")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Clinical and Functional Effects of Inhaled Dual Therapy Umeclidinium/Vilanterol in Patients with Chronic Obstructive Pulmonary Disease: A Real-Life Study
Authors Pelaia C , Ferrante Bannera A, Rotundo FL, Tropea FG, Armentaro G , Maglio A, Sciacqua A, Vatrella A , Pelaia G
Received 4 February 2023
Accepted for publication 22 May 2023
Published 26 May 2023 Volume 2023:18 Pages 995—1002
DOI https://doi.org/10.2147/COPD.S407238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Corrado Pelaia,1 Anna Ferrante Bannera,1 Fioramante Lello Rotundo,1 Francesco Giuseppe Tropea,1 Giuseppe Armentaro,2 Angelantonio Maglio,3 Angela Sciacqua,2 Alessandro Vatrella,3 Girolamo Pelaia1
1Department of Health Sciences, University “Magna Græcia” of Catanzaro, Catanzaro, Italy; 2Department of Medical and Surgical Sciences, University “Magna Græcia” of Catanzaro, Catanzaro, Italy; 3Department of Medicine, Surgery and Dentistry, University of Salerno, Salerno, Italy
Correspondence: Corrado Pelaia, Campus Universitario “S. Venuta”, Viale Europa – Località Germaneto, Catanzaro, 88100, Italy, Tel +39 0961 3647007, Fax +39 0961 3647193, Email [email protected]
Background: The pharmacological association umeclidinium/vilanterol (UMEC/VI) allows to implement a very effective dual bronchodilation in chronic obstructive pulmonary disease (COPD), thus optimizing bronchodilating therapy.
Methods: The main purpose of our real-world observational study was to evaluate in COPD patients the effects of UMEC/VI on lung function and respiratory symptoms. Functional and clinical parameters were assessed at baseline, and after 52 weeks of treatment with this combined double inhaled therapy.
Results: We enrolled 110 subjects suffering from COPD. A 12-month UMEC/VI treatment induced significant improvements in total lung capacity (TLC) (p < 0.05), and residual volume (RV) (p < 0.0001). Pulmonary deflation was paralleled by significant increases of forced expiratory volume in one second (FEV1) (p < 0.0001), forced vital capacity (FVC) (p < 0.01), forced expiratory flow between 25% and 75% of FVC (FEF25– 75) (p < 0.0001) and diffusion capacity of the lung (DLCOcSB) (p < 0.05). In addition, in the same period, we also observed significant reductions of airway resistance including total resistance (Rtot) (p < 0.0001) and specific effective resistance (sReff) (p < 0.0001). Other improvements were detected with regard to modified British Medical Research Council (mMRC) questionnaire score (p < 0.0001), COPD Assessment Test (CAT) score (p < 0.0001), and COPD exacerbation rate (p < 0.0001). In particular, the reported changes of mMRC/CAT scores and COPD exacerbation numbers were significantly correlated with UMEC/VI–induced modifications of TLC, RV, FVC and FEV1.
Conclusion: In conclusion, our study corroborates in a real-life context the effectiveness of UMEC/VI in COPD treatment. Indeed, our broad investigational strategy has allowed to better characterize the functional mechanisms underpinning the therapeutic properties of UMEC/VI association.
Keywords: COPD, dual inhaled therapy, lung function, airway resistance, exacerbations
Introduction
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder usually characterized by the persistence and poor reversibility of airflow limitation, resulting from a pathological inflammatory response of the airways and lung parenchyma to the inhalation of cigarette smoke and/or other atmospheric pollutants.1 COPD is very frequent, affecting 10% of people over the age of 45 years, and currently represents the third leading cause of death worldwide.2–4 In particular, COPD is a heterogeneous syndrome including several phenotypes such as chronic obstructive bronchitis, small airway disease with peribronchiolar fibrosis and pulmonary emphysema,5 the latter being featured by lung hyperinflation and destruction of alveolar walls. Pulmonary emphysema is often associated with the inflammatory changes shaping chronic bronchitis and small airway disease.6 7,8 On the other hand, limitation of the expiratory flow compromises the emptying of intrapulmonary air, thus leading to air trapping at the alveolar level with consequent lung hyperinflation.5 This pathophysiological factor is the main cause of COPD symptoms, such as dyspnea and decreased exercise tolerance.6 Furthermore, the destruction of interalveolar septa that characterizes emphysema also leads to amputation of the pulmonary capillary bed, with a consequent reduction of gas exchange surface and alveolar-capillary diffusion.7
The main goals of COPD treatment include relief of respiratory symptoms and prevention of exacerbations.8 In order to pursue these therapeutic goals, the most important drugs are represented by inhaled bronchodilators, which include anticholinergics/antimuscarinics and β2-adrenergic agonists.9 Regular and continuous therapies with long-acting β2-adrenergic receptor agonists (LABA) and long-acting muscarinic receptor antagonists (LAMA) play a crucial role in COPD treatment. LABA and LAMA can be used either individually or as pre-established combinations providing dual LAMA/LABA therapies.10 These pharmacological associations allow to implement a double bronchodilation, based on the reciprocal strengthening of the different mechanisms of actions driven by LABA and LAMA, respectively, which are responsible for optimization of bronchodilating therapy.11 Furthermore, LAMA/LABA combinations allow the effects of bronchodilation to be extended throughout the entire respiratory tree, as the muscarinic receptors blocked by LAMA are more concentrated in proximal large-caliber airways, while the density of β2-adrenergic receptors stimulated by LABA progressively increases moving distally towards peripheral small airways.12 When compared with the efficacy of a treatment based on either a LAMA or LABA used alone, the bidirectional positive interactions between LAMA and LABA result in a more efficient bronchodilation, associated with a powerful attenuation of lung hyperinflation.13,14 Therefore, dual bronchodilation is more effective than single LABA or LAMA monotherapies in alleviating dyspnea, increasing exercise tolerance, preventing exacerbations, and improving respiratory function, quality of life and overall health status.15
With reference to the umeclidinium/vilanterol (UMEC/VI) combination, numerous randomized and controlled international polycentric trials have unequivocally demonstrated the therapeutic superiority of this LAMA/LABA association not only in comparison to placebo but also versus LABA or LAMA single treatments, such as vilanterol or umeclidinium used individually.16–19 However, scientific literature is quite short of publications regarding clinical studies carried out in the real-world of daily medical practice. Within this context, the aim of our clinical investigation was to evaluate in patients with COPD, through a real-life observational study, the effects of the fixed dose combination UMEC/VI on respiratory symptoms, global health status, lung function, and the annual number of disease exacerbations.
Patients and Methods
Study Design and Patient Enrollment
In this single-centre real-life study, at the Respiratory Disease Unit of “Mater Domini” University Hospital of Catanzaro, Italy, we recruited COPD patients and treated them with the combined dual inhalation therapy UMEC/VI (55/22 mcg). COPD was diagnosed according to the recommendations of Global Initiative for Chronic Obstructive Lung Disease (GOLD).20 Pulmonary function tests were performed according to the American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines,21 using the “Master Screen Pulmonary Function Testing System” and “Master Screen Body” equipment (Jaeger, Hannover, Germany). Measurement of the diffusion capacity of lung for carbon monoxide (DLCO) was carried out according to ATS/ERS standards, in order to evaluate the amount of carbon monoxide retained in the lung in a single breath, and the resulting value was corrected for the anaemia effect based on hemoglobin levels.22 Lung diffusing capacity was thus expressed as single breath corrected DLCO (DLCOcSB). Only COPD patients with blood eosinophil counts less than 100 cells/µL were considered for this real-life investigation.
At baseline, all enrolled patients were regularly taking either a LAMA or combinations of inhaled corticosteroids (ICS) and LABA (ICS/LABA), and they experienced persistent dyspnea, limitation of physical exercise, and recurrent exacerbations of COPD. The inhaled therapy UMEC/VI was prescribed according to current indications and was taken at the dose of one inhalation every 24 hours.23 Previously administered inhaled therapies were then suspended without any wash-out period.
This observational study met the standards of good clinical practice (GCP) and the principles of the Declaration of Helsinki. Furthermore, written informed consent was obtained from all patients. Our investigation was conducted on the basis of what was established by the local Ethics Committee of Calabria Region, Italy (Catanzaro, Italy, document n. 263–23 July 2020).
Outcomes and Measurements
Total lung capacity (TLC), residual volume (RV), inspiratory capacity (IC), intrathoracic gas volume (ITGV), expiratory reserve volume (ERV), forced expiratory volume in one second (FEV1), forced vital capacity (FVC), peak expiratory flow (PEF), forced expiratory flow between 25% and 75% of FVC (FEF25–75) and DLCOcSB were evaluated under baseline conditions, as well as after twelve months of treatment with UMEC/VI. All functional data refer to trough measurements. In addition, in the same period of time, we also assessed airway resistance including total resistance (Rtot), effective resistance (Reff), and specific effective resistance (sReff). Modified British Medical Research Council (mMRC) questionnaire score,24 COPD Assessment Test (CAT) score,25 and the number of moderate and severe COPD exacerbations26 occurring at baseline and after 52 weeks of treatment with UMEC/VI were also recorded. The safety and tolerability profile of the above inhaled therapy was verified through monthly telephone contacts with the patients, during which they were asked if they had experienced infections, headache, cough, or gastrointestinal disturbances, and we also acquired information about any eventual deterioration of their global health state. These phone calls were also used to monitor treatment adherence.
Statistical Analysis
Statistical analysis was performed using Prism version 9.4.0 (GraphPad Software Inc., San Diego, California, USA). Data were expressed as mean ± standard deviation (SD) if normally distributed, otherwise as median values with interquartile range (IQR). Anderson-Darling test was used to assess normal distribution. Student’s t-test or Mann–Whitney U-test was applied to compare variables. Relationships between variables were assessed by Pearson correlation coefficient (r) and linear regression analysis. A p value of less than 0.05 was considered as statistically significant.
Results
In this study, we recruited 110 patients (91 males and 19 females), characterized by a mean age of 67.74 ± 9.25 years, and a median body mass index (BMI) of 28.00 kg/m2 (25.00–31.00). Mean blood eosinophil count was 58.72 ± 19.79 cells/µL. At baseline, the mean values of RV and FEV1 were 122.7 ± 40.88% and 57.91 ± 11.89% of the predicted values, respectively. Baseline patient characteristics are summarized in Table 1.
 |
Table 1 Baseline Patient Characteristics |
UMEC/VI dual therapy had a significant impact on pulmonary hyperinflation; in fact, during the study period, TLC decreased from 5.53 ± 1.21 L to 5.34 ± 1.19 L (p < 0.05) (Figure 1A), and RV diminished from 2.80 L (2.37–3.49) to 2.46 L (1.97–2.96) (p < 0.0001) (Figure 1B). Furthermore, IC augmented from 1.93 ± 0.80 L to 2.10 ± 0.76 L (p < 0.05) (Figure 1C). However, we did not find statistically significant differences with regard to ITGV (3.49 ± 1.04 L vs 3.38 ± 1.07 L; p = 0.162) (Figure 1D) and ERV (0.70 ± 0.53 L vs 0.81 ± 0.54 L; p = 0.085) (Figure 1E).
 |
Figure 1 Effects of a 52-week treatment with UMEC/VI on TLC (A), RV (B), IC (C), ITGV (D), and ERV (E). *p < 0.05; ****p < 0.0001. Abbreviations: UMEC/VI, umeclidinium/vilanterol; TLC, total lung capacity; RV, residual volume; IC, inspiratory capacity; ITGV, intrathoracic gas volume; ERV, expiratory reserve volume. Ns, not significant. |
RV reduction was associated with concomitant improvements in both FEV1 and FVC, which increased from baseline values of 1.63 ± 0.46 L and 2.40 ± 0.65 L to 1.76 ± 0.51 L (p < 0.0001) (Figure 2A) and 2.55 ± 0.69 L (p < 0.01) (Figure 2B), respectively. When compared to baseline, FEV1/FVC ratio significantly enhanced from 65.13 ± 8.79% to 70.13 ± 10.59% (p < 0.0001) after 52 weeks of dual inhaled therapy with UMEC/VI. Moreover, PEF enhanced from 5.15 ± 1.72 L/s to 5.70 ± 1.95 L/s (p < 0.0001) (Figure 2C). These results were coexistent with a parallel increment of FEF25–75, which from the baseline value of 1.01 ± 0.48 L/s rose to 1.22 ± 0.57 L/s (p < 0.0001) (Figure 2D).
 |
Figure 2 Effects of a 52-week treatment with UMEC/VI on FEV1 (A), FVC (B), PEF (C), FEF25–75 (D), and DLCOcSB (E). *p < 0.05; **p < 0.01; ****p < 0.0001. Abbreviations: UMEC/VI, umeclidinium/vilanterol; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; PEF, peak expiratory flow; FEF25–75, forced mid-expiratory flow between 25% and 75% of forced vital capacity; DLCOcSB, corrected single-breath diffusion lung capacity for carbon monoxide. |
UMEC/VI induced positive effects also on airway resistance; in fact, one year after the first inhalation the mean R tot value decreased from 0.42 kPa*s/L (0.33–0.55) to 0.34 kPa*s/L (0.26–0.43) (p < 0.0001) (Figure 3A). In particular, Reff lowered from 0.36 kPa*s (0.30–0.51) to 0.29 kPa*s (0.23–0.39) (p < 0.0001) (Figure 3B), and sReff dropped from 1.33 kPa*s (0.99–2.05) to 1.04 kPa*s (0.81–1.45) (p < 0.0001) (Figure 3C), respectively.
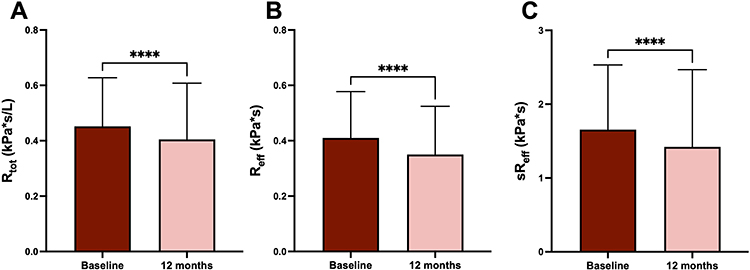 |
Figure 3 Effects of a 52-week treatment with UMEC/VI on Rtot (A), Reff (B), and sReff (C). ****p < 0.0001. Abbreviations: UMEC/VI, umeclidinium/vilanterol; Rtot, total resistance; Reff, effective resistance; sReff, specific effective resistance. |
Furthermore, DLCOcSB was also measured at baseline and one year after starting treatment with UMEC/VI. In this respect, we observed that DLCOcSB increased from 5.28 ± 1.67 mmol/min/kPa to 5.51 ± 1.65 mmol/min/kPa (p < 0.05) (Figure 2E).
The impact of UMEC/VI dual inhaled therapy on respiratory function was associated with notable clinical effects on COPD symptoms and global health status of study population. Indeed, after twelve months of treatment with UMEC/VI, both mMRC and CAT scores improved from 3.0 (3.0–4.0) to 1.0 (1.0–2.0) (p < 0.0001) (Figure 4A), and from 26.0 (23.0–32.0) to 17.0 (11.0–24.0) (p < 0.0001) (Figure 4B), respectively. Moreover, when compared to the previous year, the number of COPD exacerbations significantly diminished from 2.55 ± 0.50 to 1.68 ± 0.67 (p < 0.0001) (Figure 4C).
 |
Figure 4 Effects of a 52-week treatment with UMEC/VI on mMRC dyspnea scale (A), CAT score (B), and COPD exacerbations (C). ****p < 0.0001. Abbreviations: UMEC/VI, umeclidinium/vilanterol; mMRC, modified British Medical Research Council; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease. |
UMEC/VI–induced decrements of mMRC scores were found to be significantly correlated with the associated decreases of TLC (r = 0.374; p < 0.01) and RV (r = 0.326; p < 0.01), as well as with the reported increases of FVC (r = −0.262; p < 0.05) and FEV1 (r = −0.278; p < 0.01). In addition, CAT score improvements significantly correlated with the observed changes of TLC (r = 0.444; p < 0.001), RV (r = 0.591; p < 0.0001), FVC (r = −0.408; p < 0.001), FEV1 (r = −0.385; p < 0.001), and FEF25–75 (r = −0.266; p < 0.05). Finally, significant correlations were detected between the reductions of COPD exacerbation numbers, elicited by UMEC/VI treatment, and several functional effects including the modifications of TLC (r = 0.256; p < 0.05), RV (r = 0.331; p < 0.01), FVC (r = −0.265; p < 0.05), and FEV1 (r = −0.231; p < 0.05).
Moreover, adherence to inhaled treatment with UMEC/VI resulted to be optimal in all patients, and no side effect or adverse reaction was reported.
Discussion
Based on this real-life observational study, we herein show that COPD patients undergoing dual inhaled bronchodilator treatment with UMEC/VI manifested relevant clinical benefits including relief of dyspnea, decrease of the annual rate of disease exacerbations and a better health status, as well as they experienced significant improvements in lung function. In particular, the present results demonstrate that the above therapy significantly increased the values of several functional respiratory parameters such as FEV1, FEV1/FVC ratio, FEF25–75 and PEF, and also elicited significant decreases in RV and airway resistance. Furthermore, the inhaled treatment with UMEC/VI also enhanced DLCO. Despite the obvious limitation due to the relatively small number of patients that can be recruited in a single-centre observational study, these results confirm in a real-life setting the synergism of action between umeclidinium and vilanterol, and document even more pronounced clinical and functional effects in comparison to randomized controlled trials.
The UMEC/VI combination therapy was developed in the form of a multi-dose dry powder inhalational device.27 Each inhalation provides a pre-set pharmacological dosage, comprising 22 mcg of vilanterol and 55 mcg of umeclidinium, to be taken once a day approximately every 24 hours. In this way, an efficient LABA-LAMA synergism of action is achieved, which provides the pharmacological basis underlying the reported improvements in respiratory function, that in turn drive the consequent clinical advantages.28 Within this context, the present study was based on a real-life platform, characterized by a more complete evaluation of respiratory function in comparison to randomized controlled trials. Indeed, not only FEV1 and FEV1/FVC ratio were measured, but after one year of treatment with UMEC/VI other functional indices were recorded, also including RV. This conceptual approach is very important, since lung hyperinflation is the main pathophysiological factor responsible for dyspnea and impaired exercise tolerance in patients with COPD.6 Therefore, a careful assessment and monitoring of the functional effects of bronchodilating therapies, also including the UMEC/VI association, should not disregard the evaluation of the potential deflating actions of LABA and LAMA. Moreover, in comparison to clinical phases of relative COPD stability, exacerbations are associated with marked enhancements of lung hyperinflation, consisting of further RV increases. In this regard, it is noteworthy to consider that our present data clearly indicate that UMEC/VI regular inhalation induced a significant RV reduction. In the current study, we also show that UMEC/VI combination significantly increased FEF25–75, a functional parameter indicative of measurable airflow at the peripheral level of respiratory tract. Therefore, our results strongly suggest that the improvement of small airway patency could be the main mechanism by which dual UMEC/VI bronchodilator therapy promotes, especially during expiration, the emptying of air trapped into alveoli. The consequent lung deflation was likely responsible in our COPD patients for relief of dyspnea, amelioration of global health status, and decrease of the annual rate of disease exacerbations.29 Interestingly, the latter effects of UMEC/VI treatment were closely associated with the observed improvements in lung hyperinflation and airflow limitation. In particular, the reported changes of mMRC/CAT scores and COPD exacerbation numbers were significantly correlated with UMEC/VI–induced modifications of TLC, RV, FVC and FEV1.
It can also be inferred that the improvement of DLCO, detected in many of our patients treated with UMEC/VI, is due to a noticeable enhancement of pulmonary ventilation, leading to a consequent increase in air-blood contact surface and gas exchange. Such key changes in lung function depend on the optimal synergism resulting from the reciprocal potentiation and integration of the different mechanisms of action of vilanterol and umeclidinium. In fact, the therapeutic success of LABA and LAMA arises from the ability of these drugs to effectively counteract the exaggerated cholinergic bronchomotor tone, which is the main reversible pathophysiological component of airflow limitation characterizing patients with COPD. The positive interactions between vilanterol and umeclidinium occur primarily in airway smooth muscle. At this post-junctional level, the anticholinergic effects due to competitive receptor antagonism of M3 muscarinic receptors, operated by umeclidinium, significantly empower the functional antagonism of airway smooth muscle contraction, mediated by vilanterol via stimulation of β2-adrenergic receptors and the consequent activation of cAMP signaling pathway.30,31 Furthermore, vilanterol and umeclidinium also cooperate at a pre-junctional site, ie at the level of nerve endings of post-ganglionic vagal parasympathetic cholinergic fibers, which innervate airway smooth muscle.32,33 Indeed, in addition to providing a very effective post-junctional bronchodilation, vilanterol also activates pre-junctional β2-adrenergic receptors, thus inhibiting acetylcholine release. This mechanism is significantly potentiated by acetylcholine-induced stimulation of prejunctional inhibitory M2 muscarinic autoreceptors, whose functional activity is largely spared by umeclidinium, which behaves as a relatively selective receptor antagonist of post-junctional M3 receptors.34–36
By analogy with other similar monocentric observational studies carried out in a real-world setting, our present clinical investigation is also outlined by some limitations, including a relatively small size of patient sample and the lack of randomization design and placebo control. Of course, these considerations imply that comparative evaluations in real-life are less reliable than in randomized controlled trials. However, this limitation is widely compensated by a much larger inclusion of patients, who would be otherwise excluded by the restrictive enrollment criteria imposed by clinical trials.
In conclusion, the most interesting aspect of our experimental work is undoubtedly represented by the real-life environment related to its development and implementation. This real-world research context has indeed made it possible to evaluate several key parameters of lung function, thereby using a much more extensive and in-depth approach than the limited one commonly utilized in randomized controlled trials. Hence, such a broader investigational strategy has allowed to better characterize the functional mechanisms underpinning the therapeutic properties of UMEC/VI association.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific funds from any agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Barnes PJ, Burney PG, Silverman EK, et al. Chronic obstructive pulmonary disease. Nat Rev Dis Primers. 2015;1:15076. doi:10.1038/nrdp.2015.76
2. Blanco I, Diego I, Bueno P, Casas-Maldonado F, Miravitlles M. Geographic distribution of COPD prevalence in the world displayed by geographic information system maps. Eur Respir J. 2019;54(1):1900610. doi:10.1183/13993003.00610-2019
3. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
4. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
5. O’Donnell DE, Laveneziana P. The clinical importance of dynamic lung hyperinflation in COPD. COPD. 2006;3(4):219–232. doi:10.1080/15412550600977478
6. O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(2):180–184. doi:10.1513/pats.200508-093DO
7. Ni Y, Yu Y, Dai R, Shi G. Diffusing capacity in chronic obstructive pulmonary disease assessment: a meta-analysis. Chron Respir Dis. 2021;18:14799731211056340. doi:10.1177/14799731211056340
8. Wedzicha JA, Decramer M, Seemungal TA. The role of bronchodilator treatment in the prevention of exacerbations of COPD. Eur Respir J. 2012;40(6):1545–1554. doi:10.1183/09031936.00048912
9. Matera MG, Page CP, Cazzola M. Novel bronchodilators for the treatment of chronic obstructive pulmonary disease. Trends Pharmacol Sci. 2011;32(8):495–506. doi:10.1016/j.tips.2011.04.003
10. Cazzola M, Page CP, Calzetta L, Matera MG. Pharmacology and therapeutics of bronchodilators. Pharmacol Rev. 2012;64(3):450–504. doi:10.1124/pr.111.004580
11. Cazzola M, Tashkin DP. Combination of formoterol and tiotropium in the treatment of COPD: effects on lung function. COPD. 2009;6(5):404–415. doi:10.1080/15412550903156333
12. Coulson FR, Fryer AD. Muscarinic acetylcholine receptors and airway diseases. Pharmacol Ther. 2003;98(1):59–69. doi:10.1016/S0163-7258(03)00004-4
13. Malerba M, Foci V, Patrucco F, et al. Single inhaler LABA/LAMA for COPD. Front Pharmacol. 2019;10:390. doi:10.3389/fphar.2019.00390
14. Pelaia G, Vatrella A, Busceti MT, et al. Pharmacologic rationale underlying the therapeutic effects of tiotropium/olodaterol in COPD. Ther Clin Risk Manag. 2015;11:1563–1572. doi:10.2147/TCRM.S84151
15. Rogliani P, Calzetta L, Braido F, et al. LABA/LAMA fixed-dose combinations in patients with COPD: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:3115–3130. doi:10.2147/COPD.S170606
16. Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62. 5/25mcg in COPD. Respir Med. 2013;107(10):1538–1546. doi:10.1016/j.rmed.2013.06.001
17. Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62. 5/25mcg and tiotropium 18 mcg in chronic obstructive pulmonary disease: results of a 24-week, randomized, controlled trial. Respir Med. 2014;108(12):1752–1760. doi:10.1016/j.rmed.2014.10.002
18. Kerwin EM, Kalberg CJ, Galkin DV, et al. Umeclidinium/vilanterol as step-up therapy from tiotropium in patients with moderate COPD: a randomized, parallel-group, 12-week study. Int J Chron Obstruct Pulmon Dis. 2017;12:745–755. doi:10.2147/COPD.S119032
19. Maltais F, Bjermer L, Kerwin EM, et al. Efficacy of umeclidinium/vilanterol versus umeclidinium and salmeterol monotherapies in symptomatic patients with COPD not receiving inhaled corticosteroids: the EMAX randomised trial. Respir Res. 2019;20(1):238. doi:10.1186/s12931-019-1193-9
20. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis management and prevention of COPD. goldcopd.org/2023; 2023.
21. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. An official American thoracic society and European respiratory society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
22. Graham BL, Brusasco V, Burgos F, et al. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur Respir J. 2017;49(1):1600016. doi:10.1183/13993003.00016-2016
23. Scott LJ, Hair P. Umeclidinium/vilanterol: first global approval. Drugs. 2014;74(3):389–395. doi:10.1007/s40265-014-0186-8
24. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
25. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
26. Kim V, Aaron SD. What is a COPD exacerbation? Current definitions, pitfalls, challenges and opportunities for improvement. Eur Respir J. 2018;52(5):1801261. doi:10.1183/13993003.01261-2018
27. Cada DJ, Ingram K, Leonard J, Baker DE. Umeclidinium bromide and vilanterol trifenatate inhalation powder. Hosp Pharm. 2014;49(6):554–562. doi:10.1310/hpj4906-554
28. Cazzola M, Segreti A, Matera MG. New developments in the combination treatment of COPD: focus on umeclidinium/vilanterol. Drug Des Devel Ther. 2013;7:1201–1208. doi:10.2147/DDDT.S39449
29. Armentaro G, Pelaia C, Cassano V, et al. Association between right ventricular dysfunction and adverse cardiac events in mild COPD patients. Eur J Clin Invest. 2022;53:e13887. doi:10.1111/eci.13887
30. Casarosa P, Bouyssou T, Germeyer S, Schnapp A, Gantner F, Pieper M. Preclinical evaluation of long-acting muscarinic antagonists: comparison of tiotropium and investigational drugs. J Pharmacol Exp Ther. 2009;330(2):660–668. doi:10.1124/jpet.109.152470
31. Somlyo AP, Somlyo AV. Signal transduction and regulation in smooth muscle. Nature. 1994;372(6503):231–236. doi:10.1038/372231a0
32. Pérez Fontan JJ. On lung nerves and neurogenic injury. Ann Med. 2002;34(4):226–240. doi:10.1080/078538902320322493
33. Groneberg DA, Quarcoo D, Frossard N, Fischer A. Neurogenic mechanisms in bronchial inflammatory diseases. Allergy. 2004;59(11):1139–1152. doi:10.1111/j.1398-9995.2004.00665.x
34. Gross NJ, Co E, Skorodin MS. Cholinergic bronchomotor tone in COPD. Estimates of its amount in comparison with that in normal subjects. Chest. 1989;96(5):984–987. doi:10.1378/chest.96.5.984
35. Hall IP. Second messengers, ion channels and pharmacology of airway smooth muscle. Eur Respir J. 2000;15(6):1120–1127. doi:10.1034/j.1399-3003.2000.01523.x
36. Salmon M, Luttmann MA, Foley JJ, et al. Pharmacological characterization of GSK573719 (umeclidinium): a novel, long-acting, inhaled antagonist of the muscarinic cholinergic receptors for treatment of pulmonary diseases. J Pharmacol Exp Ther. 2013;345(2):260–270. doi:10.1124/jpet.112.202051
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.