")
Back to Journals » Open Access Journal of Contraception » Volume 13
Characteristics of Patients Requiring Surgical Removal of Subdermal Contraceptive Implants: A Case–Control Study
Authors Katabi L , Stevens E, Ascha M, Arora K
Received 27 March 2022
Accepted for publication 8 July 2022
Published 8 August 2022 Volume 2022:13 Pages 111—119
DOI https://doi.org/10.2147/OAJC.S368250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Leila Katabi,1 Erica Stevens,1 Mona Ascha,2 Kavita Arora3,4
1Case Western Reserve University School of Medicine, Cleveland, OH, 44106, USA; 2Division of Plastic and Reconstructive Surgery, Department of Surgery, University Hospitals Cleveland Medical Center, Cleveland, OH, 44106, USA; 3Department of Obstetrics and Gynecology, MetroHealth Medical Center, Cleveland, OH, 44109, USA; 4Department of Obstetrics and Gynecology, University of North Carolina, Chapel Hill, NC, 27514, USA
Correspondence: Kavita Arora, Department of Obstetrics and Gynecology, University of North Carolina, 101 Manning Drive, Chapel Hill, NC, 27514, USA, Tel +1 919-843-8295, Email [email protected]
Purpose: Etonogestrel subdermal implants are a commonly used contraceptive device placed in the medial upper arm. Plastic and orthopedic surgeons may be consulted for difficult implant removals. We performed a case–control study comparing patients undergoing surgical and uncomplicated in-office removal at our institution.
Patients and Methods: We identified patients who underwent operative removal of implantable contraceptive devices by plastic or orthopedic surgeons at our institution from January 2014 to October 2019. Patients who underwent uncomplicated office removal during the same time were compared. Demographic and surgical variables were collected, and descriptive statistics were calculated. Univariate and multivariate logistic regression was performed with surgical versus outpatient removal as the outcome of interest.
Results: A total of 669 patients undergoing etonogestrel subdermal implant removals were identified during the five-year study period, of which thirteen patients required surgical removal (1.9%) and 326 were selected as uncomplicated removal comparisons. There were no significant differences in median (IQR) body mass index (BMI) (31.1 [28.2, 35.2] versus 29.3 [24.0, 35.1], p = 0.19), median (IQR) weight gain since device placement (5 [− 0.6, 14.7] kilograms versus 1.6 [− 1.2, 5.8] kilograms, p = 0.15), or length of time since device insertion (2.3 [0.8, 2.8] years versus 1.0 [0.4, 2.2] years, p = 0.17). Of those who needed surgical removal, the most common indication for implant removal was device expiration (n = 5, 38.5%). Devices placed by OBGYN attendings were less likely to require surgical removal (p = 0.02). Family medicine attendings were more likely to refer patients for surgical removal (p = 0.02). No significant findings were detected on univariate or multivariate regression. Among surgical removals, radiography was the most frequently used imaging modality. Implants were most frequently subdermal (n = 11, 84.6%) though intramuscular placement was also identified (n = 2, 15.4%). Only one patient had residual paresthesia along the length of the incision. No other complications were identified.
Conclusion: We did not identify risk factors associated with the difficult removal of etonogestrel subdermal implants. Practitioners should consult upper extremity surgeons if they encounter difficult removals.
Keywords: nexplanon, etonogestrel subdermal implant, upper extremity surgery, implantable contraception
Introduction
Etonogestrel contraceptive implants are a widely used form of contraception in the United States. The implant is typically inserted subdermally along the medial upper arm in an outpatient clinic.1 At the time of this study period, practitioners had been instructed to place the implant just below the dermis in the sulcus between the biceps and triceps muscles. Given the difficulty with removals and the risk of migration, the insertion site was changed in 2020 to overlying the triceps muscle, about 8 to 10 cm from the medial epicondyle and 3 to 5 cm posterior to the sulcus between the biceps and triceps muscles.1 The implant is removed after three years or earlier per patient request. Patients may present for removal for a number of reasons, such as weight gain, desire to become pregnant, or unfavorable bleeding pattern.2
The device is typically removed in an outpatient setting by manipulating the rod out of a perpendicular incision made at the distal end of the implant after injection of local anesthetic. When the practitioner cannot successfully remove the implant, however, the patient may be referred to a specialized center with family planning expertise3,4 or an upper extremity surgeon for surgical removal.2 Prior case reports have described proximal migration of the device into the axilla,5 in the deep compartments of the arm, and even into pulmonary vasculature.6–8 Factors associated with difficult removals include weight gain and longer duration of device placement.9 In addition, identifying anatomic landmarks of the upper extremity can be challenging in patients with obesity,10 which may negatively impact insertion technique and palpation for removal. While there are data to support referral of difficult removals to fellowship-trained family planning providers,3,4 there is a lack of literature characterizing patients that have been referred to plastic and orthopedic surgeons for etonogestrel subdermal implant removal.11
The purpose of this case–control study is to compare patients undergoing surgical removal of etonogestrel subdermal implants with patients who undergo uncomplicated in-office removal. We hypothesize that patients requiring surgical removal will have a higher body mass index (BMI) and longer duration of implant placement and that surgical removal is generally uncomplicated.
Materials and Methods
This single institution, retrospective chart review study was approved by the institutional review board at MetroHealth Medical Center and conducted in accordance with the Declaration of Helsinki. A waiver of informed consent was granted because the study posed no more than minimal risk to participants, the data was already in existence in the medical record, obtaining specific consent from each patient in our dataset would pose logistical and confidentiality challenges, and inclusion of de-identified data in research is included in our institution’s general consent form. Patient data was kept confidential via a Research Electronic Data Capture (REDCap) database.
Study Population
Given the rarity of surgical implant removal, estimated to be about 0.05%,12 a case–control study design was used. First, Current Procedural Terminology (CPT) codes were used to identify female patients ages 14 to 52 years who underwent operative removal of a foreign body by plastic or orthopedic surgeons at MetroHealth Medical Center from January 2014 to October 2019. This age range was used, given the device’s goal as a contraceptive method. Because Nexplanon® was introduced in 2011 as the only available contraceptive implant in the United States and is removed after three years,13 we assume that all devices identified in our study are Nexplanon® devices. Medical records were reviewed to identify patients who presented specifically for surgical implantable contraceptive removal. This identified thirteen patients.
To identify patients who underwent uncomplicated removal in the outpatient office during the same time period as a comparison, a billing-based report of all patients at our institution with the International Disease Classification (ICD) diagnosis codes “Nexplanon removal”, “Encounter for Nexplanon removal”, or “Encounter for removal of subdermal contraceptive implant” were included. This identified 669 patients. We planned on selecting a minimum of 300 uncomplicated in-office removals for comparison. This was based on the sample size calculation of 95% confidence, with a 5% error rate, and a population of 669 implant removals identified, yielding a necessary minimum sample size of 245 patients. For simplicity, controls were selected by reviewing every other patient.
Data Collection
The following demographic variables were collected: age, ethnicity, BMI, parity, smoking status, comorbidities, duration of implant, handedness, and removal indication. For patients undergoing operative removal, the following additional operative characteristics were collected: imaging studies, operative time, concomitant operative procedures, intraoperative location of implant, and postoperative complications. Data was electronically entered into a Research Electronic Data Capture (REDCap) database at our institution.
Statistical Analysis
Descriptive statistics for demographic variables were calculated. Normally distributed numerical data are presented as mean and standard deviation (SD); non-normally distributed data are presented as median and interquartile range (IQR). Categorical data are presented as frequencies and percentages. Fisher’s exact test was performed for tests of proportions, and Mann Whitney test was performed for continuous variables. Univariate and multivariate logistic regression was performed with surgical versus outpatient removal as the outcome of interest and the following predictor variables: age, ethnicity, weight change since insertion (kg), parity, smoking status, and duration of implant in days. These variables were selected based upon previous studies4 and because they may influence skin and subcutaneous tissue structure and function.14,15 A p-value <0.05 was considered significant.
All analyses were performed using R (Version 4.0.1) and RStudio (Version 1.3.959).
Results
A total of 669 removals were identified during the five-year study period, of which thirteen (1.9%) patients required surgical removal by plastic and orthopedic surgeons and 326 (48.7%) were selected as uncomplicated removal controls. Patient demographics are presented in Table 1. Relative to uncomplicated removals, patients requiring surgical removal were approximately the same median (IQR) age (20.0 [17.8, 21.6] versus 23.3 [19.5, 26.8] years, p = 0.06), median (IQR) BMI (31.1 [28.2, 35.2] versus 29.3 [24.0, 35.1], p = 0.19), and with similar median (IQR) weight gain since device placement (5 [−0.6, 14.7] versus 1.6 [−1.2, 5.8] kg, p = 0.15).
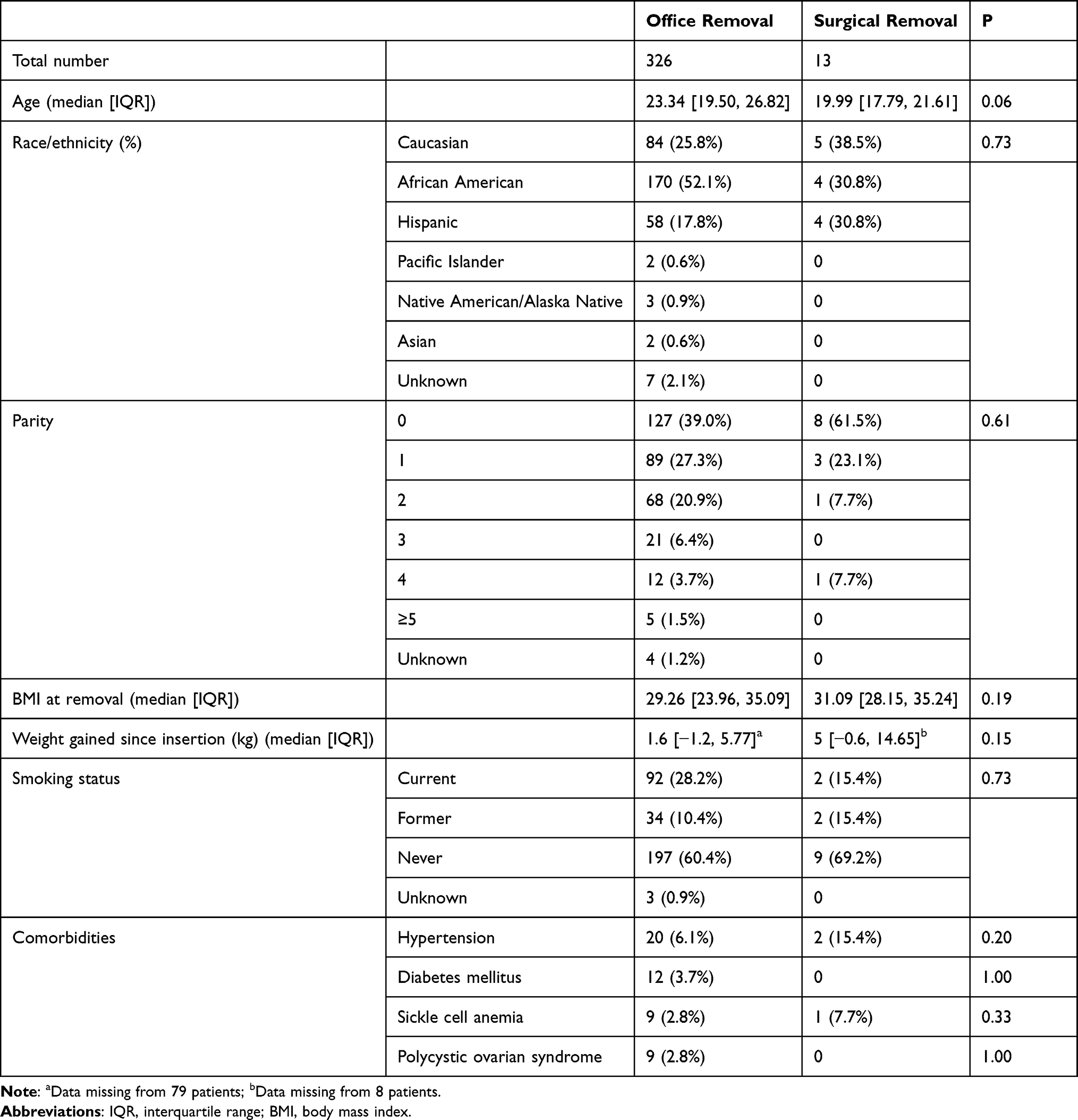 |
Table 1 Patient Demographics for Office versus Surgical Nexplanon Removal |
The most common reason for removal was unfavorable bleeding pattern in the uncomplicated removal group (n = 149, 45.7%). Of those who needed surgical removal, the most common indication for implant removal was device expiration (n = 5, 38.5%). Devices placed by OBGYN attendings were significantly less likely to require surgical removal (p = 0.02). Family medicine attendings were significantly more likely to refer patients for surgical removal (p = 0.02). Patients requiring surgical removal had the device inserted for a similar median length of time relative to patients with uncomplicated office removals (2.3 [0.8, 2.8] years versus 1.0 [0.4, 2.2] years, p = 0.17) (Table 2).
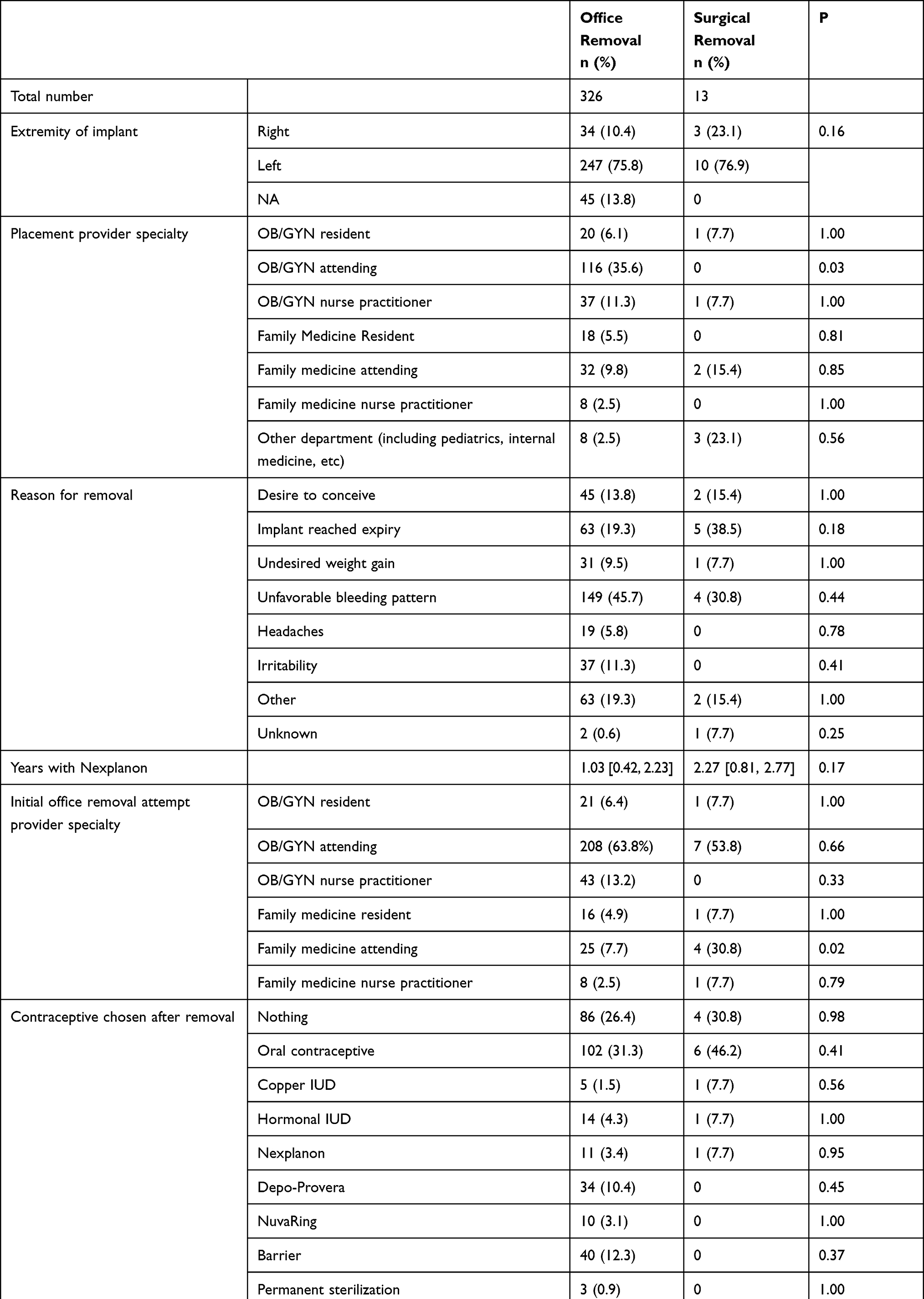 |
Table 2 Factors Related to Nexplanon Insertion and Removal |
Common reasons for surgical referral included inability to palpate the implant (n = 8, 61.5%) and/or unsuccessful attempt at office removal (n = 7, 53.8%). One implant was referred for surgical removal because it broke during attempted office removal. Patients received imaging both for implant localization and confirmation of removal, including humeral radiograph (n = 9, 69.2%), ultrasound (n = 7, 53.8%) and intraoperative fluoroscopy (n = 6, 46.2%). No patients received computed tomography or magnetic resonance imaging. Nearly half of the patients received general anesthesia (n = 6, 46.2%) with a median (IQR) operative time of 23.5 [16, 33] minutes. The implant was in the subdermal tissue the majority of the time (n = 11, 84.6%), and one patient had residual paresthesia along the length of the incision (Table 3). No other postoperative complications were reported.
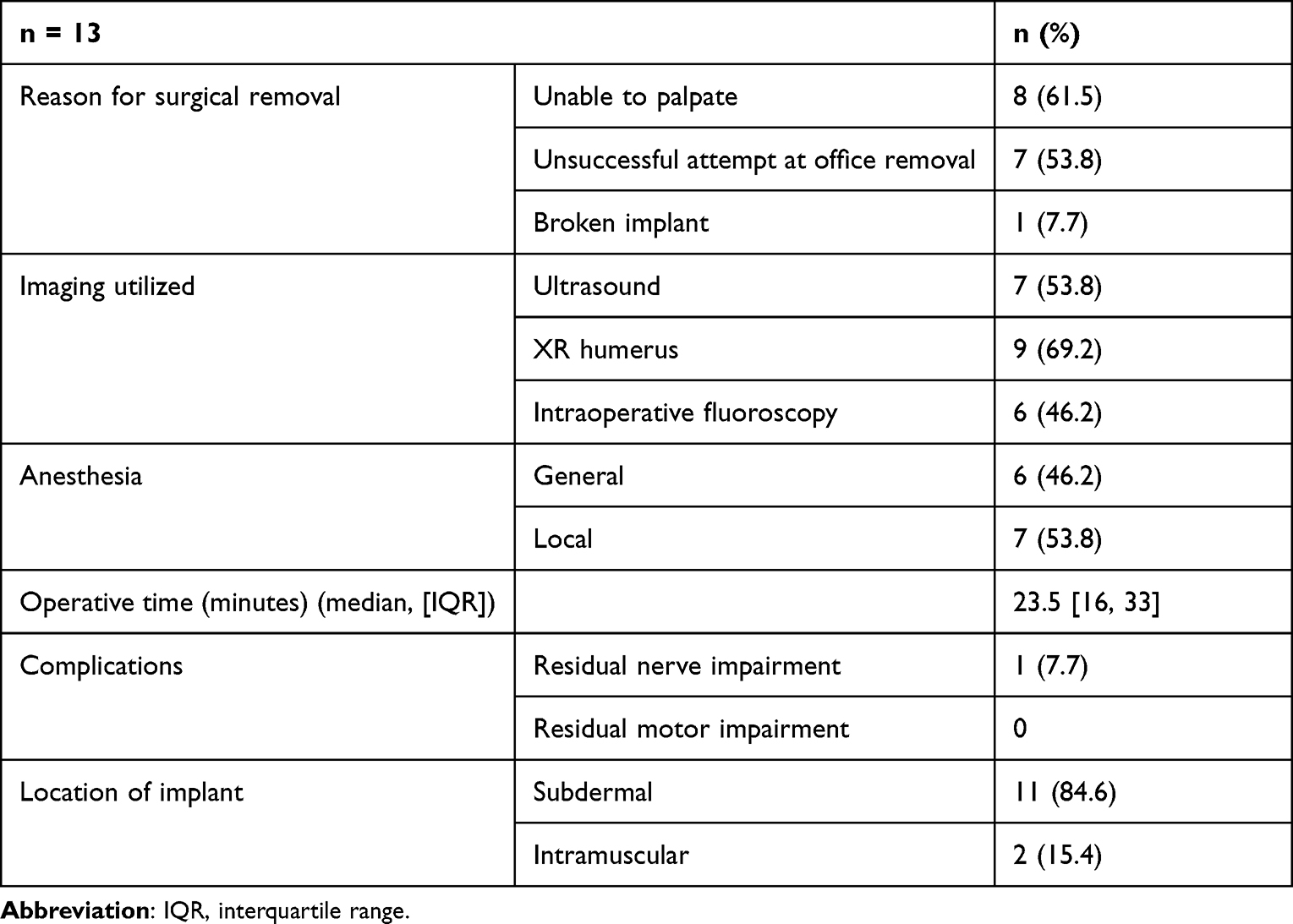 |
Table 3 Characteristics of Patients Requiring Surgical Nexplanon Removal |
Table 4 summarizes the results of univariate and multivariate logistic analyses assessing surgical versus office removal for age, weight difference between insertion and removal, parity, duration of implant, ethnicity, and smoking status. No significant findings were detected.
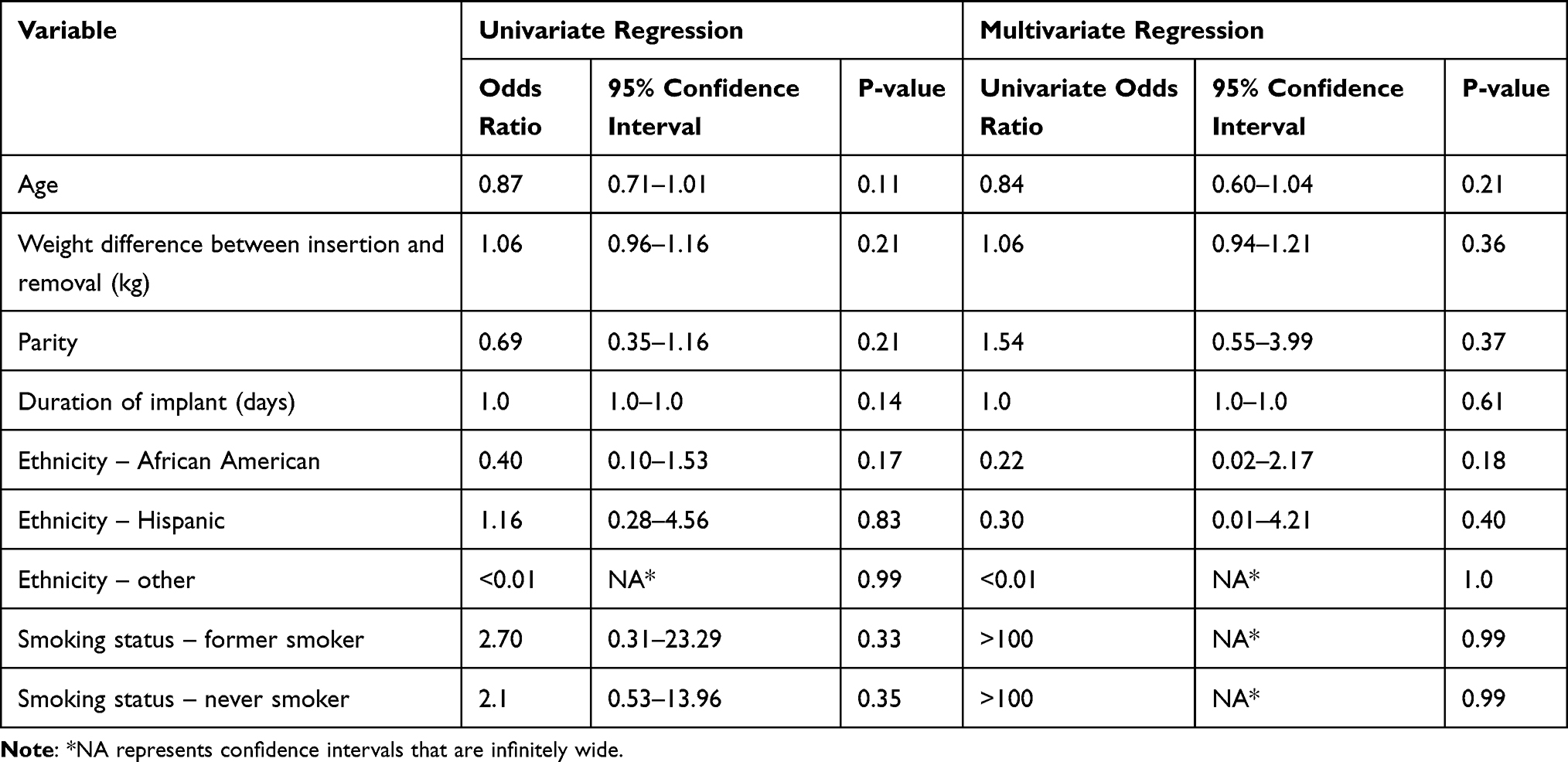 |
Table 4 Results of Univariate and Multivariate Regression |
Supplemental Table 1 reports imaging results and key operative notes for the thirteen patients who underwent surgical removal.
Discussion
The present study describes the demographic and surgical characteristics of etonogestrel subdermal implant removal in the outpatient and surgical settings. Our hypothesis was incorrect; patients requiring surgical implant removal were similar to those undergoing uncomplicated office removals in terms of median BMI, weight gain, and duration of implant placement.
One study of patients who were referred to a Family Planning clinic for inability to remove an implant in the outpatient setting suggests that weight gain since device insertion, rather than BMI at removal, may result in difficult removal.9 While our data demonstrated a difference in weight gain between surgical (5kg) and office removals (1.6kg), our findings did not reach statistical significance. The strength of our findings may be limited by an overall small sample size and a large number of missing weight variables. Methodologic and patient population differences may also contribute to this discrepancy as the prior study defined difficult removal as ultrasound guided (n = 55) or surgical removal (n = 8), whereas only surgical removals (n = 13) were examined in the present study.10 In addition, the average BMIs in both complicated and uncomplicated removals in Matulich et al’s study population were within the normal range (approximately 25); whereas the average BMI of our patient population was greater.
The duration of implant use was twice as long in the surgical removal group than the office removal group. Length of time with etonogestrel subdermal implants has been found to significantly influence the likelihood of difficult removal.9 Longer duration of the implant may allow for a longer progression of the foreign-body response, during which inflammatory mediators form a dense fibrotic capsule surrounding the foreign body.16 The fibrotic capsule may contribute to difficulty palpating the implant, as well as difficulty removing the implant during an office attempt.17 Half (n = 7) of the operative notes in the surgical cohort mentioned scar tissue around the implant, which may have contributed to difficult removal in the outpatient setting.
The Nexplanon® insertion device is designed to prevent insertion deep ito the subcutaneous tissue plane as an improvement upon predecessor devices.18 However, the present study identified two patients with intramuscular insertion. Previous reports propose that thinner women with less subcutaneous tissue may be more at risk of subfascial placement,4,18–20 but the two patients with intramuscular placement in our cohort had relatively high BMIs. Thus, while improvements to the Nexplanon® insertion device may be helpful, practitioners must remain mindful when placing implants.
Though uncommon,4,17 difficult removals can result in upper extremity neuropathy. Two case studies report median nerve damage causing both motor and sensory impairment after unsuccessful attempts at office removal. Improvement in function was achieved following secondary surgeries for neuroma excision.21,22 A case of complete ulnar nerve palsy has been reported following etonogestrel subdermal implant removal, with only marginal improvement after neuroma excision and sural nerve cable grafting.23 It is recommended that an upper extremity surgeon become involved in removal when there is an increased risk of neurovascular injury.11 All surgical removals in the present study were performed by plastic and orthopedic surgeons with peripheral nerve expertise.
If surgical removal is being performed by an upper extremity surgeon, radiography can be used as the first-line imaging modality for localization of nonpalpable devices. This takes advantage of the barium sulfate implant core that allows for radiographic visualization,18 and orthopedic and plastic surgeons often operate with radiography in real time.24 A pre-operative radiograph can be ordered by the referring provider. Intraoperative fluoroscopy was utilized in our surgical cohort for both implant localization and confirmation of device removal. This is particularly advantageous for localizing the implant in two dimensions and minimizing damage to nearby structures with blind dissection. It also confirms that no implant is left behind since the device can break during removal.25 While underutilized in our study cohort, given the short operating time and location of surgery, the use of local anesthetic rather than general anesthetic is preferable.
This investigation has limitations inherent to its retrospective design. The sample size of thirteen surgical removals is small, though the incidence of surgical etonogestrel subdermal implant removals is low; we recognize this could lead to type two errors. We assume that all devices studied were Nexplanon® given the time frame of the study, but we are unable to confirm this given the retrospective nature of the study. The study is also at risk of selection bias, given the case–control design. While selected based on position, the controls may not be representative of the entire population of patients who received etonogestrel subdermal implants at our institution. In addition, the controls all have the outcome of in-office removal because that is how they were identified via CPT codes. However, uncomplicated removals can also occur in the operating room or inpatient based on patient and clinician preference. Furthermore, the patient demographics and practice patterns may be unique to the single institution of this study cohort, limiting generalizability. In addition, the differences in study population and outcomes for referral to a family planning physician versus upper extremity surgeon are unclear and deserving of further study.
Conclusion
Age, weight difference between insertion and removal, parity, duration of implant, ethnicity, and smoking status were not associated with difficult removal of the subdermal implant in our study. Devices placed by OBGYN attendings were significantly less likely to require surgical removal, while family medicine attendings were significantly more likely to refer patients for surgical removal. Practitioners should follow manufacturer guidelines for insertion and receive adequate training in the insertion of devices. Practitioners should consult upper extremity surgeons if they encounter difficult removals.
Disclosure
Dr. Arora is funded by 1R01HD098127 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) branch of the National Institutes of Health (NIH). This manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The remaining authors report no conflicts of interest in this work.
References
1. Merk. Nexplanon prescribing information; 2017:1–23.
2. Vidin E, Garbin O, Rodriguez B, et al. Removal of etonogestrel contraceptive implants in the operating theater: report on 28 cases. Contraception. 2007;76(1):35–39. doi:10.1016/j.contraception.2007.03.012
3. Mastey N, Matulich M, Uhm S, et al. US referral center experience removing nonpalpable and difficult contraceptive implants with in-office ultrasonography: a case series. Contraception. 2021;103:428–430. doi:10.1016/j.contraception.2021.01.018
4. Matulich M, Chen M, Schimmoeller N, et al. Referral center experience with nonpalpable contraceptive implant removals. Obstet Gynecol. 2019;134:801–806. doi:10.1097/AOG.0000000000003457
5. Diego D, Tappy E, Carugno J. Axillary migration of Nexplanon®: case report. Contraception. 2017;95:218–220. doi:10.1016/j.contraception.2016.11.002
6. Carlos-Alves M, Gomes M, Abreu R, et al. Lung migration of contraceptive Implanon NXT. BMJ Case Rep. 2019;12(7):1–2. doi:10.1136/bcr-2019-230987
7. Cerato A, Luyckx M, Ghaye B. Migration of implanon contraceptive implant into the pulmonary artery. Diagn Interv Imaging. 2019;100:59–60. doi:10.1016/j.diii.2018.08.006
8. Hindy JR, Souaid T, Larus CT, et al. Nexplanon migration into a subsegmental branch of the pulmonary artery: a case report and review of the literature. Med. 2020;99:1–5.
9. Chevreau J, Krief D, Abou Arab O, et al. Factors associated with removal difficulties of etonogestrel-containing contraceptive implants (Nexplanon®). Eur J Obstet Gynecol Reprod Biol. 2018;224:81–84. doi:10.1016/j.ejogrb.2018.03.019
10. Nielsen KC, Guller U, Steele SM, et al. Influence of obesity on surgical regional anesthesia in the ambulatory setting: an analysis of 9038 blocks. Anesthesiology. 2005;102(1):181–187. doi:10.1097/00000542-200501000-00027
11. Odom EB, Eisenberg DL, Fox IK. Difficult removal of subdermal contraceptive implants: a multidisciplinary approach involving a peripheral nerve expert. Contraception. 2017;96(2):89–95. doi:10.1016/j.contraception.2017.05.001
12. Crenin MD, Kaunitz AM, Darney PD, et al. The US etonogestrel implant mandatory clinical training and active monitoring programs: 6-year experience. Contraception. 2017;95:205–210. doi:10.1016/j.contraception.2016.07.012
13. Palomba S, Falbo A, Di Cello A, et al. Nexplanon: the new implant for long-term contraception. A comprehensive descriptive review. Gynecol Endocrinol. 2012;28(9):710–721. doi:10.3109/09513590.2011.652247
14. Langton AK, Tsoureli-Nikita E, Merrick H, et al. The systemic influence of chronic smoking on skin structure and mechanical function. J Pathol. 2020;251:420–428. doi:10.1002/path.5476
15. Rawlings A. Ethnic skin types: are there differences in skin structure and function? Int J Cosmet Sci. 2006;28:79–93. doi:10.1111/j.1467-2494.2006.00302.x
16. Ward WK. A review of the foreign-body response to subcutaneously-implanted devices: the role of Macrophages and cytokines in biofouling and fibrosis. J Diabetes Sci Technol. 2008;2:768–777. doi:10.1177/193229680800200504
17. Reed S, Do Minh T, Lange JA, et al. Real world data on Nexplanon® procedure-related events: final results from the Nexplanon Observational Risk Assessment study (NORA). Contraception. 2019;100(1):31–36. doi:10.1016/j.contraception.2019.03.052
18. Mansour D. Nexplanon®: what Implanon® did next. J Fam Plan Reprod Heal Care. 2010;36:187–189. doi:10.1783/147118910793048629
19. Guiahi M, Tocce K, Teal S, et al. Removal of a Nexplanon® implant located in the biceps muscle using a combination of ultrasound and fluoroscopy guidance. Contraception. 2014;90(6):606–608. doi:10.1016/j.contraception.2014.06.030
20. Johnson TZ, Annis T, Kennedy A, et al. Intramuscular placement of birth control device: a multimodality case and review. Cureus. 2019;11:10–13.
21. Christensen JM, Caggiano NM, Giladi AM, et al. Median nerve injury after removal of subdermal implantable contraceptive. Hand. 2017;13:1–4.
22. Restrepo CE, Spinner RJ. Major nerve injury after contraceptive implant removal: case illustration. J Neurosurg. 2016;124:188–189. doi:10.3171/2015.1.JNS142642
23. Lefebvre R, Hom M, Leland H, et al. Peripheral nerve injury with Nexplanon removal: case report and review of the literature. Contracept Reprod Med. 2018;3:1–6. doi:10.1186/s40834-018-0070-0
24. Kausch L, Thomas S, Kunze H, et al. Toward automatic C – arm positioning for standard projections in orthopedic surgery. Int J Comput Assist Radiol Surg. 2020;15:1095–1105. doi:10.1007/s11548-020-02204-0
25. Crouthamel BC, Schiff MA, Amies Oelschlager AME, et al. Bits and pieces: a crowd-sourced series of 54 cases of fractured hormonal implants. J Pediatr Adolesc Gynecol. 2018;31:128–131. doi:10.1016/j.jpag.2017.10.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.