")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Chinese calligraphy handwriting (CCH): a case of rehabilitative awakening of a coma patient after stroke
Authors Kao HSR, Lam SPW, Kao TT
Received 30 July 2017
Accepted for publication 11 December 2017
Published 31 January 2018 Volume 2018:14 Pages 407—417
DOI https://doi.org/10.2147/NDT.S147753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Wai Kwong Tang
Video abstract presented by Henry Kao.
Views: 2675
Henry SR Kao,1 Stewart PW Lam,2 Tin Tin Kao3,4
1Calligraphy Therapy Laboratory, Shenzhen Institute of Neuroscience, Shenzhen, China; 2Research and Development Division, Calli-Health Society, 3Department of Geography, 4Department of Psychology, University of Hong Kong, Hong Kong
Introduction: This study investigated the efficacy of Chinese calligraphy handwriting (CCH) for the awakening of patients under a vegetative state after stroke. The theories, the instrument, and the treatment protocols were reported. A single case of a severe stroke patient who was in a coma state for 2 years is presented in this study. The objectives were to apply finger writing as a new method to awaken a stroke patient in a coma state and to test the effect of this method in improving the patient’s vegetative states over time.
Case presentation: A 55-year-old man suffered a severe stroke in 2004 which left him in a coma for 2 years without any systematic rehabilitation. A culture-based finger-writing method of visual-spatial intervention was then applied to improve his condition. The writing tasks involved aided viewing and finger tracing of sets of innovative characters with enriched visual-spatial and movement characteristics. Following regular treatment protocols involving diverse movement and sensory feedback, the patient was awakened after 12 months. As a consequence, the patient showed significant behavioral changes favoring enhanced focusing, alertness, visual scan, visual span, and quickened visual and motor responses. The treatment continued for another 12 months. As the treatment progressed, we gradually observed improvements in his attention span and mental concentration. His eye ball movements – the left eye in particular – were quickened and showed wider visual angularity in his focal vision. Currently, the patient can now watch television, engage in improved visual sighting, and focus on visual-spatial and cognitive-linguistic materials.
Conclusion: This CCH method of training by finger tracking has shown its effectiveness in awakening the patient from his coma state and in producing long-term, clinical outcomes that were similar from those that took place 10 years ago. This finding supports the efficacy of the system for clinical improvement of the patient’s conditions.
Keywords: calligraphy therapy, coma, vegetative state, awakening, functional plasticity, finger writing
Plain language summary
Calligraphy therapy involves handwriting of Chinese characters with a brush, which entails the marking of visual-spatial properties of the characters. This writing process activates and facilitates positive changes in the practitioner’s physiological, cognitive, and emotional well-being with proven therapeutic and rehabilitative success. The effective improvements include behavioral, neuro-cognitive, and somatic disorders or diseases such as posttraumatic stress disorder, autism, attention deficit hyperactivity disorder, Alzheimer’s disease, depression, and strokes. In this study, we employed Chinese calligraphy handwriting training to a stroke patient in a severe state of coma for 2 years. After 9 months of such calligraphy handwriting, the patient woke up from his coma state and showed behavior changes in the predicted direction. His conditions have remained stable in the past 10 years. The areas of improvement have included visual attention, mental concentration, quickened reactions, and wider visual span. A unique approach of finger writing was adopted in the effective treatment of this patient’s vegetative states.
Introduction
In our everyday speech, the word “coma” is often used in a general way to cover a wide range of conditions in which individuals have suffered brain injury, leaving them with no consciousness at all or with very limited consciousness.
We read or hear about celebrities, sports stars who are said to be in a “coma” for months or years, but they may probably be in a vegetative or minimally conscious state. It is very unusual for a coma to last more than a few weeks at most. People in a coma are completely unresponsive. They do not move, do not react to light or sound, and cannot feel pain. Their eyes are closed. The brain responds to extreme trauma by effectively “shutting down.”
After a few days or weeks in a coma, they may “wake up” to full consciousness with relatively little damage. If they have very severe brain injuries, they may move from coma into a vegetative or minimally conscious state.
In a vegetative state, they are still unconscious. They have no awareness of themselves or their environment. Patients in the “vegetative state” may have their eyes open and have involuntary movements of parts of their body or make reflex responses to loud noises or even occasional words. After 4 weeks, they are said to be in a “prolonged” vegetative state. If they remain in a vegetative state for several months after brain damage for 1 year after a traumatic brain injury, the chances of recovering consciousness are very low, and they are said to be in a “permanent” vegetative state.
In the areas of treatment and rehabilitation for coma recovery, brain stimulation such as fMRI, sound, light, and drug treatments has been the main system of the coma intervention. The ultimate goals are to act upon the arousal system in the cerebral cortex of the brain responsible for perception, thought, and cognitive behavior. There are growing efforts to support cognitive-linguistic therapies for people with language deficits after stroke in terms of neuro-linguistic and cognitive-neural therapies, such as visual-spatial rehabilitation for deficits associated with right hemisphere stroke in favor of the alternative conditions with cognitive rehabilitation.1 We need to examine the therapeutic factors and patient characteristics that optimize the clinical outcomes of cognitive rehabilitation. We seek long-term studies to determine its efficacy in restoring function.
In this paper, we introduce a unique, innovative, and culture-based calligraphy training as an effective system of cognitive neural therapy and rehabilitation for stroke patients. In addition, we do so by applying this evidence-based intervention in a single case of severe stroke patient from coma to vegetative awakening, which was the purpose and aim of this investigation.
Theory
A conceptual framework has been advanced to highlight a systematic analysis of the Chinese characters’ structural components and their role in the act of character writing within a dynamic behavioral cybernetic system.2,3
This writing involves the visual-spatial relations and the numerous and diverse components of Chinese characters that directly connect and promote the connections of cranial nerves. Stimulation of the cerebrum should be able to strengthen with the multidimensional visual-spatial relations, combination, variation, shape differences, and so forth. Early research discovered that Chinese character writing has the function of brain cognitive activation, which may be concerned with the functional plasticity of human cerebral cortex. When processing the visual-spatial configurations of Chinese character forms at writer’s cortical level, the writing activity constitutes reproduction, restoration, and processing of visual perception processing. This action can therefore initiate the activation function to be advantageous and facilitative to the operation of cognitive activity, and further mold and enhance the functions of related cortical substrates.4,5
The Chinese calligraphy handwriting (CCH) therapy
CCH involves visual perception of the character, spatial structuring of the character, cognitive planning, and maneuvering of the brush to follow specific character configurations. In recent years, it has been gradually established as an indigenous and complementary practice that is capable of improving people’s behavioral, psychosomatic, as well as clinical conditions. These include attention and concentration, physical relaxation, and emotional stabilization. Successful treatments with this intervention have been obtained with patients of strokes,3,6 Alzheimer’s disease,3 cancer,7 and posttraumatic stress disorder.8
In one case study, four stroke patients with a history of affected right side were treated with CCH intervention. The results of the pre- and posttreatment suggested that there were significant improvements in palm strength of the affected hand and quicker response time in their fine motor coordination tasks.6
The theoretical framework for calligraphy treatment is threefold.8,9 First is the sensory feedback: the individual receives sensory feedback from the graphic record while practicing calligraphy. Second is the bio-emotional feedback: calligraphy involves the movement of the arms and the body as the guide to regulate their movements. Finally, the cognitive feedback: the subjective experiences of heighted attention, alertness, and quickened responses during the writing acts.5,8
A suitable approach to brush handwriting especially for the stroke patients involves integration of multilevel feedback when designing the writing tasks, task materials, and training protocols, as well as some caring specifications, facilities, and training procedures similar to those used for the handicapped.10 Therefore, we adopted a conceptual principle of social feedback in task operation.11
This is done by a caregiver holding the hand of the patient to perform the brush writing act of the characters or to engage in finger writing in order for the patient to benefit from the tactile and motion feedback that is generated by the acts of finger writing.
The cognitive-neural foundations
We have identified several previous studies in the literature that provided the cortical foundations for the practice of the visual-tactile feedback in finger writing for stroke recovery.
Study group 1
Studies of some individuals in whom the intercortical pathways were sectioned with the objective of controlling convulsions showed that the cortical association neurons connecting the two sides of the brain have a significant role in determining the patient’s responses to visual, auditory, and tactile stimuli, with each channel being similarly affected by the task operations concerned.12
It was reported that extensive destruction of most of the neural connections between the two cerebral cortices produces either no diminution or at least an inconsistent diminution – of the patients’ ability to transfer the motor habits learned by use of the preferred side to the opposite side of the body.13
The following conclusions are evident: the neural integrative functions of the cortex in learning are closely bound to the specific reactive and psychophysical mechanisms of the sensory and motor projection areas of the brain. This implies that the use of one hand to perform a writing task would not hinder the reactive and physical learning mechanism of the cortex by the fingering act.
Study group 2
Recent neuroimaging research has focused on CCH and brain activation studies.14 Valid resting-state fMRI data were collected from the CCH and control participants. The CCH individuals showed better neural functions of updating and inhibition, but the two groups did not differ in shifting. The CCH group also showed stronger resting-state functional connectivity than the control group in the brain areas involved in updating and inhibition. These results suggested that long-term CCH training may be associated with improvements in specific aspects of the executive functions and the strengthened neural networks in related brain regions. This means that finger-writing would also facilitate this functional effectiveness of the brain as compared with that observed in the brush CCH training.
Study group 3
Some recent research studies have confirmed the neuroplasticity of the handwriting act. Specific findings have shown that white matter and gray matter changes occur accordingly after handwriting acts have been performed.15–21 Of particular interest to the calligraphy study is that the CCH and the control groups did not differ in intracranial volume. Compared to the control subjects, the CCH group showed a smaller cingulate gyrus volume (CGV). Previous studies15–21 discovered that the cingulate cortex is involved in the process of visual stimulus, pre-motor planning, and memory, which are vital in the CCH training. As the CCH subjects all started the exercise at a very young age, this may have promoted the efficiency of neurons in the cingulate gyrus. A smaller CGV in the CCH groups suggested that long-term CCH practice may reshape the brain structure by increasing the efficiency of the neural activity.22 An application of fingering writing as a writing task would be expected to produce and enrich similar cortical change derived from these neuroplasticity studies reported above.
Calligraphy as visual art
Study group 4
Chinese calligraphy is long regarded as a unique form of visual art, and as such, its esthetic properties deserve close examination from a neuroscience perspective. A recent study has investigated the neural responses of viewing the three forms of oil paintings, that is, the “representational,” the “indeterminate,” and the “abstract” forms through the fMRI analyses. The representational paintings, the form with the least visual indeterminacy, turned out to be the most salient and stimulating type of the three types of paintings in terms of cortical activations.23
Their results showed that the subjects recognized familiar objects faster in representational than in both the indeterminate and abstract paintings. This activation was found within a distributed cortical network that includes visual, parietal, limbic, and prefrontal regions. In plain language, the representational paintings, which depict scenes cluttered with familiar objects, evoked stronger activation than the indeterminate and abstract paintings in higher-tier visual areas. It was suggested that perception of familiar content in art works is mediated by object recognition, memory recall, and mental imagery, cognitive processes that evoke activation within a distributed cortical network.
Chinese calligraphy is the most orthodox, determinate, and invariant form of art, which is above and beyond the representational visual form of the paintings. This is so by virtue of the character’s structure, complexity as well as its graphic and linguistic forms. Chinese calligraphy training has been found to be capable of enhancing precisely such neuro-cognitive effects. It is a visual art with the fullest of visual invariability much beyond the representational paintings. Understandably, it functions more effectively than the three oil paintings in terms of the cortical activation of the brain. These findings can strengthen the neuro-cognitive impacts of the calligraphy training from a visual arts perspective.
Calligraphy as implied motion
In the arts field, an important element is implied motion, which can be suggested visually in a variety of ways: through the use of diagonal, gestural, and directional lines; repetition; position and size of objects; the position or implied eyeline of a figure, a symbolic representation of movement, and so on. The implied motion in calligraphy writing involves cognitively tracking, following or forward-recalling the established paths of the character strokes as well as the unit of the character construction. Upon executing the strokes, the writer performs real-time action of writing while at the same time mentally recalling and retrieving the ensuing parts of the character by the writing action. For the whole character, the writer mentally imagines the structure of the character and makes action plans before the specific actions. This form of implied motion comprises the dynamic processes of mental preparation, real-time execution, as well as post-task feedback of the motions and related visual results. Through this sequence, he trains the skill of writing, is rehearsing the writing act, and is fed back as his graphic, cognitive, neural as well as behavioral outcomes.
Several recent studies have examined the nature of neural and cognitive mechanisms of the real motion and implied motion that have direct relevance to the act or viewing of calligraphy writing.
Study group 5
One study on the increase of brain functional plasticity from learning real painting could be seen also from the learning experience of implied motions. This shows that learning effects from real painting could be generalized to unlearned painting by confirming that a positive transfer of learned activities, can be observed in increased functional plasticity.24 When this finding is applied to calligraphy training, the real movement or implied movement is actually shared in the same neural network in the brain, and therefore, the effects in neuronal activation must be a combined impact from both dynamic real and implied motions included in the calligraphic act showing cumulated cerebral excitation and stimulation. These may be the reasons behind the enormous impacts we have found in our past research and clinical applications of practicing calligraphy.
Study group 6
Another study25 found that brain regions involved in visual analysis of motion are also engaged in processing implied dynamic information from static images. They also found stronger cortical fMRI activation during the viewing of a static object image with implied motion than the viewing of object image without implied motion. These results suggest that brain regions involved in the visual analysis of motion are also engaged in processing implied dynamic motion from static images.25 This indicates that since calligraphy writing involves real as well as implied motions, it is natural to see some added, facilitating cognitive effects of the practice. Our past work on calligraphy treatments has confirmed such observations.
Brain activation with implied motion
Study group 7
Another study examined the neural connectivity and plasticity during the observation of a classic oil painting – Michelangelo’s frescos – with and without implied motion.26 The findings showed that observation of implied motion in a painting specifically reduces the activity of inhibitory (PMd–M1) connections. On the contrary, the (PMd–M1) facilitatory connections were not affected during the observation of the painting. The results suggest that observation of implied motion in a painting modulates (PMd–M1) connectivity and plasticity. These results are consistent in that art with implied motion might be used as a plasticity-based intervention in rehabilitation.
These findings lend strong support to our own findings on the effects of calligraphy training in enhancing neural connectivity and plasticity in that this act involves both real and implied motions in the dynamic character-based writing processes. This suggests the role and functions of implied motions in the practice of calligraphy writing. In fact, our effective treatments with a number of disorders and disease attest to the nature of calligraphy as visual art, along with added health benefits therein.
These studies reviewed above offer an excellent integration of background and theoretical foundations to the design of a unique system of treatment of a single case of a vegetated stroke patient using finger writing as a new tactile feedback system of rehabilitation.
This system consists of the strengths of cognitive neural mechanisms, visual arts advances, as well as cognitive and behavioral activation in the context of implied motion for calligraphy practice. This effort constitutes the core of our confidence in forecasting calligraphic training as a valuable innovation as well as a productive system of rehabilitation.
Written informed consent was obtained from the patient’s family for publication of this report and any accompanying images. All persons in photograph consented to the publication of their image.
Case presentation
The patient at the age of 55 years suffered a severe stroke and was treated with neurosurgery, but did not make any progress in awakening from his coma. No cognitive or behavioral interventions were available as part of the medical treatment. His family approached our research team for developing an innovative system of rehabilitation. For 2 years after the stroke incident, the patient was totally unresponsive to any known treatment system.
Case expectations
On the basis of the current status of the CCH research as well as the vast related research on handwriting and neural esthetics as reviewed in previous sections, we predicted the outcomes from the application of the finger writing treatment of a single case of a severe stroke patient in the coma state:
- Awakening from a coma state after 2 years of the patient’s stroke
- General improvement of his motor control and manipulations
- Higher visual scanning and visual span
- Increased attention span and alertness, and concentration
- Increased eye fixations, focusing, as well as broad watching activities
- Improved patient’s subjective well-being during the caring period
The method
The design of different types of writing instruments in use today provides different sources of visual, tactile, and kinesthetic feedback effects of the writing tasks.27 The practice of finger writing with tactile feedback and visual feedback was adopted for this treatment. On the basis of literature review, a recent pilot study investigating the efficacy of finger writing with respect to some cognitive and physical benefits with enhanced improvements in attention, cognition, heart rate, blood pressure, and skin temperature had been reported.28
The present stroke rehabilitation course followed a sequence involving three depths of the carved grooves of the characters: 4 mm depth for the first month; 2 mm depth for the second month, and 0 mm depth (plane) for the third month. But due to the patient’s physical conditions, the 0 mm depth of the characters was not implemented. Each character was mounted onto a plastic board to provide tactile, motor, and visual tracks when tracing by the index finger sensorimotor feedback10,27–30 throughout the treatment course before the patient’s initial awakening (Figures 1 and 2).
 | Figure 1 Some of the special characters and the design of the writing plates with grooved characters. |
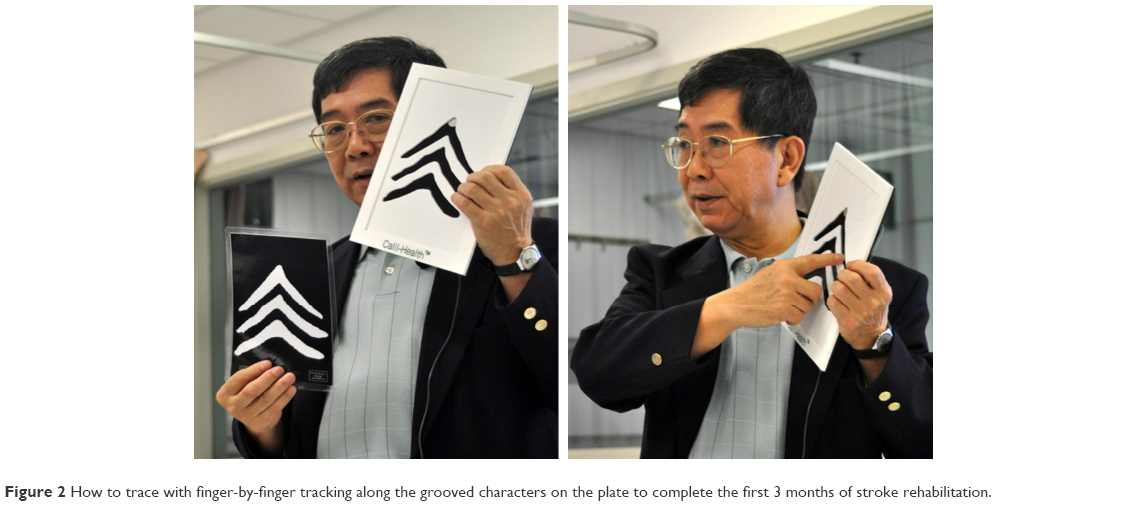 | Figure 2 How to trace with finger-by-finger tracking along the grooved characters on the plate to complete the first 3 months of stroke rehabilitation. |
The fourth month was planned at enhancing the patient’s cognitive abilities and functions as well as fine motor skills with a real brush for handwriting calligraphy.31,32 It would require suitable arm and finger dexterity for clinical implementation. The patient did not reach such a state of his conditions throughout the treatment duration. Therefore, we ran a 3-month cycle only for the finger writing training.
The 3-month treatment had 3–5 sessions a week, which was as much as could be arranged with the patient. There were 4 consecutive weeks to a month, and there were 4 months to the course. At the end of the treatment period, the whole course was to be repeated all over again for the same patient for another 4 months or until he was awakened at some stage. Then after this training, the whole protocol was repeated for another two cycles until the patient’s awakening after the 9 months.
The original design of this unique full 4 months finger and brush writing protocol for this single case stroke patient consists of 40 character plates for the finger writing tasks. Each plate had one character within an 8″×6″ plastic frame. There were two different character plates that were used for each training session, five repetitions of each character for a total of 10 character finger writing were performed for each training session. The schedule included 3–5 sessions per week and 4 weeks per month.
The first month protocol had the characters grooved at 4 mm in depth for all the plates, while the second month followed the same protocol but with a 2 mm depth for all the characters. The third month had the protocol using flat or 0 mm character depth for all characters.
Throughout the cycle of treatment, the patient was aided by two assistants, with one holding the patient’s writing hand to guide the finger movements for writing action and another helping the patient by opening his eyes during the session. The fourth month had the writing with a brush in actual writing action that adopted the same treatment strategy (Figures 1 and 2).
The patient
The patient had a severe stroke in early January 2004. His condition remained severe and unstable for more than a year. During this period, we could neither do anything for him, nor could the team of medical doctors in Hong Kong that looked after him. In March 2005, his condition stabilized. He was transferred from the acute hospital to a rehabilitation hospital. But his physical condition remained very weak and almost could not allow him to survive; neither could we apply any kind of therapy nor exercise other than daily sit-ups or sleep.
The patient takes a dosage of muscle relaxant and hypertensive drugs at 1:00 PM daily and then goes to sleep afterward for a few hours. He seldom engages in voluntary activities out of his own volition, but does engage in passive responses to some stimulation from other people. He does, however, show eye pursuits with objects or people around him occasionally. Physically, he maintains good and stable physical health, some voluntary motions, and is able to attend to voices and sound stimuli from time to time. He has been in such a condition consistently for the past 10 years.
The treatment
Below is an onsite account from the spouse and carers of the patient on their observations of the patient’s physiotherapy and calligraphy therapy. She reported that:
Nothing helped in waking up the patient, including physiotherapy, but only the calligraphy-treatment. Before the first calligraphy-training session, the patient had already been doing physiotherapy with the help of the caregivers with some physical exercises in order to keep and strengthen the physical condition of his body. During that time, the patient showed no response at all, except in one of his fingers. When we were holding his hand, there was a slight response and weak strength from this finger.
This was the reason we started to design calligraphy treatment plan with finger tactile writing movements therapy for the first 3 months with three different levels of strength of tactile feedback, and the last month was brush writing therapy for cognitive and fine motor controls if the stroke patient could perform with the help of the caregivers to guide his brush-holding acts.
In 2007 we received the permission to invite Professor Kao’s team to treat the patient for therapy and rehabilitation. Unfortunately, the arrangement of pre- and post-fMRI or DTI-fMRI measures for the patient by his medical doctors in the hospital was not possible at that period, so it was decided to start calligraphy-therapy without brain scanning and only to pursue behavioral observations. Before the treatment, the patient’s physical health remained very weak. He could only sit up with external support. He could not focus his attention on any objects. We suspected that he might have some hearing difficulty but we could not confirm. He could not respond to any external stimulation.
The calligraphy therapy was conducted on the patient with the help of three nursing staff. One helped him to sit up, the second one helped him to position his head upright and direct his attention and focus on the treatment tasks, and the third one held his index finger and ran it through the grooved Chinese characters on the board. Simultaneously, we also spoke out to describe each stroke of the character to him and called out the structure of the character to him while he was performing the finger handwriting exercise. We let him do the above therapy a few times a week if his physical condition allowed. Each session lasted for about 45 minutes to one hour. The character boards were changed occasionally at random. We used only simple characters with easy and simple constructions to facilitate the execution of the writing exercise. There were two boards used for each daily session that cover one character for each board in the training session.
The training tasks involved viewing as well as writing actions integrated during the task performance with repetitions for up to the 45-minutes required. The total duration of the training course lasted for 12 months including 3 last months while the patient was still the rehabilitation hospital. Subsequent to his discharge, the exercise continued for about 9 more months in his home before he finally woke up and regained his consciousness. He went on and continued with this calligraphy intervention regularly for another 12 months intensively following the same protocol and treatment routine for another 12 months before we suspended the exercise, making it a total of 24 months of calligraphy treatment.
After that, the patient was given such training exercise on an occasional and irregular manner.
The awakening took place about two years after the initial 12 months without the calligraphy treatment. By that time, he had turned into a vegetative state of his medical conditions.
Pretreatment: behavioral observations
The patient, who was helped by nursing care staff throughout the treatment duration, was expected to benefit from the finger writing activities and functions, which would stimulate brain response and result in elicited and increased neuroplasticity. The patient’s wife reported on the patient’s conditions that
he had a strong reaction and grumbled a few days after starting treatment, as if we forced him to work hard and did not seem to have enjoyed it. He did not experience good sleep at night, as if he was in a dream state. Now, he can look at her with his eyes.
She also said that the most significant induced changes in this stroke rehabilitation course were “arousal,” “attention,” and “mental concentration,” which was more effective than other rehabilitation methods that he had during this training period.
Posttreatment: behavioral outcomes
After starting the calligraphy therapy for the first few days, the patient’s reaction was that he grumbled and complained about the therapy, as though we were forcing him to work hard. He did not seem to be enjoying it. He also did not sleep well at night, possibly due to being over-excited by the treatment. This is unclear to us since he sometimes also had occasional sleepless nights. For a period of about 9 months at the rehabilitation center, we did not notice any improvements on him. We did not know how much he knew what was going on, and how much the finger writing therapy was benefitting him. This practice continued for almost 9 months until he was moved out of the rehabilitation hospital.
Almost after 9 months of calligraphy treatment, we gradually saw the improvements on the patient. His eyes could focus much better on objects displayed in front of him, and his eyesight could move much better and could follow moving objects slowly. He seemed to regain some attention ability. We have noticed significant improvements in his attention span, visual span, and mental concentration. His eye ball movements, in particular the left eye, was much quicker and could see a wider visual span. We observed that “he can now watch television, or focus on the screen of the TV much better.” This is the most significant improvement, and we believe this finger writing therapy had impacted him. Occasionally at night, he even entered into a crying state for about 1 hour, indicating he might have encountered some memories of sad emotions of some kind. We stopped his calligraphy treatment 12 months after its commencement.
The patient now continues to enjoy a wakeful and alerting mental state, regularly and on daily basis, for about 3–4 hours each in late morning, mid-afternoon, and early evening every day. He is now in his 10th year since his awakening in 2007 following 9 months of our finger writing treatment on him. Presently, he is given physical therapy with muscular exercise, arm and leg movements, as well as massage sessions twice a day by the caregivers. In addition, he takes regular medicine for blood pressure and muscle relaxation. Before his finger writing program, he had been already doing physiotherapy, but with a very little improvement as he showed no consequential responses at all. So, we did not believe that the waking effect was due to his physiotherapy. His present day physical exercises on daily practice are needed to maintain his physical strength and muscular comfort and relaxation. Little cognitive changes have been observed due to such therapies.
The current status of the patient
For the purpose of updating the status as well as its longer impact of the finger writing training of the patient, we visited the patient, his spouse, and his caring staff in his home on November 10, 2017. Besides interviewing the patient’s wife and staff, we conducted the first calligraphy finger writing session since 2007 in order to gain a first-hand information and observations about the patient. The session lasted 45 minutes.
We were pleasantly surprised with the following observations of the patient during the writing session:
- Clear signs of eye movements
- Eye-tracking taking place in the later stage of the finger writing session
- Eye-opening wider and broader as the session progressed
- Increasing attention to the tasks of writing, hearing the writing instruction from the nursing staff
- Increasing concentration as the tasks continue in the process
- Increasing sign of emotional relaxation and soothing states of the moods
- Relaxed and increased signs of smiles and happiness
- Increased hearing and comprehension of verbal instructions
- More focused attention and eye fixations
- Heightened states of neural-cognitive arousal
- Alerting and quickening of responses to external stimuli such as sounds, voice, movements
- Fully developed signs of emotional stability and memories
- Enhanced processing abilities in perception, cognition, and motoric responses
- Clear signs of his joy, enjoyment, and absorption in these writing activities
We are pleased to share our satisfaction of these and other forms of expression in visual perception, gestural movements, and motoric facilitation. Figures 3–5 present photographs on some of these activities of the patient which confirm the past, lasting effect as well as the patient’s current behavior activities onsite.
 | Figure 3 Stroke patient’s ability to respond to object from opening his eyes from slim (top left) to moderate (top right) and to full openings (bottom). This took place gradually from the task onset and during early stage of the training session. |
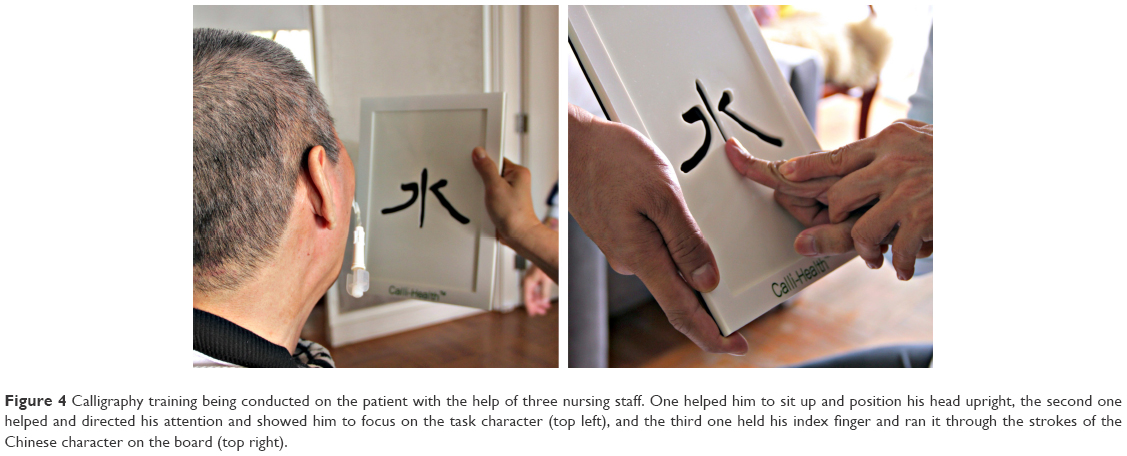 | Figure 4 Calligraphy training being conducted on the patient with the help of three nursing staff. One helped him to sit up and position his head upright, the second one helped and directed his attention and showed him to focus on the task character (top left), and the third one held his index finger and ran it through the strokes of the Chinese character on the board (top right). |
 | Figure 5 Patient’s eye opening wider and broader in increasing concentration at the task of finger writing with joy (left) and eye fixations on the tasks as the session progressed (right). |
Discussion
The significant results of this finger writing therapy for brain stroke rehabilitation are interpreted from the framework of sensorimotor feedback theory.8,10,33,34 This is learned and practiced by the finger tracing on the groove of the carved Chinese character plates, using the tactile,27,28 feeling, and the task tracking29,30 of feedback control of the sensorimotor movement of the writing finger in order to stimulate brain responses and activation14 to elicit neuroplasticity.22,33–36 This dynamic practice contributes to the effectiveness of the stroke rehabilitation.31,32
This single case clinical trial has showed that the stroke patient was awakened by the arousal effect induced by a 9-month intensive CCH treatment by finger tracing and stroke tracking which also demonstrated that the patient regained his attention span, visual span, and mental concentration. The most convincing outcome is that the patient can now watch television or focus on the screen of the TV much better. His eye ball movement, particularly his left eye, is much quicker, and his eyes had a wider visual field. This improvement on the patient’s visual span may be explained by the basic theory that is often applied to eye guidance. It is assumed first that the direction and location in space are learned by temporal association between visual and tactile experience, and second, that the two eyes are exactly conjugate in their response to visual stimuli. Findings of previous experiments in binocular synchronization with advanced computer instrumentation revealed precisely that the left eye led the right eye in most of the measures of reading. It substantiates the observations that “outward” movements of the eye were slower than “inward” movements.37
This single-trial case has yielded significant findings that are in line with our theoretical predictions of the patient’s behavioral changes through the practice of finger writing system. This is most encouraging, in that for the first time we were able to design, implement, and produce behavioral outcomes that had not been possible before we began. The patient is presently fully awake, able to watch TV programs, showing steady visual and spatial spans, attention span as well as cognitive and emotional concentration.
Conclusion
This is the first reported case of calligraphy therapy in the successful treatment of a severe vegetative patient from coma due to stroke. We have made significant contributions to the following aspects of stroke-related therapy and rehabilitation: 1) awakening the patient from his coma state after 2 years of his clinical vegetation; 2) sustained and long-term improvements of his clinical and behavioral conditions some 10 years after the suspension of the handwriting treatment; 3) retention of the patient’s posttreatment behavioral changes over time; and 4) the efficacy of the innovative system of finger writing intervention as a novel cognitive method of rehabilitation on stroke patient’s recovery and sustained clinical benefits.
Specifically, in relation to the neural foundations of handwriting and vegetative therapy and rehabilitation, we look forward to further confirming the benefits of 1) learning the cortical mechanism of the motor sensory areas of the brain, 2) enhanced functional effectiveness of the brain through the task of finger writing, and 3) increased neuroplasticity of the brain through neuronal changes from this writing task as well as from 4) the facilitated neural esthetic experience that is inherent in the process of calligraphic production and appreciation.
In conclusion, we are pleased that the present study adds to the growing efforts to support cognitive-linguistic therapies for people with language deficits after stroke. In this context, some neuro-linguistic and cognitive-neural therapies such as visual-spatial rehabilitant are important for deficits associated with right hemisphere stroke. The calligraphy handwriting training may provide favorable alternative conditions for cognitive rehabilitation.1
Acknowledgments
We would like to thank Professor Li-Hai Tan, Director of the Shenzhen Institute of Neuroscience, and Professor Cecilia LW Chan of the Department of Social Work and Social Administration, the University of Hong Kong, for their support of our work in Chinese calligraphy therapy; Dr Thomas J Smith of the School of Kinesiology of the University of Minnesota kindly offered insightful comments and Dr Min Xu helped with editorial suggestions. We also thank Ms Manlin Zhang of the National Mental Health Network, Beijing, for helpful advice on selecting Chinese characters. Preparation of this article has been supported by the Shenzhen Basic Research Grant (JCYJ20170412164259361).
Author contributions
HSRK wrote the manuscript; SPWL helped with design and instruments; TTK provided review and all revisions. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Saper CB. Waking Up from Coma: New Treatments, New Hope. Report on Progress. The Dana Alliance for Brain Initiatives, April 2013. | ||
Kao HSR. Chinese calligraphic handwriting (CCH): a science for health and behavioural therapy. Int J Psychol. 2006;41(4):282–286. | ||
Kao HSR. Calligraphy therapy: a complementary approach to psychotherapy. Asia Pac J Couns Psychother. 2010;1(1):55–66. | ||
Kao HSR. Psychogeometric principles of Chinese character writing. In: Leedham G, Leung M, Sagar V, Xiao X-H editors. Proceedings of the 9th Biennial Conference of the International Graphonomics Society. Singapore: Nanyang Technological University; 1999;107–110. | ||
Xu M, Kao HSR, Zhang M, Lam SPW, Wang W. Cognitive-neural effects of brush writing of chinese characters: cortical excitation of theta rhythm. J Evid Based Complementary Altern Med. 2013;2013(975190):11. | ||
Chiu ML, Kao HSR, Ho MY. The efficacy of Chinese calligraphic handwriting on stroke patients: a multiple cases study. Proceedings of the Second International Congress on Vascular Dementia, Salzburg, Austria; 2002:207–212. Available from: http://hub.hku.hk/handle/10722/109884. Accessed January 3, 2018. | ||
Yang XL, Li HH, Hong MH, Kao HSR. The effects of Chinese calligraphy handwriting and relaxation training in Chinese Nasopharyngeal Carcinoma patients: a randomized controlled trial. Int J Nurs Stud. 2010;47(5):550–559. | ||
Zhu ZH, Wang R, Kao HSR, et al. Effect of calligraphy training on hyperarousal symptoms for childhood survivors of the 2008 China earthquakes. J Neuropsychiatr Dis Treat. 2014;10:977–985. | ||
Kao HSR. The visual-spatial features of Chinese characters and a psychogeometric theory of Chinese character writing. In: Kao HSR, editor. Chinese Calligraphy Therapy. Hong Kong: Hong Kong University Press; 2000. Chinese. | ||
Smith TJ, Smith KU. The cybernetic basis of human behavior and performance. Continuing the Conversation, a Newsletter of Ideas in Cybernetics, Official Newsletter of the American Society of Cybernetics, ASC Issue Number 6–18. 1988;15:1–30. | ||
Ting T, Smith M, Smith KU. Social feedback factors in rehabilitative processes and learning. Am J Phys Med. 1972;51(2):86–101. | ||
Smith KU. The functions of the intercortical neurones in sensorimotor coordination and thinking in man. Science. 1947;105(2722):234–235. | ||
Smith KU. Learning and the associative pathways of the human cerebral cortex. Science. 1951;114(2953):117–120. | ||
Chen W, He Y, Gao Y, et al. Long-term experience of Chinese calligraphic handwriting is associated with better executive functions and stronger resting-state functional connectivity in related brain regions. PLoS One. 2017;12(1):e0170660. | ||
Plantona S, Juclac M, Rouxa FE, Démonetd JF. The “handwriting brain”: a meta-analysis of neuroimaging studies of motor versus orthographic processes. Cortex. 2013;49(10):2772–2787. | ||
Cao F, Vu M, Chan DHL, et al. Writing affects the brain network of reading in Chinese: a functional magnetic resonance imaging study. Hum Brain Mapp. 2013;34(7):1670–1684. | ||
Gimenez P, Bugescu N, Black JM, et al. Neuroimaging correlates of handwriting quality as children learn to read and write. Front Hum Neurosci. 2014;19(8):155. | ||
Richards TL, Grabowski TJ, Boord P, et al. Contrasting brain patterns of writing-related DTI parameters, fMRI connectivity, and DTI–fMRI connectivity correlations in children with and without dysgraphia or dyslexia. Neuroimage Clin. 2015;8:408–421. | ||
Yuan Y, Brown S. Drawing and writing: an ALE meta-analysis of sensorimotor activations. Brain Cogn. 2015;98:15–26. | ||
Cao F, Perfetti CA. Neural signatures of the reading-writing connection: greater involvement of writing in Chinese reading than English reading. PLoS One. 2016;11(12):e0168414. | ||
Planton S, Longcamp M, Péran P, Démonet JF, Jucla M. How specialized are writing-specific brain regions? An fMRI study of writing, drawing and oral spelling. Cortex. 2017;88:66–80. | ||
Chen W, Chen C, He Y, Wang Y, Wang W. Long-term Chinese calligraphy handwriting reshapes the cingulate gyrus: a VBM study. Poster presented at: 22nd Annual Meeting of the Organization for the Human Brain Mapping; June 26–30; 2016; Geneva, Switzerland. | ||
Fairhall SL, Ishai A. Neural correlates of object indeterminacy in art composition. Conscious Cogn. 2008;17(3):923–932. | ||
Kim CY, Kim JE, Park M, Lee R. Brain functional plasticity reflecting learning of implied motion in abstract painting. Proceedings of the XXIV Conference of the International Association of Empirical Aesthetics, Vienna, Austria; August 29 to September 1, 2016:41. | ||
Kourtzi Z, Kanwisher N. Activation in human MT/MST by static images with implied motion. J Cogn Neurosci. 2000;12(1):48–55. | ||
Concerto C, Infortuna C, Mineo L, et al. Observation of implied motion in a work of art modulates cortical connectivity and plasticity. J Exerc Rehabil. 2016;12(5):417–423. | ||
Kao HSR, Smith KU, Knutson R. An experimental cybernetic analysis of handwriting and penpoint design. Ergonomics. 1969;12(3):453–458. | ||
Kao HSR. Finger writing for health: cognitive & physiological benefits. Poster presented at: The First National Mental Health Forum; April 12; 2017; Beijing. | ||
Kao HSR. The effects of feedback intermittency on compensatory tracking. Percept Motor Skills. 1976;43:1339–1345. | ||
Kao HSR, Smith KU. Cybernetic television methods applied to feedback analysis of automobile safety. Nature. 1969;222(5190):299–300. | ||
Kao HSR, Lam SPW. A Biofeedback-based system of calligraphy therapy. Poster presented at: The 2007 World Mental Health Congress of the World Federation for Mental Health; August 19–23; 2007; Hong Kong SAR, China. | ||
Kao HSR, Lam SPW. A biofeedback-based system of calligraphy therapy. Poster paper and booth demonstration with the Hong Kong University, Innovation Expo07; September 14–18; 2007; Hong Kong SAR, China. | ||
Smith KU. The geometry of human motion and its neural foundations. II: neurogeometric theory and its experimental basis. Am J Phys Med. 1961;40:109–129. | ||
Stepanyants A, Chklovskii DB. Neurogeometry and potential synaptic connectivity. Trends Neurosci. 2005;28(7):387–394. | ||
Siok WT, Perfetti CA, Jin Z, Tan LH. Biological abnormality of impaired reading is constrained by culture. Nature. 2004;431:71–76. | ||
Tan LH, Spinks JA, Eden GF, Perfetti CA, Siok WT. Reading depends on writing in Chinese. Proc Natl Acad Sci U S A. 2005;102(24):8781–8785. | ||
Smith KU, Schremser R, Huang A. Experiments in binocular synchronization. Nature. 1970;228(5278):1339–1341. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.