")
Back to Journals » International Journal of Women's Health » Volume 14
Clinical and Biochemical Potential of Antioxidants in Treating Polycystic Ovary Syndrome
Received 23 October 2021
Accepted for publication 18 March 2022
Published 1 April 2022 Volume 2022:14 Pages 467—479
DOI https://doi.org/10.2147/IJWH.S345853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Xiangyi Cheng, Bing He
Department of Endocrinology, Shengjing Hospital, China Medical University, Shenyang, Liaoning Province, People’s Republic of China
Correspondence: Bing He, Department of Endocrinology, Shengjing Hospital, China Medical University, Shenyang, 110000, Liaoning Province, People’s Republic of China, Email [email protected]
Abstract: Polycystic ovary syndrome (PCOS) is the most common cause of infertility in reproductive-age women. Increased reactive oxygen species levels and decreased antioxidant capacity in PCOS patients can lead to metabolic disorders and damage the ovarian tissues, resulting in the occurrence of related symptoms. Antioxidants have been used in the treatment of PCOS and have yielded satisfactory outcomes due to their ability to counter oxidative stress. Many experiments on PCOS patients have proved that antioxidants can not only improve the ovarian environment, promote follicular maturation, and elevate oocyte quantities but can also regulate lipid and glucose metabolism as well as vascular endothelial cell function in PCOS patients, thereby attenuating adiposity and reducing the occurrence rate of chronic complications to ensure that patients can obtain long-term benefits. This review describes the use of antioxidants in PCOS, which have been used in the treatment.
Keywords: PCOS, oxidative stress, antioxidants, α-lipoic acid
Introduction
Polycystic ovary syndrome (PCOS) is a common reproductive endocrine disease that affects 5–10% of reproductive-age females.1 It is characterized by irregular menses, anovulatory infertility, and hyperandrogenism, accompanied by metabolic abnormalities, such as obesity, insulin resistance (IR), hyperinsulinemia, dyslipidemia, and glucometabolic disorders. Currently, the primary treatment strategies for PCOS are lifestyle changes and medications,2 which help control weight, induce ovulation, reduce IR, regulate the menstrual cycle, and reduce serum androgen levels.3 Clomiphene citrate (CC), metformin, ethinylestradiol, and cyproterone are among the traditional drugs used for PCOS treatment. However, these drugs may induce numerous adverse effects, including ovarian hyperstimulation syndrome (OHSS), gastrointestinal side effects, abnormal glucose and lipid metabolism, mental disorder, hair loss, vision loss, and allergic dermatitis.4–6 In addition, they may not substantially improve IR and metabolic disorders when used as a single therapy,7 requiring them to be combined with other treatment agents.
Although the pathophysiology of PCOS is quite complex,8 there is increasing evidence that oxidative stress (OS) is involved in its pathogenesis. Many studies have shown that the levels of OS markers are elevated in PCOS patients.14,15 There are also indications that genetic variability in gene coding for antioxidant enzymes modifies the risk of PCOS.9 In addition, OS in PCOS patients possibly enhance the risk of long-term complications, such as type 2 diabetes (T2DM) and endometrial cancer.9 This article therefore summarizes the relationship between OS and PCOS, and explores the application of antioxidants as treatment, with the aim of providing an effective reference for new drug research and development and for the clinical treatment of PCOS.
OS in PCOS
OS is an expression used to describe various deleterious processes resulting from an imbalance between the excessive formation of reactive oxygen species (ROS) and/or reactive nitrogen species and limited antioxidant defenses.10 The data collected by Herman et al indicate that genetic variability in gene coding for antioxidant enzymes not only modifies the risk of PCOS but also influences the metabolic characteristics of PCOS patients.11 Malondialdehyde (MDA) is a decomposition product of peroxidized polyunsaturated fatty acids, used as a biological marker for OS.12,13 Bannigida et al14 determined serum MDA, CRP, insulin levels, along with IR in 100 women diagnosed with PCOS (50 obese and 50 non-obese), and found that women with PCOS had higher CRP and MDA levels than their respective controls did, irrespective of whether they were obese or not. In addition, Özer et al15 found that PCOS patients have high MDA levels, low antioxidant indices, such as low zinc serum levels, and catalase activity, appearing to be more pronounced in patients with IR and infertility. Total antioxidant status (TAOS), which is defined as the ability of plasma/serum to inhibit free radical production, is a cumulative index of plasma antioxidant status and carbonyl content and should be considered when evaluating the effects of OS on the risk of developing cardiovascular diseases in women with PCOS.16 The presence of carbonyl groups in proteins has been used as a marker of ROS-mediated protein oxidation.17 In a study by Fenkci et al,16 which included 30 women with PCOS and 31 healthy women, the TAOS was significantly lower in women with PCOS than that in healthy women, and that protein carbonyl levels were significantly higher in women with PCOS than those in healthy women, which indicated that these proteins were attacked by ROS.16 Moreover, they found that high-density lipoprotein levels were inversely associated with protein carbonyl levels; this led them to the speculation that increased OS and decreased antioxidant capacity may increase the risk of cardiovascular disease in women with PCOS.16 Chattopadhayay et al18 examined 326 oocytes from 35 women with PCOS (group A) and 208 oocytes from 32 women with tubal infertility (group B) for meiotic spindles using PolScope. They found that the number of oocytes, which failed to form spindles and OS markers, was significantly higher in group A than those in group B.18 Furthermore, fertilization rate, the number of good-quality embryos, and clinical pregnancy rates were lower in group A than they were in group B; however, these differences were not statistically significant.18 Thus, they showed that oocyte development could be affected by increased OS, as high follicular fluid (FF) ROS levels tended to decrease the fertilization potential of oocytes, consequently lowering pregnancy rates.18 The studies by Yalcinkaya et al19 and Calonge et al20 have shown that imbalance between oxidant and antioxidant levels in the ovary may not only reduce ovarian reserve and oocyte quality but also have a negative impact on placental growth. In summary, in PCOS patients, ROS production increases, whereas antioxidant capacity decreases, and this may have adverse effects on ovarian function and body metabolism.
Antioxidants in PCOS
Alpha Lipoic Acid (ALA)
ALA, 1, 2-dithiolane-3-pentanoic acid, which has been termed “the universal antioxidant,” is one of the most powerful natural antioxidants.21 LA is an essential cofactor for the pyruvate dehydrogenase complex, and belongs to the class of metabotropic antioxidants, with both its oxidized (disulfide) and reduced (di-thiol: dihydro-lipoic acid) forms showing antioxidant activity.22,23 In addition, LA lowers blood glucose levels by enhancing the expression of glucose transporter 4 (GLUT-4), which can initiate glucose transport.24
Masharani et al25 administered 600 mg of controlled-release LA (CRLA) twice daily to six lean, nondiabetic PCOS patients, and the subjects did not develop any adverse reactions to LA over the study period. At the end of 16 weeks, they found a decrease in triglyceride levels and shift in the distribution of low-density lipoprotein (LDL) particles toward the larger, more buoyant LDL subclass fraction, thus decreasing the proportion of LDL-4, which is the most atherogenic of all LDL subfractions.25 Therefore, it was hypothesized that CRLA may have a significant anti-atherogenic effect in PCOS patients.25 In addition, there was a significant improvement in insulin sensitivity as determined by the euglycemic hyperinsulinemic clamp technique, and two subjects who were not on oral contraception had an increased frequency of menstrual cycles.25 Based on these findings, they hypothesized that improvements in insulin sensitivity may be associated with better reproductive capacity, and that CRLA may be useful in normalizing menstrual cycles in women with PCOS.25 In a study by Ivanova et al,26 45 PCOS patients were randomly allocated to an LA (n = 25) or high-protein diet (n = 20) group. Patients in the experimental group received one tablet of ALA (Thioctacid-HR) 30 minutes before breakfast, and after 3 months of intervention. A considerable decrease in basal and/or glucose-stimulated hyperinsulinemia as well as in IR index was observed in patients who received ALA as compared to those who received the high-protein diet.26 Furthermore, 16 (64%) patients in the ALA group with amenorrhea had their menstruation induced, developed dominant follicles, and the average ovarian volume was normalized.26 Another study by Genazzani et al27 also showed that low-dose integrative administration of ALA could improve insulin sensitivity in obese PCOS patients. In addition, PCOS patients with diabetic relatives showed decreased triglyceride and glutamic oxaloacetic transaminase levels, suggesting that the integrative administration of ALA improved metabolic impairment, especially in those with familial diabetes, who are potentially at high risk of developing non-alcoholic fatty liver disease and have a greater predisposition to diabetes.27 Based on the findings of these studies, ALA therapy is efficacious in both obese and non-obese PCOS patients, delaying the onset of complications, such as atherosclerosis and chronic liver injury.27 It is hence expected that ALA may be the drug of choice for the treatment of PCOS and hyperinsulinemia accompanied by liver disease (hepatitis, cirrhosis, and decompensated steatosis).26
LA and inositol can act on GLUT-4 synergistically. Genazzani et al28 and Fruzzetti et al29,30 administered ALA doses of 400 mg/day, 800 mg/day, and 600 mg/day in combination with inositol were administered to PCOS patients and found that the efficacy of the therapeutic combination was superior to that of the individual molecules; however, their optimal doses need to be determined by further research.
Vitamin C and Vitamin E
Vitamin E (α-tocopherol), which is a lipid-soluble vitamin with antioxidant properties, can activate intracellular antioxidant enzymes known as “radical scavengers,” thereby protecting the cell membrane from lipid peroxidation.31,32 Vitamin C (L-ascorbic acid; VC), another potent antioxidant, acts as a cofactor in essential enzyme reactions, and is an important nutrient for the human body.33 It elicits its antioxidant effects by directly reacting with aqueous peroxyl radicals or by indirectly restoring fat-soluble antioxidant vitamin levels.34
Olaniyan et al35 evaluated the effects of vitamin C in a dehydroepiandrosterone (DHEA)-induced mouse PCOS model and found that there was a significant decrease in MDA and cytokine levels and an increase in antioxidant and metabolic enzyme levels in the DHEA and vitamin C co-treated group as compared to the cytokine and metabolic enzyme levels in the DHEA-treated group. In addition, histopathological analyses showed a reduction in the number of cystic and atretic ovaries, and a significant downregulation of androgen receptor mRNA gene expression, which confirms that vitamin C plays a protective role against DHEA-induced PCOS via its antioxidant effects.35 Shirazi et al36 enrolled 43 PCOS patients and randomized them into two groups, subjects in the vitamin E and placebo groups received 400 IU/day of vitamin E as alpha tocopheryl acetate (n = 22) and cellulose capsules (n = 21), respectively, for eight weeks. After adjusting for potential confounders, vitamin E supplementation significantly reduced body weight, fat mass, Ang-1 levels, the Ang-1/Ang-2 ratio, and vascular endothelial growth factor (VEGF) levels, thereby improving blood circulation in ovarian tissues and normalizing ovarian follicular growth and ovulation.36 Clomiphene citrate (CC) is a commonly used ovulation-inducing drug, and OS plays a vital role in CC resistance.37 In a study by Morsy et al37 which included 60 PCOS patients, it was found that the patients who received vitamin E in addition to metformin and CC had higher clinical pregnancy rates, ovulation rates, and endometrial thickness than those who did not receive vitamin E. However, this trial did not support the hypothesis that vitamin E may increase ovulation and pregnancy rates in women with CC-resistant PCOS, but suggested that higher doses of vitamin E may be needed to enhance its effects.37 Furthermore, combined treatment with vitamin E, ethinyl estradiol, and cyproterone or metformin has facilitated ovulation more effectively and induced higher pregnancy rates than their separate application.38–41
Coenzyme Q (CoQ10)
CoQ10, also known as ubiquinone, plays an important role in cell energy supply and exhibits significant antioxidant activity.42 In addition, it is a component of the electron-transport chain, and participates in cellular aerobic respiration and generating cellular energy in the form of ATP.43
In the study by Taghizadeh et al.44 PCOS patients were randomized into two groups; subjects in group 1 (n = 22) received a 200 mg CoQ10 supplement tablet daily, while those in group 2 (n = 21) received a placebo tablet daily, over a period of eight weeks. They found that CoQ10 supplementation has a beneficial effect on inflammatory and endothelial dysfunction marker levels in overweight and obese PCOS patients, and therefore improves ovarian function.44 Impaired glucose tolerance and T2DM are common in women with PCOS. A study by Izadi et al45 showed that supplementation with CoQ10 alone or in combination with vitamin E had considerable effects on fasting plasma glucose (FPG) and homeostasis model assessment-IR (HOMA-IR) as compared to those under the placebo treatment, whereas only co-supplementation affected sex hormone-binding globulin concentrations, which decreased total serum testosterone levels. In a meta‐analysis, Liu et al46 concluded that CoQ10 administration can significantly reduce FPG and HOMA-IR, and effectively improve glucose and lipid metabolism, inflammation, and sex hormone levels. Refaeey et al47 evaluated the combined ovulation induction effects of oral CoQ10 and CC in CC-resistant PCOS patients through a prospective randomized controlled trial, and found that clinical pregnancy rate was significantly higher in the CoQ10 group than in the control group. The researchers concluded that CoQ10 could improve ovarian functions in CC-resistant PCOS and that in combination with CC was an effective and safe option to be considered before gonadotrophin therapy or laparoscopic ovarian drilling (LOD).47 However, the appropriate CoQ10 dosage and the optimal duration of treatment need to be further investigated.
N-Acetylcysteine (NAC)
NAC is a safe and commonly used mucolytic drug; at high doses, it induces an increase in cellular antioxidant levels and reduces glutathione levels.48
In a study by Fulghesu et al,49 37 PCOS patients were treated for up to six weeks with oral NAC at a dose of 1.8 g/day, and a dose of 3 g/day was arbitrarily chosen for significantly obese subjects. They found that NAC was well tolerated by all patients and no adverse effects were observed.49 At the end of the treatment, hyperinsulinemic subjects showed a significant increase in insulin sensitivity as well as a concomitant decrease in circulating insulin levels, which was followed by a significant reduction in T levels and free androgen index.49 However, similar results were not obtained for normoinsulinemic subjects.49 In addition, studies on the effects of insulin-sensitizing agents on lipidic patterns found a significant decrease in plasma lipid levels, including cholesterol, triglyceride, and LDL levels after NAC-mediated insulin-level reduction, indicating a possible additional benefit of this drug on long-term health outcomes in PCOS patients.49–51 The efficacy of metformin in PCOS was compared with that of NAC by Chandil et al,52 and they showed that NAC improved the clinical features of PCOS, IR biochemical marker levels, hormonal levels, and anovulation, in addition to the improved peripheral IR, more effectively than metformin did. Moreover, due to the absence of adverse effects, NAC can be regarded as an appropriate substitute for insulin sensitizer in the treatment of PCOS.52 In a study by Cheraghi et al,53 60 women with PCOS who underwent intracytoplasmic sperm injection (ICSI) were divided into four groups and received either metformin (1500 mg/day), NAC (1800 mg/day), metformin + NAC, or a placebo for six weeks. They found that the number of immature and abnormal oocytes substantially decreased with a concomitant increase in the number of good-quality embryos in the NAC group as compared to that of the placebo group.53 In addition, leptin, MDA, insulin, and LH levels were significantly lower in the NAC and NAC+MET groups.53 In another study by Nasr et al.54 NAC was administered as an adjunct therapy following unilateral LOD in women with CC-resistant PCOS, and they found a significant increase in ovulation, pregnancy, and live birth rates, indicating that NAC could be used as a novel adjunct therapeutic agent after unilateral LOD and may improve the overall reproductive outcome. Rizk et al55 and Badawy et al56 investigated the combined effects of NAC and clomiphene on PCOS and found that this combination helped increase pregnancy and ovulation rates and decreased OHSS rates compared with those after a single application. Sacchinelli et al57 also found that the combination of NAC + Inositol + folic acid improved ovarian function in PCOS patients, regardless of IR state, indicating that inositol and NAC may have additional non-insulin-related mechanisms of action that could allow them to elicit beneficial effects in patients with negative HOMA-indices.
Resveratrol (RSV)
RSV, a polyphenolic compound, which is found in grapes, red wine, peanuts, and some berry species, is regarded as a powerful antioxidant with anti-Inflammatory, anti-coagulant, anti aging, and anti-cancer properties.58 Its protective effects against oxidative injury are probably due to the upregulation of cellular antioxidant enzyme activity, including superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx).59
In a study by Ergenoglu et al,60 a PCOS model was formed in 14 rats using subcutaneous dihydrotestosterone, and the rats were randomly divided into two groups, treated with 1 mL/kg/day of isotonic saline or 10 mg/kg/day of resveratrol. They found a significant decrease in antral follicle counts, plasma anti-Mullerian hormone, insulin-like growth factor 1 levels, and superoxide dismutase activity, and a significant increase in glutathione peroxidase content in the resveratrol treatment group, indicating that it could be effective in the treatment of PCOS due to its antioxidant properties.60 IR in PCOS is associated with chronic low-grade inflammation. In a 3-month randomized controlled trial conducted by Banaszewska et al,61 treatment with resveratrol resulted in lower serum levels of both T and DHEA in women with PCOS, while fasted insulin levels significantly decreased and insulin sensitivity was improved following RSV treatment.61 Another study reported a significant downregulation of LH and total testosterone levels, as well as an upregulation of FSH and thyroid stimulating hormone levels in patients treated with RSV.62 Therefore, RSV may be effective in increasing FSH levels by reducing steroid-derived androgen levels, thus facilitating follicular maturity and growth, and contributing to improving oocyte quality and better pregnancy outcomes.62
Melatonin
Melatonin is a tryptophan-derived molecule with pleiotropic activities; it is secreted from the pineal gland, with a circadian rhythm that peaks at night and is low during the day.63,64 The original and primary function of melatonin in early life forms such as unicellular organisms was to serve as a free radical scavenger and an antioxidant with several unique features that differ from those of classic antioxidants, including the ability to undergo cascade reactions with free radicals, and capacity to be induced under moderate OS conditions.64
Basheer et al65 observed a downregulation of melatonin (MT1 and MT2), estrogen (ER-α), and cytokine (IL-2R and IL-6R) receptor expression levels, and high circulation levels of IL-6 and TNF-α in female Wistar rats induced by letrozole; however, these alterations were reversed after melatonin treatment. In a study by Pai et al.66 PCOS was induced in 21-day-old female rats by daily subcutaneous administration of testosterone (20 mg/kg) over a period of 35 d. The PCOS mice were administered metformin (500 mg/kg), 1 mg/kg of melatonin, or 2 mg/kg of melatonin, in combination with testosterone, over a period of 36 d.66 Both doses of melatonin significantly reduced body weight, body mass index, intra-abdominal fat (IAF), and insulin and CRP levels; in addition, a favorable lipid profile was observed.66 Moreover, histopathological examination of the ovary, uterus, and IAF tissues revealed a decrease in the number of cystic follicles, neoplastic endometrial glands, and adipocyte hypertrophy, respectively.66 Jamilian et al67 showed that melatonin administration to women with PCOS can significantly reduce hirsutism, total testosterone, high-sensitivity hs-CRP, and MDA levels, while increase TAC and GSH levels. In addition, melatonin administration was found to reduce IL-1 and TNF-α gene expression.67 In a study by Tagliaferri et al,68 after 6 months of melatonin administration in 40 normal-weight women with PCOS, menstrual irregularities and biochemical hyperandrogenism were improved, possibly through a direct insulin-independent effect on the ovaries. In a study by Shabani et al,69 58 subjects were randomized into two groups and were administered either 10 mg of melatonin or placebo once a day, 1 h before bedtime, for 12 weeks. They found that melatonin exhibited beneficial effects on mental health parameters, insulin levels, HOMA-IR, quantitative insulin sensitivity check index, total cholesterol and LDL-cholesterol levels, and gene expression of the peroxisome proliferator-activated receptor gamma (PPAR-γ) and the low-density lipoprotein receptor in women with PCOS, which indicated that melatonin supplementation may confer potential therapeutic advantages in women with PCOS.69 Based on the finding that the addition of melatonin to IVM media improves cytoplasmic maturation in human immature oocytes and subsequent clinical outcomes, Kim et al70 hypothesized that follicular melatonin may be released from luteinizing granulosa cells during late folliculogenesis, and that melatonin supplementation could hence be used to improve the clinical outcomes of in vitro maturation (IVM). Similarly, the findings by Mokhtari et al71 showed that treating PCOS patients undergoing intrauterine insemination (IUI) with melatonin significantly improves the rate of chemical pregnancy. Kun Yu et al72 showed that melatonin promoted CYP19A1 and HO-1 expression and decreased IL-18 levels in human ovarian GCs obtained from a patient with PCOS with hyperandrogenia, thereby facilitating oocyte maturation. Hence, melatonin supplementation could be beneficial for women with PCOS due to its effects on steroidogenesis, through which it regulates ovulation, reverses IR and dyslipidemia, prevents hyperplastic changes in the endometrium, and protects against endometrial cancer.66
Carnitine
Carnitine is a quaternary ammonium compound that can be synthesized from the two amino acids lysine and methionine.73 It plays important roles in carbohydrate and lipid metabolism, and improves IR and depression states.74,75
In a study by Jamilian et al,76 60 patients diagnosed with PCOS were randomized into two groups to receive either 250 mg of carnitine supplements or a placebo for 12 weeks. They found that carnitine supplementation had favorable effects on mental health, which was judged with Beck Depression Inventory (BDI), General Health Questionnaire-28 (GHQ-28) and Depression Anxiety and Stress Scale (DASS) at the beginning and the end of study, and OS biomarker levels.76 Tauqir et al77 evaluated 147 women with PCOS for 12 weeks that were randomly assigned into a combo group (n = 72) that received a combination of metformin, pioglitazone (pio), and acetyl-L-Carnitine (ALC), or the Met + Pio group (n = 75) that received metformin plus pioglitazone and placebo. They concluded that addition of ALC to metformin plus pioglitazone further ameliorates IR, polycystic ovaries, and stress burden, along with normalization of regular menstrual cycles.77 A study by Ismail et al78 included a total of 170 women with clomiphene-resistant PCOS who were divided into two groups. Group (A) included patients who received 100 to 150 mg clomiphene citrate from day three until day seven of the cycle and L-carnitine (LC) 3 g daily until a positive pregnancy test; group (B) received 100 to 150 mg clomiphene citrate with a placebo. The results show that adding LC to clomiphene from the follicular phase and extending through the luteal phase in patients with clomiphene-resistant PCOS, at the given dose and duration, may benefit the quality of ovulation and clinical pregnancy rate.78
In general, as an antioxidant, carnitine can improve IR, ovulation, and even mental health in PCOS patients.
Other Antioxidants
Selenium is an essential trace element, which is essential for human biology and health.79 In a study by Razavi et al,79 64 women with PCOS were randomized into two groups and received either 200 μg of selenium daily or a placebo. After eight weeks of intervention, patients who received selenium exhibited markedly decreased serum DHEA levels, hirsutism (modified Ferriman–Gallwey scores), serum hs-CRP levels, and plasma MDA levels compared to the levels of those who received the placebo.79 In addition, selenium elicited beneficial effects on reproductive outcomes, which indicate that PCOS-related symptoms can be improved via the antioxidant effects of selenium.79 Similar findings have been obtained for combined magnesium and zinc supplementation.80 Jamilian et al81 also reported that chromium administration in infertile women with PCOS, who were candidates for IVF, for eight weeks, had beneficial effects on glycemic control and OS. Various pharmacological studies have demonstrated that crocetin has a wide range of antioxidant, anti-cancer, hypolipidemic, and anti-atherosclerotic effects.82 Hu et al82 confirmed the attenuation of PCOS by crocetin in prenatal mice exposed to DHT. They suggested that the therapeutic effect of crocetin was likely due to the revise in kisspeptin expression in the anteroventral periventricular nucleus (AVPV) and arcuate nucleus (ARC), serum levels of estradiol (E2), progesterone (P4), T, LH, and FSH, as well as the structural and functional changes in ovaries.82 Furthermore, based on both experimental and analytical proof, Bahmani et al83 concluded that folate supplementation (5 mg/d) in women with PCOS had beneficial effects on inflammatory factor and OS biomarker levels.
Conclusion
PCOS is the most common cause of anovulatory infertility in women of reproductive age. Antioxidants can not only improve OS and IR in PCOS patients but also improve the ovarian environment, reduce androgen levels, and promote follicular maturation. In addition, they can induce better outcomes when used in combination with traditional ovulation-inducing regimens and assisted reproductive technologies, effectively improving pregnancy outcomes. As endothelial dysfunction and dyslipidemia are early signs of cardiovascular disease, antioxidants can regulate lipid metabolism and vascular endothelial cell function in PCOS patients, thereby attenuating adiposity and reducing the occurrence rate of chronic complications. Moreover, some antioxidants, including carnitine and melatonin, can enhance the quality and psychological status of PCOS patients. The reviewed articles are summarized in Table 1. In summary, numerous antioxidants with significant beneficial effects and low adverse reaction rates can significantly improve the symptoms of PCOS and prevent or treat the long-term complications. Therefore, as a drug class with useful potential, antioxidant use in clinical settings should be encouraged following careful review of the Medical history and disease profile of each individual patient with PCOS. However, the potential of antioxidants in the treatment of PCOS remains to be further explored, such as the impact on pregnancy outcomes and offspring growth and development in women with PCOS pregnancy. Optimal dosage of various antioxidants also remains to be studied.
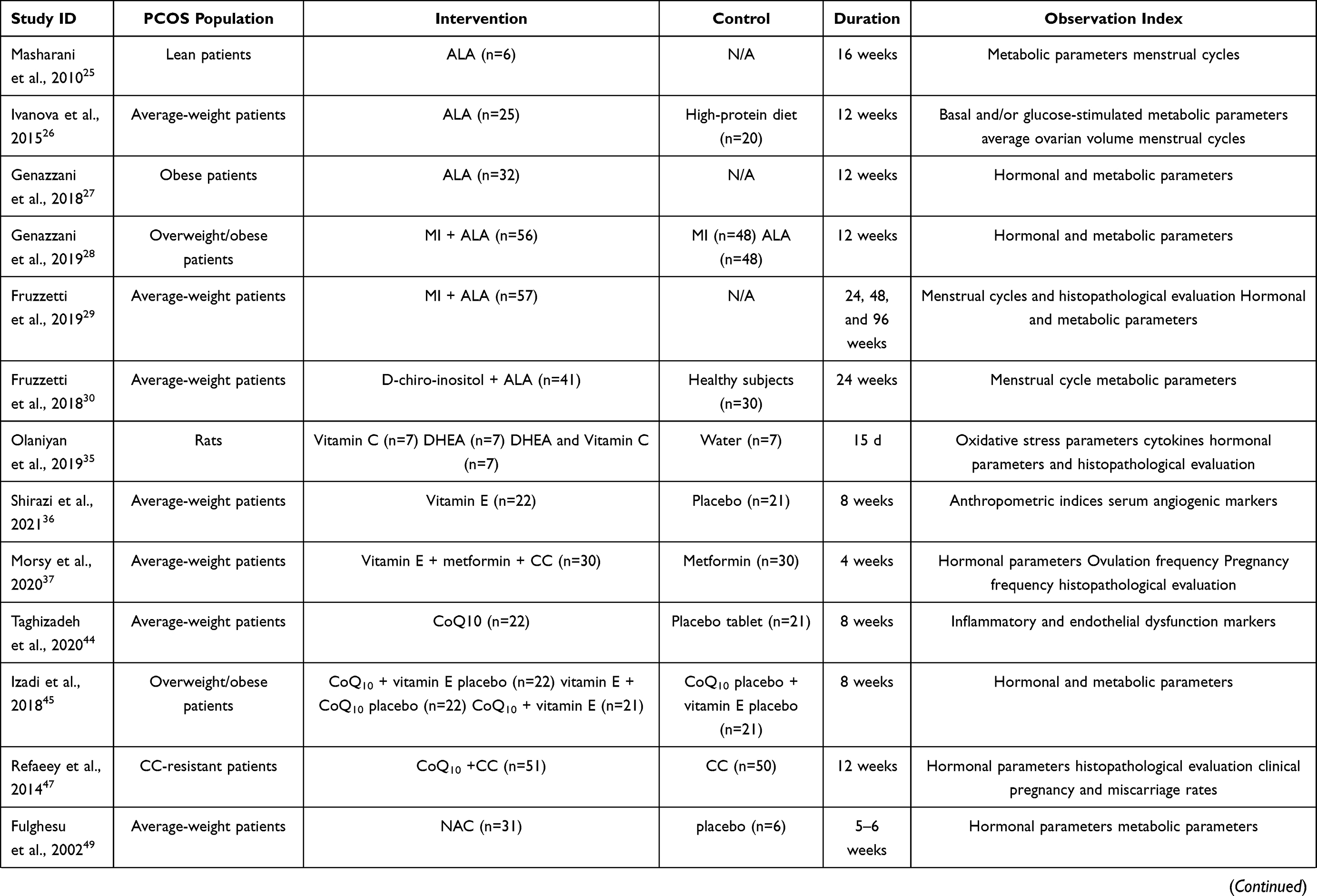 | 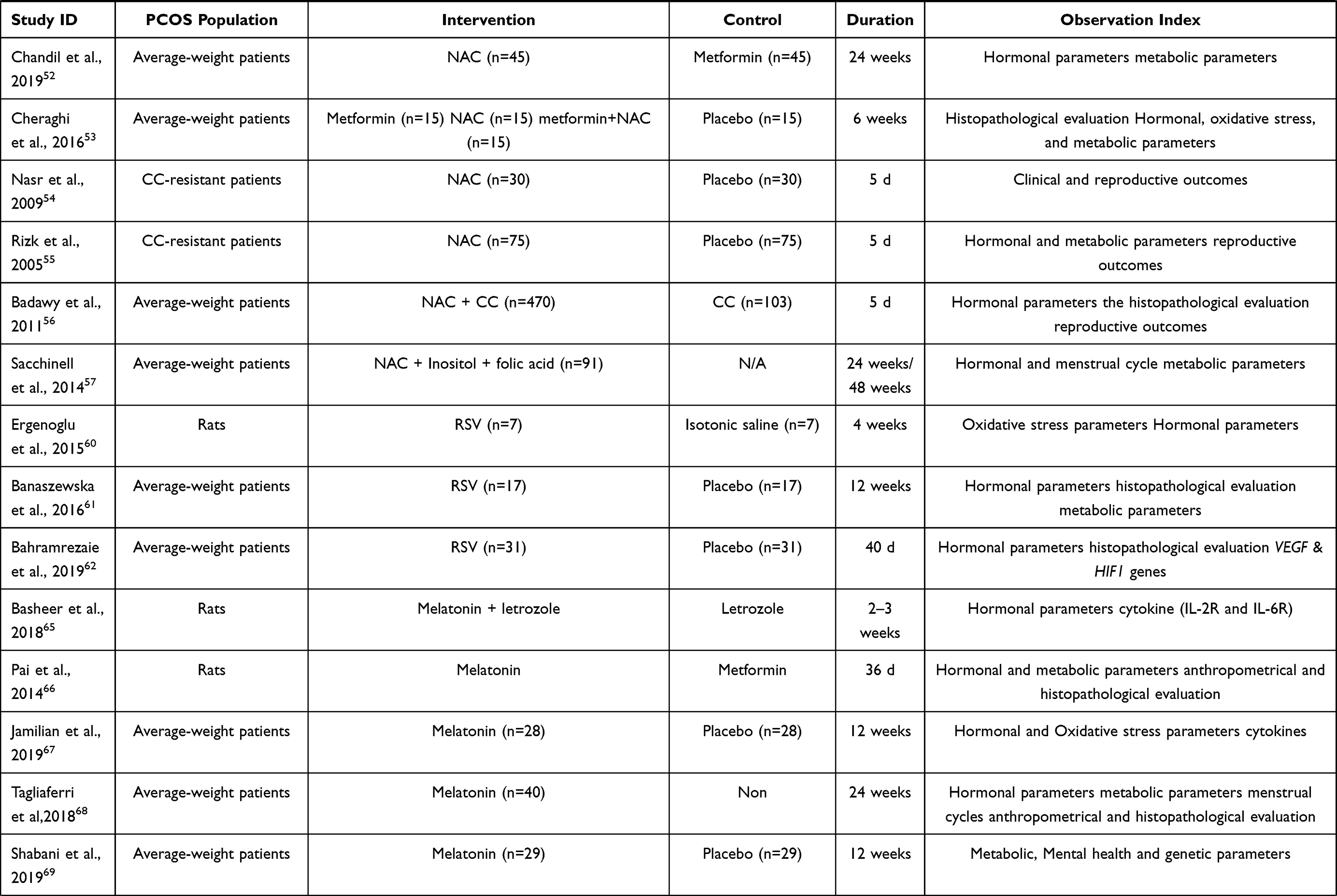 | 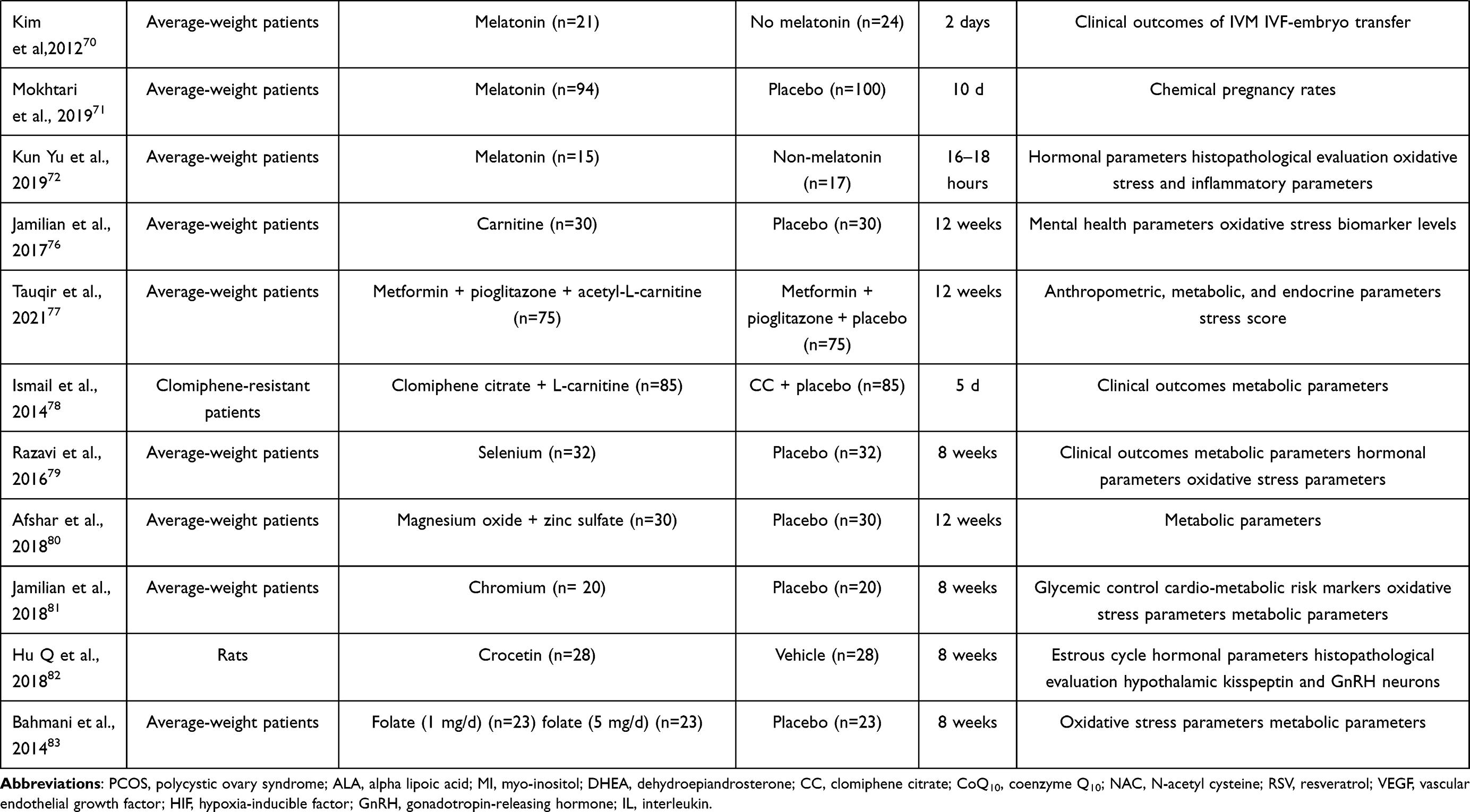 |
Table 1 Characteristics of Included Articles |
Funding
This work was supported by a grant from the National Natural Science Foundation of China (grant No. 81570765), and a “345 Talent Project” of Sheng Jing Hospital of China Medical University.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Ehrmann DA. Polycystic ovary syndrome. J Am Acad Nurse Pract. 2000;12(3):1223–1236. doi:10.1056/NEJMra041536
2. Song Y, Li R. Interpretation of Chinese guidelines for diagnosis and treatment of polycystic ovary syndrome. J Pract Obstet Gynaecol. 2018;34(10):22–26.
3. Liang R, Liu Z, Li P, et al. Kuntai capsules improve glucolipid metabolism in patients with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Medicine. 2019;98(39):e16788. doi:10.1097/MD.0000000000016788
4. Cui L, Chen Z. Introduction to diagnostic criteria and guidelines for diagnosis and treatment of polycystic ovary syndrome. Int J Reprod Health Family Plann. 2011;30(05):405–408.
5. Sharpe A, Morley LC, Tang T, Norman RJ, Balen AH. Metformin for ovulation induction (excluding gonadotrophins) in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;12(12):CD013505. doi:10.1002/14651858.CD013505
6. Lord JM, Flight I, Norman RJ. Metformin in polycystic ovary syndrome: systematic review and meta-analysis. BMJ. 2003;327(7421):951–955. doi:10.1136/bmj.327.7421.951
7. Li H, Chao J, Chen S, et al. Observation on the therapeutic effect of Diane-35 in the treatment of adolescent polycystic ovary syndrome. Int Med Health Guidance News. 2013;19(1):49–51. doi:10.3760/cma.j.issn.1007-1245.2013.01.018
8. Mancini A, Bruno C, Vergani E, d’Abate C, Giacchi E, Silvestrini A. Oxidative stress and low-grade inflammation in polycystic ovary syndrome: controversies and new insights. Int J Mol Sci. 2021;22(4):1667. doi:10.3390/ijms22041667
9. Costello MF, Shrestha B, Eden J, Johnson NP, Sjoblom P. Metformin versus oral contraceptive pill in polycystic ovary syndrome: a Cochrane review. Hum Reprod. 2007;22(5):1200–1209. doi:10.1093/humrep/dem005
10. Turrens JF. Mitochondrial formation of reactive oxygen species. J Physiol. 2003;552(2):335–344. doi:10.1113/jphysiol.2003.049478
11. Herman R, Jensterle M, Janež A, Goričar K, Dolžan V. Genetic variability in antioxidative and inflammatory pathways modifies the risk for PCOS and influences metabolic profile of the syndrome. Metabolites. 2020;10(11):439. doi:10.3390/metabo10110439
12. Chang D, Sha Q, Zhang X, et al. The evaluation of the oxidative stress parameters in patients with primary angle-closure glaucoma. PLoS One. 2011;6(11):e27218. doi:10.1371/journal.pone.0027218
13. Zheng Y, Wang Q, Zhuang W, et al. Cytotoxic, antitumor and immunomodulatory effects of the water-soluble polysaccharides from lotus (Nelumbo nucifera Gaertn) seeds. Molecules. 2016;21(11):1465. doi:10.3390/molecules21111465
14. Bannigida DM, Nayak BS, Vijayaraghavan R. Insulin resistance and oxidative marker in women with PCOS. Arch Physiol Biochem. 2020;126(2):183–186. doi:10.1080/13813455.2018.1499120
15. Özer A, Bakacak M, Kıran H, et al. Increased oxidative stress is associated with insulin resistance and infertility in polycystic ovary syndrome. Ginekol Pol. 2016;87(11):733–738. doi:10.5603/GP.2016.0079
16. Fenkci V, Fenkci S, Yilmazer M, Serteser M. Decreased total antioxidant status and increased oxidative stress in women with polycystic ovary syndrome may contribute to the risk of cardiovascular disease. Fertil Steril. 2003;80(1):123–127. doi:10.1016/s0015-0282(03)00571-5
17. Berlett BS, Stadtman ER. Protein oxidation in ageing, disease and oxidative stress. J Biochem. 1997;272:203–213.
18. Chattopadhayay R, Ganesh A, Samanta J, Jana SK, Chakravarty BN, Chaudhury K. Effect of follicular fluid oxidative stress on meiotic spindle formation in infertile women with polycystic ovarian syndrome. Gynecol Obstet Invest. 2010;69(3):197–202. doi:10.1159/000270900
19. Yalçınkaya E, Cakıroğlu Y, Doğer E, Budak O, Cekmen M, Calışkan E. Effect of follicular fluid NO, MDA and GSH levels on in vitro fertilization outcomes. J Turk Ger Gynecol Assoc. 2013;14(3):136–141. doi:10.5152/jtgga.2013.53323
20. Nuñez-Calonge R, Cortés S, Gutierrez Gonzalez LM, et al. Oxidative stress in follicular fluid of young women with low response compared with fertile oocyte donors. Reprod Biomed Online. 2016;32(4):446–456. doi:10.1016/j.rbmo.2015.12.010
21. Huang T, Huang K. The biomedical function of alpha-lipoic acid. Chem Life. 2004;24(1):58–60.
22. Yi X, Kim K, Yuan W, et al. Mice with heterozygous deficiency of lipoic acid synthase have an increased sensitivity to lipopolysaccharide-induced tissue injury. J Leukoc Biol. 2009;85(1):146–153. doi:10.1189/jlb.0308161
23. Rochette L, Ghibu S, Richard C, Zeller M, Cottin Y, Vergely C. Direct and indirect antioxidant properties of α-lipoic acid and therapeutic potential. Mol Nutr Food Res. 2013;57(1):114–125. doi:10.1002/mnfr.201200608
24. Bast A, Haenen G. Lipoic acid: a multifunctional antioxidant. Bio Factors. 2010;17(14). doi:10.1002/biof.5520170120
25. Masharani U, Gjerde C, Evans JL, Youngren JF, Goldfine ID. Effects of controlled-release alpha lipoic acid in lean, nondiabetic patients with polycystic ovary syndrome. J Diabetes Sci Technol. 2010;4(2):359–364. doi:10.1177/193229681000400218
26. Ivanova LA. Influence of thioctic acid on the hyperinsulinemia and ovarian volume in female patients with polycystic ovary syndrome. Open J Endocr Metab Dis. 2015;5(4):37–40. doi:10.4236/ojemd.2015.54005
27. Genazzani AD, Shefer K, Della Casa D, et al. Modulatory effects of alpha-lipoic acid (ALA) administration on insulin sensitivity in obese PCOS patients. J Endocrinol Invest. 2018;41((5):):583–590. doi:10.1007/s40618-017-0782-z
28. Genazzani AD, Prati A, Marchini F, Petrillo T, Napolitano A, Simoncini T. Differential insulin response to oral glucose tolerance test (OGTT) in overweight/obese polycystic ovary syndrome patients undergoing to myo-inositol (MYO), alpha lipoic acid (ALA), or combination of both. Gynecol Endocrinol. 2019;35(12):1088–1093. doi:10.1080/09513590.2019.1640200
29. Fruzzetti F, Fidecicchi T, Palla G, Gambacciani M. Long-term treatment with α-lipoic acid and myo-inositol positively affects clinical and metabolic features of polycystic ovary syndrome. Gynecol Endocrinol. 2020;36(2):152–155. doi:10.1080/09513590.2019.1640673
30. Fruzzetti F, Capozzi A, Canu A, Lello S. Treatment with d-chiro-inositol and alpha lipoic acid in the management of polycystic ovary syndrome. Gynecol Endocrinol. 2019;35(6):506–510. doi:10.1080/09513590.2018.1540573
31. Pavlik VN, Doody RS, Rountree SD, Darby EJ. Vitamin E use is associated with improved survival in an Alzheimer’s disease cohort. Dement Geriatr Cogn Disord. 2009;28(6):536–540. doi:10.1159/000255105
32. Traber MG, Atkinson J. Vitamin E, antioxidant and nothing more. Free Radic Biol Med. 2007;43(1):4–15. doi:10.1016/j.freeradbiomed.2007.03.024
33. Berretta M, Quagliariello V, Maurea N, et al. Multiple effects of ascorbic acid against chronic diseases: updated evidence from preclinical and clinical studies. Antioxidants. 2020;9(12):1182. doi:10.3390/antiox9121182
34. Saeed M, Saleem U, Anwar F, Ahmad B, Anwar A. Inhibition of valproic acid-induced prenatal developmental abnormalities with antioxidants in rats. ACS Omega. 2020;5(10):4953–4961. doi:10.1021/acsomega.9b03792
35. Olaniyan OT, Femi A, Iliya G, et al. Vitamin C suppresses ovarian pathophysiology in experimental polycystic ovarian syndrome. Pathophysiology. 2019;26(3–4):331–341. doi:10.1016/j.pathophys.2019.08.003
36. Shirazi SH, Pourghassem Gargari B, Izadi A, Taghizadeh SH, Parizad M. Effect of vitamin E on serum levels of vascular endothelial growth factor and angiopoietin-1 in women with polycystic ovary syndrome: a pilot randomized, placebo-controlled trial. Int J Fertil Steril. 2021;15(1):44–50. doi:10.22074/ijfs.2020.45677
37. Morsy AA, Sabri NA, Mourad AM, Mojahed EM, Shawki MA. Randomized controlled open-label study of the effect of vitamin E supplementation on fertility in clomiphene citrate-resistant polycystic ovary syndrome. J Obstet Gynaecol Res. 2020;46(11):2375–2382. doi:10.1111/jog.14467
38. Su N, Deng W, Zhang L, et al. Application of vitamin E combined with Diane-35 in the treatment of polycystic ovary syndrome infertility. J Trop Med. 2016;16(6):759–762.
39. Wang L. The clinical effect of vitamin E combined with ethinyl estradiol and cyproterone tablets in the treatment of infertility with polycystic ovary syndrome. Henan Med Res. 2019;28(04):124–126.
40. Xu H, Vitamin LJ. E combined with Diane-35 in the treatment of polycystic ovary syndrome infertility and analysis of adverse reactions. China Health Nutr. 2019;29(020):285–286.
41. You W. Anti-inflammatory and antioxidant effects of vitamin E combined with metformin in the treatment of insulin-resistant PCOS. Zhejiang Clin Med. 2019;21(8):1677.
42. Ernster L, Dallner G. Biochemical, physiological and medical aspects of ubiquinone function. Biochim Biophys Acta. 1995;1271(1):195–204. doi:10.1016/0925-4439(95)00028-3
43. Dutton PL, Ohnishi T, Darrouzet E, et al. Coenzyme Q oxidation reduction reactions in mitochondrial electron transport Coenzyme Q: molecular mechanisms in health and disease. Boca Raton CRC Press. 2000:65–82. doi:10.1201/9781420036701.sec1b
44. Taghizadeh S, Izadi A, Shirazi S, Parizad M, Pourghassem Gargari B. The effect of coenzyme Q10 supplementation on inflammatory and endothelial dysfunction markers in overweight/obese polycystic ovary syndrome patients. Gynecol Endocrinol. 2021;37(1):26–30. doi:10.1080/09513590.2020.1779689
45. Izadi A, Ebrahimi S, Shirazi S, et al. Hormonal and metabolic effects of coenzyme Q10 and/or vitamin E in patients with polycystic ovary syndrome. J Clin Endocrinol Metab. 2019;104(2):319–327. doi:10.1210/jc.2018-01221
46. Liu M, Zhu H, Hu X, Zhu Y, Chen H. Efficacy of coenzyme Q10 supplementation on glucose metabolism, lipid profiles, and biomarkers of inflammation in women with polycystic ovary syndrome: a protocol for a systematic review and meta-analysis. Medicine. 2020;99(46):e23130. doi:10.1097/MD.0000000000023130
47. El Refaeey A, Selem A, Badawy A. Combined coenzyme Q10 and clomiphene citrate for ovulation induction in clomiphene-citrate-resistant polycystic ovary syndrome. Reprod Biomed Online. 2014;29(1):119–124. doi:10.1016/j.rbmo.2014.03.011
48. Thakker D, Raval A, Patel I, Walia R. N-acetylcysteine for polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled clinical trials. Obstet Gynecol Int. 2015;2015:817849. doi:10.1155/2015/817849
49. Fulghesu AM, Ciampelli M, Muzj G, et al. N-acetyl-cysteine treatment improves insulin sensitivity in women with polycystic ovary syndrome. Fertil Steril. 2002;77(6):1128–1135. doi:10.1016/s0015-0282(02)03133-3
50. Moghetti P, Castello R, Negri C, et al. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol Metab. 2000;85(1):139–146. doi:10.1210/jcem.85.1.6293
51. Dunaif A, Scott D, Finegood D, Quintana B, Whitcomb R. The insulin-sensitizing agent troglitazone improves metabolic and reproductive abnormalities in the polycystic ovary syndrome. J Clin Endocrinol Metab. 1996;81(9):3299–3306. doi:10.1210/jcem.81.9.8784087
52. Chandil N, Pande S, Sen SS, Gupta D. Comparison of metformin and N acetylcysteine on clinical, metabolic parameter and hormonal profile in women with polycystic ovarian syndrome. J Obstet Gynaecol India. 2019;69(1):77–81. doi:10.1007/s13224-018-1135-3
53. Cheraghi E, Mehranjani MS, Shariatzadeh MA, Esfahani MH, Ebrahimi Z. N-Acetylcysteine improves oocyte and embryo quality in polycystic ovary syndrome patients undergoing intracytoplasmic sperm injection: an alternative to metformin. Reprod Fertil Dev. 2016;28(6):723–731. doi:10.1071/RD14182
54. Nasr A. Effect of N-acetyl-cysteine after ovarian drilling in clomiphene citrate-resistant PCOS women: a pilot study. Reprod Biomed Online. 2010;20(3):403–409. doi:10.1016/j.rbmo.2009.12.012
55. Rizk AY, Bedaiwy MA, Al-Inany HG. N-acetyl-cysteine is a novel adjuvant to clomiphene citrate in clomiphene citrate-resistant patients with polycystic ovary syndrome. Fertil Steril. 2005;83(2):367–370. doi:10.1016/j.fertnstert.2004.07.960
56. Badawy A, State O, Abdelgawad S. N-Acetyl cysteine and clomiphene citrate for induction of ovulation in polycystic ovary syndrome: a cross-over trial. Acta Obstet Gynecol Scand. 2011;86(2):218–222. doi:10.1080/00016340601090337
57. Sacchinelli A, Venturella R, Lico D, et al. The efficacy of inositol and N-acetyl cysteine administration (Ovaric HP) in improving the ovarian function in infertile women with PCOS with or without insulin resistance. Obstet Gynecol Int. 2014;2014:141020. doi:10.1155/2014/141020
58. Tomé-Carneiro J, Larrosa M, González-Sarrías A, Tomás-Barberán FA, García-Conesa MT, Espín JC. Resveratrol and clinical trials: the crossroad from in vitro studies to human evidence. Curr Pharm Des. 2013;19(34):6064–6093. doi:10.2174/13816128113199990407
59. Tung BT, Rodríguez-Bies E, Ballesteros-Simarro M, Motilva V, Navas P, López-Lluch G. Modulation of endogenous antioxidant activity by resveratrol and exercise in mouse liver is age dependent. J Gerontol a Biol Sci Med Sci. 2014;69(4):398–409. doi:10.1093/gerona/glt102
60. Ergenoglu M, Yildirim N, Yildirim AG, et al. Effects of resveratrol on ovarian morphology, plasma anti-mullerian hormone, IGF-1 levels, and oxidative stress parameters in a rat model of polycystic ovary syndrome. Reprod Sci. 2015;22(8):942–947. doi:10.1177/1933719115570900
61. Banaszewska B, Wrotyńska-Barczyńska J, Spaczynski RZ, Pawelczyk L, Duleba AJ. Effects of resveratrol on polycystic ovary syndrome: a double-blind, randomized, placebo-controlled trial. J Clin Endocrinol Metab. 2016;101(11):4322–4328. doi:10.1210/jc.2016-1858
62. Bahramrezaie M, Amidi F, Aleyasin A, et al. Effects of resveratrol on VEGF & HIF1 genes expression in granulosa cells in the angiogenesis pathway and laboratory parameters of polycystic ovary syndrome: a triple-blind randomized clinical trial. J Assist Reprod Genet. 2019;36(8):1701–1712. doi:10.1007/s10815-019-01461-6
63. Tomita T, Mori T, Onishi Y. β-Arrestin 1 (ARRB1) serves as a molecular marker of the peripheral circadian rhythm. Int J Oral Sci. 2019;11(4):32. doi:10.1038/s41368-019-0065-y
64. Tan DX, Manchester LC, Esteban-Zubero E, Zhou Z, Reiter RJ. Melatonin as a potent and inducible endogenous antioxidant: synthesis and metabolism. Molecules. 2015;20(10):18886–18906. doi:10.3390/molecules201018886
65. Basheer M, Rai S, Ghosh H, Ahmad Hajam Y. Therapeutic efficacy of melatonin against polycystic ovary syndrome (PCOS) induced by letrozole in Wistar rat. Pak J Biol Sci. 2018;21(7):340–347. doi:10.3923/pjbs.2018.340.347
66. Pai SA, Majumdar AS. Protective effects of melatonin against metabolic and reproductive disturbances in polycystic ovary syndrome in rats. J Pharm Pharmacol. 2014;66(12):1710–1721. doi:10.1111/jphp.12297
67. Jamilian M, Foroozanfard F, Mirhosseini N, et al. Effects of melatonin supplementation on hormonal, inflammatory, genetic, and oxidative stress parameters in women with polycystic ovary syndrome. Front Endocrinol. 2019;10:273. doi:10.3389/fendo.2019.00273
68. Tagliaferri V, Romualdi D, Scarinci E, et al. Melatonin treatment may be able to restore menstrual cyclicity in women with PCOS: a pilot study. Reprod Sci. 2018;25(2):269–275. doi:10.1177/1933719117711262
69. Shabani A, Foroozanfard F, Kavossian E, et al. Effects of melatonin administration on mental health parameters, metabolic and genetic profiles in women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. J Affect Disord. 2019;250:51–56. doi:10.1016/j.jad.2019.02.066
70. Kim MK, Park EA, Kim HJ, et al. Does supplementation of in-vitro culture medium with melatonin improve IVF outcome in PCOS? Reprod Biomed Online. 2013;26(1):22–29. doi:10.1016/j.rbmo.2012.10.007
71. Mokhtari F, Akbari Asbagh F, Azmoodeh O, Bakhtiyari M, Almasi-Hashiani A. Effects of melatonin administration on chemical pregnancy rates of polycystic ovary syndrome patients undergoing intrauterine insemination: a randomized clinical trial. Int J Fertil Steril. 2019;13(3):225–229. doi:10.22074/ijfs.2019.5717
72. Yu K, Wang RX, Li MH, et al. Melatonin reduces androgen production and upregulates heme oxygenase-1 expression in granulosa cells from PCOS patients with hypoestrogenia and hyperandrogenia. Oxid Med Cell Longev. 2019;2019:8218650. doi:10.1155/2019/8218650
73. Steiber A, Kerner J, Hoppel CL. Carnitine: a nutritional, biosynthetic, and functional perspective. Mol Aspects Med. 2004;25(5–6):455–473. doi:10.1016/j.mam.2004.06.006
74. Bortolato B, Miskowiak KW, Köhler CA, et al. Cognitive remission: a novel objective for the treatment of major depression? BMC Med. 2016;14(1):9. doi:10.1186/s12916-016-0560-3
75. Wang SM, Han C, Lee SJ, Patkar AA, Masand PS, Pae CU. A review of current evidence for acetyl-l-carnitine in the treatment of depression. J Psychiatr Res. 2014;53:30–37. doi:10.1016/j.jpsychires.2014.02.005
76. Jamilian H, Jamilian M, Samimi M, et al. Oral carnitine supplementation influences mental health parameters and biomarkers of oxidative stress in women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Gynecol Endocrinol. 2017;33(6):442–447. doi:10.1080/09513590.2017.1290071
77. Tauqir S, Israr M, Rauf B, et al. Acetyl-L-carnitine ameliorates metabolic and endocrine alterations in women with PCOS: a double-blind randomized clinical trial. Adv Ther. 2021;38(7):3842–3856. doi:10.1007/s12325-021-01789-5
78. Ismail AM, Hamed AH, Saso S, Thabet HH. Adding L-carnitine to clomiphene resistant PCOS women improves the quality of ovulation and the pregnancy rate. A randomized clinical trial. Eur J Obstet Gynecol Reprod Biol. 2014;180:148–152. doi:10.1016/j.ejogrb.2014.06.008
79. Razavi M, Jamilian M, Kashan ZF, et al. Selenium supplementation and the effects on reproductive outcomes, biomarkers of inflammation, and oxidative stress in women with polycystic ovary syndrome. Horm Metab Res. 2016;48(3):185–190. doi:10.1055/s-0035-1559604
80. Afshar Ebrahimi F, Foroozanfard F, Aghadavod E, Bahmani F, Asemi Z. The effects of magnesium and zinc co-supplementation on biomarkers of inflammation and oxidative stress, and gene expression related to inflammation in polycystic ovary syndrome: a randomized controlled clinical trial. Biol Trace Elem Res. 2018;184(2):300–307. doi:10.1007/s12011-017-1198-5
81. Jamilian M, Zadeh Modarres S, Amiri Siavashani M, et al. The influences of chromium supplementation on glycemic control, markers of cardio-metabolic risk, and oxidative stress in infertile polycystic ovary syndrome women candidate for in vitro fertilization: a randomized, double-blind, placebo-controlled trial. Biol Trace Elem Res. 2018;185(1):48–55. doi:10.1007/s12011-017-1236-3
82. Hu Q, Jin J, Zhou H, et al. Crocetin attenuates DHT-induced polycystic ovary syndrome in mice via revising kisspeptin neurons. Biomed Pharmacother. 2018;107:1363–1369. doi:10.1016/j.biopha.2018.08.135
83. Bahmani F, Karamali M, Shakeri H, Asemi Z. The effects of folate supplementation on inflammatory factors and biomarkers of oxidative stress in overweight and obese women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled clinical trial. Clin Endocrinol. 2014;81(4):582–587. doi:10.1111/cen.12451
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.