")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Chronic Kidney Disease and Associated Factors Among HIV/AIDS Patients on HAART in Ethiopia
Authors Manaye GA , Abateneh DD , Niguse W
Received 26 August 2020
Accepted for publication 30 September 2020
Published 19 October 2020 Volume 2020:12 Pages 591—599
DOI https://doi.org/10.2147/HIV.S276356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Gizachew Ayele Manaye,1 Dejene Derseh Abateneh,2 Wondwossen Niguse3
1Department of Medical Laboratory Science, College of Medicine and Health Sciences, Mizan-Tepi University, Mizan Teferi, Ethiopia; 2Department of Medical Laboratory Science, Menelik II College of Medicine and Health Sciences, Kotebe Metropolitan University, Addis Ababa, Ethiopia; 3Department of Nursing, College of Medicine and Health Sciences, Mizan-Tepi University, Mizan Teferi, Ethiopia
Correspondence: Gizachew Ayele Manaye
Department of Medical Laboratory Science, College of Medicine and Health Sciences, Mizan-Tepi University, P.O. Box: 206, Mizan Tefri, Ethiopia
Tel +251928444333
Email [email protected]
Background: In developing countries, both opportunistic infections and chronic diseases account a high HIV-associated mortality and morbidity. Chronic kidney disease (CKD) associated with HIV infection has got increased attention in sub-Saharan Africa as a result of the high HIV prevalence and due to the late diagnosis and initiation of HAART. Thus, this study was conducted to assess CKD and associated factors among HIV patients on HAART in Ethiopia.
Methods: A hospital-based cross-sectional study with a secondary data review was conducted on 336 on HIV/AIDS patients on HAART from February to July 2017 at University of Gondar Referral Hospital. The study participants were selected using a systematic random sampling technique. Socio-demographic and clinical data were collected using a semi-structured questionnaire at their follow-up date with interview and chart review. Three to five milliliters of venous blood and five milliliters of urine specimen were collected for serum creatinine and urine albumin determination, respectively. Data were entered into SPSS version 20 for analysis. Glomerular filtration rate was estimated using the CKD-EPI estimator. Bivariate and multivariate logistic regression was employed and p-value < 0.2 and < 0.05, respectively, was considered statistically significant.
Results: The prevalence of CKD on the study participants was 54 (16.1%) (95% CI, 12.2– 20.4%). By stage, about 27 (8.0%) had stage 1 (persistent proteinuria with eGFR ≥ 90 mL/min/1.73 m2), 16 (4.8%) had stage 2 (persistent proteinuria with eGFR of 60– 89.9 mL/min/1.73 m2), 6 (1.8%) had stage 3 (eGFR 30– 59.9 mL/min/1.73 m2 with or without proteinuria) and 5 (1.5%) had stage 5 ((kidney failure), eGFR< 15mL/min/1.73 m2 with or without proteinuria). With multivariate logistic regression analysis, being male (AOR=2.05 (1.03– 4.09), p=0.04), being merchant (AOR=2.91 (1.00– 8.48), p=0.049) and having viral load≥ 1000 copies/mm3 (AOR=3.1 (1.38– 7.00), P< 0.01) were significantly associated with CKD.
Conclusion: The prevalence of CKD among HIV patients on HARRT is high. Being male, merchant and having viral load ≥ 1000 copies/mm3 were associated factors of CKD. Patients should be regularly monitored and screened for early diagnosis and management of CKD. Those patients who have being merchant with high viral load and male patients should require close monitoring.
Keywords: chronic kidney disease, HIV/AIDS, HAART, Ethiopia
Background
Globally, an estimated 36.7 million people were living with Human immunodeficiency virus (HIV) in 2016. The majority of people living with HIV are in sub-Saharan Africa. In the era of combined antiretroviral therapy, the life expectancy of people living with HIV (PLWH) has increased.1–3 With longer life spans, however, PLWH is developing chronic medical conditions.4–6 The morbidity and mortality associated with HIV infection were due to opportunistic infections. However, in developed countries, opportunistic infections have been replaced by chronic diseases. Whereas in developing countries like Ethiopia, both the opportunistic infections and chronic diseases account a high HIV-associated mortality and morbidity.7 One of the most commonly diagnosed chronic diseases is chronic kidney disease (CKD).8–10 Chronic kidney disease is defined as kidney damage or reduced kidney function that persists for more than 3 months.11,12
Chronic kidney diseases associated with HIV infection have got increased attention in sub-Saharan Africa as a result of the high HIV prevalence and due to the late HIV diagnosis and late initiation of highly active antiretroviral therapy (HAART) before the recommendation of initiation of HAART for any person diagnosed with HIV. A research finding showed an increasing prevalence of kidney disease in PLWH compared with the general population, being related to increased mortality and morbidity.13–15 HIV-infected patients are five times more likely to develop kidney disease as compared to HIV non-infected.16 A recent systematic review and meta-analysis in sub-Saharan Africa reported a 6.42% prevalence of CKD among HIV patients in which the majority of them were in stage 3 CKD.17 Chronic kidney disease prevalence is increasing globally and recognized as a global public health problem with a major impact on health, healthcare costs and productivity.11,18,19 The involved factors related to increasing the prevalence of kidney disease in PLWH were a direct effect of the virus itself, closely related to the immune status; prolonged use of antiretroviral therapy (tenofovir, indinavir, and others); frequent use of concomitant therapy with nephrotoxic drugs; an increase of comorbidities such as diabetes mellitus, dyslipidemia, and hypertension; high prevalence of co-infection with hepatitis B and C virus compared with the general population.20–26
Ethiopia is one of the countries where the majority of CKD cases among the general population and high-risk groups such as peoples living with HIV patients have limited data in consequence of underdiagnosing. Hence, this study was conducted to assess CKD among HIV patients on HAART in Ethiopia.
Materials and Methods
Aim
The aim of this study was to assess the prevalence of CKD among HIV/AIDS patients and its associated factors.
Study Area, Design, and Population
A hospital-based cross-sectional study was conducted from February 01 to July 30, 2017, at the University of Gondar Referral Hospital (UOGRH), which is located in the North Gondar zone, 747 km from the capital city of the country, Addis Ababa. Gondar has an estimated population of more than 206,987 (98,085 males and 108,902 females) based on the 2008 central statistical agency data. Currently, 13,753 HIV patients and 5389 on ART patients are attending at the University of Gondar Referral Hospital.
Adult HIV/AIDS patients who received HAART in UOGRH were the study population. Those adult HIV/AIDS patients, who received HAART for more than 6 months, visited UOGRH during the study period and consented to be involved in the study were included. But patients who were seriously sick and unable to give response, diabetic, and hypertension were excluded from the study. In addition, patients with incomplete laboratory and clinical data such as baseline adherence, baseline drug regimen, HIV/AIDS WHO stage, weight, etc. were excluded from the study too.
Sample Size Determination and Sampling Technique
Based on single population formula and systematic random sampling technique with the following assumption, P = population proportion (estimated prevalence) = 0.5 to yield maximum sample size, precision d, 0.05, by assuming 95% confidence interval α = 0.05 and z (1-a/2) = 1.96 was used for sample size determination. Including 10% non-response rate, the final sample size was 423. However, a total of 336 HIV patients on HAART participated in the study (Figure 1).
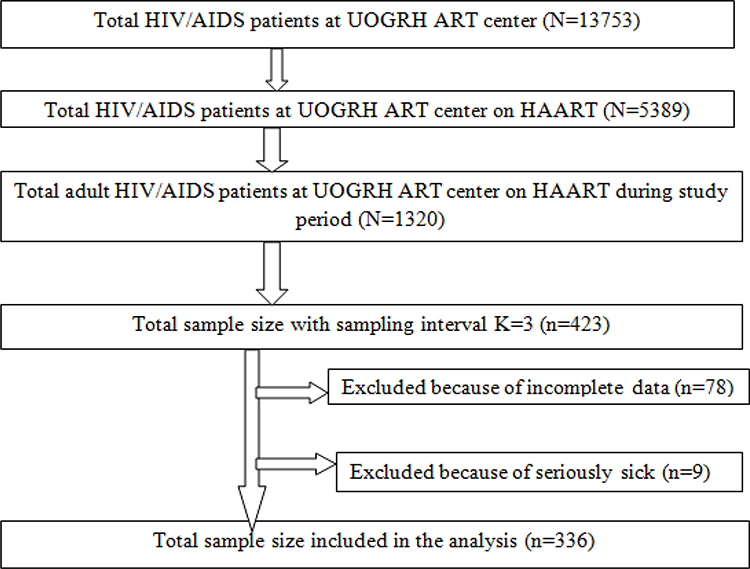 |
Figure 1 Schematic representation of the sampling procedure adult HIV/AIDS patients on HARRT at University of Gondar Referral Hospital from February to April 2017. |
During the three-month data collection period, 1320 HIV/AIDS patients on HAART (> 6 months) were expected to visit the hospital for follow-up. The average number of HIV/AIDS patients per day under follow-up was 20.Sampling intervals (K value) was calculated with 1320/423 = 3.12 = 3. Thus interviews, chart review and blood and urine specimen collection for chemistry analysis and urine dipstick were conducted at three intervals. To determine the first-person, the lottery method was used on first day from the 20 patients who had under follow-up. Then, each third client was selected for an interview, chart review and blood chemistry and urine dipstick test. If the third patient is not fulfilling the inclusion criteria; the next person was taken as a study subject.
Data Collection and Laboratory Methods
Socio-demographic characteristics and clinical data were collected by trained nurses using a semi-structured questionnaire. The patient individual was interviewed and the chart was also reviewed for relevant information. Variables included age, gender, residence, education, occupation, viral load, CD4 count, co-infections, base line CD4+ count, regimen type, WHO stage, duration of follow-up time, etc.
About 3–5mL of venous blood with serum (gel) separator tube and 5mL of urine specimen using clean, dry and leak-proof urine cup were collected from the patients for creatinine and urine albumin level determination, respectively. For creatinine determination, a serum sample was immediately separated from the collected venous blood after the blood sample clotted and centrifuged at 1000–2000g for 10 mins. The separated serum was transferred to a nunc tube and kept frozen at −20 ºC until processed. A serum creatinine level was determined by kinetic Jaffe reaction using Mindray BS-200 chemistry analyzer (Shenzhen Mindray Bio-Medical Electronics Co. Ltd, China) and reported in mg/dL. Chemical analysis of urine specimens for urine albumin level determination was performed immediately after the sample collection using urine dipsticks test (Multistix® Henry Schein, Inc. https://www.henryschein.com/medical-multistix.aspx). Urine albumin level was reported semi-quantitatively as negative, or +1, to +4. All the participants with positive urine albumin and creatinine above the normal range (0.6 to 1.2 milligrams (mg) per deciliter (dl) in adult males and 0.5 to 1.1 mg per deciliter in adult females) were also checked their serum creatinine level and urine albumin for a second time after 3 months of the first check-up for confirmation of CKD. Glomerular filtration rate (GFR) was estimated using CKD-EPI question.27
Chronic kidney disease was defined using the average of the two consecutive creatinine eGFR and presence of urine albumin and classified into five stages according to the classification of Kidney Disease Improving Global Outcomes (KDIGO).28
Variables’ Definition
Chronic kidney disease is defined as abnormalities of kidney structure or function, present for ≥3 months and evaluated by at least two measurements, with implications for health and CKD is classified based on cause, GFR category, and proteinuria category.29
- Persistent proteinuria, a positive urine albumen is positive too after 3 months of screening
- Stage 1, persistent proteinuria with eGFR ≥ 90 mL/min/1.73 m2
- Stage 2, persistent proteinuria with eGFR of 60–89.9 mL/min/1.73 m2
- Stage 3, eGFR 30–59.9 mL/min/1.73 m2 with or without proteinuria
- 3A (eGFR 45–59.9mL/min/1.73 m2)
- 3B (eGFR 30–44.9mL/min/1.73 m2)
- Stage 4, eGFR 15–29.9 mL/min/1.73 m2 with or without proteinuria
- Stage 5, (kidney failure), eGFR<15mL/min/1.73 m2 with or without proteinuria.
HAART experienced: taking HAART for more than 6 months which is composed of two NRTIs plus an NNRTI.30
Underweight, normal weight, overweight and obesity were defined as a BMI <18.5 kg/m2, 18.5–24.9 kg/m2, 25–29.9 kg/m2 and ≥30 kg/m2, respectively.31
Hypertension: defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg or taking medication for blood pressure-lowering.32
Adherence: adherence was calculated as No. of the dose of HAART taken/No. of prescribed doses of HAART x 100%. Good adherence, >95%, fair adherence, 85–95% and poor adherence, < 85% doses take.33,34
Data Processing and Analysis
The completeness of the data was checked and entered into SPSS version 20 for analysis. During analysis, descriptive statistics such as percentage, mean and standard deviation were used. Bivariate logistic regression was used to assess the crude association between independent and dependent variables, and with p-value ≤ 0.20 were considered for multivariate logistic regression. Finally, logistic regression was used to identify independent predictors of CKD and p-value < 0.05 was considered statistically significant.
Results
Socio-Demographic Characteristics
A total of 336 HIV/AIDS patients who received HAART were enrolled in the study. Of these, 215 (64%) of them were females and 121 (36%) were males. The mean (SD) age of the participants was 39.7 (±9.7) years, range 18–69 years. One hundred thirty-three (39.6%) of the study participants were within the age group of 30–39 years. At the time of study almost half of the patients, 170 (50.6%) were married and 263 (78.3%) were living in urban areas. Three hundred five (90.8%) were followers of orthodox religion (Table 1).
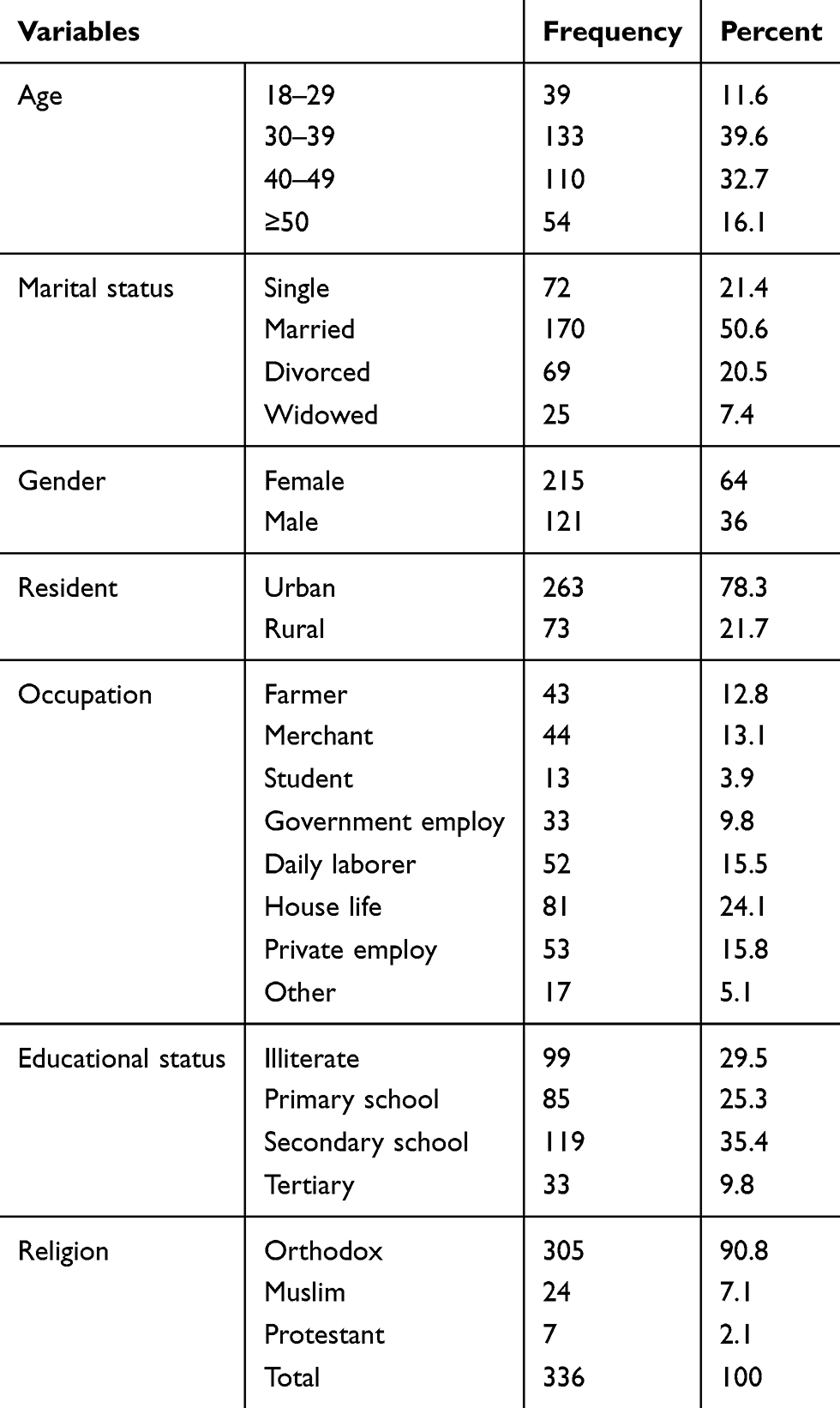 |
Table 1 Socio-Demographic Characteristics of HIV/AIDS Patients on HARRT at the University of Gondar Referral Hospital, 2017 |
Clinical Characteristics of HIV/AIDS Patients
The study patients were on ART with a minimum of 1 up to 12 years with an average time of 7.5 (± 3) years. Before ART initiation majority of patients had WHO clinical stage II and III, 251 (74.7%), CD4+T cell count < 200 cells/mm3, 221 (65.8%), good adherence 321 (95.5%) and on AZT +3TC+NVP 121 (36%) regimen followed by TDF+3TC+EFV 62 (18.5%).
Majority of study participants, 326 (97%) were on WHO clinical stage I, 28 (8.3%) had CD4+T count <200 cells/mm3, 333 (99.1%) had good adherence and 126 (37.5%) switched to first-line or second-line regimen, 11 (3.3%). The most common reason for switching was toxicity, 93 (27.7%) followed by clinical failure, 17 (5.1%). The common opportunistic infections observed during their ART follow-up were TB,77 (22.9%). The mean plasma viral load level was 6023.46 copies/mL (range 0–245,754.00 copies/mL). Among all the study participants, 27 (8.0%), 16 (4.8%), 6 (1.8%) and 5 (1.5%) of patients during follow-up were stage I, stage II, stage III and stage V, respectively (Table 2).
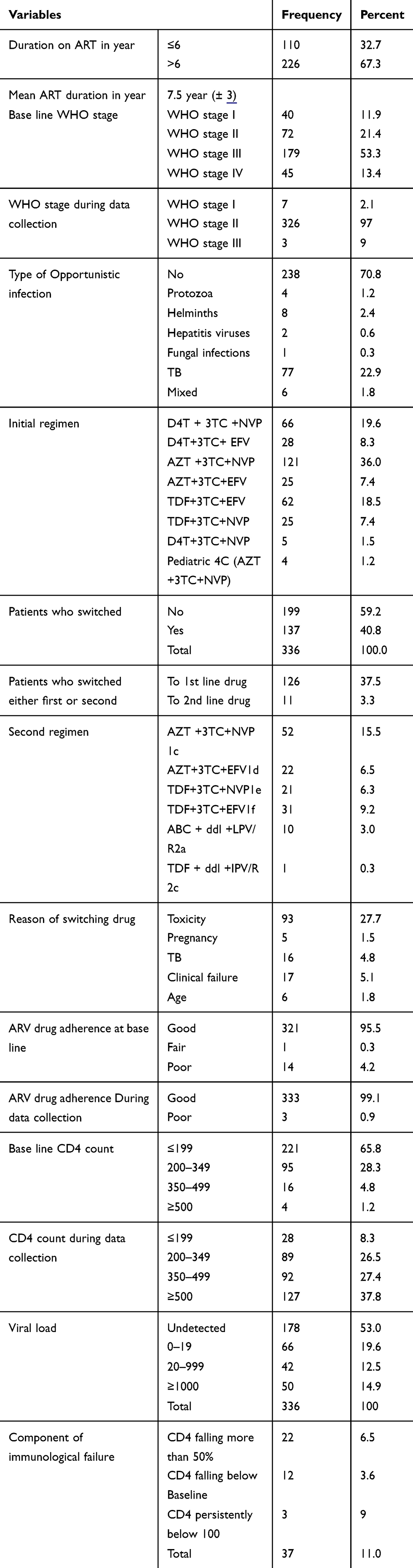 |
Table 2 Clinical Characteristics of HIV/AIDS Patients on HARRT at the University of Gondar Referral Hospital, 2017 |
Staging of Kidney Function and Prevalence of Chronic Kidney Disease
Using CKD-EPI GFR estimator, the overall prevalence of CKD was 54 (16.1% (95% CI, 12.2% - 19.9%)). By stage, about 27 (8.0%) had stage 1, 16 (4.8%) had stage 2, 6 (1.8%) had stage 3 and 5 (1.5%) had stage 5 (Table 3).
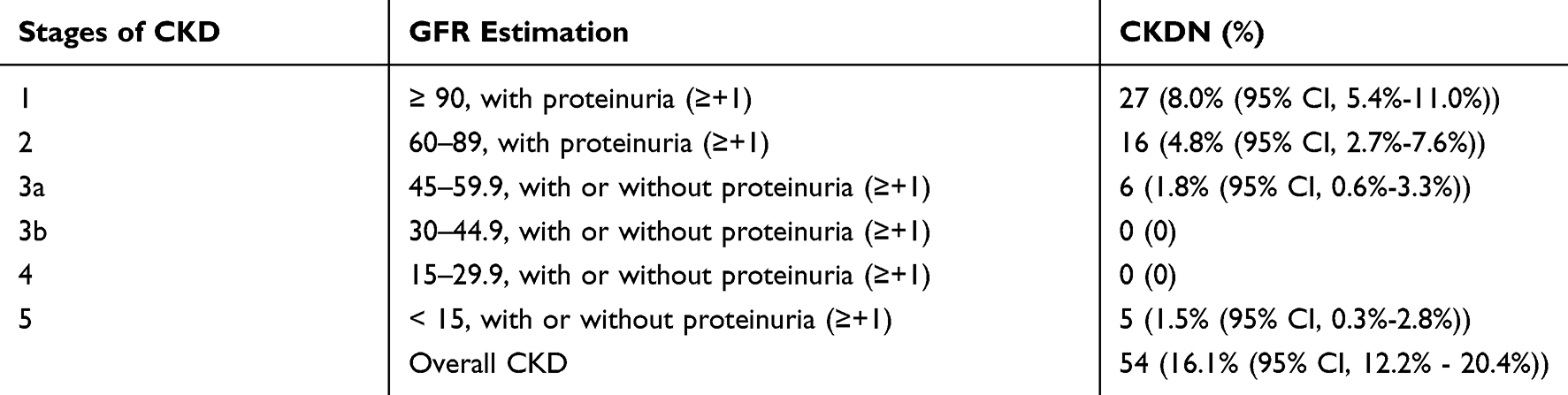 |
Table 3 Stages of Kidney Functions Using the CKD-EPI Estimator Among HIV/AIDS Patients on HARRT at the University of Gondar Referral Hospital, 2017 |
Associated Factors of Chronic Kidney Disease
In bivariate logistic regression analysis associated factors like gender, occupation, duration on ART, viral load was found to be a p-value of < 0.2. When it was analyzed with multivariate logistic regression analysis being male, occupation (merchant) and VL ≥ 100 copies/mm3 were significant factors (p < 0.05) for chronic kidney disease. Male patients on follow-up (AOR=2.05 (1.03–4.09), = 0.04), merchant patients (AOR=2.91 (1.00–8.48), P=0.049) and patients who have had VL ≥ 1000 (AOR= 3.1 (1.38–7.00), P < 0.01) were 2, 2.9 and three times more likely to have chronic kidney disease compared with their comparison group female, housewife, and viral load < 20 copies/mm3 respectively (Table 4).
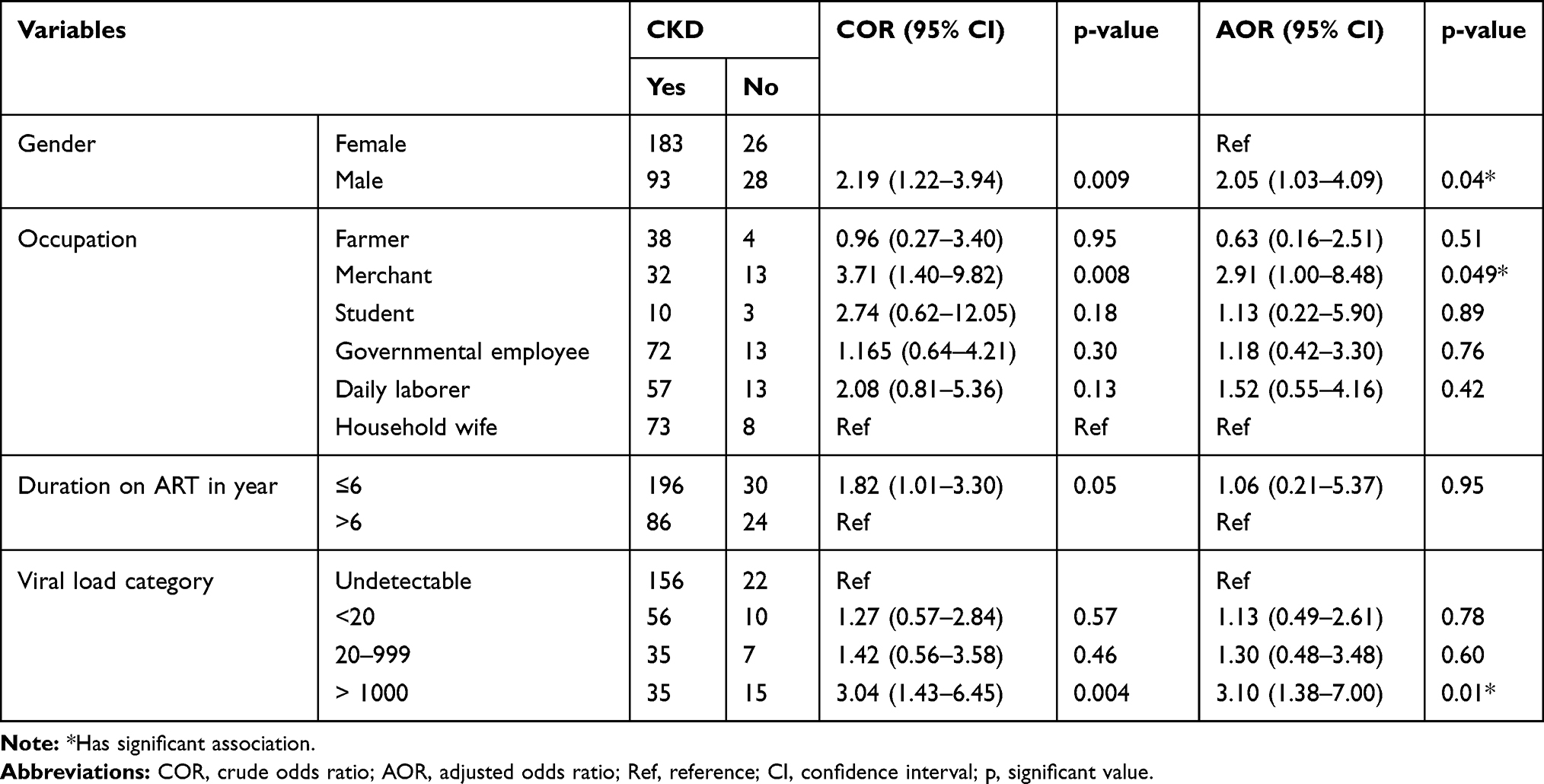 |
Table 4 Bivariate and Multivariate Analysis of Chronic Kidney Disease Associated Factors Among HIV/AIDS Patients on HARRT at the University of Gondar Referral Hospital 2017 |
Discussion
The current study assessed the prevalence and associated factors of CKD in HIV patients on HAART using the commonest estimator of kidney function method CKD-EPI. The finding of this study revealed a high frequency of CKD and the related risk factors mostly being male, occupation merchant and patients with VL ≥ 1000. The prevalence of CKD, 16.1% was consistency with the previous study conducted in Ethiopia, 12.1%,33 Ghana, 14.5%,35 Nigeria, 15.3%36 and Tokyo, 13%.37 However, the result was higher than compared to a study conducted in Uganda, 6%,38 Nigeria, 6.9%,39 Brazil, 8.4%,40 Southwest Ethiopia, 7.6%,41 Tanzania, 1.1%,42 and Lesotho, 5.5%.43 The observed differences could be due to study design, study area, their lifestyle, and the method used to estimate GFR.
Our finding showed, being male was significantly associated with renal impairment and it was 2.05 times more likely to have chronic kidney disease as compared with its comparison group female. Our finding disagrees with the findings done in Burundi and Spain4,44 but it was concurred with the study findings done in France45 and South Africa.46,47 In addition, our study also showed that being an occupation merchant was independently and significantly associated with chronic kidney disease. Occupation merchant patients were 2.9 times high risk than the comparative group housewife. In our study more than half (51%) of the occupation merchant participants were males. Hence, the lower prevalence of CKD among females and the higher prevalence of CKD among males may be due to the possible protective role encouraged by estrogen hormone or due to the absence of the profibrotic effects caused by testosterone hormone in females compared to males.48,49
In our study patients who have had VL ≥ 1000 were three times more likely to have chronic kidney disease contrasted with its comparison group patients who have had viral load < 20 copies/mm3 respectively. Our result is in line with the study done in America5,50 and Thailand.51 High viral replication increased renal damage possibly occurred due to the destruction of kidney cells, and the nephrons with the virus. Consequently, viral load suppression would improve renal function on the other hand if the viral load is not suppressed it lead to chronic kidney disease.22,52,53
Conclusion
The prevalence of CKD in our study based on the glomerular filtration rate using the CKD-EPI method was high (16.1%). Male gender, merchant, and VL ≥ 1000 were associated factors of chronic kidney diseases CKD among HIV patients on HARRT. Hence, HIV patients on HARRT should be regularly screened for early diagnosis and management of CKD. Those patients with high viral load and male patients should be closely followed.
Abbreviations
ABC, Abacavir; AIDS, Acquired Immune Deficiency Syndromes; ART, Antiretroviral Therapy; ARV, Anti-retroviral Virus; AZT/3TC, Zidovudine/Lamivudine; CKD, Chronic Kidney disease; DDI, Didanosine; EFV, Efavirenze; ESRD, end-stage renal disease; eGFR, estimated glomerular filtration rate; GFR, glomerular filtration rate; HAART, Highly Active Antiretroviral Therapy; HIV, Human Immune Deficiency Virus; LPV/R, Lopinavir/ritonavir; NNRT, Non-Nucleoside Rivers Transcriptase; NRT, Nucleoside Rivers Transcriptase; NVP, Nevirapine; OI, Opportunistic Infections; PLHIV, People Living with Human Immune Deficiency Virus; PIs, Proteinase Inhibitors; TDF, TenofovirDisoproxilFumarate; VL, Viral Load.
Author Email Addresses
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki after ethical clearance was acquired from the Research and Ethical Review Committee of School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar. The permission letter was taken from the clinical director of the University of Gondar Specialized Referral Hospital. Written informed consent was obtained from each study participants after reading and clearly explaining the reason, procedure, period, possible risks and benefits of the research in Amharic translated full participant information sheet. For this purpose, a consent form, and a participant information sheet was attached as a cover page of each questionnaire. Patients who were not willing to participate in the study were not forced to participate. The privacy of personal information was protected and kept confidential by excluding their name during the period of data collection. The laboratory results from the study participants were communicated to their physicians for appropriate management.
Acknowledgments
We would like to express our appreciation to the study participants for their willingness to give samples and required information and staff of the ART clinic of the University of Gondar Referral Teaching Hospital for their support during data collection.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
University of Gondar.
Disclosure
We declare that we do not have any conflict of interests.
References
1. Althoff KN, McGinnis KA, Wyatt CM, et al. Comparison of risk and age at diagnosis of myocardial infarction, end-stage renal disease, and non-AIDS-defining cancer in HIV-infected versus uninfected adults. Clin Infect Dis. 2015;60(4):627–638. doi:10.1093/cid/ciu869
2. Nakagawa F, Lodwick RK, Smith CJ, et al. Projected life expectancy of people with HIV according to timing of diagnosis. Aids. 2012;26(3):335–343. doi:10.1097/QAD.0b013e32834dcec9
3. Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One. 2013;8(12):e81355. doi:10.1371/journal.pone.0081355
4. Cailhol J, Nkurunziza B, Izzedine H, et al. Prevalence of chronic kidney disease among people living with HIV/AIDS in Burundi: a cross-sectional study. BMC Nephrol. 2011;12(1):40. doi:10.1186/1471-2369-12-40
5. Calza L, Vanino E, Magistrelli E, et al. Prevalence of renal disease within an urban HIV-infected cohort in northern Italy. Clin Exp Nephrol. 2014;18(1):104–112. doi:10.1007/s10157-013-0817-5
6. Campbell L, Ibrahim F, Fisher M, Holt S, Hendry B, Post F. Spectrum of chronic kidney disease in HIV‐infected patients. HIV Med. 2009;10(6):329–336. doi:10.1111/j.1468-1293.2008.00691.x
7. Wools-Kaloustian KK, Gupta SK. Will there be an epidemic of HIV-related chronic kidney disease in sub-Saharan Africa? Too soon to tell. Kidney Int. 2008;74(7):845–847. doi:10.1038/ki.2008.326
8. Bonjoch A, Juega J, Puig J, et al. High prevalence of signs of renal damage despite normal renal function in a cohort of HIV-infected patients: evaluation of associated factors. AIDS Patient Care STDS. 2014;28(10):524–529. doi:10.1089/apc.2014.0172
9. Naicker S, Rahmania S, Kopp JB. HIV and chronic kidney disease. Clin Nephrol. 2015;83(Suppl 1):S32. doi:10.5414/CNP83S032
10. Kopple JD. National kidney foundation K/DOQI clinical practice guidelines for nutrition in chronic renal failure. Am J Kidney Dis. 2001;37(1):S66–S70. doi:10.1053/ajkd.2001.20748
11. Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003;41(1):1–12. doi:10.1053/ajkd.2003.50007
12. Szczech LA, Hoover DR, Feldman JG, et al. Association between renal disease and outcomes among HIV-infected women receiving or not receiving antiretroviral therapy. Clin Infect Dis. 2004;39(8):1199–1206. doi:10.1086/424013
13. Szczech LA, Gupta SK, Habash R, et al. The clinical epidemiology and course of the spectrum of renal diseases associated with HIV infection. Kidney Int. 2004;66(3):1145–1152. doi:10.1111/j.1523-1755.2004.00865.x
14. Wyatt CM, Arons RR, Klotman PE, Klotman ME. Acute renal failure in hospitalized patients with HIV: risk factors and impact on in-hospital mortality. Aids. 2006;20(4):561–565. doi:10.1097/01.aids.0000210610.52836.07
15. Röling J, Schmid H, Fischereder M, Draenert R, Goebel F. HIV-associated renal diseases and highly active antiretroviral therapy—induced nephropathy. Clin Infect Dis. 2006;42(10):1488–1495. doi:10.1086/503566
16. Islam FM, Wu J, Jansson J, Wilson DP. Relative risk of renal disease among people living with HIV: A systematic review and meta-analysis. BMC Public Health. 2012;12:234. doi:10.1186/1471-2458-12-234
17. Baynes HW, Negash M, Geremew D, Getaneh Z. Chronic Kidney Disease among Human Immunodeficiency Virus Positive Patients on Antiretroviral Therapy in Sub-Saharan Africa: A Systematic Review and Meta-analysis. Saudi J Kidney Dis Transpl. 2019;30(6):1190–1200. doi:10.4103/1319-2442.275462
18. Gilbertson DT, Liu J, Xue JL, et al. Projecting the number of patients with end-stage renal disease in the United States to the year 2015. J Am Soc Nephrol. 2005;16(12):3736–3741. doi:10.1681/ASN.2005010112
19. Levey A, Atkins R, Coresh J, et al. Chronic kidney disease as a global public health problem: approaches and initiatives–a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72(3):247–259. doi:10.1038/sj.ki.5002343
20. Gupta SK, Eustace JA, Winston JA, et al. Guidelines for the management of chronic kidney disease in HIV-infected patients: recommendations of the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2005;40(11):1559–1585.
21. Panel of experts from the AIDS Study Group (GESIDA) and the National AIDS Plan (PNS. Diagnosis, treatment and prevention of kidney disorders in patients with infection by the human immunodeficiency virus. Recommendations of the AIDS Study Group / National Plan on AIDS. Infectious Diseases and Clinical Microbiology. 2010 Oct 1; 28 (8): 520–e1.
22. Fernando SK, Finkelstein FO, Moore BA, Weissman S. Prevalence of chronic kidney disease in an urban HIV infected population. Am J Med Sci. 2008;335(2):89–94. doi:10.1097/MAJ.0b013e31812e6b34
23. De Silva TI, Post FA, Griffin MD, Dockrell DH. HIV-1 infection and the kidney: an evolving challenge in HIV medicine. Mayo Clin Proc. 2007;2007:1103–1116. doi:10.4065/82.9.1103
24. Fulop T, Olivier J, Meador R, et al. Screening for chronic kidney disease in the ambulatory HIV population. Clin Nephrol. 2010;73(3):190–196. doi:10.5414/CNP73190
25. Di AB, Rosso R, Vitale F, et al. Risk factors for chronic kidney disease among human immunodeficiency virus-infected patients: A European case control study. Clin Nephrol. 2011;75(6):518–523. doi:10.5414/CNP75518
26. Flandre P, Pugliese P, Cuzin L, et al. Risk factors of chronic kidney disease in HIV-infected patients. Clin J Am Soc Nephrol. 2011;6(7):1700–1707. doi:10.2215/CJN.09191010
27. Crum NF, Riffenburgh RH, Wegner S, et al.; Consortium TAC. Comparisons of causes of death and mortality rates among HIV-infected persons: analysis of the pre-, early, and late HAART (highly active antiretroviral therapy) eras. J Acquir Immune Defic Syndr. 2006;41(2):194–200. doi:10.1097/01.qai.0000179459.31562.16
28. Joint U: Programme on HIV/AIDS. Prevention gap report. Geneva: Joint United Nations Programme on HIV. AIDS; 2016:3.
29. Andrassy KM. Comments on ‘KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease’. Kidney Int. 2013;84(3):622–623. doi:10.1038/ki.2013.243
30. Denue BA, Muazu PJ, Gashau W, Nkami D, Ajayi NA. Effects of highly active antiretroviral therapy (HAART) on blood pressure changes and its associated factors in HAART naive HIV-infected patients in north eastern Nigeria. Arch Appl Sci Res. 2012;4(3):1447–1452.
31. Seidell JC, Flegal KM. Assessing obesity: classification and epidemiology. Br Med Bull. 1997;53(2):238–252. doi:10.1093/oxfordjournals.bmb.a011611
32. Chalmers J, MacMahon S, Mancia G, et al. 1999 World Health Organization-International Society of Hypertension Guidelines for the management of hypertension. Guidelines sub-committee of the World Health Organization. Clin Exp Hypertens. 1999;21(5–6):1009–1060.
33. Kahsu G, Birhan W, Addis Z, Dagnew M, Abera B. Renal function impairment and associated risk factors among human immunodeficiency virus positive individuals at Flege Hiwot Referral Hospital, Northwest Ethiopia. J Interdisciplinary Histopathol. 2013;1(5):252–260. doi:10.5455/jihp.20130508063833
34. Baynes HW, Tegene B, Gebremichael M, Birhane G, Kedir W, Biadgo B. Assessment of the effect of antiretroviral therapy on renal and liver functions among HIV-infected patients: a retrospective study. HIV/AIDS (Auckland, Nz). 2017;9:1.
35. Owiredu W, Quaye L, Amidu N, Addai-Mensah O. Renal insufficiency in Ghanaian HIV infected patients: need for dose adjustment. Afr Health Sci. 2013;13(1):101–111.
36. Okpa HO, Bisong EM, Enang OE, Effa EE, Monjok E, Essien EJ. Predictors of chronic kidney disease among HIV–infected patients on highly active antiretroviral therapy at the University of Calabar Teaching Hospital, Calabar, South-South Nigeria. HIV/AIDS (Auckland, Nz). 2019;11:61.
37. Nishijima T, Kawasaki Y, Mutoh Y, et al. Prevalence and factors associated with chronic kidney disease and end-stage renal disease in HIV-1-infected Asian patients in Tokyo. Sci Rep. 2017;7(1):1–8. doi:10.1038/s41598-017-15214-x
38. Peters PJ, Moore DM, Mermin J, et al. Antiretroviral therapy improves renal function among HIV-infected Ugandans. Kidney Int. 2008;74(7):925–929. doi:10.1038/ki.2008.305
39. Yusuf R, Aliyu I, Anaja P, Muktar H. Prevalence of chronic kidney disease (CKD) in HIV-infected patients in Zaria, Nigeria. Nig J Pharm Sci. 2011;10(1):107–111.
40. Menezes AM, Torelly J
41. Mekuria Y, Yilma D, Mekonnen Z, Kassa T, Gedefaw L. Renal function impairment and associated factors among HAART Naïve and experienced adult HIV positive individuals in Southwest Ethiopia: a comparative cross sectional study. PLoS One. 2016;11(8):e0161180. doi:10.1371/journal.pone.0161180
42. Mpondo BC, Kalluvya SE, Peck RN, et al. Impact of antiretroviral therapy on renal function among HIV-infected Tanzanian adults: a retrospective cohort study. PLoS One. 2014;9(2):e89573. doi:10.1371/journal.pone.0089573
43. Bygrave H, Kranzer K, Hilderbrand K, et al. Renal safety of a tenofovir-containing first line regimen: experience from an antiretroviral cohort in rural Lesotho. PLoS One. 2011;6(3):e17609. doi:10.1371/journal.pone.0017609
44. Cristelli MP, Trullàs JC, Cofán F, et al. Prevalence and risk factors of mild chronic renal failure in HIV-infected patients: influence of female gender and antiretroviral therapy. Braz J Infect Dis. 2018;22(3):193–20145. doi:10.1016/j.bjid.2018.05.001
45. Déti EK, Thiébaut R, Bonnet F, et al. Prevalence and factors associated with renal impairment in HIV‐infected patients, ANRS C03 Aquitaine Cohort, France. HIV Med. 2010;11(5):308–317. doi:10.1111/j.1468-1293.2009.00780.x
46. Bengura P, Managa MA. Cox regression of factors associated with the onset of chronic kidney disease in HIV/AIDS patients in Albert Luthuli Municipality of South Africa.
47. Crum-Cianflone N, Ganesan A, Teneza-Mora N, et al. Prevalence and factors associated with renal dysfunction among HIV- infected patients. AIDS Patient Care STDS. 2010;24(6):353–360. doi:10.1089/apc.2009.0326
48. Silbiger SR, Neugarten J. The impact of gender on the progression of chronic renal disease. Am J Kidney Dis. 1995;25(4):515–533. doi:10.1016/0272-6386(95)90119-1
49. Neugarten J, Acharya A, Silbiger SR. Effect of gender on the progression of nondiabetic renal disease: a meta-analysis. J Am Soc Nephrol. 2000;11(2):319–329.
50. McMahon BA, Hanouneh M, Chedid A, et al. Association of HIV suppression with kidney disease progression among HIV-positive African Americans with biopsy-proven classic FSGS. J Acquir Immune Defic Syndr. 2018;79(5):639–643. doi:10.1097/QAI.0000000000001860
51. Pongpirul W, Pongpirul K, Ananworanich J, Klinbuayaem V, Avihingsanon A, Prasithsirikul W. Chronic kidney disease incidence and survival of Thai HIV-infected patients. Aids. 2018;32(3):393–398.
52. Park J, Zuniga JA. Chronic kidney disease in persons living with HIV: a systematic review. J Assoc Nurs AIDS Care. 2018;29(5):655–666. doi:10.1016/j.jana.2018.04.004
53. Wyatt CM, Morgello S, Katz-Malamed R, et al. The spectrum of kidney disease in patients with AIDS in the era of antiretroviral therapy. Kidney Int. 2009;75(4):428–434. doi:10.1038/ki.2008.604
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.