")
Back to Journals » Journal of Pain Research » Volume 15
Childbirth Pain, Labor Epidural Analgesia, and Postpartum Depression: Recent Evidence and Future Directions
Authors Du W, Bo L , Xu Z, Liu Z
Received 22 June 2022
Accepted for publication 17 September 2022
Published 24 September 2022 Volume 2022:15 Pages 3007—3015
DOI https://doi.org/10.2147/JPR.S379580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Weijia Du1 *, Lulong Bo2 *, Zhendong Xu,1 Zhiqiang Liu1
1Department of Anesthesiology, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Faculty of Anesthesiology, Changhai Hospital, Naval Medical University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhiqiang Liu; Zhendong Xu, Department of Anesthesiology, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China, Tel +86 13816877756 ; +86 13817029904, Email [email protected]; [email protected]
Abstract: Pregnancy and childbirth are major life events for women and their families, characterized by physical, psychological, and emotional changes that can trigger anxiety, depression, and mental disorders in susceptible individuals. Acute labor pain is an independent risk factor for persistent pain in the postpartum period and is associated with depressive disorders. Epidural analgesia is a well-established technique that has commonly been regarded as the gold standard in pain management during labor. Although the relationships between labor pain, labor epidural analgesia, and postpartum depression have been studied by many investigators, the results of these studies are conflicting. Some literature suggest that labor epidural analgesia is associated with a reduction in the incidence of postpartum depression; however, other studies have failed to demonstrate this association. Unmet analgesic needs expectations, unmet birth expectations, and/or the quality of social support during labor may contribute to postpartum depression. The limitations of the published studies included differential misclassification of study variables and residual confounding, variations in the diagnosis of depression, and incomplete history data. Thus, future studies should include information on sociodemographic and patient-level variables and assessments of pain during labor or in the postpartum period. Better management of labor pain should be provided to prevent long-term morbidity and improve maternal and neonatal outcomes. Anesthesiologists could collaboratively work with obstetricians and perinatal psychiatrists to ensure that hospitals prioritize screening and treatment for postpartum depression.
Keywords: epidural labor analgesia, labor pain, neuraxial analgesia, postpartum depressive disorder, pain management in labor
Introduction
Postpartum depression (PPD), defined as an episode of major depression after childbirth, affects 12–17% of women worldwide.1,2 Over the past two decades, the prevalence of PPD among Chinese women has been estimated to range from 4.3% to 29.4%,3–5 and 3.74 million women in China are estimated to be affected by PPD every year.6 PPD is associated with increased odds of severe maternal and neonatal complications, such as suicide, infanticide, and childhood and adolescent developmental and behavioral problems.7,8
Causes of PPD are multifactorial, ranging from physiological changes related to pregnancy and childbirth,9 to psychosocial and environmental factors, including a prior history of mental disorders, low levels of social support, stressful life events and traumatic birth, neonatal intensive care administration, and breastfeeding problems.10 The spread of the coronavirus disease 2019 (COVID-19) pandemic across borders has also resulted in extensive fear among pregnant women. Data from the literature indicates that the pandemic has had a significant impact on maternal depression during pregnancy and in the postpartum period.11,12
Given that approximately 140 million babies are born every year worldwide,13 PPD is a major public health challenge because of its importance for both maternal and child health. Anesthesiologists are concerned about short- and long-term adverse birth stressors and events in both mothers and babies. Thus, the current narrative review aimed to objectively summarize and synthesize the current findings on this topic, including recent developments and advances in the understanding of childbirth pain and PPD, controversies related to the relationship between labor epidural analgesia (LEA) and PPD, limitations of current studies, and further perspectives.
Childbirth Pain and Postpartum Depression
In the non-obstetric population, the association between chronic pain and depression has been well established.14 For most women, childbirth is one of the most painful and stressful events during their lives and can result in long-term maternal morbidity. The association between the intensity of childbirth pain and mood disorders, including post-traumatic stress and PPD, in the immediate postpartum period has been proposed, but this association has not been well studied.15–17 More recently, Lim et al18 found that for susceptible women, pain at all perinatal time points–prenatal, labor, and postpartum–appears to be independently linked to depression scores at 6 weeks postpartum.
These findings support the concept that labor and acute postpartum pain may influence both acute and long-term PPD symptoms. The underlying mechanisms associated with these relationships may be stress response from the pain or the maternal feeling of failure from not overcoming labor pain.15 A genetic association between labor pain and PPD has also been suggested. Since genetic variants are a common factor between perinatal pain and depression, McClain et al19 identified genetic loci (C/C genotypes for rs4633) that contribute to PPD and pain in a large cohort of perinatal women. These mapped to genetic regions that may elucidate the mechanisms underlying the relationship between PPD and labor pain.
Many studies have revealed that the pain phenotype may be a key factor in PPD and recovery. Liska et al20 indicated that women who underwent cesarean delivery (CD) had more early symptoms of PPD than those who had a vaginal birth with limit to no medical intervention. Other studies have also suggested that CD, especially emergency CD, is a risk factor for perinatal mood disorders.21–23 The mechanisms proposed to explain the relationship between CD and PPD include CD as a risk factor for hemorrhage, which increases the probability of PPD, as well as the increased risk of infant mortality, breastfeeding failure, and certain biological changes in the parturient’s body after CD.24 However, a multicenter, prospective, longitudinal, cohort study, including 1288 women hospitalized for cesarean or vaginal delivery, found that the severity of acute postpartum pain and the individual’s pain response to the injury, but not the mode of delivery, were large and independent risk factors for persistent pain and depression.25 Although the sample size of that study was large, some variables associated with persistent pain in the postoperative period, such as prior depression and anxiety, were not assessed. Therefore, the evaluation of factors associated with postpartum pain and depressive symptoms may improve the management of women undergoing either type of delivery.
Postpartum pain and PPD can also affect postpartum opioid requirements. A retrospective cohort study showed that in comparison with women without PPD, those with PPD following CD reported higher daily and average numeric rating pain scores postpartum (2.4 vs 1.7 average; P < 0.001) and used more morphine milligram equivalents each day during their postpartum hospitalization (121 mg [60.5–214.5] vs 75 mg [28.5–133.5], P < 0.001).26 However, effective pain control may protect against PPD in women who have undergone CD. Previous studies have demonstrated the effects of analgesic agents on pain control and the incidence of PPD. Yu et al27 reported that dexmedetomidine administered via patient-controlled intravenous analgesia (PCIA) after CD could be useful for alleviating PPD on postoperative days 7 and 42. Similar results were reported by We et al28 who showed that tramadol PCIA can help in reducing the risk of PPD 4 weeks postoperatively. These findings are promising because medical advancements can improve the delivery experience, and it is possible to minimize postpartum pain with effective pain management, which may present a significant opportunity for the prevention of PPD.
On the basis of these associations, it is reasonable to infer that the mitigation of labor pain through epidural analgesia may decrease the incidence of PPD. Good pain relief during delivery can give the mother better opportunities to cope after delivery and may thus help the mother to better interact with her infant.17 Since LEA is the most effective, and the gold standard, for labor analgesia and is increasingly available,29 an investigation on this topic is of interest and value. In some previous studies,30,31 provision of LEA was hypothesized to reduce the risk of PPD. However, some study results have contradicted these findings.32,33 Thus, despite numerous studies, the association between LEA exposure and PPD risk has not been well established.34
In this review, 16 studies including 3 meta-analyses were selected after thorough evaluation (Tables 1 and 2), which assessed the association between LEA and PPD.
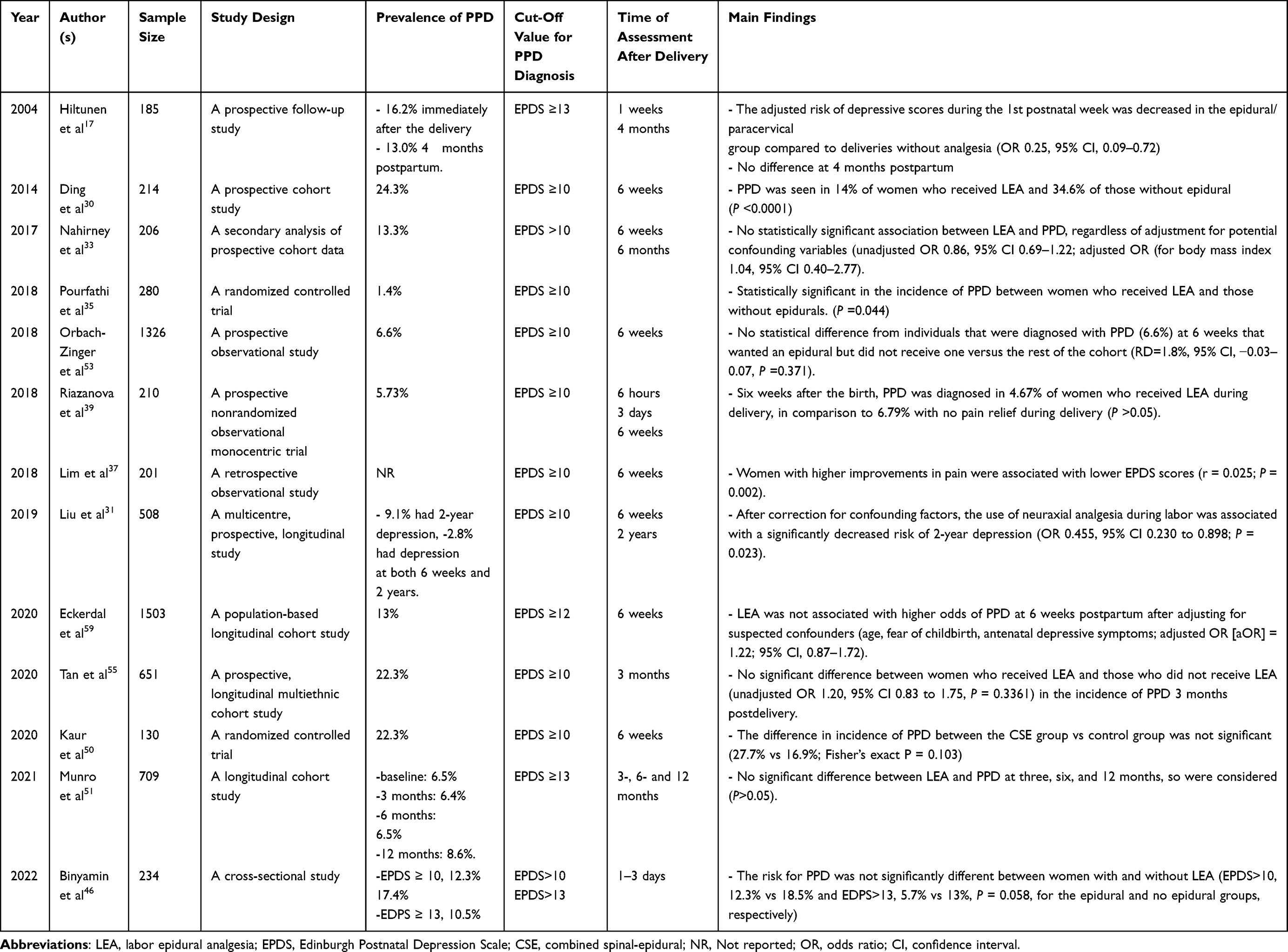 |
Table 1 Studies Selected for Review |
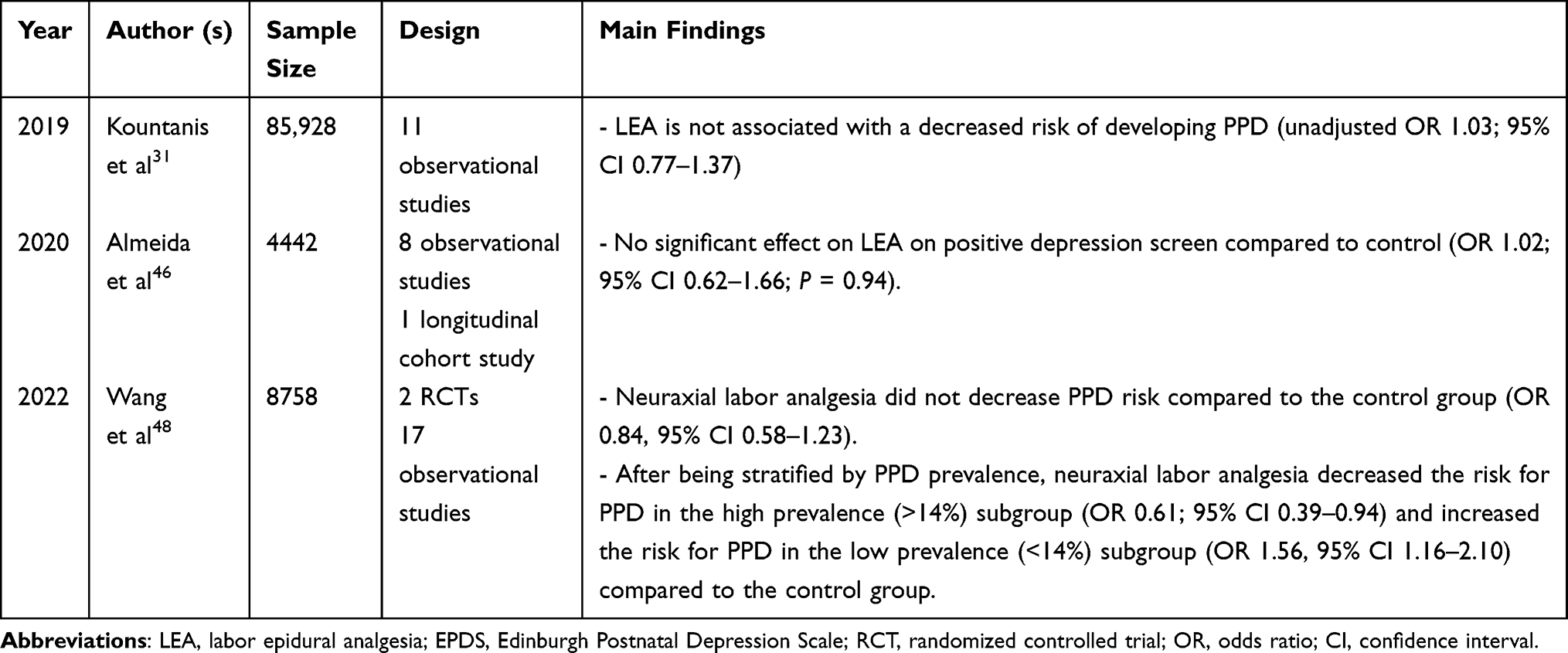 |
Table 2 Meta-Analyses Selected for Review |
Positive Relationship Between LEA and PPD
Evidence from a randomized controlled trial (RCT) showed that the incidence of PPD with LEA was significantly lower than that with natural birth.35 Similar results were demonstrated in observational studies, with Hiltunen et al17 showing that the risk of Edinburgh Postnatal Depression Score (EPDS) postpartum was significantly reduced in women who received epidural/paracervical analgesia compared with women who did not (odds ratio [OR] = 0.25; 95% confidence interval [CI], 0.09–0.72); Ding et al30 reported that LEA was associated with a reduced risk for PPD (OR = 0.31; 95% CI, 0.12–0.82). Labor pain scores might be lower in women who used LEA; however, the contribution of the severity of pain to the risk of PPD was not assessed. Since changes in pain have been shown to be more clinically significant than pain itself,36 the association between PPD and inter-individual variability in labor pain relief under LEA may have more clinical significance. In the study performed by Lim et al,37 the improvement in pain (PIP) scale score was used as a primary predictor. Although they found a relationship between higher improvements in pain and lower EPDS scores (r = 0.025; P = 0.002), the effect of labor analgesia on EPDS scores was relatively small (adjusted OR = 6.6; 95% CI, 1.9–22.4). The authors suggested that labor analgesia might be less influential than other established risk factors for PPD. The relationship between the use of LEA and a reduced risk of PPD may be better explained by other mechanisms, such as psychological, obstetric, or social factors that influence the decision to use epidural analgesia.
Several studies have suggested that the severity of pain during the early period after labor and delivery, typically a time of abrupt withdrawal on pain treatment and relaxed attention to patient care, may affect the development of PPD.25,38 The results from a multicenter, prospective, longitudinal cohort study showed that women with severe acute postpartum pain had a 2.5-fold higher risk of persistent pain and a 3.0-fold higher risk of PPD than those with mild postpartum pain.25 To illustrate the physiological relationship between labor pain management using epidural analgesia and the risk of PPD, Riazanova et al39 evaluated the serum levels of the stress hormone cortisol in the peripartum period. The results showed that the use of LEA reduced pain intensity and cortisol levels in the early postpartum period but only slightly influenced the frequency of PPD six weeks postpartum. The authors explained that this may be due to the direct influence of LEA on the stress reaction of the body during pregnancy. Effective analgesia may reduce the release of catecholamines and increase the likelihood of positive psychological outcomes.40
The sparse data available suggest that LEA may also have long-term effects on maternal mental health. Addressing PPD risk in the late postpartum period might overlook the potential impact of LEA, because depressive symptoms may recover spontaneously.41 In a multicenter, prospective, longitudinal study conducted by Dong et al,31 the use of neuraxial analgesia during labor was associated with a significantly decreased risk of PPD 2 years after childbirth (OR = 0.455; 95% CI, 0.230–0.898; P = 0.023). Chronic pain, defined as any persistent or recurrent pain lasting for more than 3 months,42 was an independent risk factor, while a higher Social Support Rating Scale score was protective against the development of 2-year depression. This was consistent with the findings of a review in which appropriate and welcome social support for women was suggested to be protective against PPD.43 Since chronic pain and depression are definitely associated, further studies should record pain scores at 6 weeks to evaluate the association between PPD and chronic pain.
PPD could have negative consequences for mothers, infants, and mother–infant relationships for up to 3 months.44,45 Mother–infant bonding can be influenced by a woman’s early maternal emotions and connectedness to her offspring. In an exploratory study conducted by Binyamin et al,46 LEA was independently associated with a better mother–infant bonding total score (beta coefficient, 0.252; 95% CI, −0.5 to 0.006; P = 0.045) after controlling for relevant confounders. Thus, monitoring postnatal mental health and maternal infant bonding may be better strategies for further exploring this association.
No Relationship Between LEA and PPD
In contrast, other retrospective and prospective observational studies have indicated no relationship between LEA and PPD. Kountanis et al32 conducted a meta-analysis of 11 observational studies involving 85,928 parturients. Their pooled results suggested that LEA was not associated with a decreased risk of developing PPD (pooled adjusted OR = 1.03; 95% CI, 0.77–1.37). Similar results were reported by Almeida et al47 and Orbach-Zinger et al48 in two other meta-analyses. Although these studies were well powered and applied strict criteria for study inclusion, none of them explored heterogeneity using subgroup analysis.32,47,48 Moreover, sensitivity analyses were not performed32 and publication bias was not assessed.32,48 In a recent meta-analysis, Wang et al49 reported contradictory and opposing effects of LEA on PPD. The pooled results indicated that neuraxial labor analgesia did not decrease PPD risk in comparison with the control group (OR = 0.84; 95% CI, 0.58–1.23); however, after subgroup analyses and meta-regression, neuraxial labor analgesia was shown to have a protective effect when applied to parturients in the region with a high prevalence of PPD (OR = 0.61; 95% CI, 0.39–0.94) but became a risk factor when applied to parturients in the region with a low prevalence of PPD (OR = 1.56; 95% CI: 1.16–2.10). Since all the evidence was not based on randomized controlled trials, the potential effects of unidentified confounders and differential inclusion in the available literature cannot be ruled out, and the interactions among them may have influenced the results. Kaur et al50 conducted an RCT including 130 women and found that the incidence of PPD at 6 weeks was not significantly different between the LEA and control groups (27.7% vs 16.9%; Fisher’s exact P = 0.103). However, perceived stress during pregnancy appeared to be the most important predictor of PPD development (adjusted OR = 11.17; 95% CI, 2.86–43.55; P = 0.001).
The relationship between LEA and PPD is difficult to determine, since depressed women may simply be more likely to request epidural analgesia.33 Four large observational cohort studies with more than 500 participants found that LEA may not have protective effects against PPD.51–54 Munro et al51 found that the only predictor of PPD risk was the presence of antenatal depressive symptoms. Similar results were identified by Tan et al55 who reported that predelivery anxiety and depression, rather than LEA, were positively associated with PPD three months post-delivery. Thus, early screening may detect patients who are at high risk of developing PPD and provide an opportunity for consultation with the anesthesiologist to discuss the labor analgesic plan.
Interestingly, unmatched expectations, such as inadequate pain control from LEA37 or failure to have a planned natural childbirth,53 have also been suggested to contribute to postpartum mood disturbances. Fulfilling women’s birth plans, particularly when they elect to receive no labor analgesia (“natural childbirth”), has been shown to positively influence labor satisfaction.56 Satisfaction with the experience of labor and delivery was lower despite receiving effective epidural analgesia in women who intended to undergo a “natural” childbirth but subsequently received epidural analgesia when labor pain became intolerable. Similarly, a study by Orbach-Zinger et al53 demonstrated a strong negative additive interaction between the intention to deliver without LEA and actually delivering with LEA (risk difference = −8.6%; 95% CI, 16.2%–1.6%; P = 0.014), suggesting that unmatched expectations are significantly associated with negative outcomes. The authors acknowledged that unplanned epidural analgesia may be an indicator of a physiologically difficult delivery, and its relationship with PPD may be mediated by negative emotions related to unmet expectations or a sense of personal failure.
The relationships of PPD with labor pain and LEA are complex and influenced by expectations, culture, and the quality of social support. Notably, the rates of PPD remain at low levels (11–21%)57 in some low-resource countries where labor analgesia utilization is even lower (1–12%),58 in sharp contrast to high-resource countries with higher labor analgesia utilization, indicating that PPD is multifactorial and not necessarily attributable to LEA alone. Most existing studies have overlooked these complex interactions among pain, fear of childbirth, social support, and antenatal depression owing to the limitations of their respective documented data. Eckerdal et al59 used a generalized structural equation model (“path analysis”) to evaluate the results from a population-based longitudinal cohort. After adjusting for potential confounders, their results showed that LEA was not associated with PPD at six weeks postpartum (adjusted OR = 1.22; 95% CI, 0.87–1.72). However, women electing to use LEA were mostly distinguished by fear of childbirth. The personality characteristics of this study may limit the generalizability of the findings.
Limitations of Current Studies
Because of ethical concerns, to the best of our knowledge, only two RCT have explored the relationship between LEA and PPD.35,50 Since observational methods remain the most practical approach for investigating the relationship between PPD, pain, and LEA, the limitations of observational studies, including differential misclassification of study variables and residual confounding, were inevitable. This may explain the conflicting results of the previous studies. First, some studies did not perform a baseline assessment of depression;30,33,53 however, prior depression carries a relative risk of approximately 2.0 for PPD.60 Second, some studies assessed PPD several days, weeks or months after delivery; by definition, PPD may occur within a year.61 Recent studies have revealed that postpartum depressive symptoms can last up to 2 years after childbirth.62 Women that were not diagnosed at 2 months postpartum may have converted to a positive EPDS score later. Thus, studies should include long-term follow-up to evaluate the effect of an intervention on the development of PPD more accurately. Third, although statistical significance for the relationship between LEA and PPD may be reached, the strength of the associations is weak, with odds ratios below 4.30,39 Weak correlations are common in observational studies and are likely to imply bias, rather than causation.63
Another limitation is the variation in the diagnosis of depression, which can hinder the generalizability of the study results, since some studies may over- or underestimate the effect of labor analgesia on PPD. Screening for PPD was based on the EPDS in most studies. Initial research reported a value ≥10 as indicative of PPD positivity.64 Some authors have used different criteria to diagnose PPD, with a less stringent cutoff (EPDS ≥ 9),65 while other observational studies examining LEA have used EPDS scores ≥ 12 to predict PPD risk.41,52,59 Since the EPDS has an estimated 80% sensitivity for the diagnosis of depression,66 it is not intended as a substitute for a mental health professional’s diagnosis of depression.
Furthermore, because most of the data from the existing studies were based on medical records, they were limited by incomplete collection of patient history during clinical visits. For example, although the history of anxiety or depression was controlled for, the severity of depressive symptoms that may have manifested in the prenatal period could not be counted, thus leading to potentially confounding diagnoses.37 This aspect is of great clinical importance given the recent paradigm shifts in the understanding of PPD. In the American Psychiatric Association’s fifth edition of the Diagnostic Statistical Manual (DSM-5), depression during the postpartum period is classified as “Major Depressive Disorder, with postpartum onset.” The addition of the “with peripartum onset” specifier reflects that almost half of “postpartum” major depressive episodes begin prior to delivery.67 Thus, incomplete historical data may lead to missing potentially confounding diagnoses. Likewise, the uncertainty regarding the completeness of the documented historical data was also a limitation. This could be most realistic if the women had a history of physical or psychiatric problems that could have influenced the reaction to labor analgesia or the incidence of PPD.
Conclusion and Further Perspectives
Despite these limitations, these studies have important implications for further research. First, we suggest that more accurate information about sociodemographic constructs should be documented, including marital status,68 migrant status,69 breastfeeding status,70 insurance status, and level of education,8 which could affect depression outcomes. Additionally, patient-level variables, such as a family history of depression, adverse life events, and environmental factors need to be included to explore the relationship between labor pain and PPD, which may help to explore the impact of LEA on these high-risk populations, potentially yielding different findings.71 Future studies should no longer focus on comparing the use or nonuse of labor analgesia, but rather should examine pain and complex intermediating factors. Furthermore, future research must include the relationships between each of the postulated factors that contribute to the development of PPD, to develop appropriate and targeted interventions. For example, if future studies verify that unmet analgesic or birth expectations are indeed associated with PPD, better preparation and anticipation of labor pain and postpartum debriefing sessions could be created.
Second, better documentation and evaluation of local data are warranted. Despite the well-established association between depression and pain, surprisingly few studies on PPD have included assessments of pain during labor or in the postpartum period. Since pain and depression commonly exhibit a comorbid relationship, future studies should examine pain and complex intermediating factors, including individual and cultural factors associated with pain experiences, which may either protect against or predispose individuals to the risk of PPD. The findings of these studies may have clinical significance since they will address knowledge gaps around individualized pain management and childbirth experience and may lead to new methods or discoveries for PPD risk assessment and treatment.72
Third, although universal screening is now recommended by numerous professional organizations, screening rates are low, and screening is often not performed using a validated instrument. For example, postpartum EPDS scores were only recorded in 55% of women who underwent a vaginal delivery in the study by Lim et al.37 Finally, since pain relief may have favorable consequences for the postpartum emotional state of the mother, these observations indicate the need to direct more of our focus to better management of labor pain in order to prevent longer-term morbidity and improve outcomes, including the duration of labor, intrapartum support, mode of pain relief, and quality of analgesia.
In summary, the relationship between the use of LEA and PPD is controversial based on the results of existing data. Labor analgesia may be less influential than other established risk factors for PPD, and its relationship with PPD needs to be more clearly defined in further large, high-quality studies. Regardless, childbirth can be a stressful experience for some individuals, and may have a substantial influence on the mother and the child. All women should be educated to make informed choices based on their personal intentions. While high-quality prospective studies are needed to understand the complex interplay between intrapartum pain and PPD, anesthesiologists should collaborate with obstetricians and perinatal psychiatrists to ensure that hospitals prioritize screening and treatment for PPD.
Funding
This manuscript was funded by National Science Foundation of China (NO. 81971418), Pudong Health Committee of Shanghai (NO. PW2021D-01), and the Science and Technology Commission of Shanghai Municipality (NO. 22ZR1449300).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang Z, Liu J, Shuai H, et al. Mapping global prevalence of depression among postpartum women. Transl Psychiatry. 2021;11(1):543.
2. Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: a systematic review and meta-analysis. J Psychiatr Res. 2018;104:235–248.
3. Yan J, Liu Y, Cao L, Zheng Y, Li W, Huang G. Association between duration of folic acid supplementation during pregnancy and risk of postpartum depression. Nutrients. 2017;9:11.
4. Ding G, Niu L, Vinturache A, et al. ”Doing the month” and postpartum depression among Chinese women: a Shanghai prospective cohort study. Women Birth. 2020;33(2):e151–e158.
5. Wu D, Jiang L, Zhao G. Additional evidence on prevalence and predictors of postpartum depression in China: a study of 300,000 puerperal women covered by a community-based routine screening programme. J Affect Disord. 2022;307:264–270.
6. Chi X, Zhang P, Wu H, Wang J. Screening for postpartum depression and associated factors among women in China: a cross-sectional study. Front Psychol. 2016;7:1668.
7. Pearson RM, Evans J, Kounali D, et al. Maternal depression during pregnancy and the postnatal period: risks and possible mechanisms for offspring depression at age 18 years. JAMA Psychiatry. 2013;70(12):1312–1319.
8. Wisner KL, Sit DK, McShea MC, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. 2013;70(5):490–498.
9. Workman JL, Barha CK, Galea LA. Endocrine substrates of cognitive and affective changes during pregnancy and postpartum. Behav Neurosci. 2012;126(1):54–72.
10. Robertson E, Grace S, Wallington T, Stewart DE. Antenatal risk factors for postpartum depression: a synthesis of recent literature. Gen Hosp Psychiatry. 2004;26(4):289–295.
11. Berard A, Gorgui J, Tchuente V, et al. The COVID-19 pandemic impacted maternal mental health differently depending on pregnancy status and trimester of gestation. Int J Environ Res Public Health. 2022;19(5):2926.
12. Najam R, Chawla N, Lalwani A, Varshney RK, Singh Parmar S. COVID-19 and anxiety in perinatal women. J Caring Sci. 2022;11(1):40–45.
13. Number of births. Available from: https://www.theworldcounts.com/populations/world/births.
14. Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433–2445.
15. Boudou M, Teissedre F, Walburg V, Chabrol H. Relation entre l’intensité de la douleur de l’accouchement et celle du postpartum blues. [Association between the intensity of childbirth pain and the intensity of postpartum blues]. Encephale. 2007;33(5):805–810. French.
16. Soet JE, Brack GA, DiIorio C. Prevalence and predictors of women’s experience of psychological trauma during childbirth. Birth. 2003;30(1):36–46.
17. Hiltunen P, Raudaskoski T, Ebeling H, Moilanen I. Does pain relief during delivery decrease the risk of postnatal depression? Acta Obstet Gynecol Scand. 2004;83(3):257–261.
18. Lim G, LaSorda KR, Farrell LM, McCarthy AM, Facco F, Wasan AD. Obstetric pain correlates with postpartum depression symptoms: a pilot prospective observational study. BMC Pregnancy Childbirth. 2020;20(1):240.
19. McClain L, Farrell L, LaSorda K, Pan LA, Peters D, Lim G. Genetic associations of perinatal pain and depression. Mol Pain. 2019;15:1744806919882139.
20. Ilska M, Banas E, Gregor K, Brandt-Salmeri A, Ilski A, Cnota W. Vaginal delivery or caesarean section - Severity of early symptoms of postpartum depression and assessment of pain in Polish women in the early puerperium. Midwifery. 2020;87:102731.
21. Sun L, Wang S, Li XQ. Association between mode of delivery and postpartum depression: a systematic review and network meta-analysis. Aust N Z J Psychiatry. 2021;55(6):588–601.
22. Zhao XH, Zhang ZH. Risk factors for postpartum depression: an evidence-based systematic review of systematic reviews and meta-analyses. Asian J Psychiatr. 2020;53:102353.
23. Xu H, Ding Y, Ma Y, Xin X, Zhang D. Cesarean section and risk of postpartum depression: a meta-analysis. J Psychosom Res. 2017;97:118–126.
24. Moameri H, Ostadghaderi M, Khatooni E, Doosti-Irani A. Association of postpartum depression and cesarean section: a systematic review and meta-analysis. Clin Epidemiol Global Health. 2019;7(3):471–480.
25. Eisenach JC, Pan PH, Smiley R, Lavandhomme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94.
26. Walker Z, Perkins C, Harper L, Jauk V, Szychowski JM, Mazzoni S. The effects of antepartum depressive symptoms on postcesarean opioid consumption. Am J Perinatol. 2022;39(1):106–112.
27. Yu HY, Wang SY, Quan CX, et al. Dexmedetomidine alleviates postpartum depressive symptoms following cesarean section in Chinese women: a randomized placebo-controlled study. Pharmacotherapy. 2019;39(10):994–1004.
28. Wu Z, Zhao P, Peng J, et al. A patient-controlled intravenous analgesia with tramadol ameliorates postpartum depression in high-risk woman after cesarean section: a randomized controlled trial. Front Med. 2021;8:679159.
29. Traynor AJ, Aragon M, Ghosh D, et al. Obstetric anesthesia workforce survey: a 30-year update. Anesth Analg. 2016;122(6):1939–1946.
30. Ding T, Wang DX, Qu Y, Chen Q, Zhu SN. Epidural labor analgesia is associated with a decreased risk of postpartum depression: a prospective cohort study. Anesth Analg. 2014;119(2):383–392.
31. Liu ZH, He ST, Deng CM, et al. Neuraxial labour analgesia is associated with a reduced risk of maternal depression at 2 years after childbirth: a multicentre, prospective, longitudinal study. Eur J Anaesthesiol. 2019;36(10):745–754.
32. Kountanis JA, Vahabzadeh C, Bauer S, et al. Labor epidural analgesia and the risk of postpartum depression: a meta-analysis of observational studies. J Clin Anesth. 2020;61:109658.
33. Nahirney M, Metcalfe A, Chaput KH. Administration of epidural labor analgesia is not associated with a decreased risk of postpartum depression in an urban Canadian population of mothers: a secondary analysis of prospective cohort data. Local Reg Anesth. 2017;10:99–104.
34. Munro A, MacCormick H, Sabharwal A, George RB. Pharmacologic labour analgesia and its relationship to postpartum psychiatric disorders: a scoping review. Can J Anaesth. 2020;67(5):588–604.
35. Pourfathi H, Farzin H. Effect of painless labor on postpartum depression. J Obstet Gynecol Cancer Res. 2018;3(3):93–97.
36. Rowbotham MC. What is a ”clinically meaningful” reduction in pain? Pain. 2001;94(2):131–132.
37. Lim G, Farrell LM, Facco FL, Gold MS, Wasan AD. Labor analgesia as a predictor for reduced postpartum depression scores: a retrospective observational study. Anesth Analg. 2018;126(5):1598–1605.
38. Shen D, Hasegawa-Moriyama M, Ishida K, Fuseya S, Tanaka S, Kawamata M. Acute postoperative pain is correlated with the early onset of postpartum depression after cesarean section: a retrospective cohort study. J Anesth. 2020;34(4):607–612.
39. Riazanova OV, Alexandrovich YS, Ioscovich AM. The relationship between labor pain management, cortisol level and risk of postpartum depression development: a prospective nonrandomized observational monocentric trial. Rom J Anaesth Intensive Care. 2018;25(2):123–130.
40. Parise DC, Gilman C, Petrilli MA, Malaspina D. Childbirth pain and post-partum depression: does labor epidural analgesia decrease this risk? J Pain Res. 2021;14:1925–1933.
41. Vliegen N, Casalin S, Luyten P. The course of postpartum depression: a review of longitudinal studies. Harv Rev Psychiatry. 2014;22(1):1–22.
42. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007.
43. Grigoriadis S, Erlick Robinson G, Fung K, et al. Traditional postpartum practices and rituals: clinical implications. Can J Psychiatry. 2009;54(12):834–840.
44. Slomian J, Honvo G, Emonts P, Reginster JY, Bruyere O. Consequences of maternal postpartum depression: a systematic review of maternal and infant outcomes. Womens Health. 2019;15:1745506519844044.
45. Righetti-Veltema M, Conne-Perreard E, Bousquet A, Manzano J. Postpartum depression and mother-infant relationship at 3 months old. J Affect Disord. 2002;70(3):291–306.
46. Binyamin Y, Wainstock T, Sheiner E, et al. The association between epidural analgesia during labor and mother-infant bonding. J Clin Anesth. 2022;80:110795.
47. Almeida M, Kosman KA, Kendall MC, De Oliveira GS. The association between labor epidural analgesia and postpartum depression: a systematic review and meta-analysis. BMC Womens Health. 2020;20(1):99.
48. Orbach-Zinger S, Heesen M, Grigoriadis S, Heesen P, Halpern S. A systematic review of the association between postpartum depression and neuraxial labor analgesia. Int J Obstet Anesth. 2021;45:142–149.
49. Wang J, Zhao G, Song G, Liu J. Association between neuraxial labor analgesia and postpartum depression: a meta-analysis. J Affect Disord. 2022;311:95–102.
50. Kaur A, Mitra S, Singh J, et al. Pain, stress, analgesia and postpartum depression: revisiting the controversy with a randomized controlled trial. Saudi J Anaesth. 2020;14(4):473–479.
51. Munro A, George RB, Mackinnon SP, Rosen NO. The association between labour epidural analgesia and postpartum depressive symptoms: a longitudinal cohort study. Can J Anaesth. 2021;68(4):485–495.
52. Eckerdal P, Georgakis MK, Kollia N, Wikstrom AK, Hogberg U, Skalkidou A. Delineating the association between mode of delivery and postpartum depression symptoms: a longitudinal study. Acta Obstet Gynecol Scand. 2018;97(3):301–311.
53. Orbach-Zinger S, Landau R, Harousch AB, et al. The relationship between women’s intention to request a labor epidural analgesia, actually delivering with labor epidural analgesia, and postpartum depression at 6 weeks: a prospective observational study. Anesth Analg. 2018;126(5):1590–1597.
54. Zhang Y, Johnston L, Ma D, Wang F, Zheng X, Xu X. An exploratory study of the effect of labor pain management on postpartum depression among Chinese women. Ginekol Pol. 2018;89(11):627–636.
55. Tan CW, Sultana R, Kee MZL, Meaney MJ, Sng BL. Investigating the association between labour epidural analgesia and postpartum depression: a prospective cohort study. Eur J Anaesthesiol. 2020;37(9):796–802.
56. Kannan S, Jamison RN, Datta S. Maternal satisfaction and pain control in women electing natural childbirth. Reg Anesth Pain Med. 2001;26(5):468–472.
57. Mohammad KI, Gamble J, Creedy DK. Prevalence and factors associated with the development of antenatal and postnatal depression among Jordanian women. Midwifery. 2011;27(6):e238–e245.
58. Ezeonu PO, Anozie OB, Onu FA, et al. Perceptions and practice of epidural analgesia among women attending antenatal clinic in FETHA. Int J Womens Health. 2017;9:905–911.
59. Eckerdal P, Kollia N, Karlsson L, et al. Epidural analgesia during childbirth and postpartum depressive symptoms: a population-based longitudinal cohort study. Anesth Analg. 2020;130(3):615–624.
60. Weissman MM, Olfson M. Depression in women: implications for health care research. Science. 1995;269(5225):799–801.
61. Bell AF, Andersson E. The birth experience and women’s postnatal depression: a systematic review. Midwifery. 2016;39:112–123.
62. Mora PA, Bennett IM, Elo IT, Mathew L, Coyne JC, Culhane JF. Distinct trajectories of perinatal depressive symptomatology: evidence from growth mixture modeling. Am J Epidemiol. 2009;169(1):24–32.
63. Grimes DA, Schulz KF. False alarms and pseudo-epidemics: the limitations of observational epidemiology. Obstet Gynecol. 2012;120(4):920–927.
64. Matthey S, Henshaw C, Elliott S, Barnett B. Variability in use of cut-off scores and formats on the Edinburgh Postnatal Depression Scale: implications for clinical and research practice. Arch Womens Ment Health. 2006;9(6):309–315.
65. Iwata H, Mori E, Tsuchiya M, et al. Predictors of depressive symptoms in older Japanese primiparas at 1 month post-partum: a risk-stratified analysis. Jpn J Nurs Sci. 2016;13(1):147–155.
66. Adouard F, Glangeaud-Freudenthal NM, Golse B. Validation of the Edinburgh postnatal depression scale (EPDS) in a sample of women with high-risk pregnancies in France. Arch Womens Ment Health. 2005;8(2):89–95.
67. Gynecology. ACoOa. Diagnostic and Statistical Manual of Mental Disorders.
68. Urquia ML, O’Campo PJ, Ray JG. Marital status, duration of cohabitation, and psychosocial well-being among childbearing women: a Canadian nationwide survey. Am J Public Health. 2013;103(2):e8–e15.
69. Gaillard A, Le Strat Y, Mandelbrot L, Keita H, Dubertret C. Predictors of postpartum depression: prospective study of 264 women followed during pregnancy and postpartum. Psychiatry Res. 2014;215(2):341–346.
70. Lara-Cinisomo S, McKenney K, Di Florio A, Meltzer-Brody S. Associations between postpartum depression, breastfeeding, and oxytocin levels in Latina mothers. Breastfeed Med. 2017;12(7):436–442.
71. Meltzer-Brody S, Larsen JT, Petersen L, et al. Adverse life events increase risk for postpartum psychiatric episodes: a population-based epidemiologic study. Depress Anxiety. 2018;35(2):160–167.
72. Lim G. Perinatal depression. Curr Opin Anaesthesiol. 2021;34(3):233–237.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.