")
Back to Journals » Journal of Pain Research » Volume 12
Chorea and the effectiveness of steroids in a patient with the syndrome of transient headache with neurologic deficits and cerebrospinal fluid lymphocytosis: a case report
Authors Zhao L, Wang R , Fang H, Song B, Liang D, Xu Y
Received 11 February 2019
Accepted for publication 24 May 2019
Published 24 July 2019 Volume 2019:12 Pages 2247—2250
DOI https://doi.org/10.2147/JPR.S204869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Katherine Hanlon
Lu Zhao,1 Ruihao Wang,1,2 Hui Fang,1 Bo Song,1 Dongyi Liang,3 Yuming Xu1
1Department of Neurology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Department of Neurology, University of Erlangen-Nuremberg, D-91054 Erlangen, Germany; 3Department of NICU, Zhengzhou Central Hospital, Zhengzhou, Henan, People’s Republic of China
Background: The clinical manifestations of the transient headache and neurologic deficits with cerebrospinal fluid lymphocytosis (HaNDL) syndrome are variable, and involuntary movements have not been reported. The etiology and treatment of the syndrome are not entirely clarified.
Case: A 25-year-old female presented with recurrent transient headache, involuntary movements (left upper extremity chorea) and paralysis. Lumbar punctures showed intracranial hypertension and cerebrospinal fluid pleocytosis. Symptoms and intracranial hypertension were relieved after administration of steroids.
Discussion/conclusion: Chorea may also present in the HaNDL syndrome. Steroids might relieve the symptoms of the HaNDL syndrome, which indicates the possible treatment strategy for HaNDL and supports the infectious or postinfectious autoimmune etiology hypothesis.
Keywords: syndrome of transient headache and neurological deficits with cerebrospinal fluid lymphocytosis (HaNDL), involuntary movement, steroids, intracranial hypertension
Background
The syndrome of transient headache and neurologic deficits with cerebrospinal fluid (CSF) lymphocytosis (HaNDL), also known as pseudomigraine with CSF pleocytosis, is a relatively rare clinical syndrome. HaNDL presents with recurrent transient episodes of headache associated with, or preceded by, neurologic deficits.1 The clinical manifestations of neurologic deficits are variable, but involuntary movements have not been reported.2–5 Although the etiology and treatment are not entirely clarified, the infectious or postinfectious autoimmune etiology has been favored.6
We present a case of HaNDL with paroxysmal headache, left upper extremity chorea and left-sided sensorimotor symptoms. Repeated lumbar punctures showed CSF lymphocytosis and intracranial hypertension. The intracranial pressure declined and symptom recurrence was terminated after administration of methylprednisolone, which may provide new insights into etiology and treatment of this condition.
Case report
A 25-year-old right-handed woman was admitted to our hospital with a 3-week history of intermittent non-throbbing bilateral headache involving frontal and temporal lobes, accompanied by nausea, vomiting, left upper extremity numbness and weakness, left-sided tongue and perioral numbness, and involuntary movements of the left upper extremity. There were five episodes with complete recovery in the last 3 weeks, of which two episodes were without any neurologic deficit and three episodes were preceded by transient symptoms. The numbness and weakness lasted for about 10 to 20 mins and were ensued by headache and involuntary movements of the left upper extremity. The headache lasted approximately 2–9 hrs and was graded as 8/10 in the VAS (with 0 indicating no headache and 10 the most severe headache). The involuntary movements of the left upper extremity occurred in two episodes and lasted for about 1 to 2 hrs. The involuntary movements of the left upper extremity and headache occurred simultaneously after numbness and weakness of the left upper extremity, and the duration of involuntary movement was shorter than that of the headache. She was conscious during the episodes. The involuntary movements were chorea of the left upper extremity, which presented as irregular, arrhythmic and brief movements of the left hand and forearm. The chorea of the left hand was more obvious than the forearm, and the movement was remarkable during the voluntary movements. Cough, yellow sputum and snot were also reported, but no fever. She had no history or relevant family history of migraine. She had a regular menstrual cycle and no history of previous pregnancy. She did not take oral contraceptives or any other medication before the headache. She was Han Chinese and worked as an office clerk.
Upon admission, she had no symptom and the neurological examinations were unremarkable. Fundus examination revealed no papilledema or any other abnormalities. The routine blood tests and autoimmune tests were both normal. Also, the cerebral magnetic resonance imaging (with contrast medium) and angiography did not show any abnormality (Figure 1).
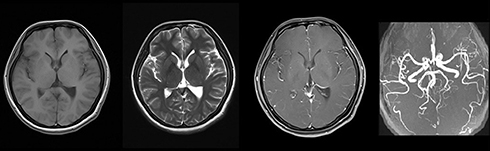 |
Figure 1 Cerebral magnetic resonance imaging and angiography. |
The first lumbar puncture at an external hospital showed intrathecal cerebrospinal fluid (CSF) opening pressure of 20cmH2O and prominent lymphocytic (90%) pleocytosis with the cell count of 114/µL.
The second lumbar puncture conducted in our hospital revealed slightly increased CSF opening pressure of 30cmH2O, and confirmed the pleocytosis with cell count of 54/µL (lymphocytes 81%). There was also increased level of protein with 5.04 g/L, but normal glucose level. Serological tests were positive for lgG coxsackie virus and lgG varicella-zoster, and CSF tests of IgM/G virus were negative. Mycobacterium tuberculosis and parasites were not detected in CSF, and oligoclonal bands were not detected as well. Electroencephalogram of asymptomatic period showed no abnormality.
Initial treatment with non-steroidal anti-inflammatory drugs, ganciclovir, mannitol and anti-epileptic medications at an external hospital did not halt the recurrence of the symptoms. During admission at our hospital, she was given ganciclovir initially, but she developed two new episodes of headache (VAS 7/10) with focal neurological symptoms, including numbness, weakness and involuntary movements of the left upper extremity. Chorea of the left hand lasted for 30–45 mins and headache for about 2 hrs. The left upper extremity weakness was graded as 4/5 using the Medical Research Council grading system. The characteristics of the episodes were similar to that described above. Meningeal irritation sign was absent during the attack.
The third lumbar puncture showed 30cmH2O of CSF opening pressure and lymphocytosis (74%). She was treated with intravenous methylprednisolone with initial dose of 120 mg/day which was tapered to 40 mg/day within 7 days. The fourth CSF examination after the administration of methylprednisolone for 7 days showed CSF opening pressure of 23cmH2O and cell number of 24/µL with 74% of lymphocytes. She did not experience any recurrence of the symptoms, and the oral methylprednisolone was discontinued gradually within 1 month. After about 1 month, she was discharged from our hospital. The final and fifth CSF examination showed CSF opening pressure of 17cmH2O and cell count of 12/µL with 79% of lymphocytes. The five CSF examinations are summarized in Table 1. At 1-year follow-up, she denied any recurrence of the symptoms. Written informed consent from the patient was obtained to perform invasive procedures and publish data. The ethics committee of our institute approved the publication of the case details.
 |
Table 1 Summary of the five cerebrospinal fluid examinations |
Discussion
The diagnostic criteria of the syndrome of HaNDL have been included in the third edition of International Classification of Headache Disorders, and are classified as a secondary headache.1 Our patient fulfills the diagnostic criteria for the syndrome of HaNDL. The diagnosis of HaNDL needs to rule out other similar diseases. Migraine with aura should be considered, since the case is about the young female with transient neurological deficits and headache.7 However, the intracranial hypertension and obvious abnormality of CSF studies can rule out the diagnosis of migraine, and the patient had no previous history or family history of migraine. The abnormality of CSF studies and paroxysmal involuntary movement may lead to the diagnosis of virus meningitis with focal epilepsy,8 but the patient was asymptomatic between attacks and had no fever or neck stiffness. The involuntary movement we observed was chorea not limb tic. Mollaret’s meningitis could present as paroxysmal course with fever, and meningeal irritation sign lasted days to weeks, and CSF Mollaret’s cell can be detected in some cases.9 Our patient had no meningeal irritation sign between attacks and the headache lasted for hours which was shorter than that of Mollaret’s meningitis. Reversible cerebral vasoconstriction syndrome and ANCA-associated vasculitis could be excluded, since the cerebral magnetic resonance imaging and blood autoimmune tests were normal.10,11
Although diverse clinical presentations of neurologic deficits are described, involuntary movements have not been reported. Gómez-Aranda presented 50 cases and reported that the most common neurologic deficit was sensory symptom (78% of episodes), followed by aphasia (66%), motor symptom (56%) and visual symptom (12%).2 The uncommon presentations such as confusional state, amnesia and cranial neuropathy have also been described.3–5 The transient neurologic deficits could occur before or during the headache.2 For our patient, the chorea occurred during the headache, while sensory and weakness occurred before the headache. To our knowledge, involuntary movements have not been described in the literature. We speculate that the involuntary movements might be caused by disorders of cerebral perfusion. Several reports showed that focal or global hemispheric hypoperfusion was observed in some HaNDL patients.2,12,13 Moreover, chorea was seen in patients with ischemic stroke or transient ischemic attack. Therefore, we suppose that the chorea of HaNDL patient might be due to local hypoperfusion involving the basal ganglia region.14
Although the pathophysiology of HaNDL remains unclear, the major hypothesis is that the viral infection triggers the immune system dysfunction and secondarily induces transient neurological symptoms by a spreading depression-like mechanism and aseptic vasculitis.6 This hypothesis is supported by the fact that approximately 25% to 50% of patients have symptoms of viral infection or fever prior to the onset of HaNDL.2,6,15 Evidence of virus infection have been reported based on the positive serology or CSF virus detection.16–18 Our patient had symptoms of upper respiratory infection. Steroid was administered in consideration of persistent intracranial hypertension and frequent symptom recurrence. Intravenous methylprednisolone 120mg/day was administered, since we considered that the high-dose of steroid could cease the disease course and its side effect was smaller than that of pulse therapy with intravenous methylprednisolone. Although the disease is benign and self-limited in most of the cases, HaNDL patients may have permanent visual sequela caused by elevated intracranial pressure.19 One report showed that methylprednisolone was effective for a HaNDL patient with obvious visual loss, papilloedema and ophthalmoplegia.19 Another case report showed frequent recurrence of the symptoms was relieved after intravenous administration of methylprednisolone 1,000 mg once daily for 5 days consecutively.16 We observed the rapid decrease of the intracranial pressure, and no further symptom recurrence after our patient was treated with methylprednisolone. The effectiveness of steroid supported the hypothesis that HaNDL could be due to an immune-mediated reaction after infection. As HaNDL is a rare disease, the standardized therapeutic strategy has not been established. Short-term use of steroid could be considered, especially when the patient has persistent elevated intracranial pressure and frequent recurrence.
In summary, we for the first time report chorea as one of the HaNDL clinical manifestations. Although the etiology of the syndrome remains unclear, the most accepted hypothesis is immune dysfunction secondary to viral infection, and therapy with glucocorticosteroid could be considered.
Clinical implications
The transient neurological symptoms of HaNDL may include chorea. Short-term use of glucocorticosteroid could be considered, especially when the patient has persistent elevated intracranial pressure and frequent recurrence.
Acknowledgment
The study was funded by Science and Technology Agency of Henan Province (152102310059).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38:1–211. doi:10.1177/0333102417738202
2. Gomez-Aranda F, Canadillas F, Marti-Masso JF, et al. Pseudomigraine with temporary neurological symptoms and lymphocytic pleocytosis. A report of 50 cases. Brain. 1997;120(Pt 7):1105–1113. doi:10.1093/brain/120.7.1105
3. Nelson S. Confusional state in HaNDL syndrome: case report and literature review. Case Rep Neurol Med. 2013;2013:317685.
4. Tada Y, Negoro K, Abe M, Ogasawara J, Kawai M, Morimatsu M. A patient of migraine-like headache with amnesia, pleocytosis and transient hypoperfusion of cerebral blood flow. Intern Med. 2005;44:743–746. doi:10.2169/internalmedicine.44.743
5. Kotan D, Sayan S, Koksal SA. A rare neurologic deficiency in HaNDL syndrome: cranial neuropathy. Arch Med Sci Atheroscler Dis. 2016;1:e49–e52. doi:10.5114/amsad.2016.60799
6. Pascual J, Valle N. Pseudomigraine with lymphocytic pleocytosis. Curr Pain Headache Rep. 2003;7:224–228.
7. Abkur TM, McGowan E, Kearney H, Counihan TJ. Getting a handle on complicated migraine. BMJ Case Rep. 2015. doi: 10.1136/bcr-2015-210763
8. Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy: position paper of the ILAE commission for classification and terminology. Epilepsia. 2017;58:522–530. doi:10.1111/epi.13670
9. Shalabi M, Whitley RJ. Recurrent benign lymphocytic meningitis. Clin Infect Dis. 2006;43:1194–1197. doi:10.1086/508281
10. Ducros A. Reversible cerebral vasoconstriction syndrome. Lancet Neurol. 2012;11:906–917. doi:10.1016/S1474-4422(12)70135-7
11. Yates M, Watts R. ANCA-associated vasculitis. Clin Med (Lond). 2017;17:60–64. doi:10.7861/clinmedicine.17-1-60
12. Pettersen JA, Aviv RI, Black SE, Fox AJ, Lim A, Murray BJ. Global hemispheric CT hypoperfusion may differentiate headache with associated neurological deficits and lymphocytosis from acute stroke. Stroke. 2008;39:492–493. doi:10.1161/STROKEAHA.107.493791
13. Burke MJ, Lamb MJ, Hohol M, Lay C. Unique CT perfusion imaging in a case of HaNDL: new insight into HaNDL pathophysiology and vasomotor principles of cortical spreading depression. Headache. 2017;57:129–134. doi:10.1111/head.12968
14. Suri R, Rodriguez-Porcel F, Donohue K, et al. Post-stroke movement disorders: the clinical, neuroanatomic, and demographic portrait of 284 published cases. J Stroke Cerebrovasc Dis. 2018;27:2388–2397. doi:10.1016/j.jstrokecerebrovasdis.2018.04.028
15. Berg MJ, Williams LS. The transient syndrome of headache with neurologic deficits and CSF lymphocytosis. Neurology. 1995;45:1648–1654. doi:10.1212/wnl.45.9.1648
16. Stelten BM, Venhovens J, van der Velden LB, Meulstee J, Verhagen WI. Syndrome of transient headache and neurological deficits with cerebrospinal fluid lymphocytosis (HaNDL): A case report with serial electroencephalography (EEG) recordings. Is there an association with human herpes virus type 7 (HHV-7) infection? Cephalalgia. 2016;36:1296–1301. doi:10.1177/0333102415618616
17. Apetse K, Breynaert L, Butaud C, et al. Transient headache and neurological deficits with cerebrospinal fluid lymphocytosis associated with igm antibodies to the epstein-barr virus viral capsid antigen. Case Rep Neurol Med. 2013;2013:975709.
18. Verentzioti A, Tavernarakis A, Mamali M, Siatouni A, Gatzonis S. Pseudomigraine with transient neurological deficits and cerebrospinal fluid lymphocytosis or HaNDL syndrome: A case report with confusion and positive IgM antibodies to CMV in serum. Cephalalgia. 2017;37:99–100. doi:10.1177/0333102416629808
19. Morrison DG, Phuah HK, Reddy AT, Dure LS, Kline LB. Ophthalmologic involvement in the syndrome of headache, neurologic deficits, and cerebrospinal fluid lymphocytosis. Ophthalmology. 2003;110:115–118.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.