")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 12
Chronic Kidney Disease And Associated Risk Factors Among Cardiovascular Patients
Authors Chala G , Sisay T , Teshome Y
Received 14 July 2019
Accepted for publication 7 September 2019
Published 18 September 2019 Volume 2019:12 Pages 205—211
DOI https://doi.org/10.2147/IJNRD.S223196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Getahun Chala,1 Tariku Sisay,2 Yonas Teshome3
1Department of Medical Physiology, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Biomedical Science, College of Health Sciences, Mizan Tepi University, Mizan, Ethiopia; 3Department of Biomedical Sciences, College of Medicine, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Getahun Chala
Department of Medical Physiology, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Tel +251 25 9 1044 2278
Email [email protected]
Background: Chronic kidney diseases (CKDs) are known in patients with cardiovascular diseases (CVDs) and cause extra morbidity and mortality. There were few related studies in Africa, and no such studies exist in Ethiopia.
Objective: To determine the magnitude of chronic kidney disease and associated risk factors among cardiovascular (CV) patients.
Methods: A cross-sectional study was conducted on randomly selected 163 CV patients attending Tikur-Anbessa Specialized Hospital (TASH), Ethiopia. Estimated glomerular filtration rate (GFR) was determined using the Simplified Modification of Diet in Renal Disease (MDRD) equation. Body weight, height, and blood pressure were recorded, and body mass index (BMI) was calculated. Serum urea and creatinine were analyzed using an automatic analyzer (MINDRAY, BE-2000), and blood urea nitrogen (BUN) was calculated.
Results: In this study, CKD, defined as estimated GFR (eGFR) < 60 mL/min/1.73m2 was found in 39 (23.9%) participants using the MDRD equation. Normal serum creatinine (SCr) was observed in 114 (69.9%) participants and proteinuria was found in 41 (25.2%) participants. CKD was significantly associated with systolic blood pressure (COR: −0.240, 95% CI: −0.439 to −0.041, p = 0.018), SCr (COR: −0.679; 95% CI: −0.778 to −0.580; p = 0.001) and BUN (COR: −0.422; 95% CI: −0.550 to −0.295; p = 0.001). In multivariate analysis, only high SCr (AOR = 47.57; 95% CI: 13.72–164.89; p = 0.001) was independently associated with CKD.
Conclusion: These findings indicated that the CKD was significantly associated with SBP and increased BUN, while independently associated with increased SCr. Thus, early detection and recognition of CKD in-patient with CVD helps to avoid extra morbidity and mortality. We recommend using the MDRD formula in health facilities for diagnosing of CKD to reduce duplication of laboratory tests (SCr and BUN), as it is the easiest practice and saves patients and the public sector costs.
Keywords: chronic kidney disease, cardiovascular disease, estimated glomerular filtration rate, serum creatinine
Introduction
Cardiovascular diseases (CVDs) are a group of disorders of the heart and blood vessels, and the number one cause of death globally.1 Global Burden of Disease study reported in Ethiopia that the mortality in CVD is 18.3% of all deaths in 2016.2 Mainly CVDs are caused by chronic kidney disease (CKD).3–5 Both CVD and kidney disease are closely interconnected and disease of one organ cause dysfunction of the other,6 finally leading to the failure of both organs and this is often referred as a cardiorenal syndrome (CRS).3
CKD is defined as structural or functional abnormalities of the kidney that persist for at least 3 months and is manifested by either kidney damage (most frequently detected as persistent albuminuria or proteinuria (> 30 mg/24h or > 1 on specific dipstick); or a decreased glomerular filtration rate (GFR), (< 60 mL/min per 1.73 m2).7 Early CKD has no sign or symptom,8 this is why CKD usually remains undetected for a longer period until a screening test identifies the silent problem.
CKD is a global health burden with a high economic cost to health systems9,10 and higher among patients with CVD.11,12 The factors underlying the increased prevalence of CKD are the progressive aging, diabetes mellitus, and high blood pressure, most of which are present in patients with CVD.4,13–15 Blood pressure may be viewed as a continuous variable that fluctuates throughout the day and night in CKD and follows a circadian rhythm with a greater prevalence of daytime hypotension and non/reverse dipper status (ie, higher night-time SBP), which are risky for cardiovascular (CV) events.16,17 These fluctuations measured accurately by 24 hr ambulatory blood pressure monitoring, whereas the office blood pressure has some limitations.16,18 Hence, blood pressure control is considered a mainstay for slowing the progressive loss of CKD, as well as to lower the risk of CVDs.16,17,19
All stages of CKD are associated with increased risks of CV morbidity, premature mortality, and decreased quality of life. Additionally, CKD is a major and serious risk factor for CVD.7,20 Death from CVD is 10 to 30 times higher in dialysis patients than in the general population.21 Some studies have confirmed that even early CKD constitutes a significant risk factor for CV events and death.22,23 Besides, proper management of CVD is different and more complex in patients with CKD.24
Although the high prevalence of CKD is known in patients with CVD and cause extra morbidity and mortality,22,23,25,26 very few studies have quantified CKD and associated risk factors among CV patients in Africa, and no such studies exist in Ethiopia. Also, the findings of the study will help as baseline data for further researches in the future.
Materials And Methods
A hospital-based cross-sectional study was conducted on 163 CV patients at the adult emergency department (ED) of Tikur Anbessa Specialized Hospital (TASH), Addis Ababa, Ethiopia for a period of three months (September to November 2017). The study was conducted following the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethics Committee of College of Health Sciences, Tikur-Anbesa, Medical School, Addis Ababa University. Written informed consent was obtained from all subjects before participation and was informed about the confidentiality of the information they gave. Participants, who were included in this study after being screened by clinicians, were older than 18 years and willing to participate. Exclusion criteria were pregnancy, malnourished, participants less than 18 years old and taking creatine dietary supplements.
Sociodemographic and some risk factor variables were collected using a structured questionnaire. Both bodyweight (kg) and height (cm) without shoes and with light clothes were measured by using a beam balance (Seca, GmbH, Germany). BMI (kg/m2) was calculated from weight in kg divided by height in meters squared (m2). Blood pressure was measured using aneroid sphygmomanometer in the right upper arm in the sitting posture after 30 mins rest. An average of two measurements with five minutes gap between measurements was recorded. Systolic blood pressure (SBP) ≥130 mmHg and/or diastolic blood pressure (DBP) ≥ 80 mmHg or current use of blood pressure-lowering medication was used to define hypertension.27
Laboratory Measurements
Five milliliters of the blood sample was collected using a disposable syringe. Serum urea and creatinine were analyzed in the clinical laboratory using an automatic biochemistry analyzer (MINDRAY, BE-2000, CHINA) and urinalysis was done immediately using dipstick dry reagent test strip. The result of 1+ or more was regarded as proteinuria.
An eGFR was calculated separately for men and women using an equation with Modification of Diet in Renal Disease (MDRD):28 GFR (expressed in mL/min/1.73 m2) = 186 × [SCr (mg/dl)] –1.154 × (age) −0.203 × (0.742 if female) × 1.212 (if black). Participants who had eGFR< 60 mL/min/1.73 m2 were advised to have their SCr checkup after a month. CKD was categorized according to the classification system guideline of Kidney Disease Outcomes Quality Initiative (K/DOQI). For the purposes of this study, CKD was defined as stages 3–5 CKD (eGFR < 60 mL/min/1.73 m2): with stage 3A (eGFR 45–59.9), 3B (30–44.9), 4 (15–29.9) and 5 (< 15) mL/min/1.73 m2, respectively.29
Statistical Analysis
Data entry and analysis were done using SPSS software version 22. The descriptive statistics were calculated and categorical variables were expressed as frequencies and percentages. Univariate analysis was used to identify risk factors. Multinomial logistic regression was computed for significant variables (p < 0.05) in the univariate analysis. Adjusted odds ratio (AOR) and their corresponding 95% confidence intervals (CI) were expressed to describe the association of independent variables with CKD (dependent variable). Statistical significance was considered at p < 0.05.
Results
Out of 163 CV patients participated in the study, 91 (55.8%) were females. The mean age of the study participants was 42 ± 18 years with 45 ± 18 for males and 40 ± 17 for females. Out of the total patients, 60 (36.8%) were between 25 and 44 years’ age group and 22 (13.5%) were 65 and above years old, ranging from 18 to 86 years old. One hundred ten (67.5%) patients were married and 51 (31.3%) were illiterate. One hundred thirteen (69.3%) patients were urban residents and 74 (45.4%) earned a monthly income of less than 1000 Ethiopian Birr.
Mean BMI of participants was 21.30 ± 4.05 kg/m2 and 26 (16.0%) participants were overweight with BMI 25–29.9 kg/m2. Mean SBP and DBP were 105 ± 20 and 67 ± 12 mmHg, respectively, and 52 (31.9%) patients had hypertension. Mean BUN was normal with 18.96 ± 12.54 mg/dl while mean SCr was increased with 1.30 ± 0.96 mg/dl. Mean eGFR values according to MDRD equation was indicated stage 2 CKD with 78 ± 30 mL/min/1.73m2. Among patients diagnosed urinalysis, 41 (25.2%) had proteinuria.
Regarding the distribution of CVDs types, chronic rheumatic valvular heart disease (CRVHD) was the most commonly diagnosed which accounted for 75 (46.0%) followed by Deep Vein Thrombosis 32 (19.6%), Ischemic Heart Disease 19 (11.7%), Stroke 14 (8.6%), Hypertension13 (8.0%), Congestive Heart Disease 3 (1.8%), and others (cardiomyopathies and pericardial disease) 7 (4.3%) in this study.
Magnitude Of CKD
A total of 124 (76.1%) patients had a normal renal function (eGFR of ≥ 60 mL/min/1.73m2); 23 (14.1%) patients had stage 3a CKD (eGFR 45–59 mL/min/1.73m2); 8 (4.9%) patients had stage 3b CKD (eGFR 30–44 mL/min/1.73m2); and 6 (3.7%) patients had stage 4 or 5 CKD (eGFR <30 mL/min/1.73m2) using MDRD equation. As shown in Table 1, 39 (23.9%) patients had CKD (defined as eGFR < 60 mL/min/1.73 m2).
 |
Table 1 GFR Category According To K/DOQI Classification Using MDRD Equation Among CV Patients Attending At ED In TASH, Addis Ababa, Ethiopia, 2017 |
Factors Associated With CKD
SBP was significantly associated with CKD (p = 0.023). Although a gender difference in CKD was not significant, it was higher in females compared to males. By age group, older age was not significantly associated with CKD (p = 0.160). CKD was significantly higher among patients with high SCr when compared with low SCr: 21.5% vs 2.5% (p = 0.001). CKD was also significantly higher in patients with high BUN compared with low BUN: 16.6% vs 7.4% (p = 0.001), (Table 2).
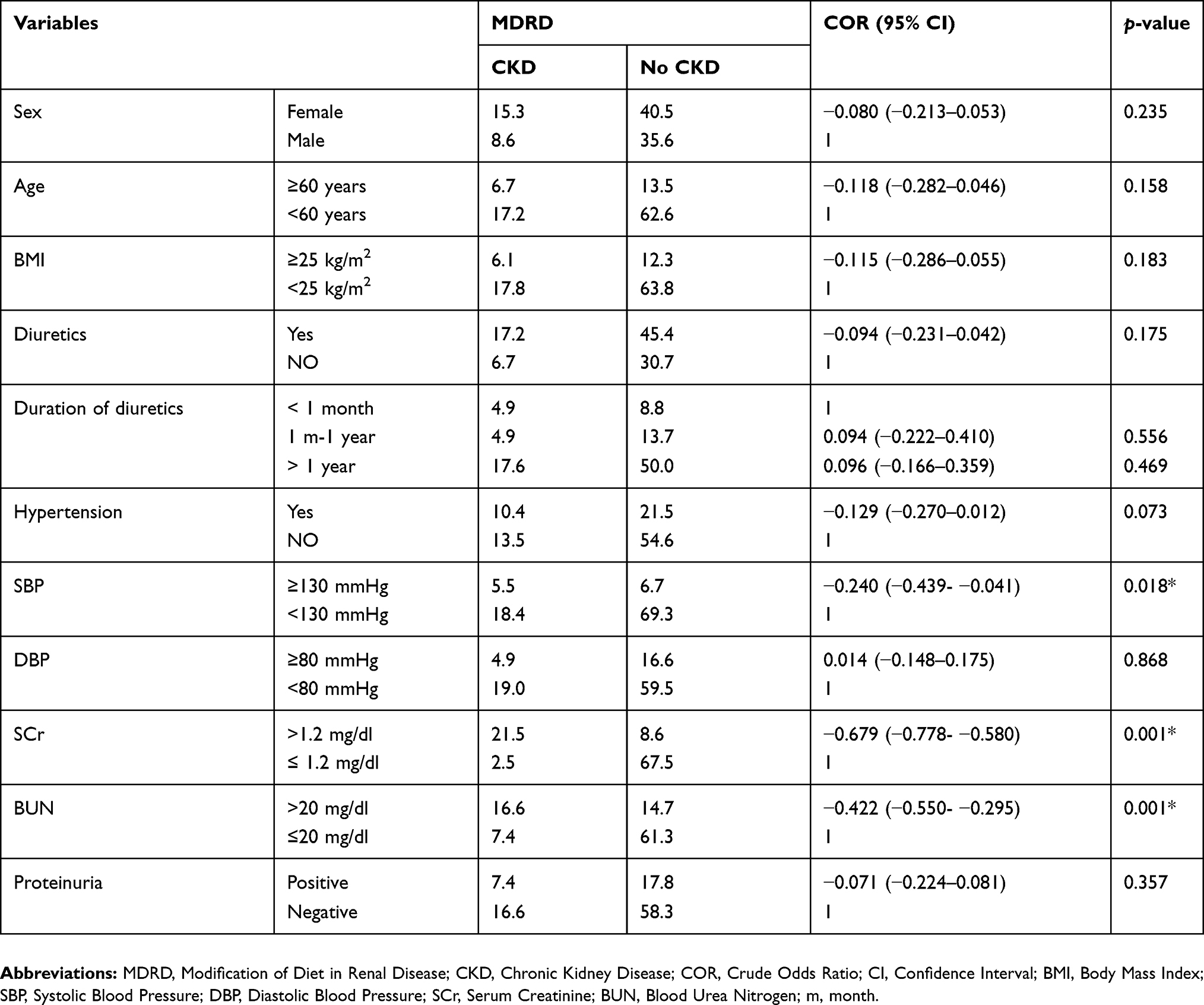 |
Table 2 Distribution Of CKD By Characteristics Of Study Participants Using MDRD Equation Among CV Patients Attending At ED In TASH, Addis Ababa, Ethiopia, 2017 |
The univariate analysis showed a significant association between CKD (eGFR < 60 mL/min/1.73 m2) and the following variables: elevated SBP, high SCr, and high BUN. After incorporating all significant (p < 0.05) variables in the univariate analysis, multivariate logistic regression was computed to identify risk factors independently associated with CKD. In multivariate analysis, only high SCr (AOR = 47.57, CI 13.72–164.89) was independently associated with CKD (Table 3).
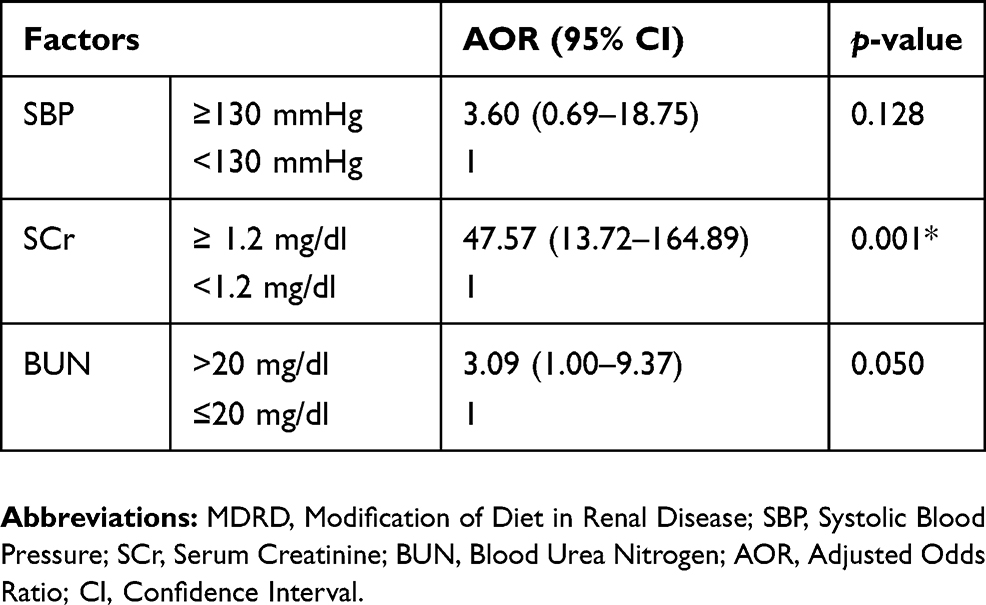 |
Table 3 Factors Associated With CKD According To The MDRD Equation Among CV Patients Attending At ED In TASH, Addis Ababa, Ethiopia, 2017 |
Discussion
Chronic kidney disease (CKD) is a global health burden with a high economic cost to health systems9,10 and higher among patients with CVD.11,12 All stages of CKD are associated with increased risks of CV morbidity, premature mortality, and/or decreased quality of life.7,23,26 Thus, early detection and recognition of CKD are important in patients with CVD to improve adverse outcomes, delay the progression to end-stage renal disease (ESRD) and encourage early referral to the nephrologist.15
In this study, CKD (eGFR < 60 mL/min/1.73 m2) was found in 23.9% of participants based on the MDRD formula used to estimate GFR, with stage 3 being dominant (19.0%). The estimated prevalence of CKD was lower than reported by Amenos et al15 and Yang et al6 These differences might be due to the study design and sample size.
The present study showed that an increase in SCr was independently associated with CKD (p= 0.001). The study done by Pandya et al showed that the serum creatinine is highly statistically significant with CKD.30 Unlike urea, creatinine is not toxic waste, but simply it is used as a marker of renal function. Although the mechanism by which an increase in SCr cause CKD is unidentified, it used to indicate that 50% of GFR had already been lost.31
In this study, BUN showed a highly significant association with CKD defined by MDRD (p = 0.001). This is consistent with the study of Amsalem et al32 Concomitant elevations of BUN implies renal excretory failure, but only at an advanced stage of kidney damage.13 BUN is an imperfect measurement of kidney function and is influenced by factors other than GFR.33 An elevated BUN can further reflect a state of renal hypoperfusion from hypovolemia, renovascular disease, or reduced cardiac output.34,35 BUN may also be raised independently of a change in GFR or SCr due to enhanced urea reabsorption under the activation of the SNS and RAAS.36
Regarding risk factors, this study found an insignificant association between older age and CKD defined by MDRD (p = 0.160). This contradicts with the finding of studies.37,38 This might be due to the small sample size used in our study. In fact, younger people have a higher GFR than older people, which may lead to a late diagnosis of kidney disease. As age increases, there is a gradual decrement in the number of nephrons and GFR. Thus, screening CKD in this age group is an important strategy to improve the outcomes.39
In this study, the self-responsive hypertension was not significantly associated with CKD (p = 0.075) although SBP was significantly associated with CKD defined by MDRD equation (p = 0.023). This contradicts with the finding of Chen et al4 and Amenos et al15 The differences might be due to many patients didn`t know whether they are hypertensive or not and our patients were mainly less than 60 years old. Nowadays, some studies suggest the greater use of antihypertensive medications and specific drug classes such as diuretics, angiotensin converting enzyme inhibitors, and angiotensin II receptor blockers to control blood pressure may affect kidney function independently of their effect on blood pressure.29,40,41 In younger people, there is high early vascular damage and particularly larger artery damage in young ages, which increases hypertension.42,43 The possible relation is that systemic hypertension is passed on to intraglomerular capillary pressure leading to glomerulosclerosis and loss of kidney function.14 Thus, the advantageous effects of controlling blood pressure in CVD has been pronounced repeatedly in current guidelines.27
Although this study is the first time in Ethiopia, it has a few limitations. First, this study was a cross-sectional study, which does not enable those patients with temporary disorders in renal function to be distinguished from those with true CKD. Second, the dipstick provides only a semi-quantitative measurement of proteinuria, relatively insensitive and does not register as positive until total protein excretion is more than 300 mg/day. Third, the influence of other medications and diet were also not taken into consideration during this study. Fourth, we used a routine manual office blood pressure measurement that is on average 9/6 mm Hg higher than standardized blood pressure measurement (24 hr ambulatory blood pressure monitoring).18 Our study also has strengths, including assessing renal function by using eGFR and proteinuria in CVD, since it is not studied and explored in Ethiopia.
Conclusion
This finding indicated that the CKD, which was observed in 23.9% of CV patients, was significantly associated with SBP and increased BUN, while independently associated with increased SCr. Thus, early detection and recognition of CKD using eGFR is essential in patients with CVD to avoid extra morbidity and mortality. We recommend using MDRD formula in hearth facilities for diagnosing of CKD to reduce duplication of laboratory test (SCr and BUN), which is the easiest practice and save costs in patient’s pockets and public sectors.
Abbreviations
BMI, Body Mass Index BUN, Blood Urea Nitrogen; CKD, Chronic Kidney Disease CRS, Cardio-renal Syndrome; CRVHD, Chronic Rheumatic Valvular Heart Disease CV, Cardiovascular; CVD, Cardiovascular Disease DBP, Diastolic Blood Pressure ED, Emergency Department; eGFR, estimated Glomerular Filtration Rate GFR, Glomerular Filtration Rate; KDOQI, Kidney Disease and Quality Outcomes Initiative MDRD, Modification of Diet in Renal Disease; SBP, Systolic Blood Pressure SCr, Serum Creatinine; TASH, Tikur Anbessa Specialized Hospital.
Acknowledgments
We are grateful to and acknowledge Addis Ababa University College of Health Sciences for providing financial assistance for the study. We also like to acknowledge data collectors and administrations of the TASH. Our appreciation also goes to the study participants and all staff of the ED in TASH for their full cooperation during this study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Noncommunicable diseases country profiles. Cardiovascular diseases. 2014. Available from: https://www.who.int/nmh/publications/ncd-profiles-2014/en/. Accessed July 13, 2019.
2. Hannah R, Max R “Causes of Death”. Published online at OurWorldInData.org; 2018. Available from: https://ourworldindata.org/causes-of-death.
3. Liu M, Li X, Lu L, et al. Cardiovascular disease and its relationship with chronic kidney disease. Eur Rev Med Pharmacol Sci. 2014;18(19):2918–2926.
4. Chen Q, Zhang Y, Ding D, et al. Estimated glomerular filtration rate and mortality among patients with coronary heart disease. PLoS One. 2016;11(8):e0161599. doi:10.1371/journal.pone.0161599
5. Yuan J, Zou X-R, Han S-P, et al. Prevalence and risk factors for cardiovascular disease among chronic kidney disease patients: results from the Chinese cohort study of chronic kidney disease (C-STRIDE). BMC Nephrol. 2017;18(1):23. doi:10.1186/s12882-017-0669-4
6. Yang J-G, Li J, Lu C, Hasimu B, Yang Y, Hu D. Chronic kidney disease, all-cause mortality and cardiovascular mortality among Chinese patients with established cardiovascular. J Atheroscler Thromb. 2010;17(4):395–401. doi:10.5551/jat.3061
7. Brosius FC, Hostetter TH, Kelepouris E, et al. REPRINT detection of chronic kidney disease in patients with or at increased risk of cardiovascular disease. Hypertension. 2006;48(4):751–755. doi:10.1161/CIRCULATIONAHA.106.177321
8. Tamadon MR, Zahmatkesh M. World kidney day 2015. J Parathyr Dis. 2015;3(2):34–36.
9. Teruel JLG, Catalán SB. Assessment of renal function, iatrogenic hyperkalemia and acute renal dysfunction in cardiology. Contrast-induced nephropathy. Revista Española De Cardiología (english Edition). 2011;64(12):1182–1192. doi:10.1016/j.rec.2011.08.012
10. Goyal A, Chatterjee K, Yadlapati S, Rangaswami J. Impact of end-stage kidney disease on costs and outcomes of clostridium difficile infection. Int J Infect Dis. 2017;62:8–9. doi:10.1016/j.ijid.2017.06.013
11. Liu J-H, Lin S-Y, Hsu C-Y, et al. The risk for chronic kidney disease in patients with heart diseases: a 7-year follow-up in a cohort study in Taiwan. BMC Nephrol. 2012;13(1):77. doi:10.1186/1471-2369-13-77
12. Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for the development of the cardiovascular disease. Circulation. 2003;108(17):2154–2169. doi:10.1161/01.CIR.0000095676.90936.80
13. Akanda M, Choudhury K, Ali M, Kabir M, Begum L, Sayami L. Serum creatinine and blood urea nitrogen levels in patients with coronary artery disease. Cardiovasc J. 2013;5(2):141–145. doi:10.3329/cardio.v5i2.14282
14. Kazancioğlu R. Risk factors for chronic kidney disease: an update. Kidney Int Suppl. 2013;3(4):368–371. doi:10.1038/kisup.2013.79
15. Amenós AC, González-Juanatey JR, Gutiérrez PC, Gilarranz AM, Costa CG. Prevalence of chronic kidney disease in patients with or at a high risk of cardiovascular disease. Revista Espanola De Cardiologia (english Edition). 2010;2(63):225–228.
16. Di Daniele N, Fegatelli DA, Rovella V, Castagnola V, Gabriele M, Scuteri A. Circadian blood pressure patterns and blood pressure control in patients with chronic kidney disease. Atherosclerosis. 2017;267:139–145. doi:10.1016/j.atherosclerosis.2017.10.031
17. Mezue K, Goyal A, Pressman GS, Horrow JC, Rangaswami J. Blood pressure variability predicts adverse events and cardiovascular outcomes in chronic kidney disease: a posthoc analysis of the SPRINT trial. Am J Hypertens. 2017;31(1):48–52. doi:10.1093/ajh/hpx128
18. Myers MG, Kaczorowski J, Dawes M, Godwin M. Automated office blood pressure measurement in primary care. Can Fam Physician. 2014;60(2):127–132.
19. Rossignol P, Massy ZA, Azizi M, et al. The double challenge of resistant hypertension and chronic kidney disease. Lancet. 2015;386(10003):1588–1598. doi:10.1016/S0140-6736(15)00418-3
20. Briasoulis A, Bakris GL. Chronic kidney disease as a coronary artery disease risk equivalent. Curr Cardiol Rep. 2013;15(3):340. doi:10.1007/s11886-012-0340-4
21. Sarnak MJ. Cardiovascular complications in chronic kidney disease. Am J Kidney Dis. 2003;41:11–17. doi:10.1016/s0272-6386(03)00372-x
22. Health NIo. Kidney Disease Statistics for the United States. Washington: NHI; 2012.
23. Anavekar NS, McMurray JJ, Velazquez EJ, et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med. 2004;351(13):1285–1295. doi:10.1056/NEJMoa041365
24. Gupta R, Birnbaum Y, Uretsky BF. The renal patient with coronary artery disease: current concepts and dilemmas. J Am Coll Cardiol. 2004;44(7):1343–1353. doi:10.1016/j.jacc.2004.06.058
25. Kughapriya PPD, Evangeline J. Evaluation of serum electrolytes in ischemic heart disease patients. Natl J Basic Med Sci. 2016;6(4).
26. Wang X, Wang Y, Wang C, et al. Association between Estimated Glomerular Filtration Rate and Clinical Outcomes in Patients with Acute Ischaemic Stroke: Results from China National Stroke Registry. Vol. 43. Oxford University Press; 2014:839–845
27. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(6):1269–1324.
28. Levey AS, Coresh J, Greene T, et al. Expressing the modification of diet in renal disease study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin Chem. 2007;53(4):766–772. doi:10.1373/clinchem.2006.077180
29. Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713–735. doi:10.1053/j.ajkd.2014.01.416
30. Pandya D, Nagrajappa AK, Ravi K. Assessment and correlation of urea and creatinine levels in saliva and serum of patients with chronic kidney disease, diabetes, and hypertension–a research study. J Clin Diagn Res. 2016;10(10):ZC58.
31. Dalton RN. Serum creatinine and glomerular filtration rate: perception and reality. J Bras Patol Med Lab. 2011;47(1):08–11. doi:10.1590/S1676-24442011000100001
32. Amsalem Y, Garty M, Schwartz R, et al. Prevalence and significance of unrecognized renal insufficiency in patients with heart failure. Eur Heart J. 2008;29(8):1029–1036. doi:10.1093/eurheartj/ehn102
33. Rosner MH, Bolton WK. Renal function testing. Am J Kidney Dis. 2006;47(1):174–183. doi:10.1053/j.ajkd.2005.08.038
34. Aronson D, Mittleman MA, Burger AJ. Elevated blood urea nitrogen level as a predictor of mortality in patients admitted for decompensated heart failure. Am J Med. 2004;116(7):466–473. doi:10.1016/j.amjmed.2003.11.014
35. Dal AC, Fuiano G, Conte G, et al. Mechanism of increased plasma urea after diuretic therapy in uraemic patients. Clin Sci (Lond). 1985;68(3):255–261. doi:10.1042/cs0680255
36. Kirtane AJ, Leder DM, Waikar SS, et al. Serum blood urea nitrogen as an independent marker of subsequent mortality among patients with acute coronary syndromes and normal to mildly reduced glomerular filtration rates. J Am Coll Cardiol. 2005;45(11):1781–1786. doi:10.1016/j.jacc.2005.02.068
37. Wagner M, Wanner C, Kotseva K, et al. Prevalence of chronic kidney disease and its determinants in coronary heart disease patients in 24 European countries: insights from the EUROASPIRE IV survey of the European Society of Cardiology. Eur J Prev Cardiol. 2017;24(11):1168–1180. doi:10.1177/2047487317708891
38. Löfman I, Szummer K, Hagerman I, Dahlström U, Lund LH, Jernberg T. Prevalence and prognostic impact of kidney disease on heart failure patients. Open Heart. 2016;3(1):e000324. doi:10.1136/openhrt-2015-000324
39. Ghonemy TA, Salim EM, Soliman SA, Allam HM. Reduced glomerular filtration rate as a predictor of coronary artery disease events in elderly patients. Alexandria J Med. 2017;53(3):221–225. doi:10.1016/j.ajme.2016.06.006
40. Group SR. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–2116. doi:10.1056/NEJMoa1511939
41. Tomlinson LA, Abel GA, Chaudhry AN, et al. ACE inhibitor and angiotensin receptor-II antagonist prescribing and hospital admissions with acute kidney injury: a longitudinal ecological study. PLoS One. 2013;8(11):e78465. doi:10.1371/journal.pone.0078465
42. Nilsson PM, Laurent S, Cunha PG, et al. Characteristics of healthy vascular aging in pooled population-based cohort studies: the global metabolic syndrome and artery research consortium. J Hypertens. 2018;36(12):2340–2349. doi:10.1097/HJH.0000000000001824
43. Cunha PG, Cotter J, Oliveira P, et al. Pulse wave velocity distribution in a cohort study: from arterial stiffness to early vascular aging. J Hypertens. 2015;33(7):1438–1445. doi:10.1097/HJH.0000000000000565
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.