difference; PLC, Primary liver cancer; RA, Radiofrequency ablation; TACE, Transcatheter arterial chemoembolization; RT, Radiotherapy; SDRVO, Selective and dynamic region-specific vascular occlusion; OS, Overall survival; DFS, Disease free survival; PSM, Propensity-score Match; CAPS, Covariate adjustment using propensity score; IPTW, Inverse Probability Weighting; MDT, Multidisciplinary team; Cm, centimetre; AFP, Alpha-fetoprotein; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; TBIL, Total bilirubin.
Data Sharing Statement
All data related to this study are included in this paper. Details are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study had been approved by the Ethics Committee of Cancer Hospital of Chinese Academy of Medical Science. All reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. According to the Helsinki’s Declaration, relevant data of patients were fully kept secret informed consent was exempted by Ethics Committee from all subjects.
Author Contributions
WJ, WF and RW conceived and designed the study. TC, WF and WH gathered data, analyzed the data, wrote the first manuscript draft, and provided the literature search. WJ, WF, LY, WA, ZL, WY, WL and CB verified the data and revised the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Beijing Hope Run Special Fund of Cancer Foundation of China (LC2020L05).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Zhou J, Sun HC, Wang Z, et al. Guidelines for diagnosis and treatment of primary liver cancer in China (2017 Edition). Liver Cancer. 2018;7(3):235–260. doi:10.1159/000488035
3. Nagtegaal ID, Odze RD, Klimstra D, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020;76(2):182–188. doi:10.1111/his.13975
4. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
5. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
6. Yu W, Rong W, Wang L, Wu F, Xu Q, Wu J. R1 hepatectomy with exposure of tumor surface for centrally located hepatocellular carcinoma. World J Surg. 2014;38(7):1777–1785. doi:10.1007/s00268-013-2429-3
7. Wu F, Chen B, Dong D, et al. Phase 2 evaluation of neoadjuvant intensity-modulated radiotherapy in centrally located hepatocellular carcinoma: a nonrandomized controlled trial. JAMA Surg. 2022;157:1089. doi:10.1001/jamasurg.2022.4702
8. Cheng CH, Yu MC, Wu TH, et al. Surgical resection of centrally located large hepatocellular carcinoma. Chang Gung Med J. 2012;35(2):178–191. doi:10.4103/2319-4170.106153
9. Shi M, Guo RP, Lin XJ, et al. Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: a prospective randomized trial. Ann Surg. 2007;245(1):36–43. doi:10.1097/01.sla.0000231758.07868.71
10. Chen MS, Li JQ, Zheng Y, et al. A prospective randomized trial comparing percutaneous local ablative therapy and partial hepatectomy for small hepatocellular carcinoma. Ann Surg. 2006;243(3):321–328. doi:10.1097/01.sla.0000201480.65519.b8
11. Xu XL, Liu XD, Liang M, Luo BM. Radiofrequency ablation versus hepatic resection for small hepatocellular carcinoma: systematic review of randomized controlled trials with meta-analysis and trial sequential analysis. Radiology. 2018;287(2):461–472. doi:10.1148/radiol.2017162756
12. Rong W, Yu W, Wang L, et al. Adjuvant radiotherapy in central hepatocellular carcinoma after narrow-margin hepatectomy: a 10-year real-world evidence. Chin J Cancer Res. 2020;32(5):645–653. doi:10.21147/j.issn.1000-9604.2020.05.09
13. Wang WH, Wang Z, Wu JX, et al. Survival benefit with IMRT following narrow-margin hepatectomy in patients with hepatocellular carcinoma close to major vessels. Liver Int. 2015;35(12):2603–2610. doi:10.1111/liv.12857
14. Chen B, Wu JX, Cheng SH, et al. Phase 2 study of adjuvant radiotherapy following narrow-margin hepatectomy in patients with HCC. Hepatology. 2021;74(5):2595–2604. doi:10.1002/hep.31993
15. Wang W, Feng X, Zhang T, et al. Prospective evaluation of microscopic extension using whole-mount preparation in patients with hepatocellular carcinoma: definition of clinical target volume for radiotherapy. Radiat Oncol. 2010;5:73. doi:10.1186/1748-717X-5-73
16. Zhao YT, Liu ZK, Wu QW, et al. Observation of different tumor motion magnitude within liver and estimate of internal motion margins in postoperative patients with hepatocellular carcinoma. Cancer Manag Res. 2017;9:839–848. doi:10.2147/CMAR.S147185
17. General Office of National Health Commission. 原发性肝癌诊疗指南(2022年版) [Standardization for diagnosis and treatment of hepatocellular carcinoma (2022 edition)]. Zhonghua Gan Zang Bing Za Zhi. 2022;30(4):367–388. Chinese. doi:10.3760/cma.j.cn501113-20220413-00193
18. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
19. Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Variable selection for propensity score models. Am J Epidemiol. 2006;163(12):1149–1156. doi:10.1093/aje/kwj149
20. Haneuse S, VanderWeele TJ, Arterburn D. Using the E-value to assess the potential effect of unmeasured confounding in observational studies. JAMA. 2019;321(6):602–603. doi:10.1001/jama.2018.21554
21. Reitz KM, Marroquin OC, Zenati MS, et al. Association between preoperative metformin exposure and postoperative outcomes in adults with type 2 diabetes. JAMA Surg. 2020;155(6):e200416. doi:10.1001/jamasurg.2020.0416
22. Radice R, Ramsahai R, Grieve R, Kreif N, Sadique Z, Sekhon JS. Evaluating treatment effectiveness in patient subgroups: a comparison of propensity score methods with an automated matching approach. Int J Biostat. 2012;8(1):25. doi:10.1515/1557-4679.1382
23. Kurth T, Walker AM, Glynn RJ, et al. Results of multivariable logistic regression, propensity matching, propensity adjustment, and propensity-based weighting under conditions of nonuniform effect. Am J Epidemiol. 2006;163(3):262–270. doi:10.1093/aje/kwj047
24. Robins JM, Hernán MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000;11(5):550–560. doi:10.1097/00001648-200009000-00011
25. Jung SM, Kim JM, Choi GS, et al. Characteristics of early recurrence after curative liver resection for solitary hepatocellular carcinoma. World J Gastrointest Surg. 2019;23(2):304–311. doi:10.1007/s11605-018-3927-2
26. Portolani N, Coniglio A, Ghidoni S, et al. Early and late recurrence after liver resection for hepatocellular carcinoma: prognostic and therapeutic implications. Ann Surg. 2006;243(2):229–235. doi:10.1097/01.sla.0000197706.21803.a1
27. Yamamoto Y, Ikoma H, Morimura R, et al. Optimal duration of the early and late recurrence of hepatocellular carcinoma after hepatectomy. World J Gastroenterol. 2015;21(4):1207–1215. doi:10.3748/wjg.v21.i4.1207
28. Chan A, Zhong J, Berhane S, et al. Development of pre and post-operative models to predict early recurrence of hepatocellular carcinoma after surgical resection. J Hepatol. 2018;12(6):1284–1293. doi:10.1016/j.jhep.2018.08.027
29. Xing H, Zhang WG, Cescon M, et al. Defining and predicting early recurrence after liver resection of hepatocellular carcinoma: a multi-institutional study. HPB. 2019;22(5):677–689. doi:10.1016/j.hpb.2019.09.006
30. Xu XF, Xing H, Han J, et al. Risk factors, patterns, and outcomes of late recurrence after liver resection for hepatocellular carcinoma: a multicenter study from China. JAMA Surg. 2019;154(3):209–217. doi:10.1001/jamasurg.2018.4334
31. Poon RT, Fan ST, Ng IO, Lo CM, Liu CL, Wong J. Different risk factors and prognosis for early and late intrahepatic recurrence after resection of hepatocellular carcinoma. Cancer. 2000;89(3):500–507. doi:10.1002/1097-0142(20000801)89:3<500::AID-CNCR4>3.0.CO;2-O
32. Singal AG, Rich NE, Mehta N, et al. Direct-acting antiviral therapy not associated with recurrence of hepatocellular carcinoma in a multicenter north American cohort study. Gastroenterology. 2019;156(6):1683–1692.e1. doi:10.1053/j.gastro.2019.01.027
33. Wu CC, Ho WL, Chen JT, et al. Mesohepatectomy for centrally located hepatocellular carcinoma: an appraisal of a rare procedure. J Am Coll Surg. 1999;188(5):508–515. doi:10.1016/S1072-7515(99)00026-5
34. Yu W, Wang W, Rong W, et al. Adjuvant radiotherapy in centrally located hepatocellular carcinomas after hepatectomy with narrow margin (<1 cm): a prospective randomized study. J Am Coll Surg. 2014;218(3):381–392. doi:10.1016/j.jamcollsurg.2013.11.030
35. Wu YL, Zhai Y, Li M, et al. Long-term outcome of centrally located hepatocellular carcinomas treated by radical resection combined with intraoperative electron radiotherapy (IOERT). Front Oncol. 2022;12:773301. doi:10.3389/fonc.2022.773301
36. Lin H, Li X, Liu Y, Hu Y. Neoadjuvant radiotherapy provided survival benefit compared to adjuvant radiotherapy for hepatocellular carcinoma. ANZ J Surg. 2018;88(10):E718–E724. doi:10.1111/ans.14387
37. Wei X, Jiang Y, Zhang X, et al. Neoadjuvant three-dimensional conformal radiotherapy for resectable hepatocellular carcinoma with portal vein tumor thrombus: a randomized, open-label, multicenter controlled study. J Clin Oncol. 2019;37(24):2141–2151. doi:10.1200/JCO.18.02184
38. Llovet JM, Lencioni R. mRECIST for HCC: performance and novel refinements. J Hepatol. 2020;72(2):288–306. doi:10.1016/j.jhep.2019.09.026
39. Aoki T, Kubota K, Hasegawa K, et al. Significance of the surgical hepatic resection margin in patients with a single hepatocellular carcinoma. Br J Surg. 2020;107(1):113–120. doi:10.1002/bjs.11329
40. Zhong FP, Zhang YJ, Liu Y, Zou SB. Prognostic impact of surgical margin in patients with hepatocellular carcinoma: a meta-analysis. Medicine. 2017;96(37):e8043. doi:10.1097/MD.0000000000008043
41. Luskin MR, Murakami MA, Manalis SR, Weinstock DM. Targeting minimal residual disease: a path to cure. Nat Rev Cancer. 2018;18(4):255–263. doi:10.1038/nrc.2017.125
42. Garcia-Murillas I, Schiavon G, Weigelt B, et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci Transl Med. 2015;7(302):302ra133. doi:10.1126/scitranslmed.aab0021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.