")
Back to Journals » Journal of Asthma and Allergy » Volume 13
Childhood Asthma Awareness in Saudi Arabia: Five-Year Follow-Up Study
Authors Alharbi SA, Kobeisy SAN , AlKhater SA , Alharbi AS, Alqwaiee MM, Alotaibi FN, Alawam KA , Alahmadi TS , Al-Somali FM, Almaghamsi TM, Yousef AA
Received 21 July 2020
Accepted for publication 3 September 2020
Published 2 October 2020 Volume 2020:13 Pages 399—407
DOI https://doi.org/10.2147/JAA.S272850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Saleh A Alharbi, 1, 2 Sumayyah AN Kobeisy, 1 Suzan A AlKhater, 3, 4 Adel S Alharbi, 5 Mansour M Alqwaiee, 5 Faisal N Alotaibi, 5 Khalid A Alawam, 6 Turki S Alahmadi, 7 Faisal M Al-Somali, 8 Talal M Almaghamsi, 9 Abdullah A Yousef 3, 4
1Department of Pediatrics, Dr. Soliman Fakeeh Hospital, Jeddah, Saudi Arabia; 2Department of Pediatrics, Umm Al-Qura University, Mecca, Saudi Arabia; 3Department of Pediatrics, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 4Department of Pediatrics, King Fahd Hospital of the University, AlKhobar, Saudi Arabia; 5Prince Sultan Military Medical City, Riyadh, Saudi Arabia; 6Inaya Medical College, Riyadh, Saudi Arabia; 7Department of Pediatrics, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 8Department of Pediatrics, Sulaiman Al Habib Hospital, Al Khobar, Saudi Arabia; 9Department of Pediatrics, King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia
Correspondence: Saleh A Alharbi
Department of Pediatrics, Dr. Soliman Fakeeh Hospital, Jeddah, Saudi Arabia
Email [email protected]
Background: Bronchial asthma is a chronic inflammatory airway disease that is characterized by reversible airway obstruction due to bronchial hyperresponsiveness. It is one of the most common chronic diseases. In Saudi Arabia, asthma affects 2 million people with asthma frequency in children markedly higher than adults with regional variations ranging from 9% to 33.7%.
Objective: The aim of this study is to measure asthma awareness and knowledge of study participants during the ongoing annual Saudi asthma awareness campaigns and compare them with previous survey data conducted in 2014.
Methods: A cross-sectional study was carried out in the form of a survey distributed across three major cities in Saudi Arabia, Jeddah, Riyadh and Dammam, during the National Asthma Awareness Campaign in major regional shopping centers in April 2019. Asthma knowledge scores across different demographic groups were generated from surveyed data. Descriptive and correlative statistical analyses were performed to identify factors associated with changes in asthma knowledge. Scores were compared to previous survey results.
Results: The mean score for asthma knowledge was 15.6 out of 25. Asthma knowledge significantly correlated with age (P=0.002), asthma status of the participants (P=0.001), having children with asthma (P=0.005) or knowing friends or family with asthma (P=0.029) but not with other socioeconomic factors such as gender, marital status, occupation, level of education and number of children in the family (P > 0.05). There was a significant difference in the asthma scores from 2014 (M= 63%, SD=26) to 2019 (M= 70%, SD= 26) conditions; t (24) = − 2.106, p=0.046.
Conclusion: Further educational campaigns are necessary to enhance and measure general public awareness of asthma, its differential diagnosis against other respiratory infections, environmental triggers, risk factors as well as treatment options.
Keywords: asthma, awareness, pediatrics, Saudi Arabia
Introduction
Bronchial asthma is a chronic inflammatory airway disease that is characterized by reversible airway obstruction due to bronchial hyperresponsiveness.1 It is one of the most common chronic diseases2 and by 2025 it is anticipated that it will affect 400 million people worldwide.3 Childhood asthma not only decreases the quality of life of the affected children, but also increases school absenteeism4 and causes a financial burden on their respective families.5 Challenges in decreasing the disease burden of asthma include, but are not limited to, poverty, pollution, tobacco usage, low level of education, cultural attitudes towards medications and emergency care dependence.6,7 Notably, increased disease severity, poor asthma management and poverty have been directly correlated to increased hospital admission in the pediatric age group.3 In light of this, the Global Initiative for Asthma (GINA) was established in 1989 in order to raise public awareness regarding asthma.6 Specifically, healthcare appointments with regular follow-up, consistent asthma education and written action plans are proposed for better disease control in asthmatics especially for those with a more severe disease course.8
In Saudi Arabia, asthma affects 2 million people, approximately 6% of the population.9 Furthermore, asthma frequency in children is markedly higher than adults with regional variations ranging from 9% to 33.7%.10 In response to the high prevalence of asthma in the region, an asthma awareness campaign was conducted in Saudi Arabia in 2014, during which a Structured Asthma Knowledge Questionnaire was formulated to assess 1039 random participants.11 This initial study concluded that asthma knowledge needs to be improved in the general population.11 In order to follow-up on these findings, this study aims to use a modified Structured Asthma Knowledge Questionnaire to evaluate the effectiveness of the annual Saudi asthma awareness campaigns during 2014–2019, with an additional focus on childhood asthma.
Patients and Methods
Study Design
A cross-sectional study was carried out in a survey format, in the major regional shopping centers of the major cities in Saudi Arabia, Jeddah, Riyadh and Dammam, during the National Asthma Awareness Campaign in April 2019. The study was approved by the Dr. Soliman Fakeeh Hospital Institutional Review Board (DSFH IRB) and the guidelines outlined in the Declaration of Helsinki were followed. The study population included any individual that was present at the sites in which the National Asthma Awareness Campaigns took place. All study participants gave full written consent to be part of the study and were assured anonymity. Those younger than 18 years of age were required to have parental consent as approved by the DSFH IRB.
The survey was implemented using a modified Arabic questionnaire adapted from a validated asthma knowledge questionnaire12 to measure awareness regarding childhood asthma in Saudi Arabia. The questionnaire consisted of three sections: demographics, questions about asthma and disease education. The demographic portion explored age, sex, marital status, number of children, level of education, city of residence and occupation, and whether the participants, their children or any of their friends and family members suffer from bronchial asthma. The second section consisted of 25 questions geared at gauging the participants’ awareness on asthma and the third part evaluated what sources were used to gain information on the disease. The original data was collected in Arabic, translated into English, and entered into a database.
The survey data used to support the findings of this study are available upon request from the corresponding author. Results of this survey were compared to previously reported survey data conducted by Al-Harbi et al during the 2014 asthma awareness campaign in Saudi Arabia which also implemented the modified asthma knowledge questionnaire.11
Asthma Knowledge Score Generation
A numerical scoring system based on 25 points from the second portion of the survey was devised to evaluate asthma knowledge. The composite asthma knowledge score was calculated by giving correct answers a score of 1 and incorrect or “do-not-know” answers a score of 0. Results were compared with the 2014 Asthma Knowledge Questionnaire results.
Statistical Analysis
Statistical analysis was done using IBM SPSS Statistics Version 20. ANOVA and independent samples t-test were used to compare the means of the sample. Paired sample T-test was used to compare the mean asthma scores between 2014 and 2019 questionnaires. Pearson’s correlation coefficient “r” was used to determine the correlations between continuous data. The level of significance (P- value), was taken at <0.05 with a confidence interval (CI) of 95%.
Results
Subject Demographics
A total of 475 people participated in the study across various age groups and regions of the country. The majority of the participants (74%) were female and 90% of those surveyed were between 18 and 50 years of age. More than two-thirds were married and 68.6% (326/475) had children. The maximum number of children was 8 and the average was 3. Approximately 34% of the participants were from the Eastern region of Saudi Arabia including cities such as Dammam, Dhahran and Al-Khobar, 37% from the Western regions of Jeddah, Makkah and Madinah and 22% from the Central region of Riyadh. The level of education and occupations of the participants varied; however, the majority (63%) held an undergraduate degree. Only 13% of survey participants claimed to have bronchial asthma and 22% stated that their children also suffered from the disease, however; more than 66% of the participants disclosed that their friends or family were asthmatic (Table 1).
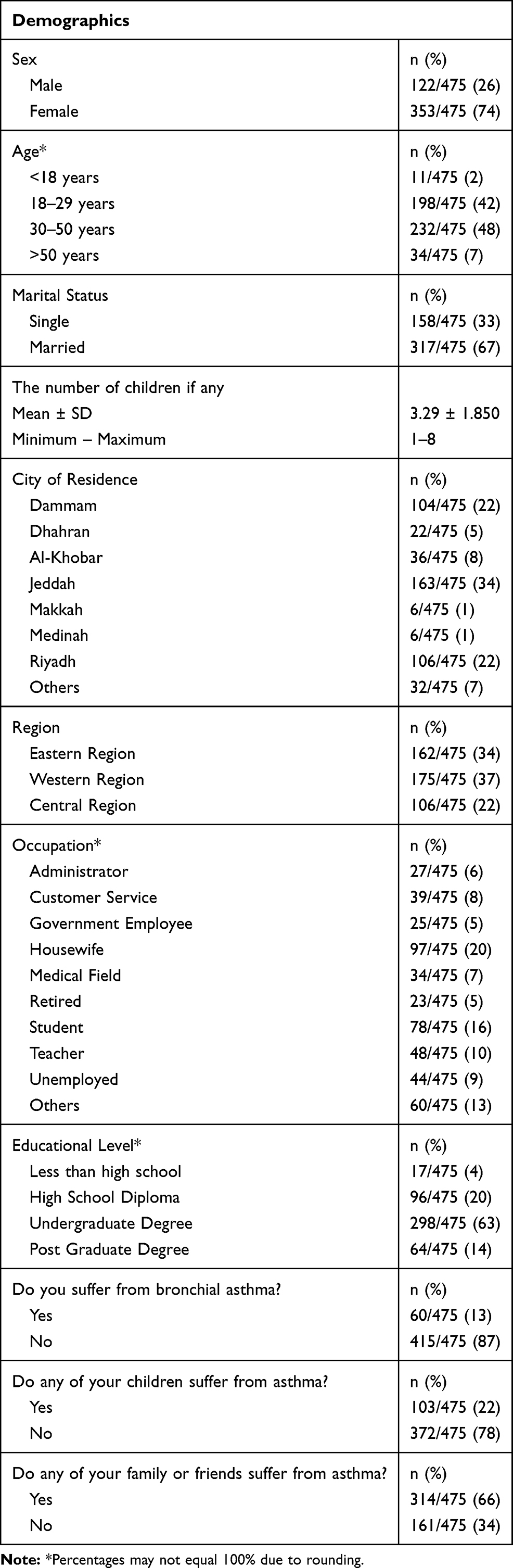 |
Table 1 Demographic Information of Survey Sample |
Asthma Knowledge
The asthma knowledge portion of the survey revealed that 90% of contributors knew that asthma is a chronic illness with acute exacerbations, 76% of the respondents correctly agreed that there is no difference between asthma and the term “chest allergies” and 70% correctly acknowledged that it can be a fatal disease.
Asthma Symptoms
Regarding disease symptoms, 88% were able to correctly identify that shortness of breath and nocturnal cough are symptoms of asthma. However, severe asthma symptoms in children were only recognized by 62% of those surveyed. Similarly, only 56% correctly understood that fever, runny nose and sore throat were not asthma symptoms. Eighty-four percent of participants properly recognized that genetic, hereditary and environmental factors play a role in asthma progression. Notably, the vast majority of participants (93%) were aware of the triggers that may lead to asthma attacks such as cigarette smoke, perfumes and paint fumes and 72% were aware of the direct relationship between respiratory infections and asthma progression. In contrast, only 58% of respondents knew that frequent antibiotic use did not diminish asthma symptoms and 55% were not sure of the relationship between eating fish at an early age and asthma development. Furthermore, 59% were not aware that sudden environmental changes could also affect the progression of asthma.
Asthma Treatment and Prevention
Regarding asthma treatment, 94% of respondents agreed that asthmatics should regularly follow up with their physicians for better results and more than 95% agree that asthmatic patients should inform their primary care providers of their symptoms and should be educated on how to manage an acute asthma attack. Similarly, the majority (87%) agreed that asthma medications cannot be used unless prescribed by a doctor and 71% believe that asthma patients need to be treated by a pulmonologist. However, only 51% of the participants knew that inhaled asthma medications do not cause an addiction and only30% correctly understood that prophylactic asthma treatment does not cause dangerous side effects if used without an acute asthma attack.
Asthma Education
Concerning the socioeconomic impact of asthma, 90% believe that specialized asthma centers are required to provide better education, 82% believe that the disease leads to school absenteeism and more than 80% see a need to include scientific content on asthma in school curricula as well as creating awareness programs (Table 2).
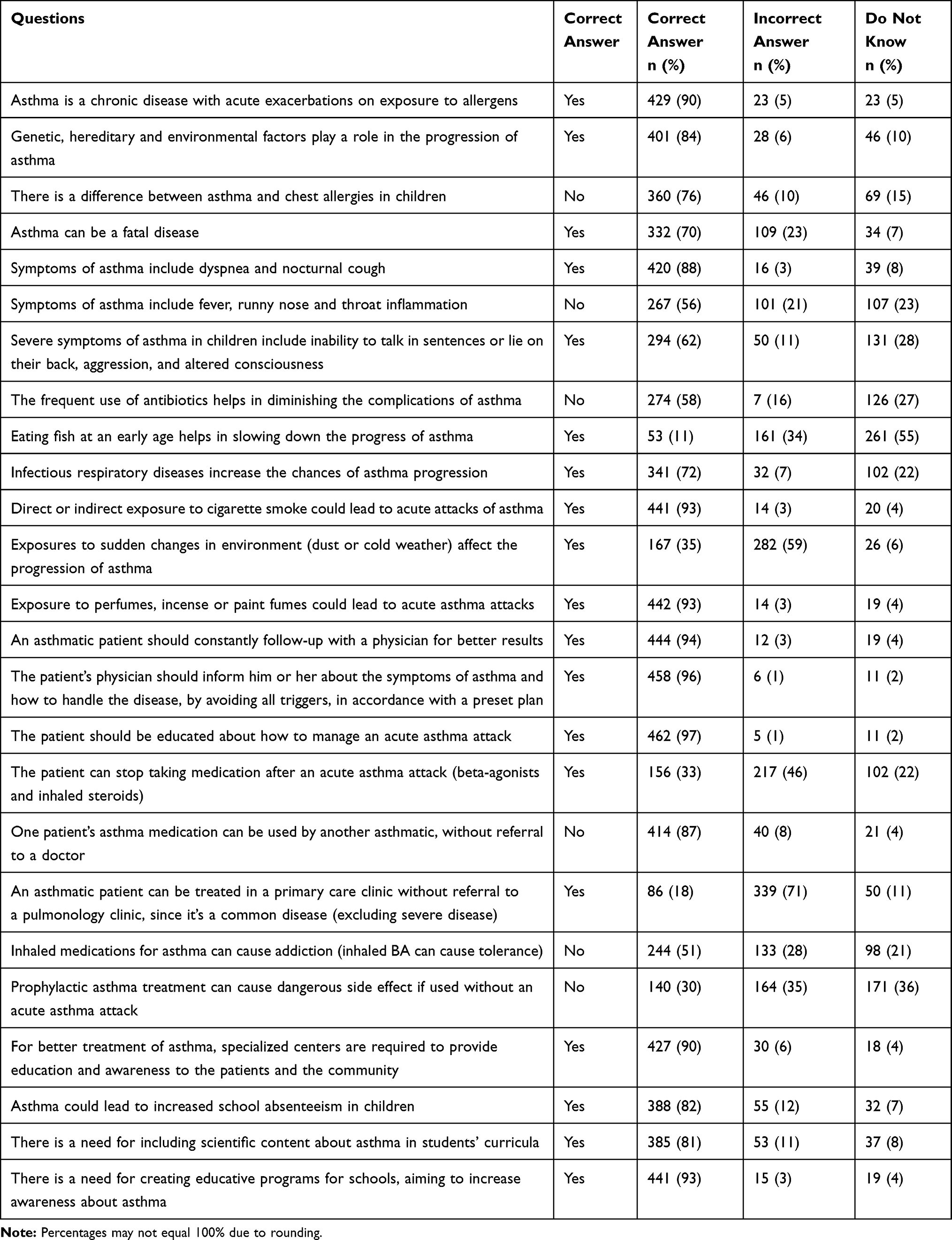 |
Table 2 Asthma Questions |
Based on the information described in Table 2, the mean score for asthma knowledge was 15.6 out of 25 (Figure 1). Demographic factors associated with asthma knowledge include age (P=0.002) as well as being affected with asthma (P=0.001), having children with asthma (P=0.005) or knowing friends or family with asthma (P=0.029). On the other hand, socioeconomic factors, such as sex, marital status, number of children and level of education did not have any statistically significant association with asthma knowledge (P > 0.05) (Table 3).
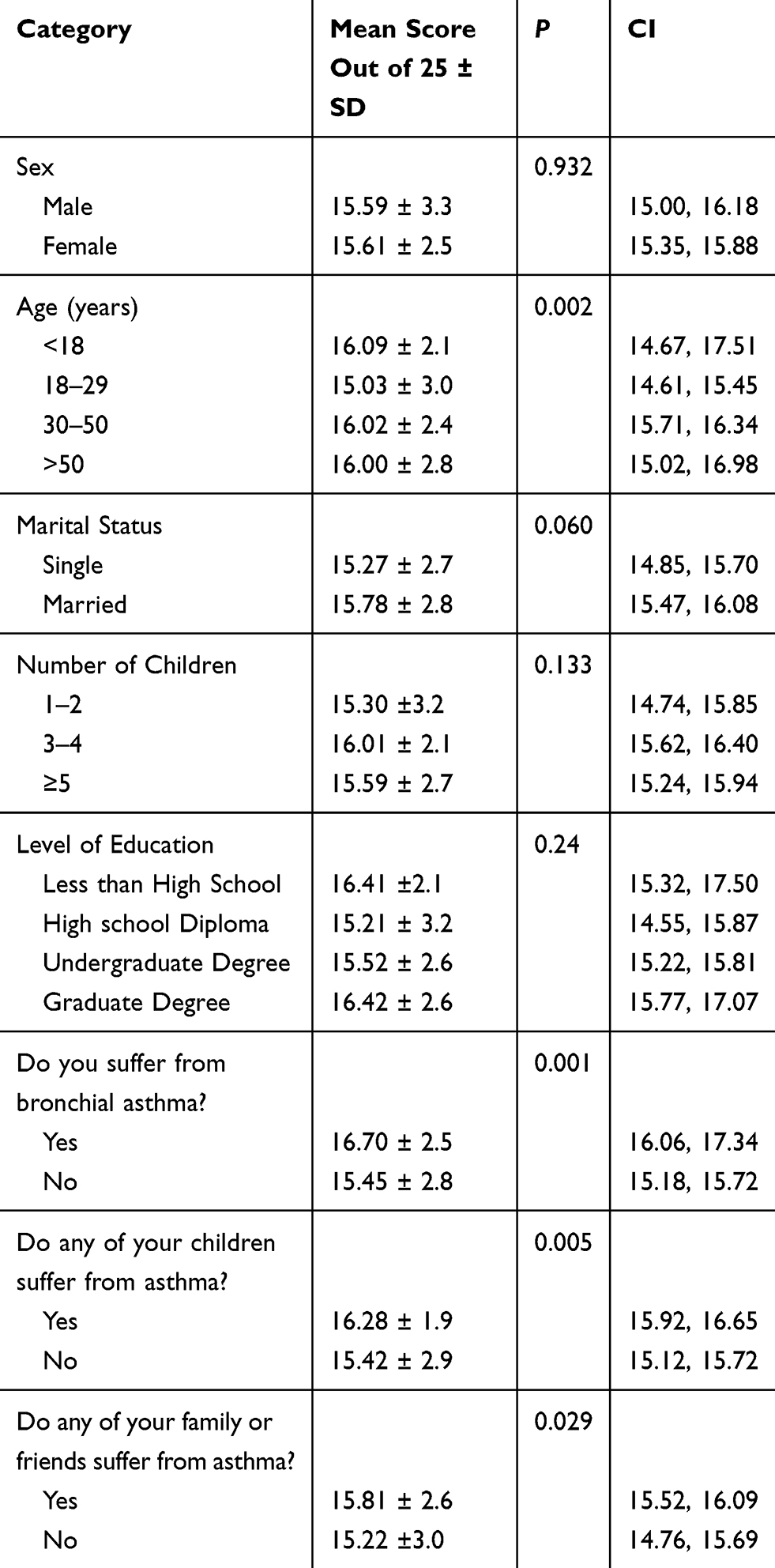 |
Table 3 Mean Score and Significance for Asthma Knowledge |
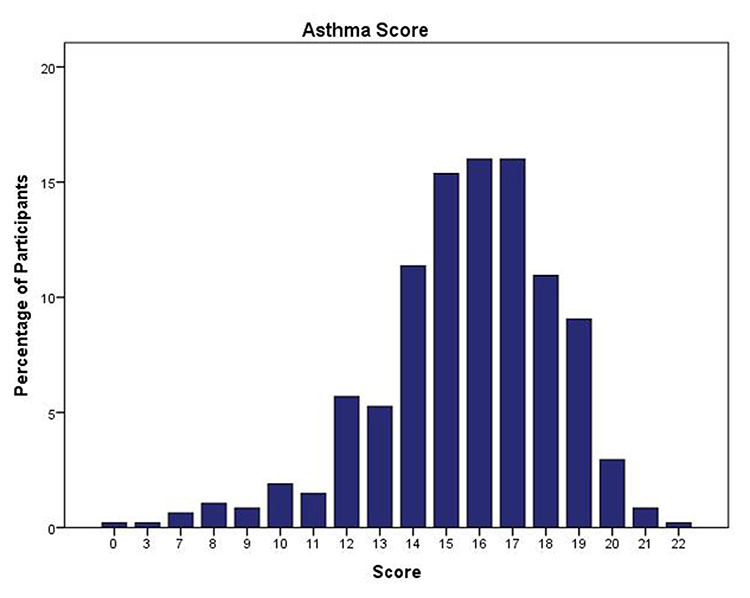 |
Figure 1 Percentage of asthma scores among study participants. |
The data show that there is a positive correlation between age group as well as asthma knowledge, r= 0.137 (P 0.003). There was a significant difference in the asthma scores from 2014 (M= 63%, SD=26) and 2019 (M= 70%, SD= 26) conditions; t (24) = −2.106, p=0.046.
Lastly, of the 475 people who took the survey, only 55% have read or searched about asthma with the most popular method being through the Internet (47%) followed by only 22% from the doctor. Other additional methods used to access information on asthma included friends and family (6%) and educational campaigns and lectures (3%) (Table 4).
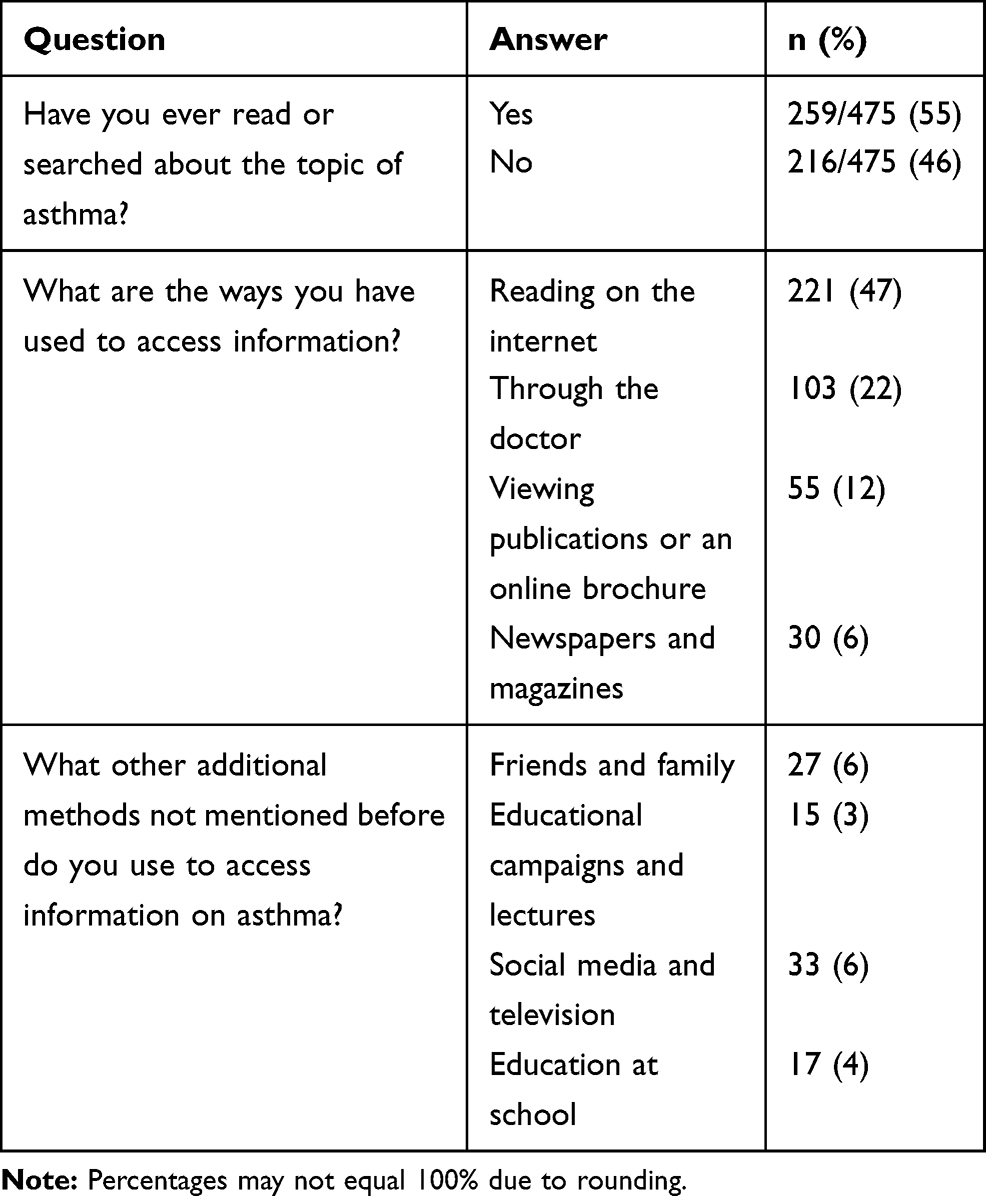 |
Table 4 Self Education Questions |
Discussion
Asthma symptoms, treatment, prevention and educational domains were explored in this study. Compared to the questionnaire conducted by Al-Harbi et al during the 2014 asthma awareness campaign in Saudi Arabia,11 the 2019 survey revealed that the majority of people in Saudi Arabia are aware of asthma as a chronic disease entity, its fatality and that genetic, hereditary and environmental factors play a role in the progression of asthma.
Regarding differentiating the term “chest allergies” from asthma, there has been an improvement from 2014 from a false belief that it is a different entity than asthma (70%) to a current 76% that there is not a difference between the two terms. Although many of the participants are aware of the classic symptoms of asthma such as shortness of breath and nocturnal cough, many still hold misconceptions regarding severe asthma symptoms among children (38%) and confuse symptoms of upper respiratory tract infections with asthma (44%). Asthmatic children tend to have overlapping symptoms of acute viral infections which lead to acute asthma exacerbations, the misdiagnosis or overtreatment of such cases with antibiotics may lead to drug-resistant organisms.13 Therefore, parents should be well educated regarding the symptoms of asthma in their children and when to seek medical help.
Of importance, while there seems to be an improvement in knowledge regarding asthma triggers such as tobacco smoke, perfumes and paint fumes in 2019, awareness of sudden environmental changes and their effects on asthma progression as well as the reduction in asthma development by consuming fish during early life decreased (56% to 35% and 26% to 11%, respectively). Interestingly, a US study found that due to lack of parental education regarding environmental asthma triggers, many resources were needlessly spent on unwarranted preventive measures.14 Since environmental triggers and risk factors are among the most significant elements in self-education to improve disease management in asthmatics,15,16 the findings of this study justify the need for further content-specific revision in future awareness campaigns.
Of specific interest is the topic of asthma medication. While the 2019 study revealed that there is a general improvement from 34% to 51% on the fallacy that inhaled ß-agonists cause tolerance, it also documented an alarmingly low percentage (30%) of the participants are still confused about the use of corticosteroids for acute asthma attacks and the inaccurate belief of the health risks associated with prophylactic asthma treatment. These results about corticosteroids and prophylactic medications are similar to other studies conducted in Saudi Arabia, where it was found that parents have poor understanding of asthma treatments.17–19 Similarly, a Turkish study found that a majority of parents have inaccurate beliefs and unfounded fears regarding inhaled corticosteroids for the use in treatment of childhood asthma.20 These beliefs can be detrimental and lead to poor outcomes in asthmatic children. Poor parental asthma awareness regarding improper asthma medication use was also reported in India.21 An Australian study found that asthma knowledge in parents of children admitted for the first time with asthma was not statistically significant than those readmitted with asthma.22 This suggests poor parental education regarding disease control is a prevalent issue not only in Saudi Arabia, but in other countries as well.
Therefore, future awareness campaign should devote additional resources to educate about proper medication usage to prevent and control asthma attacks among caregivers of asthmatics. For instance, the employment of telemedical education, community-engaged need assessment and corresponding health education programs with a special focus on proper usage of medications might present effective strategies to improve knowledge of this particular area of asthma.23–25
Awareness regarding healthcare follow-up, having a written asthma action plan and patient education about disease triggers were increased from 2014. There was a 7% increase in recognition that asthma could lead to increase school absenteeism in children. Progress has been made from the previous asthma awareness campaign in understanding the importance of specialized asthma centers for asthma treatment and education, the need for scientific material in school curricula about asthma and educational asthma awareness programs. Globally, asthma awareness programs at schools have shown great improvement in disease knowledge, medication administration techniques, decreased need for emergency care and asthma exacerbations.26,27
Similar to the 2014 asthma awareness campaign, only 55% of participants have read or searched about asthma and like the previous study, reading about the disease online or gaining information through the doctor were the most popular methods to gain information about asthma. These findings are consistent with a recent report in the United States, which revealed that virtual education is generally preferred by study participants.28 Web-based health education has been shown to be associated with high patient satisfaction, is cost-effective and widely accessible for many patients.29 Therefore, upcoming awareness campaigns should take into consideration this method of health information acquisition in order to enhance the effectiveness of the project.
Consistent with the 2014 study, asthma knowledge is positively associated with the asthma status of the participant, their children or family members and friends. These novel associations may be attributed to increased self-education as well as an interest in the biology and management of asthma among close contacts of asthmatics. A Brazilian study also showed similar findings in that asthma knowledge among those with asthmatic children, albeit insufficient knowledge, was more than those that did not have asthmatic children.30
The average asthma score increased 7% from 2014 from 63% to 70% in 2019 which is statistically significant. Notably, the associations between marital status and level of education and asthma awareness in the 2014 study are no longer observed in the current analysis. These phenomena not only suggest that socioeconomic factors might no longer be critical determinants of asthma knowledge attainment in Saudi Arabia but also potentially demonstrate the usefulness of the asthma awareness campaigns, which have allowed educational content to be accessible to different socioeconomic backgrounds who may not all readily have access to health care or the Internet.
Asthma prevalence is known to increase in the urban setting,31 this may explain the higher prevalence of asthma among study participants (16%) which was greater than the Saudi national average of 6%.9 The study was limited by the sample population to those with access to shopping centers and not being able to reach those in rural communities therefore not truly reflecting the true childhood asthma awareness of the Saudi community.
Conclusion
The approach to successful management of bronchial asthma is multidisciplinary and cannot be accomplished without a well-informed community. Although knowledge of bronchial asthma in Saudi Arabia has improved as measured by the awareness campaign surveys over the past five years, there is still latitude for improvement. Proper educational outlets should be selected based on public preference with easily accessible electronic content. More importantly, much needs to be done to better educate the society on differentiating asthma from other respiratory infections, the identification of environmental triggers and selected risk factors, and last but not least, the proper usage of asthma medications.
Abbreviations
BA, beta-agonist; SD, standard deviation; CI, confidence interval.
Acknowledgments
The authors would like to thank all volunteers who helped in distributing the questionnaire among the study participants. Saleh Alharbi, MD and Sumayyah Ahmed Nezar Kobeisy, MBBS contributed equally as co-first authors.
Funding
No funding was secured for this study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lötvall J, Akdis CA, Bacharier LB, et al. Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. J Allergy Clin Immunol. 2011;127(2):355–360. doi:10.1016/j.jaci.2010.11.037
2. Beasley R, Semprini A, Mitchell EA. Risk factors for asthma: is prevention possible? Lancet. 2015;386:1075–1085. doi:10.1016/S0140-6736(15)00156-7
3. Serebrisky D, Wiznia A. Pediatric asthma: a global epidemic. Ann Glob Health. 2019;85.
4. Tartasky D. Asthma in the inner city: a growing public health problem. Holist Nurs Pract. 1999;14:37–46. doi:10.1097/00004650-199910000-00007
5. Wood PR, Hill VL. Practical management of asthma. Pediatr Rev. 2009;30:375–385. doi:10.1542/pir.30-10-375
6. Masoli M, Fabian D, Holt S, Beasley R; Global Initiative for Asthma (GINA) Program. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy. 2004;59:469–478. doi:10.1111/j.1398-9995.2004.00526.x
7. Matsui EC, Abramson SL, Sandel MT; Section on Allergy and Immunology; Council on Environmental Health. Indoor environmental control practices and asthma management. Pediatrics. 2016;138:e20162589. doi:10.1542/peds.2016-2589
8. Ramratnam SK, Bacharier LB, Guilbert TW. Severe asthma in children. J Allergy Clin Immunol Pract. 2017;5:889–898. doi:10.1016/j.jaip.2017.04.031
9. Al-Moamary MS, Alhaider SA, Idrees MM, et al. The Saudi initiative for asthma - 2016 update: guidelines for the diagnosis and management of asthma in adults and children. Ann Thorac Med. 2016;11:3–42. doi:10.4103/1817-1737.173196
10. Alahmadi TS, Banjari MA, Alharbi AS. The prevalence of childhood asthma in Saudi Arabia. Int J Pediatr Adolesc Med. 2019;6:74–77. doi:10.1016/j.ijpam.2019.02.004
11. Al-Harbi S, Al-Harbi AS, Al-Khorayyef A, et al. Awareness regarding childhood asthma in Saudi Arabia. Ann Thorac Med. 2016;11:60–65.
12. Martínez CR, Sossa M. Validation of an asthma knowledge questionnaire for use with parents or guardians of children with asthma. Arch Bronconeumol. 2005;41(8):419–424. doi:10.1016/s1579-2129(06)60256-5
13. Bashir H, Grindle K, Vrtis R, et al. Association of rhinovirus species with common cold and asthma symptoms and bacterial pathogens. J Allergy Clin Immunol. 2018;141(2):822–824.e9. doi:10.1016/j.jaci.2017.09.027
14. Cabana MD, Slish KK, Lewis TC, et al. Parental management of asthma triggers within a child’s environment. J Allergy Clin Immunol. 2004;114(2):352–357. doi:10.1016/j.jaci.2004.04.047
15. Farzandipour M, Nabovati E, Heidarzadeh Arani M, Akbari H, Sharif R, Anvari S. Enhancing asthma patients’ self-management through smartphone-based application: design, usability evaluation, and educational intervention. Appl Clin Inform. 2019;10:870–878. doi:10.1055/s-0039-1700866
16. Murray B, O’Neill M. Supporting self-management of asthma through patient education. Br J Nurs. 2018;27:396–401. doi:10.12968/bjon.2018.27.7.396
17. AlOtaibi E, AlAteeq M. Knowledge and practice of parents and guardians about childhood asthma at King Abdulaziz Medical City for National Guard, Riyadh, Saudi Arabia. Risk Manag Healthc Policy. 2018;11:67–75. doi:10.2147/RMHP.S143829
18. BinSaeed AA. Caregiver knowledge and its relationship to asthma control among children in Saudi Arabia. J Asthma. 2014;51:870–875. doi:10.3109/02770903.2014.906608
19. Al-Zalabani AH, Almotairy MM. Asthma control and its association with knowledge of caregivers among children with asthma. A cross-sectional study. Saudi Med J. 2020;41:733–739. doi:10.15537/smj.2020.7.25167
20. Özçeker D, Uçkun U, Islamova D, Tamay Z, Güler N. Corticosteroid phobia among parents of asthmatic children. Turk J Pediatr. 2018;60(2):142. doi:10.24953/turkjped.2018.02.004
21. Shivbalan S, Balasubramanian S, Anandnathan K. What do parents of asthmatic children know about asthma?: an Indian perspective. Indian J Chest Dis Allied Sci. 2005;47(2):81–87.
22. Henry RL, Cooper DM, Halliday JA. Parental asthma knowledge: its association with readmission of children to hospital. J Paediatr Child Health. 1995;31(2):95–98. doi:10.1111/j.1440-1754.1995.tb00754.x
23. Culmer N, Smith T, Stager C, et al. Telemedical asthma education and health care outcomes for school-age children: a systematic review. Allergy Clin Immunol Pract. 2020;8:1908–1918. doi:10.1016/j.jaip.2020.02.005
24. Nguyen TS, Nguyen TLH, Pham TTV, et al. Effectiveness of a short training program for community pharmacists to improve knowledge and practice of asthma counselling - A simulated patient study. Respir Med. 2018;144:50–60. doi:10.1016/j.rmed.2018.10.003
25. Everhart RS, Haley AD, Regan GG, et al.; Engaging Richmond Team. Engaging with the Richmond community to reduce pediatric asthma disparities: findings from a community-engaged needs assessment. Am J Community Psychol. 2020. doi:10.1002/ajcp.12439
26. Liptzin DR, Gleason MC, Cicutto LC, et al. Developing, implementing, and evaluating a school-centered asthma program: step-up asthma program. J Allergy Clin Immunol Pract. 2016;4:972–979. doi:10.1016/j.jaip.2016.04.016
27. Saleh ASEM. School asthma intervention programme effectively improved children’s knowledge and attitudes, and led to decreased hospital admission, length of stay and school absences. Evid Based Nurs. 2020;23:92. doi:10.1136/ebnurs-2019-103092
28. Singh S, Surani S, McGuinness S, Eudicone J, Gilbert I, Subramanian S. Current practice patterns, challenges, and educational needs of asthma care providers in the United States. J Asthma. 2020;19:1–10. doi:10.1080/02770903.2020.1761980
29. Poowuttikul P, Seth D. New concepts and technological resources in patient education and asthma self-management. Clin Rev Allergy Immunol. 2020;59:19–37. doi:10.1007/s12016-020-08782-w
30. Roncada C, Cardoso TD, Bugança BM, Bischoff LC, Soldera K, Pitrez PM. Levels of knowledge about asthma of parents of asthmatic children. Einstein (São Paulo). 2018;16(2). doi:10.1590/s1679-45082018ao4204
31. Byrd RS, Joad JP. Urban asthma. Curr Opin Pulm Med. 2006;12(1):68–74. doi:10.1097/01.mcp.0000199001.68908.45
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.