")
Back to Journals » Journal of Pain Research » Volume 12
Chronic low back pain and postural rehabilitation exercise: a literature review
Authors Paolucci T, Attanasi C , Cecchini W, Marazzi A, Capobianco SV, Santilli V
Received 20 April 2018
Accepted for publication 24 June 2018
Published 20 December 2018 Volume 2019:12 Pages 95—107
DOI https://doi.org/10.2147/JPR.S171729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Teresa Paolucci,1 Carmine Attanasi,1 Walter Cecchini,2 Alessandra Marazzi,2 Serena V Capobianco,1 Valter Santilli1
1Department of Physical Medicine and Rehabilitation, Policlinico Universitario Umberto I, Sapienza University, Rome, Italy; 2Physical Medicine and Rehabilitation Unit, S. Filippo Neri Hospital, Rome, Italy
Abstract: Chronic low back represents one of the major causes of disability worldwide. Our narrative review has the purpose of highlighting the evidence supporting the different rehabilitative techniques described for its management. In total, 26 studies were found suitable to be included in the review (14 articles about pilates, six about McKenzie (MK), one article about Feldenkrais, three about Global Postural Rehabilitation (GPR) and two about Proprioceptive Neuromuscular Facilitation). The effect of exercise therapy was examined for each single study through changes in the main clinical outcomes (pain, disability,) quality of life (QoL) and psychological aspects and the targeted aspects of physical function (muscle strength, mobility, muscular activity and flexibility). All the techniques are effective for the study groups with respect to the control groups in reducing pain and disability and improving the QoL and maintaining benefits at follow-up; pilates, Back School, MK and Feldenkrais methods reduce pain and are more efficient than a pharmacological or instrumental approach in reducing disability and improving all psychological aspects also. GPR shows long lasting results for the last outcome. To date, it is difficult to affirm the superiority of one approach over another. Further high quality research is needed to confirm the effect of these techniques, together with the use of more appropriate evaluation measures.
Keywords: chronic low back pain, aspecific chronic low back pain, McKenzie, Global Postural Rehabilitation, pilates, Feldenkrais, Alexander method, Mézières, Souchard
Introduction
Chronic low back pain (CLBP) is defined as a pain that persists for more than 3 months, or longer than the expected healing period; it represents one of the most common and costly musculoskeletal problems in modern society.2 CLBP is experienced by 70%–80% of adults at some time in their lives.3 Its management comprises a range of different intervention strategies including surgery, drug therapy and non-medical intervention like rehabilitation.
Among alternative rehabilitative techniques, it is known that the behavioral or biopsychosocial approach offers the foundation for a better insight into persistent pain.4
Within rehabilitation approaches to CLBP, the Back School (BS), consisting of training in group exercises, has proven its efficacy in many research studies.5 BS is effective not only in improving the quality of life (QoL) and reducing disability in low back pain (LBP) but also in improving mental well-being.6
In regards to the treatment of CLBP, exercise therapy appears to be slightly effective in decreasing pain and improving function; exercise therapy encompasses heterogeneous interventions, ranging from aerobic exercises to muscle strengthening and flexibility and stretching exercises.7,8
Many techniques can provide an important positive effect on posture through muscle strengthening, flexibility and stretching exercises. Several postural rehabilitation techniques used in CLBP are based on the concept of muscular kinetic chains – such as the Global Postural Rehabilitation method (GPR), while others are based on biomechanical approaches referring to the structure of lumbar intervertebral disc during flexion and extension movements, as the McKenzie method (MK).9,10 Undoubtedly, an abnormal posture which often occurs in patients with CLBP is characterized by mild modifications of the spine curves on the sagittal plane or by the appearance of scoliotic deviations.11,12 Moreover, in postural rehabilitation approaches, great importance is given to the patients’ breathing control and therefore, to the diaphragm muscle.13 Pilates, on the other hand, emphasize the importance of isometric reinforcement of muscles of core stability. Further, one of the aims of pilates is to strengthen and train the core reference muscles for the control of trunk motion in all three planes.14,15 On the other hand, the GPR and Souchard methods do not concentrate on a specific part of the body alone, but treat the whole body in a global way, at the same time granting an active role to the patient who is also a protagonist of his/her own recovery.16
In the approach to reduce of LBP and for an easier management of chronic pain, recent guidelines recommend rehabilitative intervention in CLBP with strong evidence.17–22
Specifically, the guidelines of the American College of Physicians associate good efficacy of Yoga postures, Tai-chi exercises and the pilates method with recommendations of therapeutic exercises; the Nice guidelines also recommend core stability exercises, the MK method, the Feldenkrais method, the hydro-kinesio-therapy and aerobic exercises, while the approach of the Alexander method appears to be of less efficacy in CLBP.17,19 The aim of this narrative review is to provide the efficacy of different postural exercise interventions in reducing pain severity and their impact on function, QoL and healthcare use.
However, despite recommendations in postural exercise guidelines, there are no specific indications for clinicians in the choice of the most suitable postural technique or in the duration and the way of prescription of these exercises.
Materials and methods
A narrative review of the literature was performed using the following search engines: PubMed, Cochrane, Pedro and Scopus.
In order to perform the search, these keywords were used: Chronic Low Back Pain, Aspecific Chronic Low Back Pain AND/OR McKenzie, AND/OR Back School, AND/OR Global Postural rehabilitation, AND/OR GPR, AND/OR pilates, AND/OR Feldenkrais, AND/OR Alexander Method, AND/OR Mézières, AND/OR Souchard.
Inclusion criteria were articles published in the last 5 years, randomized clinical trial, the mean age of patients between 18 and 70 years and full English text. Exclusion criteria were observational studies, case reports and articles without abstract or full text, CAM therapy and different rehabilitative approaches. Articles published between 2012 up to 2017 were included in the research. The flow-diagram showing the selection of studies is given in Figure 1. The outcomes that were used to review included: chronic pain, disability, QoL and psychological aspects.
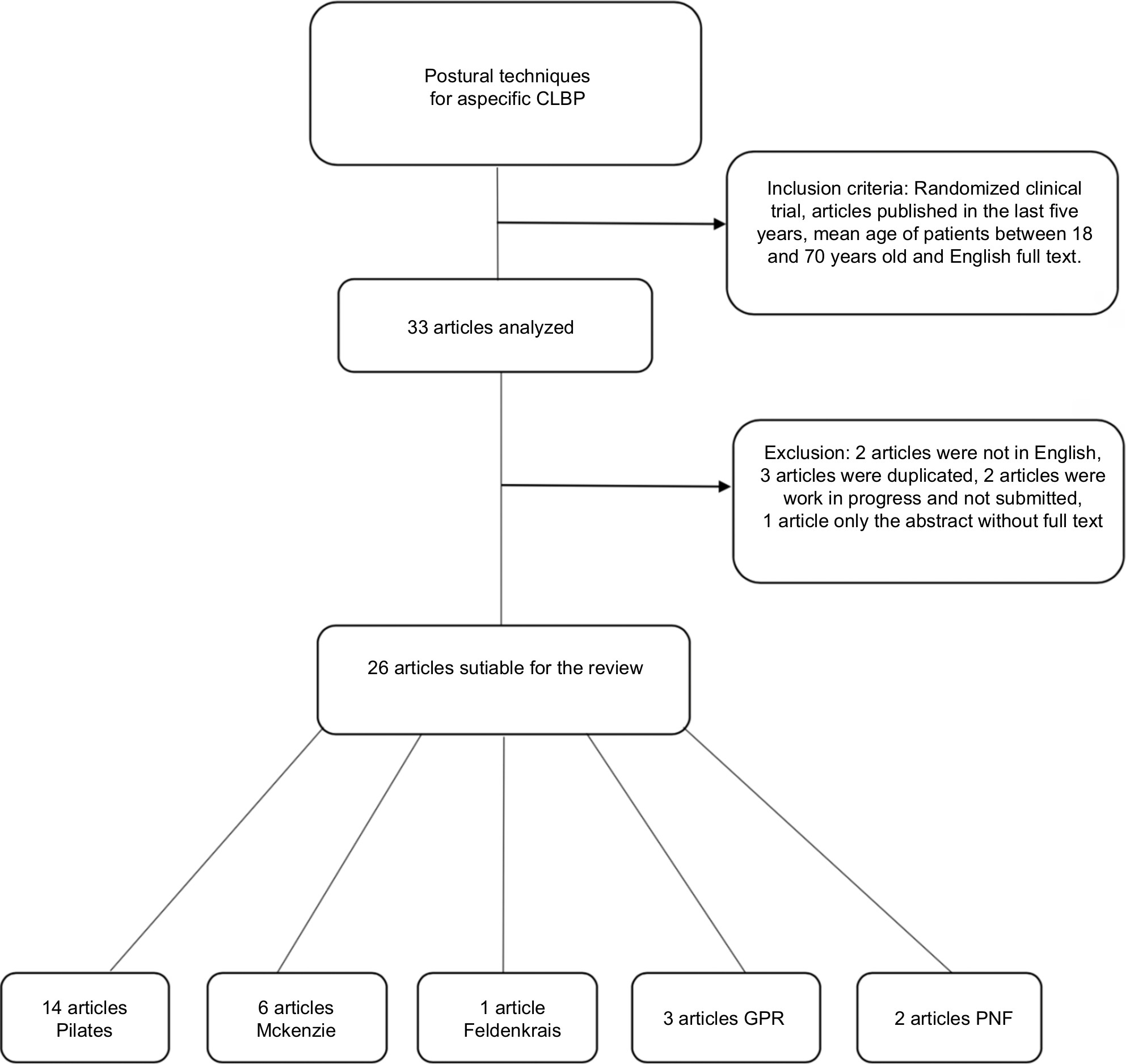 | Figure 1 Flow diagram showing study selection. Abbreviations: CLBP, Chronic low back pain; GRP, global postural rehabilitation; PNF, proprioceptive neuromuscular facilitation. |
Results
In total, 26 articles satisfied the inclusion criteria and were considered in the review: 14 articles on the pilates approach, six articles treating the MK method, three articles about GPR, one article concerning the Feldenkrais technique. In Table 1 a summary of articles included in the search is present, comparing different patient samples, interventions and outcomes in treatment of CLBP.
 | Table 1 Summary of articles comparing different patient samples, interventions and outcomes for the treatment of CLBP Abbreviations: BREF, World Health Organization WHOQOL-BREF Quality of Life; G, group; GPR, global postural rehabilitation; h, hour; HRQOL, Health-Related Quality of Life; ISO, isostretching; MAIA, Multidimensional Assessment of Interoceptive Awareness; MCS, Mental Component Summary; MGPQ, McGill Pain Questionnaire; SF NRS, Short Form Numerical Rating Scale; NSAIDs, nonsteroidal anti-inflammatory drugs; PCS, Physical Component Summary; PIP, proprioceptive neuromuscular facilitation integration pattern; PNF, proprioceptive neuromuscular facilitation; QoL, quality of life; RMDQ, Roland-Morris Disability Questionnaire; RMQ, Roland-Morris Questionnaire; ROM, range of motion; SF-36, Short Form (36) Health Survey; SF-36v2, Short Form Health Survey version-2.0; T, time of evaluation; TENS, transcutaneous electrical nerve stimulation; VAS, visual analog scale. |
Discussion
We have found no article about the Alexander method in the last 5 years. Concerning interventions with effect on proprioception, one article about Proprioceptive Neuromuscular Facilitation Integration Pattern (PIP) and one article about Proprioceptive Neuromuscular Facilitation (PNF) training were included in the review.44,45 No articles about Mézières were found in the research as a therapeutic solution of CLBP.
The results of the analyzed studies were grouped together considering the effects on these outcomes: chronic pain, disability and function, QoL and psychological aspects.
Chronic pain
Chronic pain is the most important symptom of CLBP. Therefore, it is very important to determine how to improve it. The visual analog scale (VAS) and the numerical rating scale (NRS) are the most used scales to define this symptom, but some studies also use the Oswestry Scale, the Quebec Scale and the McGill Pain Questionnaire.
The article by Ali Hasanpour-Dehkordi compares pilates and MK methods. In the MK group, participants performed 1-hour of workouts for 20 days while the pilates group practiced sessions 3 times a week for 6 weeks and both were compared with CGs. After therapeutic exercises, no big difference in pain relief was found between the pilates group and the MK group (P=0.327) but an improvement in pain score was seen in both techniques when compared to the CG.16
In Garcia’s article, the MK method is compared to BS. Exercises were performed once a week for 4 weeks but did not show a significant difference in reducing pain (average effect=0.66 points, 95% confidence interval [CI]=−0.29–1.62).23
In the article by Valenza, pilates, twice a week for 8 weeks, was compared with normal daily living activities plus an informative text; the study showed significant differences in pain in the pilates group.24
In the article by Garcia, two groups were compared; MK group and control group (CG), treated with pulsed ultrasound and short-wave diathermy. Both groups performed two sessions per week for 5 weeks. A better difference of one point was observed in pain intensity in the MK group.25
Mohammad Hosseinifaret compared a MK group and a stabilization-exercises group. Both groups performed training sessions three times per week for 6 weeks. After therapeutic interventions, the pain score decreased in both groups.26
Fernanda Queiroz Ribeiro Cerci Mostagi compared pilates and general exercises; patients were treated with pilates or with general exercises (stretching of the trunk and lumbar muscles, spinal mobilizations, cycling). Both groups performed two sessions per week for 8 weeks. No major differences in pain were found between pilates techniques and general exercises.27
One article by Katherinne Moura Franco evaluated pilates vs physical therapy devices. This trial included an active interferential current group combined with pilates (n=74) and a current interferential group sham addicted to pilates (n=74). These findings suggested that the active interferential current group prior to pilates exercise was not more effective than placebo.28
Gisela C Mijamoto examined the efficacy of modified pilates exercises with training sessions two times a week for 6 weeks. Improvements in pain were observed in pilates group, but these differences were no longer statistically significant at 6 months.29
In the article by Pawel Szulc, 20 participants were divided in three groups, MK group combined with muscle energy technique, MK group and standard exercises group, with each group performing ten sessions. The MK method enriched with muscular energy technique had the best results in reducing pain.30
Jamil Natour considered a CG with patients taking nonsteroidal anti-inflammatory drugs (NSAIDs) and the intervention group (IG) where pilates was used twice a week for 3 months in addition to NSAIDs. Pain improved in the IG also less NSAIDs than the CG.31
In the article by David Cruz Diaz, two groups of Spanish women over 65 were assigned to pilates in addition to standard therapy (n=50) and to standard therapy (transcutaneous electrical nerve stimulation, massage and stretching of the lumbar anatomical region) (n=47) only. Both groups performed two sessions per week for 6 weeks. The pilates group with added standard physiotherapy had better results in pain compared to the standard physiotherapy group measured with VAS.32
Irina Kliziene examined a pilates group (two times a week for 16 weeks) vs a no-IG. Pain was measured with VAS. At the end of the program, pain intensity decreased by 2.01±0.8 (P<0.05) in the pilates group, persisting for 1 month after the end of program.33
Another significant article by U Albert Anand compared 30 patients with modified pilates (modified lateral kick, modified shoulder bridge, swimming, modified swan dive, modified torsion) and another group with standard exercises (bridge pelvic, straight lifting, dynamic strengthening, stationary bicycle and coordination with the Swiss ball). Both groups performed twelve sessions. The results showed that pain and disability appeared much improved in the modified pilates group.34
In the article by Mark H Halliday, the MK method was compared with motor control exercises. Twelve sessions were performed over an 8-week period. No significant differences between the groups were found concerning pain or function (P=0.99 and P=0.26, respectively); the only outcome on behalf of the MK group was the perception of pain.35
The article by Priscila Lawand presents the IG compared with a CG. The IG performed postural exercises using the Souchard method and stretching (12 weeks of treatment+12 without treatment), while the CG did not perform physical intervention but used drugs only. The IG group demonstrated significant improvements (P<0.05) of pain.36
The article by Marta Lúcia Guimarães Resende Adorno evaluated isostretching effectiveness by dividing patients into three groups: isostretching group, GPR group and isostretching group with GPR additionally. All three groups performed training sessions twice a week for 6 weeks. Results indicated that physical therapies were effective in reducing pain (P<0.001); in the isostretching combined with GPR group, pain reduction was significantly greater. Moreover, in the follow-up evaluation, the GPR method was more efficient than other approaches.37
In the study by Chiara Castagnoli, GPR (Souchard) was compared with standard exercises performed twice per week for 8 weeks. This study showed how both groups registered significant improvements, but the GPR group maintained good results even at 1 year follow-up.38
A research by Paolucci Teresa considered Feldenkrais technique vs BS. Both groups performed two weekly sessions for 5 weeks. Both groups experienced significant changes in pain (P<0.001) during follow-up, demonstrating that Feldenkrais method has efficacy comparable to that of BS in improving CLDP.39
The article by David Cruz-Diaz reported the comparison between an IG (pilates) and a CG (no intervention). The pilates group was again divided into two groups: Mat pilates and Equipment-based pilates. Patients performed 12 weeks of training. Both Equipment-based pilates and Mat pilates approaches were more effective than no intervention approach in determining pain improvement.40
In the article by Ardiana Murtezani, the MKmethod was compared with electrophysical agents (EPAs: heat, ultrasound, interferential current). Participants were eligible for treatments in both groups; the first included 134 participants, the second 137. A greater improvement was noticed in the MK group a than in the EPAs group in VAS.41
Furthermore, we analyzed an article by Henry Wajswelner where pilates group and a general exercise group were compared. Both groups performed two training sessions per week for 6 weeks. Results showed that the individual pilates program produced similar benefits in pain scores as benefits gained with standard exercises.42
For Paul WM Marshall, patients were assigned in a group that underwent trunk exercises (stability, strength and flexibility, attention to muscle control, posture and breathing) (n=32) and a group treated with stationary cyclic exercises (Pedal pilates) (n=32)]. Both groups performed sessions three times per week for 8 weeks. Similar reductions in pain perception were observed in both groups at each point of time follow-up.43
In the article of Young et al (2015), a PIP (PNF-applied cross training program) was compared with Swiss ball training with a random allocation in two groups of elderly patients with CLBP pain. The training was performed for 50 minutes per day, three times a week for 6 weeks. Outcomes measured were Balance (mean velocity in the X and Y directions, functional reach test, timed up and go test) and Pain (VAS). The PIP and Swiss ball exercise groups exhibited a significant reduction in the VAS score from prior to after the exercise, but no significant difference between groups was observed. Therefore, PIP showed significant improvements in balance ability and pain for elderly persons with chronic back pain.44
Areeudomwong P et al (2016) have investigated the persistence of the effects of PNF training on pain intensity, functional disability, patient satisfaction, health-related quality of life (HRQOL) and lower back muscle activity in patients with CLBP. All the outcomes were measured before and after the intervention, and at 12 weeks of follow up. Compared to CG, both at 4-weeks and at 12 weeks follow up, PNF patients showed a significant reduction in pain intensity, better results in functional disability, HQoRL and back muscle activity. These findings confirm ythat PNF training provides positive long-term effects on pain-related outcomes and increases lower back muscle activity in patients with CLBP.45
Disability and function
Disability is another main topic of most articles examined; it is most often measured with Roland-Morris Disability Questionnaire and Oswestry Disability Index, and sometimes also with Waddell Disability Index and Patient-Specific Functional Scale.
The study of Maurcio Antonio da Luz showed, at the last follow-up (T2), a significant difference in disability scores (mean value=3.0 points, 95% CI=0.6–5.4), specific disability (mean difference=−1.1 points, 95% CI=−2.0 to −0.1) and fear of moving (average mean=−4.9 points, 95% CI=1.6–8.2) in favor of pilates group.46
In the article of Garcia, the MK group showed a significant improvement to 1-month disability (mean effect=2.37 points, 95% CI=0.76–3.99).25
For Valenza, results showed significant differences in the pilates group regarding scores in disability; Roland-Morris Disability Questionnaire between groups means a difference of 3.2±4.12, P=000.3 and the Oswestry scale improved too (P<0.001).24
In the article by Garcia, difference offour points in Disability in the MK group was observed.25
Katherinne Moura Franco did not find differences between active interferential current prior to exercise of pilates and placebo compared to outcomes evaluated with Roland-Morris Disability Questionnaire in patients with nonspecific CLBP.28
Gisela C Mijamoto noted a disability improvement in modified pilates group, but these differences were no longer statistically significant at 6 months.29
Jamil Natour found that pilates exercises in addition to NSAIDs were found favorable with regard to functional capacity.31
In the article by David Cruz Diaz, results showed that only the group of pilates plus physiotherapy standard improved in fear of falling, functional mobility and balance after treatment.32
U Albert Anand observed that pain and disability appeared much improved in the modified pilates group.34
Priscila Lawand’s article demonstrated that the IG group had significant improvements (P<0.05) in pain and disability to T1.36
In the study by Teresa Paolucci, both groups experienced significant changes in disability (P<0.001) along follow-up.39
In the article by David Cruz-Diaz, a major improvement was observed in the equipment-based pilates group (P=0.007) determining a faster and greater transversus abdominis activation (P<0.001) as well as in pain and disability (P<0.001).40
In the article of Nikolaos Kofotolis et al, the results showed that pilates participants reported greater improvements in disability and an effectiveness maintenance of 3 months.47
In the article by Ardiana Murtezani, a greater improvement was noted in the McKenzie group than in the EPAs group in Oswestry Low Back Pain Disability Questionnaire.41
The article by Henry Wajswelner showed how the individual pilates program produced similar beneficial effects in disability and pain scores when compared to nonspecific exercises.42
QoL and psychological aspects
In the examined articles the importance of QoL and psychological aspects of examination in CLBP are evident. Above all, there are many studies that link CLBP and depression or other aspects that are intimately correlated to pain perception. On the other hand, Marshall et al emphasize on the psychosocial components of pain for complementing and improving the response to physical activity interventions and confirming the fear-avoidance model used to explain the relationship between pain and disability.37
For this reason our search is also focused on QoL (evaluated with HRQOL Scale, Short Form (SF)-36, General Health Questionnaire, World Health Organization QoL -BREF instrument), global perception (evaluated with Global Perceived Effect Scale), specific disability (Patient-Specific Functional Scale), fear of moving (Tampa Scale, Falls efficacy scale-international), function perception (Patient-Specific Functional Scale, Global Perceived Effect questionnaire), Depression symptoms (Beck Inventory Scale) and mental-body interaction (Multidimensional Assessment of Interoceptive Awareness-MAIA).
The research by Maurcio Antonio da Luz Jr. showed, in T2, a significant difference in fear of moving (average mean=−4.9 points, 95% CI=1.6–8.2) in favor of pilates group.46
In the article by Alessandro Narciso Garcia, QoL improved in the MK group more than in the BS group.23
Katherinne Moura Franco did not find any difference between pilates with or without interferential current.
Gisela C Mijamoto examined the efficacy of modified pilates exercises; improvements were also observed in overall impression of recovery in the pilates group measured with Global Perceived Effect Scale and Tampa Scale.28,29
In the article by David Cruz Diaz, results showed that only the pilates group with addition of physiotherapy standard improved in fear of falling.32
In the article by Mark H Halliday, the perceived recovery was slightly higher in the MK group (−0.8; 95% CI: −1.5, −0.1) on a scale of −5 to +5.35
The article by Priscila Lawand demonstrated significant improvements (P<0.05) for pain and disability in the group with GPR approach, improving emotional aspects, limitation in physical functioning, vitality and mental health in SF-36.36
A research by Teresa Paolucci showed how BS and Feldenkrais method had the same efficacy on QoL and Mental-Body interaction.39
In the article of David Cruz Diazonly, the group of pilates with addition of standard physiotherapy improved in the fear of falling.32
In the Nikolaos Kofotolis’ article, the results showed that pilates participants reported greater improvements in HRQOL (P<0.05) compared to participants that did trunk strengthening exercises (G2) or that didn’t perform any exercise (G0). The effects were maintained for 3 months after the end of the program.47
We analyzed the article by Henry Wajswelner where results showed how the individual pilates program produced similar function and QoL improvement compared to patients treated with standard exercises.42
For Paul WM Marshall, both groups (trunk exercises and Pedal pilates) performed sessions three times a week for 8 weeks. Similar reductions in pain perception were observed in both groups at each point of time during follow-up.43
Conclusion
Till date, based on what we know from literature, this is the first recent study that has tried to compare various postural methods. Of course, it must be taken into account as already mentioned, that ours is a narrative review that has not allowed us to statistically weigh the present studies in literature, but only to highlight the state of literature regarding this field.
However, in clinical practice, the results of this study could be useful to clarify which approach is most appropriate in the management of chronic back pain considering the different therapeutic and beneficial effects of the methods discussed.
We conclude that all the analyzed techniques have proved their efficacy with respect to the CG, but it is difficult to affirm the superiority of one approach as compared to another; they are more or less equivalent in reducing pain, reducing disability and improving the QoL. Some of the studies reported in this review included CG of patients who did not perform any rehabilitative treatment;16,19,31,33,40,47 other studies used the patient’s delivery of an information booklet about home-based exercises or ergonomic advices. These research studies concluded about a non-resolution of CLBP in the untreated group, that the natural history of progression of untreated lumbar chronic pain is to remain so with peaks of recurrences and a floating but unresolved pain. We can generally observe that the pilates, the MK method, the Feldenkrais method and BS improve the pain and are more efficient than just a generic, pharmacological or instrumental approach.24–26,30,33,34,36,41 Furthermore, studies using pilates technique have shown a good efficacy in improving chronic pain and physical function. We can also observe the same results in reducing disability and improving all psychological aspects we mentioned related to CLBP. Even GPR, in three articles, has shown very good results in follow-ups at 6 months and up to 1 year.36–38 Furthermore, the Mézières technique should be investigated because there are no randomized clinical trials or studies. Concerning PNF techniques, further investigations are needed in order to confirm their efficacy although results of reported studies are promising because of their multiple effects. Finally, as can be observed in the mentioned studies, BS technique has shown good results in patient education and improving QoL and in managing pain.
We think that further scientific research is needed to strengthen the efficacy of the different techniques and to support an evidence-based approach to CLBP.
Disclosure
The authors report no conflicts of interest in this work.
References
Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009;79(12):1067–1074. | ||
Andersson GB. Epidemiological features of chronic low-back pain. Lancet. 1999;354(91789178):581–585. | ||
Crombez G, Vlaeyen JW, Heuts PH, Lysens R, Crombez G. Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain. 1999;80(1-2):329–339. | ||
Morone G, Paolucci T, Alcuri MR, et al. Quality of life improved by multidisciplinary back school program in patıents with chronic non-specific low back pain: a single blind randomized controlled trial. Eur J Phys Rehabil Med. 2011;47(4):533–541. | ||
Paolucci T, Morone G, Iosa M, et al. Psychological features and outcomes of the Back School treatment in patients with chronic non-specific low back pain. A randomized controlled study. Eur J Phys Rehabil Med. 2012;48(2):245–253. | ||
Henchoz Y, Kai-Lik So A, Henchoz Y. Exercise and nonspecific low back pain: a literature review. Joint Bone Spine. 2008;75(5):533–539. | ||
Hayden JA, Dunn KM, van der Windt DA, Shaw WS. What is the prognosis of back pain? Best Pract Res Clin Rheumatol. 2010;24(2):167–179. | ||
Lawand P, Lombardi Júnior I, Jones A, et al. Effect of a muscle stretching program using the global postural reeducation method for patients with chronic low back pain: A randomized controlled trial. Joint Bone Spine. 2015;82(4):272–277. | ||
Garcìa AN, Costa L, Hancock MJ, et al. McKenzie Method of Mechanical Diagnosis and Therapy was slightly more effective than placebo for pain, but not for disability, in patients with chronic non-specific low back pain: a randomised placebo controlled trial with short and longer term follow-up. Br J Sports Med. 2018;52(9):594–600. | ||
Korovessis P, Stamatakis M, Baikousis A, Korovessis P. Segmental roentgenographic analysis of vertebral inclination on sagittal plane in asymptomatic vs chronic low back pain patients. J Spinal Disord. 1999;12(2):131???137–7. | ||
Ebrahimi S, Kamali F, Razeghi M, Haghpanah SA, Ebrahimi S. Comparison of the trunk-pelvis and lower extremities sagittal plane inter-segmental coordination and variability during walking in persons with and without chronic low back pain. Hum Mov Sci. 2017;52:55–66. | ||
Coelho L. Mézières’ method and muscular chains’ theory: from postural re-education’s physiotherapy to anti-fitness concept. Acta Reumatol Port. 2010;35(3):406–407. | ||
Kamioka H, Tsutani K, Katsumata Y, et al. Effectiveness of Pilates exercise: A quality evaluation and summary of systematic reviews based on randomized controlled trials. Complement Ther Med. 2016;25:1–19. | ||
Moreno MA, Catai AM, Teodori RM, et al. Effect of a muscle stretching program using the Global Postural Reeducation method on respiratory muscle strength and thoracoabdominal mobility of sedentary young males. J Bras Pneumol. 2007;33(6):679–686. | ||
Castagnoli C, Cecchi F, del Canto A, et al. Effects in Short and Long Term of Global Postural Reeducation (GPR) on Chronic Low Back Pain: A Controlled Study with One-Year Follow-Up. ScientificWorldJournal. 2015;2015:1–8. | ||
Hasanpour-Dehkordi A, Dehghani A, Solati K. A Comparison of the Effects of Pilates and McKenzie Training on Pain and General Health in Men with Chronic Low Back Pain: A Randomized Trial. Indian J Palliat Care. 2017;23(1):36–40. | ||
Qaseem A, Wilt TJ, Mclean RM, Forciea MA. Clinical Guidelines Committee of the American College of Physicians. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical PracticeGuideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. | ||
Wong JJ, Côté P, Sutton DA, et al. Clinical practice guidelines for the noninvasive management of low back pain: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur J Pain. 2017;21(2):201–216. | ||
National Institute for Health and Care Excellence. Clinical Guidelines. Low Back Pain and Sciatica in Over 16s: Assessment and Management. National Guideline Centre (UK). London: National Institute for Health and Care Excellence; 2016. | ||
Delitto A, George SZ, van Dillen L, et al. Low Back Pain. Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2012;42(4):A1–57. | ||
Negrini S, Giovannoni S, Minozzi S, et al. Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical guidelines. Eura Medicophys. 2006;42(2):151–170. | ||
Santilli Vet al. Linee guida ed evidenze scientifiche in medicina fisica e riabilitativa. Universit degli Studi di Roma. La Sapienza. 2017:265–298. | ||
Garcia AN, Costa LC, da Silva TM, et al. Effectiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: a randomized controlled trial. Phys Ther. 2013;93(6):729–747. | ||
Valenza MC, Rodríguez-Torres J, Cabrera-Martos I, et al. Results of a Pilates exercise program in patients with chronic non-specific low back pain: a randomized controlled trial. Clin Rehabil. 2017;31(6):753–760. | ||
Garcia AN, Costa LC, Hancock MJ, et al. Efficacy of the McKenzie method in patients with chronic nonspecific low back pain: a protocol of randomized placebo-controlled trial. Phys Ther. 2015;95(2):267–273. | ||
Hosseinifar M, Akbari M, Behtash H, Amiri M, Sarrafzadeh J. The Effects of Stabilization and Mckenzie Exercises on Transverse Abdominis and Multifidus Muscle Thickness, Pain, and Disability: A Randomized Controlled Trial in NonSpecific Chronic Low Back Pain. J Phys Ther Sci. 2013;25(12):1541–1545. | ||
Mostagi FQ, Dias JM, Pereira LM, et al. Pilates versus general exercise effectiveness on pain and functionality in non-specific chronic low back pain subjects. J Bodyw Mov Ther. 2015;19(4):636–645. | ||
Franco KM, Franco YD, Oliveira NB, et al. Is Interferential Current Before Pilates Exercises More Effective Than Placebo in Patients With Chronic Nonspecific Low Back Pain?: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2017;98(2):320–328. | ||
Miyamoto GC, Costa LO, Galvanin T, Cabral CM. Efficacy of the addition of modified Pilates exercises to a minimal intervention in patients with chronic low back pain: a randomized controlled trial. Phys Ther. 2013;93(3):310–320. | ||
Szulc P, Wendt M, Waszak M, et al. Impact of McKenzie Method Therapy Enriched by Muscular Energy Techniques on Subjective and Objective Parameters Related to Spine Function in Patients with Chronic Low Back Pain. Med Sci Monit. 2015;21(21):2918–2932. | ||
Natour J, Cazotti LA, Ribeiro LH, Baptista AS, Jones A. Pilates improves pain, function and quality of life in patients with chronic low back pain: a randomized controlled trial. Clin Rehabil. 2015;29(1):59–68. | ||
Cruz-Díaz D, Martínez-Amat A, de La Torre-Cruz MJ, et al. Effects of a six-week Pilates intervention on balance and fear of falling in women aged over 65 with chronic low-back pain: A randomized controlled trial. Maturitas. 2015;82(4):371–376. | ||
Kliziene I, Sipaviciene S, Vilkiene J, et al. Effects of a 16-week Pilates exercises training program for isometric trunk extension and flexion strength. J Bodyw Mov Ther. 2017;21(1):124–132. | ||
Anand UA, Mariet Caroline P, Arun B, Lakshmi Gomathi G, Albert Anand U. A study to analyse the efficacy of modified Pilates based exercises and therapeutic exercises in individuals with chronic non specific low back pain: a randomized controlled trial. International Journal of Physiotherapy and Research. 2014;2(3):525–529. | ||
Halliday MH, Pappas E, Hancock MJ, et al. A Randomized Controlled Trial Comparing the McKenzie Method to Motor Control Exercises in People With Chronic Low Back Pain and a Directional Preference. J Orthop Sports Phys Ther. 2016;46(7):514–522. | ||
Lawand P, Lombardi Júnior I, Jones A, et al. Effect of a muscle stretching program using the global postural reeducation method for patients with chronic low back pain: A randomized controlled trial. Joint Bone Spine. 2015;82(4):272–277. | ||
Adorno ML, Brasil-Neto JP. Assessment of the quality of life through the SF-36 questionnaire in patients with chronic nonspecific low back pain. Acta Ortop Bras. 2013;21(4):202–207. | ||
Castagnoli C, Cecchi F, del Canto A, et al. Effects in Short and Long Term of Global Postural Reeducation (GPR) on Chronic Low Back Pain: A Controlled Study with One-Year Follow-Up. ScientificWorldJournal. 2015;2015(2):1–8. | ||
Paolucci T, Zangrando F, Iosa M, et al. Improved interoceptive awareness in chronic low back pain: a comparison of Back school versus Feldenkrais method. Disabil Rehabil. 2017;39(10):994–1001. | ||
Cruz-Díaz D, Bergamin M, Gobbo S, Martínez-Amat A, Hita-Contreras F. Comparative effects of 12 weeks of equipment based and mat Pilates in patients with Chronic Low Back Pain on pain, function and transversus abdominis activation. A randomized controlled trial. Complement Ther Med. 2017;33(72-77):72–77. | ||
Murtezani A, Govori V, Meka VS, et al. A comparison of mckenzie therapy with electrophysical agents for the treatment of work related low back pain: A randomized controlled trial. J Back Musculoskelet Rehabil. 2015;28(2):247–253. | ||
Wajswelner H, Metcalf B, Bennell K, Wajswelner H. Clinical pilates versus general exercise for chronic low back pain: randomized trial. Med Sci Sports Exerc. 2012;44(7):1197–1205. | ||
Marshall PW, Kennedy S, Brooks C, Lonsdale C. Pilates exercise or stationary cycling for chronic nonspecific low back pain: does it matter? a randomized controlled trial with 6-month follow-up. Spine. 2013;38(15):E952–959. | ||
Young KJ, Je CW, Hwa ST, Cw J, Hwa St Young KJ. Effect of proprioceptive neuromuscular facilitation integration pattern and swiss ball training on pain and balance in elderly patients with chronic back pain. J Phys Ther Sci. 2015;27(10):3237–3240. | ||
Areeudomwong P, Wongrat W, Neammesri N, Thongsakul T. A randomized controlled trial on the long-term effects of proprioceptive neuromuscular facilitation training, on pain-related outcomes and back muscle activity, in patients with chronic low back pain. Musculoskeletal Care. 2017;15(3):218–229. | ||
da Luz MA, Costa LO, Fuhro FF, et al. Effectiveness of mat Pilates or equipment-based Pilates in patients with chronic non-specific low back pain: a protocol of a randomised controlled trial. BMC Musculoskelet Disord. 2013;14:16. | ||
Kofotolis N, Kellis E, Vlachopoulos SP, Gouitas I, Theodorakis Y. Effects of Pilates and trunk strengthening exercises on health-related quality of life in women with chronic low back pain. J Back Musculoskelet Rehabil. 2016;29(4):649–659. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.