")
Back to Journals » Patient Preference and Adherence » Volume 15
Chinese Parents’ Perceptions, Attitudes, and Treatment-Seeking Intentions Toward Congenital Heart Disease with Charitable Assistance: A Cross-Sectional Study in a Congenital Heart Center in Southern China
Authors Xie WP, Liu JF, Lei YQ, Cao H , Chen Q
Received 23 August 2021
Accepted for publication 27 October 2021
Published 5 November 2021 Volume 2021:15 Pages 2459—2466
DOI https://doi.org/10.2147/PPA.S335567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Wen-Peng Xie,1– 4,* Jian-Feng Liu,1– 4,* Yu-Qing Lei,1– 4 Hua Cao,1– 4 Qiang Chen1– 4
1Department of Cardiac Surgery, Fujian Branch of Shanghai Children’s Medical Center, Fuzhou, People’s Republic of China; 2Fujian Children’s Hospital, Fuzhou, People’s Republic of China; 3Fujian Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 4Fujian Key Laboratory of Women and Children’s Critical Diseases Research, Fujian Maternity and Child Health Hospital, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiang Chen; Hua Cao
Department of Cardiac Surgery, Fujian Branch of Shanghai Children’s Medical Center, Fuzhou, People’s Republic of China
Email [email protected]; [email protected]
Objective: To investigate the perceptions, attitudes and treatment-seeking intentions of Chinese parents toward charitable assistance for congenital heart disease (CHD).
Methods: This was a cross-sectional study, and different questionnaires were used. Data on Chinese parents’ perceptions, attitudes, and treatment-seeking intentions toward charitable assistance for CHD were collected and analyzed.
Results: A total of 220 parents of children with CHD were included in the survey, and 201 completed the survey. The results showed that the perception rate of charity assistance for CHD was only 44.8%, and the channels of understanding were narrow. The majority of participants (98.0%) approved of charitable assistance. A total of 79.1% of the parents thought that charity assistance would improve their treatment-seeking intentions, and 62.7% of the parents answered that it would affect their medical institutions’ choice. The results also showed that higher treatment-seeking intention was significantly correlated with higher income and charitable assistance but not with the parents’ education level. Correlation analysis found that parents with different monthly incomes and charitable assistance had statistically significant treatment-seeking intentions. Analyzing the factors of surgical treatment in our hospital, it was found that charitable assistance was an essential factor influencing them to choose treatment.
Conclusion: Many Chinese parents of patients with CHD did not know about charity assistance, but most of them approved the project. Charitable assistance could improve parents’ treatment-seeking intentions.
Keywords: perceptions, attitudes, treatment-seeking intention, CHD, charitable assistance
Introduction
Congenital heart disease (CHD) is the most common congenital disability, with approximately 8 affected individuals per 1000 live births worldwide, and genetic factors are often responsible for the occurrence of CHD.1,2 Due to the development of medical technology and resources, an increasing number of patients with CHD have been diagnosed and treated.3,4 However, due to regional economic backwardness and uneven social development, patients in impoverished areas with insufficient medical equipment have not been diagnosed or treated until adolescence and adulthood.5–7 With the disease’s progress, repeated pneumonia, and decreased patient activity, CHD will affect children’s growth, development, and quality of life. Therefore, early treatment should be striven for in children with surgical correction.8,9 It has been reported that medical costs related to congenital cardiovascular abnormalities account for over half of all medical costs for congenital disabilities.10 For families with economic difficulties, the parents cannot raise enough funds so that the children fail to receive timely diagnostic testing and treatment and lose the opportunity for surgery, eventually leading to poor quality of life or loss of life. Additionally, the lack of funds after treatment makes it difficult for families to maintain follow-up life.10–12 Although China has a wide range of medical insurance coverage, the reimbursement rate of most rural residents is low; therefore, it is still difficult for some families to pay for high cardiac surgery. Increasing charitable assistance projects have been completed to solve the problem of medical treatment difficulties for children with CHD in low-income families. Exceptional help and support have been implemented for low-income families unable to afford treatment due to illness13 (eg, support 85% of the cost after the patient’s medical insurance reimbursement, assuming that the total treatment cost is $8000, and the final patient must pay only $840). Previous studies have found that charitable assistance can improve patients’ treatment compliance and reduce family burden,14,15 but no study has examined medical institutions’ selectivity and treatment-seeking intention. The purpose of this study was to investigate the perceptions and attitudes of Chinese parents toward charitable assistance for CHD and whether charitable assistance would improve their treatment-seeking intentions.
Methods and Materials
Ethical Consideration
Before participating in the study, participants were informed of the purpose and content of the study. All participants provided written informed consent. They were also informed that their participation was entirely voluntary, and they had the right and freedom to withdraw from the study at any time without giving any reason. This study was approved by the ethics committee of Fujian Maternity and Child Health Hospital and conducted in accordance with the Declaration of Helsinki.
Study Design
A cross-sectional survey was used that consisted of a paper- and data-collected self-administered questionnaire from our hospital between January 2020 and January 2021.
Research Object
The subjects were parents of children who were diagnosed with CHD and were hospitalized and prepared for surgical treatment in our center. The types of CHD in the study population included ventricular septal defect (VSD), atrial septal defect (ASD), patent ductus arteriosus (PDA), and other types (tetralogy of Fallot, stenosis of pulmonary artery, double chamber of right ventricle, and so on). The exclusion criteria were as follows: 1. Parents who could not read the questionnaire or communicate with others. Parents who were unwilling or unable to sign an informed consent form and participate in this study. A total of 220 parents were enrolled in this study. No other charitable assistance was received for any parents before our questionnaire survey.
Research Tool
The questionnaire used in this study was independently designed and used in simplified Chinese. This four-page questionnaire included those data in four areas: (1) sociodemographic conditions (six items), (2) perception of charitable assistance for CHD (five items), and (3) attitude toward charitable assistance for CHD (six items). (4) Treatment-seeking intention and its related factors. All the content was determined based on relevant literature, including socioeconomic factors, family income, education status, social and economic assistance, and medically related factors (technology level, serviceability, medical environment, etc.). We measured parents’ treatment-seeking intention by studying their willingness to pay (parents actively cooperated with doctors, or poor families raised funds to allow children to continue to receive treatment, that is, the enthusiasm of family members to treat their children). We assumed that this was the willingness to treat. There were three possible answer options for some questions (Yes/No/Unclear), and the remaining questions had multiple answer options.
Data Collection
A total of 220 parents of children with CHD participated in the study, and 201 participants completed the questionnaire. The questionnaire was self-administered and filled out individually by the participants under the research team’s strict supervision, which acted as an intermediary to monitor the participants. Our researchers were rigorously trained on quality control of the on-site questionnaire. When the participants refuted any questions, our researchers could help them solve the problem, such as by explaining the participants’ issues and translating the question into the local language. To ensure accuracy, two different researchers entered the data separately.
Statistical Analysis
The data were analyzed using SPSS version 25.0 (IBM, Armonk, New York). Univariate analysis was used to describe the frequency and percentage of categorical variables. Descriptive statistics were used to identify the participants’ demographic characteristics and their perceptions and attitudes toward charitable assistance programs for CHD. The relationship between treatment-seeking intention and treatment cost under different conditions was analyzed using the curve graph. The influence of education and monthly income on treatment-seeking intention was determined by multifactor analysis, and the influence of charitable assistance on treatment-seeking intention was analyzed by logistic regression. A p value< 0.05 was defined as statistically significant.
Results
A total of 220 parents participated in the study, of which 201 parents completed the questionnaire survey. The demographic characteristics of the participants are shown in Table 1. The mean age of the 201 participants was 27.9±5.3 years. Part of the participants (48.3%) had completed their senior secondary education, 23.4% had a bachelor’s degree or above, and 28.3% had a junior high school or below. Approximately 58.7% of the participants lived in cities. Most parents had a monthly income of 5001–10,000 China Yuan (CNY) (50.7%), 19.4% had an income of 10,001–20,000 CNY, 21.9% had less than 5000 CNY, and 8.0% had an income of more than 20,000 CNY.
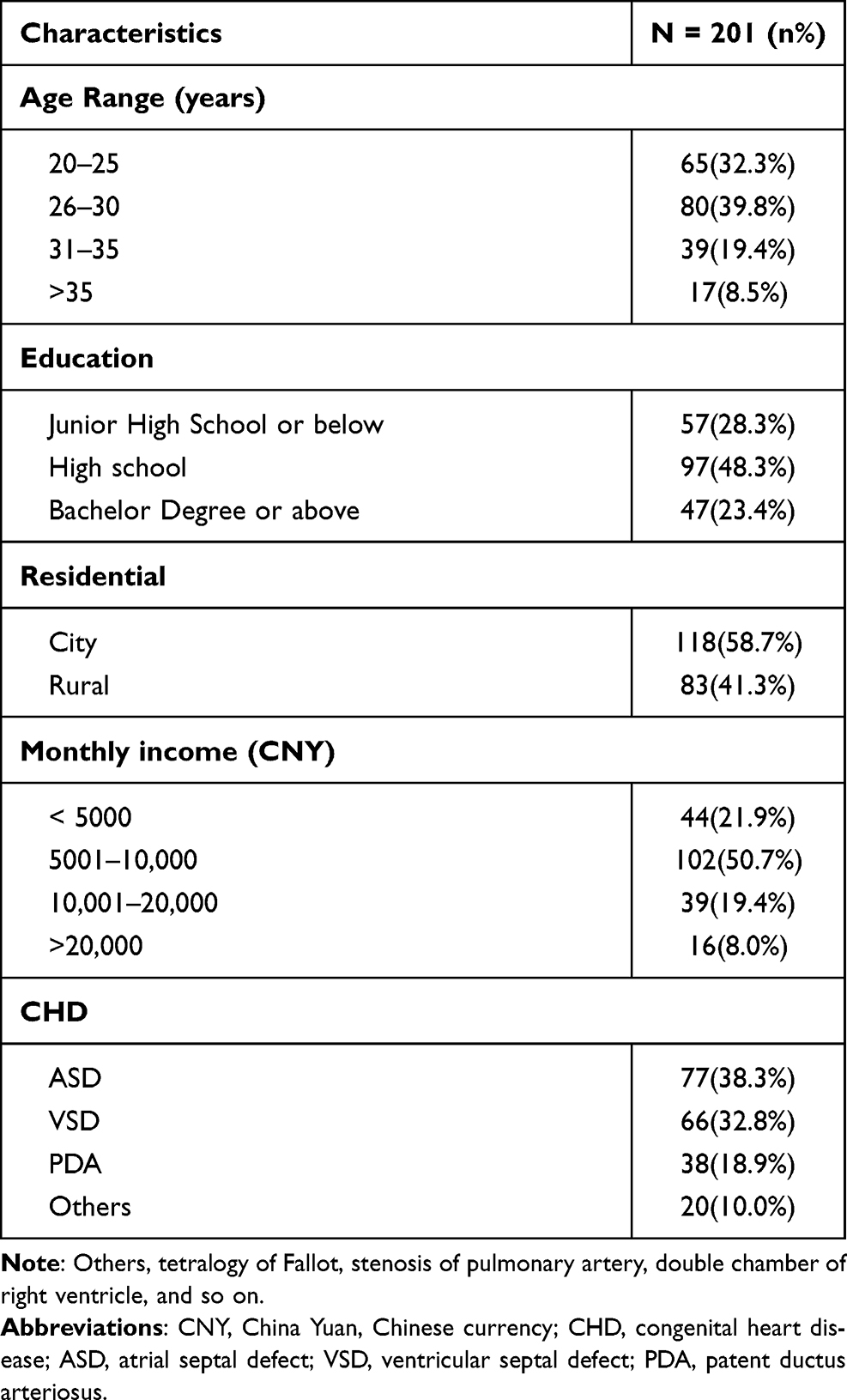 |
Table 1 Baseline Socio-Demographic Characteristics of Participants |
Perception and Attitude Toward Charity Assistance for CHD
More information about the respondents’ perception of charitable assistance programs for CHD is shown in Table 2. Only 44.8% (n=90) of the respondents knew about the CHD charitable assistance program, while the rest (55.2%) had not heard of it. Of those who knew about the program, nearly 33.8% of respondents knew the assistance program’s main evaluation criteria, and approximately 11.9% of parents knew the specific amount of assistance. In the eligibility inquiry, 59.2% of the families felt that their children were eligible for the charitable assistance program. They learned about charitable assistance programs for CHD through hospital billboards and messages from doctors or friends.
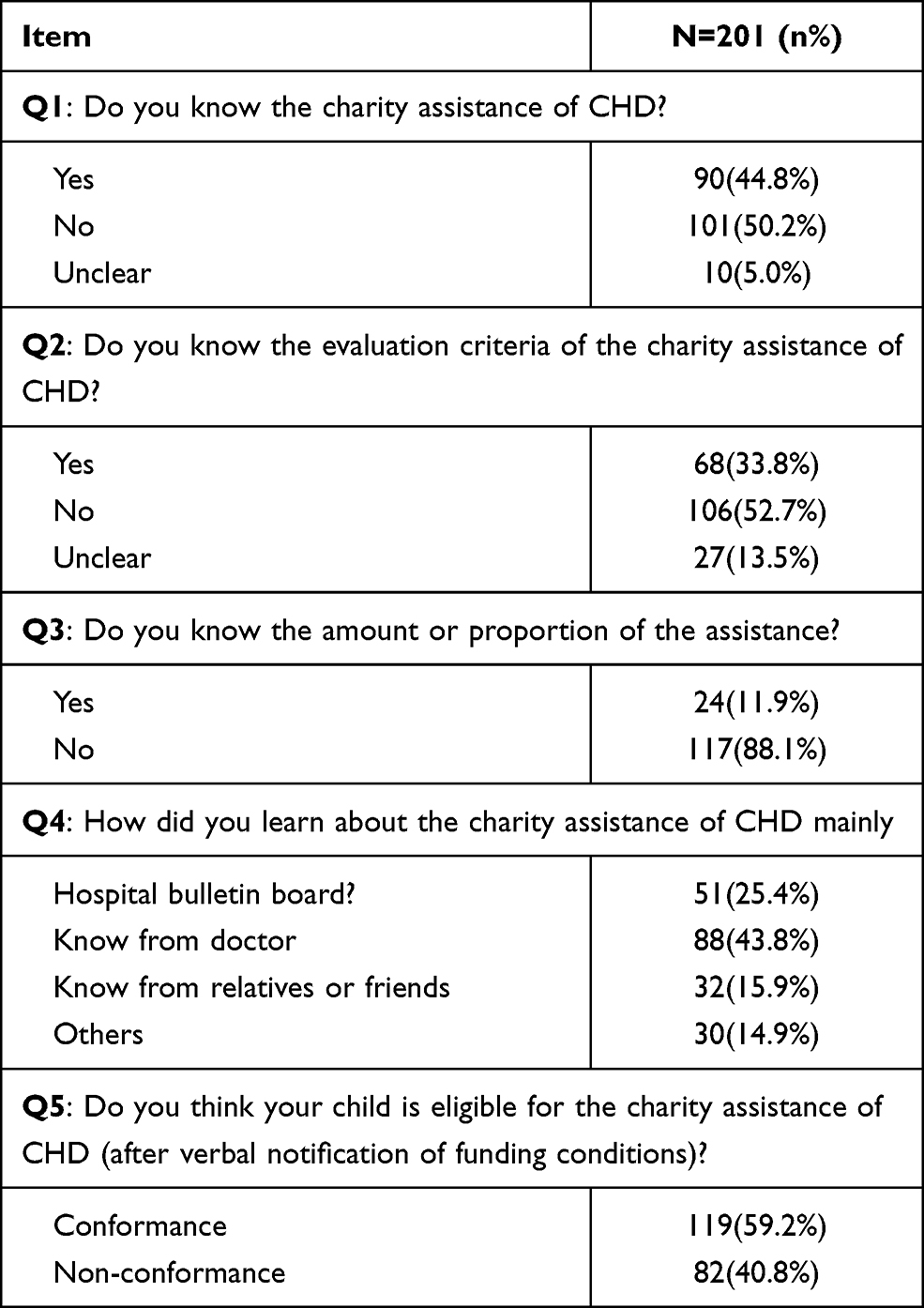 |
Table 2 Participants’ Perception of the Charity Assistance for CHD |
For charitable assistance, 98% (n=199) of parents felt it was necessary (Table 3), and their responses were as follows: a. It could help reduce medical expenses for low-income families (98.0%). b. It was helpful to increase the treatment-seeking intention of parents (68.7%). c. It helped to promote the treatment compliance of parents (49.2%). A total of 56.2% of parents thought it was difficult for them to pay medical expenses and needed charitable assistance support, and 92.5% of parents answered that the evaluation criteria of charitable assistance programs were reasonable. Approximately 62.7% of parents said they would prefer to be treated in this hospital if they met the criteria for the charitable assistance program (receiving 85% subsidy), and 79.1% of parents answered that it would increase their treatment-seeking intentions. Finally, among the treatment expenses received, most parents felt that they could afford the expenses within 20,000 to 50,000 CNY (54.7%), 28.9% of parents could afford less than 20,000 CNY, and only a small number of parents could afford more than 50,000 CNY (16.4%).
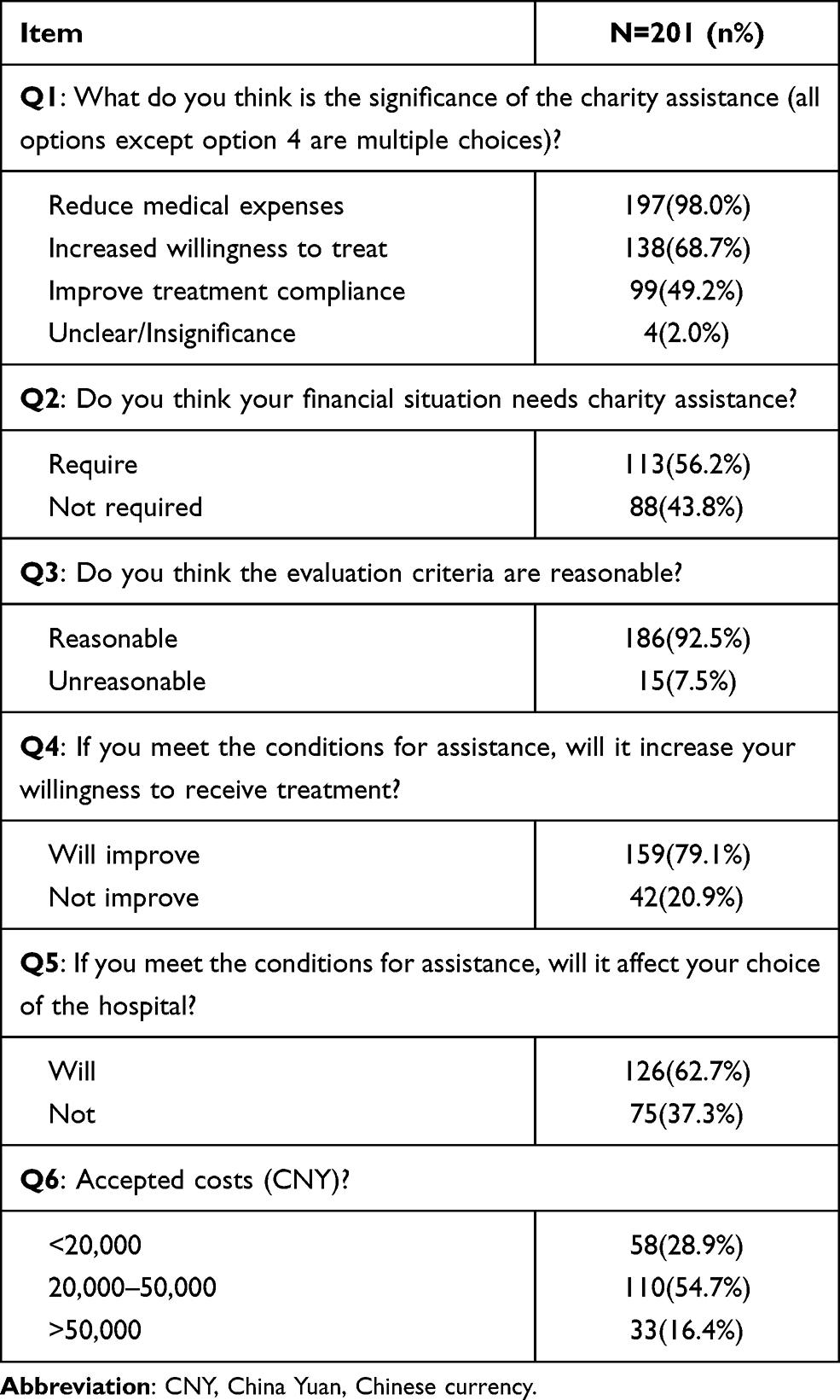 |
Table 3 Attitudes to Charity Assistance for CHD and Affordable Medical Costs |
Influencing Factors on Treatment-Seeking Intention and Their Correlation Analysis
Figure 1A–C shows that changes in parents’ treatment-seeking intention increase treatment costs under the circumstances of parents’ different levels of education, income, and charitable assistance. According to the treatment costs and willingness to pay for treatment, the graph was generated under different factors. Figure 1B shows a significant correlation between higher treatment-seeking intention and higher income levels as the treatment costs change but no significant correlation with parents’ education level (Figure 1A). Figure 1C shows that parents who received charitable assistance had a greater treatment-seeking intention when the treatment cost was more than 100,000 CNY.
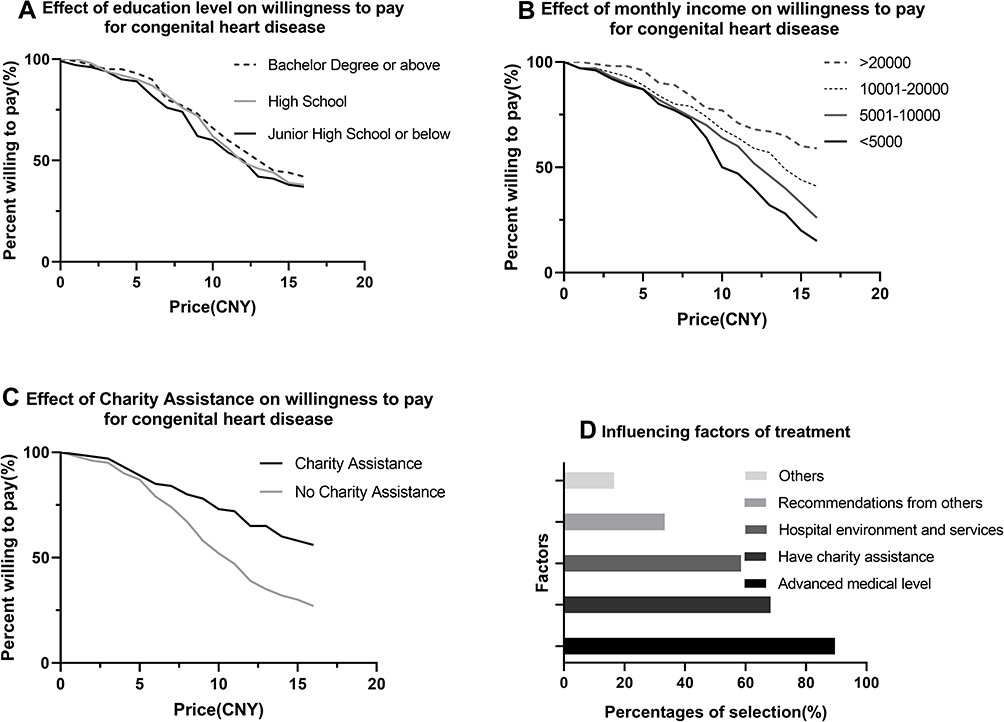 |
Figure 1 Factors affecting parents’ willingness to pay and treatment in our hospital for children with congenital heart disease. ((A) Willingness to pay in patients according to education level. (B) Willingness to pay in patients according to income. (C) Willingness to pay in patients according to charity assistance. (D) Factors of parents’ choice of treatment in our hospital). Abbreviation: CNY, China Yuan, Chinese currency. |
Table 4 shows the factors that influence respondents’ treatment-seeking intention. Education level and monthly income were included to construct a multifactor linear regression equation. The results showed that monthly income had a statistically significant effect on parents’ treatment-seeking intentions (P<0.05, b=1.87, t=4.96), and education level did not affect treatment-seeking intentions (P=0.089). Charitable assistance was taken as the dependent variable, and treatment-seeking intention was taken as the covariate; the results showed that charitable assistance had a statistically significant effect on treatment-seeking intention (OR=4.43, 95% CI: 2.47–7.48, P<0.01).
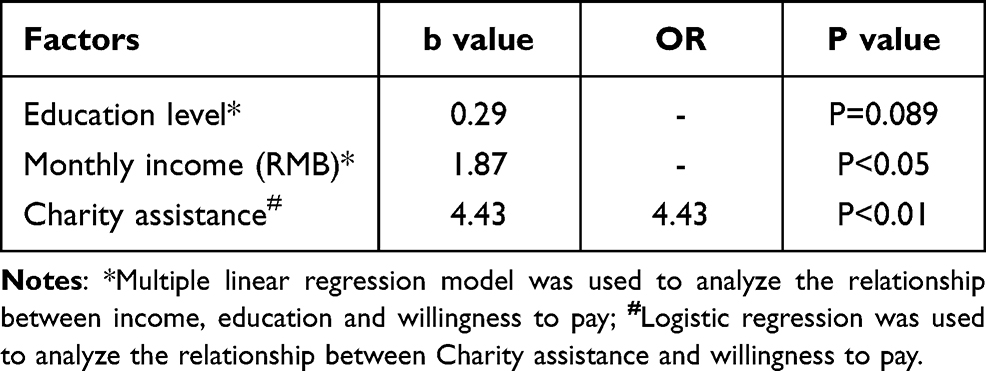 |
Table 4 Correlation Analysis of Influencing Willingness to Pay |
Factor Analysis of Received Treatment
Figure 1D analyzed the factors that influenced the choice to receive treatment in our hospital (multiple choices). It was found that 68.32% of parents answered that the hospital had a charitable assistance policy as one of the reasons for their choice; 89.56% of parents answered that this hospital had an advanced medical level; 58.54% of parents answered that the hospital had high-quality service and environment; 33.29% of parents answered that the hospital was recommended by relatives and friends; other answers accounted for 16.58% of parents, who were influenced by information from the WeChat platform, online registration platform, short videos, etc.
Discussion
CHD is the most common congenital disability, and the survival rate of these children increases as medical technology improves. Postoperative quality of life and survival time are also significantly increased.1–4,16 With the improvement and popularization of prenatal color ultrasound screening technology, most patients with severe and complex CHD are diagnosed before birth, and pregnancy is terminated. Most unterminated pregnant fetuses need further interventional or surgical treatment.17,18 However, in some Chinese regions and other impoverished areas, due to the relatively backward economy and education, limited distribution of medical resources, lack of standardized prenatal screening, or inferior technology, the prevalence of CHD remains high.19 In addition, as a result of economic backwardness, most children do not receive medical treatment in time.20,21 Whether to receive treatment and the time of treatment-seeking intention have a significant impact on the patients’ futures, such as life expectancy, quality of life, career planning, daily life, and a far-reaching impact on the family.22,23 To enable more children with CHD to receive timely treatment, charitable assistance programs can be used to provide special help and support to low-income families who cannot afford treatment.
In recognition of charitable assistance for CHD, we concluded that only 44.8% of the respondents knew about the charitable assistance program, and the awareness rate of low-income families was even lower. Among those who knew about the program, nearly 33.8% knew the assistance program’s main evaluation criteria, and approximately 11.9% of the respondents knew the specific amount of assistance (assistance rate) and the method of assistance. We conclude that the popularity and publicity of charitable assistance programs for CHD were low, especially in rural and mountainous areas. Respondents knew about the assistance program mainly through hospital bulletin boards, doctors, and friends. However, only 14.9% of respondents knew about the program through the internet (such as WeChat, online registration platforms, short videos, etc.). The rapid development of information technology has promoted medical consultation convenience, especially during the COVID-19 epidemic.24 Therefore, we could publicize and promote the charitable assistance program with the assistance of the internet and reduce the congestion of information caused by the uneven distribution of medical care and the lack of traffic in rural areas. In the future, we will cooperate and communicate with primary health care units, especially the corresponding maternal and child health centers and children’s hospitals, so that they can directly make corresponding charitable introductions to families suffering from CHD. At the same time, a network consultation platform should be established to further refer children who need surgical treatment or financial assistance to our hospital for treatment.
In terms of the attitude toward charitable assistance for CHD, most respondents affirmed this public welfare project, and most of the participants thought that the evaluation criteria were reasonable. If the participants were eligible for the assistance program, approximately 79.1% of the respondents thought that it would improve their treatment-seeking intentions, and 62.7% of the participants said they would ask to choose this heart center for treatment. Therefore, the charity assistance program is a reasonable project that can help poor families receive surgical treatment at an early stage. At present, we are working to further improve the details and simplify the application procedures according to the opinions of patients’ families, making it easy for the patient’s family to complete the application process. At the same time, every family member who is admitted to the hospital will be fully educated, so they can have sufficient time to prepare the application materials. The graph analysis concluded that there was a significant correlation between higher treatment-seeking intentions and higher income levels. Nevertheless, there was no significant effect on parents’ education levels (perhaps parents were aware of the seriousness of CHD, and surgery was the only way to save lives for most children). Parents who received charitable assistance had greater treatment-seeking intentions when the treatment cost was more than 100,000 CNY. We further confirmed this result through correlation analysis and found that monthly income and charitable assistance had a significant effect on treatment-seeking intention. Treatment for CHD is relatively expensive (especially for those patients who had been in the ICU for a long time), and poor families might stop treatment. Therefore, we needed to have a detailed understanding of the financial situation of the patients’ families. Finally, we found that a charitable assistance program was an essential factor influencing patients and parents to see a doctor, which potentially impacted the improvement of the hospital’s competitiveness.
Implementing the charitable assistance program for CHD effectively reduced low-income family medical costs and promoted timely treatment. We concluded that most of the parents affirmed the charitable assistance program and were satisfied with the evaluation criteria. To make rational use of the funds, we must exclude rich participants from the scope of assistance, give a reasonable explanation to these families who are not included and reduce unnecessary conflicts. From the perspective of treatment-seeking intentions, providing additional assistance to families with high financial stress could help them treat the disease at an early stage, promote parents’ treatment-seeking intentions, improve the quality of life of their children, and avoid the need for more expensive treatment in the future. The assistance program reduced the economic pressure and avoided the occurrence of poverty caused by illness at the family level. In terms of medical competitiveness, charitable assistance also stimulated medical demand and affected the choice of hospital. Simultaneously, the program reminded us that high-quality medical services are essential points to improve hospitals’ comprehensive strength.
Limitations
There were several limitations in this study. The data were collected through self-administered questionnaires, and some of the respondents might not have fully understood the issues presented, leading to potential bias. This study was a single-center study, and the results represented the characteristics of individuals in only our center. This study was a cross-sectional study with a large selection bias, and there was no similar study before; a longitudinal comparison was impossible to make. A group of unassisted patients should be used as a control group to better assess treatment-seeking intention and improve the comparability of the results.
Conclusion
In our study, only 44.8% of respondents were aware of the charitable assistance program for CHD, and most of them approved of the program. Implementing charitable assistance can effectively encourage early intervention for children with CHD and improve their parents’ treatment-seeking intentions, especially for families with low incomes. Hospitals can effectively influence patients to seek medical treatment and improve the competitiveness of hospitals.
Acknowledgments
We highly acknowledge the contribution of the participating doctors: Qi-Liang Zhang, Ze-Wei Lin, Wang-Sheng Dai, Li-Wen Wang and Ling-Shan Yu. We hope humans eventually defeat COVID-19. Hua Cao and Qiang Chen are co-correspondence authors for this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. van der Linde D, Konings EEM, Slager MA, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58(21):2241–2247. doi:10.1016/j.jacc.2011.08.025
2. Gug C, Stoicanescu D, Mozos I, et al. De novo 8p21.3→ p23.3 duplication with t(4;8)(q35;p21.3) translocation associated with mental retardation, autism spectrum disorder, and congenital heart defects: case report with literature review. Front Pediatr. 2020;8:375. doi:10.3389/fped.2020.00375
3. Mat Bah MN, Sapian MH, Jamil MT, et al. The birth prevalence, severity, and temporal trends of congenital heart disease in the middle-income country: a population-based study. Congenit Heart Dis. 2018;13(6):1012–1027. doi:10.1111/chd.12672
4. Helm PC, Bauer UMM, Abdul-Khaliq H, et al. Patients with congenital heart defect and their families support genetic heart research. Congenit Heart Dis. 2018;13(5):685–689. doi:10.1111/chd.12630
5. Leca F, Karam J, Vouhe PR, et al. Surgical treatment of multiple ventricular septal defects using a biologic glue. J Thorac Cardiovasc Surg. 1994;107(1):96–102. doi:10.1016/S0022-5223(94)70458-9
6. Hirata Y, Hirahara N, Murakami A, Motomura N, Miyata H, Takamoto S. Current status of cardiovascular surgery in Japan 2013 and 2014: a report based on the Japan Cardiovascular Surgery Database. 2: congenital heart surgery. Gen Thorac Cardiovasc Surg. 2018;66(1):4–7. doi:10.1007/s11748-017-0841-6
7. Serraf A, Bruniaux J, Lacour-Gayet F, et al. Anatomic correction of transposition of the great arteries with ventricular septal defect. Experience with 118 cases. J Thorac Cardiovasc Surg. 1991;102(1):140–147. doi:10.1016/S0022-5223(19)36593-6
8. Costello CL, Gellatly M, Daniel J, Justo RN, Weir K. Growth restriction in infants and young children with congenital heart disease. Congenit Heart Dis. 2015;10(5):447–456. doi:10.1111/chd.12231
9. Ferentzi H, Pfitzer C, Rosenthal L-M, Berger F, Schmitt KRL. Long-term early development research in congenital heart disease (LEADER-CHD): a study protocol for a prospective cohort observational study investigating the development of children after surgical correction for congenital heart defects during the first 3 years of life. BMJ Open. 2017;7(12):e018966.
10. Allison Russo C, Elixhauser A. Hospitalizations for birth defects, 2004: statistical brief #24. Healthcare Cost and Utilization Project (HCUP) statistical briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2007.
11. Raj M, Paul M, Sudhakar A, et al. Micro-economic impact of congenital heart surgery: results of a prospective study from a limited-resource setting. PLoS One. 2015;10(6):e0131348. doi:10.1371/journal.pone.0131348
12. Ludomirsky AB, Bucholz EM, Newburger JW. Association of financial hardship because of medical bills with adverse outcomes among families of children with congenital heart disease. JAMA Cardiol. 2021;6(6):713–717. doi:10.1001/jamacardio.2020.6449
13. Nathan PC, Henderson TO, Kirchhoff AC, Park ER, Robin Yabroff K. Financial hardship and the economic effect of childhood cancer survivorship. J Clin Oncol. 2018;36(21):2198–2205. doi:10.1200/JCO.2017.76.4431
14. Li Z, Wu J, Zhao Y, et al. Influence of medical insurance schemes and charity assistance projects on regular prophylaxis treatment of the boys with severe haemophilia A in China. Haemophilia. 2018;24(1):126–133. doi:10.1111/hae.13372
15. Fanaroff AC, Peterson ED, Kaltenbach LA, et al. Association of a P2Y12 inhibitor copayment reduction intervention with persistence and adherence with other secondary prevention medications: a post hoc analysis of the ARTEMIS cluster-randomized clinical trial. JAMA Cardiol. 2020;5(1):38–46. doi:10.1001/jamacardio.2019.4408
16. Jenkins KJ, Correa A, Feinstein JA, et al.; American Heart Association Council on Cardiovascular Disease in the Young. Noninherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007;115(23):2995–3014. doi:10.1161/CIRCULATIONAHA.106.183216
17. Qiu X, Weng Z, Liu M, et al. Prenatal diagnosis and pregnancy outcomes of 1492 fetuses with congenital heart disease: role of multidisciplinary-joint consultation in prenatal diagnosis. Sci Rep. 2020;10(1):7564. doi:10.1038/s41598-020-64591-3
18. Marantz P, Grinenco S, Pestchanker F, Meller CH, Izbizky G. Prenatal diagnosis of CHDs: a simple ultrasound prediction model to estimate the probability of the need for neonatal cardiac invasive therapy. Cardiol Young. 2016;26(2):347–353. doi:10.1017/S1047951115000293
19. Zhao L, Chen L, Yang T, et al. Birth prevalence of congenital heart disease in China, 1980–2019: a systematic review and meta-analysis of 617 studies. Eur J Epidemiol. 2020;35(7):631–642. doi:10.1007/s10654-020-00653-0
20. Knowles RL, Ridout D, Crowe S, et al. Ethnic and socioeconomic variation in incidence of congenital heart defects. Arch Dis Child. 2017;102(6):496–502. doi:10.1136/archdischild-2016-311143
21. Peyvandi S, Baer RJ, Moon-Grady AJ, et al. Socioeconomic mediators of racial and ethnic disparities in congenital heart disease outcomes: a population-based study in California. J Am Heart Assoc. 2018;7(20):e010342. doi:10.1161/JAHA.118.010342
22. Ladouceur M, Iserin L, Cohen S, Legendre A, Boudjemline Y, Bonnet D. Key issues of daily life in adults with congenital heart disease. Arch Cardiovasc Dis. 2013;106(6–7):404–412. doi:10.1016/j.acvd.2013.02.004
23. Xiang L, Su Z, Liu Y, et al. Impact of family socioeconomic status on health-related quality of life in children with critical congenital heart disease. J Am Heart Assoc. 2019;8(1):e010616. doi:10.1161/JAHA.118.010616
24. Wiegand S, Marggraf J, Wilhelm T, Eivazi B, Werner JA. Internet-mediated physician-patient interaction focusing on extracranial hemangiomas and vascular malformations. Head Neck. 2014;36(2):187–190. doi:10.1002/hed.23282
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.