")
Back to Journals » Cancer Management and Research » Volume 13
Clinical and Prognostic Implications of 1p/19q, IDH, BRAF, MGMT Promoter, and TERT Promoter Alterations, and Expression of Ki-67 and p53 in Human Gliomas
Authors Yang Z, Ling F, Ruan S, Hu J, Tang M, Sun X, Long W
Received 27 August 2021
Accepted for publication 8 November 2021
Published 23 November 2021 Volume 2021:13 Pages 8755—8765
DOI https://doi.org/10.2147/CMAR.S336213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Harikrishna Nakshatri
Zixi Yang,1 Feng Ling,1 Sibei Ruan,1 Jiajia Hu,2 Mingxi Tang,1 Xingwang Sun,1 Wenbo Long1
1Pathology Department of the First Affiliated Hospital, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 2School of Basic Medicine, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China
Correspondence: Wenbo Long Email [email protected]
Background and Objective: Genetic alterations, including IDH, BRAF, and TERT promoter mutations (IDH-mu, BRAF-mu, TERTp-mu, respectively), 1p/19q co-deletion (1p/19q-codel), and MGMT promoter methylation (MGMTp-M), are correlated with glioma tumor development. Therefore, these genetic alterations could serve as biomarkers for the diagnosis, prognosis, and classification of gliomas, combined with the immunohistochemical markers Ki-67 and p53. However, the correlation between these alterations and the expression of Ki-67 and p53 is poorly understood.
Methods: We analyzed the prevalence and prognosis of these five alterations, as well as Ki-67 and p53 expression, in 103 primary grade II–IV gliomas via fluorescence qPCR, Sanger sequencing, fluorescence in situ hybridization, and immunohistochemistry.
Results: In the 103 cases, MGMTp-M was the most common alteration (70.9%), followed by TERTp-mu (58.3%), IDH-mu (46.6%), 1p/19q-codel (34.0%), and BRAF-mu (5.8%). No cases showed quintuple-positive alterations, but 26 cases (25.2%) showed quadruple-positive alterations (IDH-mu/TERTp-mu/MGMTp-M/1p/19q-codel). The percentage of TERTp-mu and 1p/19q-codel cases decreased with p53 expression, and the percentage of IDH-mu and 1p/19q-codel cases decreased with Ki-67 expression. IDH-mu, MGMTp-M, and 1p/19q-codel were positive factors for survival rates in glioma patients, while TERTp-mu, p53, and Ki-67 positivity were negative factors. Old age, histological grade IV, IDH-mu, 1p/19q-codel, Ki-67+, and p53+/Ki-67+ were significantly correlated with overall survival (OS). However, only p53+/Ki-67+ was an independent prognostic factor for OS in the multivariate Cox-model analysis.
Conclusion: IDH-mu only and quadruple-positivity were associated with good OS in glioma patients, while TERTp-mu only, TERTp-mu/MGMTp-M and p53+/Ki-67+ were associated with poor prognosis. Combining these genomic alterations and Ki-67/p53 expression should have clinical value in gliomas.
Keywords: human glioma, biomarker, correlation analysis, genetic alteration, survival rate
Introduction
Diffuse gliomas are the most common form of primary malignant brain tumor and affect adults worldwide.1 Gliomas can be categorized as astrocytomas, oligodendrogliomas, and ependymomas and are graded II–IV according to the World Health Organization (WHO) classification, with the deadliest form being glioblastoma (GBM).2 The histopathological classification of diffuse gliomas is influenced by interobserver variation arising from morphological classification, which can result in inconsistent histological grading and typing.3 To address this challenge, molecular markers are increasingly being developed and employed to guide the diagnosis and clinical management of gliomas.
Ki-67 and p53 are two well-studied molecules in human cancer. Ki-67 is a marker of cell division and a reliable indicator of tumor cell proliferation that is associated with the histological grade of gliomas. Although there is disagreement regarding the role of Ki-67 as a prognostic marker, many studies have revealed that it predicts poor prognosis in glioma patients.4 Although altered expression of the p53 gene is not necessarily correlated with survival, immunohistochemical expression of p53 is a possible prognostic biomarker in glioma patients.5
Besides these traditional immunohistochemical markers, markers based on genomic variation have been developed to facilitate the diagnosis and prognosis of gliomas. Specifically, point mutations in isocitrate dehydrogenase genes (IDH-mu), mutations in the promoter region of the telomerase reverse transcriptase gene (TERTp-mu), and co-deletion of chromosome arms 1p and 19q (1p/19q-codel) can be used to classify gliomas into five principal groups according to age, survival, and associated genomic alterations.6 Although it is unclear how these mutations contribute to tumor development, IDH-mu and 1p/19q-codel are used to define oligodendroglioma (O), which is characterized by high interobserver discordance.7 Like IDH-mu, TERTp-mu is frequently observed in gliomas — especially primary GBM tumors — but is less frequent in low grade astrocytoma (A) tumors.8 As a result, TERTp-mu and IDH-mu are used in clinical settings and facilitate the identification of about 80% of GBMs from other tumor types.6,8,9 Methylguanine-DNA methyltransferase promoter methylation (MGMTp-M) has also been explored to stratify malignant gliomas into subgroups and is used as a prognostic marker for overall survival (OS) and a predictive factor for chemotherapy in GBM patients.10 The V600 mutation in the v-raf murine sarcoma oncogene homologue B1 (BRAF-mu) is not common in adult gliomas but frequently appears in low-grade pediatric gliomas and is highly variable across patient groups.11 Given these confusing features, further research is needed to elucidate the clinical value of the BRAF mutation.
To date, not many studies have investigated the relationships among the various glioma markers. Though some studies have analyzed the correlation among 1p/19q, IDH, TERTp, MGMTp, and BRAF alterations in recent years,6,8,9,11 there are still some controversial. Moreover, few studies discussed the combination of these alterations with the expression of p53 and Ki-67 in glioma tumors. To address this research gap, we investigated the prevalence of MGMTp-M, BRAF-mu, IDH-mu, TERTp-mu, 1p/19q-codel, and immunohistochemical expression of p53 and Ki-67 in 103 patients with grades II–IV primary gliomas. We analyzed the relationships of these molecular markers with clinicopathological characteristics and survival. We also analyzed the clinical significance of combining these markers in predicting the survival of glioma patients. The present study will contribute to an increased understanding of the molecular background of tumor types and support histological classification and prognosis of gliomas based on these markers.
Methods
Patients and Specimens
A total of 103 primary glioma samples were collected from 103 patients diagnosed with primary diffuse gliomas (grade II–IV) at the Affiliated Hospital of Southwest Medical University (Luzhou, China) between June 2017 and June 2020 (Supplementary Table 1). All patients were chemotherapy-free and targeted drug-naive at the time of surgery. All patient data in this manuscript were coded and utilized anonymously. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Research Ethics Committee of the First Affiliated Hospital of Southwest Medical University, China. Written informed consent was obtained from all patients prior to the study.
Glioma samples were formalin-fixed and paraffin-embedded (FFPE), sectioned into 4 μm thick slices, and then permanently fixed on microscope slides. After hematoxylin and eosin (H&E) staining, the slides were reviewed by two pathologists and classified according to the WHO 2016 recommendation.
DNA Extraction
Genomic DNA was extracted from 6 μm thick sections of FFPE tumor tissue using the DNA extraction kit for paraffin embedded tissues (DP331) (Tiangen, Beijing, China) according to the manufacturer’s protocol. DNA concentration and quality were measured using a Nano-Drop ND-1000 spectrophotometer (NanoDrop Technologies, Houston, USA).
IDH1, IDH2, and TERTp Mutations
Mutations in IDH1 (R132H), IDH2 (R172K), and TERTp (C228T and C250T) were determined by PCR and Sanger sequencing using detection kits (SinoMD Gene Testing Technology Co., Ltd, Beijing, China) with positive and negative controls. Sequences covering mutational hotspots in the IDH1, IDH2, and TERT core promoters were amplified by fluorescence qPCR. Assessments of IDH1 (R132), IDH2 (R172), and TERTp mutations were conducted using the following primer sets: IDH1-F: 5ʹ-CTCCT GATGA GAAGA GGGTT G-3ʹ, R: 5ʹ-TGGAA ATTTC TGGGC CATG-3ʹ; IDH2-F: 5ʹ-TGGAA CTATC CGGAA CATCC-3ʹ, R: 5ʹ-AGTCT GTGGC CTTGT ACTGC; TERTp-F: 5ʹ-GGCCG ATTCG ACCTC TCT, R: 5ʹ-AGCAC CTCGC GGTAG TGG. PCR was performed in a total volume of 25 μL comprising 2 μL DNA in solution (10–50 ng/mL), 12.5 μL IDH1, IDH2, or TERTp PCR reaction mix, 4.5 μL primers (0.25 nM each), and 6 μL ddH2O. Amplification was performed using a LightCycler480 II instrument (Roche) with an initial denaturing step at 95°C for 3 min followed by 40–45 cycles of denaturation at 94°C for 15 s, annealing at 60°C for 45 s, and a final extension at 60°C for 5 min. PCR products were treated with SAP enzyme in a product: enzyme volume ratio of 5:2 at 37°C for 60 min, followed by 80°C for 15 min. After purification, products were subjected to direct sequencing on an ABI 3500 sequencer.
MGMT Promoter Methylation
A total of 1000 ng DNA were subjected to bisulfite treatment using a DNA bisulfite transformation kit (Tiangen, DP215). Methylation of MGMTp was determined using a detection kit (SinoMD Gene Testing Technology Co., Ltd, Beijing, China) with positive and negative controls. Primers for PCR amplification of the MGMT promoter region were as follows: methylated-F: 5ʹ-GCGTT TCGAC GTTCG TAGGT-3ʹ, R: 5ʹ-CACTC TTCCG AAAAC GAAAC G-3ʹ; unmethylated-F: 5ʹ-TGTGT TTTCG ATATG TTGGG ATAGT-3ʹ, R: 5ʹ-AACTC CACAC TCTTC CAAAA ACAA-3ʹ. PCR was performed in a total volume of 25 μL comprising 2 μL sample or reference DNA in solution, 12.5 μL MGMT PCR reaction mix, 5.5 μL primers (0.25 nM each), and 5 μL ddH2O. The PCR conditions were as follows: a denaturing step at 95°C for 3 min, 45 cycles of denaturation at 94°C for 15 s, annealing at 60°C for 45 s, and a final extension at 60°C for 5 min. The Ct values of sample DNA amplification (Cts) and reference DNA amplification (Ctr) were recorded. When Ctr ≤ 35 and Cts ≤ 40, a result with Cts − Ctr ≤ 11 was defined as positive and Cts − Ctr > 11 as negative; when Ctr ≤ 35 but Cts > 40, the result was defined as negative; when Ctr > 35, the result was regarded meaningless.
BRAF V600E Mutation
Mutations in BRAF V600E were detected using the BRAF V600E fluorescence detection kit (AmoyDx Biotechnology Co., Ltd, 8.0120301X024, Xiamen, China) with positive and negative controls. Samples were amplified in a 50 μL volume in 96-well plates in duplicate. PCR amplification comprised 45 μL PCR reaction mix, 0.4 μL Taq enzymes, and 4.6 μL DNA (1–10 ng). A LightCycler480 II instrument (Roche) was used to carry out PCR as follows: 95°C for 5 min; 15 cycles of 95°C for 20 s, 64°C for 20 s, and 72°C for 20 s; 30 cycles of 93°C for 25 s, 60°C for 35 s, and 72°C for 20 s; and finally 72°C for 5 min. The Ct values of sample DNA amplification (Cts) and reference DNA amplification (Ctr) were recorded. When Ctr was between 13 and 21, a result with Cts < 30 was defined as positive, while Cts ≥30 was defined as negative; when Ctr > 21, the result was regarded meaningless or that the sample DNA load should be increased.
Deletion Test of 1p/19q
New 4 μm sections of the representative tumor areas marked by H&E staining were selected to test the status of 1p/19q. The sections were deparaffinized with xylene, rehydrated with 100%, 90%, and 70% ethanol and water for 5 min each, and then repaired with 1× EDTA in a steam cooker. After washing and drying, the sections were subjected to 30 min of pepsin digestion at 37°C. Paired 1p and 19q probes (AnBiPing Pharmaceutical Technology Co., Ltd, F.01081, Guangzhou, China) were added to each slide at a volume of 10 μL and codenatured with the target DNA at 85°C for 5 min. The slides were incubated overnight at 37°C in a humidified oven and subsequently washed for 10 min with 2× SSC. Green and red fluorescent signals were quantified using an Olympus BX60 fluorescence microscope with the appropriate filters. For each slide, a minimum of 100 non-overlapping nuclei was assessed for the numbers of green and red signals.
Immunohistochemistry of Ki-67 and p53
To detect Ki-67 and p53 expression, mouse anti‑human monoclonal primary antibodies against Ki-67 and p53 (Maixin Biotechnology Development Co., Ltd, MAB-0672, 1:1000 and MAB-0674, 1:1000, respectively, Fuzhou, China) were used according to the manufacturer’s protocol. Each slide was individually reviewed and scored by two independent pathologists. The indexes of Ki-67 and p53 were determined as the percentage of immunostained cells per 200 cells in 5 fields. For analysis, p53 was scored according to Hu et al12: negative 0, no positive cells; score 1, weakly positive (<25% positive cells); score 2, moderately positive (25–50% positive cells); and score 3, strongly positive (>50% positive cells). Similarly, we used a 0–3 scoring system for the Ki-67 index: negative 0, <5% positive cells; score 1, weakly positive (5–25% positive cells); score 2, moderately positive (25–50% positive cells); and score 3, strongly positive (>50% positive cells). Controls without the primary antibody and positive control tissues were included in all experiments to ensure quality staining.
Statistical Analysis
The chi-square test or two-tailed Fisher’s exact test was used for statistical analyses of categorical variables, such as genetic alterations, immune expression, and clinicopathological features. A p-value < 0.05 was considered statistically significant. OS was defined as the first day of surgery until death or the end of follow-up. Survival differences among groups were calculated using the Kaplan–Meier method with the Log rank test. We used the Cox proportional hazards model for univariate and multivariate OS analyses. SPSS software version 19.0 (IBM Armonk, NY, USA) was used for all statistical analyses.
Results
Clinicopathologic Characteristics
A total of 103 patients were included in this study, comprising 45 men (46.7%) and 58 women (56.3%) with a mean age of 48.5 ± 11.3 years (range 17–74 years) and 48.0 ± 14.8 years (range 16–83 years), respectively. There were 84 patients (81.6%) younger than 60 and only 19 patients (18.4%) older than 60. Histological classifications were done according to the 2016 revised criteria of the World Health Organization (WHO) as follows: 17 diffuse A (16.5%) cases, 19 anaplastic astrocytoma (AA) (18.4%) cases, 18 O (17.5%) cases, 12 anaplastic oligodendroglioma (AO) (11.7%) cases, 1 oligoastrocytoma (OA) (1.0%) cases, and 36 GBM (35.0%) cases. Categorization by WHO histological grade at diagnosis yielded 35 grade II cases (34.0%), 32 grade III cases (31.1%), and 36 grade IV cases (35.0%).
Characteristics of IDH, BRAF, and TERTp Mutations, MGMTp Methylation, and 1p/19q Codeletion in Gliomas
A total of 45 and 3 mutations (Table 1) were observed that produced R132H of the IDH1 gene and R172K of the IDH2 gene, respectively, in gliomas. However, no tumors were observed with mutations in both IDH1 and IDH2. The frequencies of MGMTp-M, BRAF-mu, and 1p/19q-codel, but not TERTp-mu, in IDH-mu cases were higher than those in IDH-wt cases. Unlike TERTp-mu, IDH-mu, MGMTp-M, BRAF-mu, and 1p/19q-codel mutations were identified with a higher frequency in grade II–III cases and a lower frequency in grade IV cases. Among the 103 cases, 5 (4.9%) showed apparent 1p deletion only, 4 (3.9%) showed apparent 19q deletion only, while 35 (34.0%) showed apparent 1p/19q-codel.
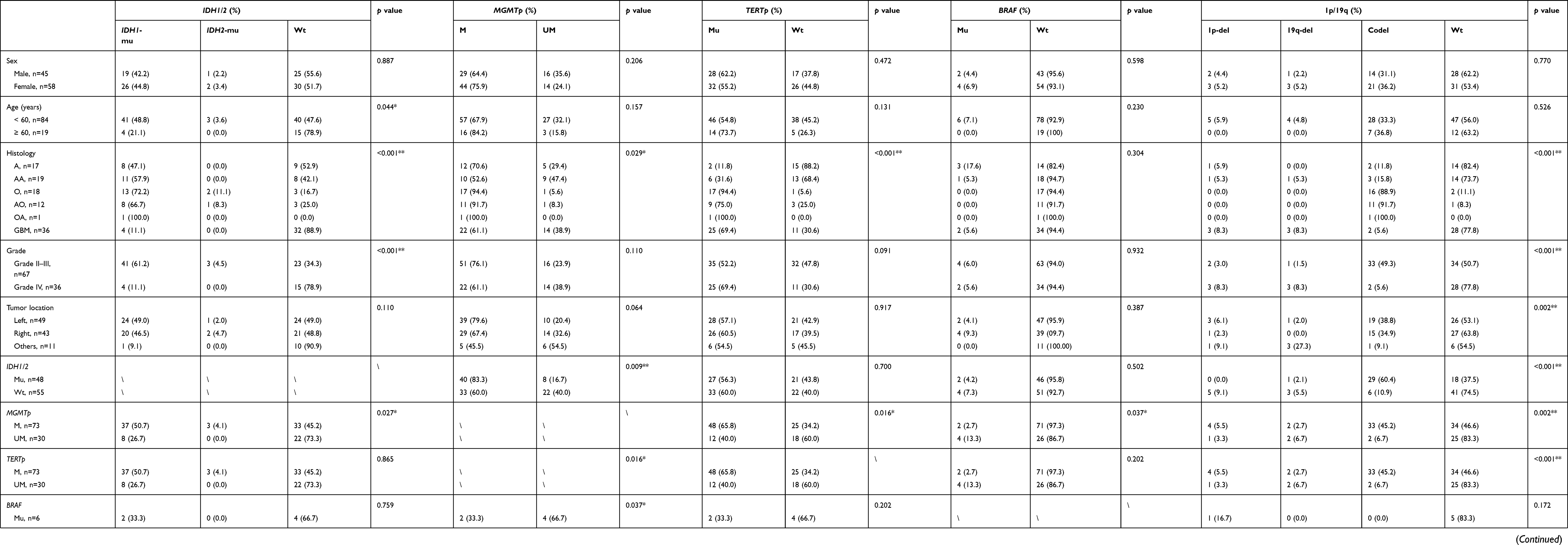 |
Table 1 Correlations Between Clinicopathological Characteristics and Alterations on IDH1/2, MGMTp, TERTp, BRAF, and 1p/19q in 103 Human Gliomas |
Of the 103 grade II–IV gliomas, there were no cases of quintuple-positive alterations (IDH-mu/BRAF-mu/TERTp-mu/MGMTp-M/1p/19q-codel). Meanwhile, 26 (25.2%), 3 (2.9%), 2 (1.9%), 1 (1.0%), and 12 (11.7%) cases showed IDH-mu/TERTp-mu/MGMTp-M/1p/19q-codel quadruple-positive alterations, TERTp-mu/MGMTp-M/1p/19q-codel triple-positive alterations, IDH-mu/MGMTp-M/1p/19q-codel triple-positive alterations, IDH-mu/TERTp-mu/1p/19q-codel triple-positive alterations, and IDH-mu/MGMTp-M double-positive alterations, respectively.
Characteristics of p53 and Ki-67 Expression in Gliomas
The immunoreactivity of Ki-67, but not p53, significantly increased with increased glioma grade (P < 0.001, Table 2). The percentage of TERTp-mu and 1p/19q-codel cases decreased with p53 immunoreactivity, while the frequencies of IDH-mu, MGMTp-M, and BRAF-mu cases were unrelated to p53 immunoreactivity. Comparatively, the percentage of IDH-mu and 1p/19q-codel cases decreased with Ki-67 immunoreactivity, whereas the percentages of MGMTp-M, TERTp-mu, and BRAF-mu cases showed no correlation to Ki-67 immunoreactivity.
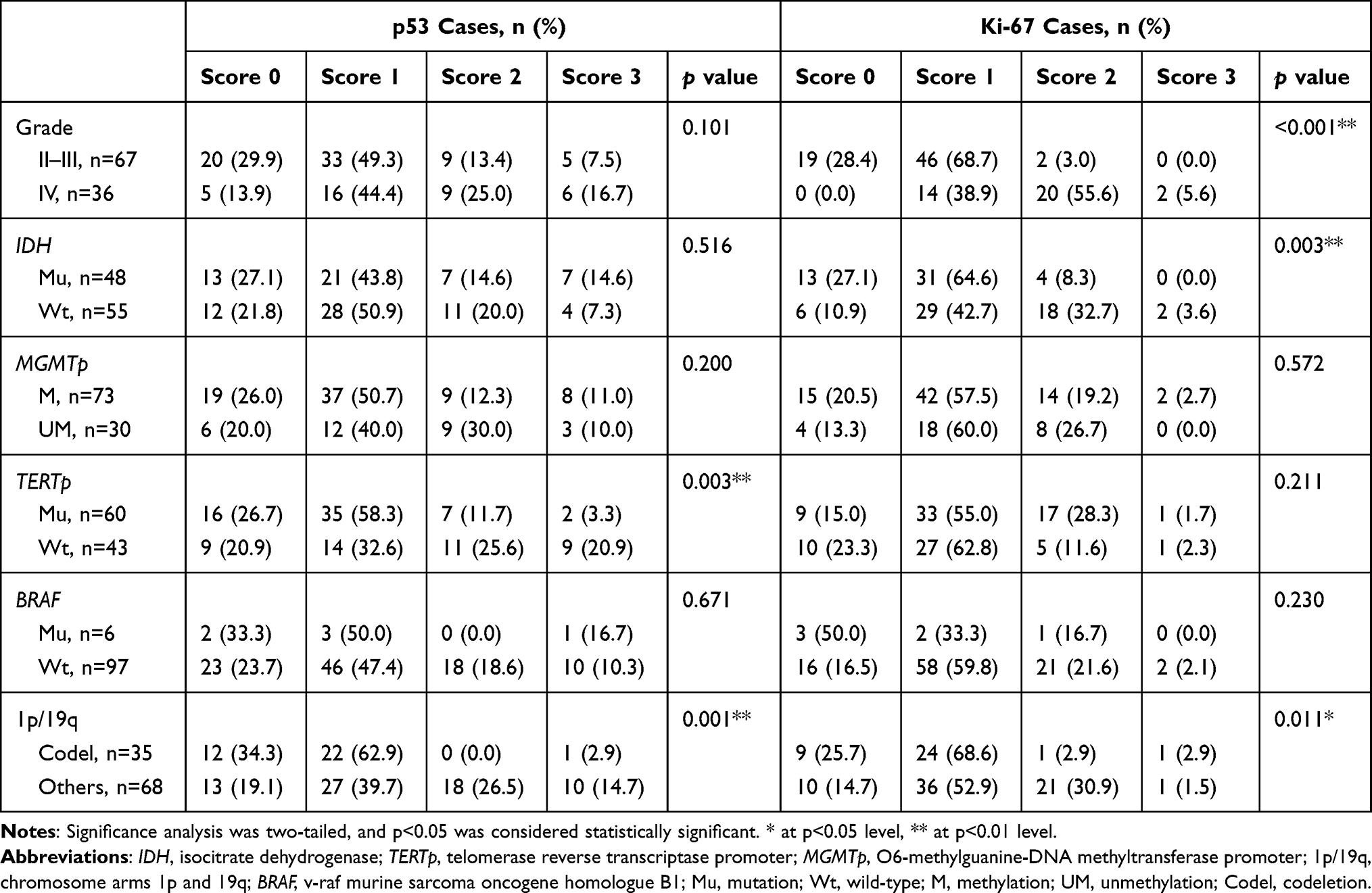 |
Table 2 Ki-67 and p53 Immunoreactivity in 103 Human Gliomas |
Relationship Between IDH-mu, TERTp-mu, MGMTp-M, 1p/19q-codel, and p53 and Ki-67 Expression with Survival Rate
Kaplan–Meier analysis showed that older patients (>60) and higher histological grade tumors had poorer OS (Figure 1A and B). For the molecular groups, patients with IDH-mu and 1p/19q-codel had significantly increased OS compared with IDH and 1p/19q wild-type patients (Figure 1D and F); OS was comparable between MGMTp-M and MGMTp-UM patients (median 18.0 vs 17.5 months) and between TERTp-mu and TERTp-wt patients (median 17.0 vs 27.0 months) (Figure 1C and E). For p53, OS was lower in p53 positive patients than in negative patients; but for Ki-67, OS was not significantly different between Ki-67 positive patients and negative patients (Figure 1G and H).
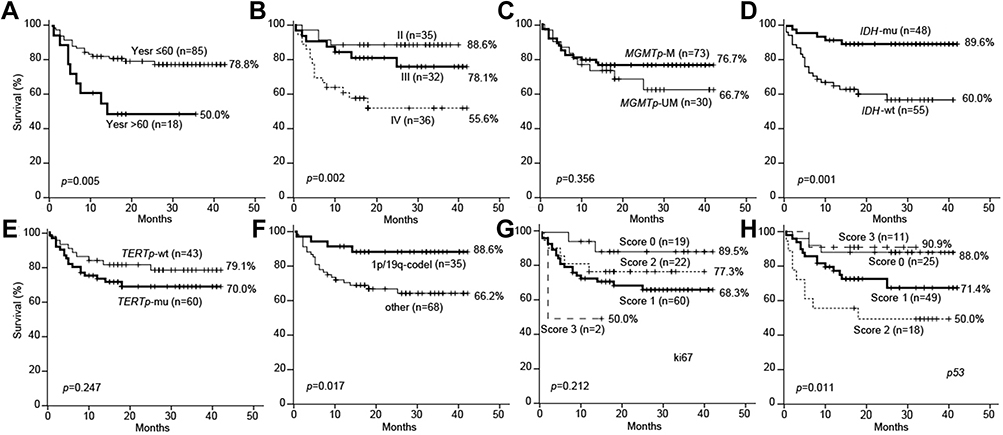 |
Figure 1 Prognostic values of patient age, histological grade, MGMT promoter methylation, IDH mutation, TERT promoter mutation, 1p/19q codeletion, and Ki-67 and p53 expressions by Kaplan–Meier Estimates of Overall Survival in 103 gliomas. Notes: Older age (>60 years) (A), higher histological grade (B), and overexpression Ki-67 (G) and p53 (H) predicted worse survival rates in glioma patients, while MGMT promoter methylation (MGMTp-M) (C), IDH mutation (IDH-mu) (D), TERT promoter mutation (TERTp-mu) (E), and 1p/19q codeletion (1p/19q-codel) (F) predicted better survival rates. Significance analysis was two-tailed, and p<0.05 was considered statistically significant.Abbreviations: IDH, isocitrate dehydrogenase;TERTp, telomerase reverse transcriptase promoter; MGMTp, O6-methylguanine-DNA methyltransferase promoter; 1p/19q-codel, chromosome arms 1p and 19q codeletion; BRAF, v-raf murine sarcoma oncogene homologue B1; Mu, mutation; Wt, wild-type; M, methylation; UM, unmethylation. |
Univariate analysis using the Cox regression model showed that old age, high histological grade, IDH-mu, 1p/19q-codel, and positive Ki-67 immunostaining were significantly correlated with OS (Table 3). We combined the two factors of p53 and Ki-67 in the univariate analysis and found that double positivity of p53 and Ki-67 (p53+/Ki-67+) was significantly correlated with OS. However, in the multivariate Cox-model analysis, none of the factors mentioned above except p53+/Ki-67+ was an independent prognostic factor for OS.
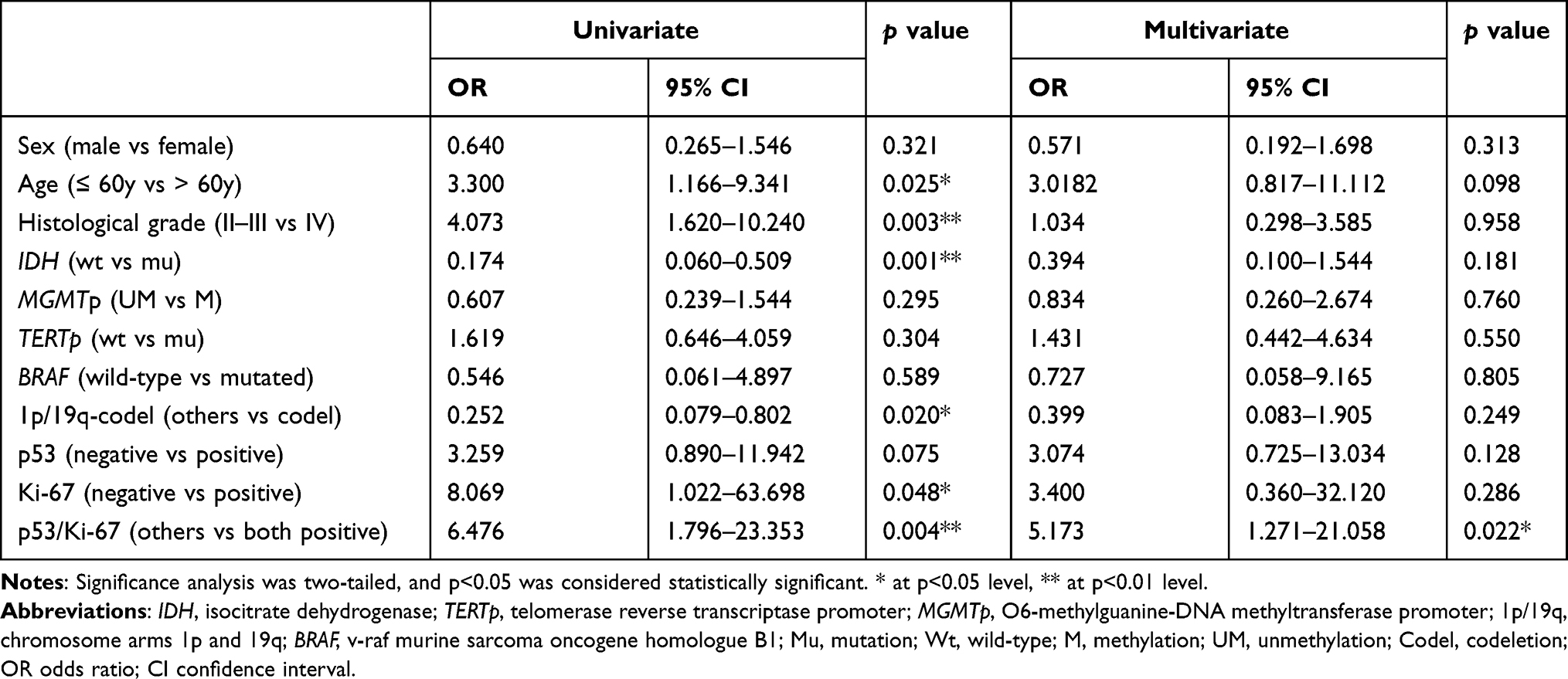 |
Table 3 Clinicopathological and Biological Factors Affecting Overall Survival Rates |
Prognostic Impact Analysis of Molecular Subgroups Stratified by MGMT Promoter Methylation, IDH Mutation, TERT Promoter Mutation, 1p/19q Codeletion, Ki-67, and p53 Expression, and Their Combination
In the combined analysis, quadruple positive (MGMTp-M/IDH-mu/TERTp-mu/1p/19q-codel) and Ki-67-/p53+ molecular groups showed the best prognosis for OS in the total 103 glioma cases (Figure 2A-C), while TERTp-mu only and Ki-67+/p53+ groups showed the worst OS. In grade II–III gliomas, Ki-67+/p53+ accounted for 52.2% of total cases. In contrast, in grade IV gliomas, Ki-67+/p53+ accounted for 86.1% of total cases, while the remaining 13.9% of cases were Ki-67+/p53− group. Patients with Ki-67+/p53+ gliomas showed the worst survival rates in both grade II–III and IV gliomas (Figure 2E and H); OS of the TERTp-mu only, MGMTp-M/TERTp-mu and quadruple negative (MGMTp-UM/IDH-wt/TERTp-wt/1p/19q-wt) groups was worse than that of the other groups (Figure 2C, F and I). Quadruple positive status was associated with a good OS no matter the Ki-67 or p53 status in grade II–III gliomas (Figure 2D). However, the quadruple positive group was absent in grade IV gliomas (Figure 2G), while IDH-mu was only was associated with a good prognosis for OS in both grade II–III and IV gliomas (Figure 2D and G). Out of the 36 grade IV gliomas, only four were IDH-mu (11.1%), thus failing to change the poor prognosis of GBMs.
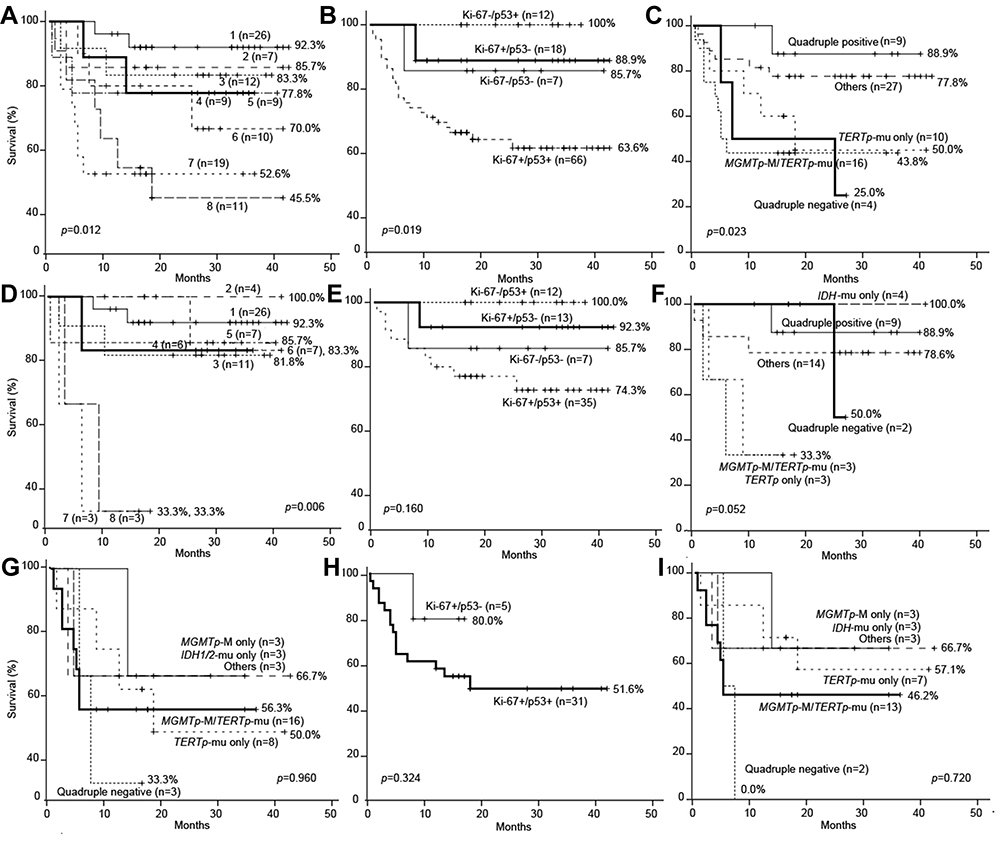 |
Figure 2 Kaplan–Meier estimates of overall survival in the glioma molecular groups. Abbreviations: IDH, isocitrate dehydrogenase; TERTp, telomerase reverse transcriptase promoter; MGMTp, O6-methylguanine-DNA methyltransferase promoter; 1p/19q-codel, chromosome arms 1p and 19q codeletion; BRAF, v-raf murine sarcoma oncogene homologue B1; Mu, mutation; Wt, wild-type; M, methylation; UM, unmethylation. Notes: Survival of the molecular subgroups stratified according to MGMT promoter methylation (MGMTp-M), IDH mutation (IDH-mu), TERT promoter mutation (TERTp-mu), and 1p/19q codeletion (1p/19q-codel) in atotal of 103 gliomas (A), comprising 67 grade II–III gliomas (D) and 36 grade IV gliomas (G). 1, quadruple positive (MGMTp-M/IDH-mu/TERTp-mu/1p/19q-codel); 2, IDH-mu only; 3, MGMTp-M/IDH-mu; 4, MGMTp-M only; 5, others; 6, quadruple negative (MGMTp-UM/IDH-wt/TERTp-wt/1p/19q-wt); 7, MGMTp-M/TERTp-mu; 8, TERTp-mu only. Survival of the subgroups stratified according to Ki-67 and p53 overexpression in a total of 103 gliomas (B), comprising 67 grade II–III gliomas (E) and 36 grade IV gliomas (H). Survival of the subgroups stratified according to MGMTp-M, IDH-mu, TERTp-mu, and 1p/19q-codel in a total of 66 Ki-67+/p53+ gliomas (C), comprising 35 Ki-67+/p53+ grade II–III gliomas (F) and 31 Ki-67+/p53+ grade IV gliomas (I). Significance analysis was two-tailed, and p<0.05 was considered statistically significant. |
Discussion
The present study investigated whether combined analysis of genetic alterations in IDH, BRAF, TERTp, MGMTp, and 1p/19q along with expression changes in p53 and Ki-67 protein is associated with the biological behaviors of gliomas. The results demonstrated significant associations of IDH-mu, BRAF-mu, TERTp-mu, MGMT-M, 1p/19q-codel, and p53 and Ki-67 expression with the survival rate of glioma patients.
Previous studies have reported that genetic alterations in IDH, BRAF, TERTp, MGMTp, and 1p/19q are associated with histological classification of gliomas.6,10,11 IDH-mu is present in 50–80% of WHO grade II–III gliomas and secondary GBM but is rare in primary GBM.13 Consistent with the reports of these studies, the present study identified 41 IDH1-mu and 3 IDH2-mu cases in 67 grade II–III gliomas, but only 4 IDH1-mu cases in 36 primary GBMs. No cases showed concurrent IDH1-mu and IDH2-mu, which could be because the two mutations are mutually exclusive.14 In contrast, we observed a high frequency of TERTp-mu and MGMTp-M in both grade II–III and IV gliomas, especially oligodendroglial gliomas, in accordance with previous reports. These findings suggest that TERTp mutation and MGMT methylation are typical molecular characteristics of these tumors.15–18 Concurrent loss of 1p/19q and IDH-mu has been used to define O tumors and resolve unclear diagnoses due to high interobserver discordance.7,19 The present study demonstrated that 1p/19q-codel is highly concentrated in oligodendrocyte-derived gliomas and strongly associated with IDH-mu in O tumors. However, 1 AO and 2 O cases were found with intact 1p/19q and MGMTp-M, confirming that parts of 1p/19q non-codeleted oligodendroglial gliomas were not astrocytic.20 Moreover, some cases showed conflicting results: two O cases showed IDH-wt/1p/19q-wt, but two A, three AA, and two GBM cases showed 1p/19q-codel, suggesting limitations of the existing molecular classification system for tumors with complex karyotypes.21
IDH1 mutation is a prognostic indicator of better survival in patients with diffuse gliomas grade II–IV tumors, with the exception of recurrent grade IV tumors.22 Similarly, we found that IDH-mu cases showed good prognosis for OS in both grade II–III and IV tumors, which was better than most other molecular subgroups. However, IDH-mu frequently appeared along with TERTp-mu/MGMTp-M/1p/19q-codel (54.2%) and MGMTp-M (25.0%) in IDH mutated cases. Thus, predicting OS according to IDH mutation only without considering other alterations may not be very reliable. Although TERTp-mu gliomas were associated with worse survival than TERTp-wt gliomas,6 patients with TERTp-mu/IDH-mu gliomas showed better survival than patients with one or none of these two mutations.8 In the present study, we did not predict the survival of the patient with TERTp-mu/IDH-mu glioma, as there was only one such case; however, we investigated whether TERTp-mu is associated with a poor prognosis in gliomas, similar to MGMTp-M/TERTp-mu. Interestingly, the occurrence of IDH-mu was significantly correlated with Ki-67 expression, but not with p53 expression, which is opposite to the finding of TERTp-mu, revealing that IDH and TERTp mutations may influence gliomagenesis through different oncogenic pathways. Ogura et al reported that p53 overexpression is associated with unfavorable outcomes in GBM/AA patients with IDH1-wt/MGMTp-UM gliomas,23 suggesting the combined profile of p53 and IDH and MGMTp status. However, we found that p53 positivity is not significantly correlated with survival in patients with IDH1-wt/MGMTp-UM gliomas, but that p53+/Ki-67+ predicts unfavorable outcomes in these patients. Thus, the combined assessment of IDH and MGMTp status with p53 and Ki-67 expression may be more useful for the prognosis of astrocyte-derived gliomas.
P53 expression was previously reported as a potential predictor of OS in glioma patients, but other studies reported contrasting findings.23,24 Our study demonstrated that patients with a stronger correlation between positive p53 expression and a worse prognosis than for patients with negative p53 expression. However, p53 expression was not an independent prognostic factor in neither univariate nor multivariate analysis. This finding may be because the cases with strong expression of p53 (p53, 3+) in this study had the highest percentage of IDH-mu (63.6%) but the lowest percentage of TERTp-mu (18.2%) compared to the other groups and thus achieved good OS due to IDH-mu status. Expression of p53 was not an independent prognostic factor for OS, indicating that further research is needed to determine the exact clinical value of p53. Ki-67 is another well-known cancer cell proliferation indicator, and its expression can reflect the proliferation and malignancy of glioma cells.4 In the present study, it was observed that most Ki-67+ glioma cases were high-grade and associated with poor OS. However, Ki-67+ was an independent prognostic factor only in the univariate analysis, not in the multivariate analysis. Although Ki-67 may be predictive of poor prognosis, using Ki-67 alone to predict survival in glioma patients may not be reliable.4,25 Instead, double positivity of Ki-67 and p53 (Ki-67+/p53+) was investigated as an independent prognostic factor for OS in both the univariate and multivariate analyses. Patients with Ki-67+/p53+ gliomas showed bad prognosis in terms of OS in both grade II–III and IV gliomas, suggesting the need to triage glioma patients based on the molecular status of Ki-67 and p53.
GBM is considered the deadliest primary brain tumor. It is characterized by high frequencies of MGMT and TERT promoter alterations and low frequencies of IDH and 1p/19q mutations in the primary tumor.26 Nevertheless, part of GBMs lack established genetic biomarkers, hence hard to classify into molecular subgroups and prognose OS for patients. For example, although TERTp and IDH mutations are clinically used to classify most of GBMs, about 20% of GBMs do not fit into this molecularly defined system and are designated IDH-wt/TERTp-wt GBM subgroups.27 In line with previous reports, we found 7 GBMs that were IDH-wt/TERTp-wt, of which 1 case had 1p/19q-codel, 3 cases had triple-negative (IDH-wt/TERTp-wt/1p/19q-wt), and the remaining cases had quadruple-negative (IDH-wt/TERTp-wt/MGMTp-UM/1p/19q-wt). Considering that the majority of GBMs were Ki-67+/p53+ and the rarity of BRAF-mu, Ki-67 and p53 expression and BRAF status is unlikely to aid in distinguishing TERTp/IDH/1p/19q wild-type GBMs from other gliomas. Furthermore, the TERTp/IDH/1p/19q wild-type GBMs cannot be distinguished from other genetic types of GBM by pathological images, highlighting the need to develop new markers to assist in defining subgroup of TERTp/IDH/1p/19q wild-type GBMs.
In conclusion, our findings confirmed existence of complex correlations among TERTp and IDH mutations, MGMTp-M, 1p/19q-codel, and expression of p53 and Ki-67 in human gliomas. BRAF mutation was uncommon in adult astrocytic and oligodendroglial gliomas. IDH-mu only and quadruple-positivity (IDH-mu/TERTp-mu/MGMTp-M/1p/19q-codel) predicted good prognosis for OS in gliomas; TERTp-mu only, TERTp-mu/MGMTp-M and quadruple-negativity predicted poor prognosis, especially in grade II–III gliomas. Ki-67/p53 was an independent prognostic factor for OS, as double positivity predicted poor prognosis in both II–III and IV gliomas. Thus, combing these genome alterations and Ki-67/p53 expression should have clinical value in the diagnosis and prognosis of glioma tumors.
Abbreviations
IDH, isocitrate dehydrogenase; TERTp, telomerase reverse transcriptase promoter; MGMTp, O6-methylguanine-DNA methyltransferase promoter; 1p/19q, chromosome arms 1p and 19q; BRAF, v-raf murine sarcoma oncogene homologue B1; Mu, mutation; Wt, wild-type; M, methylation; UM, unmethylation; 1p-del, 1p-deletion; 19q-del, 19q-deletion; Codel, codeletion; A, astrocytoma; AA, anaplastic astrocytoma; AO, anaplastic oligodendroglioma; AOA, anaplastic oligoastrocytoma; O, oligodendroglioma; OA, oligoastrocytoma; GM, glioblastoma; OS, overall survival.
Acknowledgments
This study was supported by two joint research projects of Southwest Medical University and Luzhou city (2017LZXNYD-J14 and 2018LZXNYD-ZK22), Natural Science Foundation of Southwest Medical University (2019ZQN070), as well as the doctoral research initiation fund of the Affiliated Hospital of Southwest Medical University (no. 16238).
Author Contributions
All authors contributed to data analysis, drafting, or revising the article. All authors gave final approval of the manuscript to be published, agreed to the submitted journal, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Labreche K, Kinnersley B, Berzero G, et al. Diffuse gliomas classified by 1p/19q co-deletion, TERT promoter and IDH mutation status are associated with specific genetic risk loci. Acta Neuropathol. 2018;135(5):743–755.
2. Pienkowski T, Kowalczyk T, Kretowski A, Ciborowski M. A review of gliomas-related proteins. Characteristics of potential biomarkers. Am J Cancer Res. 2021;11(7):3425–3444.
3. van den Bent MJ. Interobserver variation of the histopathological diagnosis in clinical trials on glioma: a clinician’s perspective. Acta Neuropathol. 2010;120(3):297–304.
4. Chen WJ, He DS, Tang RX, Ren FH, Chen G. Ki-67 is a valuable prognostic factor in gliomas: evidence from a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2015;16(2):411–420.
5. Jin Y, Xiao W, Song T, Feng G, Dai Z. Expression and prognostic significance of p53 in glioma patients: a meta-analysis. Neurochem Res. 2016;41(7):1723–1731.
6. Eckel-Passow JE, Lachance DH, Molinaro AM, et al. Glioma groups based on 1p/19q, IDH, and TERT promoter mutations in tumors. N Engl J Med. 2015;372(26):2499–2508.
7. Ammendola S, Caldonazzi N, Simbolo M, et al. H3K27me3 immunostaining is diagnostic and prognostic in diffuse gliomas with oligodendroglial or mixed oligoastrocytic morphology. Virchows Arch. 2021. doi:10.1007/s00428-021-03134-1
8. Vuong HG, Altibi AMA, Duong UNP, et al. TERT promoter mutation and its interaction with IDH mutations in glioma: combined TERT promoter and IDH mutations stratifies lower-grade glioma into distinct survival subgroups-A meta-analysis of aggregate data. Crit Rev Oncol Hematol. 2017;120:1–9.
9. Killela PJ, Pirozzi CJ, Healy P, et al. Mutations in IDH1, IDH2, and in the TERT promoter define clinically distinct subgroups of adult malignant gliomas. Oncotarget. 2014;5(6):1515–1525.
10. Schulze Heuling E, Knab F, Radke J, et al. prognostic relevance of tumor purity and interaction with MGMT methylation in glioblastoma. Mol Cancer Res. 2017;15(5):532–540.
11. Galbraith K, Snuderl M. Molecular pathology of gliomas. Surg Pathol Clin. 2021;14(3):379–386.
12. Hu X, Miao W, Zou Y, Zhang W, Zhang Y, Liu H. Expression of p53, epidermal growth factor receptor, Ki-67 and O6-methylguanine-DNA methyltransferase in human gliomas. Oncol Lett. 2013;6(1):130–134.
13. Ichimura K, Pearson DM, Kocialkowski S, et al. IDH1 mutations are present in the majority of common adult gliomas but rare in primary glioblastomas. Neuro Oncol. 2009;11(4):341–347.
14. Hartmann C, Meyer J, Balss J, et al. Type and frequency of IDH1 and IDH2 mutations are related to astrocytic and oligodendroglial differentiation and age: a study of 1010 diffuse gliomas. Acta Neuropathol. 2009;118(4):469–474.
15. Labussière M, Di Stefano AL, Gleize V, et al. TERT promoter mutations in gliomas, genetic associations and clinico-pathological correlations. Br J Cancer. 2014;111(10):2024–2032.
16. Weller M, Stupp R, Reifenberger G, et al. MGMT promoter methylation in malignant gliomas: ready for personalized medicine? Nat Rev Neurol. 2010;6(1):39–51.
17. Yang P, Cai J, Yan W, et al. Classification based on mutations of TERT promoter and IDH characterizes subtypes in grade II/III gliomas. Neuro Oncol. 2016;18(8):1099–1108.
18. Wesseling P, van den Bent M, Perry A. Oligodendroglioma: pathology, molecular mechanisms and markers. Acta Neuropathol. 2015;129(6):809–827.
19. Yao J, Hagiwara A, Raymond C, et al. Human IDH mutant 1p/19q co-deleted gliomas have low tumor acidity as evidenced by molecular MRI and PET: a retrospective study. Sci Rep. 2020;10(1):11922.
20. Li YX, Shi Z, Aibaidula A, et al. Not all 1p/19q non-codeleted oligodendroglial tumors are astrocytic. Oncotarget. 2016;7(40):64615–64630.
21. Ballester LY, Huse JT, Tang G, Fuller GN. Molecular classification of adult diffuse gliomas: conflicting IDH1/IDH2, ATRX, and 1p/19q results. Hum Pathol. 2017;69:15–22.
22. Tabei Y, Kobayashi K, Saito K, et al. Survival in patients with glioblastoma at a first progression does not correlate with isocitrate dehydrogenase (IDH)1 gene mutation status. Jpn J Clin Oncol. 2021;51(1):45–53.
23. Ogura R, Tsukamoto Y, Natsumeda M, et al. Immunohistochemical profiles of IDH1, MGMT and P53: practical significance for prognostication of patients with diffuse gliomas. Neuropathology. 2015;35(4):324–335.
24. Levidou G, El-Habr E, Saetta AA, et al. P53 immunoexpression as a prognostic marker for human astrocytomas: a meta-analysis and review of the literature. J Neuro-Oncol. 2010;100(3):363–371.
25. Alkhaibary A, Alassiri AH, AlSufiani F, Alharbi MA. Ki-67 labeling index in glioblastoma; does it really matter? Hematol Oncol Stem Cell Ther. 2019;12(2):82–88.
26. Thakkar JP, Dolecek TA, Horbinski C, et al. Epidemiologic and molecular prognostic review of glioblastoma. Cancer Epidemiol Biomarkers Prev. 2014;23(10):1985–1996.
27. Diplas BH, He X, Brosnan-Cashman JA, et al. The genomic landscape of TERT promoter wildtype-IDH wildtype glioblastoma. Nat Commun. 2018;9(1):2087.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.