")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Clinical and Metabolic Characteristics of Non-Alcoholic Fatty Liver Disease Patients in Saudi Arabia: Data from the Systematic Observatory Liver Disease (SOLID) Registry
Authors Alswat K , Sanai FM, Al-hamoudi W, Ismail M , Dahlan Y, AlGhamdi HS, Altraif I, Alalwan A, Babatin MMA, Alqahtani SA
Received 1 January 2021
Accepted for publication 23 February 2021
Published 16 March 2021 Volume 2021:14 Pages 1167—1175
DOI https://doi.org/10.2147/DMSO.S300051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Khalid Alswat,1 Faisal M Sanai,2 Waleed Al-hamoudi,1 Mona Ismail,3 Yaser Dahlan,2 Hamdan Saleh AlGhamdi,4,5 Ibrahim Altraif,4,5 Abduljaleel Alalwan,4,5 Mohamed MA Babatin,6 Saleh A Alqahtani7,8
1Liver Disease Research Center, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Gastroenterology Unit, Department of Medicine, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 3Division of Gastroenterology, Department of Internal Medicine, King Fahd Hospital of the University, College of Medicine, Imam Abdulrahman Bin Faisal University, Al-Khobar, Saudi Arabia; 4King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 5Hepatology Division, Department of Hepatobiliary Sciences and Organs Transplant Center, King Abdulaziz Medical City of National Guard, Riyadh, Saudi Arabia; 6Gastroenterology Unit, Department of Medicine, King Fahad Hospital, Jeddah, Saudi Arabia; 7Liver Transplant Center, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia; 8Division of Gastroenterology and Hepatology, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Khalid Alswat
Liver Disease Research Center, Department of Medicine, College of Medicine, King Saud University, P.O. Box 2925(59), Riyadh, 11461, Saudi Arabia
Tel +966114670810
Fax +966114672403
Email [email protected]
Background and Aims: The prevalence of non-alcoholic fatty liver disease (NAFLD) is increasing in Saudi Arabia (SA), but descriptions of the clinical and metabolic characteristics of these patients are limited. The present study aims to fill this gap.
Methods: Demographic, clinical, and laboratory data of all NAFLD patients from 2009 to 2019 were retrieved from the Systematic Observatory Liver Disease Registry (SOLID) [n=832 (337 males; 495 females); mean (± standard deviation, SD) age was 42.6± 13.6 years; mean body mass index (BMI) was 35.0± 9.3kg/m2]. Non-invasive surrogate scores of fibrosis (eg AST to Platelet Ratio Index (APRI), Fibrosis-4 (FIB-4), and NAFLD fibrosis (NFS) scores) were calculated and analyzed. In addition, data from NAFLD patients with normal and high alanine aminotransferase (ALT) were compared using two different methods: the standard laboratory reference range which defines normal as ALT< 61 IU/L, and the range proposed by a recent national study which sets upper limits of normal ALT at 33 IU/l for men and 22 IU/l for women.
Results: Hyperlipidemia was the most common comorbidity (41.7%), followed by type 2 diabetes mellitus (T2DM) (35.3%) and hypertension (28.4%). Prevalence of advanced fibrosis varied widely across definitions [FIB-4, N=19 (2.5%); APRI, N=21 (2.8%); NFS, N=62 (8.6%)] and exhibited sexual dimorphism with males having worse metabolic characteristics. NAFLD patients with normal ALT were more likely to be older, female, have a lower BMI, and have a higher prevalence of cirrhosis, DM, hypertension, hyperlipidemia, and renal dysfunction.
Conclusion: Patients with NAFLD have metabolic characteristics associated with several comorbidities, including NAFLD patients with normal ALT. Mechanistic studies are needed to examine and analyze complex, interactive effects between sex, age, and other factors that may accelerate NAFLD disease progression.
Keywords: non-alcoholic fatty liver disease, non-invasive biomarkers of fibrosis, Systematic Observatory Liver Disease Registry, Saudi Arabia
Introduction
Non-alcoholic fatty liver disease (NAFLD) is defined as the accumulation of excess fat in the liver among individuals who consume little or no alcohol.1,2 In particular, NAFLD is the deposition of fat in the liver exceeding 5% of hepatocytes, as well as the presence of progressive steatosis with associated pathology (ie hepatitis, cirrhosis, or hepatocellular carcinoma [HCC]). NAFLD patients can exhibit a wide spectrum of histological manifestations, such as simple steatosis, nonalcoholic fatty liver (NAFL), or nonalcoholic steatohepatitis (NASH).3
Worldwide, the prevalence of NAFLD is 25%, affecting nearly 1 billion individuals.4,5 Globally, the prevalence of NAFLD has steadily increased from 15% in 2005 to 25% in 2010.6 The steady and rapid increase in the prevalence of NAFLD has been attributed to the increased adoption of Westernized lifestyles, with the disease projected to be the leading cause of liver failure in the near future.7 While cirrhosis and HCC can lead to liver-related morbidity and mortality, NAFLD also increases the risk of cardiovascular diseases, type 2 diabetes mellitus (T2DM), and chronic kidney disease.8
Associations between metabolic diseases and NAFLD are bi-directional: NAFLD is a risk factor for metabolic diseases (ie central obesity, T2DM, dyslipidemia, and insulin resistance) and metabolic diseases are risk factors for NAFLD.9 Furthermore, obesity increases the odds of NAFLD-related complications.10 Interestingly, NAFLD can also be found in non-obese patients. These patients usually present with unique clinical characteristics, such as higher levels of transaminases and insulin, as well as a lower degree of insulin sensitivity.11 Without early diagnosis or proper management, NAFLD can progress and cause patients to suffer from advanced hepatic complications (eg fibrosis, cirrhosis, or HCC), which in turn leads to larger economic and clinical burdens on patients and health care systems.
The Middle East and North Africa (MENA) region has the highest prevalence of NAFLD in the world.12 Rapid industrialization, socioeconomic improvements, and the increased adoption of Westernized diets, particularly in Saudi Arabia (SA), have negatively impacted public health. Obesity and T2DM, which are major risk factors for NAFLD, are exceptionally common in SA,13,14 with T2DM alone accounting for as much as a third of the Ministry of Health’s annual budget expenditures.15 Undoubtedly, the aforementioned risk factors contribute to the high prevalence of NAFLD in SA, with models estimating that the prevalence of NAFLD will increase to 32% by 2030.16
Early diagnosis, monitoring, and management of NAFLD are critically important to ensure that newly diagnosed and high-risk patients receive appropriate treatment (eg anti-obesity medications or bariatric surgery, adoption of lifestyle modifications, and other weight reduction strategies).17 However, guidelines for the diagnosis and management of NAFLD patients vary between medical associations, possibly due to ethnic differences in clinical characteristics, lifestyles, and genetic backgrounds across populations.18 Despite the high prevalence of NAFLD in SA, the clinical and metabolic characteristics of NAFLD patients have not been well characterized. Empirical data that fills this knowledge gap would be advantageous for physicians who routinely diagnose, and provide care and treatment to NAFLD patients. Therefore, the purpose of this study was to identify clinical and metabolic characteristics of NAFLD patients in SA.
Methods
Study Design and Participants
Demographic, clinical, and laboratory data on all registered adult (>18 years old) NAFLD patients from multiple centers in SA between 2009 and 2019 were collected in the Systematic Observatory Liver Disease Registry (SOLID). SOLID is a multicenter, observational registry that collects clinical, biochemical, radiological, and other medical data on SA residents with liver disease. To be labelled as a NAFLD patient in the SOLID registry, the individual should have been diagnosed with fatty liver based on liver ultrasound scan or had a biopsy with fat >5%, excluding secondary causes such as viral hepatitis, autoimmune liver disease, and daily alcohol consumption >30 g for men and >20 g for women. The majority of patients included in SOLID are recruited from the following medical centers in the country: King Saud University Medical City (KSUMC) in Riyadh, King Abdulaziz Medical City (KAMC) in Jeddah and Riyadh, King Fahd Hospital (KFH) of the University in Al Khobar and KFH in Jeddah.
This study was approved by Institutional Review Board (Approval Number: E20-5163), and informed consent was obtained from all patients prior to study enrollment. The data accessed from the SOLID Registry complied with relevant data protection and privacy regulations.
Outcomes of Interest
Primary outcomes of interest were clinical and metabolic characteristics of NAFLD patients. Secondary outcomes included metabolic differences according to sex and ALT levels. We compared groups based on two different methods for evaluating ALT levels: the standard laboratory reference range which defines normal as ALT<61 IU/L, and the range proposed by a recent national study which sets upper limits of normal ALT at 33 IU/l for men and 22 IU/l for women.19 In addition, we assessed differences in non-invasive biomarkers of fibrosis (eg AST to Platelet Ratio Index (APRI), Fibrosis-4 (FIB-4), and NAFLD fibrosis (NFS) scores).
Demographics and Clinical Characteristics
Demographic and clinical characteristics of NAFLD patients were retrieved from the database (ie age, sex, body mass index (BMI), diagnostic site [eg diagnosed in an outpatient clinic, during or after bariatric surgery or elective cholecystectomy]) along with the presence of the following comorbidities: cirrhosis, diabetes mellitus, hypertension, hyperlipidemia, and renal dysfunction.
Laboratory Values
The following laboratory values were included: ALT, aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), albumin, bilirubin, hemoglobin, international normalized ratio (INR), prothrombin time (PT), platelets, alpha-fetoprotein (AFP), glycated hemoglobin (HbA1c), cholesterol, triglycerides, low-density lipoprotein (LDL), high-density lipoprotein (HDL), creatinine, and thyroid-stimulating hormone (TSH).
Non-Invasive Biomarkers of Fibrosis
Age and other laboratory values extracted from the database were used to calculate APRI, FIB-4, and NFS scores at the time of diagnosis. Formulas that were used to calculate these respective non-invasive biomarkers of fibrosis can be found elsewhere.20–22
Statistical Analysis
Data were analyzed using SPSS version 21.5 (IBM, Chicago, IL, USA). Data were presented as mean ± standard deviation (SD) for continuous variables and frequencies (percentages, %) for categorical variables. The independent samples T-test and chi-square were used to compare means and frequencies between patient groups, respectively. The Mann–Whitney U-test was used for non-normally distributed continuous variables. Figures were plotted in MS Excel. Significance was set at p<0.05.
Results
Clinical and Metabolic Characteristics: Effects of Gender
The majority of NAFLD patients were diagnosed in outpatient clinics (51.9%), while the remainder were diagnosed after an elective cholecystectomy (25.1%) or bariatric surgery (23.0%). The mean age was 42.6 ± 13.6 years and the mean BMI was 35.0 ± 9.3 kg/m2. Hyperlipidemia was the most common comorbid metabolic abnormality (41.7%), followed by T2DM (35.3%), and hypertension (28.4%) (Table 1).
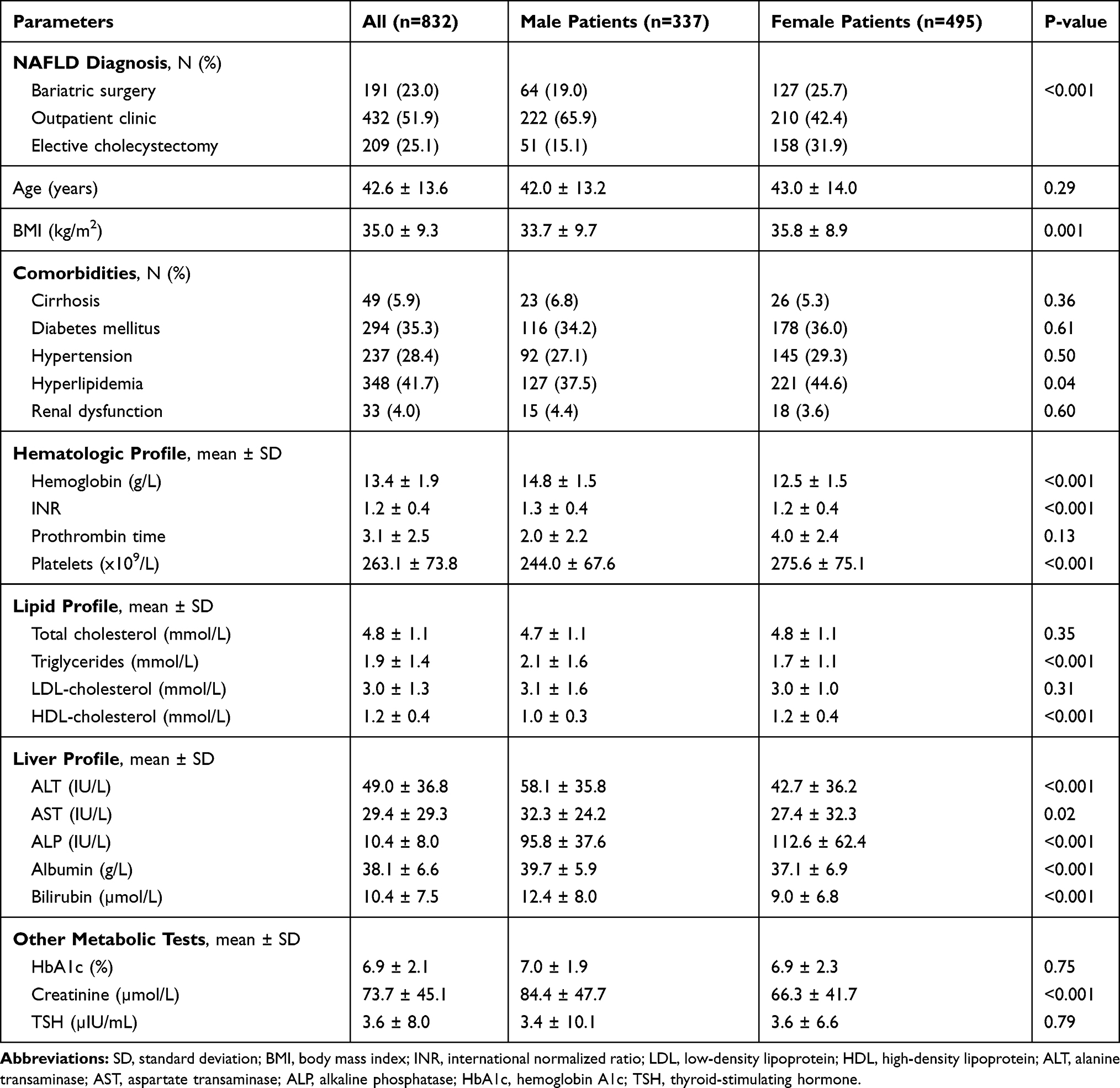 |
Table 1 Bivariate Comparisons of Male and Female NAFLD Patients on Clinical and Metabolic Characteristics |
Female patients were more common than males. No statistical differences were observed between genders for age, prevalence of cirrhosis, T2DM, hypertension, and renal dysfunction. Female patients had significantly higher BMI (p=0.001) and were more likely to have hyperlipidemia (p=0.04) than males. Compared to female patients, male patients had significantly higher levels of ALT, AST, albumin, bilirubin, INR, triglycerides, and creatinine. On the other hand, female patients had significantly higher platelet counts, HDL-cholesterol, and ALP than males (Table 1).
Patients who were diagnosed with NAFLD in outpatient clinics had the highest prevalence of cirrhosis (10.6%), T2DM (52.3%), hypertension (38.7%), and hyperlipidemia (50.9%) (Figure 1). Levels of ALT between groups were not statistically different.
 |
Figure 1 Prevalence of comorbidities among NAFLD patients according to site of diagnosis. |
Effects of Gender on Non-Invasive Biomarkers of Fibrosis
Mean FIB-4, APRI, and NFS cores were 0.8 ± 1.0, 0.4 ± 0.6, and −1.7 ± 1.8, respectively (Table 2). The prevalence of advanced fibrosis ranged from 2.5% to 8.6%. Male patients had significantly higher FIB-4 (0.9 ± 1.2 vs 0.8 ± 0.8, p=0.02) and APRI scores (0.4 ± 0.5 vs 0.35 ± 0.6, p=0.03) than females. Female patients were more likely to have low APRI scores (84.9% vs 76.1%, p=0.007). No gender differences were seen in NFS scores.
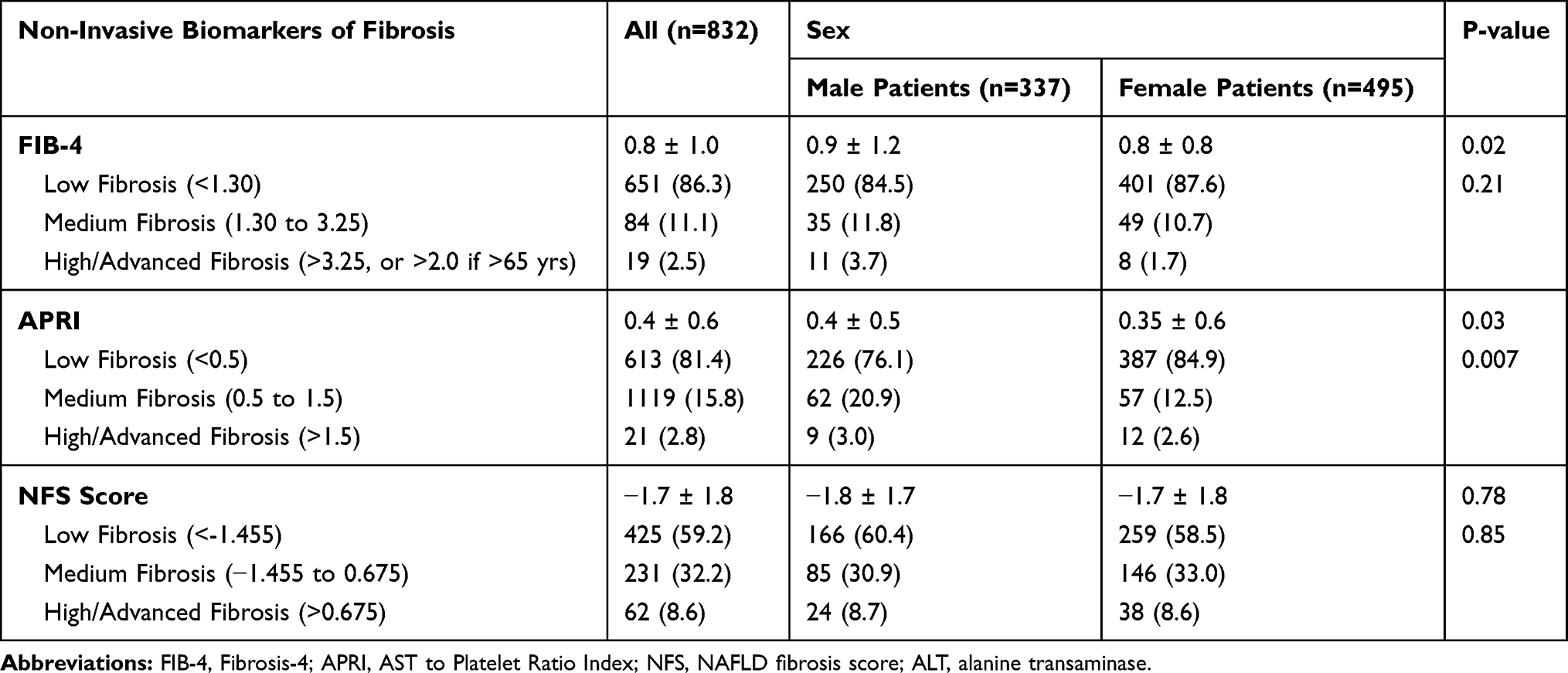 |
Table 2 Bivariate Comparisons of Male and Female NAFLD Patients on Non-Invasive Biomarkers of Fibrosis |
Clinical and Metabolic Characteristics of NAFLD Patients with Normal ALT
The prevalence of elevated ALT levels among NAFLD patients was only 25% when using the standard laboratory reference range. However, using the lower cut-off values suggested by a recent national study resulted in a higher proportion of patients with elevated ALT (77.5%).
Compared to patients with elevated ALT levels (based on the standard laboratory reference range for ALT), those with normal ALT levels were significantly older, had higher BMI, and higher levels of HDL-cholesterol. Patients with elevated ALT levels were more likely to be male and to have a significantly higher prevalence of hyperlipidemia (total cholesterol, LDL-cholesterol), and significantly higher levels of hemoglobin, AST, ALP, albumin, and bilirubin than the group with normal ALT levels (Table 3).
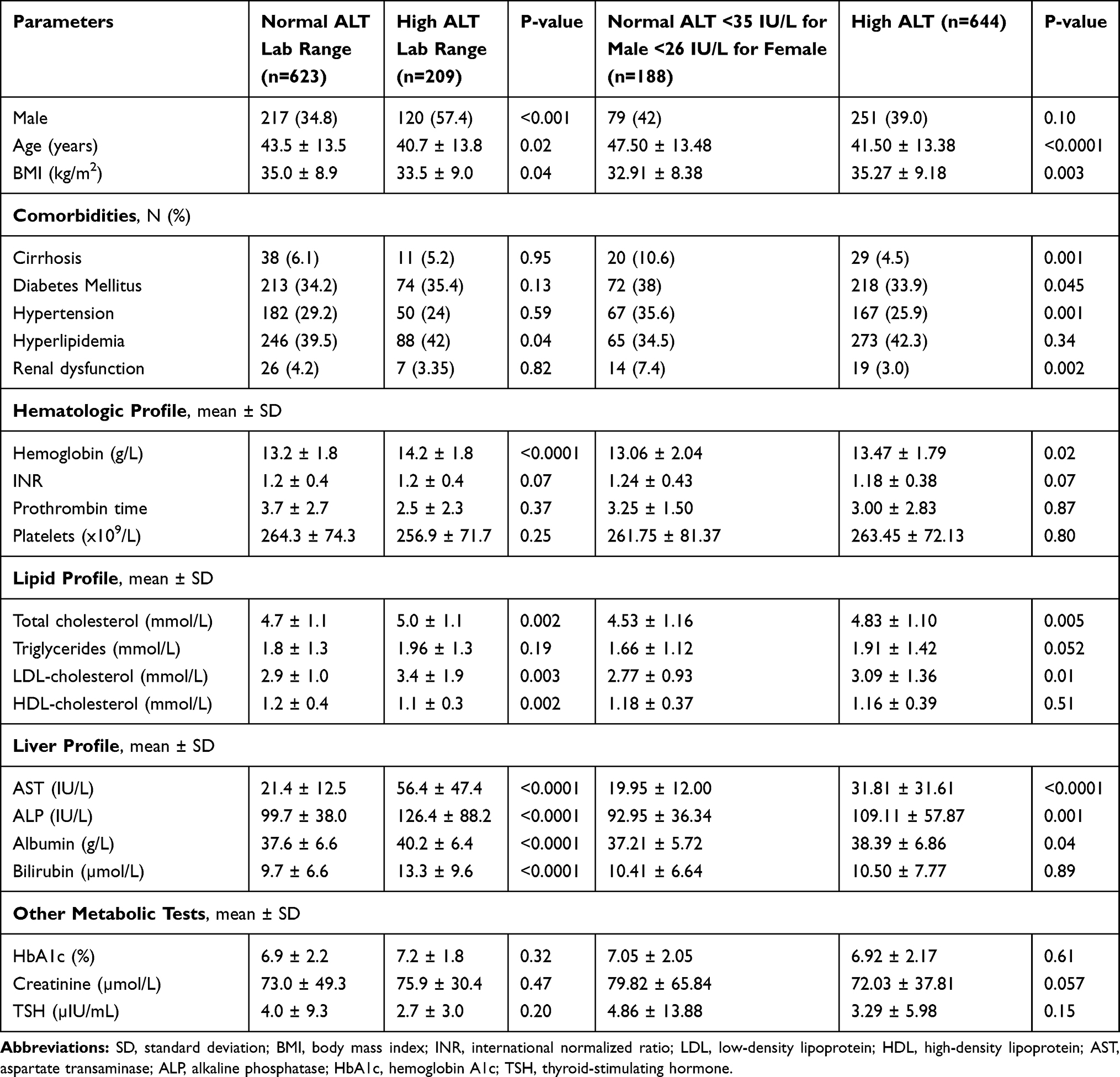 |
Table 3 Bivariate Comparisons of NAFLD Patients with Normal and High ALT on Clinical and Metabolic Characteristics |
However, when comparisons were made using the newly proposed national range, more differences were observed; patients with normal ALT were more likely to be older, female, and have lower BMI. They also had a higher prevalence of cirrhosis, DM, hypertension, hyperlipidemia, and renal dysfunction. They had lower lipid profile levels, AST, ALP, and albumin (Table 3).
Discussion
The present study is arguably the largest clinical cohort study to detail the clinical and metabolic characteristics of patients with NAFLD in SA. Patients were enrolled during outpatient visits and after elective surgery, allowing for a selected and well-characterized cohort that represents patients seeking medical care. Notable results include the high prevalence of metabolic comorbidities including hyperlipidemia, T2DM, hypertension, and elevated ALT levels. These findings are consistent with one of the earliest single-center studies conducted in SA that assessed the epidemiological, clinical, and biochemical characteristics of NAFLD patients.23 In the prospective study conducted by Al-Hamoudi and colleagues, diabetes (34.2%), hyperlipidemia (29.7%), and hypertension (26.7%) were the most frequent comorbidities among NAFLD patients, and prevalence estimates of elevated ALT levels among NAFLD patients were identical to the findings of the current study when using the lab reference values.23 The current study also replicates the prevalence of NAFLD found among published cohorts in other international studies that examined biopsy-proven NASH,6,24 highlighting that similar metabolic risk profiles exist in non-Saudi and Saudi patients.
With regard to sexual differences, although female patients accounted for the majority of NAFLD cases in the current study, male patients had more pronounced hematologic and liver profile abnormalities, as well as higher FIB-4 and APRI scores suggestive of a higher prevalence of advanced hepatic fibrosis. In the literature, a higher prevalence of NAFLD and more advanced disease stages have been described in male patients.25,26 These gender differences are however lost in post-menopausal women, highlighting age as an important factor for sex-related differences in NAFLD. The molecular mechanisms that underpin these gender disparities are not fully understood, but several theories have been proposed.27 Differences in how men and women store fat have been implicated: women tend to store more fat subcutaneously, and men have more visceral fat compared to women with similar body fat levels.28,29 Visceral fat releases excess free fatty acids into the portal vein, and more of this type of fat exacerbates the metabolic strain on the liver.30 Estrogen appears to be another key player behind these sex-specific differences.31 Estrogen is protective against the development and progression of NAFLD, possibly by preventing the development of hypercholesterolemia and anti-inflammatory effects.31–33 Consequently, men and post-menopausal women are more susceptible to liver damage, which is consistent with the generally higher ALT values reported herein and in similar studies.34 Insulin resistance is also closely associated with the development of NAFLD.35 Males are more prone to develop insulin resistance,36,37 and this has been postulated as another potential explanation for sexual dimorphism in NAFLD. While a full understanding of the pathogenesis of NAFLD has not yet been achieved, it is clear that NAFLD disease progression is quite complex, and that NALFD affects men and women differently. As such, iterative studies are encouraged to go beyond dichotomous sex comparisons and to consider close examination and analysis of complex, interactive effects between sex, age, and hormonal status that may accelerate NAFLD disease progression and severity. Findings from such studies could increase the potential for effective precision medicine for NAFLD, which in turn will likely reduce the development of cirrhosis and HCC, and improve survival in NAFLD patients. Moving forward, prospective studies exploring a balanced male and female population will be needed to define potential sex-specific differences in the prevalence and disease severity of NAFLD in SA.
An important finding in the current study was the low prevalence of advanced fibrosis among NAFLD patients according to surrogate scores of hepatic fibrosis. Overall, 2.5%, 2.8%, and 8.6% of participants exhibited high FIB-4, APRI, and NFS scores, respectively. These are in contrast to studies conducted elsewhere, where the prevalence of advanced fibrosis among NAFLD patients ranged from 20% to 30%.38,39 A meta-analysis reported that approximately 14.5% of NAFLD patients have advanced fibrosis at baseline or at the time of diagnosis. At follow-up, 34.5% of the entire sample of NAFLD patients developed progressive fibrosis, 38.8% remained stable, and 26.7% achieved fibrosis regression. Unlike that meta-analysis or studies included in that meta-analysis, the current study was cross-sectional and did not prospectively follow fibrosis outcomes in NAFLD patients. However, additional studies that analyze fibrosis over time in Saudi NAFLD patients are needed. Nonetheless, several studies have demonstrated that one-third to one-half of NAFLD patients eventually progress to advanced stages of fibrosis.40–42 More studies are needed to identify factors that inhibit and that hasten fibrosis progression and regression, and additional studies are needed to examine monitoring protocols that most optimally minimize the onset of fibrosis progression.
Another observation from the current study was the difference between normal and high ALT levels in NAFLD patients. ALT is a marker of liver inflammation, yet there is no optimal cut-off level to predict NASH and fibrosis.43 In a recent systematic review of 11 studies with 4084 patients, 25% of NAFLD patients and 19% of NASH patients had normal ALT values.44 In our study, we have a high proportion of NAFLD patients with normal ALT (75%). However, by using the lower reference range proposed by a recent national study (<35 IU/L for males and <26 IU/L for females),19 we found a higher proportion of patients with elevated ALT levels comparable to many international studies.
Compared to patients with elevated ALT levels, we found that patients with normal ALT levels were older, which is consistent with previous studies.45,46 In addition, we observed that normal ALT levels were more common in females than males, which is consistent with the findings from a meta-analysis conducted by Ma.44 In this meta-analysis, NAFLD patients with normal ALT values were more likely to be affected by diabetes, hypertension, and metabolic syndrome, which is consistent with our findings using the lower cut-offs for ALT. These differences are not consistent with all studies. Uslusoy et al demonstrated no significant difference between the clinical characteristics of patients with elevated ALT and normal ALT values.46
The current analysis has notable limitations and strengths. Causality cannot be inferred given the cross-sectional nature of the study. Findings cannot be generalized to children and adolescents in SA, as the study only included adults. Future studies should aim to include and characterize NAFLD among children and adolescents in SA. We could not differentiate NASH from non-NASH disease, as this cohort lacked biopsy data for many patients. Nonetheless, we used non-invasive surrogate scores to define the prevalence of advanced fibrosis. This study has important implications as it included patients from multiple centers in SA. To the best of our knowledge, this is the largest analysis of patients with NAFLD in SA and the entire Middle East region.
In summary, the present study adds to the growing body of literature on NAFLD, including the growing body of literature that suggests men are more severely affected by NAFLD than women. Mechanistic studies are needed to more fully understand NAFLD pathogenesis. Findings from mechanistic studies can inform and enhance guidelines for clinical management and treatment of NAFLD.
Acknowledgments
Thanks to the staff of Liver Disease Research Center, College of Medicine, King Saud University, Riyadh, Saudi Arabia for their contribution in data collection and support in preparing this work. We also wish to extend our gratitude to the National Plan for Science, Technology, and Innovation (MAARIFAH), King Abdulaziz City for Science and Technology, Riyadh, Saudi Arabia for their fund and support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the National Plan for Science, Technology, and Innovation (MAARIFAH), King Abdulaziz City for Science and Technology, Riyadh, Saudi Arabia, (Grant Number: 08-MED512-02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American association for the study of liver diseases. Hepatology. 2018;67(1):328–357.
2. Perumpail BJ, Khan MA, Yoo ER, Cholankeril G, Kim D, Ahmed A. Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J Gastroenterol. 2017;23(47):8263–8276. doi:10.3748/wjg.v23.i47.8263
3. Koch LK, Yeh MM. Nonalcoholic fatty liver disease (NAFLD): diagnosis, pitfalls, and staging. Ann Diagn Pathol. 2018;37:83–90. doi:10.1016/j.anndiagpath.2018.09.009
4. Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol. 2013;10(11):686–690. doi:10.1038/nrgastro.2013.171
5. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
6. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
7. Mitra S, De A, Chowdhury A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl Gastroenterol Hepatol. 2020;5:16. doi:10.21037/tgh.2019.09.08
8. Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62(1 Suppl):S47–64.
9. Bellentani S. The epidemiology of non-alcoholic fatty liver disease. Liver Int. 2017;37(Suppl 1):81–84. doi:10.1111/liv.13299
10. Polyzos SA, Kountouras J, Mantzoros CS. Adipose tissue, obesity and non-alcoholic fatty liver disease. Minerva Endocrinol. 2017;42(2):92–108. doi:10.23736/S0391-1977.16.02563-3
11. Vos B, Moreno C, Nagy N, et al. Lean non-alcoholic fatty liver disease (Lean-NAFLD): a major cause of cryptogenic liver disease. Acta Gastroenterol Belg. 2011;74(3):389–394.
12. Ge X, Zheng L, Wang M, Du Y, Jiang J. Prevalence trends in non-alcoholic fatty liver disease at the global, regional and national levels, 1990–2017: a population-based observational study. BMJ Open. 2020;10(8):e036663. doi:10.1136/bmjopen-2019-036663
13. Al-Daghri NM, Al-Attas OS, Alokail MS, et al. Diabetes mellitus type 2 and other chronic non-communicable diseases in the central region, Saudi Arabia (Riyadh cohort 2): a decade of an epidemic. BMC Med. 2011;9(1):76. doi:10.1186/1741-7015-9-76
14. Al-Rubeaan K, Al-Manaa H, Khoja T, et al. The Saudi abnormal glucose metabolism and diabetes impact study (SAUDI-DM). Ann Saudi Med. 2014;34(6):465–475. doi:10.5144/0256-4947.2014.465
15. Alhowaish AK. Economic costs of diabetes in Saudi Arabia. J Family Community Med. 2013;20(1):1–7. doi:10.4103/2230-8229.108174
16. Alswat K, Aljumah AA, Sanai FM, et al. Nonalcoholic fatty liver disease burden – Saudi Arabia and United Arab Emirates, 2017–2030. Saudi J Gastroenterol. 2018;24(4):211–219. doi:10.4103/sjg.SJG_122_18
17. Milic S, Lulic D, Stimac D. Non-alcoholic fatty liver disease and obesity: biochemical, metabolic and clinical presentations. World J Gastroenterol. 2014;20(28):9330–9337. doi:10.3748/wjg.v20.i28.9330
18. Leoni S, Tovoli F, Napoli L, Serio I, Ferri S, Bolondi L. Current guidelines for the management of non-alcoholic fatty liver disease: a systematic review with comparative analysis. World J Gastroenterol. 2018;24(30):3361–3373. doi:10.3748/wjg.v24.i30.3361
19. Al-hamoudi W, Ali S, Hegab B, et al. Revising the upper limit of normal for levels of serum alanine aminotransferase in a Middle Eastern population with normal liver histology. Dig Dis Sci. 2013;58(8):2369–2375. doi:10.1007/s10620-013-2659-0
20. Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–526. doi:10.1053/jhep.2003.50346
21. Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–1325. doi:10.1002/hep.21178
22. Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. doi:10.1002/hep.21496
23. Al-hamoudi W, El-Sabbah M, Ali S, et al. Epidemiological, clinical, and biochemical characteristics of Saudi patients with nonalcoholic fatty liver disease: a hospital-based study. Ann Saudi Med. 2012;32(3):288–292. doi:10.5144/0256-4947.2012.288
24. Labenz C, Huber Y, Kalliga E, et al. Predictors of advanced fibrosis in non-cirrhotic non-alcoholic fatty liver disease in Germany. Aliment Pharmacol Ther. 2018;48(10):1109–1116. doi:10.1111/apt.14976
25. Lonardo A, Nascimbeni F, Ballestri S, et al. Sex differences in nonalcoholic fatty liver disease: state of the art and identification of research gaps. Hepatology. 2019;70(4):1457–1469. doi:10.1002/hep.30626
26. Lonardo A, Suzuki A. Sexual dimorphism of NAFLD in adults. Focus on clinical aspects and implications for practice and translational research. J Clin Med. 2020;9(5):5. doi:10.3390/jcm9051278
27. Buday B, Pach PF, Literati-Nagy B, et al. Sex influenced association of directly measured insulin sensitivity and serum transaminase levels: why alanine aminotransferase only predicts cardiovascular risk in men? Cardiovasc Diabetol. 2015;14:55. doi:10.1186/s12933-015-0222-3
28. Tchernof A, Bélanger C, Morisset AS, et al. Regional differences in adipose tissue metabolism in women: minor effect of obesity and body fat distribution. Diabetes. 2006;55(5):1353–1360. doi:10.2337/db05-1439
29. Jensen MD, Cardin S, Edgerton D, Cherrington A. Splanchnic free fatty acid kinetics. Am J Physiol Endocrinol Metab. 2003;284(6):E1140–1148. doi:10.1152/ajpendo.00268.2002
30. Nielsen S, Guo Z, Johnson CM, Hensrud DD, Jensen MD. Splanchnic lipolysis in human obesity. J Clin Invest. 2004;113(11):1582–1588. doi:10.1172/JCI21047
31. Ballestri S, Nascimbeni F, Baldelli E, Marrazzo A, Romagnoli D, Lonardo A. NAFLD as a sexual dimorphic disease: role of gender and reproductive status in the development and progression of nonalcoholic fatty liver disease and inherent cardiovascular risk. Adv Ther. 2017;34(6):1291–1326.
32. Kamada Y, Kiso S, Yoshida Y, et al. Estrogen deficiency worsens steatohepatitis in mice fed high-fat and high-cholesterol diet. Am J Physiol Gastrointest Liver Physiol. 2011;301(6):G1031–1043. doi:10.1152/ajpgi.00211.2011
33. Yang JD, Abdelmalek MF, Pang H, et al. Gender and menopause impact severity of fibrosis among patients with nonalcoholic steatohepatitis. Hepatology. 2014;59(4):1406–1414. doi:10.1002/hep.26761
34. Chen ZW, Chen LY, Dai HL, Chen JH, Fang LZ. Relationship between alanine aminotransferase levels and metabolic syndrome in nonalcoholic fatty liver disease. J Zhejiang Univ Sci B. 2008;9(8):616–622. doi:10.1631/jzus.B0720016
35. Lonardo A, Bellentani S, Ratziu V, Loria P. Insulin resistance in nonalcoholic steatohepatitis: necessary but not sufficient – death of a dogma from analysis of therapeutic studies? Expert Rev Gastroenterol Hepatol. 2011;5(2):279–289. doi:10.1586/egh.11.19
36. Macotela Y, Boucher J, Tran TT, Kahn CR. Sex and depot differences in adipocyte insulin sensitivity and glucose metabolism. Diabetes. 2009;58(4):803–812. doi:10.2337/db08-1054
37. Geer EB, Shen W. Gender differences in insulin resistance, body composition, and energy balance. Gend Med. 2009;6(Suppl1):60–75. doi:10.1016/j.genm.2009.02.002
38. Pelusi S, Cespiati A, Rametta R, et al. Prevalence and risk factors of significant fibrosis in patients with nonalcoholic fatty liver without steatohepatitis. Clin Gastroenterol Hepatol. 2019;17(11):2310–2319.e2316. doi:10.1016/j.cgh.2019.01.027
39. Gawrieh S, Wilson LA, Cummings OW, et al. Histologic findings of advanced fibrosis and cirrhosis in patients with nonalcoholic fatty liver disease who have normal aminotransferase levels. Am J Gastroenterol. 2019;114(10):1626–1635. doi:10.14309/ajg.0000000000000388
40. McPherson S, Hardy T, Henderson E, Burt AD, Day CP, Anstee QM. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol. 2015;62(5):1148–1155. doi:10.1016/j.jhep.2014.11.034
41. Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol. 2015;13(4):643–654. doi:10.1016/j.cgh.2014.04.014
42. Stål P. Liver fibrosis in non-alcoholic fatty liver disease – diagnostic challenge with prognostic significance. World J Gastroenterol. 2015;21(39):11077–11087. doi:10.3748/wjg.v21.i39.11077
43. Verma S, Jensen D, Hart J, Mohanty SR. Predictive value of ALT levels for non-alcoholic steatohepatitis (NASH) and advanced fibrosis in non-alcoholic fatty liver disease (NAFLD). Liver Int. 2013;33(9):1398–1405. doi:10.1111/liv.12226
44. Ma X, Liu S, Zhang J, et al. Proportion of NAFLD patients with normal ALT value in overall NAFLD patients: a systematic review and meta-analysis. BMC Gastroenterol. 2020;20(1):10. doi:10.1186/s12876-020-1165-z
45. Fracanzani AL, Valenti L, Bugianesi E, et al. Risk of severe liver disease in nonalcoholic fatty liver disease with normal aminotransferase levels: a role for insulin resistance and diabetes. Hepatology. 2008;48(3):792–798. doi:10.1002/hep.22429
46. Uslusoy HS, Nak SG, Gülten M, Biyikli Z. Non-alcoholic steatohepatitis with normal aminotransferase values. World J Gastroenterol. 2009;15(15):1863–1868. doi:10.3748/wjg.15.1863
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.