")
Back to Journals » Clinical Interventions in Aging » Volume 18
Chronic Disease Self-Management of Post-Acute Sequelae of COVID-19 Among Older Adults: A Mixed-Methods Analysis
Authors Thomas-Purcell K , Davenport R, Ayala V, Purcell D, Ownby RL
Received 21 November 2022
Accepted for publication 5 April 2023
Published 14 April 2023 Volume 2023:18 Pages 607—617
DOI https://doi.org/10.2147/CIA.S393732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Kamilah Thomas-Purcell,1,* Rosemary Davenport,2,* Victoria Ayala,2,* Donrie Purcell,3,* Raymond L Ownby2,*
1Department of Health Science, Nova Southeastern University, Ft. Lauderdale, FL, USA; 2Department of Psychiatry, Nova Southeastern University, Ft. Lauderdale, FL, USA; 3Satcher Health Leadership Institute, Morehouse School of Medicine, Atlanta, GA, USA
*These authors contributed equally to this work
Correspondence: Raymond L Ownby, Nova Southeastern University, Center for Collaborative Research Suite 430, 3301 College Avenue, Ft. Lauderdale, FL, 33314, USA, Tel +1-954-608-4846, Email [email protected]
Introduction: Approximately 20– 30% of individuals who contract acute coronavirus disease (COVID-19) infection develop longer term complications of their initial infection, referred to as Post-Acute Sequelae of SARS-CoV-2 infection (PASC). PASC is characterized by chronic, varying symptomatology.
Methods: Using a mixed methods study design, we aimed to gain insight into individuals’ experience with PASC, including cognitive issues, fatigue, and sleep disturbances. We explored whether our previously developed application (app), aimed at improving self-management skills among individuals with chronic diseases, is relevant for individuals with PASC and gained information to adapt the app for individuals with PASC. The study included 19 individuals, aged 40 years and older, recruited from our research participant database, Nova Southeastern University clinics, and community locations. We included this age range because older adults are more likely to have comorbid conditions, allowing us to better understand the impact of COVID-19 infection in these individuals. Participants completed seven standardized self-report questionnaires online, and an individual semi-structured interview via videoconferencing. Quantitative data were assessed using descriptive statistics and calculating individuals’ scores in relation to norms. Qualitative data were analyzed using a thematic analysis approach. Triangulation of the data was accomplished by calculating correlations between participants’ responses on self-report scales and themes found in semi-structured interviews.
Results: Themes included disruption of everyday life, diverse physical symptoms, and cognitive problems including brain fog, fatigue, coping, and emotional upset. Quantitative analysis demonstrated that participants experienced high levels of fatigue, negative mood, cognitive problems, and overall reduction in health-related quality of life (HRQOL). Correlation analyses revealed that individual interview responses were related to participants’ self-report of symptoms on standard questionnaires.
Discussion: Findings indicate that self-report questionnaires may reflect the experience of individuals with PASC and its impact. Additionally, further efforts to expand our prior mobile app are warranted among individuals with PASC.
Keywords: post-acute sequelae of SARS-CoV-2 infection, COVID-19, long COVID, SARS-CoV-2 cognitive issues, health-related quality of life, self-report questionnaires, qualitative analysis
Introduction
Research on the effects of acute COVID-19 infection remain ongoing, which has increasingly demonstrated that approximately 20–30% of individuals will develop longer term complications of their initial infection, referred to as Post-Acute Sequelae of SARS-CoV-2 infection (PASC). Symptoms of PASC, including fatigue, post-exertional malaise (PEM), muscle and joint pain, sleep disturbances, respiratory and cardiovascular complications, and cognitive issues, can range in severity and continue months after the initial infection.1–3
As research on PASC continues to evolve it is clear that many affected individuals will require healthcare services to address these symptoms.4 In addition, further research is needed to provide insight into PASC presenting and ongoing symptomatology and to understand the most effective methods to successfully support affected individuals. The problems encountered by individuals with PASC are in many respects like those of persons with other chronic health conditions, including Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and autoimmune diseases.5,6
The impetus for this research endeavor was based on a previous mobile application (app) our research team developed to improve the health literacy of individuals with chronic diseases through improved chronic disease self-management (CDSM).7 Using computer-tailoring to match CDSM information to participants’ level of health literacy and reported problems,8 the app provided basic information on CDSM for problems that often arise in individuals with chronic health conditions, such as fatigue, sleep disturbance, and cognitive problems.
Based on participants’ positive reaction to our app as well as to other interventions focused on developing chronic disease management skills9–11 in improving self-management in established chronic diseases, our research team aimed to gain insight into whether this previously-developed CDSM app might be helpful to individuals with PASC. As such, it was determined that additional information on PASC, especially with respect to the problems addressed by the mobile app, would be necessary to further develop the app to make it useful to individuals with PASC. Our research team was most interested in how standardized self-report questionnaires could be used to accurately measure PASC symptoms. Therefore, the purpose of this study was to use a triangulation mixed methods design to provide information on individuals’ experience of PASC symptoms such as fatigue, sleep disturbance, and cognitive problems and relate them to their responses on standard self-report questionnaires.
The findings of this research effort will facilitate understanding PASC from the perspective of the patient, including understanding the challenges of symptom self-management and help to determine which symptoms are amenable for intervention via a modification of our previously developed mobile app. In addition, understanding the meaning of self-report questionnaires in persons with PASC may improve the health assessment phase of the patient encounter, providing a starting point for treatment.
Materials and Methods
Study Design
A mixed methods triangulation study design was employed using semi-structured individual in-depth interviews to describe the acute and PASC experience from the perspective of patients. In addition, seven standardized questionnaires were administered in effort to determine whether standardized self-report questionnaires can be used to accurately measure reported PASC symptoms. All study procedures were carried out under a protocol approved by the Nova Southeastern University (NSU) Institutional Review Board (IRB;# 2021–315-NSU) which complies with the Declaration of Helsinki.
Recruitment
Study recruitment methods consisted of contacting potential individuals from our research study participant database (this included names of past participants who consented to be contacted for future research studies) and advertising via flyers within NSU’s university clinics and community locations. A purposeful sampling method was used. Purposeful sampling is widely used in qualitative research for the identification and selection of information-rich cases related to a phenomenon of interest. Eligible participants included those who were 1) 40 years of age and older, 2) met Centers for Disease Control and Prevention (CDC) criteria for probable COVID-19 infection,12 and 3) continued to have characteristics PASC symptoms after the resolution of the acute illness. Individuals who met the inclusion criteria were invited to schedule a time for an online video informed consent interview. We included persons in this age range because older adults are more likely to have comorbid conditions, allowing us to better understand the impact of COVID infection in these individuals.13
We completed informed consent procedures online in a video interview during which a written information form was reviewed with the potential participants and his or her questions were answered. Participants had been mailed a link to an online form in the REDCap electronic data capture tools hosted at Nova Southeastern University.14,15 The form included a statement about the potential participant’s willingness to participate in the study and required an affirmative response (checking a box for “yes”) before proceeding. After indicating their willingness in this form, an electronic popup box was presented to electronically record their signature. The person conducting the interview recorded the interview and the person’s responses on a form during the interview. After obtaining participants’ consent for their participation, they completed the battery of self-report measures and then were scheduled to sit for an online interview later.
Study Instruments
Quantitative
Participants completed self-report questionnaires online using Research Electronic Data Capture (REDCap) software.16 Self-report questionnaires were chosen to include widely used measures of health-related quality of life (HRQOL), cognitive function, fatigue, and sleep. These included the 36-Item Short Form Survey ([SF-36],17 the Cognitive Failures Questionnaire (CFQ),18 the Center for Epidemiological Studies-Depression scale (CESD),19 the Chalder Fatigue Scale (Chalder),20 and the Perceived Stress Scale, 10-item version.21 The battery also included measures from the Patient Reported Outcomes Measurement System (PROMIS),22 including Sleep Disturbance, Sleep Impairment, Cognitive Function, and Fatigue. Finally, we included the Pittsburgh Sleep Quality Index (PSQI).23
Qualitative
A semi-structured in-depth interview guide was developed based on a review of the most current PASC literature available at the time of the study. The questions elicited information on symptoms and experiences tied to the acute COVID-19 infection and PASC. All interviews were conducted via video conferencing (Zoom Video Communications, Inc: San Jose, CA) by a trained interviewer to ensure consistency and monitored by a lead investigator to support in the event of technical issues. With the consent of the participants, interview responses were audio recorded and additional handwritten notes were taken.
Sample Size
The target sample size balanced the need to be able to detect relations between qualitative findings and quantitative measures. We aimed for a sample size of 20 because that would provide a power of 0.80 to detect large effect size (eg, correlations > 0.60) relations between the two types of data. Power analyses were completed using Power Analysis and Sample Size (PASS)15 (NCSS, Kaysville UT). Given others’ findings on sample size needed for thematic analysis,24,25 we believed that this sample size was likely to allow us to achieve saturation in coding interviews.
Data Analysis
Qualitative Evaluation
Thematic analysis26,27 was used to better understand qualitative findings. Interviews were transcribed and entered into NVivo 11 (QSR International, Burlington MA). The first 10 interviews were coded by the first and senior author (KTP and RLO), who then discussed codes and content and agreed on a coding approach for the remainder of the interviews. Any disagreements were resolved through iterative discussion between researchers. We used the procedure recommended by Guest et al24 to assess the likelihood that we had achieved saturation, which indicated a high probability (> 0.95) that saturation was obtained after 12 interviews, a number similar to that found in other studies.25 Since we intended to evaluate the relation of codes to the self-report questionnaire responses, all interviews were coded.
Quantitative Evaluation
Descriptive statistics were calculated using Statistical Package for the Social Sciences (SPSS, Armonk, NY: IBM). Self-report questionnaires were scored according to each one’s standard procedure, and for the questionnaires with normative data (PROMIS measures), the T score for each was obtained and reported. Correlations were calculated between the occurrence of each code in interviews (scored as 1, present, or 0, absent) and raw scores on questionnaires using the nonparametric Spearman rank order correlation coefficient because of the small sample size and likelihood that distributions analyzed would not be normal.28
Results
Qualitative
Seven themes were identified that encompassed much of our participants’ experience of both the acute COVID-19 infection and resulting PASC.
Physical Symptoms
When asked about their experience with the acute COVID-19 infection, participants often listed a number of physical symptoms that characterized their experience with the infection. Symptoms such as chronic cough, shortness of breath, fever, headache, fatigue, and loss of sense of taste or smell were common. For many, symptoms persisted long after the acute infection, resulting in PASC.
Participant 110: And I have a chronic cough…The cough that I have. At night, when – and when I am – during the day, and I have to take a mentho-lyptus because I am choking. It’s really bothersome. And I do not know what to – to do to get – and that’s very, very, really hard. And then, people think you are sick with COVID. Because you are always coughing.
Participant 105: I have had reoccurring headaches. I have had fever that have come and gone. When I first got ill, I had a fever for probably three months. And most recently, I have had it for four months. And I take a picture every day because it’s just so abnormal and no one can explain it.
Fatigue was not only a physical symptom but was in some cases so severe that the person could no longer work and might even find self-care difficult.
Participant 110: I–I am up on the third floor. I could not even walk downstairs to the mailbox.
Participant 111: But in one of those fatigue days, I end up staying in bed for the majority. I would just get out of bed to do things that are extremely necessary, like I have to take out my dog otherwise, he’s gonna pee, things like that. But if I can, I just stay laying down.
Disruption of activities of daily living. One of the most common comments focused on how having acute COVID infection and the resulting PASC had upended participants’ daily activities.
Participant 105: I could not drive this whole time. I have not driven since August 2020.
Participant 112: I am just taking more time off. And I work more part-time, not as much as I used to… I was working full-time. I was going in every day. I am part-time now.
Cognition. Similarly, cognitive difficulties, sometimes referred to as “brain fog”, made work difficult for some participants and interfered with other daily activities. Participants described lapses in memory, feeling as though their thinking was slow, and problems in concentrating.
Participant 108: … right after COVID, oh my God. …I can recall going into the bank, I could not think of my account number… One of the bank officials came over and asked, and I said I am so sorry, I am just recovering from COVID, I cannot think of my account number. And I have had this account for over 40 years, and it was routine.
Participant 119: I was a wiz at mathematics. I mean, I could do scientific numeration, logarithm readings, I could read blood work, everything like that. I have got to grab a calculator now. Because I will look at zeros and commas, and I will just draw a blank.
Notably, some older participants attributed cognitive difficulties after COVID to the aging process.
Participant 117: … And being the forgetful I think is just part of aging, you are going to forget anyway.
Emotional upset. Participants understandably described strong emotional reactions to the experience of having acute COVID infection, including fear before and after the acute infection. Many described frustrations with the slow pace of recovery and their ongoing difficulties, especially those related to PASC.
Participant 101: In every way because I look at people differently. I do not wanna go in. I mean, I am just afraid, I am just afraid. I was sitting at a table August the 1st with a lady–and it was like scattered tables…and August the 18th I found out she died from COVID. I am afraid, okay? I am totally afraid–
Participant 112: It’s still bad. It affects my body. It seems like things are ongoing. It seems like it’s staying the same.
Coping. In the face of the stress of having persistent and ongoing symptoms, especially related to PASC, we were interested in individuals’ coping strategies. Participants reported learning to reduce activities, for example, in coping with fatigue. A number had developed compensatory strategies in coping with memory lapses, such as writing themselves reminder notes or enlisting the assistance of others to remember important appointments.
Participant 105: … I just use natural remedies like cava root, which is a tea, and – It’s just a drink. It’s a tea that I make. But that – I have to watch that because it can bother my organs.
Participant 101: But some days I do not want to get up, I am like–’cause I started a routine as far as I said, “Okay, you got to do this, you got through this.” And I listen to a seminar, so I’m like, “You got to get up, you gotta do a stretch”, just positive things. So, I started walking, and some days I do not even wanna walk. After I walk, I feel better, but some days I do not even wanna get up.
Participant 118: Well, I got a little better with the anxiety. The depression is just a little now…I would just pray and sit still and just talk myself down. I used self-talk to help me calm down.
“Don’t be too anxious. This will pass.”
Experience of self. A small number reported a change in how they saw themselves as a result of the illness.
Participant 116: No, I have not experienced the brain fog, in fact, I was going to say it’s almost the opposite, it’s also almost a brain clarity. It could also be a function of aging too of just simply having a better grasp of what’s important and what’s not important.
Participant 103: I lost something in the progress – in the process of my sickness. I lost something with myself. Yeah. I lost myself somewhere.
Summary. These findings emphasize the substantial impact becoming ill with acute COVID infection and resulting PASC had on our participants. Fatigue was mentioned by all participants as an aspect of the illness that had an impact on their lives. Perhaps in response to questions that included prompts about sleep and cognition, participants provided information on these topics as well. Possibly most significant, was the level of disruption of everyday life experienced by the participants, many of whom were at least partially disabled by PASC.
Quantitative
Nineteen persons completed study procedures, including 11 women and eight men. Of the 19 participants, five were African American and 14 were white. Their ages ranged from 40 to 85 years of age, with a mean of 60.3 years (SD = 9.1). Descriptive statistics for the self-report measures are presented in Table 1.
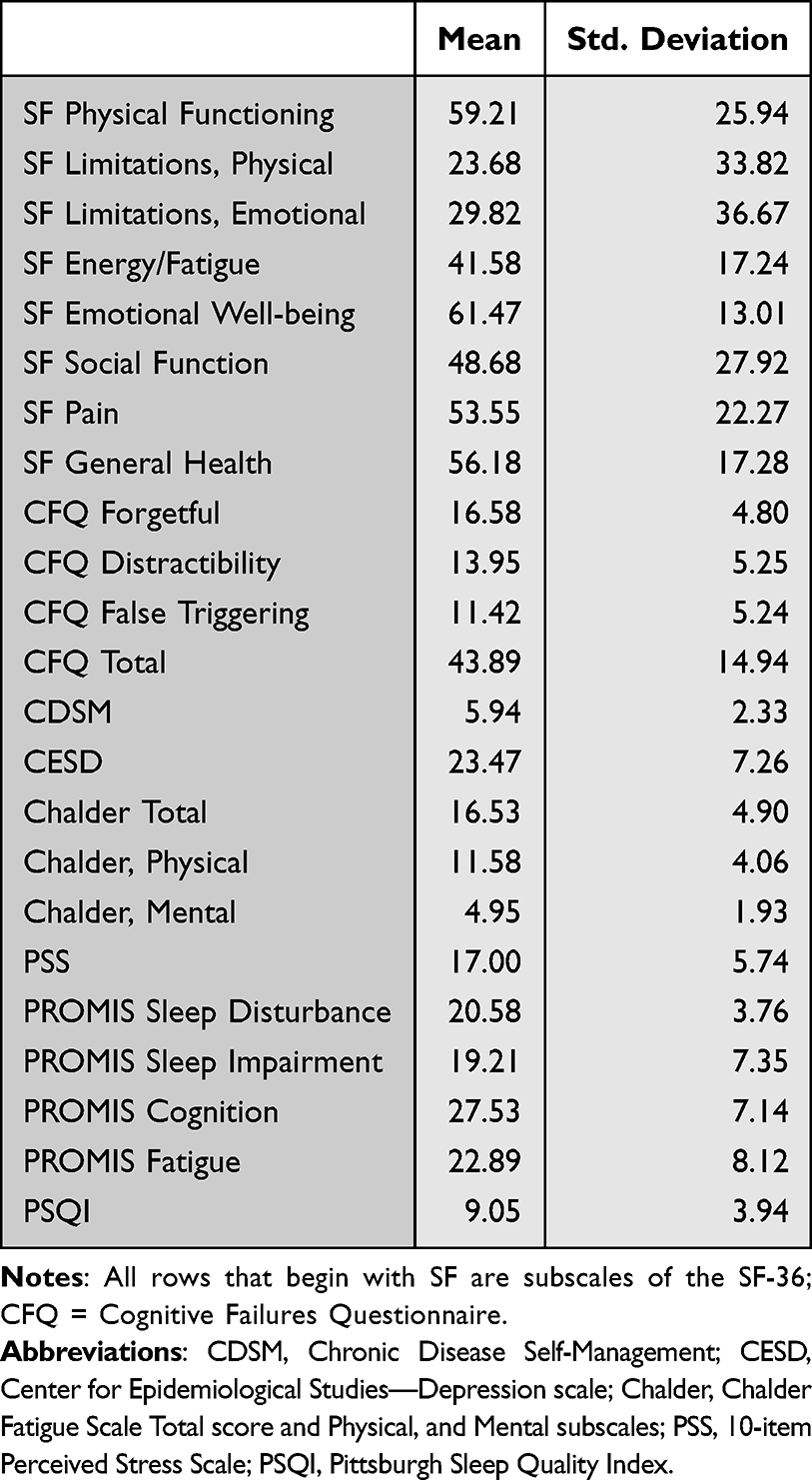 |
Table 1 Descriptive Statistics for Self-Report Measures |
The most common symptoms during acute illness were fever (84%), followed by fatigue (79%), taste disorder (79%), olfactory disturbance (74%), headache (68%), shortness of breath (63%), and sore throat (63%). Based on CDC criteria for probable or confirmed COVID-19 infection, 10 participants had probable cases of acute COVID-19 infection and nine confirmed cases. We assessed the time between the acute infection and the telephone recruitment screening and found that the average number of months that participants had experienced persistent symptoms was 10.9 months (standard deviation (SD) 7.6 months).
Many participants reported low levels of HRQOL (SF-36, general health sub-scale) and high levels of depression symptoms (CESD); 16 is often used as a cutoff for depression), fatigue (Chalder scale; SF-36 energy/fatigue sub-scale), and sleep disturbance (PSQI; Scores greater than 5 suggest sleep problems).
Descriptions of codes and tallies of their frequencies are presented in Table 2. It is noteworthy that all participants reported that acute COVID-19 infection and the resulting PASC had disrupted their daily lives, and that nearly all reported fatigue.
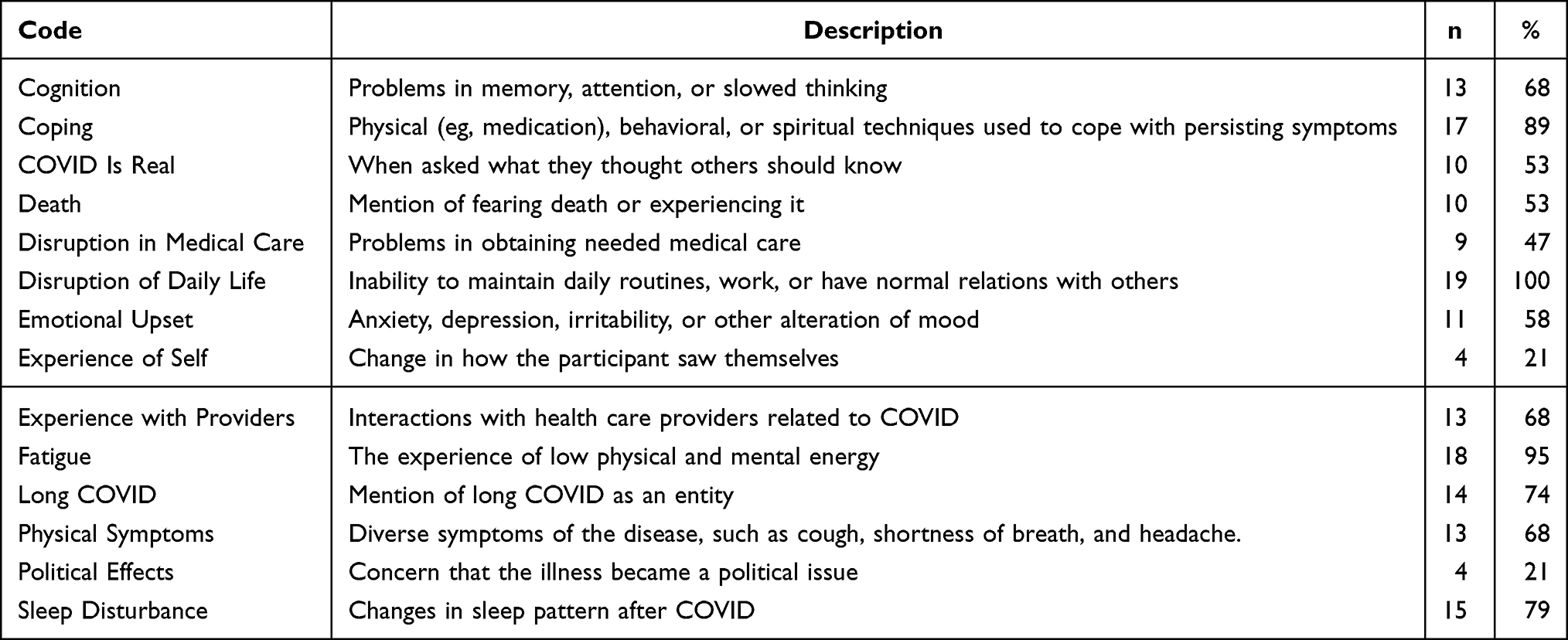 |
Table 2 Codes and Their Frequencies |
Integration
Correlations Between Scores and Themes
Spearman correlations of codes with self-report measures are presented in Table 3. We present tests of the statistical significance of the relationship between codes and the questionnaire responses (bolded in the table). However because of our small sample size, we also present correlations of 0.20 and greater (in italics) as they may be meaningful.29 A subset of all possible correlations is presented in the table, with the complete correlation matrix included in Table 3.
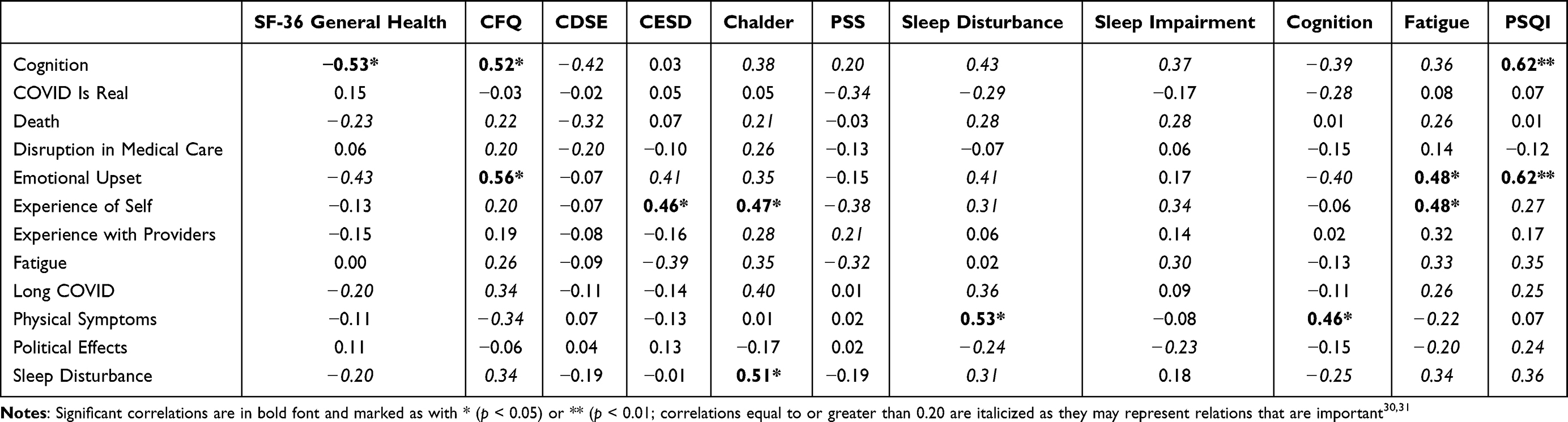 |
Table 3 Correlations of Self-Report Measures with Codes |
We found that several qualitative interview codes were related to several measures. Specifically, report of cognitive difficulties was inversely related to HRQOL (SF-36 general health sub-scale). On the other hand, the report of cognitive difficulties was positively related to questionnaire report of cognitive difficulties (CFQ). In addition, participants’ report of emotional upset was related to questionnaire report of cognitive problems (CFQ), fatigue (PROMIS fatigue scale), and sleep disturbance (PSQI).
Several relations, while not statistically significant, appear likely to be meaningful. Interviewee report of sleep disturbance was only significantly related to scores on the Chandler, but were related at the level of a moderate effect size to cognitive difficulties (CFQ), and questionnaire reports of sleep problems (PROMIS sleep disturbance scale; PSQI). Overall, participants’ experience of PASC as revealed in their qualitative interviews is similarly reflected in the results of their completed standardized questionnaires. These results provide evidence for the usefulness of the questionnaires for reporting symptoms of PASC.
Discussion
PASC comprises several symptoms, including fatigue, sleep disturbances, cognitive issues, muscle and joint pain, cardiovascular and respiratory dysfunction, which result from the impact of COVID-19 on multiple organ systems. This study aimed to understand the challenges of symptom self-management and determine which are amendable for intervention via our previously developed mobile app. Similar to our findings, researchers have argued that several symptoms can persist long after the acute COVID-19 infection has resolved.32 Fatigue as episodic disability is characterized by periods of wellness and fatigue that fluctuate over time. Brown and O’Brien33 argued that PASC can be presented with clusters of overlapping and episodic symptoms such as fatigue or exhaustion. Indeed, Ceban et al (2022)1 found fatigue and cognitive impairment to be amongst the most common and debilitating symptoms of post-COVID-19 syndrome. Groff et al (2021),3 and Nalbandian et al (2021)2 noted that even months after acute COVID-19 infection, PASC had a profound impact on individuals’ lives, in some cases severely impairing their ability to carry out activities of daily living including dressing, self-care, work, etc. Groff et al (2021) also noted that ongoing and persistent symptoms for persons suffering PASC include continuing respiratory problems and other physical symptoms that impacted individual daily lives.3 Eaton et al (2022) in their qualitative study also uncovered a deep sense of emotional upset as a result coping with confinement and social isolation recovery after being discharged.34
Some of our participants attributed their post-acute COVID-19 infection cognitive difficulties to natural aging rather than the infection itself. This finding may be significant for clinicians, as previous studies have shown that older persons may attribute treatable functional and cognitive problems to “old age” rather than seek help.35,36 Given the evidence that cognition can be affected in PASC37–39 it may be helpful to educate older persons on the symptoms of PASC and help them to find ways to cope with them.
Our findings were also consistent with that of Case et al (2022), Jacobs et al (2020), and Suyanto et al (2022)40–42 who observed their study participants as having a low HRQOL score after a COVID-19 infection. These findings indicate the need for broader interventions to support self-care in individuals with PASC. Indeed, self-management of symptoms in the long term is often costly, with some individuals using a substantial proportion of their income, which threatens to widen existing health inequalities.43 Even with excellent support from healthcare providers, much of the burden of coping with PASC will fall on patients,44 many of whom may not be well prepared to develop routines for self-management and advocate on their own for the support and services they need.43
The implementation and deployment of digital tutorials have proven to be a quick and effective health education tool to alleviate the burden that healthcare professionals and patients face due to the COVID-19 pandemic.45 The use mobile health (mHealth) apps have facilitated symptom monitoring of COVID-19 infection and have been used to share data with health care professionals and support disease prediction, prevention, management, diagnostics, and improvements in treatments and patient education.46 Using the results of this study, we plan to modify our previously developed digital health app to address the needs of those coping with PASC. Research has supported the use of mobile apps to assist patient chronic disease self-management via digital education, self-monitoring, and feedback.47
Conclusion
In this study, we explored the experience of individuals with persistent symptoms after acute COVID-19 infection, especially with respect to fatigue, sleep, and cognition. We found that while they are affected by diverse symptoms based in multiple organ systems, some problems cut across types of physical symptoms and are like those encountered by others with chronic diseases. By relating participants’ response in interviews to their responses to widely used self-report questionnaires, we were able to better understand the meaning of these scales in the context of PASC, supporting their further use. These data may be helpful in further developing digital health apps to assist persons with PASC better manage their symptoms, and our research team aims to expand these research efforts to explore our previously developed mobile app for this application.
Acknowledgments
The authors would like to thank the community members who participated in this study without whom this research would not be possible.
Disclosure
Dr Raymond L Ownby is a stockholder of and officer in entity focused on the development of digital therapeutics for Enalan Communications, Inc. In addition, Dr Raymond L Ownby has a patent Assessment of Human Comprehension by an Automate Agent pending to Nova Southeastern University. The authors report no other conflicts of interest in this work.
References
1. Ceban F, Ling S, Lui LMW, et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: a systematic review and meta-analysis. Brain Behav Immun. 2022;101:93–135. doi:10.1016/j.bbi.2021.12.020
2. Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–615. doi:10.1038/s41591-021-01283-z
3. Groff D, Sun A, Ssentongo AE, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Network Open. 2021;4(10):e2128568–e2128568. doi:10.1001/jamanetworkopen.2021.28568
4. Department of Health and Human Services. Services and Supports for Longer-Term Impacts of COVID-19. US Department of Health and Human Services; 2022.
5. Centers for Disease Control. Post-COVID conditions: information for healthcare providers; 2022. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html.
6. Nurek M, Rayner C, Freyer A, et al. Recommendations for the recognition, diagnosis, and management of long COVID: a Delphi study. Br J Gen Pract. 2021;71(712):e815–e825. doi:10.3399/bjgp.2021.0265
7. Ownby RL, Acevedo A, Waldrop-Valverde D, et al. A mobile app for chronic disease self-management: protocol for a randomized controlled trial. JMIR Res Protoc. 2017;6(4):e53. doi:10.2196/resprot.7272
8. Ownby RL, Acevedo A, Waldrop-Valverde D. Enhancing the impact of mobile health literacy interventions to reduce health disparities. Q Rev Distance Educ. 2019;20(1):15–34.
9. Lorig K, Ritter PL, Ory MG, Whitelaw N. Effectiveness of a generic chronic disease self-management program for people with type 2 diabetes: a translation study. Diabetes Educ. 2013;1:453.
10. Lorig KR, Ritter P, Stewart AL, et al. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med Care. 2001;39(11):1217–1223.
11. Lorig KR, Ritter PL, Laurent DD, Plant K. Internet-based chronic disease self-management: a randomized trial. Med Care. 2006;44(11):964–971. doi:10.1097/01.mlr.0000233678.80203.c1
12. Centers for Disease Control. Coronavirus Disease 2019 (COVID-19) 2020 Interim Case Definition, Approved August 5, 2020; 2020. Available from: https://ndc.services.cdc.gov/case-definitions/coronavirus-disease-2019-2020-08-05/.
13. Tinetti ME, Fried TR, Boyd CM. Designing health care for the most common chronic condition--multimorbidity. JAMA. 2012;203(23):2493–2494. doi:10.1001/jama.2012.5265
14. Harris PATR, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
15. Harris PATR, Minor BL, Elliott V, et al.; REDCap Consortium. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95(103208). doi:10.1016/j.jbi.2019.103208
16. Harris PA, Taylor R, Minor BL; The REDCap consortium, et al. Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
17. Hays RD, Sherbourne CD, Mazel R. User’s Manual for the Medical Outcomes Study (MOS) Core Measures of Health-Related Quality of Life. RAND Corporation; 1995.
18. Broadbent DE, Cooper PF, FitzGerald P, Parkes KR. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br J Clin Psychol. 1982;21(1):1–16. doi:10.1111/j.2044-8260.1982.tb01421.x
19. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–481.
20. Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–153. doi:10.1016/0022-3999(93)90134-2
21. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Social Behavior. 1983;24:385–396. doi:10.2307/2136404
22. Cella D, Riley W, Stone A, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J Clin Epidemiol. 2010;63(11):1179–1194. doi:10.1016/j.jclinepi.2010.04.011
23. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90013-9
24. Guest G, Namey E, Chen M. A simple method to assess and report thematic saturation in qualitative research. PLoS One. 2020;15(5):e0232076. doi:10.1371/journal.pone.0232076
25. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
26. Clarke V, Braun V. Using thematic analysis in counselling and psychotherapy research: a critical reflection. Counselling Psychotherapy Re. 2018;18(2):107–110. doi:10.1002/capr.12165
27. Guest G, MacQueen K, Namey E Applied thematic analysis. Sage; 2012. Available from: https://methods.sagepub.com/book/applied-thematic-analysis.
28. Sedgwick P. Spearman’s rank correlation coefficient. BMJ. 2014;349:g7327. doi:10.1136/bmj.g7327
29. Hemphill JF. Interpreting the magnitudes of correlation coefficients. Am Psychol. 2003;58(1):78–79. doi:10.1037/0003-066x.58.1.78
30. Funder DC and Ozer DJ. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Advances in Methods and Practices in Psychological Science. 2019;2(2):156–168. doi:10.1177/2515245919847202
31. Gignac GE and Szodorai ET. Effect size guidelines for individual differences researchers. Pers Individ Dif. 2016;102:74–78. doi:10.1016/j.paid.2016.06.069
32. Gluckman TJ, Bhave NM, Allen LA, et al. 2022 ACC expert consensus decision pathway on cardiovascular sequelae of COVID-19 in adults: myocarditis and other myocardial involvement, post-acute sequelae of SARS-CoV-2 infection, and return to play. J Am Coll Cardiol. 2022;79(17):1717–1756. doi:10.1016/j.jacc.2022.02.003
33. Brown DA, O’Brien KK. Conceptualising long COVID as an episodic health condition. BMJ Global Health. 2021;6(9):e007004. doi:10.1136/bmjgh-2021-007004
34. Eaton TL, Sevin CM, Hope AA, et al. Evolution in Care Delivery within Critical Illness Recovery Programs during the COVID-19 Pandemic: a Qualitative Study. Ann Am Thorac Soc. 2022;19(11):1900–1906. doi:10.1513/AnnalsATS.202203-255OC
35. Williamson JD, Fried LP. Characterization of older adults who attribute functional decrements to “Old Age”. J Am Geriatr Soc. 1996;44(12):1429–1434. doi:10.1111/j.1532-5415.1996.tb04066.x
36. Hurt CS, Burns A, Brown RG, Barrowclough C. Why don’t older adults with subjective memory complaints seek help? Int J Geriatr Psychiatry. 2012;27(4):394–400. doi:10.1002/gps.2731
37. Apple AC, Oddi A, Peluso MJ, et al. Risk factors and abnormal cerebrospinal fluid associate with cognitive symptoms after mild COVID-19. Ann Clin Translat Neurol. 2022;9(2):221–226. doi:10.1002/acn3.51498
38. Lamontagne SJ, Winters MF, Pizzagalli DA, Olmstead MC. Post-acute sequelae of COVID-19: evidence of mood & cognitive impairment. Brain Behav Immun Health. 2021;17:100347. doi:10.1016/j.bbih.2021.100347
39. Whiteside DM, Basso MR, Naini SM, et al. Outcomes in post-acute sequelae of COVID-19 (PASC) at 6 months post-infection Part 1: cognitive functioning. Clin Neuropsychol. 2022;36(4):806–828. doi:10.1080/13854046.2022.2030412
40. Case JB, Mackin S, Errico JM, et al. Resilience of S309 and AZD7442 monoclonal antibody treatments against infection by SARS-CoV-2 Omicron lineage strains. Nat Commun. 2022;13(1):3824. doi:10.1038/s41467-022-31615-7
41. Jacobs LG, Gourna Paleoudis E, Lesky-di bari D, et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS One. 2020;15(12):e0243882. doi:10.1371/journal.pone.0243882
42. Suyanto S, Kandel S, Kemal RA, Arfianti A. The Quality of Life of Coronavirus Disease Survivors Living in Rural and Urban Area of Riau Province, Indonesia. Infect Dis Rep. 2022;14(1):33–42.
43. Brown K, Yahyouche A, Haroon S, Camaradou J, Turner G. Long COVID and self-management. Lancet. 2022;399(10322):355. doi:10.1016/s0140-6736(21)02188-7
44. Parker AM, Brigham E, Connolly B, et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: a multidisciplinary model of care. Lancet Respir Med. 2021;9(11):1328–1341. doi:10.1016/s2213-2600(21)00166-1
45. Ros M, Neuwirth LS. Increasing global awareness of timely COVID-19 healthcare guidelines through FPV training tutorials: portable public health crises teaching method. Nurse Educ Today. 2020;91:104479. doi:10.1016/j.nedt.2020.104479
46. Schmeelk S, Davis A, Li Q, et al. Monitoring Symptoms of COVID-19: review of Mobile Apps. JMIR Mhealth Uhealth. 2022;10(6):e36065. doi:10.2196/36065
47. Agarwal P, Gordon D, Griffith J, et al. Assessing the quality of mobile applications in chronic disease management: a scoping review. Npj Digital Med. 2021;4(1):46. doi:10.1038/s41746-021-00410-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.