")
Back to Journals » Journal of Pain Research » Volume 12
Characteristics of pharmacological pain treatment in older nursing home residents
Authors Nowak T, Neumann-Podczaska A , Tobis S , Wieczorowska-Tobis K
Received 31 October 2018
Accepted for publication 18 February 2019
Published 25 March 2019 Volume 2019:12 Pages 1083—1089
DOI https://doi.org/10.2147/JPR.S192587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael Schatman
Tomasz Nowak,1 Agnieszka Neumann-Podczaska,2 Slawomir Tobis,2 Katarzyna Wieczorowska-Tobis1
1Laboratory of Geriatric Medicine, Department of Palliative Medicine, Poznan University of Medical Sciences, Poznan, Poland; 2Department of Geriatric Medicine and Gerontology, Poznan University of Medical Sciences, Poznan, Poland
Background: Pain in older subjects with cognitive impairement is frequently undertreated.
Purpose: The aim of the study was to characterize pain treatment among 199 elderly nursing home residents (NHR), aged 65 years and above.
Patients and methods: In all studied subjects, cognitive functions were assessed. Based on the results, participants were divided into two groups: group 1 – cognitively intact subjects in whom the pain was evaluated based on Numerical Rating Scale (NRS), and group 2 – subjects with cognitive impairment, in whom Abbey Pain Scale (APS) was used to assess pain. Thereafter, subjects with inappropriately treated pain (ie, ineffectively treated or untreated) were analyzed in detail as group 1a (NRS >0) and group 2a (Abbey >2).
Results: The prevalence of pain in group 1 and 2 did not differ (65% and 70% respectively). However, inappropriately treated pain occurred more frequently in group 2 (2a=85% vs 1a=64%; p<0.01). This was related to the more frequent occurrence of untreated pain (52% vs 22%; p<0.001), because the presence of ineffectively treated pain was comparable in both groups (34% vs 42%). Qualitative analysis of pharmacotherapy in subjects with inappropriately treated pain demonstrated that acetaminophen in low dosages was the most frequently consumed drug from the first step of the analgesic ladder (16 individuals), from the second step – a combination of tramadol and acetaminophen (8 individuals), and from the third step – buprenorphine was the only drug applied (6 individuals).
Conclusion: Our study showed a high frequency of untreated or ineffectively treated pain in NHR, regardless of the cognitive status of studied subjects. However, these phenomena were particularly frequent in subjects with cognitive impairment. Thus, proper education of the staff is needed to increase their knowledge about both the pain assessment and its treatment.
Keywords: pain, treatment, cognitive impairment, nursing home residents, analgesics
Introduction
Pain is one of the most frequent problems reported by patients who consult a doctor. However, data regarding the prevalence of pain among older people are not consistent, mainly due to differences in research methodologies. It is estimated that the prevalence of pain in European long-term care facilities varies among the countries between 32% and 57% of residents.1 Moreover, according to these data, moderate to severe pain is present in over 50% of cases across Europe. Older subjects and their caregivers commonly believe that pain is a normal feature of aging, hence they generally do not report it.2 Consequently, actual figures for the prevalence of pain in older patients may be much higher.
Among older individuals, pain is frequently accompanied by cognitive impairment.3 Achterberg et al suggest that there exists a self-accelerating mechanism: underdiagnosed pain intensifies the cognitive impairment, and these, in turn, impede or even preclude effective pain diagnostics and treatment.4 According to a number of studies, older subjects with cognitive impairment receive fewer analgesics in comparison to subjects with normal cognition.1,5,6
Various barriers to appropriate pain management in subjects with dementia have been identified, in particular those relating to staff and patients.7 Among the staff-related barriers, insufficient healthcare providers’ knowledge of pain assessment, resulting in non-use or under-use of assessment tools, should be pointed out.8 Patient-related barriers are predominantly caused by communication problems – for example, subjects unable to communicate verbally are likely to express pain mainly via behavioral problems.7
One of the challenges of the pharmacological treatment of subjects with advanced cognitive impairment results from the accompanying agitation and aggression. Agitation and aggression is present in as much as half of the patients with moderate and severe impairment. As we observed in our previous study, this may be the result of pain, particularly in the case of impaired communication skills and abstract reasoning disability. This relationship is demonstrated by a positive correlation between the intensity of pain and agitation.9 Hence, effective diagnosis and treatment of pain can translate into a reduction of behavioral disturbances which can lead to the discontinuation of antipsychotic medication (or lowered doses), thus avoiding serious, life-threatening adverse effects of these drugs.
Addressing this problem is crucial in the wake of reports regarding undertreated pain among older subjects, especially those with cognitive impairment. Therefore, the quantitative and qualitative characteristics of pharmacological pain treatment in nursing homes’ older residents (NHR) were the aim of the study.
Materials and methods
The project was approved by the Bioethical Committee of the Poznan University of Medical Sciences (Resolution number 598/14).
Participants
Residents of two nursing homes, in the Greater Poland (Wielkopolska) region of Poland, aged 65 years and above, were included in the study. All subjects or their representatives gave their written informed consent after receiving a full explanation of the nature of the study. This study was conducted in accordance with the Declaration of Helsinki.
Age was the only inclusion criterion besides the consent to participate in the study.
Study procedure
The medical files of the residents were screened for diagnoses and drugs. In all included subjects, functional capacity and cognitive functions were assessed by nurses who knew the patients.
Functional capacity was assessed with the Barthel Index.10 The scale consists of 10 variables describing activities of daily living (ADL) and mobility (eg, toileting, bathing, eating, dressing, continence, transfers, and ambulation). Total possible scores range from 0 to 100, with lower scores indicating increased disability.
Cognitive functions were assessed with the Abbreviated Mental Test Score (AMTS).11 The test is composed of 10 questions; each correctly answered question is scored with 1 point with a maximum score of 10 points. A score above 6 points implies normal cognition, 4–6 points – the presence of a moderate cognitive impairment, and 0–3 points – severe cognitive impairment. AMTS is a cognitive assessment tool which successfully differentiates subjects with dementia from those without dementia and can be used for dementia screening.12
According to the obtained AMTS results, subjects were divided into two groups in which the presence and intensity of pain were examined with different tools:
Each part has three levels of intensity in the range of 0 – 3, where 0 means the absence of a symptom, 1 – mild intensity, 2 – moderate intensity, and 3 corresponds to severe intensity. APS results’ interpretation is as follows: 0–2 points refer to no pain, 3–7 points – mild pain, 8–13 points – moderate pain, and a score of 14 and more corresponds to severe pain. The assessment of pain with the APS was performed by trained nurses employed by the nursing homes, who knew the patients.
The analysis of residents’ pharmacotherapy
Each studied subject was assigned to one of the following categories, regardless of belonging to group 1 or 2:
- ineffectively controlled pain – persons with pain (according to NRS and APS) who received analgesics,
- uncontrolled pain – persons with pain (according to NRS and APS), without analgesics,
- effectively controlled pain – persons without pain (according to NRS and APS), but with analgesics,
- no pain – persons without diagnosed pain and without analgesics.
Additionally, subjects in whom pain was inappropriately treated (interpreted as pain treated ineffectively or untreated), were analyzed in detail. Depending on whether the pain intensity was evaluated with NRS or APS, two groups were distinguished:
- Group 1a – persons with NRS result above 0,
- Group 2a – persons with APS result above 2.
In regards to the drugs used to treat each individual, they were initially calculated and then qualitatively analyzed using coding based on the Anatomical Therapeutic Chemical (ATC) classification system recommended by The World Health Organization.15 All analgesics were divided according to the WHO analgesic ladder16 (step I - non-opioids: acetaminophen, nonsteroidal anti-inflammatory drugs [NSAIDs], step II - weak opioids, step III - strong opioids).
Statistical analysis
The results were expressed as a mean ± standard deviation. To evaluate the normality of distribution of the variables, the Shapiro-Wilk test was applied. Comparison between two groups was made with the Mann-Whitney test. Statistical significance of differences in the distribution of quality variables between the groups was analyzed with the Fisher’s exact test, due to the small sample size. Statistical significance was set at p<0.05. The STATISTICA software was used to perform all statistical analyses.
Results
The analyzed group consisted of 199 residents. The mean age of studied subjects was 81.6±8.7 years. Among them, 142 were females (71%). The mean length of institutionalization was 61±57 months.
Pain (effectively/ineffectively treated and untreated) was diagnosed in 67 subjects of group 1 (65%). In group 2 pain was present in 68 subjects (70%). There was no difference in pain frequency between the groups.
Among the subjects with pain from group 1 (n=67), inappropriately treated pain (treated ineffectively or untreated) was observed in 43 individuals (→group 1a – 64% of subjects with pain from group 1). Regarding the applied pain therapy, 28 persons received it ineffectively (42%), and for as many as 15 persons (22%) no treatment was provided.
Among studied subjects with pain from group 2 (n=68), inappropriately treated pain was present in 58 individuals (→group 2a – 85% of persons with pain from group 2). Inappropriately treated pain was observed more often in group 2 than in group 1 (p<0.01). The reason for this was the more frequent occurrence of untreated pain (52% vs 22% – p<0.001) as the presence of ineffective treatment was found comparable with that of group 1 (34% vs 42%).
Detailed analysis characterizing subjects with inappropriately treated pain (groups 1a and 2a) is presented in Table 1. Inappropriately treated subjects with cognitive impairment were characterized by a higher number of diagnoses (p<0.05), lower functional capacity assessed with the Barthel Scale (p<0.0001) and lower number of drugs used in therapy (p<0.0001).
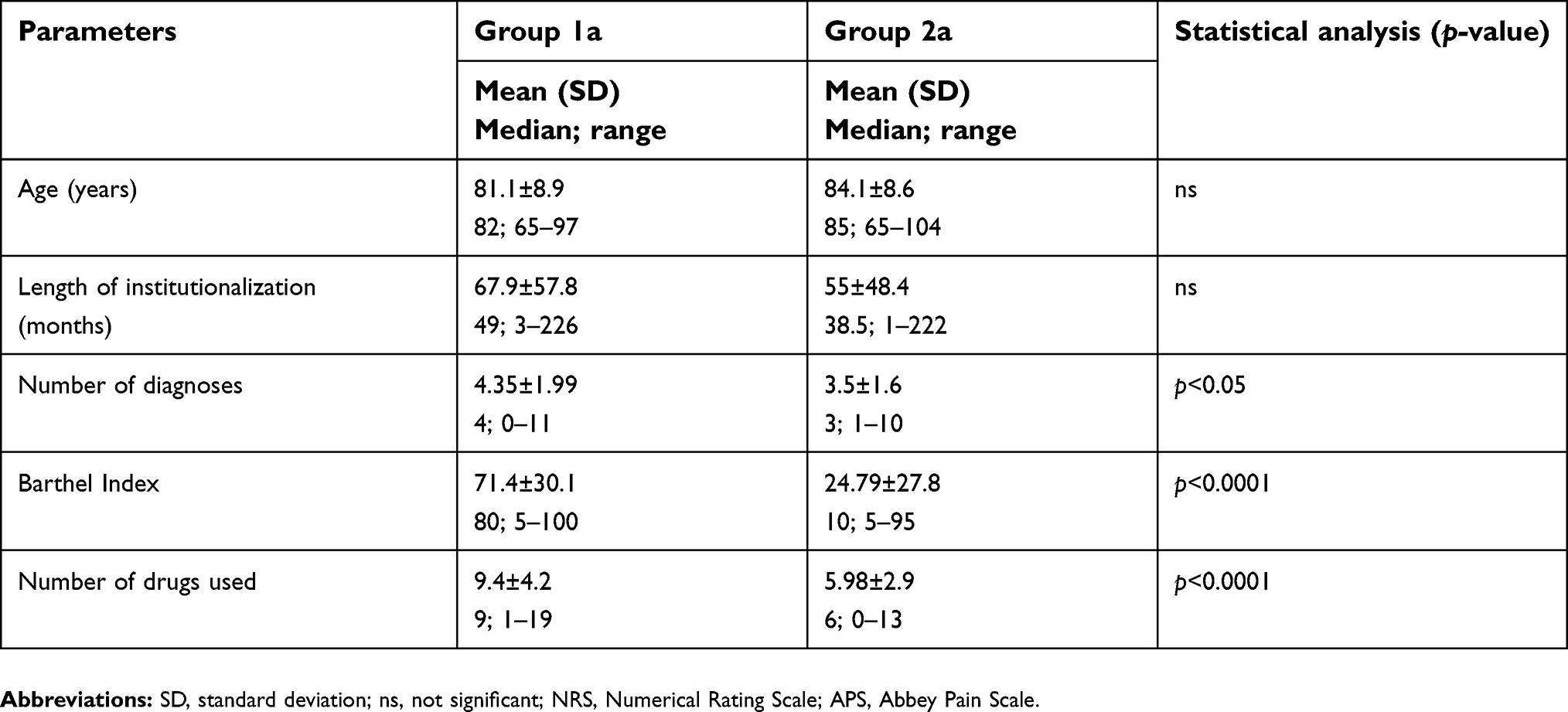 | Table 1 Detailed characteristic of inappropriately treated subjects (untreated or ineffectively treated), divided by their cognitive functions |
Qualitative analysis of pharmacotherapy in subjects with ineffectively treated pain (groups 1a and 2a)
Among the drugs from the first step of the analgesic ladder, acetaminophen was used most frequently (24 individuals); 16 subjects received acetaminophen in monotherapy and 8 – in combinations with substances from the second step of the analgesic ladder. As far as the daily dosage of acetaminophen in chronic treatment was concerned, the dose of 500 mg was received most frequently (9 individuals). Only two subjects consumed 1,000 mg of acetaminophen daily. The average daily dose of acetaminophen in ineffectively treated subjects was significantly lower than in effectively treated ones (590±193 mg vs 1,100±144 mg, p<0.001).
Nonsteroidal anti-inflammatory drugs (NSAIDs) were consumed by 21 subjects – 9 individuals received them in monotherapy whereas 6 – in combinations with acetaminophen and 6 – in combination with drugs from the second and third step of the analgesic ladder. Within different NSAIDs schemes of treatment, the most frequently used NSAID was diclofenac (n=14). There were two subjects receiving two oral NSAIDs concomitantly in their daily regimen: one of them received ibuprofen and naproxen, and the other one – diclofenac and meloxicam.
The second step of the analgesic ladder was mainly represented by a poly-pill preparation of tramadol and acetaminophen which was consumed by 13 individuals (8 of them were treated with single poly-pill preparation, 4 – in combination with acetaminophen and NSAIDs: meloxicam, diclofenac, 1 – in combination with tramadol). Only one subject received tramadol as a single preparation.
As few as six subjects received drugs from the third step of the analgesic ladder. This included buprenorphine in monotherapy (3 persons) or its combinations with NSAIDs (diclofenac and naproxen – 2 persons), and a poly-pill preparation of tramadol, acetaminophen and naproxen (1 person).
The qualitative characteristics of pharmacotherapy for residents with inappropriately treated pain (groups 1a and 2a), conducted according to the rules of the WHO analgesic ladder, are presented in Table 2.
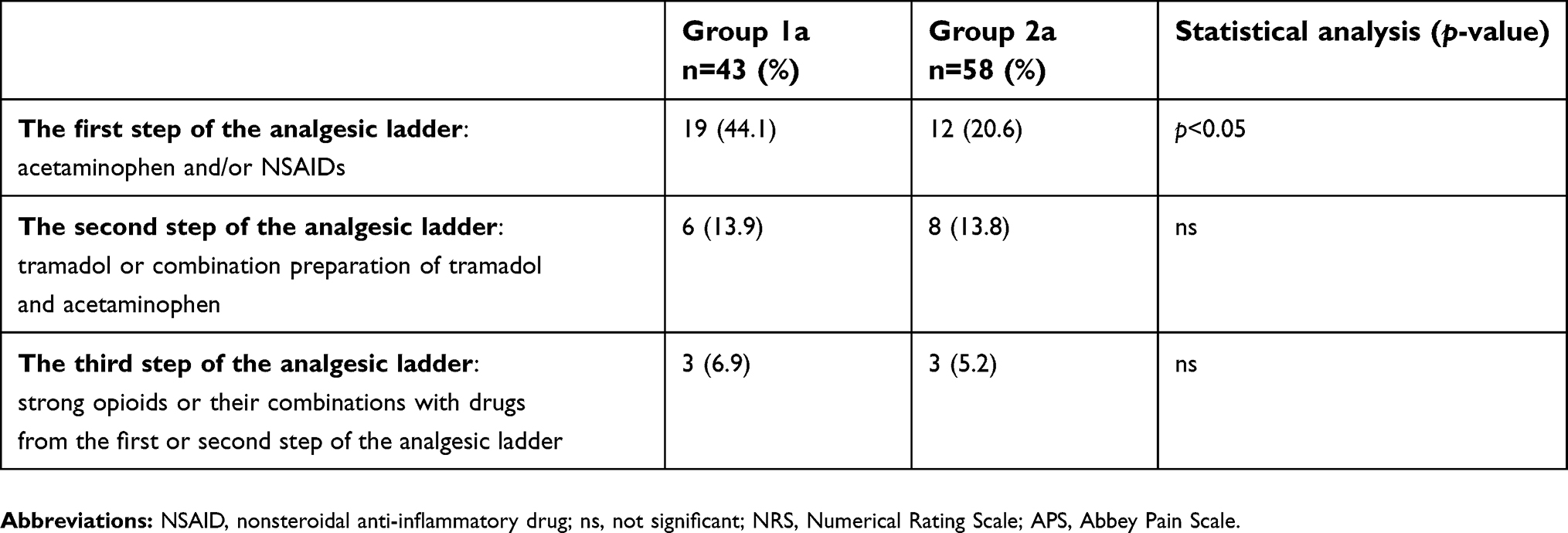 | Table 2 The qualitative characteristics of pharmacotherapy for residents with inappropriately treated pain (untreated or ineffectively treated), conducted according to the rules of the WHO analgesic ladder |
Discussion
The prevalence of pain in the analyzed groups was very high regardless of their cognitive status. Pain was diagnosed among in half of the subjects – this data is congruent with the study of Monroe et al who showed that the prevalence of pain was comparable among patients with normal cognition and those with dementia, and equaled 63.2% and 69.2%, respectively.17
In our study, no pharmacologic intervention took place, despite existing pain, in almost every fourth cognitively intact person and over half of the subjects with cognitive impairment. Similar results were presented by de Souto Barreto et al who conducted a multinational research project in nursing homes in Europe. In their study, pharmacological pain control was applied among 38.8–79.6% of older people with normal cognition and 20.2–61.2% of persons with dementia.18 There may be many reasons for such infrequent pharmacologic intervention among patients with cognitive impairment. Although, we did not examine pain knowledge of the nursing home staff, it seems possible that the level of their education could have contributed, as insufficient knowledge on pain management is stressed in the literature.4
It has been shown previously that nursing home residents with cognitive impairment were not asked about pain by the nursing staff even if they were able to verbalize it properly.17 Additionally, the same studies showed that subjects with cognitive impairment were not motivated to report their pain to medical staff. However, when asked by a caregiver, more than 50% of them declared an occurrence of pain, and even in almost 80% of the cases – moderate or major pain. Moreover, lack of effective pain assessment is currently observed in various clinical settings19 which is in agreement with the results of our study. There is a great need to provide support and clear guidance for all health professionals who are involved in the treatment and care for people with dementia, to enable them to make informed decisions and also to evade the apparent reluctance to prescribe effective analgesia.4
In our study, even when pharmacological intervention was undertaken, both the frequency of usage and the daily doses of analgesics from all steps of the analgesic ladder were very low. Within the first step, acetaminophen was used in only slightly more than every tenth subject. According to the current recommendations, it is the first-line analgesic for the treatment of various type of pain among older patients.20,21 Moreover, in our study, the average dosage of acetaminophen was much lower than the recommended daily dose. Low frequency of acetaminophen administration was also observed in a study conducted among German nursing home residents.22 Given a relatively low price of acetaminophen, it seems that the limited knowledge of both medical staff and patients of the high safety profile and effectiveness of acetaminophen should be taken into consideration when explaining this phenomenon.23
The quantitative and qualitative analysis of drugs from the second and third step of the analgesic ladder in our study showed extremely low frequency of using opioids. Less than every tenth patient was treated with tramadol, and only slightly more than every twentieth patient received buprenorphine. It may represent the phenomenon of “opiophobia,” which means avoiding opioids due to exaggerated concern over the adverse effects. Opiophobia is described in the context of patients, their caregivers and medical staff engaged in the administration of these drugs.24,25 It can also be related to the lack of sufficient knowledge about pain.
In the current study, we noted significantly lower Barthel Index scores in inappropriately treated subjects with cognitive impairment compared to those cognitively intact. This difference may be due to the residents’ lower functional capacity and can be at least partially related to their lower cognitive functions. This finding is consistent with the literature, as it was noticeably shown that dementia affected functional capacity. Abreu et al observed that activities of daily living (such as: food preparation, medication/taking pills, looking after the home, toilet use, sensory problems, communication/interaction, bladder and bowel function, eating and drinking, memory, sleeping, and falls prevention) were among the most prevalent healthcare needs in subjects with moderate to severe dementia.26
Limitations of our study include, for example, that it was necessary to select the diagnostic tools pertinent to the cognitive functions. Thus, in cognitively intact subjects NRS was used whereas in those with cognitive impairment – APS. Moreover, although APS is recommended as a standard tool for diagnosis and monitoring of pain, it must be pointed out that pain may not be the only reason for behavioral disturbances in subjects with cognitive impairment. Still, this type of limitation applies not only to APS but equally to all observational scales dedicated to the assessment of pain in subjects with cognitive impairment.
Also, despite the fact that did not analyze untreated pain factors, it should be noted that proper pain management is not limited to providing enough analgesia. Detecting and treating the underlying pain-predisposing diagnoses are definitely the crucial steps in management of pain as they ensure a causative rather than symptomatic treatment. Although addressing pain predisposing factors is extremely important, it was not the objective of the present study (our aim was to characterize the pharmacological pain treatment).
The consequences of underdiagnosed or untreated pain are not only a threat to the functional independence of older persons, but they can even be fatal. Detecting the existence of pain and routine use of at least one pain assessment scale dedicated to subjects with cognitive impairment should be the gold standard in the treatment of patients with dementia and intercurrent behavior disorders, particularly if they have difficulties with or inability of their verbalization.27–29
Conclusion
In our study, we observed a high prevalence of untreated or ineffectively treated pain regardless of the cognitive status of the studied NHR. These phenomena were particularly frequent in subjects with cognitive impairment. Therefore, appropriate education of the nursing and medical staff is necessary to increase their knowledge about both the pain assessment and its treatment.
Acknowledgment
Tomasz Nowak and Agnieszka Neumann-Podczaska are co-first authors of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Achterberg WP, Gambassi G, Finne-Soveri H, et al. Pain in European long-term care facilities: cross-national study in Finland, Italy and The Netherlands. Pain. 2010;148(1):70–74. doi:10.1016/j.pain.2009.10.008
2. van Herk R1, Boerlage AA, van Dijk M, Baar FP, Tibboel D, de Wit R. Pain management in Dutch nursing homes leaves much to be desired. Pain Manag Nurs. 2009;10(1):32–39. doi:10.1016/j.pmn.2008.06.003
3. Erdal A, Flo E, Selbaek G, et al. Associations between pain and depression in nursing home patients at different stages of dementia. J Affect Disord. 2017;218:8–14. doi:10.1016/j.jad.2017.04.038
4. Achterberg WP, Pieper van Dalen-Kok AH, de Waal MW, et al. Pain management in patients with dementia. Clin Interv Aging. 2013;8:1471–1482. doi:10.2147/CIA.S36739
5. Tan EC, Jokanovic N, Koponen MP, Thomas D, Hilmer SN, Bell JS. Prevalence of analgesic use and pain in people with and without dementia or cognitive impairment in aged care facilities: a systematic review and meta-analysis. Curr Clin Pharmacol. 2015;10(3):194–203.
6. Neumann-Podczaska A, Nowak T, Suwalska A, et al. Analgesic use among nursing homes residents, with and without dementia, in Poland. Clin Interv Aging. 2016;21(11):335–340.
7. McAuliffe L, Nay R, O`Donnell M, Fetherstonhaugh D. Pain assessment in older people with dementia: literature review. J Adv Nurs. 2009;65:2–10.
8. Cohen-Mansfield J, Thein K, Marx MS, Dakheel-Ali M. What are the barriers to performing nonpharmacological interventions for behavioral symptoms in the nursing home? J Am Med Dir Assoc. 2012;13:400–405. doi:10.1016/j.jamda.2011.07.006
9. Nowak T, Neumann-Podczaska A, Deskur-Śmielecka E, Styszyński A, Wieczorowska-Tobis K. Pain as a challenge in nursing home residents with behavioral and psychological symptoms of dementia. Clin Interv Aging. 2018;25(13):1045–1051. doi:10.2147/CIA.S157246
10. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
11. Qureshi KN, Hodkinson HM. Evaluation of a ten-question mental test in the institutionalized elderly. Age Ageing. 1974;3(3):152–157.
12. Foroughan M, Wahlund LO, Jafari Z, Rahgozar M, Farahani IG, Rashedi V. Validity and reliability of Abbreviated Mental Test Score (AMTS) among older Iranian. Psychogeriatrics. 2017;17(6):460–465. doi:10.1111/psyg.12229
13. Farrar JT, Young JP
14. Abbey J, Piller N, De Bellis A et al. The Abbey pain scale: a 1-minute numerical indicator for people with end-stage dementia. Int J Palliat Nurs. 2004;10(1):6–13.
15.
16.
17. Monroe TB, Misra SK, Habermann RC, Dietrich MS, Cowan RL, Simmons SF. Pain reports and pain medication treatment in nursing home residents with and without dementia. Geriatr Gerontol Int. 2014;14(3):541–548. doi:10.1111/ggi.12130
18. de Souto Barreto P, Lapeyre-Mestre M, Vellas B, Rolland Y. Potential underuse of analgesics for recognized pain in nursing home residents with dementia: a cross-sectional study. Pain. 2013;154(11):2427–2431. doi:10.1016/j.pain.2013.07.017
19. McAuliffe L, Brown D, Fetherstonhaugh D. Pain and dementia: an overview of the literature. Int J Older People Nurs. 2012;7(3):219–226. doi:10.1111/j.1748-3743.2012.00331.x
20. Makris U, Abrams R, Gurland B, Reid C. Management of persistent pain in the older patient a clinical review. JAMA. 2014;312:825–836. doi:10.1001/jama.2014.9405
21. Abdulla A, Adams N, Bone M, et al;
22. Kölzsch M, Wulff I, Ellert S, et al. Deficits in pain treatment in nursing homes in Germany: a cross-sectional study. Eur J Pain. 2012;16:439–446. doi:10.1002/j.1532-2149.2011.00029.x
23. Zwakhalen S, Hamers J, Peijnenburg R, Berger M. Nursing staff knowledge and beliefs about pain in elderly nursing home residents with dementia. Pain Res Manag. 2007;12:177–184. doi:10.1155/2007/518484
24. Webster F, Bremner S, Oosenbrug E, Durant S, McCartney C, Katz J. From opiophobia to overprescribing: a critical scoping review of medical education training for chronic pain. Pain Med. 2017;18:1467–1475. doi:10.1093/pm/pnw352
25. Spitz A, Moore AA, Papaleontiou M, Granieri E, Turner BJ, Reid MC. Primary care providers’ perspective on prescribing opioids to older adults with chronic non-cancer pain: a qualitative study. BMC Geriatr. 2011;11:35. doi:10.1186/1471-2318-11-35
26. Abreu W, Tolson D, Jackson GA, Staines H, Costa N. The relationship between frailty, functional dependence, and healthcare needs among community-dwelling people with moderate to severe dementia. Health Soc Care Community. 2018. doi:10.1111/hsc.12678
27. Cohen-Mansfield J. Pain assessment in noncommunicative elderly persons–PAINE. Clin J Pain. 2006;22(6):569–575. doi:10.1097/01.ajp.0000210899.83096.0b
28. Reid MC, Eccleston C, Pillemer K. Management of chronic pain in older adults. BMJ. 2015;350:h532. doi:10.1136/bmj.h532
29. Schofield P, Abdulla A. Pain assessment in the older population: what the literature says. Age Ageing. 2018;47:324–327. doi:10.1093/ageing/afy018
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.