")
Back to Journals » International Journal of Women's Health » Volume 14
Chronic Pelvic Pain in Women with Endometriosis is Associated with Psychiatric Disorder and Quality of Life Deterioration
Authors Muharam R , Amalia T, Pratama G , Harzif AK, Agiananda F , Maidarti M, Azyati M, Sumapraja K, Winarto H , Wiweko B, Hestiantoro A, Suarthana E, Tulandi T
Received 19 October 2021
Accepted for publication 3 January 2022
Published 4 February 2022 Volume 2022:14 Pages 131—138
DOI https://doi.org/10.2147/IJWH.S345186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
R Muharam,1 Titi Amalia,1 Gita Pratama,1 Achmad Kemal Harzif,1 Feranindhya Agiananda,2 Mila Maidarti,1 Mazaya Azyati,1 Kanadi Sumapraja,1 Hariyono Winarto,1 Budi Wiweko,1 Andon Hestiantoro,1 Eva Suarthana,3 Togas Tulandi3
1Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia; 2Department of Psychiatry, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia; 3Department of Obstetrics and Gynecology, McGill University, Montreal, Quebec, Canada
Correspondence: R Muharam
Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jl. Pangeran Diponegoro No.71, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430, Indonesia
, Tel +62 812 85143491
, Fax +1 205 975-6110
, Email [email protected]
Background: Endometriosis is a condition associated with pelvic pain, infertility, and possibly with decreased quality of life as well as psychiatric disorder. The purpose of our study was to evaluate the association between pain characteristic, psychiatric disorder, and quality of life in women with endometriosis.
Methods: A cross-sectional study was done involving 160 women with medical diagnosis of endometriosis. Pain intensity was evaluated using Visual Analog Scale (VAS), Quality of Life with Endometriosis Health Profile (EHP-30), and psychologic condition with Mini International Neuropsychiatric Interview International Classification of Diseases (Mini-ICD).
Results: VAS and psychiatric disorder were associated with higher EHP-30 score (β = 9.3 (95% CI: 7.15– 11.45; p < 0.001 and β = 28.51 (95% CI: 20.06– 36.05; p < 0.001), respectively) and hence, lower quality of life. The strongest correlation between VAS and EHP-30 was in pain (r=0.586; p< 0.001) and ‘control and powerlessness’ (r = 0.583; p < 0.001). VAS was also higher in subjects with depression (49.5 (25.4– 77.8) vs 34.4 (6.1– 74.6); p < 0.001).
Conclusion: We conclude that severe endometriosis-related pain and the presence of psychiatric disorder were associated with lower quality of life. Comprehensive management of endometriosis is crucial to improve patients’ quality of life.
Keywords: endometriosis, pain, depression, psychiatric disorder, quality of life
Introduction
Endometriosis is a condition in which endometrium-like tissue is located outside the uterus. It is estimated that 176 million women worldwide suffer from endometriosis and 1.5 to 10% of them were in the reproductive age.1,2 Endometriosis is associated with reduced quality of life due to chronic pelvic pain, dysmenorrhea, and dyspareunia as well as with infertility. It has been reported that 35 to 50% of women with endometriosis suffer from pain, infertility, or both.3,4 Endometriosis symptoms can progressively impair a woman’s ability to carry out some daily activities and result in a perception of worsening health status and overall wellbeing.5
Pain associated with endometriosis can persist after medical treatment and/or surgery, and similarly with the quality of life.6,7 Since chronic pelvic pain is the most common symptom of endometriosis, people who suffer from a chronic illness or condition are exposed to a negative challenge for a long time.8 Accordingly, pain management should be initiated at the beginning of the treatment. In view of endometriosis-related infertility, reproductive health is not commonly discussed in Indonesia. It appears that Indonesian parents feel awkward discussing reproduction with their children.9 This cultural obstacle may cause participants to have little knowledge of their own parent’s reproductive health history.
The purpose of our study was to evaluate the association between pain characteristic, psychiatric disorder, and quality of life in women with endometriosis using the EHP-30 and Mini ICD-10 questionnaire.
Methods
This was a cross-sectional study conducted at National Referral Hospital Cipto Mangunkusumo (RSCM), Jakarta. Between June 2019 and August 2020, we consecutively recruited women aged 18–49 years diagnosed with endometriosis. We included only those with a confirmed diagnosis of endometriosis and suffered from chronic cyclic pelvic pain for at least 6 months. The diagnosis of endometriosis was established by history taking, physical examination, visual detection of endometriotic lesions during previous surgeries, ultrasound examination, or histopathology.
All participants provided a written consent before taking part in the study. Women with chronic pelvic pain due to diseases other than endometriosis were excluded. The women who were excluded, were not undergo endometriosis evaluation. We evaluated demographic data including age, education, history of surgery, parity, body mass index (BMI), and previous medical history. Visual Analogue Scale (VAS) was used to measure pain intensity (scale 1–10); 1: no pain and 10: the worst pain imaginable.
Questionnaires
Patients were asked to fill Endometriosis Health Profile (EHP) questionnaire with a total score of 0 (best quality of life) to 100 (worst quality of life). EHP-30 questionnaire consists of two parts. The first part is a core questionnaire with 30 items applicable to women with endometriosis covering five areas including pain, emotional well-being, control and powerlessness, social support, and self-imaging scales. The second part is a modular section containing six domains, which comprised of 23 questions covering areas such as work, relationship with children, sexual activity, infertility, medical profession and treatment that are not necessarily relevant to all women with endometriosis.10 With the assistance of an interviewer, patients completed Mini ICD-10 questionnaire. The Mini ICD-10 method was chosen because its validity and reliability, and it has been tested using CIDI (Composite International Diagnostic Interview) dan SCID (Structured Clinical Interview for DSM) as gold standards.11 The study was approved by medical research ethics committee of Faculty of Medicine, Universitas Indonesia (Study number: KET-753/UN.2. F1/ETIK/PPM.00.02.2019).
Statistical Analysis
Statistical analysis was conducted using SPSS version 23 (IBM, New York). We grouped the participants into two groups based on VAS value: low3,4 and high VAS.7–10 Data with normal distribution were presented as mean ± standard deviation while skewed data as median and range. Spearman’s rank correlation analysis was used to analyze the relationship between two continuous variables that were not normally distributed. Pearson product moment test was utilized to analyze the normally distributed data. Comparison was measured using t test or Mann–Whitney U-test when appropriate. Multivariate regression analysis was done by including determinant variables with univariate p-value <0.10. A p-value of less than 0.05 was considered significant.
Results
Characteristics of the Study Population and Outcomes Distributions
The study consisted of 160 participants. Their mean duration of formal education was 12 years (56.0%) and most of them were nulliparous (46.3%); 52% had normal BMI, 47.5% were overweight. A half of the participants (50.6%) had a history of surgical treatments. Because the insurance health system in our country did not allow patients to go to a referral hospital, patients were first treated in community hospitals. When we evaluated medical treatment, we found that 45.6% of the participants had been treated with nonsteroid anti-inflammatory drugs (NSAID) and 54.4% with hormonal therapy (DMPA, Leuprorelin acetate, Dienogest, and Goserelin) (Table 1).
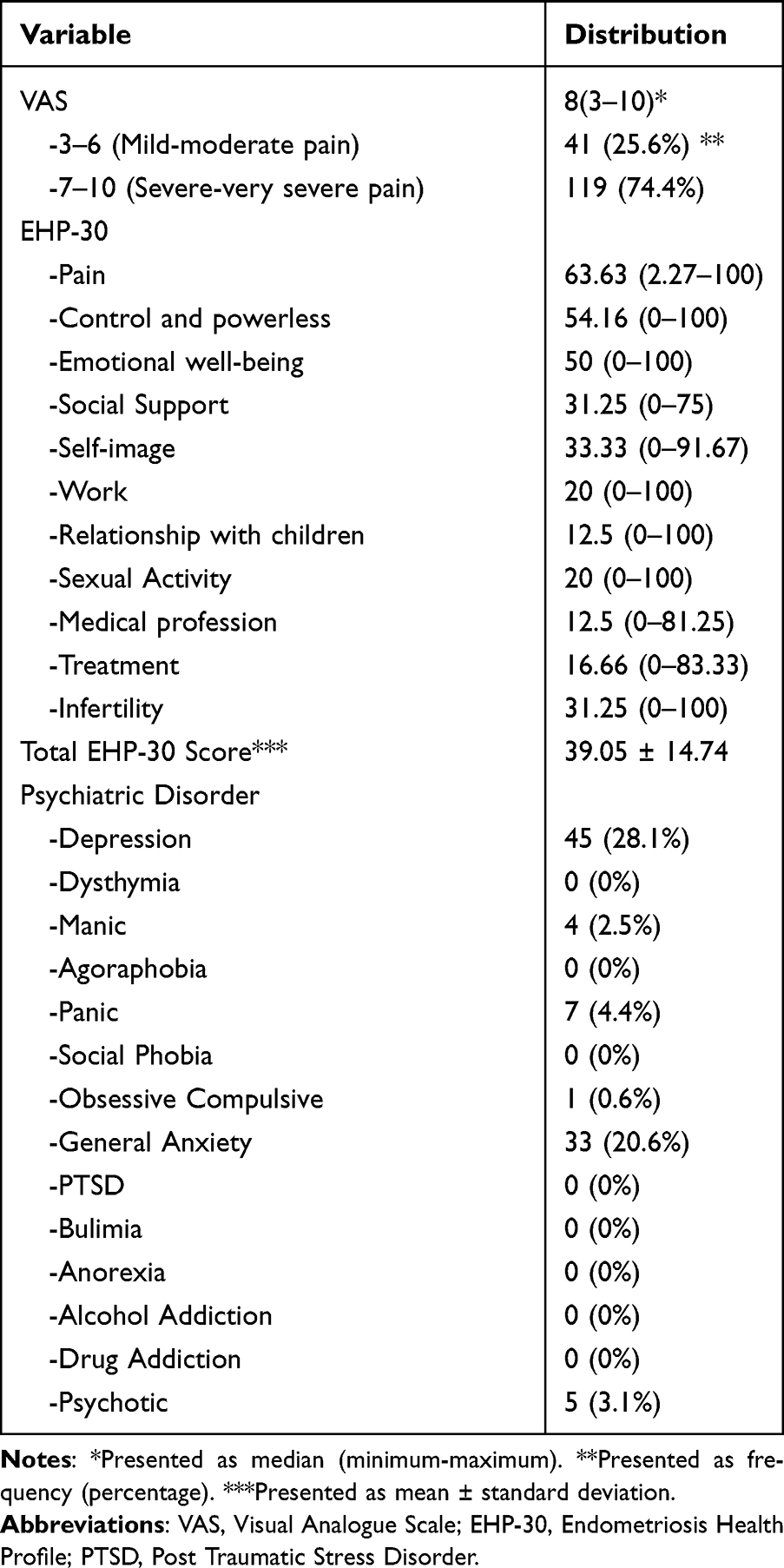 |
Table 1 Characteristic of VAS, EHP-30, and Psychiatric Disorder in Women with Endometriosis-Associated Chronic Pelvic Pain |
In view of pain score, the median VAS value was 8 (range 3–10) and we found that most participants suffered from severe pain (74%). The mean EHP score was 39 14.7% with the highest score observed in the pain component (63.6%) and the “control and powerless” component (54.1%).
14.7% with the highest score observed in the pain component (63.6%) and the “control and powerless” component (54.1%).
The most prevalent psychiatric disorder among the participants was depression (28%) followed by generalized anxiety (20%). We did not encounter other psychiatric disorders such as dysthymia, agoraphobia, social phobia, post-traumatic stress, bulimia, anorexia, alcohol dependence, and drug addiction (Table 1).
Correlation Between Pain Intensity and Quality of Life
When we evaluated the correlation between pain intensity as determined by VAS and the EHP-30 score for quality of life, we found that pain intensity significantly correlated with the total score of EHP-30 (p < 0.001, r = 0.573) (Table S1). There was also a significant correlation between VAS levels and EHP-30 components of pain (p<0.001), control and powerlessness (p<0.001), emotional well-being (p<0.001), social support (p<0.001), self-image (p=0.002), relationships with children (p<0.001), medical profession (p=0.033), treatment (p=0.028), and infertility (p=0.001).
Factors Associated with Severe Pain
Table 2 shows univariate associations between demographic and clinical characteristics and pain intensity using VAS levels. We found significant associations between VAS levels and surgical history (p<0.001), Body Mass Index (BMI) with p=0.014, and psychiatric disorder (p=0.087). Table 3 shows that surgical history had the strongest significant association with pain intensity (p=0.002).
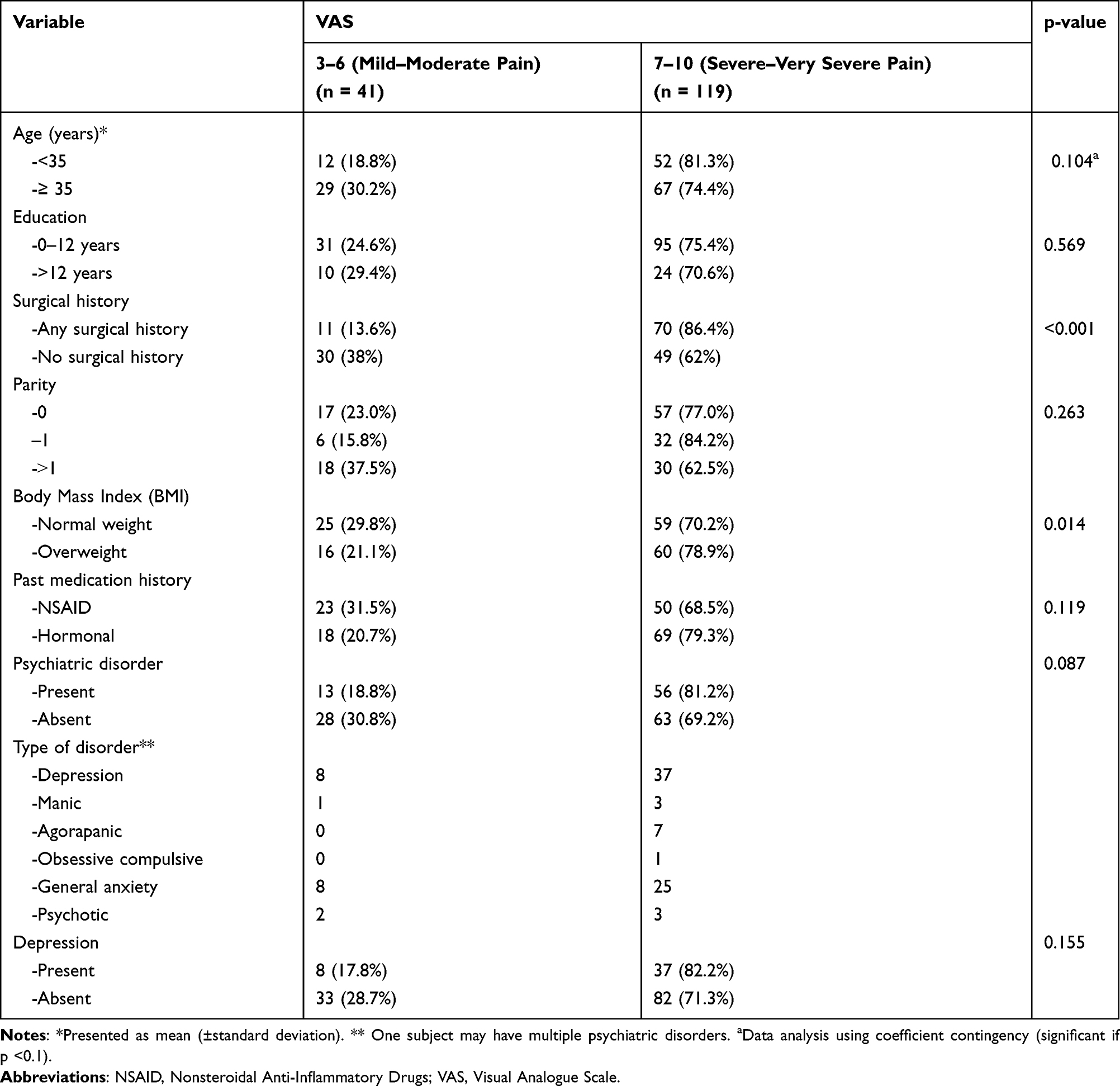 |
Table 2 Univariate Analysis of the Pain Level (VAS) |
 |
Table 3 Multivariate Analysis for Severe and Very Severe Pain (VAS 7–10) in Women with Endometriosis |
Factors Associated with Quality of Life
Univariate associations between the characteristics of the subjects and the quality of life using EHP-30 score are shown in Table 4. EHP-30 score was significantly higher, which reflected a lower quality of life, in subjects with than without psychiatric disorders. Subsequently, we found that EHP-30 score was significantly higher in subjects with than without depression 9.84 (6.07–13.60); p<0.001)) (Table S2). Other psychiatric disorders were not significantly associated with EHP-30 score. We also found that VAS (p<0.001) and depression (p<0.001) were independently associated with quality of life in women with endometriosis (Table S3).
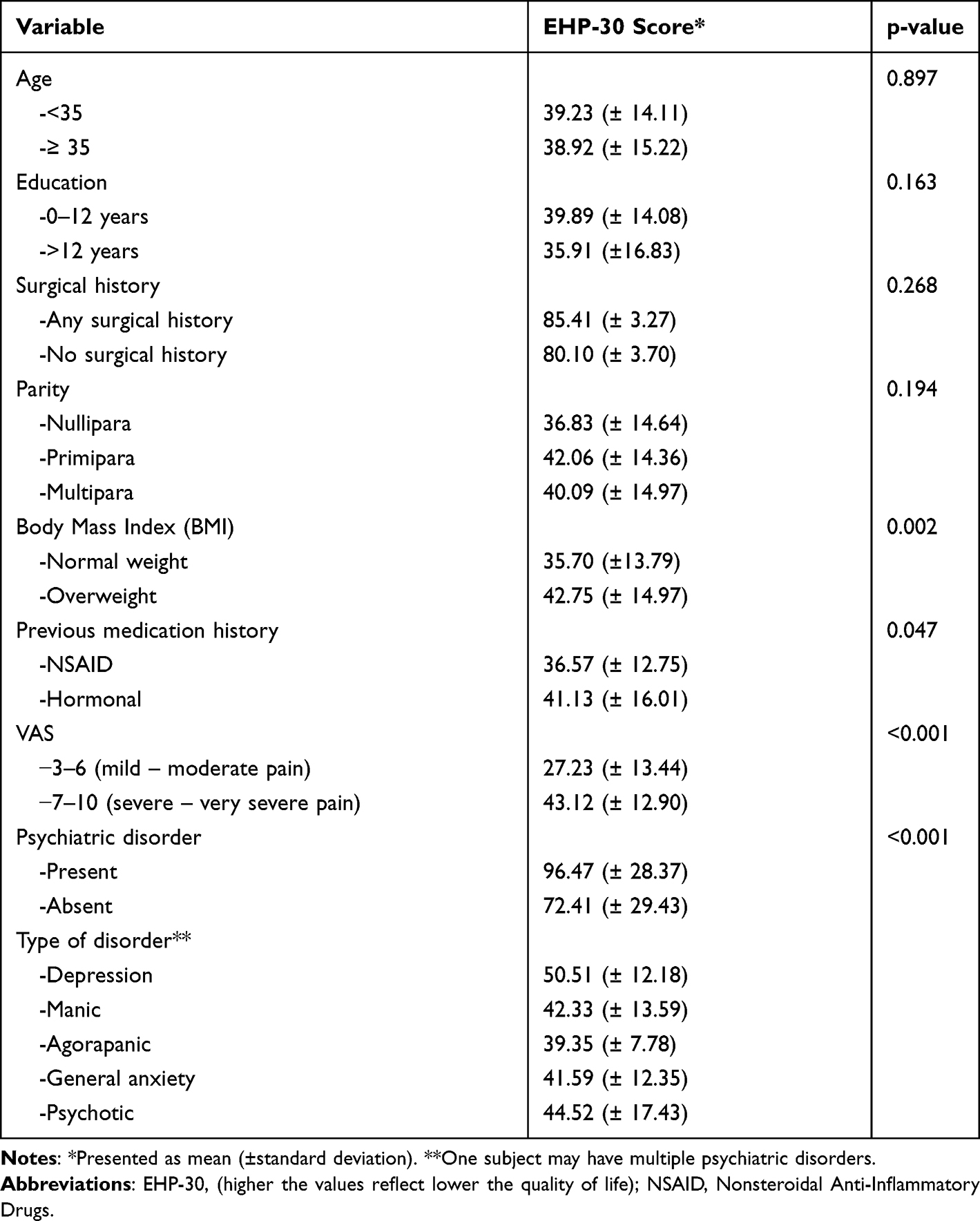 |
Table 4 Univariate Analysis of Quality of Life |
There was no significant difference between history of medical management and VAS (p=0.288), EHP-30 (p=0.254), or depression (p=0.380) (Tables S4 and S5). Of interest, history of surgical management was significantly associated with VAS (p<0.001), but not with EHP-30 or depression (Tables S6 and S7).
Multivariate analysis demonstrated that VAS and psychiatric disorders were independently associated with EHP-30 score (Table 5). Based on the formula for this linear regression model, a point increase in VAS would increase EHP-30 score by 9.30 (95% CI: 7.15–11.45; p<0.001) and psychiatric disorders would increase EHP-30 score by 28.51 (95% CI: 20.06–36.05; p<0.001).
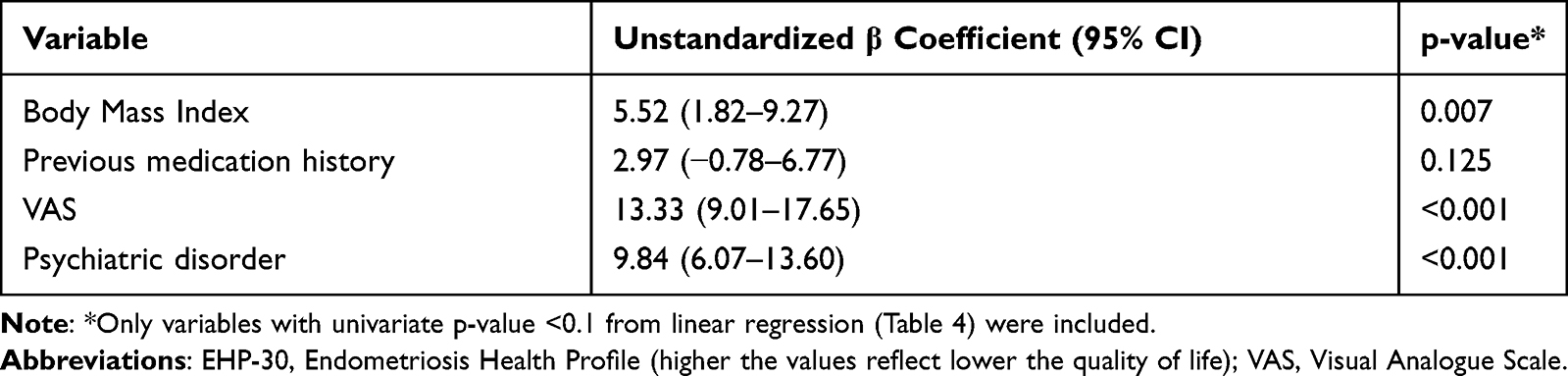 |
Table 5 Multivariate Analysis of Quality of Life (EHP-30 Score) in Endometriosis Patients |
Discussion
We found that pain and “control and powerless” were the components with the highest score in women with endometriosis. The high pain score indicates severe pain among our patients. Lower score of pain has been reported previously.12 The high level of control and powerlessness could be attributed to the pain experienced suggesting impairment in their life control. Emotional well-being component scored high as well. This component evaluated emotional disturbances faced by the participants as well as their perception of psychiatric disorders. The components that scored low in our study were relationship with children, treatment, and medical profession, substantially lower than other studies.12 This might be due to the unique Indonesian culture.
Depression and anxiety disorder were the most prevalent psychiatric disorder among our patients. Previous study showed that depression was higher in women due to hormonal changes.13 Depression and generalized anxiety disorders are common in women with endometriosis.14,15 It has been reported that those women have a high risk of developing generalized anxiety disorder and depression, alcohol addiction, and attention deficit hyperactivity disorder.16 Endometriosis women were at highest risk of depression with a hazard ratio of 1.98 and16 about 23% of them suffered from depression.17 In our study, 28.1% of the participants were found to have depression.
Multivariate analysis indicated that VAS score was independently associated with EHP-30 and its components consisting of pain, control and powerless, emotional well-being, social support, self-image, relationships with children, medical profession, treatment, and infertility. Components with moderate correlation in our study were pain, control and powerless, and emotional well-being, while others showed weak correlations with VAS score. The association between chronic pelvic pain and reduced quality of life has been previously described.18 Patients that affected by posterior DIE (Deep Infiltrating Endometriosis) usually have severe painful symptoms (dysmenorrhea, chronic pelvic pain, dyspareunia, pain on defecation, and pain on micturition) that severely reduce the quality of life.19 Yela et al reported that chronic pelvic pain was the only factor associated with poor quality of life, and quality of life improved following pain control.20 Although the EHP-30 and VAS both measure pain scale, the EHP-30 questionnaire contains other components such as control and powerless. The results show that pain influences patient’s perception of disease control.
We found that endometriosis patients with psychiatric disorder had a higher EHP-30 score (by almost 30 points) than those without. This means endometriosis patients with psychiatric disorder had lower quality of life.21 In this context, endometriosis patients diagnosed with psychiatric disorder, especially depression, may require psychiatric management to prevent psychiatric disease progression and deterioration of quality of life.
Limitations
The limitations of our study included the fact that some participants were previously treated before data collection. Further, 37% of them were treated with dienogest, which could be associated with depression in long term usage.22 However, the mean duration of dienogest treatment was less than six months. Further, primary and secondary health care providers in Indonesia do not use of dienogest or GnRH agonists. As a result, patients seek treatment at tertiary care centers. The implementation of stepwise approach in Indonesian healthcare system led to the difficulty in excluding participants who had received treatment. Accordingly, most patients had received treatment before they were referred to our institution. Also, the cross-sectional nature of our study prevents causation identification and the lack of visual confirmation at laparoscopy and pathological confirmation of endometriosis.
The strength of our study was that we included both quality of life and the presence of psychiatric disorder and correlate them with the degree of pain assessed by VAS score. This may add additional information that when dealing with endometriosis patients diagnosed with psychiatric disorders, especially depression, a multidisciplinary approach is necessary to prevent the progression of psychiatric disorders and deterioration of the quality of life. To the best of our knowledge, this is the first study correlating the level of pain score, quality of life and psychiatric disorders among women with endometriosis. The use of Mini ICD-10 in this study allowed a quick and easy process for screening psychiatric disorders. Yet, diagnosis of psychiatric disorder still requires an in-depth interview by a psychiatrist. Accordingly, patients with psychiatric disorders discovered by Mini-ICD 10 questionnaire should be referred to a psychiatrist for further evaluation and treatment.
Conclusion
We conclude that severe endometriosis-related pain and the presence of psychiatric disorder were associated with lower quality of life. Comprehensive management of endometriosis is crucial to improve patients’ quality of life.
Abbreviations
BMI, Body Mass Index; CIDI, Composite International Diagnostic Interview; EHP, endometriosis health profile; GnRH, gonadotropin-releasing hormone; Mini-ICD, Mini International Neuropsychiatric Interview International Classification of Diseases; NSAID, nonsteroid anti-inflammatory drugs; RSCM, National Referral Hospital Cipto Mangunkusumo; SCID, Structured Clinical Interview for DSM; VAS, visual analog scale.
Ethics Approval
Ethical approval was granted by the Ethics Committee at the Faculty of Medicine, University of Indonesia (KET-753/UN2.F1/ETIK/PPM.00.02/2019). Informed consent was obtained from all patients. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all participants.
Consent for Publication
Not applicable.
Author Contributions
MR designed the project. TA, GP, AKH, and FA took part in the acquisition and management of data. TA and MA performed the analysis under the supervision of KS, HW, BW, and AH. MR, TA, and MM drafted the manuscript. TT, ES critically reviewed the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any external funding from sponsors or any other third parties for this study. This study was self-funded by the authors.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Johnson NP, Hummelshoj L, Adamson GD, et al. World Endometriosis Society consensus on the classification of endometriosis. Hum Reprod. 2017;32(2):315–324. doi:10.1093/humrep/dew293
2. Bulletti C, Coccia ME, Battistoni S, Borini A. Endometriosis and infertility. J Assist Reprod Genet. 2010;27(8):441–447. doi:10.1007/s10815-010-9436-1
3. Kennedy S, Bergqvist A, Chapron C, et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod. 2005;20(10):2698–2704. doi:10.1093/humrep/dei135
4. Nnoaham KE, Hummelshoj L, Webster P, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril. 2011;96(2):366–73.e8. doi:10.1016/j.fertnstert.2011.05.090
5. Parra RS, Feitosa MR, Camargo HP, et al. The impact of laparoscopic surgery on the symptoms and wellbeing of patients with deep infiltrating endometriosis and bowel involvement. J Psychosom Obstet Gynaecol. 2021;42(1):75–80. doi:10.1080/0167482X.2020.1773785
6. Howard FM. Endometriosis and mechanisms of pelvic pain. J Minim Invasive Gynecol. 2009;16:540–550. doi:10.1016/j.jmig.2009.06.017
7. Osório FL, Carvalho AC, Donadon MF, Moreno AL, Polli-Neto O. Chronic pelvic pain, psychiatric disorders and early emotional traumas: results of a cross sectional case-control study. World J Psychiatry. 2016;6(3):339–344. doi:10.5498/wjp.v6.i3.339
8. Škegro B, Bjedov S, Mikuš M, et al. Endometriosis, pain and mental health. Psychiatr Danub. 2021;33(Suppl 4):632–636.
9. Hull TH, Hasmi E, Widyantoro N. “Peer” educator initiatives for adolescent reproductive health projects in Indonesia. Reprod Health Matters. 2004;12(23):29–39. doi:10.1016/S0968-8080(04)23120-2
10. Nojomi M, Bijari B, Akhbari R, Kashanian M. The assessment of reliability and validity of Persian Version of the Endometriosis Health Profile (EHP-30). Iran J Med Sci. 2011;36(2):84–89.
11. Quintana MI, JdJ M, Ribeiro WS, Jorge MR, Andreoli SB. Accuracy of the Composite International Diagnostic Interview (CIDI 2.1) for diagnosis of post-traumatic stress disorder according to DSM-IV criteria. Cadernos de Saúde Pública. 2012;28:1312–1318. doi:10.1590/S0102-311X2012000700009
12. Khong S-Y, Lam A, Luscombe G. Is the 30-item Endometriosis Health Profile (EHP-30) suitable as a self-report health status instrument for clinical trials? Fertil Steril. 2010;94(5):1928–1932. doi:10.1016/j.fertnstert.2010.01.047
13. Muharam R, Setiawan MW, Ikhsan M, Rizkinya HE, Sumapraja K. Depression and its link to other symptoms in menopausal transition. Middle East Fertility Soc J. 2018;23(1):27–30. doi:10.1016/j.mefs.2017.08.003
14. Novais RFSR, Camara-Frana B, Lasmar RB, Lasmar BP. Endometriosis and its relationship with depression. Int J Clin Med. 2018;09(2):8. doi:10.4236/ijcm.2018.92008
15. Laganà AS, La Rosa VL, Rapisarda AMC, et al. Anxiety and depression in patients with endometriosis: impact and management challenges. Int J Womens Health. 2017;9:323–330. doi:10.2147/IJWH.S119729
16. Gao M, Koupil I, Sjöqvist H, et al. Psychiatric comorbidity among women with endometriosis: nationwide cohort study in Sweden. Am J Obstet Gynecol. 2020;223:
17. Pope CJ, Sharma V, Sharma S, Mazmanian D. A systematic review of the association between psychiatric disturbances and endometriosis. J Obstet Gynaecol Can. 2015;37(11):1006–1015. doi:10.1016/S1701-2163(16)30050-0
18. Stull DE, Wasiak R, Kreif N, et al. Validation of the SF-36 in patients with endometriosis. Qual Life Res. 2014;23(1):103–117. doi:10.1007/s11136-013-0442-5
19. Spagnolo E, Zannoni L, Raimondo D, et al. Urodynamic evaluation and anorectal manometry pre- and post-operative bowel shaving surgical procedure for posterior deep infiltrating endometriosis: a pilot study. J Minim Invasive Gynecol. 2014;21(6):1080–1085. doi:10.1016/j.jmig.2014.05.012
20. Yela DA, Quagliato IP, Benetti-Pinto CL. Quality of life in women with deep endometriosis: a cross-sectional study. Rev Bras Ginecol Obstet. 2020;42(02):90–95. doi:10.1055/s-0040-1708091
21. Friedl F, Riedl D, Fessler S, et al. Impact of endometriosis on quality of life, anxiety, and depression: an Austrian perspective. Arch Gynecol Obstet. 2015;292:1393–1399. doi:10.1007/s00404-015-3789-8
22. Heinemann K, Imthurn B, Marions L, et al. Safety of dienogest and other hormonal treatments for endometriosis in real-world clinical practice (VIPOS): a large noninterventional study. Adv Ther. 2020;37(5):2528–2537. doi:10.1007/s12325-020-01331-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.