")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 9 » Issue 1
Clinical benefit of fixed-dose dual bronchodilation with glycopyrronium and indacaterol once daily in patients with chronic obstructive pulmonary disease: a systematic review
Authors Ulrik CS
Received 9 January 2014
Accepted for publication 20 February 2014
Published 1 April 2014 Volume 2014:9(1) Pages 331—338
DOI https://doi.org/10.2147/COPD.S60362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Charlotte Suppli Ulrik
Department of Respiratory Medicine, Hvidovre Hospital and University of Copenhagen, Hvidovre, Denmark
Background and aim: Long-acting bronchodilators are the preferred option for maintenance therapy of patients with chronic obstructive pulmonary disease (COPD). The aim of this review is to provide an overview of the clinical studies evaluating the clinical efficacy of the once-daily fixed-dose dual bronchodilator combination of indacaterol and glycopyrronium bromide in patients suffering from COPD.
Methods: This study comprised a systematic review of randomized controlled trials identified through systematic searches of different databases of published trials.
Results: Nine trials (6,166 participants) were included. Fixed-dose once-daily indacaterol/glycopyrronium seems to be safe and well tolerated in patients with COPD. Compared with single therapy with other long-acting bronchodilators (indacaterol, glycopyrronium, and tiotropium) and fixed-combination long-acting β2-agonist/inhaled corticosteroid (salmeterol/fluticasone twice daily), once-daily fixed-dose indacaterol/glycopyrronium has clinically important effects on symptoms, including dyspnea score, health status, level of lung function, and rate of moderate or severe exacerbations in patients with moderate-to-very severe COPD (Global initiative for chronic Obstructive Lung Disease [GOLD] spirometric criteria). Furthermore, a very recent study has shown that fixed-dose indacaterol/glycopyrronium improves exercise endurance time compared with placebo, although no significant difference was observed between fixed-dose indacaterol/glycopyrronium and tiotropium.
Conclusion: Fixed-dose indacaterol/glycopyrronium has clinically relevant effects on important COPD outcome measures and is, in general, superior to therapy with a single long-acting bronchodilator (with or without inhaled corticosteroid) indicating long-acting dual bronchodilation as a potential important maintenance therapeutic option for patients with symptomatic COPD, possibly also for the treatment of naïve patients.
Keywords: COPD, long-acting bronchodilators, glycopyrronium, indacaterol
Introduction
The Global initiative for chronic Obstructive Lung Disease (GOLD) strategy document recommends that the pharmacological therapy of chronic obstructive pulmonary disease (COPD) should be predicated according to the individual patient’s level of symptoms, airflow limitation, and history of exacerbations.1 The preferred option for maintenance therapy of COPD is long-acting bronchodilators,1,2 either alone or in combination with an inhaled corticosteroid (ICS).
The GOLD strategy document1 recommends treatment with at least one long-acting bronchodilator for patients with moderate-to-very severe COPD. The strategy of combining short-acting bronchodilators with different mechanisms of action, ie, ipratropium bromide and salbutamol, has previously been shown to provide better symptomatic relief and to be cost-saving in patients with COPD.3,4 In line with this, more recent studies have shown that also combining long-acting bronchodilators with different mechanisms of action provides additional benefits over the use of a single long-acting bronchodilator, without significantly increasing the risk of adverse effects.5–7 Previous studies have shown that combining a long-acting β2-agonist with a long-acting anti-muscarinic antagonist leads to significant improvements in symptoms and lung function compared with either type of bronchodilator used alone.5,7
Acute exacerbations of COPD are associated with a poor prognosis in regard to health status, physical activity, decline in lung function, and mortality.8–13 Prevention of exacerbations is therefore of outmost importance in the management of COPD,1 and, in keeping with this, a key objective for new drugs for COPD.
The aim of this review is to provide an overview of the clinical studies evaluating the safety and clinical efficacy of the once-daily fixed-dose dual bronchodilator combination of indacaterol and glycopyrronium bromide for the treatment of COPD.
Materials and methods
In order to perform this review, the general principles of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines14,15 were adopted. A planned series of systematic searches was carried out, last updated February 2014, using the databases PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov using the following algorithm of MeSH terms: “glycopyrronium bromide”, “indacaterol”, “QVA149”, “long-acting bronchodilators”, “QAB149”, “NVA237”, “aclidinium bromide”, “tiotropium bromide”, “formoterol”, “salmeterol”, and “COPD”. These searches were repeated with these terms in combination with “FEV1”, “dyspnoea”, “health status”, “quality of life”, “day-time symptoms”, “night-time symptoms”, “exacerbations”, “hyperinflation”, and “exercise capacity”, in order to identify published studies. All searches were limited to English-language articles. As the methods and results could not be fully assessed, clinical trials published only in abstract form were excluded from this review.
Studies were included if they met all of the following criteria: 1) published in a peer-reviewed journal; 2) inclusion of adults ≥40 years of age with stable COPD defined according to the GOLD strategy document1 or the American Thoracic Society/European Respiratory Society guideline criteria;2 3) comparison of fixed-dose glycopyrronium bromide plus indacaterol with placebo, glycopyrronium bromide, indacaterol, tiotropium bromide, aclidinium bromide, formoterol, or salmeterol; and 4) also reporting at least one of the following outcomes: onset of action; trough forced expiratory volume in 1 second ([FEV1] 24 hours post-dosing) at the end of the treatment period; peak change in FEV1; health status (St George’s Respiratory Questionnaire [SGRQ]); symptom relief Transition Dyspnea Index (TDI); use of rescue medication; acute exacerbations; exercise capacity; and inspiratory capacity (IC).
Due primarily to the relatively limited number of published clinical trials fulfilling all inclusion criteria, a meta-analysis was not included in the present review.
Results
Of the 147 potential relevant citations identified by the series of searches, nine clinical trials fulfilled all inclusion criteria (6,166 participants). Characteristics of the included studies are given in Table 1. All subjects included in the trials were stable but symptomatic at baseline and fulfilled the spirometric criteria for a diagnosis of COPD. Two studies compared fixed-dose indacaterol/glycopyrronium with indacaterol (and placebo); one study with indacaterol and glycopyrronium; two studies with tiotropium (and placebo); one study with glycopyrronium and tiotropium; one study with fixed-combination salmeterol/fluticasone (SFC); one study with indacaterol, glycopyrronium, and tiotropium (and placebo); and one study with placebo.
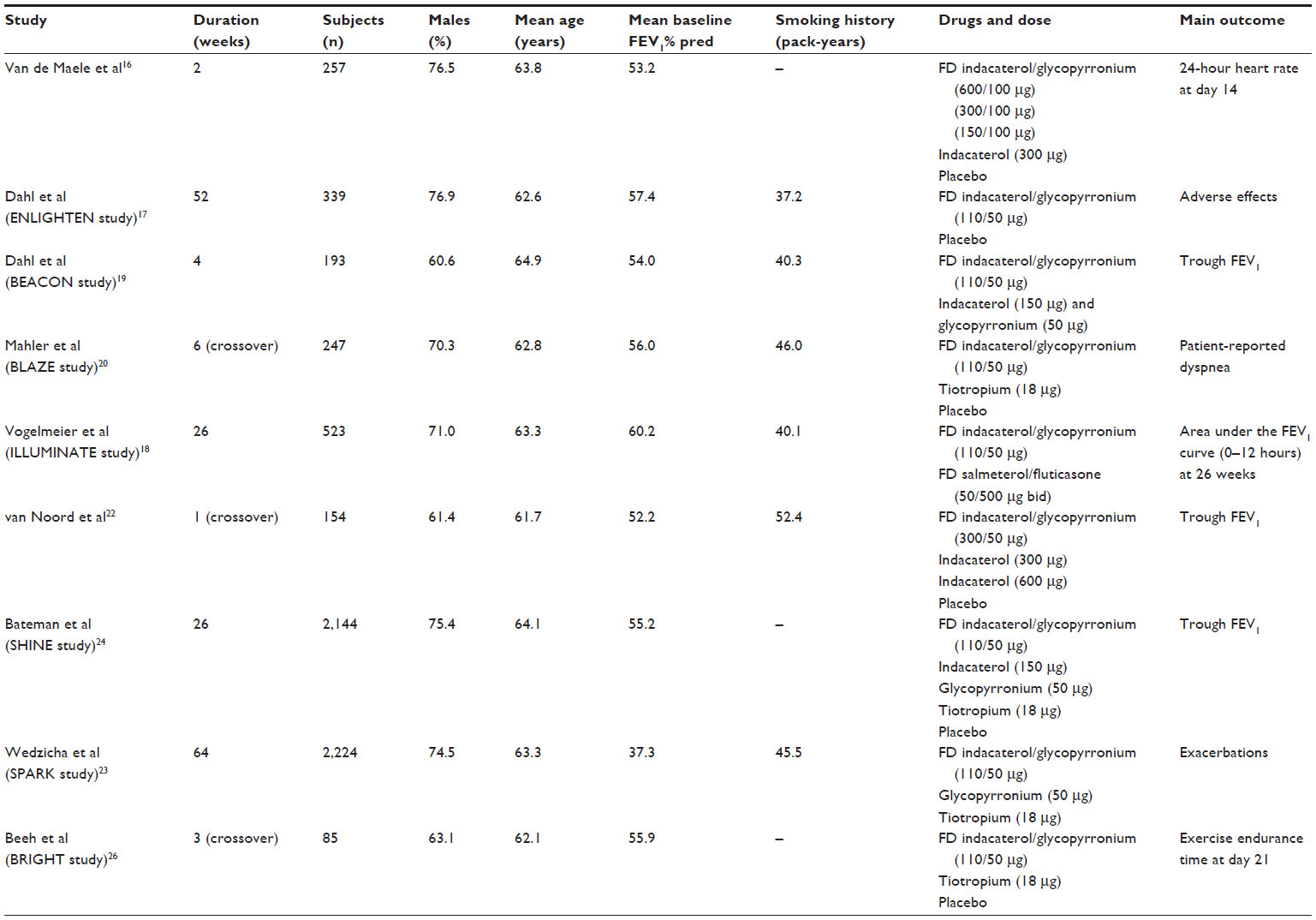 | Table 1 Characteristics of included FD indacaterol/glycopyrronium bromide studies in patients with chronic obstructive pulmonary disease |
Safety profile
The cardiovascular safety of fixed-dose indacaterol/glycopyrronium was evaluated by Van de Maele et al16 in a randomized, double-blind, placebo-controlled, parallel-group study of 257 patients with moderate-to-severe COPD. The enrolled patients were randomized to receive fixed-dose indacaterol/glycopyrronium (600/100 μg, 300/100 μg, or 150/100 μg), indacaterol 300 μg, or placebo once daily for 14 days, and the primary endpoint was change from baseline in 24-hour mean heart rate versus placebo on day 14. No clinical significant difference was observed for the primary endpoint, and once-daily fixed-dose indacaterol/glycopyrronium was, in general, well tolerated among the enrolled COPD patients with a cardiovascular safety profile, including QTc interval, and an overall rate of adverse events (AEs) similar to that of placebo.
The safety of fixed-dose indacaterol/glycopyrronium was further investigated in the ENLIGHTEN study by Dahl et al,17 in which 339 patients were randomized to either fixed-dose indacaterol/glycopyrronium or placebo for 52 weeks. The primary endpoint was safety and tolerability for treatment-emergent AEs. No difference between treatment groups was observed for the primary endpoint; likewise, no clinically relevant differences were observed for vital signs and electrocardiographic parameters. The overall incidence of AEs was similar between the two treatment arms (57.8% and 56.6%, respectively), and the most frequently reported AE was worsening of COPD (28.5% and 25.7%, respectively, for active and placebo treatment). The most common severe AE was exacerbation of COPD, and the second most common severe AE was pneumonia, the latter only reported in the indacaterol/glycopyrronium-treated group (n=8). A post hoc analysis of serious pneumonia AEs stratified by COPD severity was reported not to provide conclusive evidence that fixed-dose indacaterol/glycopyrronium was associated with a higher incidence of pneumonia than placebo (rate of events 3.6%, odds ratio 5.11; P=0.10). Although no statistically significant difference was observed, AEs that led to hospitalization or prolonged hospitalization were reported for 15.1% and 8.8%, respectively, of patients treated with fixed-dose indacaterol/glycopyrronium and placebo. In contrast to this, in the ILLUMINATE study,18 pneumonia (confirmed by chest X-ray) was only reported in patients treated with fixed-combination SFC (1.5%; no cases among patients treated with fixed-dose indacaterol/glycopyrronium).
The BEACON study by Dahl et al19 compared fixed-dose indacaterol/glycopyrronium with the concurrent administration of the mono-components indacaterol and glycopyrronium and found that the safety and efficacy profile was similar for the two treatment arms.
Symptom relief and use of rescue medication
Mahler et al20 investigated the effect of fixed-dose indacaterol/glycopyrronium versus placebo and tiotropium on dyspnea in the blinded, double-dummy, crossover BLAZE study comprising 247 patients with moderate-to-severe COPD (staging according to the GOLD 2007 criteria; mean post-bronchodilator FEV1 56% predicted [pred]). Changes in dyspnea were assessed by the self-administered computerized versions of the Baseline Dyspnea Index and the TDI after 6 weeks. The TDI total score was statistically significantly improved with fixed-dose indacaterol/glycopyrronium at 6 weeks compared to both placebo and tiotropium. However, only the improvement with fixed-dose indacaterol/glycopyrronium versus placebo reached the minimal clinically important difference (MCID) of ≥1 point;21 this MCID in total TDI score with fixed-dose indacaterol/glycopyrronium was seen in patients with both moderate (least squares mean [LSM] treatment difference 1.11; P<0.001) and severe (LSM treatment difference 1.92; P<0.001) COPD (defined on spirometric criteria) compared with placebo. A TDI responder analysis comparing fixed-dose indacaterol/glycopyrronium and tiotropium revealed that the proportion of patients achieving the MCID of at least 1 point was higher with fixed-dose indacaterol/glycopyrronium than with either placebo (35.9% and 18.1%, respectively; P<0.001) or tiotropium (24.4%; P=0.012). However, it should be noted that the MCID for comparisons between active treatments has not yet been established.
The BLAZE study20 also showed a significant improvement in percentage of nights with no awakenings, days with no daytime symptoms, and days with usual daily activities compared with placebo, whereas no significant difference in these outcomes was observed between fixed-dose indacaterol/glycopyrronium and tiotropium; in line with this, no statistically significant differences were observed between the two active treatment arms with regard to mean daily total and individual symptom (respiratory symptoms, cough, wheeze, and amount of sputum) scores. However, the patients treated with fixed-dose indacaterol/glycopyrronium used less rescue medication and had a higher percentage of days with no use of rescue medication compared to both placebo (P<0.001) and tiotropium (P=0.002 and P<0.001). Similar findings with regard to symptoms and use of rescue medication were reported in the ENLIGHTEN study.17
Vogelmeier et al18 reported that fixed-dose indacaterol/glycopyrronium significantly increased the TDI focal score after 26 weeks of treatment compared with fixed-combination SFC, with a treatment difference of 0.76 (P=0.003). Although, on average, not reaching the MCID for TDI score, 67.5% of patients treated with fixed-dose indacaterol/glycopyrronium compared with 56.8% of patients on SFC had an increase of at least 1 point in TDI score (P=0.046). However, no difference in change in total SGRQ score was observed between the two treatment groups; likewise, only modest and, in general, nonsignificant differences were reported with regard to symptoms and use of rescue medication.18
With regard to rescue medication, van Noord et al22 found no difference in number of puffs used by patients treated with fixed-dose indacaterol/glycopyrronium and indacaterol, whereas Wedzicha et al23 reported a significant decrease in use of rescue medication (salbutamol) for patients treated with fixed-dose indacaterol/glycopyrronium compared with glycopyrronium and tiotropium.
The SHINE study24 showed significant improvements in TDI focal score, use of rescue medication, daytime symptoms, nighttime symptoms, and ability to perform usual daily activities for fixed-dose indacaterol/glycopyrronium compared with monotherapy with a long-acting bronchodilator and placebo. Furthermore, the SHINE study also showed a significant improvement in SGRQ total score at week 12 and week 26 compared with placebo, whereas no significant improvement was observed for the other active treatments (indacaterol, glycopyrronium, and tiotropium) or placebo.24
Wedzicha et al23 reported an improvement in SGRQ total score from baseline of 8–9 units with fixed-dose indacaterol/glycopyrronium; 6 units with glycopyrronium; and 5–6 units with tiotropium, and the treatment differences in SGRQ total score between fixed-dose indacaterol/glycopyrronium were −1.9 to −2.8 and −1.7 to −3.1, respectively, compared with glycopyrronium (P<0.01) and tiotropium (P<0.05). In keeping with this, the percentage of patients achieving the MCID in total SGRQ score was significantly higher for fixed-dose indacaterol/glycopyrronium compared with both glycopyrronium and tiotropium up to week 52.
FEV1
van Noord et al,22 in a four-period crossover study (n=154), compared the efficacy of once-daily fixed-dose indacaterol/glycopyrronium (300/50 μg) with indacaterol (600 μg and 300 μg) and placebo. The primary outcome variable was trough FEV1 on day 7 (Table 1). The LSM trough FEV1 on day 7 was significantly higher for fixed-dose indacaterol/glycopyrronium compared with placebo (treatment difference 0.226 L; P<0.001) and with indacaterol 300 μg or 600 μg (treatment difference 0.123 L and 0.117 L, respectively; P<0.001). Furthermore, fixed-dose indacaterol/glycopyrronium had a faster onset of action (at 5 minutes post-dose on day 1) compared with placebo and with indacaterol 300 μg or 600 μg (P<0.0001); the treatment difference between fixed-dose indacaterol/glycopyrronium and placebo was 0.141 L, whereas no exact data were reported for the treatment difference between fixed-dose indacaterol/glycopyrronium and indacaterol.
In the SHINE study, Bateman et al24 investigated the efficacy of fixed-dose indacaterol/glycopyrronium versus its mono-components indacaterol and glycopyrronium, tiotropium, and placebo over 26 weeks. Patients with moderate-to-severe COPD (defined according to the GOLD 2007 spirometric criteria; n=2,144) were randomized to once-daily fixed-dose indacaterol/glycopyrronium (110/50 μg), indacaterol (150 μg), glycopyrronium (50 μg), open-label tiotropium (18 μg), or placebo (Table 1). The primary outcome was trough FEV1 at week 26 for fixed-dose indacaterol/glycopyrronium versus its mono-components. At week 26, a significant improvement was seen in trough FEV1 for fixed-dose indacaterol/glycopyrronium compared with both indacaterol (treatment difference 0.07 L; P<0.001) and glycopyrronium (treatment difference 0.09 L; P<0.001); likewise, a significant improvement was observed for fixed-dose indacaterol/glycopyrronium compared with tiotropium and placebo (treatment difference 0.08 L and 0.20 L, respectively; P<0.001). The observed statistically significant differences between fixed-dose indacaterol/glycopyrronium versus all active treatments and placebo in trough FEV1 were maintained throughout the study period. Similar to the findings reported by van Noord et al,22 the SHINE study24 revealed that fixed-dose indacaterol/glycopyrronium provides rapid bronchodilation after administration of the first dose on day 1, as the FEV1, FEV1 4-hour area under the curve, and peak FEV1 were higher compared with placebo, glycopyrronium, and tiotropium, whereas data were not given for the comparison with indacaterol. Subgroup analysis showed that the improvement in trough FEV1 was seen both in patients with moderate and with severe COPD (defined by the spirometric GOLD criteria), although the treatment differences between fixed-dose indacaterol/glycopyrronium and monotherapy with a long-acting bronchodilator (indacaterol, glycopyrronium, and tiotropium) was less than 0.10 L.
Vogelmeier et al,18 in the ILLUMINATE study, compared the safety and efficacy of fixed-dose indacaterol/glycopyrronium versus fixed-combination SFC over 26 weeks in patients with moderate-to-severe COPD. In this double-blind, double-dummy, parallel-group study, 523 patients (without exacerbations in the year prior to study entry) were randomized to either fixed-dose indacaterol/glycopyrronium (110/50 μg once daily) or SFC (50/500 μg twice daily). The primary outcome was the standardized area under the FEV1 curve from 0–12 hours post-dose (FEV1AUC0–12) at week 26. Thirty-five percent of the enrolled patients were treated with ICS at baseline, and the mean post-bronchodilator FEV1 was 60.2% pred (Table 1). The FEV1AUC0–12 was significantly higher for patients treated with fixed-dose indacaterol/glycopyrronium (1.70 L) than for patients treated with SFC (1.56 L), with a treatment difference of 0.14 L (P<0.0001) at week 26; this treatment difference in FEV1AUC0–12 was observed throughout the study period. Similar findings were reported for other spirometric parameters, including peak FEV1 and forced vital capacity.18
After 6 weeks of treatment in the BLAZE study,20 a significant and clinically meaningful25 improvement in mean FEV1 was seen at every time point from 45 minutes pre-dose to 4 hours post-dose versus both placebo and tiotropium (P<0.001).
The ENLIGHTEN study17 showed a significant improvement in pre-dose FEV1 at week 52 compared with placebo (treatment difference 0.189 L; P<0.001), and the treatment difference in pre-dose FEV1 from week 3 to week 52 versus placebo was in the range of 0.152–0.189 L (P<0.001). Furthermore, the 60-minute post-dose FEV1 was significantly higher for patients treated with fixed-dose indacaterol/glycopyrronium compared with placebo (treatment difference 0.200–0.286 L; P<0.001).
Trough FEV1 in the SPARK study23 was significantly higher for fixed-dose indacaterol/glycopyrronium at all evaluated time points compared with glycopyrronium (treatment difference 0.08–0.09 L; P<0.0001) and tiotropium (treatment difference 0.06–0.08 L; P<0.0001).
Exercise capacity and hyperinflation
In the BRIGHT study, Beeh et al26 investigated the effect of fixed-dose indacaterol/glycopyrronium compared with placebo and tiotropium on exercise tolerance in patients with moderate-to-severe COPD (defined according to the GOLD 2007 spirometric criteria; mean FEV1 55.9% pred) (Table 1). A total of 85 patients were randomized to fixed-dose indacaterol/glycopyrronium (110/50 μg), placebo, or tiotropium (18 μg) once daily in a blinded, three-period, crossover study for 3 weeks. The primary outcome variable was exercise endurance time at day 21 for fixed-dose indacaterol/glycopyrronium versus placebo. Fixed-dose indacaterol/glycopyrronium significantly improved exercise endurance time at day 21 compared with placebo (LSM treatment difference 60 seconds). A similar improvement in exercise endurance time was observed with tiotropium compared with placebo (LSM treatment difference 66 seconds). In line with this, an analysis of data for the subgroup of patients with hyperinflation (defined as functional residual capacity [FRC] >120% pred), showed that the mean changes in exercise endurance time from baseline were 85 seconds and 88 seconds, respectively, for indacaterol/glycopyrronium and tiotropium. A significant improvement in IC at peak exercise was observed for fixed-dose indacaterol/glycopyrronium compared with both placebo and tiotropium, and a similar difference was observed for trough IC.
In the study by van Noord et al,22 changes in IC, although not stated as a secondary outcome variable, were also determined. The authors reported that both LSM IC and trough IC were significantly better for fixed-dose indacaterol/glycopyrronium compared with both indacaterol and placebo (P=0.02).
Exacerbations
Wedzicha et al, in the SPARK study,23 investigated the effect of fixed-dose indacaterol/glycopyrronium on exacerbations in patients with severe and very severe COPD (defined according to the GOLD 2007 spirometric criteria). In a parallel-group study, 2,224 patients (having had at least one exacerbation of COPD in the year prior to enrollment) were randomized to fixed-dose indacaterol/glycopyrronium (110/50 μg), glycopyrronium (50 μg), or open-label tiotropium (18 μg) for 64 weeks. The primary outcome variable was to demonstrate superiority of fixed-dose indacaterol/glycopyrronium for the rate of moderate (defined as worsening of symptoms treated with systemic corticosteroids or antibiotics or both) and severe (defined as worsening of symptoms requiring emergency treatment or hospitalization) exacerbations compared to monotherapy with glycopyrronium. The key secondary outcome variable was to demonstrate superiority of fixed-dose indacaterol/glycopyrronium compared with tiotropium with regard to the rate of moderate and severe exacerbations. Twenty-two percent of the patients included in the efficacy analyses had had two or more exacerbations in the previous year, and 88% of the patients had one or more cardiovascular risk factors at baseline, although few patients had a history of cardiovascular disease. Furthermore, 75% of the patients in all three treatment arms were treated with ICSs throughout the study period. The rate of moderate or severe exacerbations was significantly reduced by 12% for the fixed-dose indacaterol/glycopyrronium group compared with the glycopyrronium group (P=0.038), whereas the 10% reduction in the rate of moderate or severe exacerbations with fixed-dose indacaterol/glycopyrronium compared with tiotropium was nonsignificant. The overall rate of exacerbations (mild, moderate, and severe) was significantly reduced with fixed-dose indacaterol/glycopyrronium, by 15% and 14%, respectively, compared with glycopyrronium and tiotropium. The number of severe exacerbations was low, with no differences between treatment arms.
Discussion
The combination of two long-acting bronchodilators with different mechanisms of action is likely to have the potential to enhance efficacy compared with single long-acting bronchodilators, without a concomitant increase in adverse effects. Fixed-dose indacaterol/glycopyrronium is, based on the available evidence, a safe and well-tolerated dual long-acting bronchodilator. In patients with moderate-to-very severe COPD (defined by GOLD spirometric criteria), fixed-dose indacaterol/glycopyrronium has clinically important effects on symptoms, including dyspnea score, health status, level of FEV1, exercise endurance time, and rate of exacerbations.
Bronchodilation improves airway conductance and airflow and reduces hyperinflation, which subsequently leads to a reduction in dyspnea. Sustained bronchodilation is therefore, in accordance with the current GOLD strategy document,1 recommended as maintenance therapy for patients with symptomatic COPD. The published studies show that treatment with once-daily fixed-dose indacaterol/glycopyrronium leads to clinically important improvements, not only in lung function, but also in other important endpoints such as dyspnea index, health status, symptoms, exercise endurance time, and use of rescue medication, although the findings with regard to use of rescue medication were not absolutely consistent. The studies of fixed-dose indacaterol/glycopyrronium are therefore in accordance with several previously published studies that have investigated the efficacy of free combinations of long-acting β2-agonists and long-acting anti-muscarinic agents27–30 in patients with COPD. Furthermore, these studies are also in accordance with a very recently published study by Celli et al31 investigating the safety and efficacy of once-daily fixed-dose umeclidinium/vilanterol in patients with COPD.
Sustained bronchodilation is also thought to contribute to the reduction in exacerbations of COPD seen with treatment with long-acting bronchodilators, and, although long-acting anti-muscarinic agents are primarily thought to reduce exacerbations by reducing dynamic hyperinflation, both long-acting β2-agonists and long-acting anti-muscarinic agents may have anti-inflammatory effects.32–34
The studies published so far investigating the safety and, not least, efficacy of fixed-dose indacaterol/glycopyrronium support the GOLD 2013 strategy1 alternative-choice recommendation that add-on of a second long-acting bronchodilator in patients with moderate-to-very severe COPD (GOLD 2013 groups B–D) may improve symptom control, and, in line with this, that patients classified as being “low-risk” (group B), who remain symptomatic on a single long-acting bronchodilator, may significantly benefit from fixed-dose indacaterol/glycopyrronium. Furthermore, the reported findings also support the GOLD 2013 strategy secondary choice recommendation for “high-risk” patients (groups C and D based on symptoms and exacerbations), as a long-acting β2-agonist plus a long-acting anti-muscarinic agent is recommended as an alternative to a long-acting β-agonist plus ICS (group C) or ICS plus long-acting β2-agonist and/or long-acting anti-muscarinic agent (group D).
Conclusion
The published studies indicate that once-daily fixed-dose indacaterol/glycopyrronium may become an important therapeutic maintenance option for patients with moderate-to-very severe COPD. In years to come, combination therapy with a long-acting antimuscarinic agent and a long-acting β2-agonist, preferably as fixed combination, may become the treatment of choice for maintenance therapy-naïve patients with symptomatic COPD.
Disclosure
The author has received honorarium for lectures etc from Novartis, GSK, AZ, Boehringer-Ingelheim, Takeda, Teva, Pfizer, Cephalon, Stallergenes, Norpharma, Almirall, and MSD within the last 5 years.
References
Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. | |
Celli BR, MacNee W; ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. | |
[No authors listed]. In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. COMBIVENT Inhalation Aerosol Study Group. Chest. 1994;105(5):1411–1419. | |
Benayoun S, Ernst P, Suissa S. The impact of combined inhaled bronchodilator therapy in the treatment of COPD. Chest. 2001;119(1):85–92. | |
Vogelmeier C, Kardos P, Harari S, Gans SJ, Stenglein S, Thirlwell J. Formoterol mono- and combination therapy with tiotropium in patients with COPD: a 6-month study. Respir Med. 2008;102(11):1511–1520. | |
Cazzola M, Molimard M. The scientific rationale for combining long-acting beta2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23(4):257–267. | |
van Noord JA, Aumann JL, Janssens E, et al. Combining tiotropium and salmeterol in COPD: Effects on airflow obstruction and symptoms. Respir Med. 2010;104(7):995–1004. | |
Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. | |
Donaldson GC, Wilkinson TM, Hurst JR, Perera WR, Wedzicha JA. Exacerbations and time spent outdoors in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(5):446–452. | |
Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Physical activity and hospitalization for exacerbation of COPD. Chest. 2006;129(3):536–544. | |
Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. | |
Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. | |
Kanner RE, Anthonisen NR, Connett JE; Lung Health Study Research Group. Lower respiratory illnesses promote FEV(1) decline in current smokers but not ex-smokers with mild chronic obstructive pulmonary disease: results from the lung health study. Am J Respir Crit Care Med. 2001;164(3):358–364. | |
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–e34. | |
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. | |
Van de Maele B, Fabbri LM, Martin C, Horton R, Dolker M, Overend T. Cardiovascular safety of QVA149, a combination of Indacaterol and NVA237, in COPD patients. COPD. 2010;7(6):418–427. | |
Dahl R, Chapman KR, Rudolf M, et al. Safety and efficacy of dual bronchodilation with QVA149 in COPD patients: the ENLIGHTEN study. Respir Med. 2013;107(10):1558–1567. | |
Vogelmeier CF, Bateman ED, Pallante J, et al. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomised, double-blind, parallel group study. Lancet Respir Med. 2013;1(1):51–60. | |
Dahl R, Jadayel D, Alagappan VK, Chen H, Banerji D. Efficacy and safety of QVA149 compared to the concurrent administration of its monocomponents indacaterol and glycopyrronium: the BEACON study. Int J Chron Obstruct Pulmon Dis. 2013;8:501–508. | |
Mahler DA, Decramer M, D’Urzo A, et al. Dual bronchodilation with QVA149 reduces patient-reported dyspnoea in COPD: BLAZE study. Eur Respir J. Epub October 31, 2013. | |
Mahler DA, Witek TJ Jr. The MCID of the transition dyspnea index is a total score of one unit. COPD. 2005;2(1):99–103. | |
van Noord JA, Buhl R, Laforce C, et al. QVA149 demonstrates superior bronchodilation compared with indacaterol or placebo in patients with chronic obstructive pulmonary disease. Thorax. 2010;65(12):1086–1091. | |
Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med. 2013;1(3):199–209. | |
Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–1494. | |
Donohue JF. Minimal clinically important differences in COPD lung function. COPD. 2005;2(1):111–124. | |
Beeh KM, Korn S, Beier J, et al. Effect of QVA149 on lung volumes and exercise tolerance in COPD patients: the BRIGHT study. Respir Med. Epub January 21, 2014. | |
Mahler DA, D’Urzo A, Bateman ED, et al; INTRUST-1 and INTRUST-2 study investigators. Concurrent use of indacaterol plus tiotropium in patients with COPD provides superior bronchodilation compared with tiotropium alone: a randomised, double-blind comparison. Thorax. 2012;67(9):781–788. | |
van Noord JA, Aumann JL, Janssens E, et al. Comparison of tiotropium once daily, formoterol twice daily and both combined once daily in patients with COPD. Eur Respir J. 2005;26(2):214–222. | |
Berton DC, Reis M, Siqueira AC, et al. Effects of tiotropium and formoterol on dynamic hyperinflation and exercise endurance in COPD. Respir Med. 2010;104(9):1288–1296. | |
Tashkin DP, Pearle J, Iezzoni D, Varghese ST. Formoterol and tiotropium compared with tiotropium alone for treatment of COPD. COPD. 2009;6(1):17–25. | |
Celli B, Crater G, Kilbride S, et al. Once-daily umeclidinium/vilanterol 125/25 mcg in copd: a randomized, controlled study. Chest. Epub January 2, 2014. | |
Domínguez-Fandos D, Ferrer E, Puig-Pey R, et al. Effects of aclidinium bromide in a cigarette smoke-exposed Guinea pig model of chronic obstructive pulmonary disease. Am J Respir Cell Mol Biol. 2014;50(2):337–346. | |
Johnson M, Rennard S. Alternative mechanisms for long-acting beta(2)-adrenergic agonists in COPD. Chest. 2001;120(1):258–270. | |
Wedzicha JA, Decramer M, Seemungal TA. The role of bronchodilator treatment in the prevention of exacerbations of COPD. Eur Respir J. 2012;40(6):1545–1554. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.