")
Back to Journals » International Journal of General Medicine » Volume 15
Clinical and Genetic Comparison of Birt–Hogg–Dubé Syndrome (Hornstein–Knickenberg Syndrome) in Chinese: A Systemic Review of Reported Cases
Authors Zhou W, Liu K, Xu KF, Liu Y, Tian X
Received 23 January 2022
Accepted for publication 16 May 2022
Published 23 May 2022 Volume 2022:15 Pages 5111—5121
DOI https://doi.org/10.2147/IJGM.S359660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wangji Zhou,1,* Keqiang Liu,2,3,* Kai-Feng Xu,1 Yaping Liu,4 Xinlun Tian1
1Department of Pulmonary and Critical Care Medicine, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, People’s Republic of China; 2Xinhua Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Shanghai Institute of Pediatric Research, Shanghai, People’s Republic of China; 4McKusick-Zhang Center for Genetic Medicine, State Key Laboratory of Medical Molecular Biology, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinlun Tian, Department of Pulmonary and Critical Care Medicine, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, #1 Shuaifuyuan, Wangfujing, Beijing, 100730, People’s Republic of China, Tel +86 13911204657, Email [email protected] Yaping Liu, McKusick-Zhang Center for Genetic Medicine, State Key Laboratory of Medical Molecular Biology, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100005, People’s Republic of China, Email [email protected]
Background: Birt–Hogg–Dubé syndrome (BHD), also named Hornstein–Knickenberg syndrome, is a rare autosomal dominant disease characterized by lung cysts, recurrent pneumothoraxes, renal cell carcinoma and skin fibrofolliculomas.
Purpose: This study summarizes the clinical and genetic information of Chinese BHD patients from all available reported cases and explores the relationship between the clinical and genetic spectrum in the hope of improving the prognosis of Chinese BHD patients.
Methods: Relative studies were collected by searching PubMed, Cochrane Library, Embase, OVID medicine, SinoMed, Web of Science, China National Knowledge Infrastructure, Wanfang Data and China Hospital Knowledge Database from January 1, 1977 to December 31, 2021. The search strategy included the following term keys: (Birt–Hogg–Dubé syndrome OR Hornstein-Kinckenberg syndrome OR familial pulmonary cysts OR familial spontaneous pneumothorax OR fibrofolliculomas OR trichodiscomas OR inherited renal cancer syndromes OR FLCN) AND (Chinese OR China).
Results: In total, 287 Chinese patients from 143 families described in 31 references were included in this article. Chinese BHD patients tended to present more pulmonary symptoms but fewer skin lesions and renal malignancies, which appeared to be atypical when compared with Caucasian patients. The FLCN mutation spectrum among Chinese BHD patients was established with the mutational hot spot c.1285depC/delC as the most frequent mutation. In addition, this mutation spectrum also showed some differences from other races, with a relatively frequent large deletion c.872– 429_1740+1763del (exon 9– 14 deletion) reported only in Chinese individuals but no observation of the two mutational hot spots found in Japanese individuals. We also attempted to establish potential pheno-genotype correlations in Chinese BHD patients, but the results were negative.
Conclusion: To improve the prognosis of BHD patients, physicians need to increase their awareness of BHD by focusing on the family history of pneumothorax as well as skin lesions in patients with lung cysts and promptly advising patients on genetic sequencing.
Keywords: Birt–Hogg–Dubé syndrome, Chinese, FLCN, genetics, phenotype
Introduction
Birt–Hogg–Dubé syndrome (BHD), also named Hornstein–Knickenberg syndrome, is a rare autosomal dominant disease characterized by lung cysts, spontaneous pneumothorax, skin fibrofolliculomas and various types of renal tumours. In 1975, Otto P. Hornstein and Monika Knickenberg from Germany described a new autosomal dominant trait characterized by “perifollicular fibromatosis cutis”, multiple skin tags and multiple colonic polyps with proneness to cancer.1 In 1977, Arthur R. Birt, Georgina R. Hogg and W. James Dube from Canada reported a pedigree in which several family members had fibrofolliculomas with trichodiscomas and acrochordons.2 The disease “BHD” was named after the three Canadian doctors. Today, it is believed that “fibrofolliculoma” and “perifollicular fibroma” are essentially the same.3 Although BHD is more widely accepted today, we should not forget the two doctors, Otto P. Hornstein and Monika Knickenberg, who first discovered the disease.
The only known causative gene currently for BHD is the folliculin (FLCN) gene located on chromosome 17p11.2, consisting of 14 exons. FLCN encodes a tumour suppressor protein, folliculin, whose function is not fully understood. It was reported to be involved in the signalling of the mammalian target of rapamycin (mTOR) and 5′AMP-activated protein kinase (AMPK).4 More than 200 FLCN mutations have been identified5 since it was first reported in 2002,6 most of which are truncating mutations, including frameshift, nonsense, splice site mutations and large intragenic deletions.5 Germline insertion or deletion of a cytosine in the hypermutable polycytosine (C8) tract in exon 11 has been detected as the most common mutation in several different countries or races,7–9 including previously reported Chinese BHD cohorts.10,11
Compared with Caucasians and Japanese, there are fewer clinical and genetic studies about BHD patients of Chinese origin. Recently, Hu et al reviewed the epidemiology and clinical characteristics of 120 Chinese BHD families and found that Chinese patients reported more pulmonary cysts and recurrent pneumothorax and fewer skin lesions and renal tumours than USA and Japanese BHD cohorts.12 However, the research did not systematically describe the genetic spectrum of Chinese BHD patients. In this systematic review, we summarize the clinical and genetic information of Chinese BHD patients from all available reported cases and explore the relationship between clinical and genetic spectrum in the hope of increasing the awareness of BHD by Chinese physicians and thus improving the prognosis of Chinese BHD patients.
Materials and Methods
Information Sources and Search Strategies
Relevant studies were collected by searching PubMed, Cochrane library, Embase, OVID medicine, SinoMed, Web of Science, China National Knowledge Infrastructure, Wanfangdata and China Hospital Knowledge Database from January 1, 1977 to December 31, 2021. The search strategy included the following term keys: (Birt–Hogg–Dubé syndrome OR Hornstein–Knickenberg syndrome OR familial pulmonary cysts OR familial spontaneous pneumothorax OR fibrofolliculomas OR trichodiscomas OR inherited renal cancer syndromes OR FLCN) AND (Chinese OR China). Publications were limited to HUMAN, written in English or Chinese. Study types were limited to clinical trials, meta-analyses, randomized controlled trials, case reports, case series or reviews. In addition, we reviewed the references of included articles as a supplement to relevant articles not included in the initial search.
Study Selection
Two reviewers (WZ and KL) independently conducted the initial search and the eligibility assessment. They screened out the relevant studies according to the titles and abstracts of all articles. Disagreements were resolved by consensus among all authors. Then, full-text articles were assessed for eligibility by the authors.
Inclusion and Exclusion Criteria
Original articles were included if they met the following inclusion criteria: 1) diagnosis in accordance with BHD (see below); 2) patients of Chinese descent; and 3) clinical or genetic data available in the full text.
The exclusion criteria were as follows: 1) duplicate publications; 2) interim or extension findings of the same study or with duplicate patients; and 3) studies without detailed clinical and genetic data.
Data Collection
Data were extracted from all eligible articles using standardized Excel forms. Included data were: 1) basic information of studies: publication year, first author name, corresponding author department, study location, title, journal name; 2) clinical symptoms: a) basic information of patients: gender, age at diagnosis, family history, smoking history; b) pulmonary manifestations: pneumothorax history, age at first pneumothorax, number and location of pneumothorax episodes, pulmonary cysts history, location, number and maximum diameter of pulmonary cysts; c) skin manifestations: types of skin lesions (fibrofolliculoma or others), location and number of skin lesions; d) renal manifestations: types of renal lesions (renal cysts, renal tumours and their pathological types), age at diagnosis of renal disease; e) other relevant manifestations; 3) FLCN mutations: details about genetic screening of FLCN including nucleotide change, amino acid change and screening method.
Diagnosis of Birt–Hogg–Dubé Syndrome
According to the criteria proposed by the European BHD Consortium in 2009,13 BHD diagnosis will be made if a patient fulfils one major or two minor criteria. Major criteria: 1) at least five fibrofolliculomas or trichodiscomas, at least one histologically confirmed, of adult onset; 2) pathogenic FLCN germline mutation. Minor criteria: 1) multiple lung cysts: bilateral basally located lung cysts with no other apparent cause, with or without spontaneous primary pneumothorax; 2) renal cancer: early onset (<50 years) or multifocal or bilateral renal cancer, or renal cancer of mixed chromophobe and oncocytic histology; 3) a first-degree relative with BHD.
Mutation Nomenclature
Mutation information was collected from the original publications and rechecked manually. Wrong variant descriptions or legacy names were reconciled according to the HGVS (Human Genome Variation Society) recommendations.14 The mutation positions were recorded according to the transcript reference NM_144997.6. Mutations were described at both the DNA and protein levels.
Data Analysis
Data analysis was conducted using SPSS version 22.0 software (IBM SPSS, USA). All continuous variables were evaluated for a normal distribution with a Kolmogorov–Smirnov test. Parametric data are presented as the mean ± standard deviation, and nonparametric data are presented as the median and extreme values. Categorical variables are presented as either a percentage of the total or as absolute values. The chi-square test was used to compare categorical variables. Differences with a value of P<0.05 were considered statistically significant. To avoid potential bias caused by different reporting methods (eg, case reports with several mutation-positive patients in the same family vs cohort studies with only the proband’s mutation information available in each family), the variant frequency and percentages were calculated based on the data of the probands but not all reported patients.
Results
The process of study searching and including is shown in Figure 1. In total, 287 Chinese patients from 143 families described in 31 references were included in this article. Among them, 267 were from mainland China, 12 were from Hong Kong, China, and 8 were from Taiwan, China.10,11,15–43
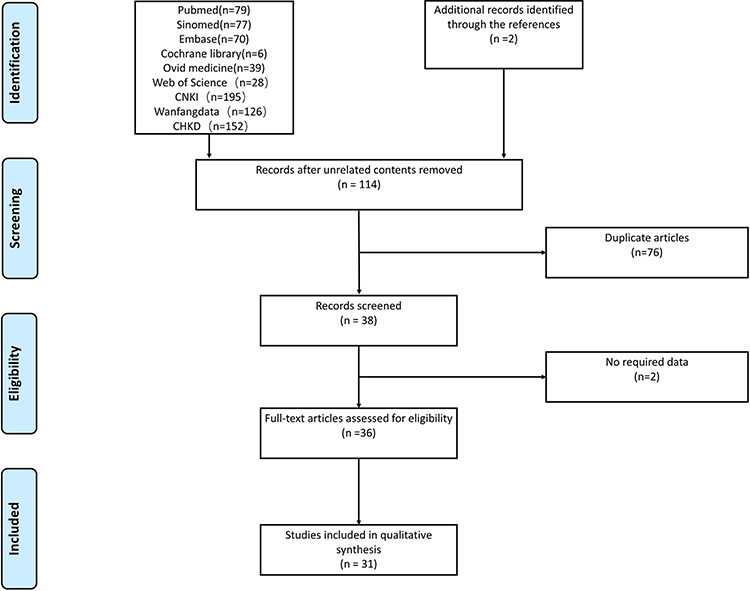 |
Figure 1 Trial inclusion and exclusion flow chart. Using (Birt–Hogg–Dubé syndrome OR Hornstein-Knickenberg syndrome OR familial pulmonary cysts OR familial spontaneous pneumothorax OR fibrofolliculomas OR trichodiscomas OR inherited renal cancer syndromes OR FLCN) AND (Chinese OR China) as the key words, limited to full text, 774 records were retrieved from PubMed, Cochrane library, Embase, OVID medicine, SinoMed, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfangdata and China Hospital Knowledge Database (CHKD). A total of 660 unrelated articles, 76 duplicate articles, 2 articles without required data and 5 articles reporting duplicated cases were excluded. |
Basic Information of Chinese BHD Patients
Certain details about the sex of 13 patients20,35 and family history of 3 patients10 were not available in the full text. Among the 274 patients, 160 were female, and 114 were male (F/M=1.40). A total of 255 patients had a definite family history of pneumothorax or lung cysts (255/284, 89.8%). The average age at diagnosis was 46.9 ± 14.4 years old (range, 8 to 84). Among the patients whose smoking history was known, 36 (36/179, 20.1%) patients were smoking at present or in the past, ranging from 5 to 40 pack-years.
Clinical Manifestations of Chinese BHD Patients
Pulmonary Manifestations
Among all clinical manifestations, pulmonary manifestations were the most common in Chinese patients (273/282, 96.8%). Of them, 202 patients (202/275, 73.5%) had at least one episode of pneumothorax, and the average age at first pneumothorax was 39.2 ± 12.9 years old (range, 15 to 71). Until diagnosis, the number of pneumothorax episodes was up to 6 times, with an average of 1.8 times. No tendency for pneumothorax episodes to occur was recognized. Of the 89 pneumothoraxes in which the location of occurrence was recorded, 40 occurred on the left side and 49 on the right side. Out of the 248 patients who underwent chest computed tomography scans, 234 (234/248, 94.4%) had lung cysts. Specific information on pulmonary cysts was not described in all articles. Of the 116 records on the location of the pulmonary cysts, bilateral was mentioned in 87 (87/116, 75.0%). In this study, we defined three or more cysts as multiple cysts. Of the 99 records on the number of pulmonary cysts, multiple cysts were mentioned in 92 of the cases (92/99, 92.9%). Five patients had one bullae, and two patients had two bullae. The maximum diameter of the pulmonary cyst was mentioned in only 35 records, and it ranged from 1 to 12 centimetres.
Cutaneous Manifestations
Fifty-one (51/229, 22.3%) patients were reported to have skin manifestations. However, only 6 (6/51, 11.8%) cases were confirmed as fibrofolliculoma by pathology, and 34 (34/51, 66.7%) cases showed fibrofolliculoma-like changes (multiple, dome-shaped, whitish papules on the face, neck or trunk),13 which were not confirmed by histology. Fat granules and sarcoma cutis had one case each.
Renal Manifestations
Regarding renal manifestations, 221 of 287 patients underwent abdominal computed tomography scan or ultrasound, and renal cell carcinoma (RCC) was diagnosed in 16 cases (16/221, 7.2%). Among the 16 RCC patients, 6 cases of clear cell RCC, 3 cases of chromophobe RCC, 1 case of mixed pattern of chromophobe RCC and oncocytoma and 1 case of papillary RCC were found. Detailed pathological results of RCC in the remaining 5 patients were unavailable. For 9 RCC patients with a recorded age at diagnosis, the age at diagnosis of BHD was exactly the same as that of RCC, with an average age of 51.2 ± 11.5 years old (range, 37 to 67). There were also 19 (19/221, 8.6%) cases of renal cysts and 3 (3/221, 1.4%) cases of renal hamartoma in Chinese BHD patients.
Other Manifestations
We also found 2 cases of papillary thyroid carcinoma21 and 4 cases of liver cysts24,32 among Chinese BHD patients. Detailed information on the clinical features of the 279 Chinese BHD patients is summarized in Table 1.
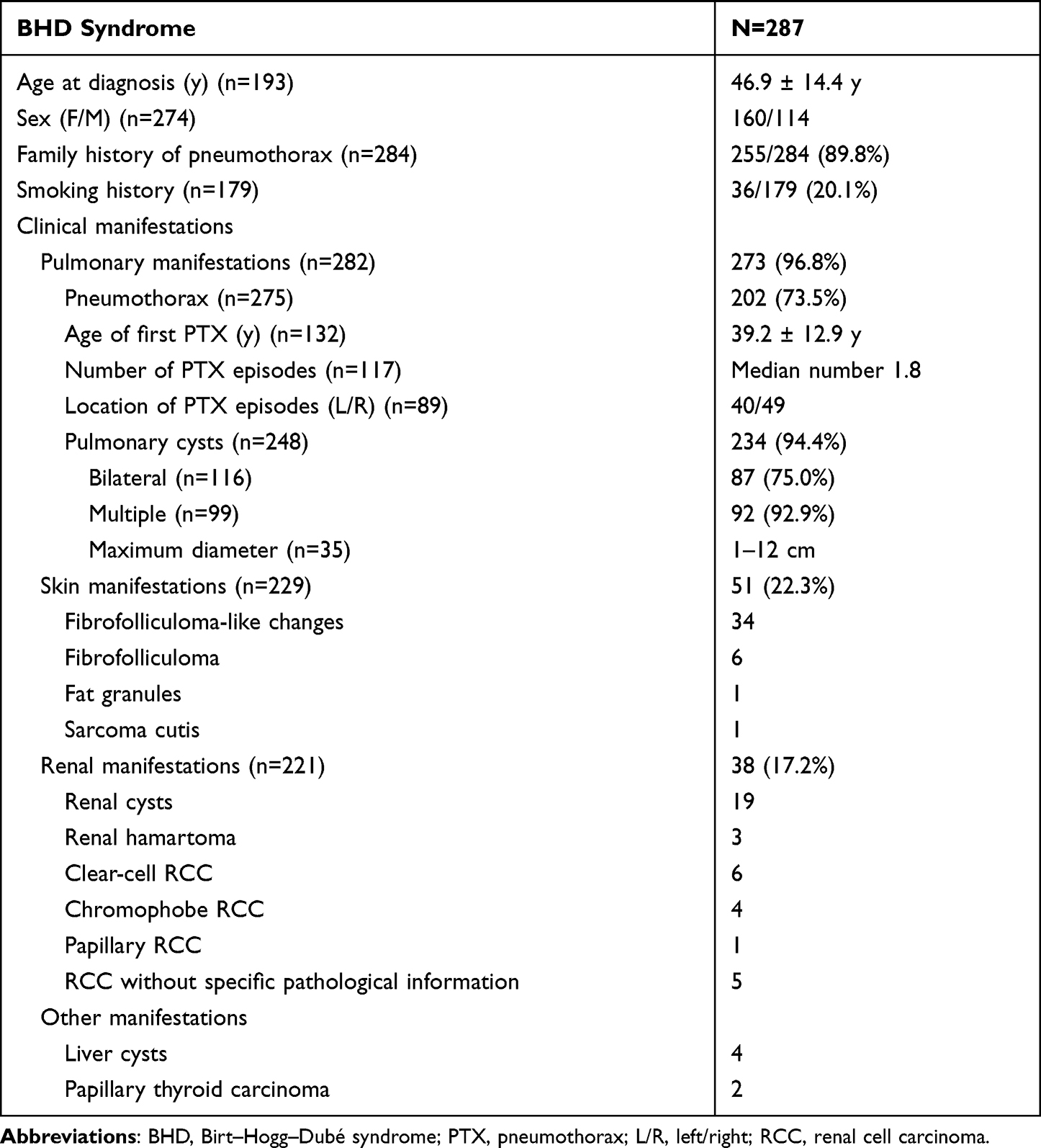 |
Table 1 Clinical Manifestations of Chinese BHD Patients |
FLCN Variant Spectrum Among Chinese BHD Patients
According to the Human Genome Mutation Database (HGMD), over 200 FLCN mutations have been reported in BHD patients around the world. In this review, a total of 120 probands were reported to have definitive FLCN mutations. In total, 63 distinct FLCN mutations were identified in Chinese patients. Among all these mutations, the 1-bp deletion or duplication (c.1285delC/dupC) within the polyC5 tract in exon 11 was found to be the most frequent mutation among Chinese BHD patients, with a frequency of 25.0% (30/120). In addition, three mutations were observed in five probands (4.2% for each, 5/120), including c.1579_1580insA (p. R527Qfs*75), c.469_471delTTC (p. F157del) and gross deletion of exon 9–14 (ΔE9–14), and two mutations were observed in four probands (3.3% for each, 4/120), including c.1015C>T (p. Q339*) and c.1156_1175del20 (p.S386Dfs*63). Variants reported more than once in Chinese BHD patients are listed in Table 2. For the full list of reported FLCN variants in Chinese patients, see supplementary material Table S1.
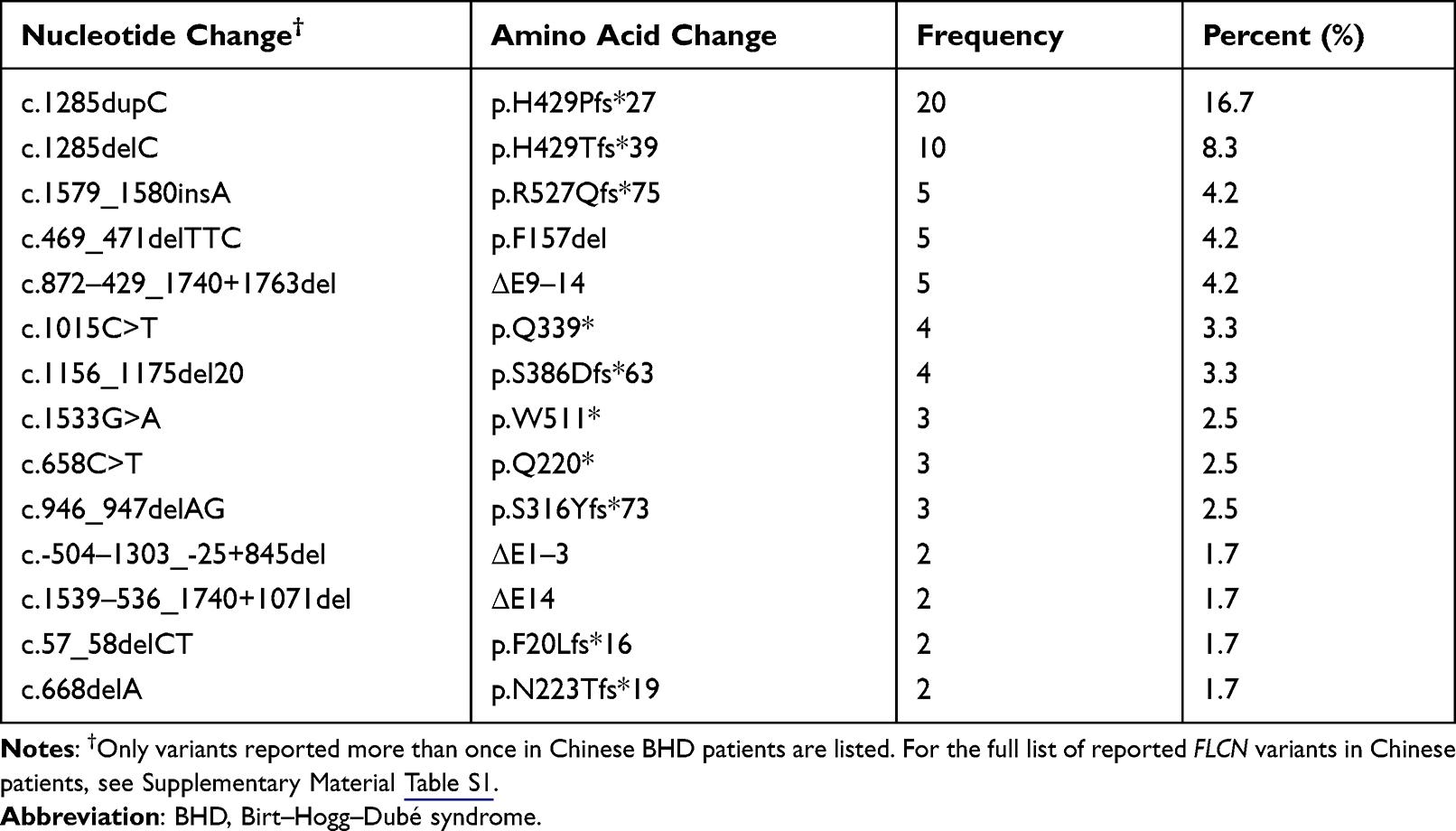 |
Table 2 Frequency of FLCN Mutations Among Chinese BHD Patients |
Most of the mutations are truncating mutations, including nonsense, frameshift, splicing mutation and gross deletion, with a total frequency of 87.5% (105/120), which are predicted to cause premature terminal codons and complete loss of function of folliculin. Moreover, there is a synonymous mutation c.1287C > T (p. His429=) reported, which was classified as a variant of uncertain significance.10
Comparison of Clinical and Genetic Spectrum in Chinese BHD Patients
To establish potential pheno-genotype correlations in Chinese BHD patients, we compared the clinical manifestations of patients carrying frequent FLCN mutations (observed more than 5 times) (Table 3). However, no statistically significant difference was observed for these mutations (χ2, 6.495; P value, 0.09).
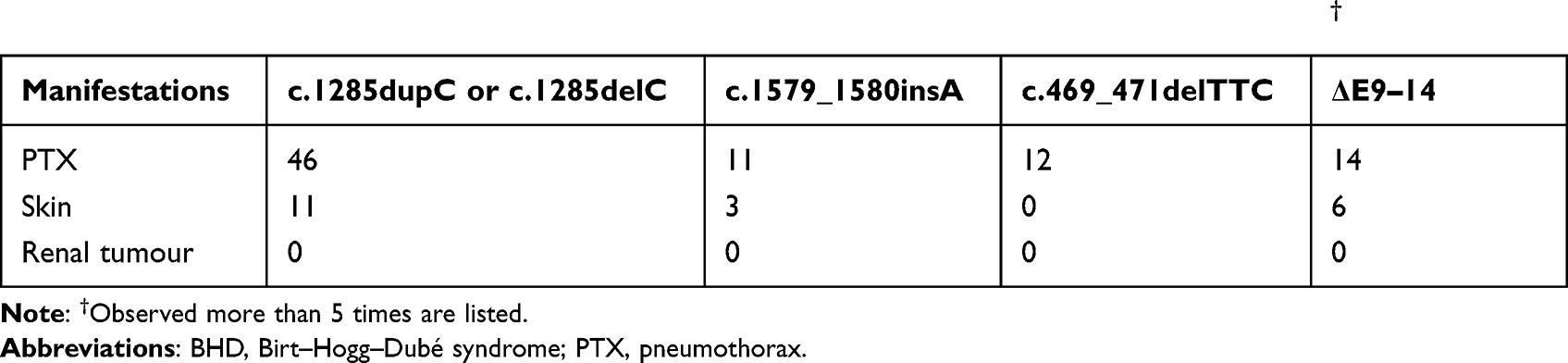 |
Table 3 Clinical Manifestations of Chinese BHD Patients Carrying Frequent FLCN Mutations† |
Discussion
In this systematic review, we summarized the clinical and genetic characterizations of Chinese BHD patients based on the available information of 287 reported cases from 143 families. To the best of our knowledge, our study included the largest number of BHD patients and families in a Chinese population.
Typical symptoms of BHD include recurrent pneumothorax, multiple pulmonary cysts, fibrofolliculomas and renal cell carcinomas. Nevertheless, those symptoms usually appear separately and atypically. In our study, only 1 (1/287, 0.3%) patient had all four typical symptoms mentioned above.16 In addition to insufficient awareness of the disease, physicians tend to treat each symptom individually and might ignore the presence of BHD, which leads to a high rate of misdiagnosis and missed diagnosis.
The most commonly affected system in Chinese BHD patients is the respiratory system, with frequencies of 94.4% and 73.5% for lung cysts and pneumothorax, respectively. A family history of pneumothorax or lung cysts is an important clue to suggest the diagnosis of BHD. In our study, 89.8% of patients had a definite family history of pneumothorax or lung cysts.
In contrast, the prevalence of lung cysts is reported to be lower in Caucasian BHD patients (84–89.4%), and only approximately one-third (24–38%) of patients reported a history of spontaneous pneumothorax.8,44,45 There was no significant difference between Chinese (median age: 39.2 y, range 15–71 y) and Caucasian (median age: 38 y, range 22–71 y)44 patients in the age of first pneumothorax. Compared with previous studies in Japan and South Korea, the incidence of pneumothorax and pulmonary cysts in Chinese patients in our study was similar, which is significantly higher than that in the Caucasian population.9,46,47 This suggests that East Asian BHD patients may indeed have a higher proportion of pneumothorax occurrence and pulmonary involvement.
In addition to racial differences, this difference may also be related to the department of the researcher. Previous studies have reported that the incidence of spontaneous pneumothorax in BHD patients in pulmonary cohorts (42–76%) is approximately twice that in renal/dermatologic cohorts (23–38%) (6). In our study, similar conclusions were found. The incidence of spontaneous pneumothorax in BHD patients in the pulmonary cohorts (82.8%) was higher than that in the renal cohorts (50%). Among the 31 corresponding authors of the references included in this article, 11 were from the Department of Respiratory Medicine, 7 were from the Department of Thoracic Surgery, 4 were from the Department of Urology Surgery and 9 were from other departments. More than half (18/31, 58.1%) were chest doctors. Therefore, the presence of reporting bias between different departments may have contributed to the high incidence of pulmonary symptoms in our study.
As the most common symptoms reported among Caucasian patients (79.1–93%),8,44,45 cutaneous findings were much less frequently observed in Chinese patients, with a percentage of only 22.3%. It is noteworthy that only six (6/51, 11.8%) of the 51 patients with skin lesions underwent histological examination, while most patients (34/51, 66.7%) only had fibrofolliculoma-like changes without a histological examination. In contrast, more than half (26/46, 57%) of the Caucasian patients with skin lesions underwent histological examination.44 Considering that respiratory and skin manifestations can occur independently, although most BHD patients in China are treated with respiratory manifestations, it does not mean that there will be fewer skin manifestations. Therefore, there are differences in the incidence of skin lesions between Chinese and Western BHD patients. Beyond race, the fewer cutaneous findings in Chinese patients may be partly due to doctors’ inadequate awareness of BHD and thus ignoring the existence of skin lesions. Moreover, skin biopsy is an invasive procedure, and neither doctors nor patients are willing to carry out the examination. It is particularly important for doctors to improve the understanding of BHD to find the characteristic skin lesions and more actively conduct histological examinations to diagnose BHD.
According to relevant studies, Caucasian BHD patients have a higher risk of renal tumours (12–34%).8,44,45 Chromophobe renal cell carcinoma and a mixed pattern of chromophobe and oncocytic renal cell carcinoma are typical in patients with BHD.13 However, malignant renal tumours were diagnosed in only 7.2% (16/221) of patients in our analysis, and the typical chromophobe RCC was rare in 4 cases. Despite the potential selection bias that most BHD patients visited a doctor specifically for lung cysts or pneumothorax in China, malignant renal tumours were rarely detected in Chinese FLCN mutation carriers. As the most serious clinical manifestation of BHD, screening for renal tumours at the time of diagnosis or from the age of 20 years is crucial to improve the prognosis.48 However, only 9 patients16,18,21,24,29,37,38 in our analysis who had a record age of diagnosis of renal cancer were also diagnosed with BHD within one year. Most of these patients were considered to have BHD because of pulmonary cysts or a history of pneumothorax on routine screening at the time of renal cancer surgery. If we can diagnose BHD as soon as possible, we will be more alert to renal tumours and thus improve the prognosis of patients. There are 23.0% of Chinese BHD patients who are not routinely screened for renal tumours, perhaps making renal tumours underdiagnosed. In addition, given that most of the articles included in this study are cross-sectional studies, renal tumours may occur after the diagnosis of BHD, which may also underestimate their incidence rate.
The clinical manifestations of BHD patients in different populations are summarized in Table 4. From the clinical manifestations in Chinese BHD patients mentioned above, we found that Chinese BHD patients have different clinical features from Caucasians, with more pulmonary manifestations but fewer skin lesions and renal malignancy, which is consistent with the conclusion of the study by Hu et al.12 In contrast, in addition to the various bias factors mentioned above, we also tried to understand whether there are differences in the genotypes among different races, which might explain the atypical phenotypes of Chinese BHD patients compared with Caucasians.
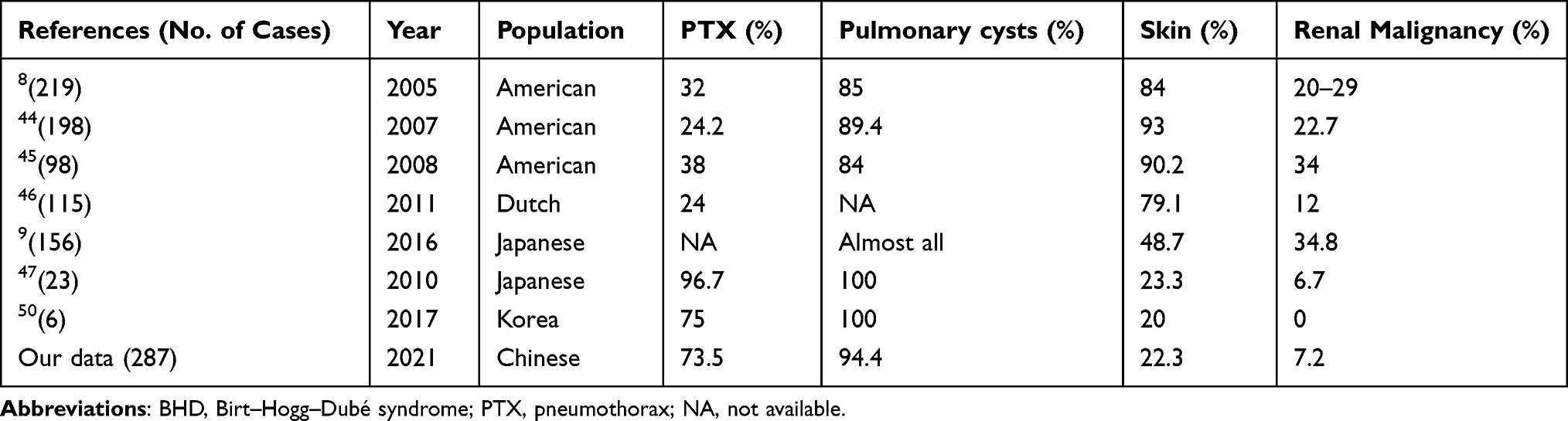 |
Table 4 Clinical Manifestations of BHD Patients in Different Populations |
In 2002, FLCN was first reported as the pathogenic gene of BHD syndrome,6,49 thus making genetic screening an effective method for BHD diagnosis. The FLCN mutation spectrum has been well established in Caucasian populations8,44 and in some Asian populations, such as the Japanese population.9 In this review, we established the FLCN mutation spectrum among Chinese patients based on a relatively large BHD population of 120 probands. Our data show that the previously reported mutational hot spot, c.1285dupC/delC, is also the most common mutation in Chinese BHD patients, with a similar frequency (25.0%). However, there are also some differences between this spectrum and others. First, more than half of the mutations identified in Chinese patients have never been reported in other races before.10,11 Second, the other two mutational hot spots c.1533_1536delGATG (20.8%) and c.1347_1353dupCCACCCT (15.8%) reported in Japanese patients were not observed in Chinese patients. Third, there is a relatively common large deletion c.872–429_1740+1763del (ΔE9–14, 4.2%) found in our patients, which shares a common disease haplotype back to approximately 16 generations ago, suggesting a founder effect.26 However, this mutation has never been reported in other populations, except one report in a Japanese BHD patient, for which the exact breakpoints were not determined. Collectively, these characteristics demonstrate the variability of the FLCN mutation spectrum between Chinese and other races.
Despite the different mutation spectrum, most FLCN mutations found in Chinese patients are truncating mutations, which is consistent with Caucasians45 and Japanese Asians.9 These mutations all result in complete loss of folliculin function, thereby causing BHD syndrome. Thus, the different phenotypes between BHD patients of Chinese and other origins cannot be explained by the FLCN genotype per se. Genomic background, environmental factors and gene–environment interactions might contribute to this lack of correlation. This speculation certainly needs further studies to be verified in a much larger collection of patients with BHD from different ethnic backgrounds.
In addition, we also attempted to establish potential pheno-genotype correlations in Chinese BHD patients. We compared the clinical features of patients carrying frequent FLCN mutations (observed more than 5 times), but no statistically significant differences were observed for all these mutations. It is important to emphasize that, unlike the study by Hu et al, to avoid potential bias caused by different reporting modalities, the FLCN variant frequency and percentages were calculated based on the probands when describing the genetic spectrum, which was detailed in the previous data analysis section. While describing the relationship between phenotype and genotype here, we counted the number of all patients with specific mutations. We believe that such a differential treatment is more consistent with the actual situation.
It is worth noting that there were 12 gross deletions reported in Chinese BHD patients, accounting for 10% of all mutations. In particular, Ding et al collected 12 unrelated primary spontaneous pneumothorax patients with no FLCN sequence mutation detected by Sanger sequencing. A multiplex ligation-dependent probe amplification (MLPA) assay allowed them to identify large FLCN intragenic deletions in 9 of them (75%, 9/12).26 Further characterization of the deletion breakpoints showed that the breakpoints were all located in Alu repeats.26 Similarly, Liu et al detected a 3.6 kb deletion encompassing the entire exon 1 in a Chinese BHD patient, which was also flanked by Alu repeat elements on both sides.10 Thus, Alu element-mediated FLCN intragenic gross deletion could be an important cause of BHD syndrome, and MLPA analysis should be considered an important genetic test complementary to Sanger sequencing for the genetic diagnosis of BHD syndrome.
As mentioned above, the vast majority of reported FLCN mutations are loss-of-function mutations, including nonsenses, frameshifts, splice site mutations and gross genomic rearrangements. These mutations often result in truncated protein or complete absence of folliculin, thereby causing BHD syndrome. In contrast, missense mutations or in-frame insertions/deletions are rarely reported, with a frequency of 11.7% reported in Chinese BHD patients. Similar results were reported in previous studies.5,9 To determine the pathogenicity of these mutations, Nahorski et al transiently expressed mutant folliculin with missense mutation or in-frame deletions in the FTC-133 cell line and found that most of these nontruncating mutations significantly disrupted the stability of the folliculin protein. Moreover, we previously investigated the potential effects of FLCN nontruncating mutations on mRNA processing by a systematic in vitro minigene assay.10 The results showed that none of the 21 nontruncating mutations disrupted the splicing pattern, which in turn supports that these mutations cause BHD syndrome by disrupting folliculin protein stability.
This article systematically reviewed the reported cases but lacks follow-up information. Due to the small number of patients and varying degrees of bias, the relative rates of occurrence of various characteristics of BHD patients in China are uncertain.
Conclusion
Chinese BHD patients have different clinical features from Caucasians, with more pulmonary manifestations but fewer skin lesions and renal malignancies. Despite the common mutational hot spot, the FLCN mutation spectrum among Chinese BHD patients shows some variability from other races. We attempted to establish potential pheno-genotype correlations in Chinese BHD patients, but the results were negative. To detect more Chinese-origin BHD patients and improve their prognosis, physicians need to increase awareness of BHD by focusing on the family history of pneumothorax as well as skin lesions in all patients with pulmonary cysts and timely advise patients to undergo genetic sequencing for the FLCN gene.
Abbreviations
BHD, Birt–Hogg–Dubé syndrome; FLCN, folliculin; RCC, renal cell carcinoma.
Funding
This work was supported by the “CAMS Innovation Fund for Medical Sciences” (CIFMS 2018-I2 M-1-003, CIFMS-2020-I2 M-C&T-B-002 and CIFMS 2016-I2 M-1-002) and the “National Key Research and Development Program of China” (2016YFC0901502).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hornstein OP, Knickenberg M. Perifollicular fibromatosis cutis with polyps of the colon–a cutaneo-intestinal syndrome sui generis. Arch Dermatol Res. 1975;253(2):161–175. doi:10.1007/BF00582068
2. Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol. 1977;113(12):1674–1677. doi:10.1001/archderm.1977.01640120042005
3. Happle R. Hornstein-Knickenberg syndrome vs. Birt-Hogg-Dubé syndrome: a critical review of an unjustified designation. J Eur Acad Dermatol Venereol. 2020;34(4):885–887. doi:10.1111/jdv.16190
4. Schmidt LS, Linehan WM. FLCN: the causative gene for Birt-Hogg-Dubé syndrome. Gene. 2018;640:28–42. doi:10.1016/j.gene.2017.09.044
5. Lim DH, Rehal PK, Nahorski MS, et al. A new locus-specific database (LSDB) for mutations in the folliculin (FLCN) gene. Hum Mutat. 2010;31(1):E1043–1051. doi:10.1002/humu.21130
6. Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell. 2002;2(2):157–164. doi:10.1016/S1535-6108(02)00104-6
7. Khoo SK, Giraud S, Kahnoski K, et al. Clinical and genetic studies of Birt-Hogg-Dubé syndrome. J Med Genet. 2002;39(12):906–912.
8. Schmidt LS, Nickerson ML, Warren MB, et al. Germline BHD-mutation spectrum and phenotype analysis of a large cohort of families with Birt-Hogg-Dubé syndrome. Am J Hum Genet. 2005;76(6):1023–1033.
9. Furuya M, Yao M, Tanaka R, et al. Genetic, epidemiologic and clinicopathologic studies of Japanese Asian patients with Birt-Hogg-Dubé syndrome. Clin Genet. 2016;90(5):403–412.
10. Liu K, Xu W, Tian X, et al. Genotypic characteristics of Chinese patients with BHD syndrome and functional analysis of FLCN variants. Orphanet J Rare Dis. 2019;14(1):223. doi:10.1186/s13023-019-1198-y
11. Liu Y, Xu Z, Feng R, et al. Clinical and genetic characteristics of Chinese patients with Birt-Hogg-Dubé syndrome. Orphanet J Rare Dis. 2017;12(1):104. doi:10.1186/s13023-017-0656-7
12. Hu X, Zhang G, Chen X, Xu KF. Birt-Hogg-Dubé syndrome in Chinese patients: a literature review of 120 families. Orphanet J Rare Dis. 2021;16(1):223. doi:10.1186/s13023-021-01848-8
13. Menko FH, van Steensel MA, Giraud S, et al. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol. 2009;10(12):1199–1206. doi:10.1016/S1470-2045(09)70188-3
14. Den Dunnen JT, Dalgleish R, Maglott DR, et al. HGVS recommendations for the description of sequence variants: 2016 update. Hum Mutat. 2016;37(6):564–569. doi:10.1002/humu.22981
15. Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin Genet. 2008;74(2):178–183. doi:10.1111/j.1399-0004.2008.01030.x
16. Han J, Hao J, Liu R, Xie Y, Kang Z. Birt-Hogg-Dubé syndrome caused by a mutation of FLCN gene in a CVST patient: a case report. Int J Neurosci. 2020;130(5):438–442. doi:10.1080/00207454.2019.1691204
17. Hou X, Zhou Y, Peng Y, et al. Birt-Hogg-Dubé syndrome in two Chinese families with mutations in the FLCN gene. BMC Med Genet. 2018;19(1):14. doi:10.1186/s12881-017-0519-z
18. Lin Z, Gong K, Pang B, Zeng C, Zhang D. Birt-Hogg-Dubé syndrome with clear cell renal cell carcinoma in a Chinese family. Intern Med. 2014;53(24):2825–2828. doi:10.2169/internalmedicine.53.2814
19. Hao S, Long F, Sun F, Liu T, Li D, Jiang S. Birt-Hogg-Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN mutation. BMC Pulm Med. 2017;17(1):43. doi:10.1186/s12890-017-0383-9
20. Luk HM, Tong TM, Lo IF. Birt-Hogg-Dube syndrome: a rare cause of familial spontaneous pneumothorax. Hong Kong Med J. 2017;23(4):
21. Dong L, Gao M, Hao WJ, et al. Case report of Birt-Hogg-Dubé syndrome: germline mutations of FLCN detected in patients with renal cancer and thyroid cancer. Medicine. 2016;95(22):e3695. doi:10.1097/MD.0000000000003695
22. Sze ECW, Lai AWK, Sin KM. A case series of hereditary cystic lung disease in a Chinese family. Respirology. 2017;22:23–24.
23. Xing H, Liu Y, Jiang G, et al. Clinical and genetic study of a large Chinese family presented with familial spontaneous pneumothorax. J Thorac Dis. 2017;9(7):1967–1972. doi:10.21037/jtd.2017.06.69
24. Liu L, Yang K, Wang X, et al. Detection of folliculin gene mutations in two Chinese families with Birt-Hogg-Dube syndrome. Biomed Res Int. 2017;2017:8751384. doi:10.1155/2017/8751384
25. Liu Y, Xing H, Huang Y, Meng S, Wang J. Familial spontaneous pneumothorax: importance of screening for Birt-Hogg-Dubé syndrome. Eur J Cardio-Thoracic Surg. 2020;57(1):39–45. doi:10.1093/ejcts/ezz171
26. Ding Y, Zhu C, Zou W, et al. FLCN intragenic deletions in Chinese familial primary spontaneous pneumothorax. Am J Med Genet A. 2015;167a(5):1125–1133. doi:10.1002/ajmg.a.36979
27. Yang GG, Chiang CC. Recurrent spontaneous pneumothoraces. Am J Respir Crit Care Med. 2013;188(1):e1–2. doi:10.1164/rccm.201206-0981IM
28. Zhu JF, Shen XQ, Zhu F, Tian L. Novel folliculin (FLCN) mutation and familial spontaneous pneumothorax. Qjm. 2017;110(1):23–26. doi:10.1093/qjmed/hcw109
29. Li T, Ning X, He Q, Gong K. Novel germline mutations in FLCN gene identified in two Chinese patients with Birt-Hogg-Dubé syndrome. Chin J Cancer. 2017;36(1):4. doi:10.1186/s40880-016-0172-5
30. Zheng CM, Hu XX, Gao YL, Miao JB, Li H. Recurrent primary spontaneous pneumothorax in a large Chinese family: a clinical and genetic investigation. Chin Med J. 2019;132(20):2402–2407. doi:10.1097/CM9.0000000000000442
31. So SY. Spontaneous pneumothorax due to Birt-Hogg-Dube syndrome in a Chinese family. Respirology. 2009;14(5):775–776. doi:10.1111/j.1440-1843.2009.01558.x
32. Guo T, Shen Q, Ouyang R, et al. The clinical characteristics of East Asian patients with Birt-Hogg-Dubé syndrome. Ann Transl Med. 2020;8(21):1436. doi:10.21037/atm-20-1129
33. Zong D, Li J, Liu X, Guo T, Ouyang R. Identification of a novel pathogenic folliculin variant in a Chinese family with Birt-Hogg-Dubé syndrome (Hornstein-Knickenberg Syndrome). Front Genet. 2020;11:565566. doi:10.3389/fgene.2020.565566
34. HUXiaowen SGFW. Recurrent pneumothorax with diffuse cystic lesions in both lungs: a case report. Chin J Lung Dis. 2019;12(02):241–243.
35. Zhang Q, Zhu CC. Mutation screening of FLCN gene in Chinese patients with sporadic and familial primary spontaneous pneumothorax. Chin J Thorac Cardiovasc Surg. 2011;07:426–430.
36. Ren DQ, Xiao BH, Wang SH, Zhang P. CT findings of pulmonary lesions in Birt-Hogg-Dubé syndrome: an analysis of 8 cases and literature review. J QINGDAO UNIV. 2018;54(06):
37. Xie F. A case of Birt-Hogg-Dubé syndrome with renal hybrid oncocytic /chromophobe tumors. Med J Peking Union Med Coll Hospital. 2019;10(02):162–165.
38. Ma SZ, Xie ZK, Yang H, et al. A case report of Birt-Hogg-Dubé syndrome. Chin J Uro. 2019;05:390.
39. Liu Z, Xu KF, Hu C, et al. Use of whole-exome sequencing for the diagnosis of atypical Birt-Hogg-Dubé syndrome. J Genet Genom. 2014;41(8):449–451. doi:10.1016/j.jgg.2014.06.005
40. Yang CY, Chen JS, Yu CJ. Isolated familial pneumothorax in a Taiwanese family with Birt-Hogg-Dubé syndrome. J Postgrad Med. 2013;59(4):321–323. doi:10.4103/0022-3859.123169
41. Ren S, Luo C, Wang Y, et al. Birt-Hogg-Dubé syndrome with rare unclassified renal cell carcinoma: a case report. Medicine. 2021;100(51):e28380. doi:10.1097/MD.0000000000028380
42. Cai M, Zhang X, Fan L, et al. A novel FLCN intragenic deletion identified by NGS in a BHDS family and literature review. Front Genet. 2021;12:636900. doi:10.3389/fgene.2021.636900
43. Lu YR, Yuan Q, Liu J, et al. A rare occurrence of a hereditary Birt-Hogg-Dubé syndrome: a case report. World J Clin Cases. 2021;9(24):7123–7132. doi:10.12998/wjcc.v9.i24.7123
44. Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med. 2007;175(10):1044–1053. doi:10.1164/rccm.200610-1483OC
45. Toro JR, Wei MH, Glenn GM, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet. 2008;45(6):321–331. doi:10.1136/jmg.2007.054304
46. Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer. 2011;105(12):1912–1919. doi:10.1038/bjc.2011.463
47. Kunogi M, Kurihara M, Ikegami TS, et al. Clinical and genetic spectrum of Birt-Hogg-Dube syndrome patients in whom pneumothorax and/or multiple lung cysts are the presenting feature. J Med Genet. 2010;47(4):281–287. doi:10.1136/jmg.2009.070565
48. Stamatakis L, Metwalli AR, Middelton LA, Marston Linehan W. Diagnosis and management of BHD-associated kidney cancer. Fam Cancer. 2013;12(3):397–402. doi:10.1007/s10689-013-9657-4
49. Daccord C, Good JM, Morren MA, Bonny O, Hohl D, Lazor R. Birt-Hogg-Dubé syndrome. Eur Respir Rev. 2020;29:157. doi:10.1183/16000617.0042-2020
50. Park HJ, Park CH, Lee SE, et al. Birt-Hogg-Dube syndrome prospectively detected by review of chest computed tomography scans. PLoS One. 2017;12(2):e0170713. doi:10.1371/journal.pone.0170713
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.