")
Back to Journals » Cancer Management and Research » Volume 11
Chinese expert consensus on diagnosis and treatment of nasopharyngeal carcinoma: evidence from current practice and future perspectives
Authors Lang J , Hu C, Lu T, Pan J, Lin T
Received 8 December 2018
Accepted for publication 16 May 2019
Published 10 July 2019 Volume 2019:11 Pages 6365—6376
DOI https://doi.org/10.2147/CMAR.S197544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Jinyi Lang*,1 Chaosu Hu*,2 Taixiang Lu,3 Jianji Pan,4 Tongyu Lin5
1Department of Radiation Oncology, Sichuan Cancer Hospital and Institute, Sichuan Cancer Center, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Department of Radiation Oncology, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 3Department of Radiation Oncology, State Key Laboratory of Oncology in Southern China, Sun Yat-sen University Cancer Center, Collaborative Innovation Center for Cancer Medicine, Guangzhou, People’s Republic of China; 4Department of Radiation Oncology, Fujian Cancer Hospital & Fujian Medical University Cancer Hospital, Fuzhou, People’s Republic of China; 5Department of Medical Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in Southern China, and Collaborative Innovation Center of Cancer Medicine, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Abstract: Nasopharyngeal carcinoma (NPC) is a rare type of head and neck cancer, with a higher incidence reported only in Southeast Asia and Northern Africa. Owing to the rarity of NPC occurrence, no internationally accepted consensus or guideline for its diagnosis and treatment is available. Based on the current evidences and practices, the Chinese experts on multidisciplinary diagnosis and treatment of NPC were designated to develop a national consensus for the treatment strategy of NPC. In this consensus, we report the development for improving the treatment efficacy and quality of life of NPC patients in China. The consensus also describes and recommends the role of multidisciplinary management approach in the management of NPC. A multidisciplinary team should include experts from different domains who can cater to the individualized needs of patients with NPC in a much more efficient manner. In addition, the team may also play a key role in developing guiding principles for future research, contributing to the improvement in the management of NPC.
Keywords: Asian, Chinese, consensus, nasopharyngeal carcinoma, radiotherapy
Introduction
Nasopharyngeal carcinoma (NPC) is a relatively rare type of malignancy worldwide, with an age-standardized rate (ASR) of 1.2 per 1,00,000 person-year and a death rate of 0.7 per 1,00,000 person-year.1 However, NPC is highly prevalent among the populations of the developing and underdeveloped countries in Southeast Asia, East Asia, and Northern Africa.1–3 In China, the ASR and death rate of NPC are 2.0 and 1.2 per 1,00,000 person-years, respectively, which are much higher than the average rate worldwide. Furthermore, morbidity and mortality vary with race and geographical area in China. Southern China, especially Hong Kong and Guangdong, has reported an incidence rate of 20–30 per 1,00,000 person-year, which is over 10 times than the average.4
Although NPC is histopathologically classified as keratinizing squamous cell carcinoma (with varying degrees of differentiation), non-keratinizing carcinoma (differentiated and undifferentiated types), and basaloid squamous cell carcinoma by the World Health Organization,5 its etiology is not completely known. The occurrence of NPC is considered to be the result of interactions between Epstein-Barr virus (EBV) infection, genetic and environmental factors such as alcohol consumption and smoking, and consumption of salted fish,3,6,7 with EBV infection playing a major role.6 Other than the conventionally known risk factors of NPC, nose/ear infections have been found to be associated with NPC in China.8–10 Prognosis of NPC has been found to be associated with TNM staging, primary tumor size, biomarkers such as circulating plasma DNA, EBV DNase-specific neutralizing antibody, lactate dehydrogenase (LDH), beclin-1, galectin-3, and other associated comorbidities.11,12
Accurate and appropriate clinical staging plays a key role in the diagnosis and management of cancer. Owning to the higher incidence of NPC reported in China and the advances in diagnostic and therapeutic area, the Chinese Committee for Staging of Nasopharyngeal Carcinoma (CCSNPC) revised the previously validated 1992 Chinese staging system on December 16, 2008 and a new version of the clinical staging was recommended in the same year by CCSNPC. However, further evidences are warranted to validate the effectiveness, and further improve the staging system used in China.13 In order to facilitate the comparison and exchange of data and results between the different research centers, the TNM classification used the seventh edition of the American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC) staging system.14 However, with the progress of radiodiagnosis and radiotherapy, the current AJCC/UICC staging system needs further evaluation for its applicability and improvement, especially for NPC.
The routine clinical staging identification in NPC includes medical history, physical examination (including cranial nerve examination), complete blood biochemical analysis including complete blood count, liver and kidney function tests, EBV DNA copy, chest computed tomography (CT), nasopharyngoscopy and CT or magnetic resonance imaging (MRI) of nasopharynx, skull base and neck. MRI is an initial choice; however, each center can choose the best imaging tools based on daily clinical practices and experiences. For high risk patients (those with N3 disease or biochemical abnormalities), isotope bone scans or CT scans of the upper abdomen and chest are recommended. Positron emission tomography (PET-CT), with better sensitivity, specificity and accuracy is a replacement of traditional techniques for the diagnosis of distant metastasis while PET-MRI may play a role in the staging of NPC.
According to the current TNM staging, NPC patient is diagnosed as N3 when there are unilateral or bilateral metastasis in cervical node(s), invading below the caudal border of cricoid cartilage including those extending to the supraclavicular fossa (SCF). SCF described by Ho is a triangular region which is bounded anatomically by the superior margin of the sternal head and the lateral edge of the clavicle and the area of shoulder and neck confluence. However the definition of N3 is mostly based on clinical examination15 and there are some concerns while demarcating the SCF radiologically as the area may extend to lower neck including the IV and Vb areas.16 Evidences from recent studies have reported an assessment of radiological lower levels (LL) IV and Vb as a potential replacement for the SCF in the demarcating criteria for the N3 category.16,17 This newly defined area can be assessed by imaging tools and will not influence the overall prognosis of N3. Similarly, there is a lack of universal consensus on the significance of involvement of various muscles in defining the T4 stage in NPC, thereby affecting the treatment and prognosis. According to the current definition, NPC with intracranial extension and/or involvement of cranial nerves, hypopharynx, or orbit, parotid gland, and/or extensive soft tissue infiltration beyond the lateral surface of the lateral pterygoid are defined as stage T4. Even though the patients with tumor invasion limited to the exoskeleton muscle are categorized as T4, they have a better prognosis, comparable to that of T2 phase. Hence clarification and the need to redefine the criteria are considered necessary.5,18 As per the consensus, we recommend the T-staging as suggested by Ng et al (Box 1).5
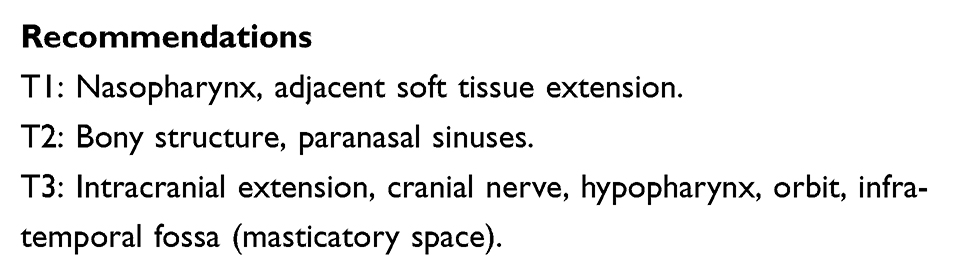 |
Box 1: Tumor staging in nasopharyngeal carcinoma |
Pan et al (2016) analyzed 1609 NPC patients treated with IMRT using the seventh AJCC/UICC staging system and suggested that the difference between adjacent stages in patients with non-metastatic cancer need to be improved. Based on these findings, the author proposed the changes for the eighth edition of the AJCC/UICC staging system for NPC. The changes recommended are changing medial pterygoid/lateral pterygoid involvement from T4 to T2, adding prevertebral muscle involvement as T2, replacing the SCF with the lower neck, merging this with a maximum nodal diameter of >6 cm as N3, and classifying T4 and N3 collectively as stage IVA.19 The Pan et al study results were unanimously approved and relevant recommendations were incorporated into the AJCC/UICC 8th edition of staging20 and the 2017 China NPC staging system, thereby achieving unification in the internal and domestic NPC staging.
The management of NPC has undergone dramatic evolution as a result of advances in radiotherapy technology, including the transition from 2-dimensional to 3-dimensional conformal and intensity-modulated radiotherapy (IMRT), improvement in concurrent chemotherapy, and accurate disease staging. This article is a consensus on treatment strategies for NPC, which was developed by the domestic experts after several group discussions on their own experiences along with published reference. The consensus aims to update the clinicians and provide guidance for the management of NPC, thereby improving the overall survival (OS) and quality of life with minimal complications. Further, the recommendations put forward in this consensus was arrived when there was ≥80% level of agreement between the members of the consensus group.
Consensus recommendations
Recommended treatment options for stage I and stage II NPC are presented below, along with the recommended therapy regimen, doses, and evidence from previous studies.
Treatment options for stage I NPC
Radiotherapy is the main treatment for the NPC patients without distant metastasis. For stage I, a radical dose of 66–70 Gy and 56 Gy administered to the primary tumor and the upper neck, respectively, is necessary for tumor control and prevention of local recurrence, and the local control rate is over 90% for patients with stage T1N0M0.21,22 A single-center retrospective study by Gao et al reported a 5-year OS of 85% and a local control rate of 90% in stage N0 cases without irradiating the lower cervical region. The study reported a very low failure rate of <0.2%. This evidence suggested that radiotherapy is not necessary in the lower cervical region in stage N0 cases.23
Treatment options for stage II NPC
Radiotherapy to primary tumor and lymphatic drainage are the standard treatment options for stage II NPC, including T2N0 and T1N1.24,25 A retrospective study by Su et al that included patients with early-stage (T1-T2bN0-N1M0) NPC who underwent only IMRT (N=198) reported a 5-year estimated disease-specific survival of 97.3% and a distant metastasis-free survival rate of 97.8%. It was noted that patients with T2b had a relatively greater risk of local recurrence, whereas those with T2bN1 disease had a greater risk of distant metastasis. Therefore, patients with T2bN1 NPC were considered requiring intensified therapy.25 Cheng et al also reported a high 3-year locoregional control rate of 91.7% and 100% in the groups receiving only radiotherapy and concurrent chemotherapy and radiotherapy (CCRT) (P=0.10), respectively. In addition, the authors also reported a similar 3-year disease-free survival (DFS) rate in the groups receiving radiotherapy and CCRT (91.7% and 96.9%, P=0.66).26 Evidence from the concerned studies showed that synchronized radiotherapy as the first choice of treatment for stage II NPC, especially for patients with T2N1, for the local control and distant metastasis. Supporting the evidence, a phase III randomized trial that compared CCRT with 2-dimensional radiotherapy (RT) in 230 patients with stage II NPC reported that CCRT significantly improved the 5-year OS rate of patients (94.5% vs 85.5%, hazard ratio [HR]: 0.30; 95% CI: 0.12–0.76; P=0.007) and distant metastasis-free survival rate (94.8% vs 83.9%, HR: 0.27; 95% CI: 0.10–0.74; P=0.007).27 However, it should be noted that in these studies, 2-dimensional RT was administered to the control group, and currently IMRT is widely used. These data indicate toward an important question: whether chemotherapy is still necessary in patients treated with IMRT.
Owing to the greater toxicity associated with CCRT, physicians should be more cautious while prescribing chemotherapy to patients. In the INT-0099 trial, 63% patients receiving cisplatin 100 mg/m2 for 3 cycles completed the trial. The major reason for withdrawal from the study was toxicity to the therapy.2 A phase III randomized control study by Chen et al also reported that patients receiving CCRT experienced more severe grades 3–4 acute toxicities, including adverse events (AEs) of blood, gastrointestinal system, and mucositis in comparison with those receiving radiotherapy alone.27 Therefore, IMRT has replaced the conventional 2-dimensional radiotherapy techniques as the standard therapy for stage 2 NPC (Box 2).
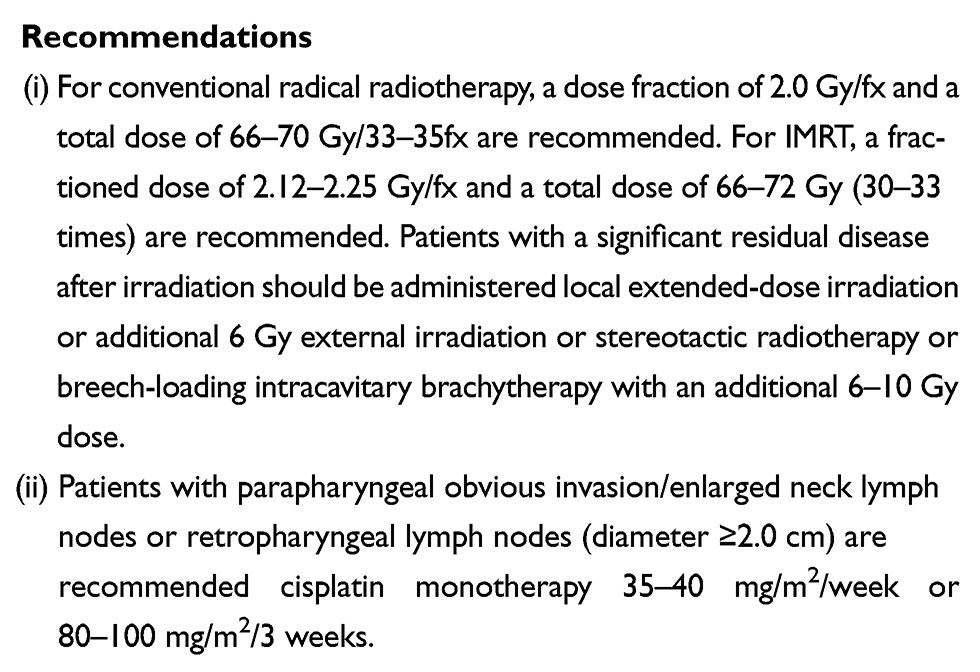 |
Box 2: Treatment recommendations in stage II NPC |
Treatment options for locally advanced NPC (Box 3)
CCRT with or without adjuvant chemotherapy is the standard therapy in patients with locally advanced (LA) NPC (stages III, IVA, or IVB). The patients may also be prescribed induction/neoadjuvant chemotherapy sequential CCRT, cetuximab targeted therapy, and chemoradiation combination. In addition, cervical lymph node dissection is recommended for refractory or recurrent lymph node enlargements.28 Lately, there has been a major focus on the treatment of LA NPC with combined radiotherapy and chemotherapy showing improved clinical outcomes. This treatment strategy has been an important milestone in the treatment of LA NPC. To date, at least 5 phase III randomized controlled trials (RCTs) that compared the efficacy of concurrent chemoradiation with radiotherapy alone in LA NPC25,29–33 have reported concurrent chemoradiotherapy significantly improved DFS, while other phase III RCTs have reported a significant improvement in progression-free survival (PFS) and OS.34–38 The HR for OS in these studies ranged from 0.4 to 0.71, with a follow-up period of 2–5 years. Not only RCTs, but more robust evidence from several meta-analyses (n>8000 patients with LA NPC) have also shown a significant benefit of CCRT in clinical outcomes in comparison to radiotherapy alone.39–41 A recent meta-analysis of 19 trials (n=4806) and patients treated with CCRT reported a significantly improved PFS (HR: 0.75; 95% CI: 0.69–0.81), OS (HR: 0.79; 95% CI: 0.73–0.86; P<0.0001), locoregional control (HR: 0.74; 95% CI: 0.65–0.85), and distant control (HR: 0.68; 95% CI: 0.60–0.76).41 Based on these findings, CCRT is currently recommended as the standard treatment option for LA NPC. Although the beneficial clinical outcome of CCRT is not related to the type of chemotherapy used, a few exploratory analyses have shown the beneficial effect of cisplatin in both local control and OS.42,43 Although cisplatin-based regimens are commonly used in CCRT and have shown benefits in relapse-free survival and OS rates, cisplatin is associated with significantly increased toxicity, and hence, there is reduced patient compliance, which must also be taken into account while prescribing cisplatin. Hence, carboplatin may be considered for use in CCRT because of its lower nephrotoxicity.
The dose of chemotherapy to be used in CCRT is still under exploration in clinical research. A phase III, non-inferiority, multicenter RCT involving 526 patients with LA NPC was conducted to assess the efficacy and toxicity profiles of CCRT between every 3-week (ETW) versus once-in-a-week (OAW) schedule of cisplatin. After 24 months, the failure-free survival (FFS) and 2-year OS of OAW compared with ETW were similar in both groups; 93.1% vs 89.1% (HR: 1.217; 0.684–2.163; P=0.504) and 98.6% vs 97.4% (HR: 1.271; 0.441–3.664; P=0.657), respectively. However, the incidence of grades 3–4 leukopenia and thrombocytopenia were significantly higher in the group receiving weekly OAW cisplatin in comparison to the group receiving ETW cisplatin (27.3% vs 16.2%; 4.8% vs 1.2%). However, more evidences are warranted to conclude on the efficacy of the therapies after longer follow-up.44
To date, RCTs showing survival benefit with CCRT in combination with adjuvant chemotherapy are scarce and the significance of adjuvant chemotherapy for LA NPC remains to be determined. Previous meta-analysis has shown that compared to CCRT, the addition of adjuvant chemotherapy did not show a significant improvement on local control rate, distant metastasis rate and OS.37 However, based on the previous study comparing between CCRT and radiotherapy, it could be speculated that CCRT combined with adjuvant chemotherapy may improve clinical outcomes in LA NPC. As CCRT has proven to be superior to radiotherapy alone, an unmet need to increase the significance of adjuvant chemotherapy on this basis exists. The largest phase III study to date comparing adjuvant chemotherapy (cisplatin and 5-fluorouracil [5-FU]) + CCRT and CCRT alone reported an estimated 2-year FFS rate of 86% in the adjuvant chemotherapy + CCRT group in comparison to 84% in the CCRT alone group (HR: 0.74; 95% CI: 0.49–1.10; P=0.13). In addition, patient compliance was lower in the group receiving adjuvant chemotherapy + CCRT, with 63% of the patients receiving adjuvant chemotherapy and 49% receiving reduced doses of chemotherapy.45 However, meta-analyses of MACH-NPC showed that CCRT combined with adjuvant chemotherapy is more effective (n=1267; HR: 0.65; 95% CI: 0.56–0.76) for OS than radiotherapy alone (n=1834; HR: 0.80; 95% CI: 0.70–0.93).41 Nevertheless, it should be noted that the above-mentioned comparison between the two groups was indirect. On the basis of the current literature data, CCRT sequential adjuvant chemotherapy has not been specifically recommended for the treatment of LA NPC. Further studies should be performed to determine subsequent directions and identify subgroups that can derive the maximum benefit from CCRT and adjuvant chemotherapy. The ongoing RCTs (NCT00370890 and NCT02135042) are evaluating the role of persistent infection of EBV DNA after treatment to guide subsequent adjuvant chemotherapy, which is one of the patient groups considered to be beneficial from the CCRT and adjuvant chemotherapy. Another potential group of patients likely to benefit from adjuvant chemotherapy is NPC patients with large cervical lymph nodes (N2, N3). In a recent study involving 547 NPC patients with N2-3, no significant benefit was observed in the adjuvant chemotherapy subgroup analyses of patients with N3. However, the patient subgroup had a significantly lower risk of distant metastases (HR: 0.413; 95% CI: 0.194–0.881; P=0.022) and survival benefit (HR: 0.398; 95% CI: 0.187–0.848; P=0.017) after adjuvant chemotherapy. More evidence is therefore required to confirm the efficacy of CCRT and adjuvant chemotherapy in these subpopulations.46
Neoadjuvant or induction chemotherapy shrinks the tumor, which increases the likelihood of curative dose to be used in subsequent radiotherapy regimens. In addition, induction chemotherapy may also reduce distant metastasis of head and neck cancer. Therefore, in the past few years, efficacy of chemoradiotherapy (CRT) in combination with induction chemotherapy has been determined in patients with LA NPC. Efficacy of induction chemotherapy has been evaluated in two phase II, single-arm studies in patients with LA NPC (n=33, n=28, respectively).47,48 In both studies, patients achieved good clinical outcomes with carboplatin + gemcitabine or docetaxel, cisplatin, and 5-FU induction chemotherapy regimens with 3-year OS rate ranging from 86.1% to 89.3%. Owing to the limited evidence from only 2 studies, efficacy of both induction regimens warrants further investigation. The phase II trial that compared the effect of CRT and CRT combined with docetaxel and cisplatin as induction chemotherapy lacked the power to observe a statistically significant OS. However, the results at 3 years indicated a much higher OS rate with induction chemotherapy (94.1% vs 67.7%, HR: 0.24; 95% CI: 0.078–0.73; P=0.012).49 The promising results from this phase II study is not yet confirmed in larger phase III RCTs. In another two phase II/III studies, the regimen of induction chemotherapy are paclitaxel, cisplatin, epirubicin or paclitaxel, carboplatin, and gemcitabine.50,51 In comparison with CCRT, induction chemotherapy did not show any significant benefit in terms of response rates, PFS, and OS in either of the studies. The multi-arm trial NPC-0501 compared CCRT with CCRT induction chemotherapy, capecitabine versus 5-FU, and accelerated radiotherapy versus conventional RT in 706 patients randomized to 6 treatment groups, with concurrent cisplatin and RT followed by cisplatin and 5-FU adjuvant treatment as the standard control group. Over 3 years, the OS rate increased from 85% to 91%, with preliminary analysis showing no significant difference in PFS between cisplatin + fluorouracil (PF) induction chemotherapy and PF-adjuvant therapy. However, the subgroup analysis showed less toxicity and better efficacy with capecitabine in comparison with 5-fluorouracil (FU).52 Based on the results, the patients were not recommended to use the accelerated fraction radiotherapy due to toxicity considerations. The study involved a relatively short follow-up period of 3 years and further long-term follow-up results are required to determine the role of induction chemotherapy.
Another recent phase III RCT showed a significant improvement in 3-year FFS with induction chemotherapy + CCRT compared with CCRT alone (80% vs 72%, HR: 0.68; P=0.034). This evidence suggested that for patients with LA NPC, docetaxel + cisplatin + fluorouracil (TPF)-induced radiotherapy in addition to concurrent chemoradiotherapy may benefit in prolonging the survival. In terms of safety, induction chemotherapy + CCRT resulted in a greater incidence of AEs, with the most common grade 3 or 4/severe adverse reactions being neutropenia (42% vs 7%), leukopenia (41% vs 17%), and stomatitis (41% vs 35%).53 More long-term follow-ups of the study can further clarify the long-term efficacy and safety of the therapy. A report released in the American Society of Clinical Oncology Assembly in 2017 concluded similarly, wherein the intent-to-treat population analysis showed that the addition of a 2-courses PF regimen to the CCRT significantly improved DFS (P=0.028) in comparison with CCRT only, with no significant difference in OS and distant metastases-free survival (DMFS) between the two groups.
The epidermal growth factor receptor (EGFR) monoclonal antibody cetuximab has found clinically significant application in the treatment of NPC as it is expressed in more than 80–90% of patients with NPC.54–56 Cetuximab monotherapy or combination with chemotherapy or radiotherapy has shown to significantly inhibit tumor growth and proliferation and increase the sensitivity of NPC tumor cell lines to radiotherapy or chemotherapy, and therefore have a synergistic effect.57,58 Collecting the evidence from preclinical studies, some phase II trials investigated the use of cetuximab therapy in combination with or without chemotherapy. Recently 2 phase II trials that evaluated the efficacy of IMRT in combination with cetuximab and cisplatin in 130 patients with LA NPC reported good short-term effects, with 2-year DFS rates of 86.5–89%. One of the studies even reported a 2-year OS rate of 91%. Cetuximab combined with chemotherapy or radiotherapy was well tolerated with very few controllable and reversible cutaneous AEs and mucositis.59–61 However, the phase II RCT that evaluated the efficacy and safety of IMRT in combination with cetuximab or cisplatin after 2 courses of induction chemotherapy (docetaxel + cisplatin) was terminated prematurely because of higher rates of mucositis and skin reactions. Nevertheless, in terms of efficacy, the combination of cetuximab and IMRT reported a higher 3-year DFS rate of 85.7% in comparison to 78.3% reported in the group receiving cisplatin + IMRT. Similarly, multiple single-arm clinical studies of cetuximab + radiotherapy/chemotherapy (with or without induction chemotherapy) have also been performed in LA NPC patients.62–64 In accordance with the results from previous trials, the 2-year DFS was around 89% while the 3 year OS reached approximately 90%. On the basis of the results from these studies, it is evident that cetuximab in combination with CRT or radiotherapy is a viable treatment regimen in patients with LA NPC with acceptable toxicity. Therefore, for some patients with LA NPC, it may be advisable to add cetuximab to the standard CRT regimens. However, there is a need for further prospective phase III clinical trials to confirm the efficacy and safety of cetuximab in patients with LA NPC. Another targeted therapy that has been explored for NPC is bevacizumab. In a phase II one-arm study among the 44 patients with NPC, the estimated 2 year locoregional PFS, distant metastasis-free survival, PFS, and OS rates were 83.7% (95% CI: 72.6–94.9), 90.8% (82.2–99.5), 74.7% (61.8–87.6), and 90.9% (82.3–99.4), respectively. Addition of bevacizumab to chemoradiation was feasible for NPC treatment and the combination also delayed distant metastasis.65 IMRT being the standard radiotherapy for NPC reported a significant reduction in the risk of dry mouth and improved local control and safety in comparison to conventional 2-dimensional radiotherapy in RCTs.66–68 It is also reported that with IMRT, patients with T3 and T4 disease generally have a 5-year local control rate of ≥90% and 74–80%, respectively,69,70 along with long-term toxicity and damage to the nervous system. Hence, the overall treatment principle is to consider the risk-benefit profile of the largest dose of the drug. The dose should have a tolerable risk to the vital organs, balance the local control of the tumor, and prevent the occurrence of organ complications.
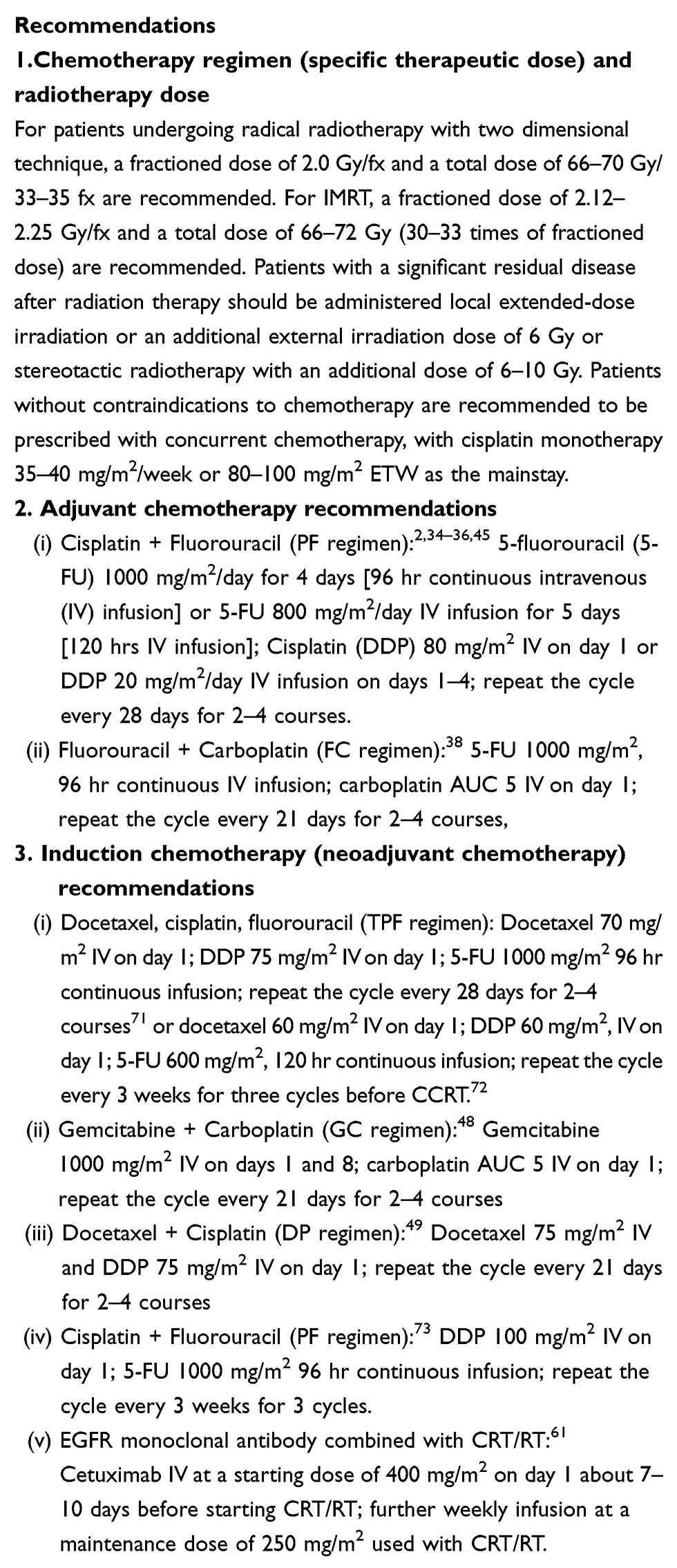 |
Box 3: Treatment recommendations for locally advanced NPC |
Treatment of recurrent or metastatic NPC (Box 4 and 5)
NPC patients who experience recurrence after treatment are required to undergo a pathological biopsy and MRI restaging, and then choose a different treatment mode according to the type of staging and patient status. A salvage surgery for disease recurrence can be performed in patients with no comorbidities who are otherwise in good health.74 If the disease relapses after >1 year of radiotherapy, re-radiation therapy should be considered.75,76
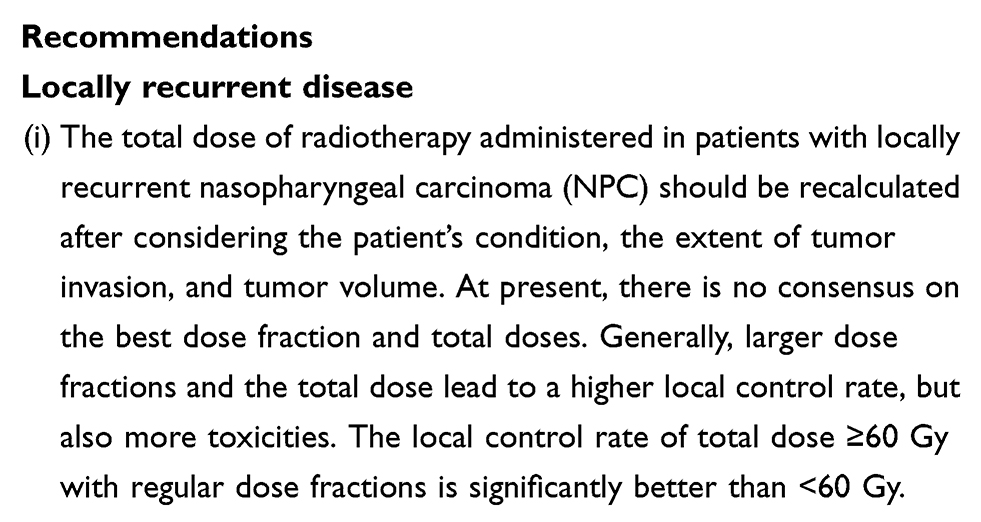 |
Box 4: Treatment recommendations for recurrent or metastatic NPC |
Platinum-based chemotherapeutic combinations are commonly used as first-line treatment in patients contraindicated for re-radiation or surgery and in patients with recurrent or metastatic (R/M) NPC who are otherwise in good condition. In the Taiwanese population, a multicenter phase II study showed gemcitabine plus cisplatin as an effective, well tolerated, first-line treatment regimen for R/M NPC. The response rate, median PFS, and median OS reported in ITT were 51.9%, 9.8 months, and 14.6 months, respectively.77 In another recently reported multicenter phase III RCT in China, the efficacy and safety of gemcitabine plus cisplatin (GP) compared with 5-FU plus cisplatin (FP) showed that the GP regimen significantly prolonged the median PFS (7 vs 5.6 months, HR: 0.55; 95% CI: 0.44–0.68; P<0.001) and OS (29.1 vs 20.9 months, HR: 0.62; 95% CI: 0.45–0.84; P=0.0025) in comparison with the FP regimen. Overall safety of GP regimen was acceptable and manageable despite major hematologic grade 3/4 AEs, including leukopenia (29%), neutropenia (23%), and thrombocytopenia (13%).78 Although platinum-based chemotherapy has rarely been evaluated in a larger phase III clinical trial, it is still recommended because of its efficacy and lesser side effects. The most commonly recommended regimens include cisplatin or carboplatin in combination with docetaxel or paclitaxel, cisplatin/5-FU chemotherapy, and paclitaxel in combination with cisplatin and 5-FU as triple regimen therapy.79–83 The response rates of these regimens have been reported to be between 25% and 78.9%, of which TPF triple regimen had the highest response rate.84,85 In addition, the combination of gemcitabine and oxaliplatin has also shown certain effects on patients with R/M NPC. The efficacy of this regimen was 56.1% in a single-arm phase II study that included 42 patients with R/M NPC, with a median OS and time to progression (TTP) of 19.6 and 14.8 months, respectively.86,87 In patients who had previously received platinum-based chemotherapy, the option of combined chemotherapy or single-agent chemotherapy that included gemcitabine in combination with vinorelbine, capecitabine, and oxaliplatin has been explored in clinical studies.87–89 The response rates reported in these studies ranged from 23.5% to 43.8% and the median PFS ranged from 4.9 m to 5.1 m. In addition, a study that included 30 patients with R/M NPC suggested that docetaxel monotherapy [30 mg/m2 on days 1, 8, and 15, quarterly every 4 weeks (q4w)] has an active role in treatment of patients with disseminated NPC and those previously exposed and largely refractory to platinum-based chemotherapy.90
Also, the use of cetuximab combined with chemotherapy for patients with R/M NPC has been evaluated in a multicenter phase II study, where efficacy and toxicity of cetuximab plus carboplatin was evaluated in the platinum-resistant patients with R/M NPC. The results showed that cetuximab combined with carboplatin achieved considerable clinical efficacy, with a response rate of 11.7%, and approximately 50% of patients achieving stable disease (SD).91 The median TTP was 3months while the median OS was 8months. The study showed the efficacy of the combination particularly in patients who had been treated with multiline chemotherapy, and hence, the regimen is also recommended in the National Comprehensive Cancer Network guideline. In another retrospective study, cetuximab and chemotherapy were administered in 30 patients with R/M NPC with or without IMRT and yielded a response rate of 70% and median OS of 23.6 months.92 Based on the above-mentioned findings, cetuximab combined with chemotherapy is recommended as one of the treatment options for patients with R/M NPC. In order to reach an agreement for the use of cetuximab, more evidence from RCTs are warranted. A phase III RCT (NCT02633176), which compares cisplatin plus docetaxel with or without cetuximab followed by concurrent chemoradiation in previously untreated patients with metastatic NPC (mNPC), is ongoing to determine whether the addition of cetuximab to induction chemotherapy and chemoradiation could improve therapeutic efficacy in mNPC. The interim results showed that a response rate of 77.3% has been achieved in 17 patients, which shows a great efficacy of the cetuximab and chemotherapy combination. Among other small-molecule- or monoclonal antibody (MAB) targeted therapies, gefitinib failed to demonstrate its efficacy in previous phase II clinical studies. Another small-molecule targeted drug pazopanib used as the second-line treatment option in a phase II study of 33 patients with R/M NPC has reported a clinical benefit in 54.5% of patients, with 6.1%, 48.5% and 21.2% of patients achieving partial responses (PRs), stable disease (SD), and PR/SD, respectively, that lasted ≥6 months.93 Pazopanib has shown encouraging outcome in NPC with an acceptable toxicity profile. Targeted therapies with sorafenib and denosumab and immunotherapy are still under study, and there is a need for clinical trials to further validate their efficacy and safety.
A number of RCTs have been conducted to evaluate the efficacy and safety of immunotherapy in NPC. The KEYNOTE-028 trial (NCT02054806) assessed the efficacy and safety of 10 mg/kg biweekly pembrolizumab (MK-3475) given intravenously in patients with advanced NPC and PD-L1 expression (n=27). The study showed an overall response rate (ORR), DCR, SD, median response time, and median PFS of 22.2%, 77.8%, 55.6%, 10.3 months, and 5.6 months (3.6–11.0 months), respectively. The regimen was safe with a few grade 3–4 AEs of hepatitis (7.4%) and pneumonia (7.4%).94 The CheckMate 358 enrolled patients with R/M NPC and with ≤2 prior systemic therapies in the R/M setting. The patients received nivolumab 240 mg every 2 weeks until progression or unacceptable toxicity. The study reported about 20.8% of patients achieving partial response (PRs) while 25% patients had confirmed SD, with a median response time of 4.4 months and 8.3% grades 3–4 AE.95 In the Ma et al study (NCI-9742), 44 R/M NPC patients who were not amenable to curative treatment were treated with nivolumab at a dosage of 3 mg/kg intravenously every 2 weeks until they experienced disease progression. The study reported an overall ORR of 20.5% with 1 patient achieving confirmed complete response (CR) and 8 patients having PR. The one-year OS rate was 59% while PFS rate was 19.3% and reported no unexpected toxicity among the patients.96
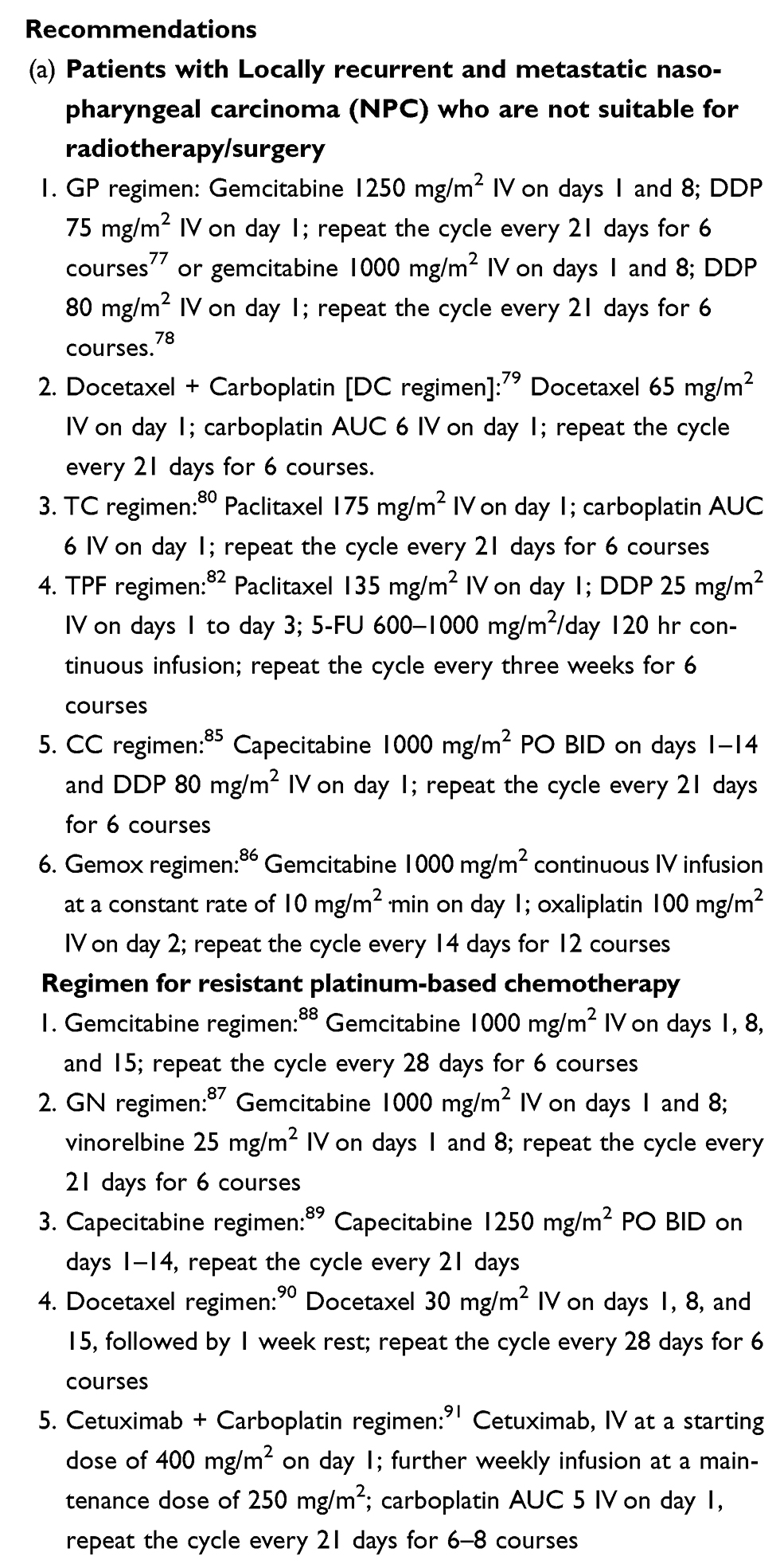 |
Box 5: Treatment recommendations for recurrent/metastatic NPC not suitable for radiotherapy/surgery |
Multidisciplinary approach for NPC management
The NPC consensus recommended a multidisciplinary approach for the management of NPC, which includes constituting a multidisciplinary team (MDT), which in turn includes a fixed panel of experts in various fields. The panel holds regular meetings to discuss and formulate treatment plans for various diseases including cancers. In order to facilitate timely and appropriate evidence-based management of cases with NPC, most centers have now established MDTs and conduct meetings in which each of the medical and allied health specialties are represented, so that accurate tumor staging and treatment plans can be best tailored to meet the need of individual patients. This will help to optimize tumor staging, assess the rationality of treatment options, facilitate individualized treatment, protect a patient’s breathing, speech, and eating functions, improve the patient’s quality of life, and develop the most appropriate treatment for the patient. In addition, an MDT greatly shortens the time from diagnosis to treatment. A typical MDT should include experts from the fields of otolaryngology, oral and maxillofacial-head and neck surgery, radiotherapy, radiation diagnosis, oncology, pathology, and adjuvant treatment group including nursing, psychotherapy, rehabilitation, clinical, and social support and nutritional support groups. Clinicians in various fields can share the clinical data and determine the best individualized treatment strategy based on treatment principles and guidelines. An MDT has a positive impact on communication among doctors in different fields, thereby expanding the knowledge about various diseases, which in turn improves the diagnosis and clinical outcomes of the disease. It can also have an impact on guiding preclinical and clinical research, helping to update field information, and ultimately benefit more NPC patients.
Conclusion
On the basis of this consensus, we have laid down a few treatment recommendations for patients in different NPC stages. These recommendations based on our clinical experience and literature review have been jointly agreed upon by our team of experts. With this consensus, we aim to improve the diagnosis and management of NPC, especially in the Chinese population.
Acknowledgment
The authors would like to acknowledge Dr Dhanya Mukundan and Karan Sharma (Indegene Pvt. Ltd.) for providing writing support and technical assistance in developing the consensus manuscript.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012: globocan 2012. Int J Cancer. 2015;136(5):E359–E386. doi:10.1002/ijc.29210
2. Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup study 0099. J Clin Oncol Off J Am Soc Clin Oncol. 1998;16(4):1310–1317. doi:10.1200/JCO.1998.16.4.1310
3. Tang -L-L, Chen W-Q, Xue W-Q, et al. Global trends in incidence and mortality of nasopharyngeal carcinoma. Cancer Lett. 2016;374(1):22–30. doi:10.1016/j.canlet.2016.01.040
4. Forman D, Bray F, Brewster DH, et al. Cancer incidence in five continents. International Association of Cancer Registries Scientific Publications. 2013;164.
5. Ng WT, Yuen KT, Au KH, Chan OSH, Lee AWM. Staging of nasopharyngeal carcinoma–the past, the present and the future. Oral Oncol. 2014;50(6):549–554. doi:10.1016/j.oraloncology.2013.06.003
6. Chen L, Gallicchio L, Boyd-Lindsley K, et al. Alcohol consumption and the risk of nasopharyngeal carcinoma: a systematic review. Nutr Cancer. 2009;61(1):1–15. doi:10.1080/01635580802372633
7. Chien YC, Chen JY, Liu MY, et al. Serologic markers of Epstein-Barr virus infection and nasopharyngeal carcinoma in Taiwanese men. N Engl J Med. 2001;345(26):1877–1882. doi:10.1056/NEJMoa011610
8. Yu MC, Garabrant DH, Huang TB, Henderson BE. Occupational and other non-dietary risk factors for nasopharyngeal carcinoma in Guangzhou, China. Int J Cancer. 1990;45(6):1033–1039.
9. Yuan JM, Wang XL, Xiang YB, Gao YT, Ross RK, Yu MC. Non-dietary risk factors for nasopharyngeal carcinoma in Shanghai, China. Int J Cancer. 2000;85(3):364–369.
10. Guo X, Johnson RC, Deng H, et al. Evaluation of nonviral risk factors for nasopharyngeal carcinoma in a high-risk population of Southern China. Int J Cancer. 2009;124(12):2942–2947. doi:10.1002/ijc.24293
11. Thompson LDR. Update on nasopharyngeal carcinoma. Head Neck Pathol. 2007;1(1):81–86. doi:10.1007/s12105-007-0012-7
12. Wan X, Wei L, Li H, et al. High pretreatment serum lactate dehydrogenase level correlates with disease relapse and predicts an inferior outcome in locally advanced nasopharyngeal carcinoma. Eur J Cancer Oxf Engl 1990. 2013;49(10):2356–2364.
13. Chinese Committee for Staging of Nasopharyngeal Carcinoma. Report on revision of the Chinese 1992 staging system for nasopharyngeal carcinoma. J Radiat Oncol. 2013;2(3):233–240.
14. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
15. Davis W. Nasopharyngeal carcinoma: etiology and control. International Agency for Research on Cancer Scientific Publications. 1978;20.
16. Ng WT, Lee AWM, Kan WK, et al. N-staging by magnetic resonance imaging for patients with nasopharyngeal carcinoma: pattern of nodal involvement by radiological levels. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2007;82(1):70–75. doi:10.1016/j.radonc.2006.11.010
17. Yue D, Xu Y-F, Zhang F, et al. Is replacement of the supraclavicular fossa with the lower level classification based on magnetic resonance imaging beneficial in nasopharyngeal carcinoma? Radiother Oncol J Eur Soc Ther Radiol Oncol. 2014;113(1):108–114. doi:10.1016/j.radonc.2014.08.036
18. Sze H, Chan LLK, Ng WT, et al. Should all nasopharyngeal carcinoma with masticator space involvement be staged as T4? Oral Oncol. 2014;50(12):1188–1195. doi:10.1016/j.oraloncology.2014.09.001
19. Pan JJ, Ng WT, Zong JF, et al. Proposal for the 8th edition of the AJCC/UICC staging system for nasopharyngeal cancer in the era of intensity-modulated radiotherapy. Cancer. 2016;122(4):546–558. doi:10.1002/cncr.29795
20. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging: the Eighth Edition AJCC Cancer Staging Manual. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
21. Mesic JB, Fletcher GH, Goepfert H. Megavoltage irradiation of epithelial tumors of the nasopharynx. Int J Radiat Oncol Biol Phys. 1981;7(4):447–453.
22. Wei WI, Kwong DLW. Current management strategy of nasopharyngeal carcinoma. Clin Exp Otorhinolaryngol. 2010;3(1):1–12. doi:10.3342/ceo.2010.3.1.1
23. Gao Y, Zhu G, Lu J, et al. Is elective irradiation to the lower neck necessary for N0 nasopharyngeal carcinoma? Int J Radiat Oncol Biol Phys. 2010;77(5):1397–1402. doi:10.1016/j.ijrobp.2009.06.062
24. Xiao -W-W, Han F, Lu T-X, Chen C-Y, Huang Y, Zhao C. Treatment outcomes after radiotherapy alone for patients with early-stage nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2009;74(4):1070–1076. doi:10.1016/j.ijrobp.2008.09.008
25. Su S-F, Han F, Zhao C, et al. Long-term outcomes of early-stage nasopharyngeal carcinoma patients treated with intensity-modulated radiotherapy alone. Int J Radiat Oncol Biol Phys. 2012;82(1):327–333. doi:10.1016/j.ijrobp.2010.09.011
26. Cheng SH, Tsai SY, Yen KL, et al. Concomitant radiotherapy and chemotherapy for early-stage nasopharyngeal carcinoma. J Clin Oncol Off J Am Soc Clin Oncol. 2000;18(10):2040–2045. doi:10.1200/JCO.2000.18.10.2040
27. Chen Q-Y, Wen Y-F, Guo L, et al. Concurrent chemoradiotherapy vs radiotherapy alone in stage II nasopharyngeal carcinoma: phase III randomized trial. J Natl Cancer Inst. 2011;103(23):1761–1770. doi:10.1093/jnci/djr432
28. Mendenhall WM, Werning JW, Pfister DG. Treatment of Head and Neck Cancer. In: DeVita VT
29. Chan ATC, Teo PML, Ngan RK, et al. Concurrent chemotherapy-radiotherapy compared with radiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: progression-free survival analysis of a phase III randomized trial. J Clin Oncol Off J Am Soc Clin Oncol. 2002;20(8):2038–2044. doi:10.1200/JCO.2002.08.149
30. Chan ATC, Leung SF, Ngan RKC, et al. Overall survival after concurrent cisplatin-radiotherapy compared with radiotherapy alone in locoregionally advanced nasopharyngeal carcinoma. J Natl Cancer Inst. 2005;97(7):536–539. doi:10.1093/jnci/dji084
31. Wu X, Huang PY, Peng PJ, et al. Long-term follow-up of a phase III study comparing radiotherapy with or without weekly oxaliplatin for locoregionally advanced nasopharyngeal carcinoma. Ann Oncol Off J Eur Soc Med Oncol. 2013;24(8):2131–2136. doi:10.1093/annonc/mdt163
32. Zhang L, Zhao C, Peng P-J, et al. Phase III study comparing standard radiotherapy with or without weekly oxaliplatin in treatment of locoregionally advanced nasopharyngeal carcinoma: preliminary results. J Clin Oncol Off J Am Soc Clin Oncol. 2005;23(33):8461–8468. doi:10.1200/JCO.2004.00.3863
33. Lin J-C, Jan J-S, Hsu C-Y, Liang W-M, Jiang R-S, Wang W-Y. Phase III study of concurrent chemoradiotherapy versus radiotherapy alone for advanced nasopharyngeal carcinoma: positive effect on overall and progression-free survival. J Clin Oncol Off J Am Soc Clin Oncol. 2003;21(4):631–637. doi:10.1200/JCO.2003.06.158
34. Wee J, Tan EH, Tai BC, et al. Randomized trial of radiotherapy versus concurrent chemoradiotherapy followed by adjuvant chemotherapy in patients with American Joint Committee on Cancer/International Union against cancer stage III and IV nasopharyngeal cancer of the endemic variety. J Clin Oncol Off J Am Soc Clin Oncol. 2005;23(27):6730–6738. doi:10.1200/JCO.2005.16.790
35. Chen Y, Sun Y, Liang S-B, et al. Progress report of a randomized trial comparing long-term survival and late toxicity of concurrent chemoradiotherapy with adjuvant chemotherapy versus radiotherapy alone in patients with stage III to IVB nasopharyngeal carcinoma from endemic regions of China. Cancer. 2013;119(12):2230–2238. doi:10.1002/cncr.28049
36. Lee AWM, Tung SY, Chua DTT, et al. Randomized trial of radiotherapy plus concurrent-adjuvant chemotherapy vs radiotherapy alone for regionally advanced nasopharyngeal carcinoma. J Natl Cancer Inst. 2010;102(15):1188–1198. doi:10.1093/jnci/djq258
37. Lee AWM, Tung SY, Chan ATC, et al. A randomized trial on addition of concurrent-adjuvant chemotherapy and/or accelerated fractionation for locally-advanced nasopharyngeal carcinoma. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2011;98(1):15–22. doi:10.1016/j.radonc.2010.09.023
38. Dechaphunkul T, Pruegsanusak K, Sangthawan D, Sunpaweravong P. Concurrent chemoradiotherapy with carboplatin followed by carboplatin and 5-fluorouracil in locally advanced nasopharyngeal carcinoma. Head Neck Oncol. 2011;3:30. doi:10.1186/1758-3284-3-30
39. Langendijk JA, Leemans CR, Buter J, Berkhof J, Slotman BJ. The additional value of chemotherapy to radiotherapy in locally advanced nasopharyngeal carcinoma: a meta-analysis of the published literature. J Clin Oncol Off J Am Soc Clin Oncol. 2004;22(22):4604–4612. doi:10.1200/JCO.2004.10.074
40. Huncharek M, Kupelnick B. Combined chemoradiation versus radiation therapy alone in locally advanced nasopharyngeal carcinoma: results of a meta-analysis of 1,528 patients from six randomized trials. Am J Clin Oncol. 2002;25(3):219–223.
41. Blanchard P, Lee A, Marguet S, et al. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the MAC-NPC meta-analysis. Lancet Oncol. 2015;16(6):645–655. doi:10.1016/S1470-2045(15)70126-9
42. Lee AWM, Tung SY, Ngan RKC, et al. Factors contributing to the efficacy of concurrent-adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: combined analyses of NPC-9901 and NPC-9902 trials. Eur J Cancer Oxf Engl 1990. 2011;47(5):656–666.
43. Loong HH, Ma BBY, Leung S-F, et al. Prognostic significance of the total dose of cisplatin administered during concurrent chemoradiotherapy in patients with locoregionally advanced nasopharyngeal carcinoma. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2012;104(3):300–304. doi:10.1016/j.radonc.2011.12.022
44. Liang H, Wei-Xiong X, Xing L, Sun R, Zeng Q, Si-Wei L. Concurrent chemoradiotherapy with 3-weekly versus weekly cisplatin in patients with locoregionally advanced nasopharyngeal carcinoma: a phase 3 multicentre randomised controlled trial (ChiCTR-TRC-12001979). J Clin Oncol Off J Am Soc Clin Oncol. 2017;15(35):6006. doi:10.1200/JCO.2017.35.15_suppl.6006
45. Chen L, Hu C-S, Chen X-Z, et al. Concurrent chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma: a phase 3 multicentre randomised controlled trial. Lancet Oncol. 2012;13(2):163–171. doi:10.1016/S1470-2045(11)70320-5
46. Xu T, Shen C, Ou X, He X, Ying H, Hu C. The role of adjuvant chemotherapy in nasopharyngeal carcinoma with bulky neck lymph nodes in the era of IMRT. Oncotarget. 2016;7(15):21013–21022. doi:10.18632/oncotarget.7849
47. Bae WK, Hwang JE, Shim HJ, et al. Phase II study of docetaxel, cisplatin, and 5-FU induction chemotherapy followed by chemoradiotherapy in locoregionally advanced nasopharyngeal cancer. Cancer Chemother Pharmacol. 2010;65(3):589–595. doi:10.1007/s00280-009-1152-0
48. Lim AM, Corry J, Collins M, et al. A phase II study of induction carboplatin and gemcitabine followed by chemoradiotherapy for the treatment of locally advanced nasopharyngeal carcinoma. Oral Oncol. 2013;49(5):468–474. doi:10.1016/j.oraloncology.2012.12.012
49. Hui EP, Ma BB, Leung SF, et al. Randomized phase II trial of concurrent cisplatin-radiotherapy with or without neoadjuvant docetaxel and cisplatin in advanced nasopharyngeal carcinoma. J Clin Oncol Off J Am Soc Clin Oncol. 2009;27(2):242–249. doi:10.1200/JCO.2008.18.1545
50. Tan T, Lim W-T, Fong K-W, et al. Concurrent chemo-radiation with or without induction gemcitabine, Carboplatin, and Paclitaxel: a randomized, phase 2/3 trial in locally advanced nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2015;91(5):952–960. doi:10.1016/j.ijrobp.2015.01.002
51. Fountzilas G, Ciuleanu E, Bobos M, et al. Induction chemotherapy followed by concomitant radiotherapy and weekly cisplatin versus the same concomitant chemoradiotherapy in patients with nasopharyngeal carcinoma: a randomized phase II study conducted by the Hellenic Cooperative Oncology Group (HeCOG) with biomarker evaluation. Ann Oncol Off J Eur Soc Med Oncol. 2012;23(2):427–435.
52. Lee AWM, Ngan RKC, Tung SY, et al. Preliminary results of trial NPC-0501 evaluating the therapeutic gain by changing from concurrent-adjuvant to induction-concurrent chemoradiotherapy, changing from fluorouracil to capecitabine, and changing from conventional to accelerated radiotherapy fractionation in patients with locoregionally advanced nasopharyngeal carcinoma. Cancer. 2015;121(8):1328–1338. doi:10.1002/cncr.29208
53. Li W-F, Chen L, Sun Y, Ma J. Induction chemotherapy for locoregionally advanced nasopharyngeal carcinoma. Chin J Cancer. 2016;35(1):94. doi:10.1186/s40880-016-0157-4
54. Ma BBY, Poon TCW, To KF, et al. Prognostic significance of tumor angiogenesis, Ki 67, p53 oncoprotein, epidermal growth factor receptor and HER2 receptor protein expression in undifferentiated nasopharyngeal carcinoma–a prospective study. Head Neck. 2003;25(10):864–872. doi:10.1002/hed.10307
55. Chua DTT, Nicholls JM, Sham JST, Au GKH. Prognostic value of epidermal growth factor receptor expression in patients with advanced stage nasopharyngeal carcinoma treated with induction chemotherapy and radiotherapy. Int J Radiat Oncol Biol Phys. 2004;59(1):11–20. doi:10.1016/j.ijrobp.2003.10.038
56. Leong J-L, Loh KS, Putti TC, Goh BC, Tan LKS. Epidermal growth factor receptor in undifferentiated carcinoma of the nasopharynx. Laryngoscope. 2004;114(1):153–157. doi:10.1097/00005537-200401000-00029
57. Huang SM, Bock JM, Harari PM. Epidermal growth factor receptor blockade with C225 modulates proliferation, apoptosis, and radiosensitivity in squamous cell carcinomas of the head and neck. Cancer Res. 1999;59(8):1935–1940.
58. Sung FL, Poon TCW, Hui EP, et al. Antitumor effect and enhancement of cytotoxic drug activity by cetuximab in nasopharyngeal carcinoma cells. Vivo Athens Greece. 2005;19(1):237–245.
59. Lu T, Zhao C, Chen C, et al. An open, multicenter clinical study on cetuximab combined with intensity modulated radiotherapy (IMRT) plus concurrent chemotherapy in nasopharyngeal carcinoma (NPC): preliminary report. J Clin Oncol. 2010;28(15_suppl):5577. doi:10.1200/jco.2010.28.15_suppl.5577
60. Chen C-Y, Zhao C, Gao L, et al. An open-labeled, multicentric clinical study of cetuximab combined with intensity-modulated radiotherapy (IMRT) plus concurrent chemotherapy in locoregionally advanced (LA) nasopharyngeal carcinoma (NPC): A 2-year follow-up report. J Clin Oncol. 2012;30(15_suppl):5535.
61. Ma BBY, Kam MKM, Leung SF, et al. A phase II study of concurrent cetuximab-cisplatin and intensity-modulated radiotherapy in locoregionally advanced nasopharyngeal carcinoma. Ann Oncol Off J Eur Soc Med Oncol. 2012;23(5):1287–1292. doi:10.1093/annonc/mdr401
62. Feng H-X, Guo S-P, Li G-R, et al. Toxicity of concurrent chemoradiotherapy with cetuximab for locoregionally advanced nasopharyngeal carcinoma. Med Oncol Northwood Lond Engl. 2014;31(9):170. doi:10.1007/s12032-014-0170-x
63. Niu X, Hu C, Kong L. Experience with combination of cetuximab plus intensity-modulated radiotherapy with or without chemotherapy for locoregionally advanced nasopharyngeal carcinoma. J Cancer Res Clin Oncol. 2013;139(6):1063–1071. doi:10.1007/s00432-013-1419-z
64. He X, Xu J, Guo W, Jiang X, Wang X, Zong D. Cetuximab in combination with chemoradiation after induction chemotherapy of locoregionally advanced nasopharyngeal carcinoma: preliminary results. Future Oncol Lond Engl. 2013;9(10):1459–1467. doi:10.2217/fon.13.151
65. Lee NY, Zhang Q, Pfister DG, et al. Addition of bevacizumab to standard chemoradiation for locoregionally advanced nasopharyngeal carcinoma (RTOG 0615): a phase 2 multi-institutional trial. Lancet Oncol. 2012;13(2):172–180. doi:10.1016/S1470-2045(11)70303-5
66. Pow EHN, Kwong DLW, McMillan AS, et al. Xerostomia and quality of life after intensity-modulated radiotherapy vs. conventional radiotherapy for early-stage nasopharyngeal carcinoma: initial report on a randomized controlled clinical trial. Int J Radiat Oncol Biol Phys. 2006;66(4):981–991. doi:10.1016/j.ijrobp.2006.06.013
67. Lee AWM, Ng WT, Chan LLK, et al. Evolution of treatment for nasopharyngeal cancer–success and setback in the intensity-modulated radiotherapy era. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2014;110(3):377–384. doi:10.1016/j.radonc.2014.02.003
68. Peng G, Wang T, Yang K-Y, et al. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2012;104(3):286–293. doi:10.1016/j.radonc.2012.08.013
69. Sun X, Su S, Chen C, et al. Long-term outcomes of intensity-modulated radiotherapy for 868 patients with nasopharyngeal carcinoma: an analysis of survival and treatment toxicities. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2014;110(3):398–403. doi:10.1016/j.radonc.2013.10.020
70. Lin S, Pan J, Han L, et al. Update report of nasopharyngeal carcinoma treated with reduced-volume intensity-modulated radiation therapy and hypothesis of the optimal margin. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2014;110(3):385–389. doi:10.1016/j.radonc.2014.01.011
71. Jin T, Zhang Q, Jiang F, et al. Neoadjuvant chemotherapy with different dose regimens of docetaxel, cisplatin and fluorouracil (TPF) for locoregionally advanced nasopharyngeal carcinoma: a retrospective study. Oncotarget. 2017;8:59. doi:10.18632/oncotarget.21992
72. Sun Y, Li W-F, Chen N-Y, et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016;17(11):1509–1520. doi:10.1016/S1470-2045(16)30410-7
73. Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med. 2007;357(17):1705–1715. doi:10.1056/NEJMoa070956
74. Vikram B, Strong EW, Shah JP, et al. Intraoperative radiotherapy in patients with recurrent head and neck cancer. Am J Surg. 1985;150(4):485–487.
75. Chen CY, Han F, Zhao C, et al. Treatment results and late complications of 556 patients with locally advanced nasopharyngeal carcinoma treated with radiotherapy alone. Br J Radiol. 2009;82(978):452–458. doi:10.1259/bjr/72813246
76. Koutcher L, Lee N, Zelefsky M, et al. Reirradiation of locally recurrent nasopharynx cancer with external beam radiotherapy with or without brachytherapy. Int J Radiat Oncol Biol Phys. 2010;76(1):130–137. doi:10.1016/j.ijrobp.2009.01.055
77. Hsieh JC-H, Hsu C-L, Ng S-H, et al. Gemcitabine plus cisplatin for patients with recurrent or metastatic nasopharyngeal carcinoma in Taiwan: a multicenter prospective Phase II trial. Jpn J Clin Oncol. 2015;45(9):819–827. doi:10.1093/jjco/hyv083
78. Zhang L, Huang Y, Hong S, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet Lond Engl. 2016;388(10054):1883–1892. doi:10.1016/S0140-6736(16)31388-5
79. Samlowski WE, Moon J, Kuebler JP, et al. Evaluation of the combination of docetaxel/carboplatin in patients with metastatic or recurrent squamous cell carcinoma of the head and neck (SCCHN): a Southwest Oncology Group Phase II study. Cancer Invest. 2007;25(3):182–188. doi:10.1080/07357900701209061
80. Tan EH, Khoo KS, Wee J, et al. Phase II trial of a paclitaxel and carboplatin combination in Asian patients with metastatic nasopharyngeal carcinoma. Ann Oncol Off J Eur Soc Med Oncol. 1999;10(2):235–237. doi:10.1023/A:1008390929826
81. Wang TL, Tan YO. Cisplatin and 5-fluorouracil continuous infusion for metastatic nasopharyngeal carcinoma. Ann Acad Med Singapore. 1991;20(5):601–603.
82. Chen C, Wang F, An X, et al. Triplet combination with paclitaxel, cisplatin and 5-FU is effective in metastatic and/or recurrent nasopharyngeal carcinoma. Cancer Chemother Pharmacol. 2013;71(2):371–378. doi:10.1007/s00280-012-2020-x
83. Ji JH, Korean Cancer Study Group (KCSG), Yun T, et al. A prospective multicentre phase II study of cisplatin and weekly docetaxel as first-line treatment for recurrent or metastatic nasopharyngeal cancer (KCSG HN07-01). Eur J Cancer Oxf Engl 1990. 2012;48(17):3198–3204.
84. Jin Y, Shi Y-X, Cai X-Y, et al. Comparison of five cisplatin-based regimens frequently used as the first-line protocols in metastatic nasopharyngeal carcinoma. J Cancer Res Clin Oncol. 2012;138(10):1717–1725. doi:10.1007/s00432-012-1219-x
85. Li Y-H, Wang F-H, Jiang W-Q, et al. Phase II study of capecitabine and cisplatin combination as first-line chemotherapy in Chinese patients with metastatic nasopharyngeal carcinoma. Cancer Chemother Pharmacol. 2008;62(3):539–544. doi:10.1007/s00280-007-0641-2
86. Ma BBY, Hui EP, Wong SCC, et al. Multicenter phase II study of gemcitabine and oxaliplatin in advanced nasopharyngeal carcinoma–correlation with excision repair cross-complementing-1 polymorphisms. Ann Oncol Off J Eur Soc Med Oncol. 2009;20(11):1854–1859. doi:10.1093/annonc/mdp065
87. Chen C, Wang F, Wang Z, et al. Salvage gemcitabine-vinorelbine chemotherapy in patients with metastatic nasopharyngeal carcinoma pretreated with platinum-based chemotherapy. Oral Oncol. 2012;48(11):1146–1151. doi:10.1016/j.oraloncology.2012.05.021
88. Zhang L, Zhang Y, Huang P-Y, Xu F, Peng P-J, Guan -Z-Z. Phase II clinical study of gemcitabine in the treatment of patients with advanced nasopharyngeal carcinoma after the failure of platinum-based chemotherapy. Cancer Chemother Pharmacol. 2008;61(1):33–38. doi:10.1007/s00280-007-0441-8
89. Chua DTT, Sham JST, Au GKH. A phase II study of capecitabine in patients with recurrent and metastatic nasopharyngeal carcinoma pretreated with platinum-based chemotherapy. Oral Oncol. 2003;39(4):361–366.
90. Ngeow J, Lim WT, Leong SS, et al. Docetaxel is effective in heavily pretreated patients with disseminated nasopharyngeal carcinoma. Ann Oncol Off J Eur Soc Med Oncol. 2011;22(3):718–722. doi:10.1093/annonc/mdq425
91. Chan ATC, Hsu -M-M, Goh BC, et al. Multicenter, phase II study of cetuximab in combination with carboplatin in patients with recurrent or metastatic nasopharyngeal carcinoma. J Clin Oncol Off J Am Soc Clin Oncol. 2005;23(15):3568–3576. doi:10.1200/JCO.2005.02.147
92. Xu T, Ou X, Shen C, Hu C. Cetuximab in combination with chemoradiotherapy in the treatment of recurrent and/or metastatic nasopharyngeal carcinoma. Anticancer Drugs. 2016;27(1):66–70. doi:10.1097/CAD.0000000000000294
93. Lim W-T, Ng Q-S, Ivy P, et al. A Phase II study of pazopanib in Asian patients with recurrent/metastatic nasopharyngeal carcinoma. Clin Cancer Res Off J Am Assoc Cancer Res. 2011;17(16):5481–5489. doi:10.1158/1078-0432.CCR-10-3409
94. Hsu C, Lee S-H, Ejadi S, et al. Safety and antitumor activity of pembrolizumab in patients with programmed death-ligand 1-positive nasopharyngeal carcinoma: results of the KEYNOTE-028 study. J Clin Oncol Off J Am Soc Clin Oncol. 2017;35(36):4050–4056. doi:10.1200/JCO.2017.73.3675
95. Delord J-P, Antoine Hollebecque JP, De Boer J, De Greve Jean-Pascal H, Leidner RS. An open-label, multicohort, phase I/II study to evaluate nivolumab in patients with virus-associated tumors (CheckMate 358): efficacy and safety in recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC). J Clin Oncol. 2017;35(15_suppl):6025. doi:10.1200/JCO.2017.35.15_suppl.6025
96. Ma BBY, Lim W-T, Goh B-C, et al. Antitumor activity of nivolumab in recurrent and metastatic nasopharyngeal carcinoma: an international, multicenter study of the mayo clinic phase 2 consortium (NCI-9742). J Clin Oncol. 2018;36(14):1412–1418. doi:10.1200/JCO.2017.77.0388
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.