")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Cigarette Smoking and Peripheral Vascular Disease are Associated with Increasing Risk of ESKAPE Pathogen Infection in Diabetic Foot Ulcers
Authors Li T, Li Z , Huang L, Tang J, Ding Z, Zeng Z, Liu Y, Liu J
Received 1 August 2022
Accepted for publication 18 October 2022
Published 26 October 2022 Volume 2022:15 Pages 3271—3283
DOI https://doi.org/10.2147/DMSO.S383701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Gian Paolo Fadini
Tingting Li,* Zhaoyinqian Li,* Li Huang, Jingyang Tang, Zixuan Ding, Zhangrui Zeng, Yao Liu, Jinbo Liu
Department of Laboratory Medicine, the Affiliated Hospital of Southwest Medical University, Lu Zhou, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinbo Liu, Department of Laboratory Medicine, the Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China, Tel +86 08303165730, Email [email protected]
Objective: Diabetic foot ulcers (DFUs) and ESKAPE pathogens have attracted attention globally, but the role of ESKAPE pathogens in diabetic foot infection is not well described. The purpose of this study was to evaluate the clinical features, antimicrobial resistance, and risk factors for ESKAPE infection in patients with DFUs.
Methods: A retrospective study was conducted on 180 patients with diabetic foot infection admitted to The Affiliated Hospital of Southwest Medical University (Luzhou, China), from January 2017 to April 2021. Antimicrobial susceptibilities of all isolates were determined. Multivariate logistic regression analysis was performed to analyze the independent risk factors for ESKAPE infection, multidrug-resistant (MDR)-ESKAPE infection, MDR-pathogen infection, and severe group in patients with DFUs.
Results: A total of 206 isolates were collected, of which 42.2% were ESKAPE pathogens. The independent risk factors for ESKAPE infection were cigarette smoking (OR = 1.958; 95% CI, 1.015– 3.777) and peripheral vascular disease (OR = 2.096; 95% CI, 1.100– 3.992), while alcohol consumption (OR = 2.172; 95% CI, 1.104– 4.272) was the independent risk factor for MDR-pathogen infection. Additionally, the independent risk factors for severe DFU group were invasive treatment (OR = 326.642; 95% CI, 76.644– 1392.08), the duration of systemic antibiotic treatment (OR = 0.918; 95% CI, 0.849– 0.992), and length of hospital stay (OR = 1.145; 95% CI, 1.043– 1.256). No independent risk factors for MDR-ESKAPE infection were found.
Conclusion: Our data established the microbiological features of ESKAPE pathogens and clinical manifestations of diabetic foot infection, and provide support for monitoring and management of ESKAPE infection in patients with DFUs in southwest China.
Keywords: diabetic foot ulcers, ESKAPE pathogens, infection, antimicrobial resistance, risk factors
Introduction
A recent study of adults between the ages of 20 and 79 worldwide suggested that there was a total of 537 million patients with diabetes in 2021, and the number is expected to increase to 643 million and 784 million by 2030 and 2045.1 Diabetic foot ulcers (DFUs) are caused mainly by a combination of the following three factors: an extrinsic mechanical factor, such as high plantar pressures or local trauma; an intrinsic factor, such as peripheral neuropathy or micro-vascular disease; impaired host immune response.2 At present, DFUs have become one of the most common, expensive, and serious complications of diabetes.3 In China, approximately 25% hospitalization among patients with diabetes are related to infection or ischemic diabetic foot, of which infection is more common. Diabetic foot infections can manifest as local signs of inflammation, including erythema, swelling, increased skin temperature, pain, and purulent discharge formation, and also display systemic inflammatory symptoms, such as fever, hemodynamic instability, and metabolic disorders.4,5 Patients with DFUs not only have a high amputation rate, accounting for 60% of non-traumatic amputees,6 but their risk of death is 2.5 times higher than that of patients without DFUs,6,7 which places a huge psychological and financial burden on patients, their families, and public health system. Currently, the main treatment strategies for diabetic foot infections are wound care, antibiotics, and amputation.8 However, their limitations result in unsatisfactory treatment outcomes. Moreover, no empirical antimicrobial therapy has been shown to be effective in the treatment of diabetic foot infection.9 Therefore, strengthening early diagnosis is an essential part of the effective treatment of DFUs.
Diabetic foot infections are caused by a myriad of microorganisms, but Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp., which are particularly prevalent nosocomial pathogens and are often referred to by the mnemonic acronym “ESKAPE” originally defined by the Infectious Diseases Society of America.10 S. aureus is the most common pathogen isolated from DFUs globally, and K. pneumoniae and P. aeruginosa are the most frequent isolates among Gram-negative bacteria other than Escherichia coli. Moreover, chronic infection and relapse are tightly associated with Enterococcus and Acinetobacter.11–14 The clinical treatment of ESKAPE pathogens is receiving increasing attention in recent years, not only due to the high pathogenicity, but also the rapid dissemination of antimicrobial resistance.15 In February 2017, the World Health Organization released a list of pathogens for which there is an urgent need to develop new antibiotics to treat them. The ESKAPE group was selected as the “priority state”.16
Although many studies have reported the risk factors of diabetic foot infection,17,18 the characteristics of patients with diabetic foot infection caused by specific ESKAPE pathogens are still unknown. Therefore, the purpose of this study is to investigate the clinical manifestations, antimicrobial resistance, and risk factors for ESKAPE infection in patients with DFUs in southwest China.
Materials and Methods
Study Design
The retrospective data of all patients hospitalized with DFUs from January 2017 to April 2021 in The Affiliated Hospital of Southwest Medical University (Luzhou, China) were obtained and used in this study. A total of 180 patients were included in this study and were selected according to the following criteria: (1) met the clinical diagnostic criteria of DFUs; (2) had at least one hospitalization record from January 2017 to April 2021; (3) had complete clinical data. The exclusion criteria were the following: (1) missing wound culture during hospitalization; (2) no screening for diabetic complications; (3) incomplete or omitted medical record information. The list of patients included in the study is shown in Figure 1.
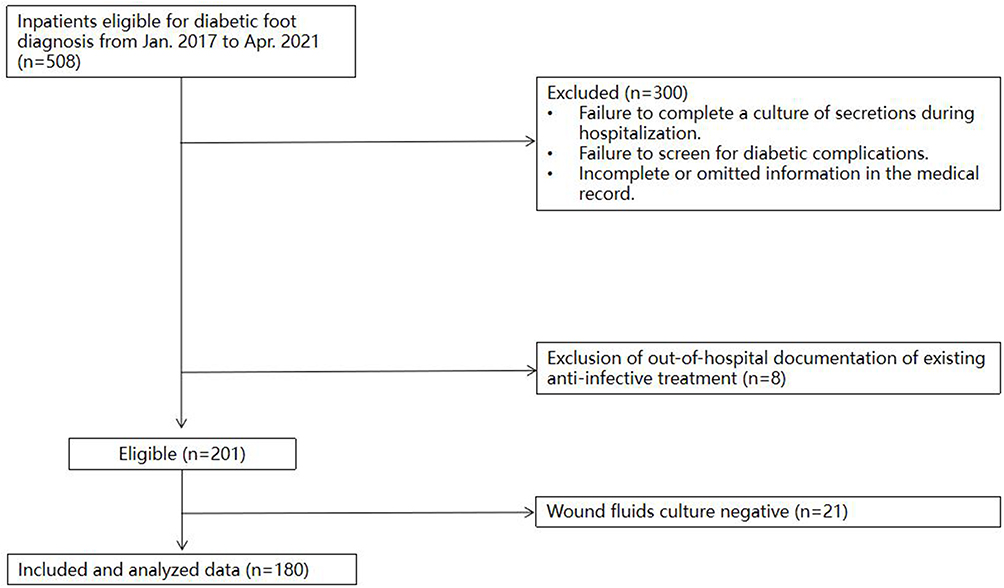 |
Figure 1 Inclusion of the study population. |
Data Collection and Definitions
The information of all qualified patients with DFUs was collected from medical records, including basic demographic data (age, sex, duration of diabetes, length of hospital stay, etc.), characteristics of DFUs (ulcer area, depth, ischemic necrosis, etc.), underlying diseases (hypertension, hyperlipidemia, coronary heart disease, etc.), clinical treatment (blood glucose control, foot wound care, toe resection, surgery, antimicrobial therapy, etc.), and laboratory results (white blood cell count, neutrophil ratio, etc.).
Identification and Antimicrobial Susceptibility Testing
Identification and antimicrobial susceptibility testing of all clinical isolates that were collected from patients with DFUs were performed using the MicroScan Walkaway 96 Plus system (Beckman Coulter, Brea, CA, USA) and the matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry (MS) Biotyper Microflex LT system (Bruker Daltonics, Fremont, CA, USA). Gram-positive bacteria were tested for susceptibility to 14 antimicrobial agents, including penicillin, ampicillin, oxacillin, ciprofloxacin, levofloxacin, daptomycin, gentamicin, erythromycin, tetracycline, nitrofurantoin, vancomycin, rifampicin, quinopristine-dalfopristin, and linezolid. In addition, 16 antimicrobial agents, namely imipenem, meropenem, gentamicin, tobramycin, amikacin, piperacillin-tazobactam, ampicillin-sulbactam, cefuroxime, cefotaxime, ceftriaxone, ceftazidime, cefepime, aztreonam, ciprofloxacin, levofloxacin, and cotrimoxazole, were selected to detect gram-negative bacteria. The results were interpreted according to the Clinical and Laboratory Standards Institute (CLSI-2020).
Statistical Analysis
Statistical analysis was performed using the IBM SPSS software version 28.0 (IBM Corporation, Armonk, NY, USA) for Windows. Classification variables are expressed in frequency and percentage. Continuous variables are expressed as the mean ± standard deviation (SD) or median and interquartile range (IQR). Chi-square test and Fisher’s exact test were used to analyze classified variables. The continuity variables were tested by rank sum test. Multivariate Logistic regression analysis was used to determine the independent risk factors of infection in patients with DFUs between ESKAPE group and non-ESKAPE group, multidrug-resistant (MDR)-ESKAPE group and non-MDR-ESKAPE group, mild DFU group (Wagner 0–2) and severe DFU group (Wagner 3–5). Significance was defined as single factor P < 0.1, multi-factor P < 0.05.
Results
Clinical Characteristics
A total of 7966 patients with diabetes were hospitalized from January 2017 to April 2021, of which 508 (6.4%) were diagnosed with DFUs. In this study, 180 patients with DFUs were included in the following analysis. The average age of the patients was 63.42 ± 10.98 years old, and 38.8% were female. Hypertension (57.7%) and anemia (38.3%) were the two most common underlying comorbidities. Peripheral neuropathy (85.6%) was most associated with DFUs among other diabetes complications, and neuropathy was the most common type of ulcers (51.2%). The Wagner grade of the patients with diabetic foot infection was generally between 2 and 4. The median course of diabetes in these patients was 10.21 ± 7.172 years, and oral hypoglycemic drugs (38.3%) were the most common treatment (Table 1).
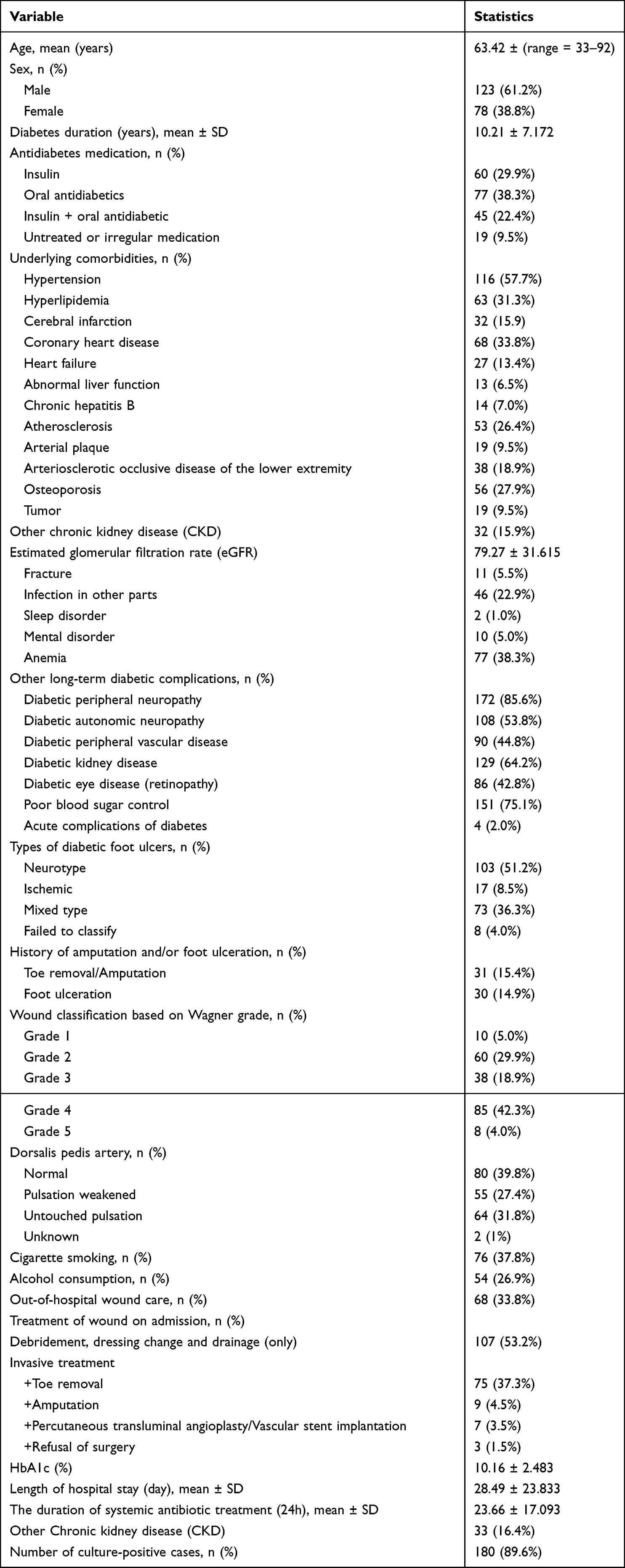 |
Table 1 Clinical Characteristics of 180 Patients with Diabetic Foot Infection |
Distribution of Bacterial Isolates
A total of 206 isolates were isolated from 180 patients with DFUs. In addition, 25 patients (11.9%) were positive to two or more isolates during hospitalization. Among the 46 species of microorganisms present, 98 isolates (47.6%) were gram-negative bacteria and 97 isolates (47.1%) were gram-positive bacteria, and 11 isolates (5.3%) were fungi. S. aureus (52.6%) was the most common isolate, followed by Proteus, E. coli, P. aeruginosa and Enterobacter spp., accounting for 22.5, 18.3, 17.4 and 11.2%, respectively (Figure 2). Of the 206 isolates, 87 (42.2%) were ESKAPE pathogens, including 4 isolates of E. faecium, 51 isolates of S. aureus, 3 isolates of K. pneumoniae, 1 isolate of A. baumannii, 17 isolates of P. aeruginosa, and 11 isolates of Enterobacter spp.
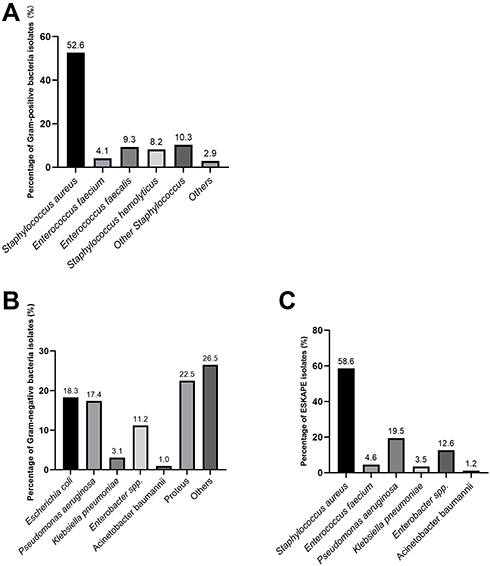 |
Figure 2 Distribution characteristics of pathogens isolated from DFUs. (A) Distribution of various types of Gram-positive bacteria; (B) Distribution of various types of Gram-negative bacteria; (C) Distribution of various types of ESKAPE pathogens. |
Antimicrobial Susceptibility Profiles
The antimicrobial susceptibility test was carried out on all ESKAPE pathogens (Tables 2 and 3). S. aureus was highly resistant to ampicillin and penicillin, accounting for 88.2 and 86.3%, respectively. It is worth noting that a total of 8 isolates of methicillin-resistant S. aureus (MRSA) were detected in this study. All E. faecium were resistant to ciprofloxacin, levofloxacin, and erythromycin. Both K. pneumoniae and A. baumannii were relatively susceptible, even though only 3 isolates and 1 isolate were collected, respectively. Meanwhile, all the resistance rates of the antimicrobial agents tested on P. aeruginosa and Enterobacter spp. were less than 36%.
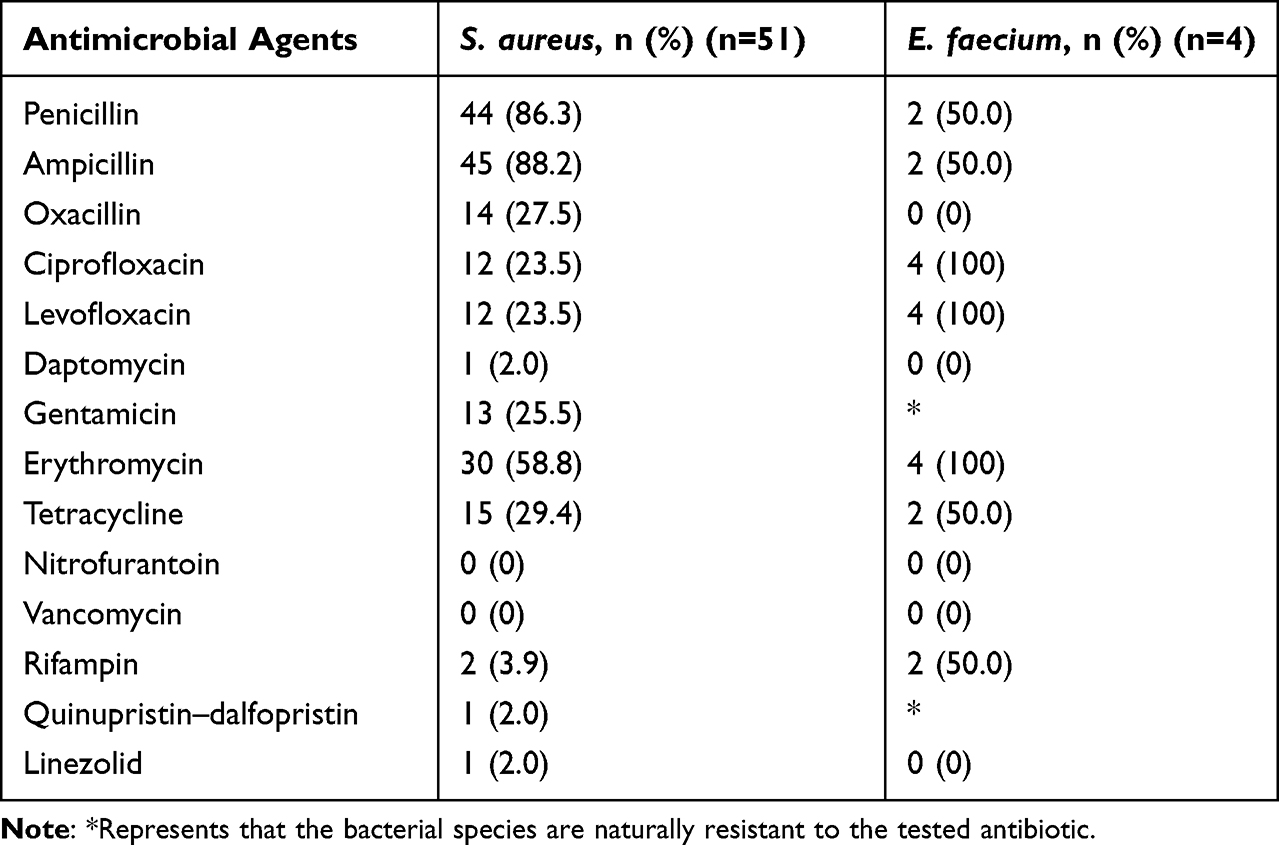 |
Table 2 Antimicrobial Susceptibility of ESKAPE: Gram-Positive Pathogens |
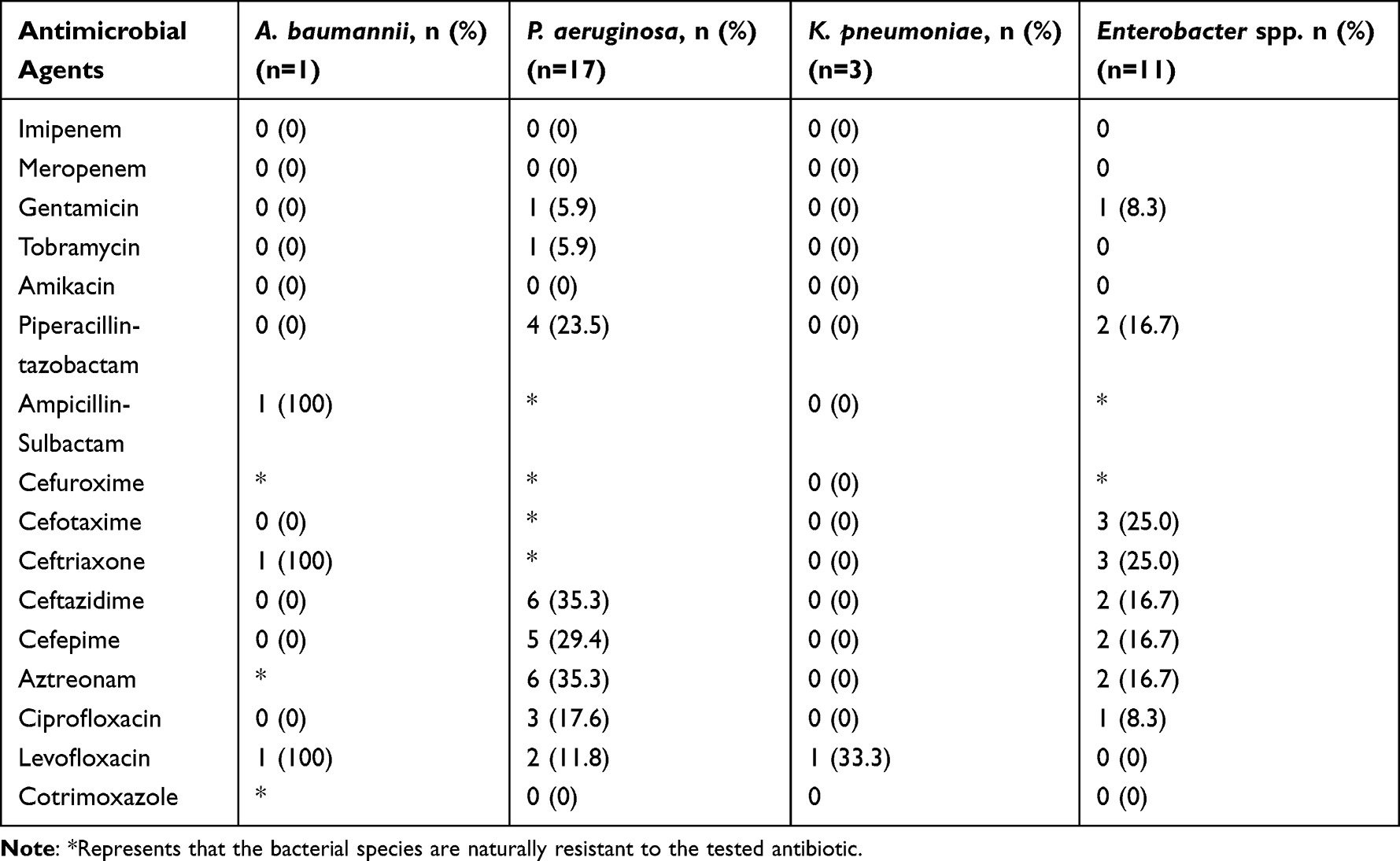 |
Table 3 Antimicrobial Susceptibility of ESKAPE: Gram-Negative Pathogens |
Comparison of Diabetic Foot Infection Between the ESKAPE Group and Non-ESKAPE Group
Compared with patients with non-ESKAPE infection, patients infected with ESKAPE pathogens were more likely to cigarette smoking (45.6% vs 33.7%, P = 0.100) and had more peripheral vascular disease complications (57.0% vs 40.6%, P = 0.029). However, the length of hospital stay (27.54 ± 31.557 vs 29.78 ±17.907, P = 0.040) and the duration of systemic antibiotic treatment (21.76 ± 19.503 vs 25.52 ± 15.668, P = 0.021) were shorter (Table 4). Patients with non-ESKAPE infection had a higher proportion of diabetic kidney disease (68.3% vs 54.4%, P = 0.057) and mental disorders (9.9% vs 0%, P = 0.004) (Table 4). Logistic regression analysis showed that peripheral vascular disease (odds ratio [OR] = 2.096; 95% confidence interval [CI], 1.100–3.992) and cigarette smoking (OR = 1.958; 95% CI, 1.015–3.777) were independent risk factors for ESKAPE infection in patients with DFUs (Table 5).
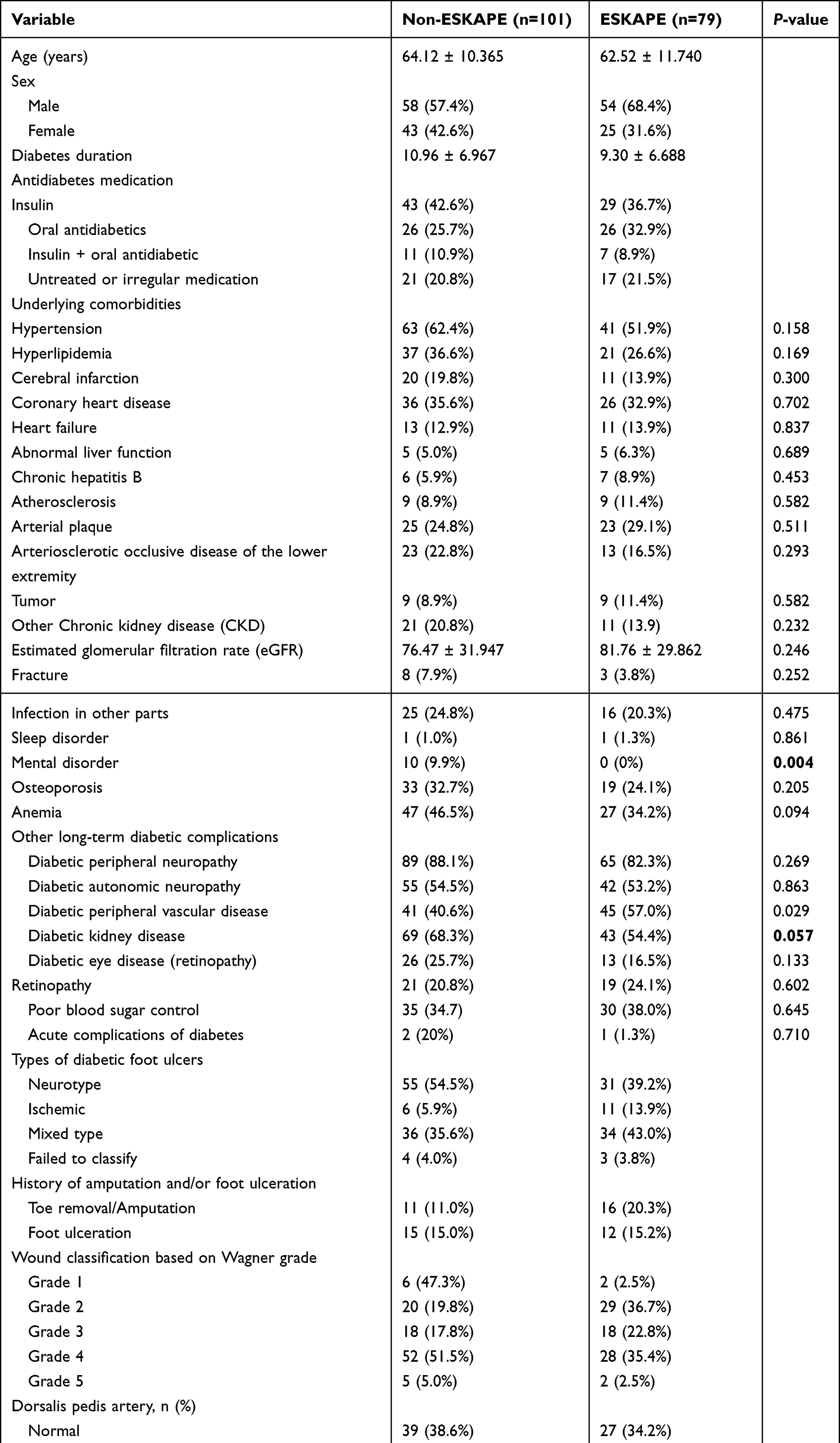 |
Table 4 Clinical Characteristics and Laboratory Records of Patients with ESKAPE Pathogen Infection |
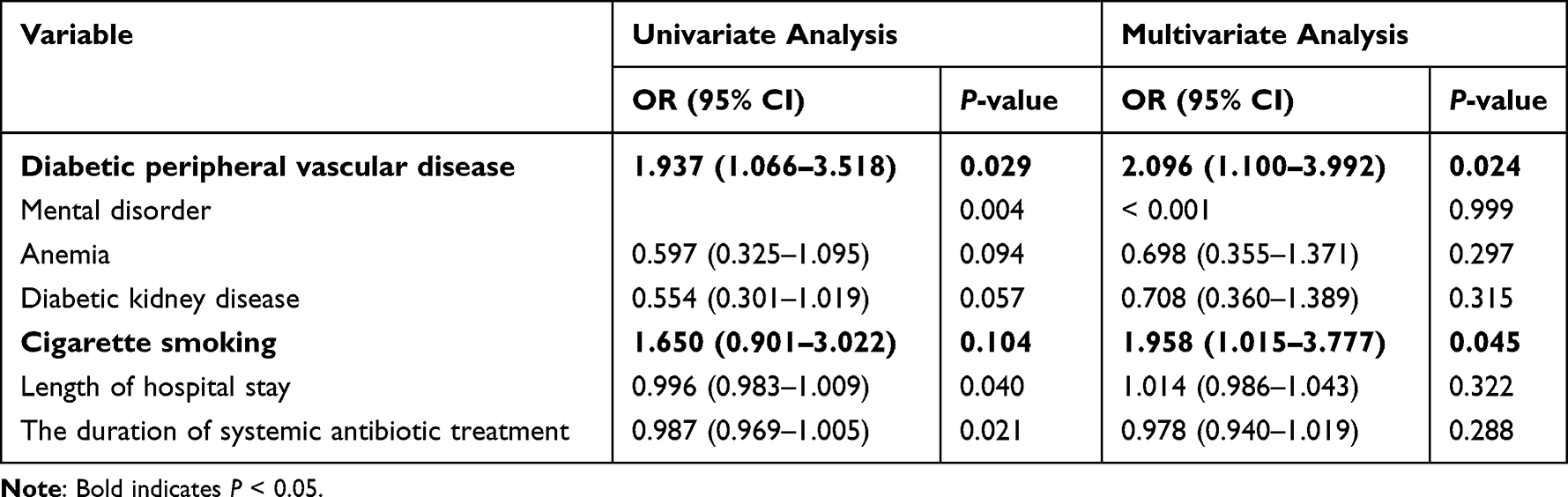 |
Table 5 Clinical Risk Factors for ESKAPE Pathogen Infection in Patients with DFUs |
Comparison of Diabetic Foot Infection Between the MDR-ESKAPE Group and Non-MDR-ESKAPE Group
Patients with non-MDR-ESKAPE infection were more prone to develop lower extremity arteriosclerotic occlusive disease (8.8% vs 24.4%, P = 0.083), and weakened or non-palpable dorsalis pedis artery (50.0% vs 73.3%, P = 0.330). In contrast, the MDR-ESKAPE infection was more likely to be associated with patients who had infections in other sites. (29.4% vs 13.3% P = 0.078). However, no independent risk factors for MDR-ESKAPE infection in patients with DFUs were found.
Comparison of Diabetic Foot Infection Between the MDR-Pathogen Group and Non-MDR-Pathogen Group
Patients infected with MDR-pathogens were more likely to suffer from coronary heart disease (41.6% vs 29.1%, P = 0.082) and autonomic neuropathy (61.0% vs 48.5%, P = 0.096). Also, higher rate of alcohol consumption appeared in the MDR-pathogen group, and it was the only independent risk factor for MDR-pathogen infection in patients with DFUs (OR = 2.172; 95% CI, 1.104–4.272) (Table 6).
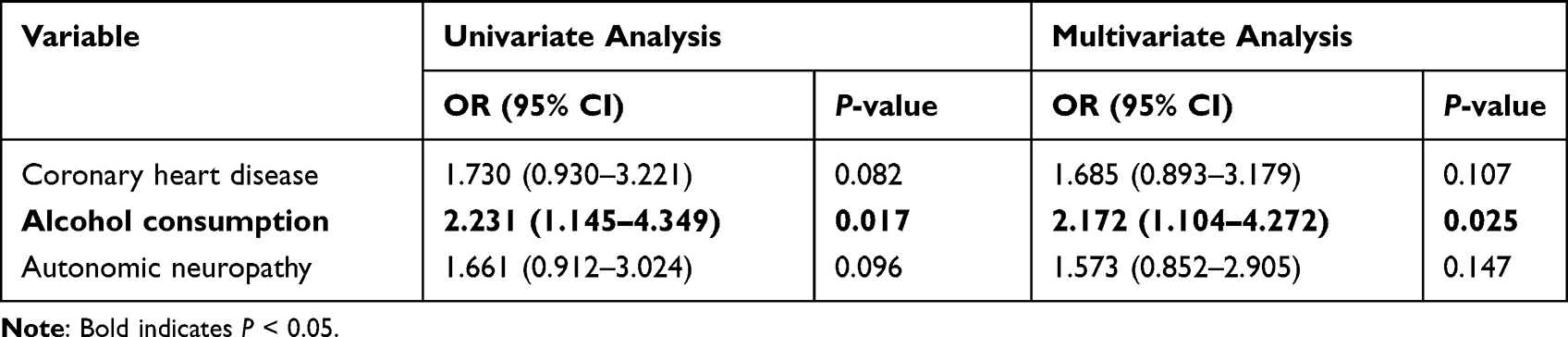 |
Table 6 Clinical Risk Factors for MDR-Pathogen Infection in Patients with DFUs |
Comparison of Diabetic Foot Infection Between the Mild DFU Group and Severe DFU Group
As shown in Table 7, severe patients (Wagner 3–5) had a higher rate of anemia than those in the mild group (Wagner 0–2) (50.6% vs 32.3%, P = 0.013), and their dorsalis pedis arteries were weakened, or non-palpable and showed more abnormalities (70.1% vs 57.0% P = 0.068). In addition, a trend of higher incidence of invasive treatment (94.1% vs 7.5%, P < 0.001) was observed in patients with severe DFUs, and significantly higher rates of the duration of systemic antibiotic treatment (27.59±17.299 vs 20.4±17.063, P = 0.001) and length of hospital stay (31.66±18.513 vs 26.13±29.325, P = 0.001) were also observed in patients with severe DFUs. Importantly, invasive treatment (OR = 326.642; 95% CI, 76.644–1392.08), the duration of systemic antibiotic treatment (OR = 0.918; 95% CI, 0.849–0.992), and length of hospital stay (OR = 1.145; 95% CI, 1.043–1.256) were independent risk factors for patients with severe DFUs.
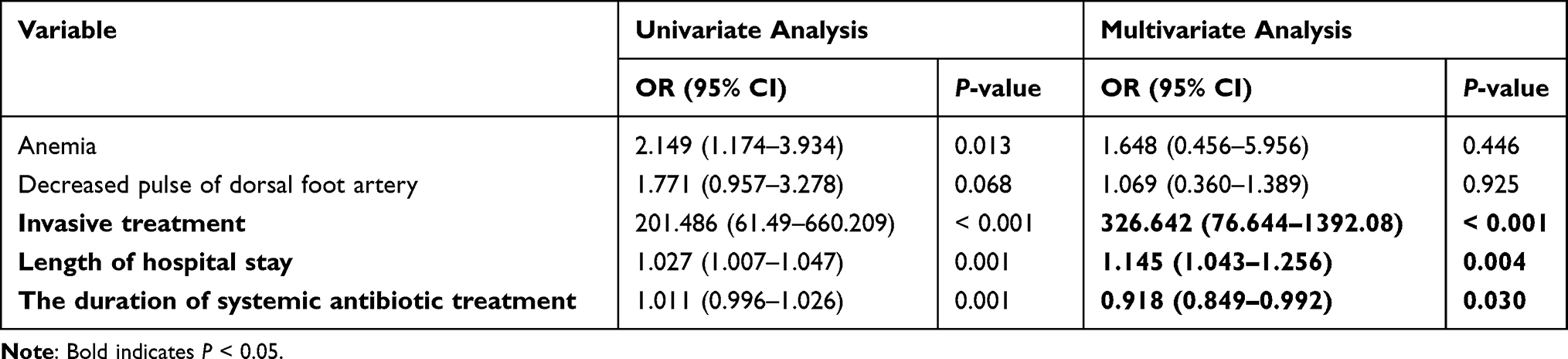 |
Table 7 Clinical Risk Factors for Patients with Severe DFUs |
Discussion
As a metabolic syndrome, the clinical feature of diabetes is a hyperglycemic state resulting from decreased insulin secretion, insulin malfunction, or both.3 Persistent hyperglycemia will lead to systemic diabetic chronic inflammation due to increased inflammatory cytokine levels and secretion of cytotoxic mediators.19,20 As a result, both the hyperglycemic state and the chronic systemic inflammation put patients with diabetes at risk of developing several disabling and life-threatening complications, leading to an increased need for medical care, reduced quality of life, and premature death.1 During the lifetime of a patient with diabetes, the chances of developing DFUs are as high as 25%.9 DFUs are always colonized by microorganisms and more than 60% of ulcers end up with infections.21 Amputation is required for approximately 20% of patients with moderate to severe levels of DFUs. After undergoing a diabetes-related amputation, death still occurs in over 70% of patients within 5 years.2
ESKAPE pathogens are involved in nearly one-fifth of nosocomial infections and are associated with the highest mortality rates, resulting in increased healthcare burdens.22,23 With the increasing prevalence of antimicrobial resistance,24 the number of antimicrobial agents effective against ESKAPE pathogens are decreasing, and there is even no drug for some pan-drug resistant pathogens. Novel antibiotics are being developed at a rate that is far slower than the rate of resistance development, suggesting that early identification and diagnosis of ESKAPE infection are extremely important.
In this study, bacteria were the dominant microorganisms isolated from wound fluids of DFUs, with roughly similar number of gram-positive and gram-negative pathogens. Remarkably, S. aureus was the most common isolate in DFUs, accounting for approximately one third of all isolates and more than half of ESKAPE pathogens, which is consistent with other studies.25–27 As a commensal organism and an opportunistic pathogen, besides being the most common pathogen responsible for skin and soft tissue infections worldwide,28 S. aureus is the most frequently isolated pathogens from the bone tissue specimens from patients with diabetic foot osteomyelitis.14 P. aeruginosa represents the second most common organism isolated from chronic wound infections, accounting for 17.3% of ESKAPE pathogens in our study. Here, S. aureus showed high antimicrobial resistance, and although the resistance rate of P. aeruginosa is not as high as that of S. aureus, the wound that was infected with P. aeruginosa was usually associated with a significantly greater area and a longer healing process and resulted in a serious treatment-challenging ESKAPE infections.29
This study revealed that cigarette smoking and peripheral vascular disease were independent risk factors for ESKAPE infection. The associations between cigarette smoking and risks of all types of diabetes have been reported in multiple studies, and cigarette smoking was confirmed as a risk factor for amputation in DFUs.30,31 A possible reason is that cigarette smoking generates high levels of reactive oxygen species, which can induce cellular oxidative stress in blood vessels and nervous system, leading to inflammation, cellular damage, and apoptosis.30 Choi et al determined that cigarette smoking can increase the concentration of hydroquinone, which can significantly inhibit interferon-gamma (IFN-γ) secretion in a dose-dependent manner. In addition, Tollerud et al and Hogan et al reported that cigarette smoking is associated with a decrease in the number and proportion of circulating natural killer T (NKT) cells and invariant NKT cells, respectively.32,33 These findings seem to be consistent with the results of a previous study indicating that serum NKT% and IFN-γ were significantly decreased in patients with diabetic foot infection compared to patients with non-infected DFUs and diabetes only.34 Furthermore, cigarette smoking can systemically decrease immune responses, leading to ESKAPE infection.35 It has been shown that hyperglycemia affects the vasoconstriction response and platelet aggregation by inhibiting endothelial nitric oxide synthase activation and increasing reactive oxygen species, leading to atherothrombosis in the vessels and ultimately to peripheral vascular disease.36 Diabetic vascular disease is diagnosed in about 30% of patients with DFUs, and both macrovascular and microvascular diseases contributed to ischemia in the foot tissue and delayed wound healing, resulting in increased chance of acquiring ESKAPE infection in persistently exposed wounds. Importantly, cigarette smoking weakens vasodilation in skin microvasculature and further decreases the tissue oxygen tension and blood flow, placing patients at high risk for ESKAPE infection.37,38 Cigarette smoking has always been a major factor in the development of peripheral vascular disease caused by increased formation of atherosclerotic plaques. Therefore, the correlation between cigarette smoking and peripheral vascular disease increases the risk of infection and complicates treatment.
It has been shown that alcohol consumption is an important factor in the development of DFUs due to the impairment of the wound-healing process by the ethyl-toxic effect of alcohol and thus promotes wound infection.39 Moreover, although granulocytes are the front line of the innate immune defense against bacterial infection, chronic or acute alcohol consumption can impair granulocyte function and then hinder the immune response, leading to a significantly higher risk of MDR-pathogen infection.40 The Wagner system is the most widely used classification system for DFUs, which depends on the depth of ulceration and extent of gangrene.41 In our study, the results showed that the longer length of hospital stay, longer duration of systemic antibiotic treatment, and more invasive treatments were significantly associated with patients with severe DFUs (Wagner 3–5), which were consistent with the actual clinical situation. Although no independent risk factors for MDR-ESKAPE infection were identified in this study, it is still very important to monitor and control the spread of ESKAPE resistance.
This study has some limitations. First, the retrospective data may deviate from the accuracy of the diagnosis of diabetic foot and several complications studied. Second, we only included the complete baseline characteristics in the medical records, some of which were excluded due to incomplete records, such as body mass index and procalcitonin. These variables may also be risk factors for ESKAPE infection in DFUs. Finally, due to the small sample size, there may be a selection bias in the results.
Conclusion
DFUs and ESKAPE pathogens share a significant concern about the limited treatment strategy and increasing healthcare costs. In this study, the incidence of ESKAPE infection in patients with DFUs was nearly 50%. Given that cigarette smoking and alcohol consumption were associated with ESKAPE infection and MDR-pathogen infection, respectively, we encourage smoking cessation and abstention from alcohol as part of the therapeutic strategy for patients with DFUs. Moreover, clinicians should be vigilant in patients with DFUs accompanied with peripheral vascular disease, planning appropriate antimicrobial agents and rigorous wound care to avoid ESKAPE infection.
Ethics Statement
This study was approved by the Institutional Review Board of the affiliated Hospital of Southwest Medical University (KY2020043). Written informed consent was obtained from all participants, and was conducted according to the guidelines of the Declaration of Helsinki.
Funding
This work was supported by the grants from Sichuan Science and Technology Program (2022YFQ0093, 2020LZXNYD02) and Luxian Government and Southwest Medical University Cooperation Program (2020LXXNYKD-04).
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Jneid J, Lavigne JP, La Scola B, Cassir N. The diabetic foot microbiota: a review. Hum Microbiome J. 2017;5–6:1–6. doi:10.1016/j.humic.2017.09.002
3. Noor S, Zubair M, Ahmad J. Diabetic foot ulcer--A review on pathophysiology, classification and microbial etiology. Diabetes Metabol Syndrome. 2015;93:192–199. doi:10.1016/j.dsx.2015.04.007
4. Wang A, Lv G, Cheng X, et al. Guidelines on multidisciplinary approaches for the prevention and management of diabetic foot disease (2020 edition). Burns Trauma. 2020;8. doi:10.1093/burnst/tkaa017
5. Lipsky BA, Berendt AR, Cornia PB, et al. Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;2012(5412):e132–e73.
6. Pitocco D, Spanu T, Di Leo M, et al. Diabetic foot infections: a comprehensive overview. Eur Rev Med Pharmacol Sci. 2019;232:26–37.
7. Walsh JW, Hoffstad OJ, Sullivan MO, Margolis DJ. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabetic Med. 2016;3311:1493–1498. doi:10.1111/dme.13054
8. Nigi L, Fondelli C, de Donato G, Palasciano G, Setacci C, Dotta F. Fighting diabetic foot ulcers-The diabetologist: a king maker of the fight. Semin Vasc Surg. 2018;312–314:49–55. doi:10.1053/j.semvascsurg.2018.12.003
9. Lipsky BA, Berendt AR, Cornia PB, et al. Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;2012(5412):e132–e173.
10. Rice LB. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: no ESKAPE. J Infect Dis. 2008;1978:1079–1081. doi:10.1086/533452
11. Breen JD, Karchmer AW. Staphylococcus aureus infections in diabetic patients. Infect Dis Clin North Am. 1995;91:11–24. doi:10.1016/S0891-5520(20)30638-3
12. Macdonald KE, Boeckh S, Stacey HJ, Jones JD. The microbiology of diabetic foot infections: a meta-analysis. BMC Infect Dis. 2021;211:770. doi:10.1186/s12879-021-06516-7
13. Shanmugam P. The bacteriology of diabetic foot ulcers, with a special reference to multidrug resistant strains. J Clin Diagnostic Res. 2013;73:441–445.
14. Li X, Cheng Q, Du Z, Zhu S, Cheng C. Microbiological concordance in the management of diabetic foot ulcer infections with osteomyelitis, on the basis of cultures of different specimens at a diabetic foot center in China. Diabetes Metab Syndr Obes. 2021;14:1493–1503. doi:10.2147/DMSO.S296484
15. Lipsky BA, Berendt AR, Cornia PB, et al. Executive summary: 2012 Infectious Diseases Society of America Clinical Practice Guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):1679–1684. doi:10.1093/cid/cis460
16. Li Z, Xie J, Yang J, et al. Pathogenic characteristics and risk factors for ESKAPE pathogens infection in burn patients. Infect Drug Resist. 2021;14:4727–4738. doi:10.2147/IDR.S338627
17. Ouyang W, Jia Y, Jin L. Risk factors of diabetic foot ulcer in patients with type 2 diabetes: a retrospective cohort study. Am J Transl Res. 2021;138:9554–9561.
18. Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care. 2006;296:1288–1293. doi:10.2337/dc05-2425
19. Moura J, Madureira P, Leal EC, Fonseca AC, Carvalho E. Immune aging in diabetes and its implications in wound healing. Clin Immunol. 2019;200:43–54. doi:10.1016/j.clim.2019.02.002
20. Perera D, Kleinstein SE, Hanson B, et al. Impaired host response and the presence of Acinetobacter baumannii in the serum microbiome of type-II diabetic patients. iScience. 2021;241:101941. doi:10.1016/j.isci.2020.101941
21. Liu C, Ponsero AJ, Armstrong DG, Lipsky BA, Hurwitz BL. The dynamic wound microbiome. BMC Medicine. 2020;181:358. doi:10.1186/s12916-020-01820-6
22. Founou RC, Founou LL, Essack SY, Butaye P. Clinical and economic impact of antibiotic resistance in developing countries: a systematic review and meta-analysis. PLoS One. 2017;1212:e0189621. doi:10.1371/journal.pone.0189621
23. Pendleton JN, Gorman SP, Gilmore BF. Clinical relevance of the ESKAPE pathogens. Expert Rev Anti Infect Ther. 2013;113:297–308. doi:10.1586/eri.13.12
24. Mulani MS, Kamble EE, Kumkar SN, Tawre MS, Pardesi KR. Emerging strategies to combat ESKAPE pathogens in the era of antimicrobial resistance: a review. Front Microbiol. 2019;10:539. doi:10.3389/fmicb.2019.00539
25. Tascini C, Piaggesi A, Tagliaferri E, et al. Microbiology at first visit of moderate-to-severe diabetic foot infection with antimicrobial activity and a survey of quinolone monotherapy. Diabetes Res Clin Pract. 2011;941:133–139. doi:10.1016/j.diabres.2011.07.017
26. Jneid J, Cassir N, Schuldiner S, et al. Exploring the microbiota of diabetic foot infections with culturomics. Front Cellular Infect Microbiol. 2018;8:282. doi:10.3389/fcimb.2018.00282
27. Al Benwan K, Al Mulla A, Rotimi VO. A study of the microbiology of diabetic foot infections in a teaching hospital in Kuwait. J Infect Public Health. 2012;51:1–8. doi:10.1016/j.jiph.2011.07.004
28. Castleman MJ, Pokhrel S, Triplett KD, et al. Innate sex bias of staphylococcus aureus skin infection is driven by α-hemolysin. J Immunol. 1950;2018(2002):657–668.
29. Serra R, Grande R, Butrico L, et al. Chronic wound infections: the role of Pseudomonas aeruginosa and Staphylococcus aureus. Expert Rev Anti Infect Ther. 2015;135:605–613. doi:10.1586/14787210.2015.1023291
30. Xia N, Morteza A, Yang F, Cao H, Wang A. Review of the role of cigarette smoking in diabetic foot. J Diabetes Investig. 2019;102:202–215. doi:10.1111/jdi.12952
31. Sen P, Demirdal T, Emir B. Meta-analysis of risk factors for amputation in diabetic foot infections. Diabetes Metab Res Rev. 2019;357:e3165.
32. Tollerud DJ, Clark JW, Brown LM, et al. Association of cigarette smoking with decreased numbers of circulating natural killer cells. Am Rev Respir Dis. 1989;1391:194–198. doi:10.1164/ajrccm/139.1.194
33. Hogan AE, Corrigan MA, O’Reilly V, et al. Cigarette smoke alters the invariant natural killer T cell function and may inhibit anti-tumor responses. Clin immunol. 2011;1403:229–235. doi:10.1016/j.clim.2011.01.011
34. Hammad R, Elmadbouly AA, Ahmad IH, et al. T-natural killers and interferon gamma/interleukin 4 in augmentation of infection in foot ulcer in type 2 diabetes. Diabetes Metab Syndr Obes. 2021;14:1897–1908. doi:10.2147/DMSO.S305511
35. Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med. 2004;16420:2206–2216. doi:10.1001/archinte.164.20.2206
36. Saeed K, Esposito S, Akram A, et al. Hot topics in diabetic foot infection. Int J Antimicrobial Agents. 2020;556:105942. doi:10.1016/j.ijantimicag.2020.105942
37. Sørensen LT, Jørgensen S, Petersen LJ, et al. Acute effects of nicotine and smoking on blood flow, tissue oxygen, and aerobe metabolism of the skin and subcutis. J Surg Res. 2009;1522:224–230. doi:10.1016/j.jss.2008.02.066
38. Dryden M, Baguneid M, Eckmann C, et al. Pathophysiology and burden of infection in patients with diabetes mellitus and peripheral vascular disease: focus on skin and soft-tissue infections. Clin Microbiol Infect. 2015;21(Suppl 2):S27–S32. doi:10.1016/j.cmi.2015.03.024
39. Altenburg N, Joraschky P, Barthel A, et al. Alcohol consumption and other psycho-social conditions as important factors in the development of diabetic foot ulcers. Diabetic Med. 2011;282:168–174. doi:10.1111/j.1464-5491.2010.03151.x
40. Shi X, DeLucia AL, Bao J, Zhang P. Alcohol abuse and disorder of granulopoiesis. Pharmacol Ther. 2019;198:206–219. doi:10.1016/j.pharmthera.2019.03.001
41. Monteiro-Soares M, Russell D, Boyko EJ, et al. Guidelines on the classification of diabetic foot ulcers (IWGDF 2019). Diabetes Metab Res Rev. 2020;36(Suppl 1):e3273. doi:10.1002/dmrr.3273
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.