")
Back to Journals » International Medical Case Reports Journal » Volume 13
Charles Bonnet Syndrome in a Patient with Parkinson’s Disease and Bilateral Posterior Capsule Opacification
Authors Osa AA, Bowen TJ, Whitson JT
Received 7 June 2019
Accepted for publication 3 December 2019
Published 10 January 2020 Volume 2020:13 Pages 7—10
DOI https://doi.org/10.2147/IMCRJ.S218687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Amenze Angel Osa, 1, 2 Trent J Bowen, 1 Jess T Whitson 1
1Department of Ophthalmology, University of Texas Southwestern Medical Center, Dallas, TX, USA; 2Department of Ophthalmology, The Ohio State University, Columbus, OH, USA
Correspondence: Jess T Whitson
5323 Harry Hines Blvd, Dallas, TX 75390-9057, USA
Tel +1 214-648-4733
Fax +1 214 645-9482
Email [email protected]
Abstract: Charles Bonnet syndrome (CBS) is a condition of visual hallucinations or disturbances occurring in patients with visual pathway pathology not due to underlying psychiatric, metabolic, or neurologic disease. A patient with Parkinson’s disease experiencing visual hallucinations was evaluated by the ophthalmology service and found to have decreased vision due to bilateral reversible posterior capsular opacification. The patient’s hallucinations did not improve on clozapine, a medication requiring careful monitoring due to potentially severe systemic side effects. However, the hallucinations resolved and vision improved after bilateral treatment of the posterior capsular opacification. Clozapine was then discontinued, and the patient was able to resume his previous Parkinson’s disease therapy. This case highlights the importance of considering visual pathway pathology as a contributing factor to visual hallucinations, even in patients with previously diagnosed underlying psychiatric, metabolic, or neurologic disease that could additionally be the etiology of the visual disturbances.
Keywords: visual hallucinations, clozapine, vision
Introduction
Charles Bonnet syndrome (CBS) is a condition of visual hallucinations or disturbances occurring in patients with visual pathway pathology. These are not due to underlying psychiatric, metabolic, or neurologic disease.1 The incidence of CBS increases with age and severity of vision loss.2 The differential diagnosis of CBS includes etiologies of dementia (vascular dementia, Alzheimer’s disease, etc.), psychosis (psychiatric disease, metabolic causes, etc.), Parkinson’s disease, and delirium. CBS is essentially a diagnosis of exclusion; therefore, other etiologies of hallucinations must be excluded.3 Although there is no specific and clearly agreed upon diagnostic criteria for CBS, the general required elements are (1) visual hallucinations, (2) vision loss, and (3) lack of confounding neuropsychiatric disorders causing visual hallucinations.4 There are many reports of CBS occurring in conditions that can cause severe vision loss such as macular degeneration and glaucoma.5 Additionally, there are reports of patients with relatively less severe and reversible vision loss also experiencing CBS and resolution after treatment.6–8 Table 1 highlights the case reports of CBS and the visual pathway pathology.
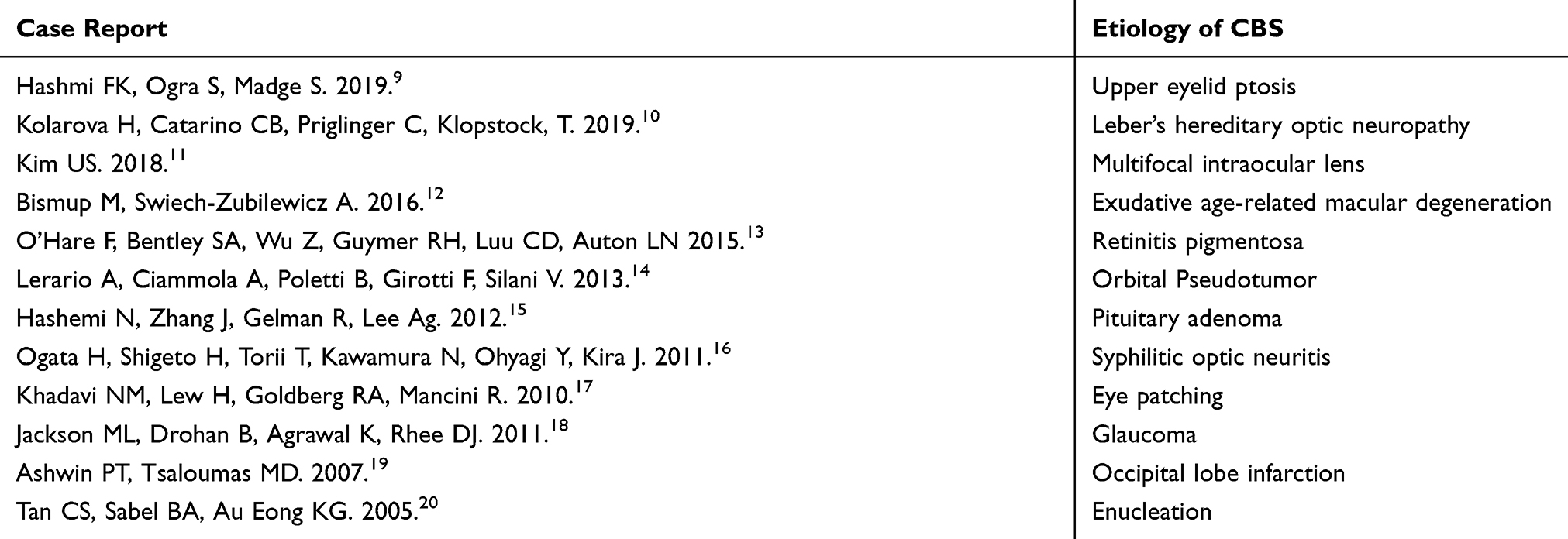 |
Table 1 Highlighted Case Reports of Visual Pathway Pathology Leading to CBS |
Nguyen8 previously reported a CBS case of a patient with visually significant bilateral posterior capsular opacification (PCO) experiencing hallucinations. After undergoing sequential treatment with neodymium-doped yttrium aluminum garnet (Nd:YAG) capsulotomy in both eyes, the patient had an improvement in the perceived hallucinations. In this case report, we present a unique case of a patient with a baseline neurologic disorder also experiencing hallucinations in the setting of visually significant bilateral PCO.
Case Report
A 76-year-old white male with severe Parkinson’s disease leading to severe motor impairment and mild cognitive impairment was referred by to us by the neurology and psychiatry services for decreased vision affecting his ability to conduct his daily activities. He also reported seeing daily images of a little girl playing with blocks, a cat in his window, and men tearing down his neighbor’s roof that he recognized were not real. These visual disturbances were debilitating to the patient and made it difficult to complete work around his home and interact with family members. Prior to our evaluation, physicians from neurology and psychiatry had recently adjusted the patient’s pharmacotherapy in attempts to manage these visual disturbances thought initially to be due to the progression of his Parkinson’s disease. A trial of atypical antipsychotic therapy including gradually increasing quetiapine to 300 mg twice daily over the course of 3 weeks followed by the addition of pimavanserin 34 mg daily for 3 weeks failed to relieve his hallucinations. Most recently, his dose of carbidopa/levodopa was decreased, and clozapine was initiated and gradually increased to 150 mg twice daily for 3 weeks since the visual disturbances continued to be debilitating. Clozapine, in particular, is a high-risk antipsychotic medication with the potentially serious adverse effect of agranulocytosis along with possible metabolic, neurologic, and cardiac toxicities including hyperglycemia, hyperlipidemia, seizures, myocarditis, and pulmonary embolism.21 He continued to experience hallucinations while on clozapine when he presented to the ophthalmology service. His ophthalmic exam revealed a best-corrected visual acuity (BCVA) of 20/200 in each eye (OU). Ocular examination was remarkable for mild corneal guttae OU, posterior chamber intraocular lenses (PCIOL) OU, and visually significant PCO OU. The anterior and posterior segments were otherwise unremarkable. He underwent sequential Nd:YAG capsulotomy OU. At his one-month follow-up, the patient reported complete resolution of his hallucinations with BCVA of 20/25 in his right eye (OD) and 20/30 in his left eye (OS). The patient then resumed his previous carbidopa/levodopa dose and was tapered off clozapine with sustained resolution of the visual disturbances.
Discussion
Charles Bonnet Syndrome can occur in patient with both severe or nonsevere and both irreversible or reversible vision loss.4–7 Parkinson’s disease is a progressive neurologic disorder characterized by tremor, bradykinesia, and gait disturbances. Visual hallucinations are the most common psychotic symptom of Parkinson’s disease.22,23 These psychosis symptoms relating to Parkinson’s disease can be treated with a range of antipsychotics, including pimavanserin and clozapine, but overall, these therapies may not be effective and safe in all cases.24 We present a patient who experienced vision loss from posterior capsular opacification, a treatable cause of vision loss. With resolution of the patient’s visual hallucinations and disturbances after sequential Nd:YAG capsulotomy OU, the bilateral PCO was the apparent etiology of both the decreased visual acuity and visual disturbances, indicating CBS. Bilateral YAG capsulotomies resulted in improved visual acuity and complete resolution of his visual hallucinations. This case report demonstrates the importance of a thorough ocular exam and treating any potential reversible visual pathway pathology to improve visual function to assist in decreasing hallucinations in CBS. This patient’s case, in particular, had a co-existing neurologic condition that can cause hallucinations, but with improvement in visual function by treating the PCO, the patient was able to be relieved of his hallucinations and taken off of anti-psychotic pharmacotherapy, which has the potential for serious adverse systemic events. A clear etiology explaining how PCO could lead to visual hallucinations is not known, but a prevailing theory for CBS is that any visual pathway pathology can lead to visual deafferentation and then cortical hyperexcitability within the occipital cortex.25 It is critical for providers to consider CBS as a diagnosis in patients with visual hallucinations or disturbances, especially those patients with an underlying confounding neurologic disorder. Referrals for ophthalmological evaluation may uncover diagnoses and etiologies of visual pathway pathology that may be treatable and assist in improving visual disturbances due to CBS.
Ethics Statement
Written informed consent was provided by the patient to have the case details published. Institutional approval was not required to publish case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boller F, Birnbaum DS, Caputi N. Charles Bonnet syndrome and other hallucinatory phenomena. Front Neurol Neurosci. 2018;41:117–124.
2. Pang L. Hallucinations experienced by visually impaired: Charles Bonnet syndrome. Optom Vis Sci. 2016;93(12):1466–1478. doi:10.1097/OPX.0000000000000959
3. Vale TC, Fernandes LV, Caramelli P. Chalres Bonnet syndrome: characteristics of its visual hallucinations and differential diagnosis. Arg Neuropsiquiatr. 2014;72(5):333–336. doi:10.1590/0004-282X20140015
4. Hamedani AG, Pelak VS. The Charles Bonnet syndrome: a systematic review of diagnostic criteria. Cur Treat Options Neurol. 2019;21(9):41. doi:10.1007/s11940-019-0582-1
5. Singh A, Sørensen TL. Charles Bonnet syndrome improves when treatment is effective in age-related macular degeneration. Br J Ophthalmol. 2011;95(2):291–292. doi:10.1136/bjo.2010.179465
6. Smith CS, Nichols J, Riaz KM. Remission of Charles Bonnet syndrome after cataract extraction. Can J Ophthal. 2018;53(6):e221–e222. doi:10.1016/j.jcjo.2018.01.036
7. Beaulieu RA, Tamboli DA, Armstrong BK, Hogan RN, Mancini R. Reversible Charles Bonnet syndrome after oculoplastic procedures. J Neuroophthalmol. 2018;38(3):334–336. doi:10.1097/WNO.0000000000000477
8. Nguyen M. A case of resolving Charles Bonnet syndrome following treatment of intraocular posterior capsular opacification. Clini Refractive Optometry. 2018;28(2).
9. Hashmi FK, Ogra S, Madge S. Reversible Charles Bonnet syndrome secondary to upper lid ptosis. Orbit. 2019;1–3. doi:10.1080/01676830.2019.1648522
10. Kolarova H, Catarino CB, Priglinger C, Klopstock T. Charles Bonnet syndrome in Leber’s hereditary optic neuropathy. J Neurol. 2019;266(3):777–779. doi:10.1007/s00415-019-09205-3
11. Kim US. Charles Bonnet syndrome secondary to multifocal intraocular lens implantation. J Cataract Refract Surg. 2018;44:
12. Bismup M, Swiech-Zubilewicz A. Charles Bonnet syndrome secondary to exudative age-related macular degeneration - a case report. Klin Oczna. 2016;117(4):253–255.
13. O’Hare F, Bentley SA, Wu Z, Guymer RH, Luu CD. Charles Bonnet syndrome in advanced retinitis pigmentosa. Ophthalmology. 2015;122(9):1951–1953. doi:10.1016/j.ophtha.2015.03.006
14. Lerario A, Ciammola A, Poletti B, Girotti F, Silani V. Charles Bonnet syndrome: two case reports and review of the literature. J Neurol. 2013;260(4):1180–1186. doi:10.1007/s00415-013-6857-7
15. Hashemi N, Zhang J, Gelman R, Lee A. Visual hallucinations (Charles Bonnet syndrome) as the presenting sign of pituitary adenoma. Can J Ophthalmol. 2012;47(3):e5–e6. doi:10.1016/j.jcjo.2012.03.029
16. Ogata H, Shigeto H, Torii T, Kawamura N, Ohyagi Y, Kira J. A case of Charles Bonnet syndrome following syphilitic optic neuritis. Rinsho Shinkeigaku. 2011;51(8):595–598. doi:10.5692/clinicalneurol.51.595
17. Khadavi NM, Lew H, Goldverg RA, Mancini R. A case of acute reversible Charles Bonnet syndrome following postsurgical unilateral eye patch placement. Ophthalmic Plast Reconstr Surg. 2010;26(4):302–304. doi:10.1097/IOP.0b013e3181c2a188
18. Jackson ML, Drohan B, Agrawal K, Rhee DJ. Charles Bonnet syndrome and glaucoma. Ophthalmology. 2011;118(5):1005. doi:10.1016/j.ophtha.2011.01.007
19. Ashwin PT, Tsaloumas MD. Complex visual hallucinations (Charles Bonnet syndrome) in the hemianopic visual field following occipital infarction. J Neurol Sci. 2007;263(1–2):184–186. doi:10.1016/j.jns.2007.05.027
20. Tan CS, Sabel BA, Au Eong KG. Charles Bonnet syndrome following enucleation. Eye (Lond). 2005;18(7):811–812.
21. Haidary HA, Padhy RK. Clozapine. StatPearls; 2019.
22. Frei K, Truong D. Hallucinations and the spectrum of psychosis in Parkinson’s disease. J Neurol Sci. 2017;374:56–62. doi:10.1016/j.jns.2017.01.014
23. Armstrong RA. Visual dysfunction in Parkinson’s disease. Int Rev Neurobiol. 2017;134:921–946.
24. Fredericks D, Norton JC, Atchison C, Schoenhaus R, Pill MW. Parkinson’s disease and Parkinson’s disease psychosis: a perspective on the challenges, treatments, and economic burden. Am J Manag Care. 2017;23(5 Suppl):S83–S92.
25. Painter DR, Dwyer MF, Kamke MR, Mattingley JB. Stimulus-driven cortical hyperexcitability in individuals with Charles Bonnet hallucinations. Curr Biol. 2018;28(21):3475–3480. doi:10.1016/j.cub.2018.08.058
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.