")
Back to Journals » Infection and Drug Resistance » Volume 13
Chronic Perioral Tuberculosis Skin Lesions in a 21-Year-Old Male
Authors Gharabaghi N, Sedokani A
Received 15 July 2020
Accepted for publication 4 September 2020
Published 25 September 2020 Volume 2020:13 Pages 3273—3276
DOI https://doi.org/10.2147/IDR.S260796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Naser Gharabaghi,1 Amin Sedokani2
1Department of Infectious Disease, Taleghani Hospital, Urmia University of Medical Sciences, Urmia, Iran; 2Department of Cardiology, School of Medicine, Seyedoshohada Hospital, Urmia University of Medical Sciences, Urmia, Iran
Correspondence: Amin Sedokani
Department of Cardiology, School of Medicine, Seyedoshohada Hospital, Urmia University of Medical Sciences, 17 Sharivar Street, Urmia 571478334, Iran
Tel +98 443 237 5907
Fax +98 443 237 2917
Email [email protected]
Abstract: Cutaneous tuberculosis is a rare form of tuberculosis infection that may lead to chronic lesions of skin and be missed in diagnosis due to location of the appearance of the lesions. This is a very rare case of peri-oral cutaneous tuberculosis in a 21-year-old man with no other specific sign of symptoms of tuberculosis infection but mimics signs of Herpesviridae family infection. The biopsy of the lesions and Ziehl–Neelsen stain revealed the diagnosis of cutaneous tuberculosis. By the beginning of the treatment of this unusual form of tuberculosis, the lesions had begun to fade and after 8 months, they were totally faded.
Keywords: Mycobacterium tuberculosis, cutaneous tuberculosis, orolabial lesions
Introduction
Mycobacterium tuberculosis is an acid-fast bacillus, responsible for the tuberculosis disease in human. The high prevalence worldwide and the mortality/morbidity of the disease, have made tuberculosis one of the top health-threatening diseases and one of the top 10 causes of deaths worldwide.1,2 Cutaneous TB (CTB) is a rare manifestation of TB, presenting only in 1–2% of all cases.3–5 However, the importance of CTB is not only the disease itself, but it is the misdiagnosis and progression of the disease in addition to risk of spread of the disease in the society and misdiagnosed as orolabial Herpes Simplex infections (HSV-1 and HSV-2). The differential diagnosis of exudative and ulcerative lesions, includes both HSV and CTB infection. However, the period of signs and symptoms and reactivation of disease differ from the above infections.6–9 This is a rare case of perioral cutaneous tuberculosis in a 21-year-old male that mimics closely the signs of Herpesviridae family infection.
Case Presentation
The patient was a 21-year-old male plaster worker, living in one of the North-Western provinces of Iran, who presented with skin lesions on his face and upper lip that had appeared about 3 months previously. Skin lesions were prurient and some of them were prominent and hemorrhagic. The patient reported no other symptoms, such as fever, chills, fatigue, urinary and/or respiratory symptoms. Familial, allergy and drug history were negative. On physical examination vital signs were normal. On facial skin examination; lesions appeared as multiple separate hyperkeratotic nodular lesions with erythematic and prominent borders on the face and upper lip with normally appearing skin around the lesions (Figure 1). The skin demonstrated no other significant changes, and the patient had no notable local lymphadenopathy. Other examinations demonstrated no significant findings. The patient had visited multiple physicians/clinics and had been treated with multiple topical therapies, oral antibiotics, and antihistamines but the medications had no affect on the lesions. Topical corticosteroids subsided inflammation and swelling of the skin lesions. Finally, a skin biopsy, a chest x-ray and blood tests were performed. The patient’s blood tests were normal but skin biopsy revealed skin tissue with multiple granuloma formation in a subepithelial area composed of epithelioid cells, with giant cell and lymphocyte around them (Figure 2).
 |
Figure 1 Multiple separated hyperkeratotic nodular lesions with erythematic and prominent borders on the patient’s face. |
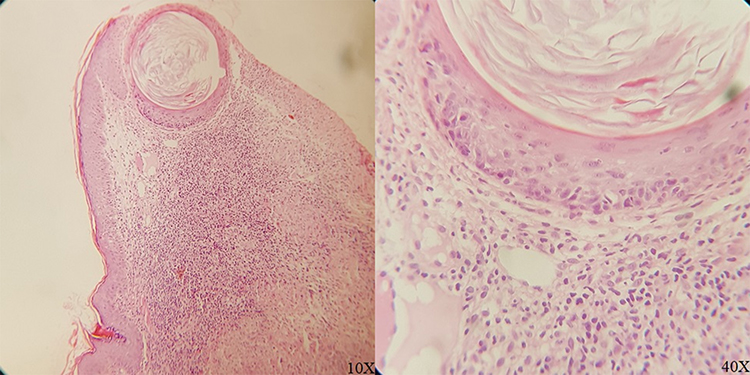 |
Figure 2 Histopathological assessment of lesions revealing skin tissue with multiple granuloma formation in the subepithelial area composed of epithelioid cells, Langhans giant cell, and lymphocyte around them (Magnifications: 10× and 40×). |
Acid-fast stain of Ziehl–Neelsen (Figure 3) and a purified protein derivative (PPD) skin test due to epidemiology of the tuberculosis helped in the final diagnosis of cutaneous tuberculosis (CTB), caused by acid-fast positive bacteria Mycobacterium tuberculosis infection. Due to the high prevalence of TB infection in North-Western Iran,10 no response to medications but topical corticosteroids, and normal blood tests we suspected the cutaneous manifestation of TB in spite of its rarity. Also, a 2-time rapid ELISA test for HIV infection was negative. The Ziehl–Neelsen stained histopathological assessment and positive PPD test confirmed the tuberculosis diagnosis. The patient underwent standard anti-TB regimens involving 2 months of quadruple therapy of isoniazid, rifampin, pyrazinamide, and ethambutol followed by a further 4 months of isoniazid plus rifampin. Continued treatment resulted in lesions clearance at the end of the course of treatment and even the scars had begun to regress. At the end of the 8th month (2 months after ending the medical therapy), the patient had no cutaneous and systemic signs or symptoms and the course of treatment ended without any complications (Figure 3).
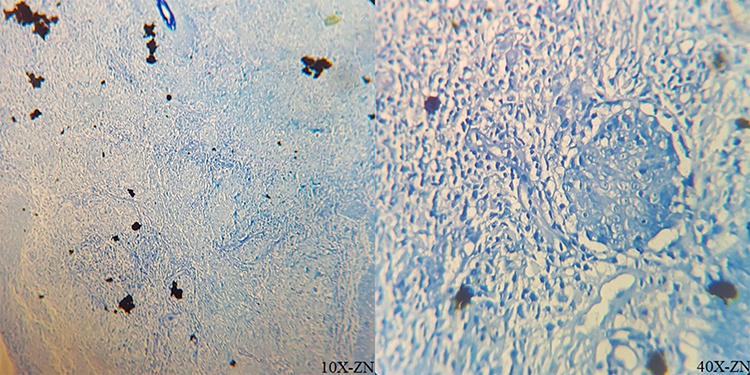 |
Figure 3 The Ziehl–Neelsen stained histopathological assessment (Magnifications: 10× and 40×). |
 |
Figure 4 Clinical appearance of lesions at the end of the 6th (left) month of treatment, and after the second month after treatment (right). |
Discussion
According to WHO reports, TB is one of the top 10 causes of deaths globally and the first cause of death from a single infectious agent.2 Worldwide Prevalence of tuberculosis is increasing but CTB occurs rarely (1–2% of all cases).4,5 Inflammatory papules, verrucous plaques, suppurative nodules, chronic ulcers and other lesions can be identified in CTB.11,12 The most important point in this case was the first presentation of TB as cutaneous involvement in absence of any other symptoms such as cough with sputum and blood at times, chest pains, weakness, weight loss, fever and night sweats or chest X-ray graphical findings. Also, the clinical appearance of disease and location of involvement put the disease on a differential diagnosis list of herpes zoster, herpes simplex, dermatitis herpetiformis and impetigo, and skin reactions caused by contact dermatitis. The interesting points in this case are the location and the mimic of the viral cutaneous infection such as Herpes zoster and as in the pervious report of the authors, rarely as dermatomal pattern of cutaneous manifestation of brucellosis.13 These cases and the similar case reports/series may trigger a hypothesis that in endemic regions, in addition to drug resistance, bacterial infections may develop themselves to mimicking the other microbial infections such as viruses. This hypothesis must be evaluated by RNA, DNA, and protein assessments of the infections that present rare forms, signs or symptoms especially now that in 21st century that we are facing a new era of infections such as COVID-19.14 However, unfortunately in this case report, due to the lack of sufficient funding we could not assess QuantiFeron or GeneXpert assay to identify microbiologic findings and rifampicin resistance. But, due to national tuberculosis guideline’s 6-month therapy, the lesions clearance at the end of the 6th month and even clearance of scars at the end of the 2nd month after therapy, we could conclude absence of main anti-TB drugs resistance (isoniazid and rifampin).
Ethical Issues
The patient’s identity is secret and preserved unknown in the article and the patient received oral and written permission form that was approved by ethics committee of Taleghani Hospital and Urmia University of Medical Sciences. The consent was obtained from the study participant prior to study commencement and the study participant gave consent to publish (including publication of the images).
Acknowledgments
We would like to thank the health care personnel, attendings, and especially medical interns of the infectious disease ward of Taleghani Hospital of Urmia for the great health care services, helping and supporting this paper specially in the crisis of the COVID-19.
Disclosure
The authors report no conflict of interest in this work.
References
1. Lonnroth K, Raviglione M. Global epidemiology of tuberculosis: prospects for control. Semin Respir Crit Care Med. 2008;29(5):481–491. doi:10.1055/s-0028-1085700
2. WHO. Tuberculosis. WHO; 2020 [updated March 24, 2020]. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
3. Bravo FG, Gotuzzo E. Cutaneous tuberculosis. Clin Dermatol. 2007;25(2):173–180. doi:10.1016/j.clindermatol.2006.05.005
4. James WD, Elston DM, Berger TG, Andrews GD. Andrews’ Diseases of the Skin: Clinical Dermatology.
5. Yates VM, Ormerod LP. Cutaneous tuberculosis in Blackburn district (U.K.): a 15-year prospective series, 1981–95. Br J Dermatol. 1997;136(4):483–489. doi:10.1111/j.1365-2133.1997.tb02127.x
6. Amir J, Harel L, Smetana Z, Varsano I. The natural history of primary herpes simplex type 1 gingivostomatitis in children. Pediatr Dermatol. 1999;16(4):259–263. doi:10.1046/j.1525-1470.1999.00072.x
7. Annunziato PW, Gershon A. Herpes simplex virus infections. Pediatr Rev Dec. 1996;17(12):
8. McMillan JA, Weiner LB, Higgins AM, Lamparella VJ. Pharyngitis associated with herpes simplex virus in college students. Pediatr Infect Dis J. 1993;12(4):280–284. doi:10.1097/00006454-199304000-00004
9. Zhu J, Peng T, Johnston C, et al. Immune surveillance by CD8 alphaalpha+ skin-resident T cells in human herpes virus infection. Nature. 2013;497(7450):494–497. doi:10.1038/nature12110
10. Bialvaei AZ, Asgharzadeh M, Aghazadeh M, Nourazarian M, Kafil HS. Challenges of tuberculosis in Iran. Jundishapur J Microbiol. 2017;10:3.
11. Lai-Cheong JE, Perez A, Tang V, Martinez A, Hill V, Menage Hdu P. Cutaneous manifestations of tuberculosis. Clin Exp Dermatol. 2007;32(4):461–466. doi:10.1111/j.1365-2230.2007.02352.x
12. Handog EB, Gabriel TG, Pineda RT. Management of cutaneous tuberculosis. Dermatol Ther. 2008;21(3):154–161. doi:10.1111/j.1529-8019.2008.00186.x
13. Gharebaghi N, Mehrno M, Sedokani A. A rare case of brucellosis with dermatomal pattern of cutaneous manifestation. Int Med Case Rep J. 2019;12:223–228. doi:10.2147/IMCRJ.S203682
14. WHO. WHO Director-General’s opening remarks at the media briefing on COVID-19. World Health Organization; August 28, 2020. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march–2020.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.