")
Back to Journals » Infection and Drug Resistance » Volume 14
Clinical and Laboratory Characteristics of Patients infected by Listeria monocytogenes at a Tertiary Hospital in Hefei City, China
Authors Shi C , Lv D, Zhou K, Jin T , Wang G , Wang B, Li Y , Xu Y
Received 18 August 2021
Accepted for publication 13 October 2021
Published 25 October 2021 Volume 2021:14 Pages 4409—4419
DOI https://doi.org/10.2147/IDR.S334929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Cuixiao Shi,1 Dongmei Lv,1 Kai Zhou,1 Tengchuan Jin,2 Gang Wang,3 Bo Wang,1 Yajuan Li,1 Yuanhong Xu1
1Department of Clinical Laboratory, The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China; 2Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, 230027, People’s Republic of China; 3The Second Hospital of Anhui Medical University, Hefei, 230601, People’s Republic of China
Correspondence: Yuanhong Xu; Yajuan Li
Department of Clinical Laboratory, The First Affiliated Hospital of Anhui Medical University, 218 Jixi Road, Hefei, People’s Republic of China
Email [email protected]; [email protected]
Background: Human listeriosis is a severe foodborne infection caused by Listeria monocytogenes and the data of patients with this infection are largely limited for the Hefei population.
Purpose: This is a retrospective study that evaluated the clinical and laboratory data of patients with listeriosis at a tertiary hospital in Hefei City.
Patients and Methods: A total of 24 listeriosis patients were admitted to the First Affiliated Hospital of Anhui Medical University from January 2003 to July 2021. Data from all patients were collected from the hospital’s electronic medical records.
Results: The most common symptom of all patients was fever (91.7%), followed by altered consciousness (50.0%), rashes (45.8%), respiratory distress symptoms (37.5%), nuchal rigidity (29.2%), and headaches (20.8%). Laboratory results also indicated elevated C-reactive protein (CRP) (79.1%), hypoproteinemia (75.0%), anemia (62.5%), leukocytosis (45.8%), and neutrophilia (45.8%). The mean value of 5.1 μg/mL (SD, 3.8) for D‐dimer (D‐D) was significantly higher than the normal value ((0.00– 0.50) μg/mL), while both altered consciousness (6 vs 4, P = 0.034) and headaches (4 vs 1, P = 0.036) occurred more frequently in the neurolisteriosis group compared with the bacteremia one. Additionally, the mean maximal body temperature (°C) (40.5 ± 0.7) as well as white blood cell (WBC) (15.3 vs 7.5 × 109/L, P = 0.014) and neutrophil (NEUT#) (13.2 vs 6.1 × 109/L, P = 0.026) counts of neurolisteriosis patients were higher than those of bacteremia (39.4 ± 0.4) (P = 0.001). Of all patients, four (50%) from the maternal-neonatal group remained uncured.
Conclusion: Listeriosis is a rare disease with extremely variable clinical characteristics in Hefei City. Our data indicated that unexplained fever, altered consciousness, hypoproteinemia, anemia, elevated CRP and DD should be considered to assist diagnosis of listeriosis for early treatment interventions.
Keywords: Listeria monocytogenes, listeriosis, clinical and laboratory characteristics
Introduction
Listeria monocytogenes (L. monocytogenes) is an intracellular, aerobic or facultative anaerobic, gram-positive bacterium,1 and although its main route of transmission is fecal-oral transmission,2 it can also infect newborns through the placenta and birth canal.1 This bacteria, belonging to the Listeria genus, is widely distributed and commonly found in different environments. More importantly, out of the 17 described Listeria species, it is the main pathogenic species that causes disease in both humans and animals, even though, Listeria ivanovii is also known to be pathogenic to humans.3,4 Listeriosis is a life-threatening disease with a very high mortality in humans and it is caused by the foodborne pathogen L. monocytogenes, whose invasive form is classified into three types: bacteremia, neurolisteriosis, and maternal-neonatal infection.5,6 L. monocytogenes infection can cause a variety of syndromes in humans, ranging from mild to severe.7 In immunocompetent individuals, the symptoms are mild and usually manifest as self-limiting gastroenteritis, accompanied by symptoms including fever, diarrhea, nausea, and vomiting. However, pregnant women, fetuses, and neonates, as well as the elderly, and immunocompromised individuals, are particularly susceptible to developing severe forms of the disease characterized by symptoms of septicemia, meningitis, or encephalitis.7
Despite the availability of effective antibiotic treatments, cases of listeriosis are increasing around the world, thereby posing a global threat to public health.8 Listeriosis cases have been reported in many mainland provinces of China, but it has not yet been regulated as a notifiable disease in China. Affected areas have mainly been in Beijing, and the coastal areas probably due to higher detection rates of listeria, dietary habits, and high population density.9,10 A disease is diagnosed as listeriosis when a positive bacterial culture is obtained from clinical specimens collected from sterile sites, such as blood, cerebrospinal fluid (CSF), amniotic fluid, and uterine swabs.11 Additionally, PCR assays can be applied for diagnostic purposes and it is particularly useful when cultures are compromised by prior administration of antimicrobial agents which lead to false-negative results.11 However, for the commonly applied culture method, the disease itself has a long incubation period while being characterized by a wide spectrum of infections. As such, it becomes difficult to track an accurate food eating history.12 Therefore, listeriosis can be easily overlooked and misdiagnosed, thereby leading to further difficulties in a timely diagnosis in clinical practice.
Since 2000, the Chinese government has stepped up efforts to control listeriosis and improve the monitoring system for the disease.13 However, due to the relatively late start of this program, there is a paucity of data regarding listeriosis in humans in China.13 In particular, there are only few investigations describing listeriosis in Hefei City, with our knowledge of L. monocytogenes infection and its resulting disease being extremely limited. Therefore, the present study aimed to explore the clinical presentations of patients infected by L. monocytogenes before further assessing the laboratory findings, treatment history and outcomes associated with the disease in Hefei City, in the Province of Anhui. It is expected that this will serve as a starting point for future listeriosis-based studies and provide valuable information for improving the detection and diagnosis of listeriosis.
Patients and Methods
Recruitment Criteria and Listeriosis Diagnosis
This is a retrospective study that included all patients diagnosed with listeriosis from January 2003 to July 2021 at the First Affiliated Hospital of Anhui Medical University (Hefei, Anhui Province, China). There is no generally accepted diagnostic criteria for listeriosis. So, in this study, a case was considered to be positive when L. monocytogenes was isolated from a normally sterile site such as blood or cerebrospinal fluid (CSF) which was submitted to the laboratory during admission of the patients. Those diagnosed with listeriosis were grouped according to earlier reports from France and China,5,9 with patients being divided into a maternal-neonatal infection group, a bacteremia group, and a neurolisteriosis group. Maternal-neonatal infection was defined based on the isolation of L. monocytogenes from pregnant women, as well as one-month old or younger neonates. On the other hand, bacteremia was diagnosed when L. monocytogenes was isolated from a patient’s blood culture without neurolisteriosis or maternal-neonatal infections, while neurolisteriosis was considered to have occurred when L. monocytogenes was isolated from the CSF or a brain abscess or even when a positive blood culture test for L. monocytogenes was accompanied by altered consciousness, seizures, nuchal rigidity, focal neurological symptoms, as well as an increased white blood cell count in the CSF. Overall, eight patients were assigned to the maternal-neonatal infection group and ten patients, with positive blood culture tests for L. monocytogenes infection, were assigned to the bacteremia one. Finally, six patients were included in the neurolisteriosis group, with five of these being positive during CSF culture only and another one being positive during both CSF and blood culture tests.
Data Collection
Demographic information (age, gender, occupation), together with clinical, laboratory, physical examination, basic diseases and comorbidities, complications, treatment history, and in-hospital outcomes (length of hospital stay, and discharge clinical status) data were obtained from the hospital’s electronic medical records.
Statistical Analysis
The statistical analysis was conducted using SPSS version 25.0. Continuous variables that assumed normal distribution were presented as the mean ± standard deviation (SD) and compared by Student’s t-test, while those without a normal distribution were presented as medians (interquartile range (IQR)) and compared by the Mann‐Whitney U-test. For categorical variables, data were provided as n (%) and compared by Fisher’s exact test. Results was considered to be statistically significant at a two-tailed P value of less than 0.05.
Results
Patients and Demographics
From January 2003 to July 2021, a total of 24 patients were diagnosed with listeriosis from the First Affiliated Hospital of Anhui Medical University. They were then further divided into the three groups namely the maternal-neonatal group (8 cases), the bacteremia group (10 cases), and the neurolisteriosis group (6 cases) (Table 1).
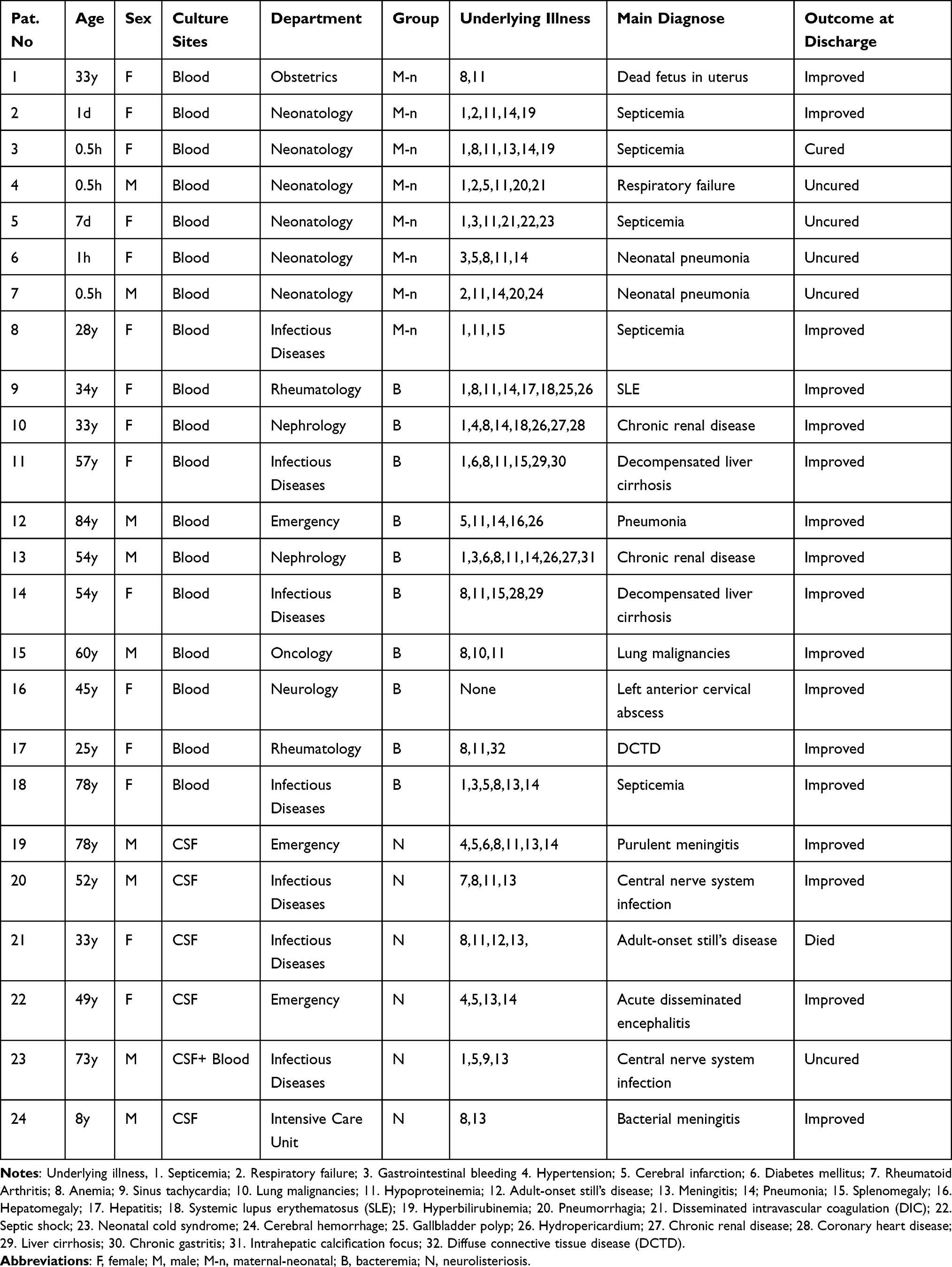 |
Table 1 Detailed Information of the 24 Listeriosis Patients |
For the 24 hospitalized patients, the age range was from 0.5 hours to 84 years, with 6 of them aged less than 1 month and an overall median age of 33.5 years (IQR, 2–56.3).
Furthermore, more than half of the participants were female (15/24, 62.5%), with nine of them (37.5%) being male. Among other characteristics, 11 cases (45.8%) were diagnosed with listeriosis in spring while 13 patients (54.2%) had one or more basic diseases, including cardiovascular and cerebrovascular diseases (10/24, 41.7%), diabetes mellitus (3/24, 12.5%), malignancy (1/24, 4.2%), chronic kidney diseases (2/24, 8.3%), auto-immune diseases (4/24, 16.7%), or even hepatic diseases (5/24, 20.8%). However, differences in demographic characteristics and basic disease parameters between the bacteremia and neurolisteriosis group were not statistically significant (P > 0.05) (Table 2). Of all the patients, 11 were from Hefei and its surrounding districts while the others were from the nearby cities of Luan (5 cases), Suzhou (2 cases), Bozhou (2 cases), Anqing (1 case), Huaibei (1case), Huangshan (1 case), and Xinyang, Henan province (1 case).
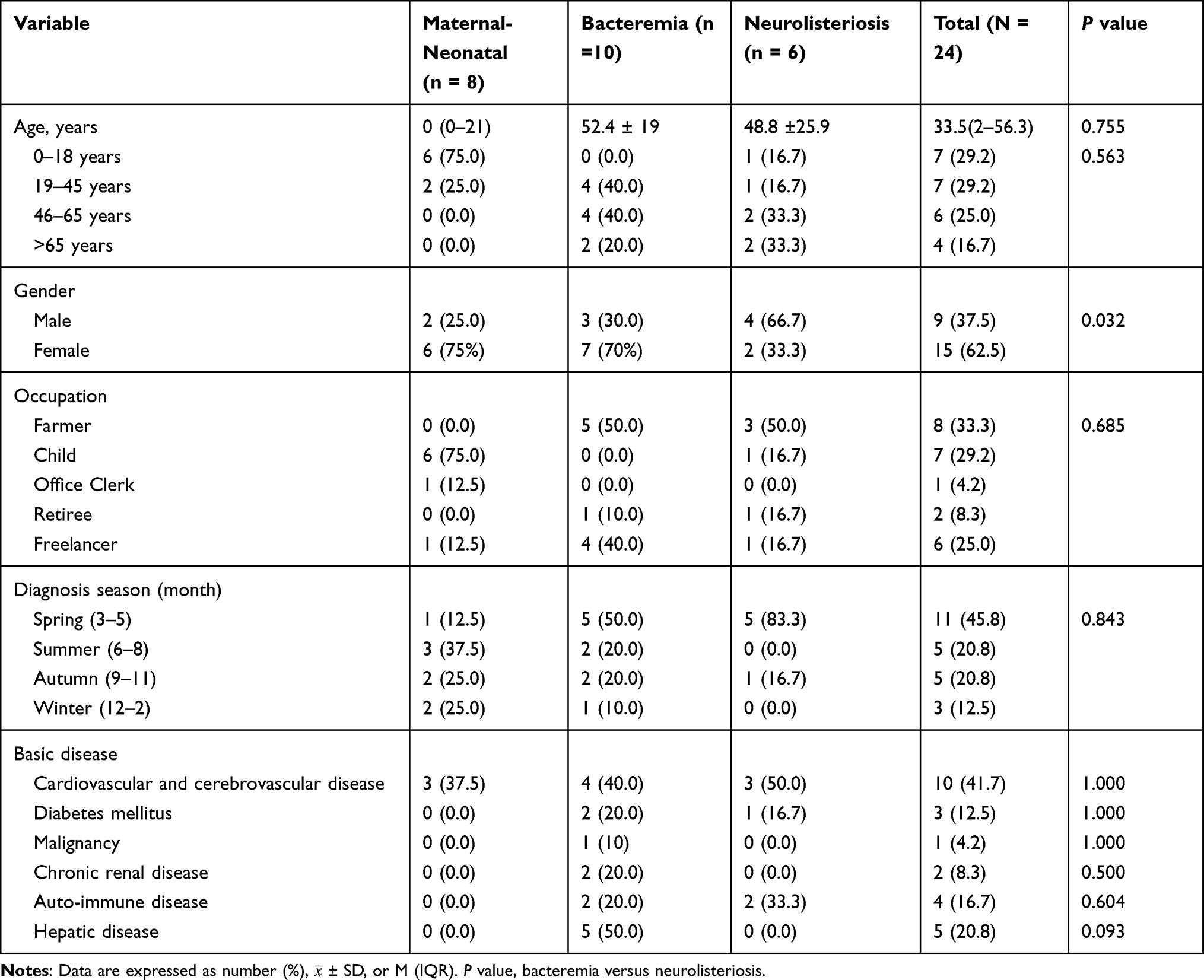 |
Table 2 Demographic and Basic Disease Analysis of Listeriosis Patients (N = 24) |
Clinical Characteristics
The most common symptom observed for the 24 patients on presentation was fever (91.7%), followed by altered consciousness (45.8%), rashes (45.8%), respiratory distress symptoms (37.5%), cough (37.5%), sputum (29.2%), nuchal rigidity (25.0%), headache (20.8%), nausea and vomiting (16.7%), diarrhea (12.5%), abdominal distension (12.5%), abdominal pain (12.5%), and seizures (12.5%). Regarding complications, pneumonia was very common and was observed in 11 of the cases (45.8%) while gastrointestinal bleeding was observed in 4 cases (16.7%). Of the 24 patients, eight (33.3%) received immunosuppressive treatments and they were all from the non-maternal-neonatal group. All the six newborns in the maternal-neonatal group had respiratory distress.
In terms of symptoms, fever was the most common symptom of all the three groups in this study. In addition, the common symptoms for each group of patients were as follows: in the maternal-neonatal group, respiratory distress (75.0%), and rashes (50.0%) were frequent while the common symptoms for the bacteremia group were cough (60.0%), sputum (50.0%), and rashes (50.0%). Finally, altered consciousness (100.0%), headache (66.7%), and nuchal rigidity (66.7%) were found to be common in the neurolisteriosis group. More patients with neurolisteriosis presented altered consciousness (6 vs 3, P = 0.011), nuchal rigidity (4 vs 0, P = 0.008) and headache (4 vs 1, P = 0.036) compared with those with bacteremia. Similarly, the mean maximum body temperature (°C) for neurolisteriosis patients (40.5 ± 0.7) was higher than that of bacteremia ones (39.4 ± 0.4) (P = 0.001). However, the differences in other clinical parameters between the bacteremia and neurolisteriosis groups were not statistically significant (P > 0.05) (Table 3).
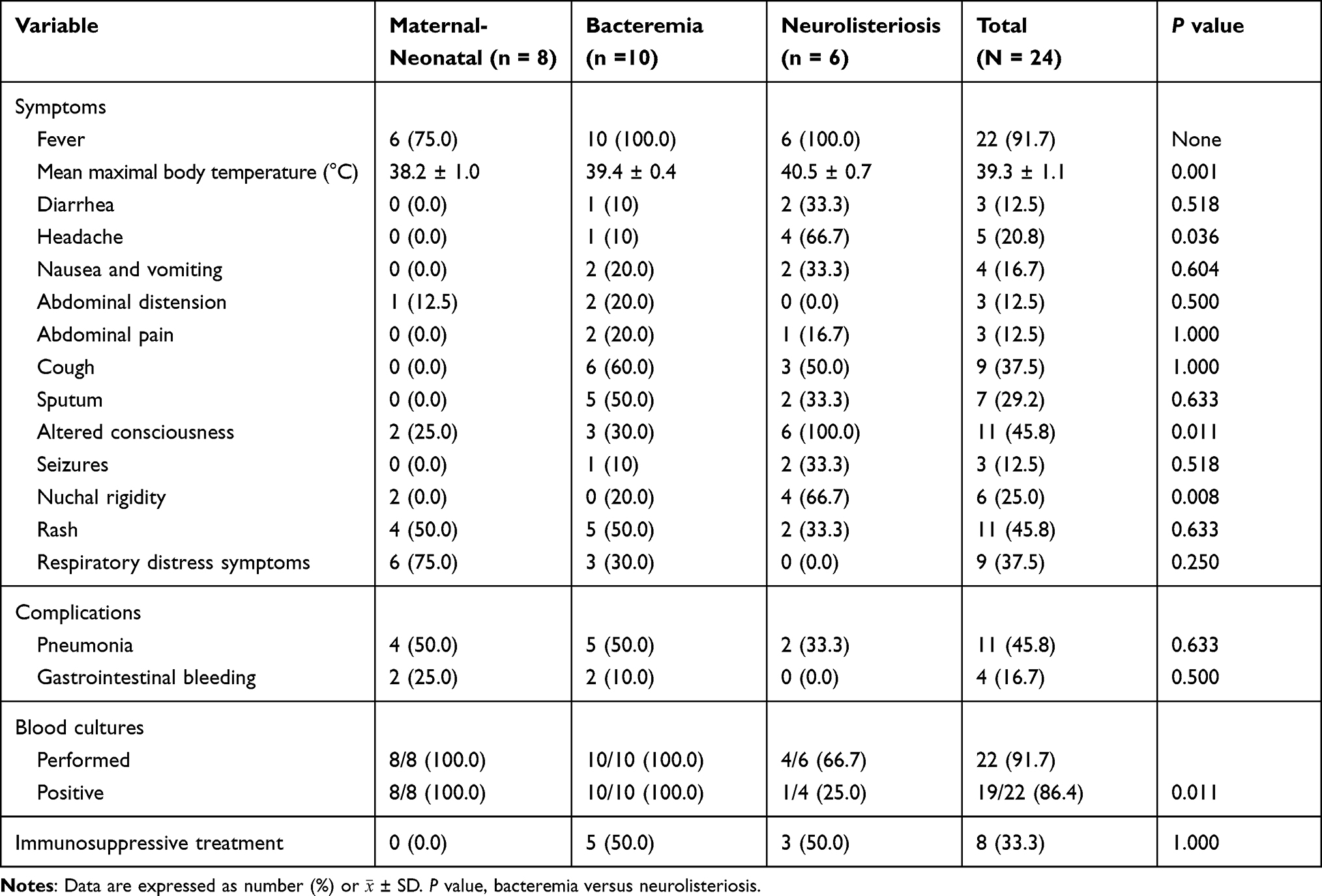 |
Table 3 Clinical Symptoms Analysis of Listeriosis Patients (N = 24) |
Laboratory Findings
Laboratory data was available for all the 24 patients and indicated that elevated C-reactive protein (CRP) levels was the most common disorder (79.1%). Furthermore, common, hematological changes included 18 cases of hypoproteinemia (75.0%), 15 cases of anemia (62.5%), 11 cases of leukocytosis (45.8%), and 11 cases of neutrophilia (45.8%). Twenty patients had different degrees of abnormal liver functions, with at least one of the following liver enzymes, namely alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (GGT) or lactate dehydrogenase (LDH) being above the normal range. Overall, the median levels of ALT, AST, ALP, GGT, LDH were 26.5 U/L (IQR,16.5–49.5), 44.5 U/L (IQR, 25.0–121.0), 93.0 U/L (IQR, 64.5–130.8), 55.0 U/L (IQR, 21.3–132.0), and 415.0 U/L (IQR, 269.3–825.0), respectively. Through additional analyses, the results of haemostatic functions were also described. In this case, the mean value of D‐dimer (D‐D) was 5.1 (SD, 3.8) μg/mL, and it was significantly higher than the normal value ((0.00–0.50) μg/mL). Moreover, the mean values of activated partial thromboplastin time (APTT) and prothrombin time (PT) were 45.8 (SD, 31.4) s and 15.6 (SD, 5.0) s respectively while the mean CSF glucose and the median CSF protein levels were 2.6 (SD, 1.8) mmol/L and 1.4 g/L (IQR, 0.7–2.9) respectively.
Leukocytosis occurred in six (100.0%) of the patients from the neurolisteriosis group, as well as in two (20.0%) of those from the bacteremia one, with statistical analysis showing that leukocytosis was more frequently in in the former (P = 0.007). In addition, even though the differences in other laboratory findings between the bacteremia and neurolisteriosis groups were not statistically significant, white blood cell (WBC) counts (P = 0.014) and neutrophil counts (NEUT#) (P = 0.026) were found to be statistically different between the two groups. In this case, the mean values of WBC counts and NEUT# in the neurolisteriosis group were 15.3 (SD, 5.8) ×109/L and 13.2 (SD, 6.7) ×109/L, respectively, and they were both higher than the mean values of 7.5 (SD, 5.2) ×109/L and 6.1 (SD, 4.8) ×109/L, respectively, for the bacteremia group (Table 4).
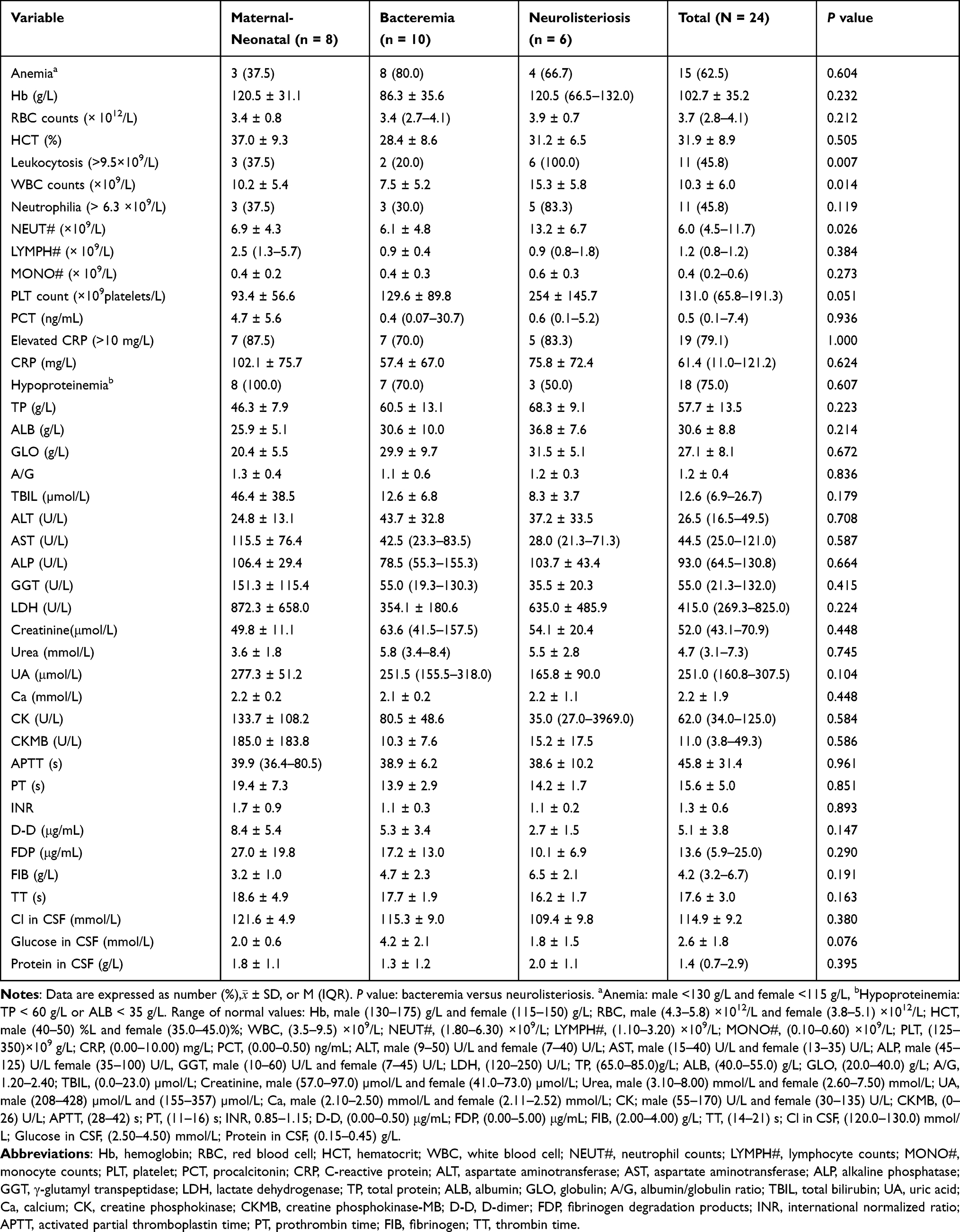 |
Table 4 Laboratory Results of Listeriosis Patients (N = 24) |
Antibacterial Treatment History and Outcomes
For patients with listeriosis, ampicillin or penicillin is the first-choice antibiotic treatment. For antimicrobial susceptibility tests involving L. monocytogenes from 10 patients, the results showed that all the isolates were sensitive to both antibiotics. As shown in Table 5, eight patients (33.3%) were treated with ampicillin, seven (29.2%) were provided with penicillin while nine patients (37.5%) had been given cephalosporin treatment. In the absence of etiological information, the physician would often choose cephalosporin antibiotics based on clinical symptoms and experience, but this treatment could not completely cover all of the pathogens. After treatment, 18 patients (75%) were discharged within 3 to 5 days after the improvement of clinical symptoms but 1 patient also died during hospitalization. In addition, four patients within the maternal-neonatal group remained uncured, with three of them giving up treatment. Overall, the median duration of hospitalization for the 24 patients was 13.5 days (IQR, 5.8–27.3).
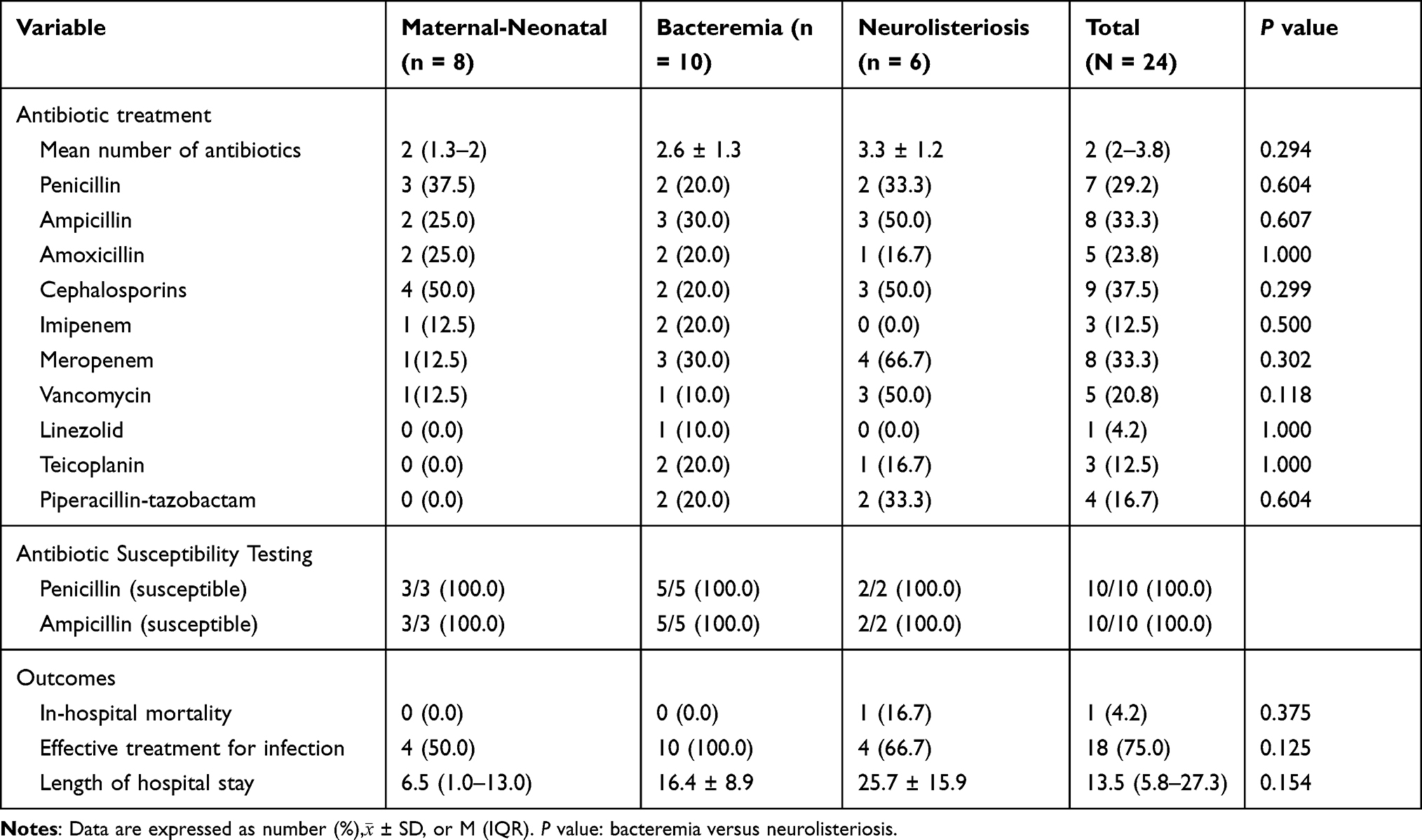 |
Table 5 Antibacterial Treatment History and Outcomes of Listeriosis Patients (N = 24) |
Discussion
L. monocytogenes, a ubiquitous bacterium, is widely distributed in nature, and can exist in water, soil, human and animal feces, as well as in vegetables and fruits.14 L. monocytogenes is mainly transmitted to humans through ingestion of contaminated food and as such, human listeriosis can be prevented.15 The prevalence of L. monocytogenes in food products in Anhui Provinces was 1.58%, a value which was lower than the average prevalence of 4.42% in Chinese food products from 28 provinces.16 Therefore, listeriosis is uncommon and even though there are many reports regarding its outbreak in other countries,5,17,18 sporadic cases are the main ones occurring in China, with most of them appearing in the form of case reports.8,19–21 However, this could also be due to a lack of surveillance, or a less widespread distribution of processed foods unlike in countries where outbreaks are more common. As mentioned earlier, the areas where listeriosis were mainly distributed were the cities of Beijing, Sichuan, Zhejiang, Liaoning, and Shaanxi.13 Prior to this study, information on cases of this disease, as well as its treatment in Hefei City was limited. Hence, this work retrospectively collected clinical data from the medical records of 24 patients diagnosed with listeriosis. Details regarding the demographics, clinical and laboratory characteristics, treatment history and outcomes of infection were also provided. This report, to our knowledge, is the first one which analyzed data on patients with listeriosis in Anhui Province.
In our study, farmers (33.3%) were found to be at a high risk of contracting the disease and this could be related to their occupational exposure to L. monocytogenes contaminated food. Furthermore, the number of female cases were higher (15 vs 9), with this situation being similar to that of many provinces or cities in China.13 Listeriosis occurred all over the year but was more common in spring (45.8%), followed by summer (20.8%) and autumn (20.8%). Previous studies have reported that listeriosis were more often observed during spring and autumn,15 although many patients were also admitted in the summer months9 and this could be attributed to geographical differences. All the 24 cases were sporadic infections that we know very little about and there were no epidemiological and microbiological criteria to classify them as an outbreak. However, comparative sequence analysis of strains from clinical specimens in Shanghai suggested that infection was likely the result of foodborne transmission.22 Generally, invasive listeriosis affects people with compromised immune systems and rarely affects healthy individuals.20 As such, many patients mainly suffered from basic forms of the disease and similar findings have been described in Beijing.21
The most common clinical manifestation of the cases in Hefei City was fever (91.7%). It was slightly higher than the 88.6% of fever rate previously reported in southern Taiwan.23 As listeriosis during pregnancy is severe and difficult to diagnose, blood cultures should be considered for any pregnant woman who develops this common symptom, especially those which are accompanied by flu-like or gastrointestinal symptoms.11 We also paid attention to two neonates without fever for whom respiratory distress could be the primary symptoms. This was especially the case for the maternal-neonatal group where 75.0% of patients had respiratory distress symptoms and all of them were neonates. This was similar to findings from a study conducted in Beijing.21 In addition to symptoms such as altered consciousness and nuchal rigidity where the central nervous system (CNS) is involved, patients from the neurolisteriosis group also had a higher mean maximal body temperature than the bacteremia one (40.5 °C vs 39.4 °C). These results may indicate a poor prognosis in the neurolisteriosis group. Furthermore, symptoms of cough and sputum occurred frequently in patients with bacteremia (60.0%, 50.0%), and this could be helpful for the diagnosis of the disease. A significant proportion of listeriosis patients had symptoms of fever, respiratory distress, cough, gastrointestinal, and CNS involvement. However, the clinical manifestations were largely varied while being similar to those of common bacterial infections. Moreover, most of the patients are treated for basic diseases, thus making the diagnosis of listeriosis much more difficult.
Pneumonia was very common and was observed in eleven cases (45.8%) in our study. A study in South Africa showed that 33.3% of neonates were diagnosed with congenital pneumonia,24 but this value was lower than the 66.7% found in our study. Similarly, in the past 40 years, only 16 pneumonia cases have been reported in France, either as isolated case reports or as small groups of two to seven cases.25 L. monocytogenes can also be carried in the gastrointestinal tract as reflected in the 44.7% of listeriosis patients in a study at Peking Union Medical College Hospital who had gastrointestinal symptoms.21 This was consistent with the current study in which 45.8% of listeriosis patients showed gastrointestinal symptoms and 16.7% of them had gastrointestinal bleeding. In terms of comorbidities, a study completed in Belgium showed that the most frequent ones were immunosuppressive therapy, cancer, and severe cardiovascular diseases.26 Another study conducted in the United States also indicated that the most frequent comorbidities were immunosuppressive therapy, malignancy, and diabetes mellitus.27 In the case of this study, it was found that that cerebrovascular diseases (41.7%), immunosuppressive treatment (33.3%), and hepatic diseases (20.8%) occurred more frequently in listeriosis patients.
Very little was found in existing literature regarding the laboratory characteristics of listeriosis. In a similar way to common bacterial infections, the WBC and neutrophils counts in peripheral blood as well as the biochemical index CRP increased in most patients with listeriosis. This was consistent with the previous studies,5,28,29 and indicated the likelihood of missed or misdiagnosed cases of the disease. Specifically, the most relevant clinically-relevant finding in our study was that of hypoproteinemia (75.0%) and anemia (62.5%) which occurred in the majority of the patients. Therefore, we hypothesized that monitoring the levels of total protein (TP), albumin (ALB), and hemoglobin (Hb) could assist in the diagnosis of listeriosis. Twenty patients presented at least one elevated liver enzyme, including ALS, AST, ALP, GGT, LDH. Therefore, the impact of L. monocytogenes on liver function is also worthy of attention during the disease progression. In our study WBC count (15.3 vs 7.5 ×109/L, P = 0.014) and NEUT# (13.2 vs 6.1 ×109/L, P = 0.026) were found to be much higher in the neurolisteriosis group compared with the bacteremia one. Furthermore, while the effective treatment percentage for the bacteremia group was 100%, that of patients in the neurolisteriosis group was only 66.7%. Contrary to the present results, a previous study in Italy has demonstrated that an unfavorable outcome frequently occurred for those patients presenting a low WBC count.30 Human neurolisteriosis is a bloodborne infection and positive blood cultures at the time of diagnosis can not only reflect higher circulating bacteria in the blood as well as weaker host defenses, but also a higher risk of mortality due to other opportunistic infections.5 In our study, an elderly patient with positive blood and CSF cultures was not cured at discharge.
Antibiotics, as key factors affecting the prognosis, is an important part of treatment. Ampicillin or penicillin, alone or in combination with aminoglycosides are used as the first choice for listeriosis.31 Previous studies in China have shown that 144 isolates of L. monocytogenes strains were uniformly susceptible to ampicillin, penicillin, and meropenem.32 This was consistent with our research in which 10 isolates of L. monocytogenes were sensitive to both ampicillin and penicillin. Therefore, both can still be used as effective antibiotics to treat listeriosis, although it should be noted that L. monocytogenes, despite being susceptible to a variety of antibiotics in vitro, is not highly sensitive to cephalosporins.33,34 However, despite the availability of treatment methods, the biggest challenge for treating listeriosis is the inability to diagnose the disease early enough to provide adequate treatment.
Early diagnosis and treatment can, therefore, improve the prognosis of the infection. Since L. monocytogenes has several antigens, including listeriolysin O and Rantz antigen, which can cross-react with other gram-positive bacteria,35 serological tests are insensitive for routine diagnosis. As such, microbial culture has been shown to be a useful method for diagnosing listeriosis.36 For those patients with fever, diarrhea, nausea, vomiting, altered consciousness, nuchal rigidity and seizures, isolation of pathogens from sterile sites should be carried out at the earliest. A previous epidemiological investigation of listeriosis in China showed that 18.0% of patients-isolated L. monocytogenes could be found from suspicious food, chopping boards, refrigerator, or kitchen sinks.37 The surveillance of L. monocytogenes in related foods should, therefore, be strengthened to reduce its transmission.
Despite the results, some limitations are recognized for our study. There were no detailed epidemiological investigations for patients, and hence, we could not identify the sources of the patient’s infections nor formulate clear recommendations. Moreover, due to the small sample size in this study, the interpretation of our findings might not be representative in the bigger population. Nevertheless, despite these limitations, our study still provides important perspectives for listeriosis in Hefei City. We also expect that our study will provide guidance and references to clinicians for the prompt diagnosis and treatment of listeriosis.
Conclusion
Unexplained fever, altered consciousness, hypoproteinemia, anemia, elevated CRP and DD should be considered to aid diagnosis of listeriosis for early treatment interventions.
Listeriosis causes public health concern and additional large-scale studies are needed to gain a thorough understanding of this disease in China. This study summarized eighteen years of patient data in Hefei City and it could serve as a reference for other cities and provinces of China to improve prevention, diagnosis, and treatment strategies against listeriosis.
Ethical Approval
This study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Anhui Medical University in accordance with the Declaration of Helsinki (reference number: Quick-PJ 2021-11-17). The written informed consent was obtained from patients and a parent or legal guardian of patients under 18 years of age.
Acknowledgments
This work was financially supported by Anhui Natural Science Foundation (grant number: 9021138201) and Scientific Research Project of Universities in Anhui Province (grant number: KJ2020A0170).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Wang Z, Tao X, Liu S, Zhao Y, Yang X. An update review on listeria infection in pregnancy. Infect Drug Resist. 2021;14:1967–1978. doi:10.2147/IDR.S313675
2. Maertens DNC, Devleesschauwer B, Maertens DNA, et al. Comorbidities and factors associated with central nervous system infections and death in non-perinatal listeriosis: a clinical case series. BMC Infect Dis. 2016;16:256. doi:10.1186/s12879-016-1602-3
3. Kaptchouang TC, Fri J, De Santi M, et al. Listeriosis outbreak in South Africa: a comparative analysis with previously reported cases worldwide. Microorganisms. 2020;8(1):135.
4. Orsi RH, Wiedmann M. Characteristics and distribution of Listeria spp., including Listeria species newly described since 2009. Appl Microbiol Biotechnol. 2016;100(12):5273–5287. doi:10.1007/s00253-016-7552-2
5. Charlier C, Perrodeau É, Leclercq A, et al. Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study. Lancet Infect Dis. 2017;17(5):510–519.
6. Disson O, Moura A, Lecuit M. Making Sense of the Biodiversity and Virulence of Listeria monocytogenes. Trends Microbiol. 2021;29(9):811–822. doi:10.1016/j.tim.2021.01.008
7. Duze ST, Marimani M, Patel M. Tolerance of Listeria monocytogenes to biocides used in food processing environments. Food Microbiol. 2021;97:103758. doi:10.1016/j.fm.2021.103758
8. Zhang X, Niu Y, Liu Y, et al. Isolation and Characterization of Clinical Listeria monocytogenes in Beijing, China, 2014–2016. Front Microbiol. 2019;10:981. doi:10.3389/fmicb.2019.00981
9. Fan Z, Xie J, Li Y, Wang H. Listeriosis in mainland China: a systematic review. Int J Infect Dis. 2019;81:17–24. doi:10.1016/j.ijid.2019.01.007
10. Zhang Y, Dong S, Chen H, et al. Prevalence, Genotypic Characteristics and Antibiotic Resistance of Listeria monocytogenes From Retail Foods in Bulk in Zhejiang Province, China. Front Microbiol. 2019;10:1710. doi:10.3389/fmicb.2019.01710
11. Allerberger F, Wagner M. Listeriosis: a resurgent foodborne infection. Clin Microbiol Infect. 2010;16(1):16–23. doi:10.1111/j.1469-0691.2009.03109.x
12. Swaminathan B, Gerner-Smidt P. The epidemiology of human listeriosis. Microbes Infect. 2007;9(10):1236–1243. doi:10.1016/j.micinf.2007.05.011
13. Chen S, Meng F, Sun X, et al. Epidemiology of human listeriosis in China during 2008–2017. Foodborne Pathog Dis. 2020;17(2):119–125. doi:10.1089/fpd.2019.2683
14. Li C, Zeng H, Ding X, et al. Perinatal listeriosis patients treated at a maternity hospital in Beijing, China, from 2013–2018. BMC Infect Dis. 2020;20(1):601. doi:10.1186/s12879-020-05327-6
15. Feng Y, Wu S, Varma JK, Klena JD, Angulo FJ, Ran L. Systematic review of human listeriosis in China, 1964–2010. Trop Med Int Health. 2013;18(10):1248–1256. doi:10.1111/tmi.12173
16. Li W, Bai L, Fu P, Han H, Liu J, Guo Y. The Epidemiology of Listeria monocytogenes in China. Foodborne Pathog Dis. 2018;15(8):459–466. doi:10.1089/fpd.2017.2409
17. Elinav H, Hershko-Klement A, Valinsky L, et al. Pregnancy-Associated Listeriosis: clinical Characteristics and Geospatial Analysis of a 10-Year Period in Israel. Clin Infect Dis. 2014;59(7):953–961. doi:10.1093/cid/ciu504
18. Mook P, O’Brien SJ, Gillespie IA. Concurrent conditions and human listeriosis, England, 1999–2009. Emerg Infect Dis. 2011;17(1):38–43. doi:10.3201/eid1701.101174
19. Luo L, Chen X, Payne M, et al. Case report: whole genome sequencing based investigation of maternal-neonatal listeriosis in Sichuan, China. BMC Infect Dis. 2019;19(1):893. doi:10.1186/s12879-019-4551-9
20. Li N, Huang HQ, Zhang GS, Hua W, Shen HH. Encephalitis caused by Listeria monocytogenes in a healthy adult male in China: a case report. Medicine. 2019;98(25):e16145. doi:10.1097/MD.0000000000016145
21. Wang H, Ghanem KG, Wang P, Yang S, Li T. Listeriosis at a Tertiary Care Hospital in Beijing, China: high Prevalence of Nonclustered Healthcare-Associated Cases Among Adult Patients. Clin Infect Dis. 2013;56(5):666–676. doi:10.1093/cid/cis943
22. Zhang J, Cao G, Xu X, et al. Evolution and Diversity of Listeria monocytogenes from Clinical and Food Samples in Shanghai, China. Front Microbiol. 2016;7:1138.
23. Lee CY, Tsai HC, Kunin CM, Lee SS, Wu KS, Chen YS. Emergence of sporadic non-clustered cases of hospital-associated listeriosis among immunocompromised adults in southern Taiwan from 1992 to 2013: effect of precipitating immunosuppressive agents. BMC Infect Dis. 2014;14:145. doi:10.1186/1471-2334-14-145
24. Ntuli N, Wadula J, Nakwa F, et al. Characteristics and Outcomes of Neonates With Blood Stream Infection Due to Listeria monocytogenes. Pediatr Infect Dis J. 2021;40(10):917–921. doi:10.1097/INF.0000000000003213
25. Morgand M, Leclercq A, Maury MM, et al. Listeria monocytogenes-associated respiratory infections: a study of 38 consecutive cases. Clin Microbiol Infect. 2018;24(12):1331–1339. doi:10.1016/j.cmi.2018.03.003
26. Maertens DNC, Devleesschauwer B, Maertens DNA, et al. Comorbidities and factors associated with central nervous system infections and death in non-perinatal listeriosis: a clinical case series. BMC Infect Dis. 2016;16:256.
27. Centers for Disease Control and Prevention (CDC). Vital signs: listeria illnesses, deaths, and outbreaks–United States, 2009–2011. MMWR Morb Mortal Wkly Rep. 2013;62(22):448–452.
28. Arslan F, Meynet E, Sunbul M, et al. The clinical features, diagnosis, treatment, and prognosis of neuroinvasive listeriosis: a multinational study. Eur J Clin Microbiol Infect Dis. 2015;34(6):1213–1221. doi:10.1007/s10096-015-2346-5
29. Sisó C, Goncé A, Bosch J, Salvia MD, Hernández S, Figueras F. Listeriosis in pregnancy: a secular trend in a tertiary referral hospital in Barcelona. Eur J Clin Microbiol Infect Dis. 2012;31(9):2125–2132. doi:10.1007/s10096-012-1545-6
30. Pagliano P, Attanasio V, Rossi M, et al. Listeria monocytogenes meningitis in the elderly: distinctive characteristics of the clinical and laboratory presentation. J Infect. 2015;71(1):134–136. doi:10.1016/j.jinf.2015.02.003
31. Yu W, Huang Y, Ying C, et al. Analysis of Genetic Diversity and Antibiotic Options for Clinical Listeria monocytogenes Infections in China. Open Forum Infect Dis. 2021;8(6):b177. doi:10.1093/ofid/ofab177
32. Lu B, Yang J, Gao C, et al. Listeriosis Cases and Genetic Diversity of Their L. monocytogenes Isolates in China, 2008–2019. Front Cell Infect Microbiol. 2021;11:608352. doi:10.3389/fcimb.2021.608352
33. Hansen JM, Gerner-Smidt P, Bruun B. Antibiotic susceptibility of Listeria monocytogenes in Denmark 1958–2001. Apmis. 2005;113(1):31–36. doi:10.1111/j.1600-0463.2005.apm1130105.x
34. Fischer MA, Wamp S, Fruth A, Allerberger F, Flieger A, Halbedel S. Population structure-guided profiling of antibiotic resistance patterns in clinical Listeria monocytogenes isolates from Germany identifies pbpB3 alleles associated with low levels of cephalosporin resistance. Emerg Microbes Infect. 2020;9(1):1804–1813. doi:10.1080/22221751.2020.1799722
35. Delvallez M, Carlier Y, Bout D, Capron A, Martin GR. Purification of a surface-specific soluble antigen from Listeria monocytogenes. Infect Immun. 1979;25(3):971–977. doi:10.1128/iai.25.3.971-977.1979
36. Gellin BG, Broome CV. Listeriosis. JAMA. 1989;261(9):1313–1320. doi:10.1001/jama.1989.03420090077035
37. Li W, Bai L, Ma X, et al. Sentinel Listeriosis Surveillance in Selected Hospitals, China, 2013–2017. Emerg Infect Dis. 2019;25(12):2274–2277. doi:10.3201/eid2512.180892
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.