")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Chronic obstructive lung disease and posttraumatic stress disorder: current perspectives
Authors Abrams T, Blevins A, Vander Weg M
Received 1 May 2015
Accepted for publication 12 August 2015
Published 15 October 2015 Volume 2015:10(1) Pages 2219—2233
DOI https://doi.org/10.2147/COPD.S71449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Thad E Abrams,1,2 Amy Blevins,1,3 Mark W Vander Weg1,2,4
1Department of Internal Medicine, University of Iowa, 2Center for Comprehensive Access and Delivery Research and Evaluation, Iowa City VA Health Care System, 3Hardin Health Sciences Library, 4Department of Psychological and Brain Sciences, University of Iowa, Iowa City, IA, USA
Background: Several studies have reported on the co-occurrence of chronic obstructive pulmonary disease (COPD) and psychiatric conditions, with the most robust evidence base demonstrating an impact of comorbid anxiety and depression on COPD-related outcomes. In recent years, research has sought to determine if there is a co-occurrence between COPD and posttraumatic stress disorder (PTSD) as well as for associations between PTSD and COPD-related outcomes. To date, there have been no published reviews summarizing this emerging literature.
Objectives: The primary objective of this review was to determine if there is adequate evidence to support a co-occurrence between PTSD and COPD. Secondary objectives were to: 1) determine if there are important clinical considerations regarding the impact of PTSD on COPD management, and 2) identify targeted areas for further research.
Methods: A structured review was performed using a systematic search strategy limited to studies in English, addressing adults, and to articles that examined: 1) the co-occurrence of COPD and PTSD and 2) the impact of PTSD on COPD-related outcomes. To be included, articles must have addressed some type of nonreversible obstructive lung pathology.
Results: A total of 598 articles were identified for initial review. Upon applying the inclusion and exclusion criteria, n=19 articles or abstracts addressed our stated objectives. Overall, there is inconclusive evidence to support the co-occurrence between PTSD and COPD. Studies finding a significant co-occurrence generally had inferior methods of identifying COPD; in contrast, studies that utilized more robust COPD measures (such as a physician exam) generally failed to find a relationship. Among studies that examined the impact of PTSD on COPD-related outcomes, there was more consistent evidence that PTSD affects the perception of respiratory symptom burden and management. In addition, methods for measuring an important confounder (smoking) were generally lacking.
Conclusion: There is inconclusive evidence to support the co-occurrence of COPD and PTSD. There was stronger evidence implicating PTSD as an important comorbidity impacting COPD management. Further research is needed to: 1) determine whether or not COPD and PTSD are likely to be comorbid, and 2) further elucidate the mechanisms connecting PTSD and COPD-related outcomes.
Keywords: chronic lung disease, nonproductive cough, WTC cough syndrome, posttraumatic stress disorder, Veterans
Background
Chronic obstructive pulmonary disease (COPD) is a preventable chronic condition best characterized by measurable, nonreversible restrictions in air flow with repeated, intermittent exacerbation of symptoms generally manifested by shortness of breath, nonproductive cough, sensations of air hunger, and reduced capacity for physical activity.1 It is the third leading cause of mortality in the USA, with a prevalence estimate approximately 9%–10%.2–4 COPD also contributes to substantial direct and indirect costs to both patients and systems of care.1
In many ways, the course and characteristics of posttraumatic stress disorder (PTSD) are similar to COPD. For example, PTSD is characterized by marked intermittent patterns of exacerbations of the core symptoms – intrusive thoughts, avoidance, hyperarousability, and negative cognitions. PTSD is common (estimates ranging from 1% to 32%), generally considered treatable but incurable,5–7 and is associated with increased morbidity, mortality, and health care costs.8
A considerable body of research has examined the bidirectional associations between psychiatric comorbidity and COPD; efforts that have largely been limited to the conditions of anxiety and depression.9 For example, a recent meta-analysis identified 22 papers encompassing a pooled population of nearly 30,000 subjects revealed important bidirectional relationships between both anxiety and/or depression on COPD co-occurrence and the impact of anxiety and/or depression on COPD outcomes. The meta-analysis reported on three key findings: 1) mortality risk in patients with COPD and depression, 2) mortality risk or COPD outcomes and anxiety exposure, and 3) COPD and depression and/or anxiety risk. Notwithstanding methodological heterogeneity, the meta-analysis reported a higher risk for mortality among patients with COPD suffering from depression (relative risk [RR] =1.83; 95% confidence interval [CI] =1.00–3.36). Similarly, the RR for mortality or worse COPD outcomes was higher among patients with COPD and anxiety (RR =1.27; 1.02–1.58). COPD severity was also associated with greater relative risk of anxiety or depression (1.69; 1.45–1.96). In conclusion, the report emphasized the importance of performing routine monitoring for anxiety or depression in patients with COPD.
In contrast to this evidence base, we were unable to locate any reviews addressing the associations between PTSD and COPD. Our interest in performing a review of this topic was primarily driven by three factors: 1) our clinical observations, 2) the individual studies that have investigated this association, and 3) a recent review article discussing plausible immune-mediated mechanisms supporting a biological framework for the association.10
Thus, in the context of the emerging evidence base outlining the associations between psychiatric comorbidity and COPD and because of the lack of a review specifically addressing PTSD, we performed this review with the following aims: 1) to provide a comprehensive review of the literature examining the co-occurrence of PTSD and COPD, and 2) to identify areas for more focused research efforts. To the best of our knowledge this is the first review article on this topic.
Methods
This structured review began with an initial literature search performed by a health sciences librarian (AB) using several indexed databases: MEDLINE through Ovid, Cochrane Database of Systematic Reviews through Wiley, Database of Abstracts of Reviews of Effects through Wiley, Cochrane Central Register of Controlled Trials through Wiley, Embase through Wiley, Web of Science, and ClinicalTrials.gov in January 2015. Terms included subject headings and keywords for posttraumatic stress disorder, chronic obstructive pulmonary disease, emphysema, asthma, and chronic bronchitis. No filters for language, year, etc, were applied to the searches. Full search strategies from all databases are listed in the Supplementary materials. TA reviewed the reference lists provided in each of the final selected studies to identify studies not captured in the preliminary literature search (n=8).
Inclusion and exclusion criteria
To be included in this review, publications must have included: 1) COPD or other nonreversible obstructive lung disease states, 2) PTSD in the sample, and 3) an examination of associations between COPD and PTSD reflecting at least one of the following main topical areas: epidemiology, treatment receipt, or outcomes (eg, risk of hospitalization, and medication adherence). The review was limited to studies available in the English language. In a stepwise fashion, Figure 1 illustrates the number of articles examined and the reasons for exclusion.
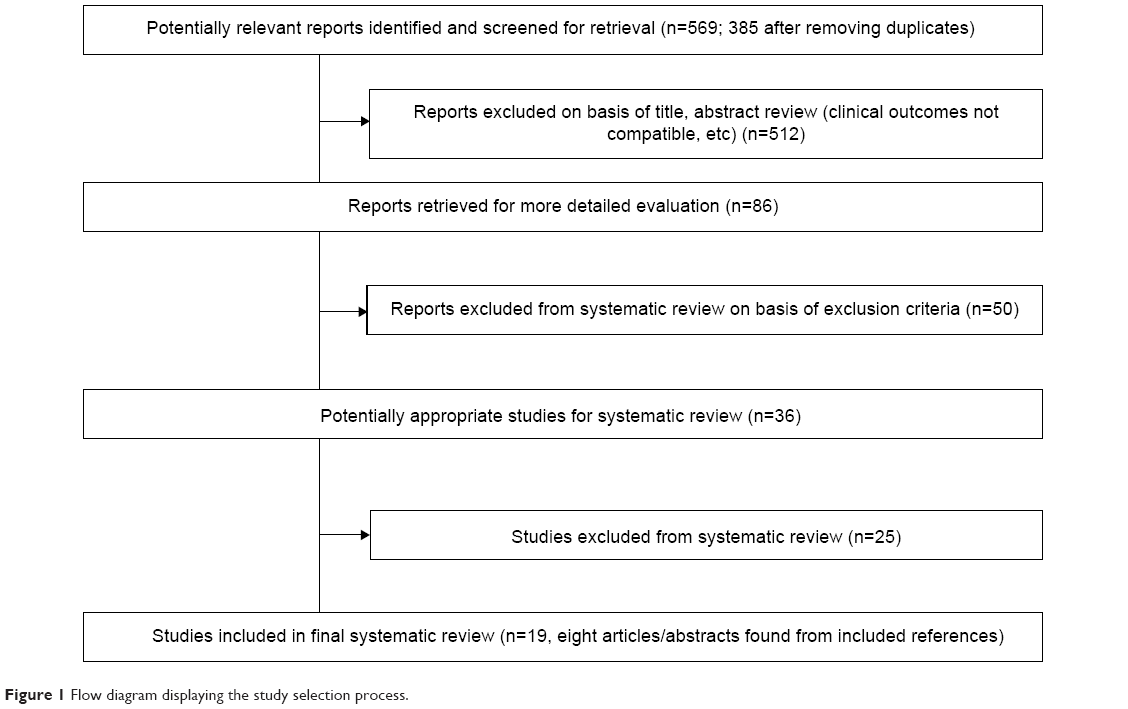 | Figure 1 Flow diagram displaying the study selection process. |
Several identified studies were excluded as the focus was on the impact of PTSD on asthma or on self-reported symptoms of shortness of breath rather than COPD. We also excluded several studies examining the impact of trauma on pulmonary diseases in children. Several studies with a primary focus on the relationship between PTSD and more broadly defined medical comorbidities were also identified. In some of these studies, the methods for identifying COPD captured all respiratory illnesses; eg, cases of asthma were included with the COPD definition, or other bronchial asthma or chronic bronchitis. We elected to include these reports.11–14 In at least one other case, a study examined associations between PTSD and respiratory diseases (including COPD); however, the authors only reported broad associations between the degree of medical comorbidity and PTSD and not the specific relationship between the respiratory conditions and PTSD. Consequently, this article was excluded.15
Furthermore, we identified several manuscripts focused on first responders for the events following 9/11. From this literature, there was a notable emphasis on first responders’ exposure to high concentrations of air particulate matter and subsequent development of lower respiratory airway symptoms corresponding with trauma exposure and/or probable PTSD. Many of these studies evaluated exposure to the World Trade Center (WTC) dust cloud according to various factors: self-reported degree of exposure, type of first responder, and the timing of arrival to the recovery scene. Therefore, even if the studies did not specifically identify COPD per se, we included this literature in the review. Our reasoning for including this population is due to the fact that the clinical description of the lower respiratory symptoms reported by responders in the WTC recovery effort reflects many of the same symptoms of COPD. For example, official description of the symptoms related to the WTC recovery effort has been characterized by Niles et al
WTC cough syndrome is a descriptive term and requires at least one symptom in each of the three categories (upper respiratory, lower respiratory, and gastroesophageal reflux disease (p 1147)).16
The similarities between the WTC cough syndrome and COPD include measurable obstructive airflow limitations, an intermittent pattern of exacerbations of nonproductive cough, and shortness of breath. Because we thought that these studies could potentially help to shed light on the associations between PTSD and COPD, we decided to include them in the review.
Results
From an initial pool of 598 articles, we identified 19 articles for final review. Eight articles were identified by hand searching the references for eleven of the articles identified by the literature review strategy. We found notable heterogeneity between the final studies included in the review and thus have organized the results according to the key methodological characteristics including population, methods for identifying the obstructive lung pathology, including obstructive lung pathology, COPD, and PTSD, and the primary and secondary outcomes. A focused summary containing the key elements for each of the articles is provided in Tables 1 and 2.
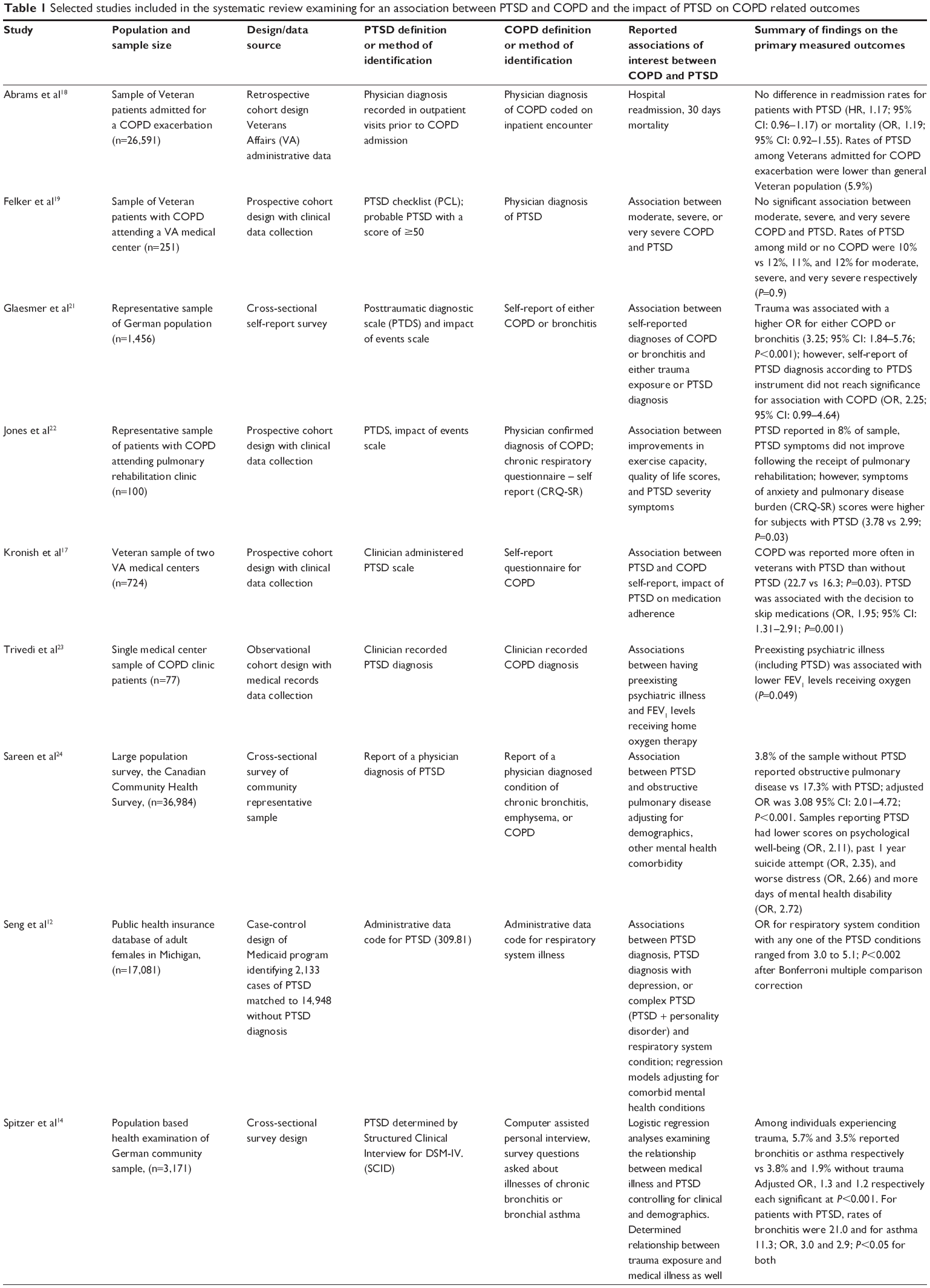 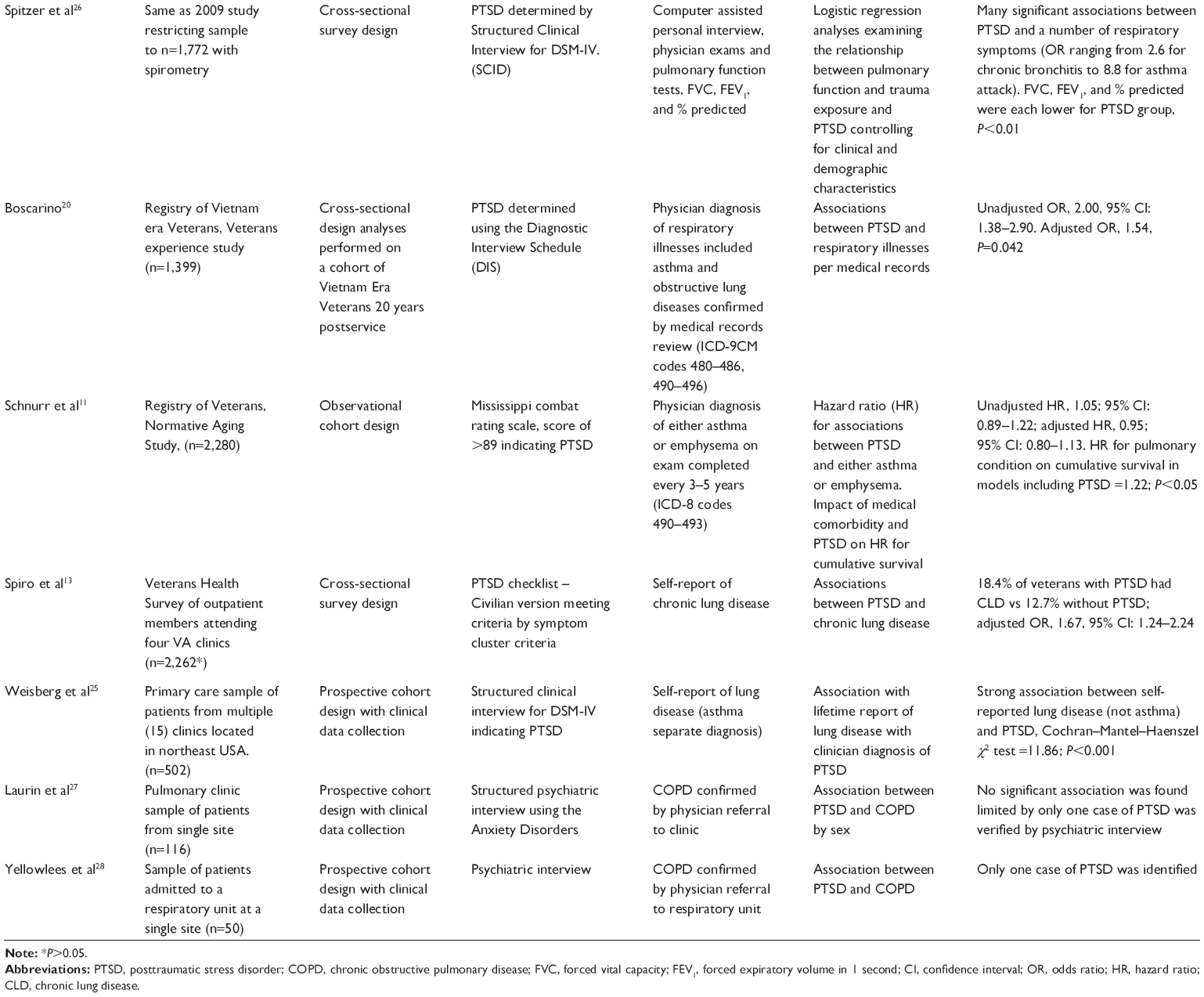 | Table 1 Selected studies included in the systematic review examining for an association between PTSD and COPD and the impact of PTSD on COPD related outcomes |
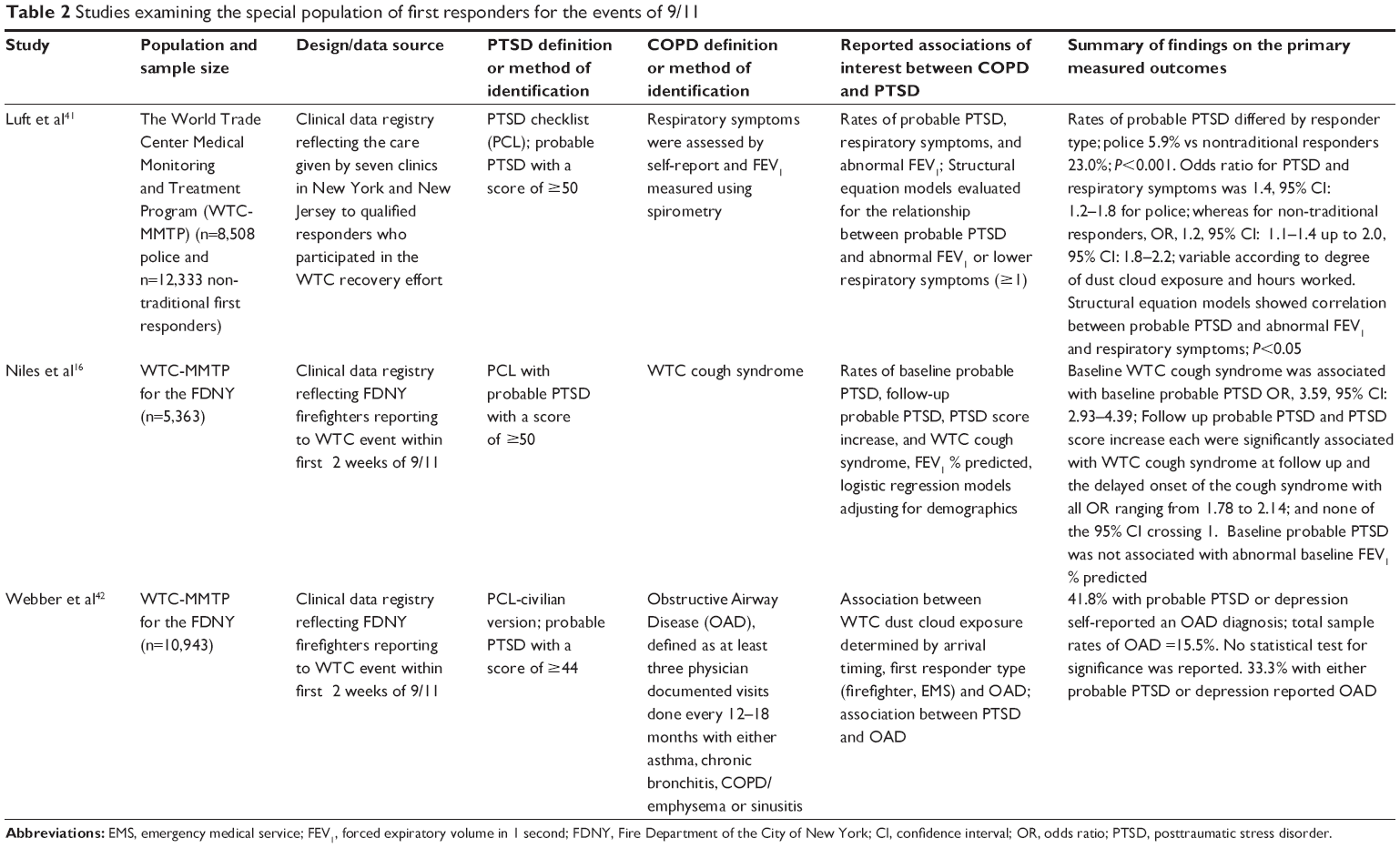 | Table 2 Studies examining the special population of first responders for the events of 9/11 |
Studies examining for the co-occurrence between obstructive lung disease, COPD, and PTSD
We initially focused on studies that utilized methods to separate the diagnosis of COPD from respiratory illnesses more broadly. Within this group of studies, important differences in sample characteristics were observed. Six studies focused on Veteran samples.11,13,17–20 The others included community-dwelling adults, samples of patients attending outpatient clinics, and samples of patients enrolled in health organizations.12,14,21–28
Studies of Veterans examining for the co-occurrence of respiratory conditions, COPD and PTSD
These Veteran-based studies provided mixed evidence to support the co-occurrence between COPD and PTSD. Two studies17,19 used a prospective study design with samples of Veterans recruited from outpatient clinics and tested for the co-occurrence between COPD and PTSD, but reported conflicting results. Kronish et al17 investigated the impact of PTSD on medication adherence and reported a co-occurrence between COPD and PTSD. Felker et al19 aimed to determine the impact of depression and anxiety on health-related quality of life among a sample of Veterans attending Veterans Health Administration outpatient clinics with at least moderate COPD, as measured by physician exam. In this study, Felker et al19 utilized a self-report PTSD assessment. Thus, the lack of structured illness assessments for both PTSD and COPD in both studies may have contributed to the disparate findings.
Another study examined the impact of PTSD on rates of hospital readmission and mortality among a group of Veterans admitted for an exacerbation of COPD using Veterans Health Administration medical records data.18 Although there were no direct tests for the significant co-occurrence of COPD and PTSD, the observed rates of PTSD (5.9%) were considerably lower than those observed in the general Veteran population,29 suggesting a nonsignificant co-occurrence with COPD.
Three other studies among Veterans focused on the association between PTSD symptoms and respiratory illnesses more broadly. Schnurr et al11 examined a longitudinal cohort of Veterans with the primary objective of exploring the relationship between PTSD symptoms and the risk for developing a pulmonary condition and cumulative survival. The pulmonary conditions included both reversible and nonreversible obstructive pulmonary disease types. The burden of PTSD symptoms was not associated with an increased risk for the development of any of the included respiratory illnesses following adjustment for baseline smoking, alcohol, and body mass index. However, a subanalysis on the mediation effect of combat exposure and PTSD symptom burden on the risk of developing a respiratory illness revealed a significant hazard ratio (HR) of 1.22 (P<0.05). Using a similar approach, Boscarino20 analyzed a registry of Vietnam era Veterans with the primary objective of determining the relationship between PTSD and medical comorbidities. Clinical exams were used to determine all key variables, the respiratory conditions (including emphysema and asthma), and PTSD. Boscarino20 found that PTSD increased the risk of having a respiratory condition which remained significant after adjustment for up to 14 control variables including demographics, drug use, alcohol abuse, tobacco use, army enlistment status, and baseline enlistment physical and psychiatric status. While each of these studies utilized longitudinal registries and similar PTSD and pulmonary condition identification methods, a strength of the Boscarino study20 was the inclusion of a large number of PTSD cases relative to the study by Schnurr et al11 (n=332 vs n=6). The Schnurr study11 overcame limitations of statistical power by examining PTSD symptom burden as a continuous variable.
The final Veteran-based study was performed by Spiro et al13 who examined an ambulatory sample of Veterans accessing outpatient services. The study was conducted to address prior studies’ conflicting results regarding associations between PTSD and health status using medical claims based data. The authors reasoned that a study design using self-reported illness measures would be a better representation of health status relative to coded medical data.13 As with the aforementioned studies, the authors characterized the pulmonary conditions as chronic lung disease and did not distinguish COPD from related respiratory disorders. The study found higher rates of chronic lung disease among a sample of Vietnam Veterans with PTSD relative to those without PTSD.
We conclude that, among studies focused on Veterans testing for the co-occurrence of respiratory conditions or COPD, and PTSD, there is insufficient evidence to support a clear relationship. While several studies identified a significant co-occurrence between PTSD and COPD, only one study had the primary objective of determining the presence of a significant co-occurrence between COPD severity and PTSD.19 Also, while older studies benefitted from a more robust method of determining PTSD, these studies lacked the ability to distinguish COPD from other respiratory conditions more broadly. This methodological heterogeneity likely accounted for the disparate findings across studies.
Studies of clinic and community samples examining for the co-occurrence of respiratory conditions, COPD and PTSD
A second set of studies was identified that focused on non-Veteran samples. From this group, ten studies examined community-dwelling adults, clinical samples, or health system enrollees.12,14,21–28 As with the Veteran-based literature, there was inconclusive evidence to support a clear co-occurrence of PTSD and COPD. Glaesmer et al21 examined for the co-occurrence between PTSD and trauma exposure with several medical conditions, including COPD, within a sample of German community members. Four hundred twenty-three subjects (29.1%) reported trauma exposure with 67 (4.6%) classified as having PTSD based on a validated clinician-administered scale. All medical conditions were determined using self-report. The authors found an association between either COPD or chronic bronchitis and trauma exposure. However, when the sample was restricted to those with PTSD based on responses to a validated symptom scale,21 the association was no longer statistically significant. As with the Schnurr et al report,11 the relatively low numbers of cases of PTSD may have contributed to the absence of a statistically significant association.
Jones et al22 examined the prevalence of PTSD among patients with COPD attending a pulmonary rehabilitation program. Health status was assessed by self-report, while PTSD was measured using the Posttraumatic Diagnostic Scale. As the prevalence of PTSD in the study sample (8%) is similar to the prevalence of PTSD observed in the general population this suggests the lack of a relationship with COPD,22 although again, it is unlikely that the study had adequate statistical power to detect an association if one existed. The remaining three studies either identified PTSD too infrequently (eg, <5 cases) for meaningful analysis or did not distinguish PTSD from other psychiatric conditions.23,27,28
The remaining five studies are discussed individually, primarily because each of the study methods relied on a broader definition of respiratory illness that also included COPD.12,14,24–26 Sareen et al24 examined associations between PTSD and respiratory disease in a sample of nearly 37,000 community members. COPD, chronic bronchitis, and emphysema were combined into a composite measure of respiratory conditions. Each condition, as well as PTSD, was determined according to whether the respondents had ever been diagnosed with the condition by a physician.24 Despite the relatively low rate of PTSD (ie, 1%, n=478), individuals with PTSD reported a fourfold increase in the odds of obstructive lung conditions relative to those without PTSD.
In a series of two smaller, similarly designed studies on a representative sample of community-dwelling adults in Germany, Spitzer et al14,26 report a significant co-occurrence between obstructive respiratory conditions and PTSD. The initial study identified PTSD based on a clinical exam, while the respiratory conditions were determined by a computer-assisted telephone survey. PTSD, which was identified in 62 subjects (2%), was associated with a threefold increase in reporting one of the respiratory conditions. The follow-up study utilized the same cohort and augmented the analyses by using spirometry to define the degree of pulmonary dysfunction. The authors reported a positive relationship between PTSD and the percent predicted forced expiratory volume spirometry abnormalities. The authors performed additional examinations on the mediation effect of trauma exposure and PTSD on the spirometry findings. After including trauma in the models, the association between PTSD and abnormal spirometry no longer retained significance. As noted in the review by Douwes et al30 factors which may have contributed to this inconsistency included the low rate of PTSD in the sample (n=28/1%) as well as the clinical and demographic differences between the subjects with and without PTSD.
Among studies examining community-dwelling samples, there appears to be some evidence of a significant co-occurrence between PTSD and obstructive lung disease more broadly. However, this may not be representative of obstructive lung disease or specifically COPD, particularly when more definitive measures are used (eg, spirometry). In a study involving a clinical sample of primary care patients, Weisberg et al25 examined the relationship between PTSD and somatic complaints. Consistent with findings from treatment-seeking populations, PTSD was found in 37% of the sample. A significant co-occurrence between PTSD and self-reported lung disease was reported. As with several prior studies described above, details regarding how many of these cases actually represented COPD were not discussed.25
Finally, one study was identified that used administrative data to examine patterns of medical comorbidity associated with PTSD. Using medical encounter diagnostic codes to identify PTSD and respiratory system illnesses, the authors reported a 4-year period prevalence of PTSD of 14.3% and a 4-year period prevalence of respiratory system conditions of 51%. The odds of having a respiratory condition based on the presence (vs absence) of PTSD ranged from threefold to sixfold higher depending on comorbid depression.12
In summarizing this particular group of studies, we found inconclusive evidence to support the significant co-occurrence between COPD and PTSD. While some studies report a substantive co-occurrence of PTSD and respiratory illnesses, these reports tend to suffer from an inability to distinguish COPD from respiratory illnesses more broadly. Based on the evidence reviewed above, it is difficult to draw firm conclusions due to the heterogeneity of the published methods, small numbers of cases of PTSD, and the lack of sufficient diagnostic procedures for definitively identifying COPD. Acknowledging the robust evidence base30 between anxiety conditions and asthma, one could conclude that the studies reporting a significant co-occurrence using nonspecific respiratory illness methods (eg, ICD-9 codes for all respiratory conditions) were much more likely to have identified samples predominantly suffering from asthma.
Associations between lower respiratory symptoms and PTSD among WTC survivors
This review revealed a relevant group of studies (n=3) that examined the impact of the events of September 11, 2001. This historic event resulted in a mass population exposure to a traumatic event coupled with a dust cloud characterizing a severe single exposure to a lung irritant. For many community dwellers living in close proximity to the WTC and for first responders, this dust cloud exposure has been linked to a COPD-like illness that has been further classified as WTC cough syndrome. This syndrome shares many specific signs and symptoms with COPD (eg, nonproductive cough, shortness of breath, obstructive spirometry pattern).16,31,32 Among the studies that assessed for PTSD, there were strong positive associations with WTC cough syndrome (further summarized in Table 2). It is important to note, however, the WTC cough syndrome that has emerged largely represents airway dysfunction from one pinpoint exposure to the dust cloud and is likely not representative of the average experience with COPD.
Associations between PTSD and obstructive lung disease outcomes
Several studies reported COPD-related outcomes in relation to PTSD. Outcomes examined included medication adherence, hospital readmission, mortality, COPD severity, quality of life, and response to cardiopulmonary exercise therapy. In our previous study of Veterans with a COPD-related admission, there was a slight but nonsignificant trend toward a positive relationship between PTSD and mortality (odds ratio [OR], 1.19; 0.92–1.55) or readmission (HR, 1.16; 0.96–1.42).18 Other studies provided evidence for PTSD negatively impacting other important outcomes. For example, Jones et al22 reported worse COPD illness burden (measured by the chronic respiratory questionnaire – self report) among patients with PTSD and a lack of response to cardiopulmonary therapy.22 In addition, patients with PTSD have been found to be more likely to skip medications17 and are subject to delays in the delivery of oxygen therapy.23 The finding that PTSD adversely affects adherence was also reported in another study by Kronish et al33 and has been replicated in other populations.34–36 The evidence from this literature base indicates that nonadherence to medications for medical problems is associated with PTSD, acting independent to other mental health conditions. This evidence has important implications for medical outcomes.17 Therefore, it is feasible that poor adherence to COPD treatment contributes to the worse outcomes observed among those with PTSD.
In summary, there is some evidence that PTSD plays a role in the perception of COPD illness burden and subsequent illness management goals (eg, adherence) and treatment response rates. In part, this relationship may well be mediated by tobacco as it is established that individuals suffering from PTSD have higher rates of tobacco abuse.37–39 Unfortunately, in our review of the methods used to capture tobacco use we found a high degree of variability which limited our ability to infer the degree by which tobacco mediated the impact of PTSD on COPD outcomes.
Implications of comorbid COPD and PTSD
As the population ages, COPD prevalence is likely to increase, emphasizing the need for health care systems to recognize patterns of comorbidity associated with COPD. Although there is no firm evidence to support the co-occurrence of COPD and PTSD per se, the evidence supports conclusions that when the two chronic conditions are comorbid, there are important considerations for management. The inconsistencies observed in this review of the literature may be due, in part, to methodological heterogeneity as reflected by differences in case identification, symptom measurement, and sample characteristics. This observation supports the need for more research in this area. However, we do acknowledge that prior research suggests that individuals with anxiety and depressive conditions perceive a greater respiratory symptom burden relative to controls.40
Irrespective of the mixed research findings, it is important that clinicians recognize that evolving medical illnesses represent a point of vulnerability within the mental health of aging adults. It is therefore incumbent upon clinicians to utilize adequate mental health screening approaches to identify anxiety, depression, and trauma exposures until future studies can more definitively address the extant methodological limitations outlined by this review.
Disclosure
The views reflected in this report are those of the authors and do not necessarily reflect the opinions of the Department of Veterans Affairs. The authors report no conflicts of interest in this work.
References
Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. | ||
Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28(3):523–532. | ||
Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006; 27(2):397–412. | ||
Almagro P, Castro A. Helping COPD patients change health behavior in order to improve their quality of life. Int J Chron Obstruct Pulmon Dis. 2013;8:335–345. | ||
Jones RC, Chung MC, Berger Z, Campbell JL. Prevalence of post-traumatic stress disorder in patients with previous myocardial infarction consulting in general practice. Br J Gen Pract. 2007;57(543):808–810. | ||
van Zelst WH, de Beurs E, Beekman AT, Deeg DJ, van Dyck R. Prevalence and risk factors of post-traumatic stress disorder in older adults. Psychother Psychosom. 2003;72(6):333–342. | ||
Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J Trauma Stress. 2013;26(5):537–547. | ||
Boscarino JA. Post-traumatic stress disorder and mortality among US army veterans 30 years after military service. Ann Epidemiol. 2006;16(4):248–256. | ||
Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysis. Chest. 2013;144(3):766–777. | ||
Griffin GD, Charron D, Al-Daccak R. Post-traumatic stress disorder: revisiting adrenergics, glucocorticoids, immune system effects and homeostasis. Clin Transl Immunol. 2014;3(11):e27. | ||
Schnurr PP, Spiro A 3rd, Paris AH. Physician-diagnosed medical disorders in relation to PTSD symptoms in older male military veterans. Health Psychol. 2000;19(1):91–97. | ||
Seng JS, Clark MK, McCarthy AM, Ronis DL. PTSD and physical comorbidity among women receiving Medicaid: results from service-use data. J Trauma Stress. 2006;19(1):45–56. | ||
Spiro A 3rd, Hankin CS, Mansell D, Kazis LE. Post-traumatic stress disorder and health status: the Veterans health study. J Ambul Care Manage. 2006;29(1):71–86. | ||
Spitzer C, Barnow S, Völzke H, John U, Freyberger HJ, Grabe HJ. Trauma, post-traumatic stress disorder, and physical illness: findings from the general population. Psychosom Med. 2009;71(9):1012–1017. | ||
Beckham JC, Moore SD, Feldman ME, Hertzberg MA, Kirby AC, Fairbank JA. Health status, somatization, and severity of post-traumatic stress disorder in Vietnam combat veterans with post-traumatic stress disorder. Am J Psychiatr. 1998;155(11):1565–1569. | ||
Niles JK, Webber MP, Gustave J, et al. Comorbid trends in world trade center cough syndrome and probable post-traumatic stress disorder in firefighters. Chest. 2011;140(5):1146–1154. | ||
Kronish I, Li Y, Edmondson D, Cohen B, et al. Post-traumatic stress disorder (PTSD) is associated with lower medication adherence in US veterans. J Gen Intern Med. 2012;27:S274–S275. | ||
Abrams TE, Vaughan-Sarrazin M, Van der Weg MW. Acute exacerbations of chronic obstructive pulmonary disease and the effect of existing psychiatric comorbidity on subsequent mortality. Psychosomatics. 2011;52(5):441–449. | ||
Felker B, Bush KR, Harel O, Shofer JB, Shores MM, Au DH. Added burden of mental disorders on health status amongpatients with chronic obstructive pulmonary disease. Prim Care Companion J Clin Psychiatr. 2010;12(4):pii:PCC.09m00858. | ||
Boscarino JA. Diseases among men 20 years after exposure to severe stress: implications for clinical research and medical care. Psychosom Med. 1997;59(6):605–614. | ||
Glaesmer H, Brähler E, Gündel H, Riedel-Heller SG. The association of traumatic experiences and post-traumatic stress disorder with physical morbidity in old age – a German population based study. Psychosom Med. 2011;73(5):401–406. | ||
Jones RC, Harding SA, Chung MC, Campbell J. The prevalence of post-traumatic stress disorder in patients undergoing pulmonary rehabilitation and changes in PTSD symptoms following rehabilitation. J Cardiopulm Rehabil Prev. 2009;29(1):49–56. | ||
Trivedi K, Nellaiappan V, Al-Dliw M, Nadeem R. Effect of pre-existing psychiatric illness on home oxygen requirement in COPD patients: a pilot study. Chest. 2013;144(4):738A. | ||
Sareen J, Cox BJ, Stein MB, Afifi TO, Fleet C, Asmundson GJ. Physical and mental comorbidity, disability, and suicidal behavior associated with post-traumatic stress disorder in a large community sample. Psychosom Med. 2007;69(3):242–248. | ||
Weisberg RB, Bruce SE, Machan JT, Kessler RC, Culpepper L, Keller MB. Nonpsychiatric illness among primary care patientswith trauma histories and post-traumatic stress disorder. Psychiatr Serv. 2002;53(7):848–854. | ||
Spitzer C, Koch B, Grabe HJ, et al. Association of airflow limitation with trauma exposure and post-traumatic stress disorder. Eur Respir J. 2011;37(5):1068–1075. | ||
Laurin C, Lavoie KL, Bacon SL, et al. Sex differences in the prevalence of psychiatric disorders and psychological distress in patients with COPD. Chest. 2007;132(1):148–155. | ||
Yellowlees PM, Alpers JH, Bowden JJ, Bryant GD, Ruffin RE. Psychiatric morbidity in patients with chronic airflow obstruction. Med J Aust. 1987;146(6):305–307. | ||
Seal KH, Bertenthal D, Miner CR, Sen S, Marmar C. Bringing the war back home: mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs facilities. Arch Intern Med. 2007;167(5):476–482. | ||
Douwes J, Brooks C, Pearce N. Asthma nervosa: old concept, new insights. Eur Respir J. 2011;37(5):986–990. | ||
Niles AN, Dour HJ, Stanton AL, et al. Anxiety and depressive symptoms and medical illness among adults with anxiety disorders. J Psychosom Res. 2015;78(2):109–115. | ||
Niles JK, Webber MP, Cohen HW, et al. The respiratory pyramid: from symptoms to disease in World Trade Center exposed firefighters. Am J Ind Med. 2013;56(8):870–880. | ||
Kronish IM, Edmondson D, Li Y, Cohen BE. Post-traumatic stress disorder and medication adherence: results from the mind your heart study. J Psychiatr Res. 2012;46(12):1595–1599. | ||
Delahanty DL, Bogart LM, Figler JL. Post-traumatic stress disorder symptoms, salivary cortisol, medication adherence, and CD4 levels in HIV-positive individuals. AIDS Care. 2004;16(2):247–260. | ||
Cavalcanti-Ribeiro P, Andrade-Nascimento M, Morais-de-Jesus M, et al. Post-traumatic stress disorder as a comorbidity: impact on disease outcomes. Expert Rev Neurother. 2012;12(8):1023–1037. | ||
Beckerman NL, Auerbach C. Post-traumatic stress disorder and HIV: a snapshot of co-occurrence. Soc Work Health Care. 2010;49(8):687–702. | ||
Vander Weg MW, Mengeling MA, Booth BM, Torner JC, Sadler AG. Prevalence and correlates of cigarette smoking among operation iraqi freedom-era and operation enduring freedom-era women from the Active Component military and Reserve/National Guard. Med Care. 2015;53(4 Suppl 1):S55–S62. | ||
Beckham JC, Kirby AC, Feldman ME, et al. Prevalence and correlates of heavy smoking in Vietnam veterans with chronic post-traumatic stress disorder. Addict Behav. 1997;22(5):637–647. | ||
Fu SS, McFall M, Saxon AJ, et al. Post-traumatic stress disorder and smoking: a systematic review. Nicotine Tob Res. 2007;9(11): 1071–1084. | ||
Spitzer C, Gläser S, Grabe HJ, et al. Mental health problems, obstructive lung disease and lung function: findings from the general population. J Psychosom Res. 2011;71(3):174–179. | ||
Luft BJ, Schechter C, Kotov R, et al. Exposure, probable PTSD and lower respiratory illness among World Trade Center rescue, recovery and clean-up workers. Psychol Med. 2012;42(5):1069–1079. | ||
Webber MP, Glaser MS, Weakley J, et al. Physician-diagnosed respiratory conditions and mental health symptoms 7–9 years following the World Trade Center disaster. Am J Ind Med. 2011;54(9):661–671. |
Supplementary materials
Ovid MEDLINE(R) in-process and other non-indexed citations and Ovid MEDLINE(R) 1946 to present (run on January 2, 2015, 103 results)
- exp Stress Disorders, Post-Traumatic/
- (PTSD or Posttraumatic Neuroses or Post traumatic Neuroses or Post-traumatic Neuroses or Posttraumatic Stress Disorder* or Post traumatic Stress Disorder*).tw
- exp Combat Disorders/
- (Combat Disorder* or Combat Neurosis or Combat Neuroses or War Neurosis or War Neuroses or Shell Shock* or Combat Stress Disorder*).tw
- 1 or 2 or 3 or 4
- exp Pulmonary Disease, Chronic Obstructive/
- exp asthma/
- (COPD or Chronic Obstructive Pulmonary Disease or COAD or Chronic Obstructive Airway Disease or Chronic Obstructive Lung Disease or Chronic Airflow Obstruction* or Chronic Bronchitis or Emphysema* or Asthma*).tw
- 6 or 7 or 8
- 5 and 9
CINAHL via EBSCO (Run on January 6, 2015, 42 Results)
- (MH “Stress Disorders, Post-Traumatic+”)
- PTSD or “Posttraumatic Neuroses” or “Post traumatic Neuroses” or “Post-traumatic Neuroses” or “Posttraumatic Stress Disorder*” or “Post traumatic Stress Disorder*”
- “Combat Disorder*” or “Combat Neurosis” or “Combat Neuroses” or “War Neurosis” or “War Neuroses” or “Shell Shock*” or “Combat Stress Disorder*”
- S1 OR S2 OR S3
- (MH “Pulmonary Disease, Chronic Obstructive+”)
- (MH “Asthma+”)
- (MH “Emphysema”)
- COPD or “Chronic Obstructive Pulmonary Disease” or COAD or “Chronic Obstructive Airway Disease” or “Chronic Obstructive Lung Disease” or “Chronic Airflow Obstruction*” or “Chronic Bronchitis” or Emphysema* or Asthma*
- S5 OR S6 OR S7 OR S8
- S4 AND S9
Cochrane Library via Wiley (Searched on January 6, 2015, Cochrane Database of Systematic Reviews, 0, Database of Abstracts of Reviews of Effects, 0, CENTRAL 6)
- MeSH descriptor: [Stress Disorders, Post-Traumatic] explode all trees
- PTSD or “Posttraumatic Neuroses” or “Post traumatic Neuroses” or “Post-traumatic Neuroses” or “Posttraumatic Stress Disorder*” or “Post traumatic Stress Disorder*”:ti, ab, kw (Word variations have been searched)
- MeSH descriptor: [Combat Disorders] explode all trees
- “Combat Disorder*” or “Combat Neurosis” or “Combat Neuroses” or “War Neurosis” or “War Neuroses” or “Shell Shock*” or “Combat Stress Disorder*”:ti, ab, kw (Word variations have been searched)
- #1 or #2 or #3
- MeSH descriptor: [Pulmonary Disease, Chronic Obstructive] explode all trees
- MeSH descriptor: [Asthma] explode all trees
- COPD or “Chronic Obstructive Pulmonary Disease” or COAD or “Chronic Obstructive Airway Disease” or “Chronic Obstructive Lung Disease” or “Chronic Airflow Obstruction*” or “Chronic Bronchitis” or Emphysema* or Asthma*:ti, ab, kw (Word variations have been searched)
- #6 or #7 or #8
- #5 and #9
Web of Science (Searched on January 6, 2015, 114 results found)
- PTSD or “Posttraumatic Neuroses” or “Post traumatic Neuroses” or “Post-traumatic Neuroses” or “Posttraumatic Stress Disorder*” or “Post traumatic Stress Disorder*”
- “Combat Disorder*” or “Combat Neurosis” or “Combat Neuroses” or “War Neurosis” or “War Neuroses” or “Shell Shock*” or “Combat Stress Disorder*”
- 1 or 2
- COPD or “Chronic Obstructive Pulmonary Disease” or COAD or “Chronic Obstructive Airway Disease” or “Chronic Obstructive Lung Disease” or “Chronic Airflow Obstruction*” or “Chronic Bronchitis” or Emphysema* or Asthma*
- 3 and 4
Embase (Run on January 6, 2015, 296 results found)
- ‘posttraumatic stress disorder’/exp
- PTSD or “Posttraumatic Neuroses” or “Post traumatic Neuroses” or “Post-traumatic Neuroses” or “Posttraumatic Stress Disorder” or “Post traumatic Stress Disorder” OR “Posttraumatic Stress Disorders” or “Post traumatic Stress Disorders”
- “Combat Disorder” or “Combat Neurosis” or “Combat Neuroses” or “War Neurosis” or “War Neuroses” or “Shell Shock” or “Combat Stress Disorder” OR “Combat Disorders” or “Combat Neurosis” or “Combat Neuroses” or “War Neurosis” or “War Neuroses” or “Shell Shocked” or “Combat Stress Disorders”
- #1 OR #2 OR #3
- ‘chronic obstructive lung disease’/exp
- ‘asthma’/exp
- ‘lung emphysema’/exp
- COPD or “Chronic Obstructive Pulmonary Disease” or COAD or “Chronic Obstructive Airway Disease” or “Chronic Obstructive Lung Disease” or “Chronic Airflow Obstruction” or “Chronic Bronchitis” or Emphysema* or Asthma* or “Chronic Airflow Obstructions” or Emphysemas or Asthmatic OR asthmas
- #5 Or #6 OR #7 OR #8
- #4 AND #9
Clinicaltrials.gov (Run on January 7, 2015, 8 results found)
Searches
COPD OR Chronic Obstructive Pulmonary Disease OR COAD OR Chronic Obstructive Airway Disease OR Chronic Obstructive Lung Disease OR Chronic Airflow Obstruction* OR Chronic Bronchitis OR Emphysema* OR Asthma*
With condition: post traumatic stress disorder
1 result
COPD OR Chronic Obstructive Pulmonary Disease OR COAD OR Chronic Obstructive Airway Disease OR Chronic Obstructive Lung Disease OR Chronic Airflow Obstruction* OR Chronic Bronchitis OR Emphysema* OR Asthma*
With condition: posttraumatic
1 result found
COPD OR Chronic Obstructive Pulmonary Disease OR COAD OR Chronic Obstructive Airway Disease OR Chronic Obstructive Lung Disease OR Chronic Airflow Obstruction* OR Chronic Bronchitis OR Emphysema* OR Asthma*
With condition: combat
0 results
Asthma
With condition: war
0 results
Asthma
With condition: combat
0 results
Asthma
With condition: posttraumatic
3 results
COPD
With condition: war
0 results
COPD
With condition: combat
0 results
COPD
With condition: posttraumatic
0 results
Bronchitis
With condition: war
0 results
Bronchitis
With condition: combat
0 results
Bronchitis
With condition: posttraumatic
0 results
Emphysema
With condition: war
0 results
Emphysema
With condition: combat
0 results
Emphysema
With condition: posttraumatic
0 results
Post traumatic
With condition: asthma
3 results
Post traumatic
With condition: chronic obstructive airway
0 results
Post traumatic
With condition: emphysema
0 results
Post traumatic
With condition: bronchitis
0 results
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.