")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 9
Chronic radiation-induced dermatitis: challenges and solutions
Authors Spałek M
Received 16 September 2016
Accepted for publication 16 November 2016
Published 9 December 2016 Volume 2016:9 Pages 473—482
DOI https://doi.org/10.2147/CCID.S94320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Mateusz Spałek
Department of Radiotherapy I, The Maria Sklodowska-Curie Memorial Cancer Center and Institute of Oncology, Warsaw, Poland
Abstract: Chronic radiation dermatitis is a late side effect of skin irradiation, which may deteriorate patients’ quality of life. There is a lack of precise data about its incidence; however, several risk factors may predispose to the development of this condition. It includes radiotherapy dose, fractionation, technique, concurrent systemic therapy, comorbidities, and personal and genetic factors. Chronic radiation dermatitis is mostly caused by the imbalance of proinflammatory and profibrotic cytokines. Clinical manifestation includes changes in skin appearance, wounds, ulcerations, necrosis, fibrosis, and secondary cancers. The most severe complication of irradiation is extensive radiation-induced fibrosis (RIF). RIF can manifest in many ways, such as skin induration and retraction, lymphedema or restriction of joint motion. Diagnosis of chronic radiation dermatitis is usually made by clinical examination. In case of unclear clinical manifestation, a biopsy and histopathological examination are recommended to exclude secondary malignancy. The most effective prophylaxis of chronic radiation dermatitis is the use of proper radiation therapy techniques to avoid unnecessary irradiation of healthy skin. Treatment of chronic radiation dermatitis is demanding. The majority of the interventions are based only on clinical practice. Telangiectasia may be treated with pulse dye laser therapy. Chronic postirradiation wounds need special dressings. In case of necrosis or severe ulceration, surgical intervention may be considered. Management of RIF should be complex. Available methods are rehabilitative care, pharmacotherapy, hyperbaric oxygen therapy, and laser therapy. Future challenges include the assessment of late skin toxicity in modern irradiation techniques. Special attention should be paid on genomics and radiomics that allow scientists and clinicians to select patients who are at risk of the development of chronic radiation dermatitis. Novel treatment methods and clinical trials are strongly needed to provide more efficacious therapies.
Keywords: chronic radiation dermatitis, radiation-induced fibrosis, late skin toxicity, radiotherapy side effects
Introduction
The rapid development of radiation oncology in recent years caused significant improvement of cancer treatment effectiveness. Irradiation is associated with a variety of side effects, which depend on several factors, for example, site of treatment, radiation dose, and technique. One of the visible and common manifestations of radiation toxicity are acute and chronic skin reactions, commonly described as “radiation dermatitis”.1,2 Originally, dermatitis is defined as “inflammation of the skin”. However, in the literature data, the term “radiation dermatitis” covers a broader spectrum of symptoms and manifestations of postirradiation skin toxicity.3 Acute skin toxicity usually develops within 90 days after the beginning of irradiation, whereas chronic radiation dermatitis may develop many years after treatment. The skin after radiotherapy may look healthy, but the occurrence of chronic postirradiation reaction may develop suddenly and with various severity.2 Chronic radiation dermatitis is usually an irreversible and progressive condition, which may heavily deteriorate patients’ quality of life.4 This review presents a contemporary view on chronic radiation dermatitis and point out the challenges that ought to be taken up.
Incidence and risk factors
Incidence
There is no precise data on the incidence of chronic radiation dermatitis. In general, 95% patients who undergo radiotherapy develop some form of skin toxicity.1,5 There is no direct connection between experiencing an acute skin reaction and further development of chronic radiation dermatitis.3
Risk factors
Factors related to the higher incidence of chronic radiation dermatitis may be divided into two groups – directly dependent on irradiation and nondependent on irradiation. The factors increasing the risk of chronic radiation dermatitis dependent on radiotherapy include
altered fractionation (single fraction, hypofractionation, hyperfractionation, sometimes data on altered fractionation schemes are conflicting);8,9
radiotherapy technique without intensity modulation and large fields (two-dimensional [2D] radiotherapy, three-dimensional [3D]-conformal radiotherapy);10,11
kind of radiotherapy (postoperative radiotherapy);12
use of bolus, which increases dose received by skin.
There are also several factors not directly connected with radiotherapy modality, which include
Concurrent chemotherapy – some agents may significantly increase the risk of late skin complications, but a clear correlation has not been yet established. Results of randomized clinical trial comparing sequential vs concurrent chemotherapy in irradiated breast cancer patients show a significantly higher risk of radiation-induced fibrosis (RIF) in concurrent chemotherapy group.13
Concurrent targeted therapy – biological and/or targeted therapies are a novel approach in many malignancies. They are often combined with radiotherapy. Some recently published reports show that this combination may lead to increased treatment toxicity manifested as severe skin complications. Known examples are BRAF inhibitors and epidermal growth factor receptor inhibitors.14–16
Connective tissue disorders – there is a connection between a higher incidence of postirradiation skin toxicity and connective tissue disorders (such as systemic lupus erythematosus, scleroderma, and rheumatoid arthritis). The review of eight observational studies that included 404 patients with connective tissue diseases who were treated with radiotherapy showed that there was a statistically significant association with late radiation-induced complications in normal tissues (fibrosis, osteonecrosis, and bone fractures).17
Skin disorders – although radiation therapy was used by dermatologists in the treatment of some skin disorders, such as acne, psoriasis, or atopic eczema, these conditions increase the risk of chronic radiation dermatitis.2
Genetic factors – the response to radiation therapy may vary among patients, including both benefits and toxicity of treatment. Patients with DNA repair-deficiency disorders present symptoms of chronic radiation dermatitis.18 Moreover, some genes responsible for increased risk of RIF have been already identified.19
Personal factors – some of individual factors that may be both modifiable and nonmodifiable are connected with the higher risk of chronic radiation dermatitis. Female sex was identified as an independent predictor of severe late skin reaction.20 The reaction on radiation is related to the healing ability of skin, which decreases with age. It is caused by aging of cell lines, thickening of epidermis, loss of collagen, and reduction in the capillary network.21 Healing process of skin may be also disrupted by poor nutritional status, which affects ~50% of cancer patients.22 In smokers, several mechanisms, such as impaired oxygenation and elevated carboxyhemoglobin levels, disturb the postirradiation skin recovery and may exacerbate acute and chronic skin reactions.21 There is no clear connection between skin color and severity of skin reaction; however, it is thought that individuals with fair or pale skin suffer from more severe skin toxicity.21 Another considerable risk factors of chronic radiation dermatitis are obesity, chronic sun exposure, and ethnicity.2,5,23
Pathophysiology
Available data suggest that chronic radiation dermatitis is caused by imbalance of proinflammatory and profibrotic cytokines, which starts after irradiation and lasts for months or even many years. These include tumor necrosis factor-alpha (TNF-alpha), interleukins 6 and 1 (IL-6 and IL-1), tumor growth factor beta (TGF-beta), platelet-derived growth factor (PDGF), and connective tissue growth factor.24–28
TNF-alpha, IL-6, and IL-1 are responsible for persistent inflammation, whereas TGF-beta and PDGF promote fibrosis by activating fibroblasts and inducing synthesis of extracellular matrix proteins and matrix metalloproteinases.24–26,29,30
The concomitant radiation-induced endothelium damage results in improper vascularization of irradiated skin and restricts blood perfusion. It may exacerbate the fibrosis and deteriorate healing process.31 This phenomenon, together with secretion of PDGF, can also play a role in pathogenesis of telangiectasia.32
In addition, persistent inflammation and secretion of proinflammatory cytokines lead to leukocyte infiltration, which may cause other manifestations of chronic radiation dermatitis, such as skin atrophy or necrosis.33
Clinical manifestations
Chronic postirradiation skin reaction may develop years after treatment, and it is sometimes misdiagnosed as another skin condition not related to radiotherapy. Ionizing radiation can cause latent reaction on cellular level, which is clinically manifested as chronic radiation dermatitis. It includes changes in vascularity, pigmentation, fibrous tissue, number of cells, and others.
Skin appearance, wounds, and ulceration
Chronic radiation dermatitis may be clinically visible as a change of skin appearance. It includes skin hypo- and hyperpigmentation, skin atrophy, hyperkeratosis, loss of skin appendages, hair follicles, sebaceous, and sudoriferous glands.2 The common cosmetic defect after irradiation is telangiectasia – the dilation of small blood vessels.34 Damage caused by ionizing radiation to the blood vessels may lead to insufficient oxygenation of the skin cells and predispose to ulceration and/or chronic wounds.2 Moreover, this effect may be strengthened by skin atrophy and hyperkeratosis.35,36 Weakened and dehydrated skin is sensitive to injuries, and the addition of hypoxia can cause severe and nonhealing wound or even skin necrosis.2
RIF
RIF is commonly described as severe, progressive, and irreversible late complication of radiotherapy, but some literature data suggest that fibrotic changes may be reversible.37 RIF may lead to cosmetic and functional defects, which can deteriorate patients’ quality of life. It manifests in many ways, which includes induration and retraction of the skin, lymphedema, joint motion restriction, changes in skin appearance, wounds, and ulcerations.38 The fibrotic lesions are usually restricted only to the irradiated area. Adding a boost dose to particular area increases a risk of RIF.39
Secondary cancers
Ionizing radiation may lead to the development of many form of skin cancers, especially basal cell carcinoma and squamous cell carcinoma.40,41 Some studies suggest a connection between irradiation and melanoma.42 Radiotherapy also increases a risk of chronic radiation keratosis and precancerous keratotic skin lesion.43
Diagnosis and assessment
Diagnosis
Diagnosis is usually made by taking a medical history and clinical examination. It should include a detailed information about radiotherapy (irradiated fields, irradiated volume, technique, dose, and fractionation), chemotherapy, surgery or other oncological interventions, previous skin complications after radiotherapy, comorbidities (connective tissue disorders and genetic disorders), and taken medications. Examination of skin is based on palpation and inspection. During the first examination, it is important to describe precisely the affected area (size, depth, morphological aspects, and color) to assess the efficacy of treatment in the future. In some cases, especially when the clinical presentation is unclear or suspicious, a biopsy and histopathological examination are obligatory. It includes conditions that may mimic chronic radiation dermatitis, such as secondary cancers, angiosarcoma, or radiation-induced morphea.44 However, the biopsy or any other surgical intervention may deteriorate the course of RIF and cause prolonged wound healing.31
In some cases, the differential diagnosis between RIF and malignancy can be confirmed by magnetic resonance imaging (MRI).45,46 Differential diagnosis should include nephrogenic systemic fibrosis (NSF, also known as nephrogenic fibrosis dermopathy). It is a serious condition with unknown cause that involves extensive fibrosis of skin, joints, and internal organs. It is suggested that pathophysiology of NSF may be associated with gadolinium-based MRI contrast agents.47
Grading
In a routine clinical practice, two scales are used to assess the grade of chronic radiation dermatitis. They are summarized in Table 1. The toxicity criteria of the Radiation Therapy Oncology Group and the European Organization for Research and Treatment of Cancer assess two aspects of chronic radiation dermatitis – skin and subcutaneous tissue.48 More detailed assessment can be done through The Common Terminology Criteria for Adverse Events (CTCAE) version 4.03.
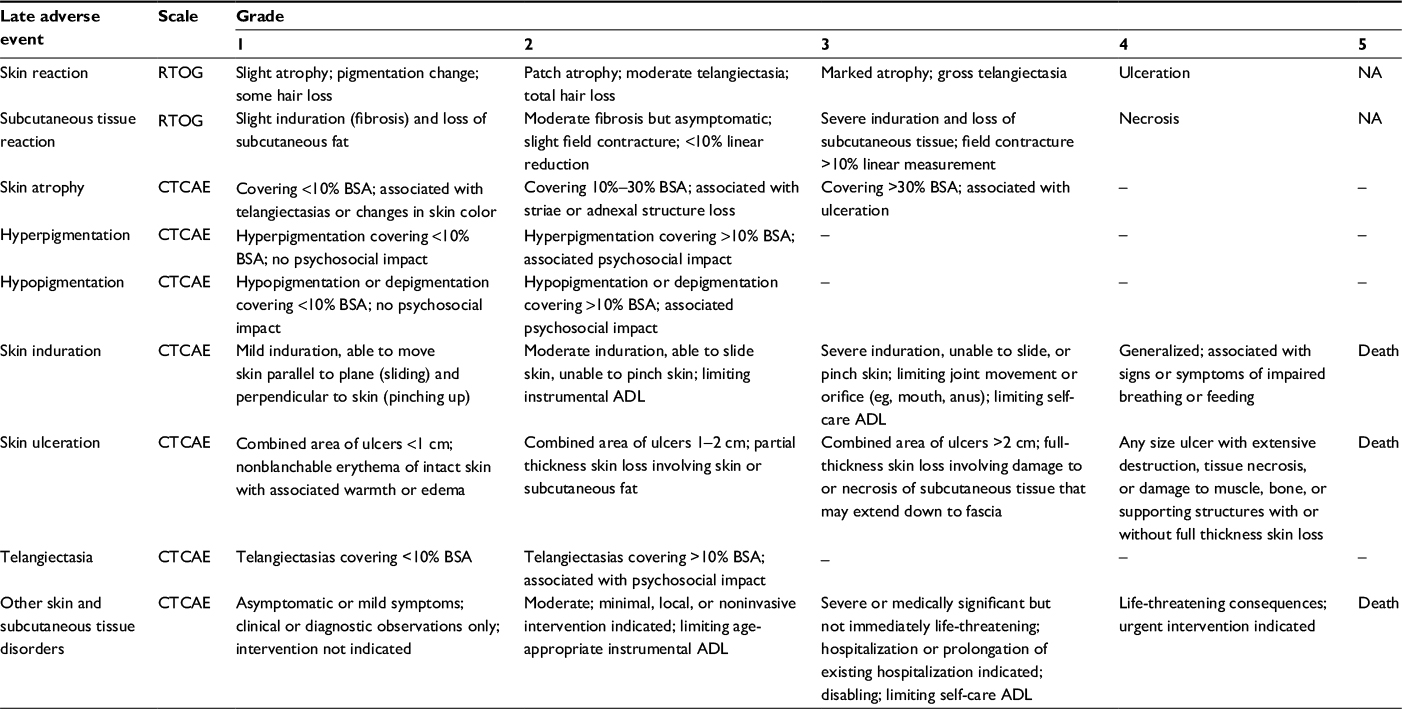 | Table 1 Assessment of chronic radiation dermatitis Abbreviations: ADL, activities of daily living; BSA, body surface area; CTCAE, Common Terminology Criteria for Adverse Event; NA, not applicable; RTOG, Radiation Therapy Oncology Group. |
It includes skin atrophy, skin hyper- and hypopigmentation, skin induration, skin ulceration, telangiectasia, and other skin and subcutaneous tissue disorders.
It is known that acute radiation dermatitis in patients who receive radiotherapy combined with biological agents (such as cetuximab) has a different pathophysiological ground and clinical manifestation in comparison to radiation dermatitis caused by radiation therapy alone or given concomitantly with conventional chemotherapy. It was suggested that existing grading tools need a strong revision and a new grading system was proposed.49,50 Currently, an international group of experts proposed a new classification that considers the CTCAE recommendations regarding the activities of daily living to assess acute bioradiation dermatitis.51 However, there is no such grading system designed to assess chronic radiation dermatitis caused by combined radiation and biological agents therapy – this topic needs a separate expert consensus.
Prevention
From the clinical perspective, the reduction in the incidence of chronic radiation dermatitis is expected especially for soft tissue sarcomas and breast or head and neck cancer patients due to the high dose received by skin and predictable long survival. The most important prevention method of chronic radiation dermatitis is the use of proper radiation therapy techniques to avoid unnecessary irradiation of healthy skin. It was shown that the application of intensity-modulated radiation therapy (IMRT) leads to the reduction of late radiation complications, for example, breast induration and telangiectasia.52,53 IMRT allowed to reduce acute wound healing complication rates in patients with lower extremity sarcomas.54 However, the results may vary depending on treatment site and localization of target volumes, thus preparing a few treatment plans in different techniques and comparing them is recommended. Another approach for skin sparing may be the avoidance of putting bolus when there is no necessity to ensure the full dose to targets near or at the skin. The trends in modern radiotherapy allow to use altered fractionation schedules, such as hypofractionation. It was shown that late skin reactions are related to the dose per fraction. Larger daily doses received by skin may increase the risk of chronic radiation dermatitis, so it is important to apply skin-sparing techniques of irradiation, but only when it is possible to obtain satisfactory dose coverage of target volumes.55 Further observations regarding late skin toxicity after new radiotherapy methods (particle therapy, stereotactic radiotherapy, and radiosurgery) are obligatory. To avoid severe skin toxicity, it is recommended to hold BRAF and MEK inhibitors 3 or more days before and after fractionated radiotherapy and 1 day or more before and after stereotactic radiosurgery (SRS).16
Literature data suggest that supplementation with antioxidants (eg, vitamin E, vitamin C, selenium, and melatonin) during radiotherapy may decrease radiation injury in healthy cells and enhance the immune response.56–58
Treatment
Available literature data on the management of chronic radiation dermatitis are unsatisfactory. Most of the interventions are based only on clinical practice and extrapolation of management used in similar conditions.
Telangiectasia
Telangiectasia is a form of chronic radiation dermatitis that may be psychologically distressing for a patient and cause physical disfiguration. The only method with limited evidence of efficacy is pulse dye laser therapy. In the retrospective study conducted at the Dermatology Division of Memorial Sloan-Kettering Cancer Center, 11 patients with telangiectasias received pulse dye laser therapy. The improvement was observed in all patients, including both physical appearance of the skin and general well-being.59 In another study, the efficacy of the pulse dye laser in the treatment of postirradiation telangiectasia of breast or chest wall was investigated.60 Eight patients were treated with this method, obtaining satisfactory clinical effect.
Ulceration and necrosis
Chronic ulceration and necrosis are significant manifestations of chronic radiation dermatitis. Due to the effects caused by ionizing radiation, vascularization of ulcerated areas of skin is commonly very poor and refractory to conservative treatment. Some chronic postirradiation wounds may be treated with special dressings. Infected wounds may be covered by dressings, which contains sliver, whereas wound with moderate or large exudation requires absorbent dressings.2 Severe ulcerations and/or necrosis require surgical management, which includes methods from simple removal to advanced reconstructions with skin flaps or artificial skin.61,62 The considerable, but not established in postirradiation ulcers, method of treatment is maggot debridement therapy. It involves the application of living disinfected fly larvae into the nonhealing skin and soft tissue wound. The aim is to clean the wound from necrotic tissue and help it to heal.63 In one case report, it was shown that low-intensity laser therapy for postirradiation chronic ulcer increases the number of dermal vessels, so this approach may be beneficial for patients with radiation ulcers and radiation necrosis.64 A case study described by Wollina et al presents another method of treatment of chronic radiation ulcers with recombinant PDGF and a hydrophilic copolymer membrane.65 Hypericum perforatum and neem oil may also be a considerable option in patients with severe chronic skin reaction; however, this combination of agents was tested only in the management of acute skin toxicity.66 Refractory or nonhealing ulcers are always to be treated as being suspected of secondary malignancy.
Fibrosis
The management of RIF is demanding. Available methods include rehabilitative care, pharmacotherapy, hyperbaric oxygen therapy, and laser therapy. Patients presenting RIF also require a supportive therapy (pain management, psychological support, wound care, and cosmetic interventions) to avoid the deterioration of quality of life.
Rehabilitative care
Early initiation of rehabilitative care is beneficial for patients who are thought to be at high risk of RIF or who are at the early stage of its development. Although, even in patients with advanced RIF, rehabilitation should be considered as a therapeutic option. Bourgeois et al conducted a randomized, prospective clinical trial regarding the LPG technique in treating RIF in a group of 20 breast cancer patients divided into two groups (LPG technique vs observation only).67 The LPG technique is described as a mechanical massage that allows skin mobilization by folding/unfolding. LPG treatment lead to decrease in erythema (10% vs 40% before treatment), pain and pruritus (10% vs 20% and 40% before treatment), and a feeling of induration of the skin (10% vs 70% before treatment). There is also a single case study describing the deep friction massage technique, which can reduce the symptoms of RIF, but this method needs to be proven in a larger group of patients.68 Active and passive physical therapy may be useful in reducing contractors and improving movability.
Pharmacotherapy
There is a lack of strong evidences for the use of pharmacological methods in the management of RIF, although several substances are used to treat this condition.
A few publications describe the beneficial effect of pentoxifylline, a methylated xanthine derivative. It works as a competitive nonselective phosphodiesterase inhibitor, which increases concentration of intracellular cyclic adenosine monophosphate, activates protein kinase A, inhibits TNF and leukotriene synthesis, decreases granulocyte–macrophage colony-stimulating factor and interferon gamma, and suppress the TGF expression.38,69–73 The suppression of TGF-beta may influence fibroblasts and reduce or even reverse fibrosis. It is sometimes used in combination with tocopherol (vitamin E). Results of small randomized clinical trials provided mixed data on the efficacy of aforementioned drugs combination.38,74–76 In some of them, the effect of pentoxifylline ± tocopherol on RIF was not higher than placebo.75,76 However, a study conducted by Delanian et al show a clear reduction of superficial fibrosis in a group of 44 women who received pentoxifylline (800 mg/day) plus tocopherol (1000 units/day) for 6–48 months.77 A total of 37 patients were receiving therapy for 24–48 months, 7 patients discontinued treatment after 6–12 months. It was found that pentoxifylline and tocopherol need a prolonged amount of time (average 24 months) to obtain clinically significant effect manifested as reduction of RIF (68% of mean estimated maximal regression in surface area of RIF). Larger randomized clinical trials are required to confirm the efficacy of these drug combinations and to set the optimal dose and duration of therapy.
Other pharmacological interventions that were tested on limited group of patients are superoxide dismutase. Liposomal-encapsulated superoxide dismutase is an antioxidant enzyme that catalyzes the dismutation of superoxide radical into hydrogen peroxide and oxygen. It also works as a suppressor of TGF-beta in myofibroblasts, thus it may be effective in conditions with fibroblasts hyperactivity.26
In 1994, Delanian et al performed a clinical trial on a group of 34 patients with RIF.78 Participants received liposomal-encapsulated superoxide dismutase >3 weeks in twice weekly intramuscular injections of 5 mg for a total of 30 mg. Some clinical regression of fibrosis in all patients was found.
Hyperbaric oxygen
Some clinical data suggest that hyperbaric oxygen may have a positive impact on the reduction of late radiation toxicity; however, its efficacy in reducing the incidence of RIF has not yet been proven. Clinical research confirmed the benefits of hyperbaric oxygen in the management of lymphedema caused by conservative breast therapy.79,80
Laser therapy
Clinical experience and data from other conditions suggest that laser therapy can stop the excessive fibrosis and induce normal scar remodeling in patients with RIF. In the ongoing clinical trial NCT01910818 (pilot study of the effect of laser on reversing chronic radiation injury), research team proposed the use of fractional laser treatment to treat fibrosis associated with hypertrophic scars and morphea.81 The final data collection date for the primary outcome measure is planned by the end of August 2017. Combination of laser therapy with epidermal grafting was also shown as an effective treatment method. Vietnamese researchers used laser therapy with epidermal skin grafting in three children with chronic radiation dermatitis after radiotherapy for infantile hemangioma. The obtained clinical result was satisfactory – skin repigmentation, softening, and increased flexibility were observed.82
Surgical intervention
In extremely rare clinical situations (severe deterioration of quality of life, very limited movability, and pain that cannot be managed by other methods), a surgical intervention may be considered, but it can also potentially exacerbate fibrosis, thus the assessment of benefits vs risks ratio is mandatory.31 The exceptional situation is the suspicion of tumor recurrence or second cancer formation where surgical approach is preferable over conservative methods or observation. One publication describes a study performed on a small group of patients with severe RIF after breast conserving therapy for breast cancer.83 In these patients, surgeons performed partial mastectomy and latissimus dorsi muscle reconstruction obtaining a satisfactory reduction of symptoms.
Further challenges
The rapid development of radiotherapy in the last 20 years allowed to introduce innovative techniques, such as IMRT. It provides a better dose homogeneity and allows to avoid hot spots on skin. However, application of IMRT may increase the volumes of tissues, which receive small doses, so comparison of treatment plans prepared in different techniques is recommended. Increasingly popular modern radiotherapy techniques based on prescribing a large dose of radiation to a small volume in one or a few fractions, such as stereotactic body radiotherapy (SBRT) and SRS, may cause another clinical manifestation of chronic radiation dermatitis, thus it is highly recommended to follow SBRT/SRS guidelines during treatment planning. Also there are no data concerning late skin toxicity of the new particles (protons, heavy ions), which become more available and used in clinical practice. Nonetheless, this may be relevant only in case of superficially located target volumes that are close to the skin. Another promising technology is 3D printing of customized boluses. Conventional boluses have often fixed size. That increases an area of covered skin and may lead to higher skin toxicity. In addition, a process of bolus application may be inaccurate. Three-dimensional calculated and printed bolus may allow to deliver a dose to target tissues with avoidance of healthy skin.84 Moreover, a rapid development of targeted therapy and immunotherapy with concomitant radiotherapy opens a new field for potential side effects related to skin. Increasing knowledge about genomics and radiomics will allow scientists and clinicians to select patients who are at risk of the development of chronic radiation dermatitis, so a prophylaxis and special caution may be implemented before and after irradiation. Novel agents and treatment modalities, such as antioxidants or inflammation suppressors, are under investigation. These include superoxide dismutase and catalase mimetics, curcumin, and quercetin.85–87
Conclusion
Chronic radiation dermatitis can develop years after radiotherapy. Its manifestations, such as RIF, may cause disfiguring cosmetics effect, reduce mobility, and severely impair patients’ quality of life. It is dependent on the dose, irradiated volume, and other factors, such as comorbidities and individual predispositions. The choice of proper radiotherapy technique, dose, and fractionation may reduce a risk of radiation-induced dermatitis. However, it should not be prioritized over the main aim of irradiation – proper dose coverage of target volumes and achieving the highest probability of tumor control. There are several treatment modalities that can be approached to reduce symptoms of chronic radiation dermatitis, but they are not based on strong scientific evidence, thus their value is limited. A novel treatment methods and clinical trials are strongly needed to provide more efficacious therapies for this radiotherapy complication.
Disclosure
The author reports no conflicts of interest in this work.
References
Hickok JT, Morrow GR, Roscoe JA, Mustian K, Okunieff P. Occurrence, severity, and longitudinal course of twelve common symptoms in 1129 consecutive patients during radiotherapy for cancer. J Pain Symptom Manage. 2005;30(5):433–442. | ||
Hymes SR, Strom EA, Fife C. Radiation dermatitis: clinical presentation, pathophysiology, and treatment 2006. J Am Acad Dermatol. 2006;54(1):28–46. | ||
Bray FN, Simmons BJ, Wolfson AH, Nouri K. Acute and chronic cutaneous reactions to ionizing radiation therapy. Dermatol Ther (Heidelb). 2016;6(2):185–206. | ||
Wolff K, Johnson R, Saavedra A. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 7th ed. New York, NY: McGraw Hill; 2013. | ||
Ryan JL. Ionizing radiation: the good, the bad, and the ugly. J Invest Dermatol. 2012;132(3 Pt 2):985. | ||
Geara FB, Komaki R, Tucker SL, Travis EL. Factors influencing the development of lung fibrosis after chemoradiation for small cell carcinoma of the lung: evidence for inherent interindividual variation. J Radiat Oncol Biol Phys. 1998;41(2):279. | ||
Collette S, Collette L, Budiharto T, et al. Predictors of the risk of fibrosis at 10 years after breast conserving therapy for early breast cancer – a study based on the EORTC trial 22881–10882 “boost versus no boost.” Eur J Cancer. 2008;44(17):2587–2599. | ||
Cuttino LW, Heffernan J, Vera R, Rosu M, Ramakrishnan VR, Arthur DW. Association between maximal skin dose and breast brachytherapy outcome: a proposal for more rigorous dosimetric constraints. Int J Radiat Oncol Biol Phys. 2011;81(3):e173–e177. | ||
Saunders M, Dische S, Barrett A, Harvey A, Griffiths G, Parmar M. Continuous, hyperfractionated, accelerated radiotherapy (CHART) versus conventional radiotherapy in non-small cell lung cancer: mature data from the randomised multicentre trial. Radiother Oncol. 1999;52(2):137–148. | ||
Donovan E, Bleakley N, Denholm E, et al. Randomised trial of standard 2D radiotherapy (RT) versus intensity modulated radiotherapy (IMRT) in patients prescribed breast radiotherapy. Radiother Oncol. 2007;82(3):254–264. | ||
Barnett GC, Wilkinson JS, Moody AM, et al. Randomized controlled trial of forward-planned intensity modulated radiotherapy for early breast cancer: interim results at 2 years. Int J Radiat Oncol Biol Phys. 2012;82(2):715–723. | ||
Davis AM, O’Sullivan B, Turcotte R, Bell R. Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol. 2005;75(1):48–53. | ||
Toledano A, Garaud P, Serin D, et al. Concurrent administration of adjuvant chemotherapy and radiotherapy after breast-conserving surgery enhances late toxicities: long-term results of the ARCOSEIN multicenter randomized study. Int J Radiat Oncol Biol Phys. 2006;65(2):324–332. | ||
Satzger I, Degen A, Asper H, Kapp A, Hauschild A, Gutzmer R. Serious skin toxicity with the combination of BRAF inhibitors and radiotherapy. J Clin Oncol. 2013;31(13):e220–e222. | ||
Tejwani A, Wu S, Jia Y, Agulnik M, Millender L, Lacouture ME. Increased risk of high-grade dermatologic toxicities with radiation plus epidermal growth factor receptor inhibitor therapy. Cancer. 2009;115(6):1286–1299. | ||
Anker CJ, Grossmann KF, Atkins MB, Suneja G, Tarhini AA, Kirkwood JM. Avoiding severe toxicity from combined BRAF inhibitor and radiation treatment: consensus guidelines from the Eastern Cooperative Oncology Group (ECOG). Int J Radiat Oncol Biol Phys. 2016;95(2):632–646. | ||
Hölscher T, Bentzen SM, Baumann M. Influence of connective tissue diseases on the expression of radiation side effects: a systematic review. Radiother Oncol. 2006;78(2):123–130. | ||
West CM, Barnett GC. Genetics and genomics of radiotherapy toxicity: towards prediction. Genome Med. 2011;3(8):52. | ||
Andreassen CN, Overgaard J, Alsner J, et al. ATM sequence variants and risk of radiation-induced subcutaneous fibrosis after postmastectomy radiotherapy. Int J Radiat Oncol Biol Phys. 2006;64(3):776–783. | ||
Meyer F, Fortin A, Wang CS, Liu G, Bairati I. Predictors of severe acute and late toxicities in patients with localized head-and-neck cancer treated with radiation therapy. Int J Radiat Oncol Biol Phys. 2012;82(4):1454–1462. | ||
Porock D. Factors influencing the severity of radiation skin and oral mucosal reactions: development of a conceptual framework. Eur J Cancer Care (Engl). 2002;11(1):33–43. | ||
Bruera E, MacDonald RN. Nutrition in cancer patients: an update and review of our experience. Issues in symptom control. Part 3. J Pain Symptom Manage. 1988;3(3):133–140. | ||
Morgan K. Radiotherapy-induced skin reactions: prevention and cure. Br J Nurs. 2014;23(16):S24–S26–32. | ||
Haase O, Rodemann HP. Fibrosis and cytokine mechanisms: relevant in hadron therapy? Radiother Oncol. 2004;73:S144–S147. | ||
Bentzen SM. Preventing or reducing late side effects of radiation therapy: radiobiology meets molecular pathology. Nat Rev Cancer. 2006;6(9):702–713. | ||
Martin M, Lefaix J, Delanian S. TGF-beta1 and radiation fibrosis: a master switch and a specific therapeutic target? Int J Radiat Oncol Biol Phys. 2000;47(2):277–290. | ||
Vozenin-Brotons MC, Milliat F, Sabourin JC, et al. Fibrogenic signals in patients with radiation enteritis are associated with increased connective tissue growth factor expression. J Radiat Oncol Biol Phys. 2003;56(2):561–572. | ||
Yarnold J, Brotons MC. Pathogenetic mechanisms in radiation fibrosis. Radiother Oncol. 2010;97(1):149–161. | ||
Pohlers D, Brenmoehl J, Löffler I, et al. TGF-beta and fibrosis in different organs – molecular pathway imprints. Biochim Biophys Acta. 2009;1792(8):746–756. | ||
Abdollahi A, Li M, Ping G, et al. Inhibition of platelet-derived growth factor signaling attenuates pulmonary fibrosis. J Exp Med. 2005;201(6):925–935. | ||
Hermann T, Baumann M, Dörr W. Klinische Strahlenbiologie. Stuttgart, German: Urban & Fischer Verlag; 2006. German. | ||
Denham JW, Hauer-Jensen M. The radiotherapeutic injury – a complex “wound.” Radiother Oncol. 2002;63(2):129–145. | ||
Quarmby S, Kumar P, Kumar S. Radiation-induced normal tissue injury: role of adhesion molecules in leukocyte–endothelial cell interactions. Int J Cancer. 1999;82(3):385–395. | ||
Bentzen SM, Overgaard J. Patient-to-patient variability in the expression of radiation-induced normal tissue injury. Semin Radiat Oncol. 1994;4(2):68–80. | ||
Mendelsohn FA, Divino CM, Reis ED, Kerstein MD. Wound care after radiation therapy. Adv Skin Wound Care. 2002;15(5):216. | ||
Harper JL, Franklin LE, Jenrette JM, Aguero EG. Skin toxicity during breast irradiation: pathophysiology and management. South Med J. 2004;97(10):989–994. | ||
Anscher MS. The irreversibility of radiation-induced fibrosis: fact or folklore? J Clin Oncol. 2005;23(34):8551–8552. | ||
Delanian S, Porcher R, Balla-Mekias S, Lefaix JL. Randomized, placebo-controlled trial of combined pentoxifylline and tocopherol for regression of superficial radiation-induced fibrosis. J Clin Oncol. 2003;21(13):2545–2550. | ||
Bartelink H, Maingon P, Poortmans P, et al. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lancet Oncol. 2015;16(1):47–56. | ||
Suárez B, López-Abente G, Martínez C, et al. Occupation and skin cancer: the results of the HELIOS-I multicenter case-control study. BMC Public Health. 2007;7(1):180. | ||
James WD, Berger TG, Elston DM. Andrews’ Diseases of the Skin: Clinical Dermatology. Philadelphia, PA: Saunders Elsevier; 2006. | ||
Fink CA, Bates MN. Melanoma and ionizing radiation: is there a causal relationship? Radiat Res. 2009;164(5):701–710. | ||
Freedberg MD, Eisen AZ, Wolff K, et al, editors. Fitzpatrick’s Dermatology in General Medicine. 6th ed. New York, NY: McGraw-Hill; 2003. | ||
Spalek M, Jonska Gmyrek J, Gałecki J. Radiation-induced morphea – a literature review. J Eur Acad Dermatol Venereol. 2015;29(2):197–202. | ||
Hoeller U, Bonacker M, Bajrovic A, Alberti W, Adam G. Radiation-induced plexopathy and fibrosis. Strahlenther Onkol. 2004;180(10):650–654. | ||
Semiz Oysu A, Ayanoglu E, Kodalli N, Oysu C, Uneri C, Erzen C. Dynamic contrast-enhanced MRI in the differentiation of posttreatment fibrosis from recurrent carcinoma of the head and neck. Clin Imaging. 2005;29(5):307–312. | ||
Thomsen HS. Nephrogenic systemic fibrosis: history and epidemiology. Radiol Clin North Am. 2009;47(5):827–31–vi. | ||
Cox JD, Stetz JA, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys. 1995;30;31(5):1341–1346. | ||
Bernier J, Russi EG, Homey B, Merlano MC, Mesía R, Peyrade F, Budach W. Management of radiation dermatitis in patients receiving cetuximab and radiotherapy for locally advanced squamous cell carcinoma of the head and neck: proposals for a revised grading system and consensus management guidelines. Ann Oncol. 2011;22(10):2191–2200. | ||
Cante D, La Porta MR, Franco P, et al. Management of “in-field” skin toxicity in head and neck cancer patients treated with combined cetuximab and radiotherapy. Oncology. 2013;85(5):257–261. | ||
Russi EG, Moretto F, Rampino M, et al. Acute skin toxicity management in head and neck cancer patients treated with radiotherapy and chemotherapy or EGFR inhibitors: literature review and consensus. Crit Rev Oncol Hematol. 2015;96(1):167–182. | ||
Keller LMM, Sopka DM, Li T, et al. Five-year results of whole breast intensity modulated radiation therapy for the treatment of early stage breast cancer: the fox chase cancer center experience. Int J Radiat Oncol Biol Phys. 2012;84(4):881–887. | ||
Mukesh MB, Qian W, Wilkinson JS, et al. Patient reported outcome measures (PROMs) following forward planned field-in field IMRT: results from the Cambridge Breast IMRT trial. Radiother Oncol. 2014;111(2):270–275. | ||
Tiong SS, Dickie C, Haas RL, O’Sullivan B. The role of radiotherapy in the management of localized soft tissue sarcomas. Cancer Biol Med. 2016;13(3):373–383. | ||
Astrahan M. Some implications of linear-quadratic-linear radiation dose-response with regard to hypofractionation. Med Phys. 2008;35(9):4161–4172. | ||
Kiremidjian-Schumacher L, Roy M. Effect of selenium on the immunocompetence of patients with head and neck cancer and on adoptive immunotherapy of early and established lesions. Biofactors. 2001;14(1–4):161–168. | ||
Malmberg K-J, Lenkei R, Petersson M, et al. A short-term dietary supplementation of high doses of vitamin E increases T helper 1 cytokine production in patients with advanced colorectal cancer. Clin Cancer Res. 2002;8(6):1772–1778. | ||
Prasad KN, Cole WC, Kumar B, Che Prasad K. Pros and cons of antioxidant use during radiation therapy. Cancer Treat Rev. 2002;28(2):79–91. | ||
Rossi AM, Nehal KS, Lee EH. Radiation-induced breast telangiectasias treated with the pulsed dye laser. J Clin Aesthet Dermatol. 2014;7(12):34–37. | ||
Lanigan SW, Joannides T. Pulsed dye laser treatment of telangiectasia after radiotherapy for carcinoma of the breast. Br J Dermatol. 2003;148(1):77–79. | ||
Veness M, Richards S. Radiotherapy. In: Bolognia J, Jorizzo J, Schaffer J, editors. Dermatology. New York, NY: Elsevier; 2012. | ||
Smith A, Fife CE. Advanced therapeutics: the biochemistry and biophysical basis of wound products. In: Sheffield PJ, editor. Wound Care Practice. Flagstaff, AR: Best Publishing; 2004. | ||
Sun X, Jiang K, Chen J, Wu L, Lu H, Wang A, Wang J. A systematic review of maggot debridement therapy for chronically infected wounds and ulcers. Int J Infect Dis. 2014;25:32–37. | ||
Schindl A, Schindl M, Schindl L, Jurecka W, Hönigsmann H, Breier F. Increased dermal angiogenesis after low-intensity laser therapy for a chronic radiation ulcer determined by a video measuring system. J Am Acad Dermatol. 1999;40(3):481–484. | ||
Wollina U, Liebold K, Konrad H. Treatment of chronic radiation ulcers with recombinant platelet-derived growth factor and a hydrophilic copolymer membrane. J Eur Acad Dermatol Venereol. 2001;15(5):455–457. | ||
Franco P, Potenza I, Moretto F, et al. Hypericum perforatum and neem oil for the management of acute skin toxicity in head and neck cancer patients undergoing radiation or chemo-radiation: a single-arm prospective observational study. Radiat Oncol. 2014;9(1):297. | ||
Bourgeois JF, Gourgou S, Kramar A, Lagarde JM, Guillot B. A randomized, prospective study using the LPG technique in treating radiation-induced skin fibrosis: clinical and profilometric analysis. Skin Res Technol. 2008;14(1):71–76. | ||
Warpenburg MJ. Deep friction massage in treatment of radiation-induced fibrosis: rehabilitative care for breast cancer survivors. Integr Med (Encinitas). 2014;13(5):32–36. | ||
Essayan DM. Cyclic nucleotide phosphodiesterases. J Allergy Clin Immunol. 2001;108(5):671–680. | ||
Deree J, Martins JO, Melbostad H, Loomis WH, Coimbra R. Insights into the regulation of TNF-alpha production in human mononuclear cells: the effects of non-specific phosphodiesterase inhibition. Clinics (Sao Paulo). 2008;63(3):321–328. | ||
Marques LJ, Zheng L, Poulakis N, Guzman J, Costabel U. Pentoxifylline inhibits TNF-alpha production from human alveolar macrophages. Am J Respir Crit Care Med. 1999;159(2):508–511. | ||
Peters-Golden M, Canetti C, Mancuso P, Coffey MJ. Leukotrienes: underappreciated mediators of innate immune responses. J Immunol. 2005;174(2):589–594. | ||
Samlaska CP, Winfield EA. Pentoxifylline. J Am Acad Dermatol. 1994;30(4):603–621. | ||
Jacobson G, Bhatia S, Smith BJ, Button AM, Bodeker K, Buatti J. Randomized trial of pentoxifylline and vitamin E vs standard follow-up after breast irradiation to prevent breast fibrosis, evaluated by tissue compliance meter. Int J Radiat Oncol Biol Phys. 2013;85(3):604–608. | ||
Magnusson M, Höglund P, Johansson K, et al. Pentoxifylline and vitamin E treatment for prevention of radiation-induced side-effects in women with breast cancer: a phase two, double-blind, placebo-controlled randomised clinical trial (Ptx-5). Eur J Cancer. 2009;45(14):2488–2495. | ||
Gothard L, Cornes P, Earl J, et al. Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer. Radiother Oncol. 2004;73(2):133–139. | ||
Delanian S, Porcher R, Rudant J, Lefaix JL. Kinetics of response to long-term treatment combining pentoxifylline and tocopherol in patients with superficial radiation-induced fibrosis. J Clin Oncol. 2005;23(34):8570–8579. | ||
Delanian S, Baillet F, Huart J, Lefaix JL, Maulard C, Housset M. Successful treatment of radiation-induced fibrosis using liposomal CuZn superoxide dismutase: clinical trial. Radiother Oncol. 1994;32(1):12–20. | ||
Gothard L, Stanton A, MacLaren J, et al. Non-randomised phase II trial of hyperbaric oxygen therapy in patients with chronic arm lymphoedema and tissue fibrosis after radiotherapy for early breast cancer. Radiother Oncol. 2004;70(3):217–224. | ||
Teas J, Cunningham JE, Cone L, et al. Can hyperbaric oxygen therapy reduce breast cancer treatment-related lymphedema? A pilot study. J Womens Health (Larchmt). 2004;13(9):1008–1018. | ||
Massachusetts General Hospital. Pilot study of the effect of laser on reversing chronic radiation injury. Available from: https://clinicaltrials.gov/ct2/show/NCT01910818. NLM identifier: NCT01910818. Accessed August 1, 2016. | ||
Tran TN, Hoang MV, Phan QA, et al. Fractional epidermal grafting in combination with laser therapy as a novel approach in treating radiation dermatitis. Semin Cutan Med Surg. 2015;34(1):42–47. | ||
van Geel AN, Lans TE, Haen R, Tjong Joe Wai R, Menke-Pluijmers MB. Partial mastectomy and m. latissimus dorsi reconstruction for radiation-induced fibrosis after breast-conserving cancer therapy. World J Surg. 2011;35(3):568–572. | ||
Kim SW, Shin HJ, Kay CS, Son SH. A customized bolus produced using a 3-dimensional printer for radiotherapy. PLoS One. 2014;9(10):e110746. | ||
A Rosenthal R, Fish B, P Hill R, et al. Salen Mn complexes mitigate radiation injury in normal tissues. Anticancer Agents Med Chem. 2011;11(4):359–372. | ||
Okunieff P, Xu J, Hu D, et al. Curcumin protects against radiation-induced acute and chronic cutaneous toxicity in mice and decreases mRNA expression of inflammatory and fibrogenic cytokines. Int J Radiat Oncol Biol Phys. 2006;65(3):890–898. | ||
Horton JA, Li F, Chung EJ, et al. Quercetin inhibits radiation-induced skin fibrosis. Radiat Res. 2013;180(2):205–215. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.