")
Back to Journals » Journal of Healthcare Leadership » Volume 12
Characteristics of Faculty at Risk of Leaving Their Medical Schools: An Analysis of the StandPoint™ Faculty Engagement Survey
Authors Zimmermann EM, Mramba LK, Gregoire H, Dandar V, Limacher MC , Good ML
Received 30 July 2019
Accepted for publication 25 November 2019
Published 8 January 2020 Volume 2020:12 Pages 1—10
DOI https://doi.org/10.2147/JHL.S225291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Russell Taichman
Ellen M Zimmermann, 1 Lazarus K Mramba, 2 Hamleen Gregoire, 3 Valerie Dandar, 4 Marian C Limacher, 5 Michael L Good 6
1Faculty Development, College of Medicine, Department of Medicine, Division of Gastroenterology, University of Florida, Gainesville, FL, USA; 2Department of Biostatistics & Data Science, University of Kansas, Kansas City, KS, USA; 3Faculty Affairs in the College of Medicine, University of Florida, Gainesville, FL, USA; 4Medical School Operations, Academic Affairs, Association of American Medical Colleges, Washington, DC, USA; 5Faculty Affairs and Professional Development, College of Medicine, Department of Medicine, Division of Cardiology, University of Florida, Gainesville, FL, USA; 6University of Utah School of Medicine, Health Sciences, University of Utah, Salt Lake City, UT, USA
Correspondence: Ellen M Zimmermann
University of Florida, 1329 SW 16th ST, Suite 5251, Gainesville, FL 32608, USA
Tel +1352-273-9474
Email [email protected]
Purpose: This study seeks to identify the characteristics and attitudes of faculty in US medical colleges who are at risk of leaving their institution.
Methods: This research leverages data from the AAMC StandPoint Faculty Engagement Survey administered to 37,779 faculty representing 36 institutions participating during 2013– 2016. Univariate and multivariable robust logistic regression models were used to assess predictors of the intent to leave based on the question: “Do you plan to leave this medical school in the next 1– 2 years?”.
Results: Thirty percent (n=5559/18,475) of faculty responded that they were considering leaving their institution. Thirty-one percent of female faculty vs 29% of male faculty expressed an intent to leave. At-risk faculty were likely to be at junior faculty rank and at their institutions for 6– 15 years vs other time periods (OR=1.16; p≤ 0.001). Having an administrative title (OR=0.72; p≤ 0.001) and receiving formal mentorship (OR=0.65; p≤ 0.001) were protective. Finally, faculty answering “disagree” or “strongly disagree” to any one of these StandPoint Survey questions were at > 6 fold risk of expressing an intent to leave: 1) I am satisfied with my opportunities for professional development, 2) I feel appreciated by my supervisor, 3) My day-to-day activities give me a sense of accomplishment.
Conclusion: Faculty expressing an intent to leave their institution have an identifiable profile. Top concerns of at-risk faculty relate to supervisory relationships and growth opportunities rather than compensation or governance. Institutional leaders should consider these factors in the development of a proactive strategy to retain talented faculty.
Keywords: retention, professional development, mentorship, medical school governance
Introduction
Recruiting and retaining valued faculty are time-consuming activities that draw resources away from other missions of academic medical centers. The cost of recruitment has increased drastically in the past decade with a premium paid for successful basic science investigators and specialty clinicians, especially surgeons.1,2 While many medical schools struggle with the challenges of faculty retention, there is a paucity of data available to help leaders know who is at risk for leaving their institution and how to intervene before a faculty member commits to a position elsewhere.
Previous studies of faculty turnover have examined retention and the predictors of faculty decision-making in selected populations. Among clinical faculty, studies indicate a strong association between lack of reward for excellence in teaching and clinical service, and the intent to leave.3,4 In particular, clinicians who reported a lack of adequate services and facilities to provide excellent patient care were more likely to express an intent to leave their academic positions.3 Research also shows that female faculty were more likely to express an intent to leave if time or stress associated with work impacted their family life.5 Further, institutional “fit” between the individual and the job, described as the matching of expectations between the faculty and institution, was recognized as important for job satisfaction, important to prevent burnout, and as a deterrent to attrition.6–8 With respect to “fit”, a mismatch between the perception of an institution’s emphasis on reimbursement and billing vs faculty’s personal values stood out as significantly associated with an intent to leave.9
The experiences of US medical schools in addressing faculty departures reveal that faculty turnover includes many hidden costs. The cost of faculty loss includes the costs of recruitment and hiring and the cost of lost clinical income. A 2009 study estimated that replacing a single faculty in a department of medicine exceeded $400,000.10 There are added human costs to a department related to the “piling on” phenomenon of additional faculty leaving after key members of the faculty depart. Nonfinancial costs include reduced teaching and loss of opportunities for research and training; these losses affect institutional reputation and standing.11 Losing key faculty can negatively impact departmental climate which can have downstream effects on the volume of scholarly work and grant dollars brought into an institution.6
This study aims to identify factors associated with an intention to leave an institution that might help academic medical center leadership develop a proactive faculty retention strategy. We used a national faculty engagement survey to establish a profile of faculty expressing an intent to leave their institution for reasons other than leaving academic medicine or retirement. Our study focused on medical school faculty across clinical and basic science departments. The faculty concerns identified from our study are not medicine-specific. They parallel similar issues identified by talent managers in the business world and are likely to be relevant to other units within academic centers.
Methods
The AAMC Standpoint Faculty Engagement Survey is a validated survey tool offered by the AAMC to member medical schools to inform institutions about faculty engagement, satisfaction, and workplace culture. The web-based survey has been administered by the AAMC since 2009 and is an optional fee-based service by which the AAMC administers the survey on an institution’s behalf. Faculty participation is voluntary and respondents are permitted to skip questions while completing the survey. Responses are kept confidential by the AAMC and schools receive only aggregated reports of resulting data. There are survey items that address the factors known to drive employee engagement within academic medicine such as perceptions of institutional mission, opportunities for development, and governance. Survey items are organized into topic-based domains upon which data can be aggregated for reporting purposes and represented as summary scores (Descriptions provided in Table 1). Summary scores were calculated across items using similar response scales (e.g. 5-point Likert-scales for Satisfaction and Agreement). Previous studies from Bunton et al and others have described the survey content and validity measures in greater detail.12–14 For the purposes of this study, the research team was granted the use of the AAMC Standpoint data from 2013 to 2016 through a licensing agreement with the AAMC. Data were de-identified to protect both participating individuals and institutions. No additional questions were added for this analysis and survey questions were not altered for the purposes of this study.
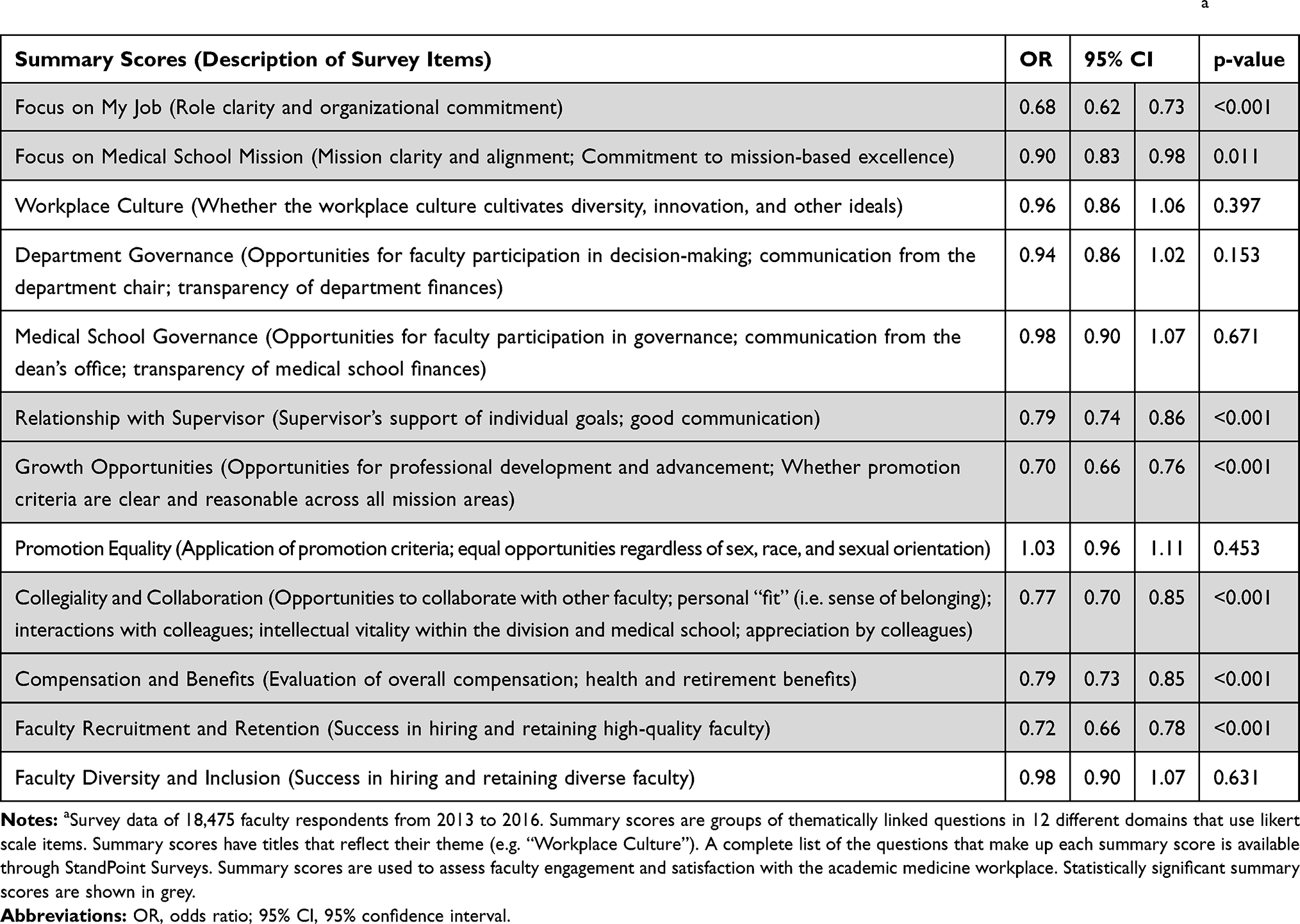 |
Table 1 Multivariable Robust Logistic Regression Models of Intent to Leave Based on StandPoint Survey Summary Scoresa |
Univariate multilevel and multivariable logistic regression models were performed based on the survey question: “Do you plan to leave this medical school in the next 1–2 years?” with response options of “Yes”, “I don’t know”, and “No”. Faculty answering “Yes” and “I don’t know” were combined to provide insight into the faculty “at-risk” of leaving. The “at-risk” faculty were compared to “control” faculty who responded “No” to the same question. Faculty were excluded if they intended to retire in the next 1–2 years, if they expressed an intention to leave academic medicine as a field, and if they were part-time.
To identify a clear profile of at-risk faculty, we examined survey data across all relevant demographic variables, including gender, race, age, department type, faculty rank, title beyond academic rank, years at their institution, promotion track, and receiving formal mentorship. Both summary scores and individual survey items were analyzed to understand if particular faculty perceptions of the workplace were associated with or predicted their expressing an intent to leave. Clustering effects between institutions and interactions between variables were also explored. All analyses were conducted using Stata Statistical Software, release 15. The American Institutes for Research, on behalf of the AAMC, approved this study.
Results
This study used data collected between 2013 and 2016, administered to 37,779 faculty with a 62.8% response rate representing 23,731 faculty at 36 United States Liaison Committee on Medical Education-accredited medical schools and representing a wide variety of geographic locations, faculty sizes, and research rankings.11 Overall, 18,475 faculty met inclusion criteria and provided an answer to the survey question, “Do you plan to leave this medical school in the next 1–2 years?” Approximately 30% (30.1%; n=5559) of faculty answered “yes” or “I don’t know” to this question, and were therefore considered as faculty “at-risk” of leaving their institution. When using univariate analyses to examine the demographics of “at risk” faculty, 31.0% of female faculty vs 29.4% of male faculty expressed an intent to leave (OR=1.08, 95% CI [1.02–1.16], p=0.019). At-risk faculty were likely to be at junior faculty (assistant professor) rank (OR=1.11, 95% CI [1.04–1.18], p=0.002), non-tenured (OR=1.05, 95% CI [0.97–1.12], p<0.001), and at their institutions for 6–15 years (OR=1.16, 95% CI [1.08–1.25], p<0.001) compared to shorter or longer duration as faculty at that institution. Faculty aged 46–65 were less likely to consider leaving, when compared to faculty 45 years of age and younger (OR=0.76, 95% CI [0.68–0.85], p<0.001). Further, having an administrative title (OR=0.72, 95% CI [0.68–0.77], p<0.001), and receiving formal mentorship (OR=0.65, 95% CI [0.61–0.70], p<0.001) reduced the odds of expressing and intent to leave by 28 and 35%, respectively (Figure 1). Race was not a significant factor in predicting intent to leave. (p=0.444)
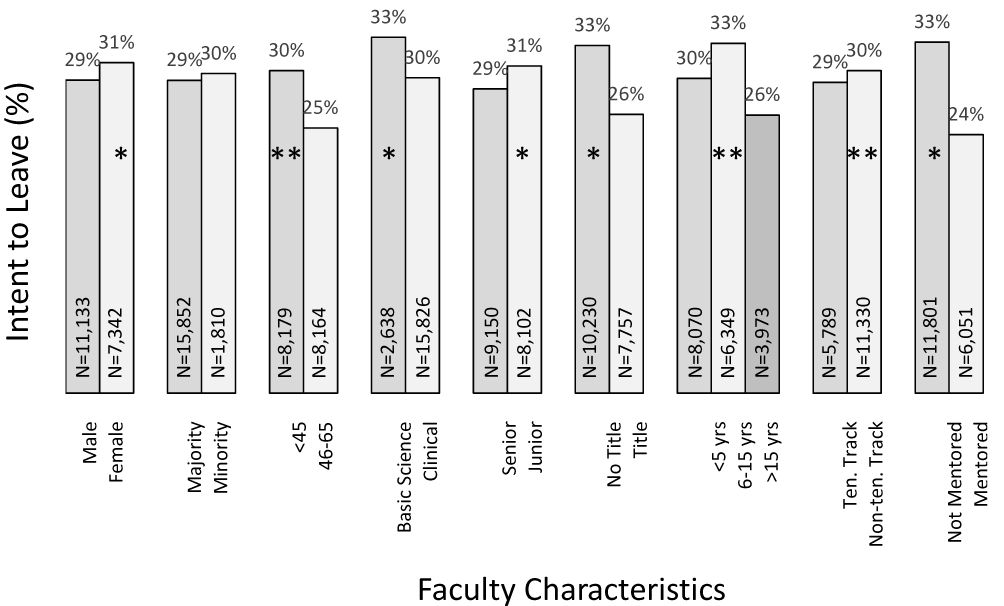 |
Figure 1 Univariate and multivariable robust logistic regression models of intent to leave based on faculty demographics. Proportion of faculty expressing an intent to leave based on their answer to the research question “Do you intend to leave this medical school in the next 1–2 years?” National StandPoint Faculty Engagement Survey data of 18,475 faculty respondents from 2013 to 2016. The symbol *indicates statistical significant difference in univariate multilevel analysis; **indicates statistical significant difference in multivariable robust logistic regression modeling (see text for details). Variables from left to right: gender, race (majority defined as Asian/White and minority defined as All Other Races/Ethnicities), age, department focus, faculty rank (Senior defined as full and associate professor and Junior as assistant professor), title beyond academic rank (defined as those who have an administrative title such as dean, chair, center director, course director, etc. or those without an administrative title), years at institution, tenure track, formal mentoring (defined as those with an identified formal mentor at their medical school or not). N = the total number of respondents per group. Not all respondents answered every question so totals for each characteristic vary slightly. |
In the multivariable logistic regression analyses, there were significant effect modifications between age and rank, age and promotion track, appointment duration and promotion track, and clinical role and promotion track (Figure 2). The regression model indicated that junior faculty between 46 and 65 years of age were less likely to leave than junior faculty ≤45 years (OR=0.70, 95% CI [0.54–0.91], p=0.008), whereas at the senior faculty rank, age had less effect on the intent to leave (Figure 2A). Similarly, non-tenure track faculty between ages of 46–65 were less likely to express an intent to leave than non-tenure track faculty ≤45 years (OR=0.73, 95% CI [0.58–0.91], p=0.005), whereas for tenure track faculty, age had a less pronounced effect (Figure 2B). While in univariate analyses non-tenure track faculty were more likely to express an intent to leave (Figure 1), when the length of appointment was paired with the tenure variable, one tenure track group stood out as being at high risk. Tenure track faculty who had been at their institution between 6 and 15 years were at higher risk than any other group of expressing an intent to leave (Figure 2C). Finally, faculty who did not provide clinical care (not active) and were not on a tenure track were more likely to express an intent to leave (OR=1.33, 95% CI [1.03–1.72], p=0.031) (Figure 2D).
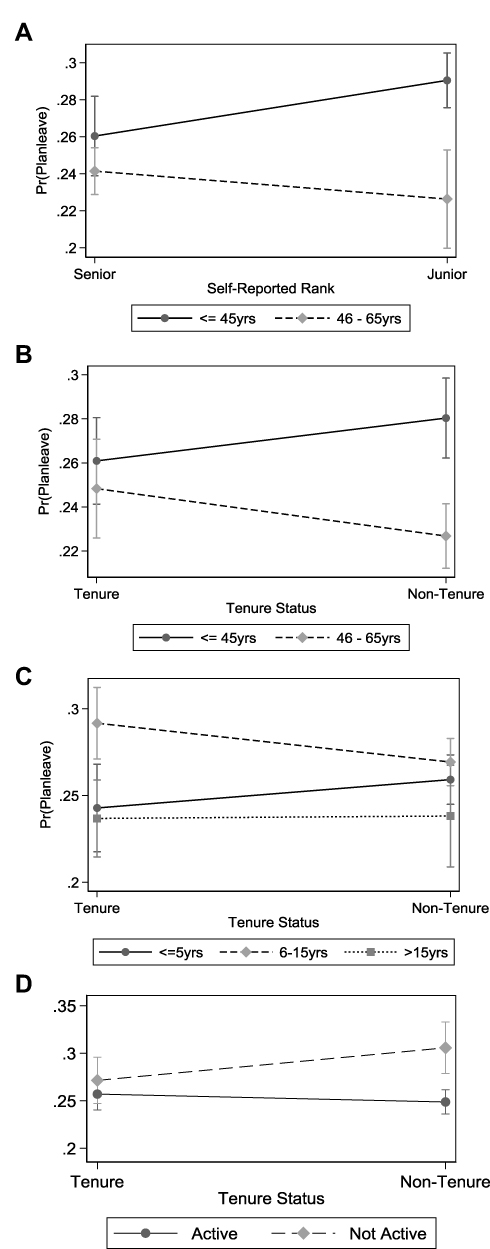 |
Figure 2 Interactions between variables in the multivariable logistic regression analyses were performed. There were significant effect modifications between: (A) age and rank, (B) age and promotion track, (C) appointment duration and promotion track, and (D) clinical role and promotion track. Pr(Planleave) means the probability of expressing an intent to leave. Bars indicate standard error. |
Based on multivariable regression models, faculty who expressed positive perceptions across seven of the survey’s summary score domains were less likely to express an intent to leave (grey rows in Table 1). Faculty agreeing with positively worded questions regarding the nature of their everyday job (OR=0.68, 95% CI [0.62–0.73]), medical school mission (OR=0.90, 95% CI [0.83–0.98]), relationships with their supervisors (OR=0.79, 95% CI [0.74–0.86]), professional development and career opportunities (OR=0.70, 95% CI [0.66–0.76]), compensation including benefits (OR=0.79, 95% CI [0.73–0.85]), their school and department’s ability to recruit and retain high quality faculty (OR=0.72, 95% CI [0.66–0.78]), and sense of collegiality within their department (OR=0.77, 95% CI [0.670–0.85]) were less likely to express an intent to leave. Results for summary scores are shown in Table 1; summary scores or aggregated data across thematically linked survey items, that were significant predictors of intent to leave are shown in grey.
When questions were individually analyzed, several themes emerged. The top 10 questions most closely associated with an intent to leave are listed in Table 2. In this table, odds ratios demonstrated the likelihood of expressing an intent to leave when respondents indicated that they “strongly disagreed” or “disagreed” with the statements. For example, respondents who disagreed with the statement that they were satisfied with their opportunities for professional development were approximately 7 times more likely to express an intent to leave. While not reported in this table, faculty who responded that they were “dissatisfied” or “strongly dissatisfied” with their medical school overall as a place to work were 11 times more likely to express intent to leave. This survey question is considered to be a highly important faculty engagement outcome variable that is provided to institutions when they request StandPoint Survey analyses. To summarize the logistic regression analyses, a profile of at-risk faculty, including personal characteristics and the top predictive questions, is shown in Figure 3.
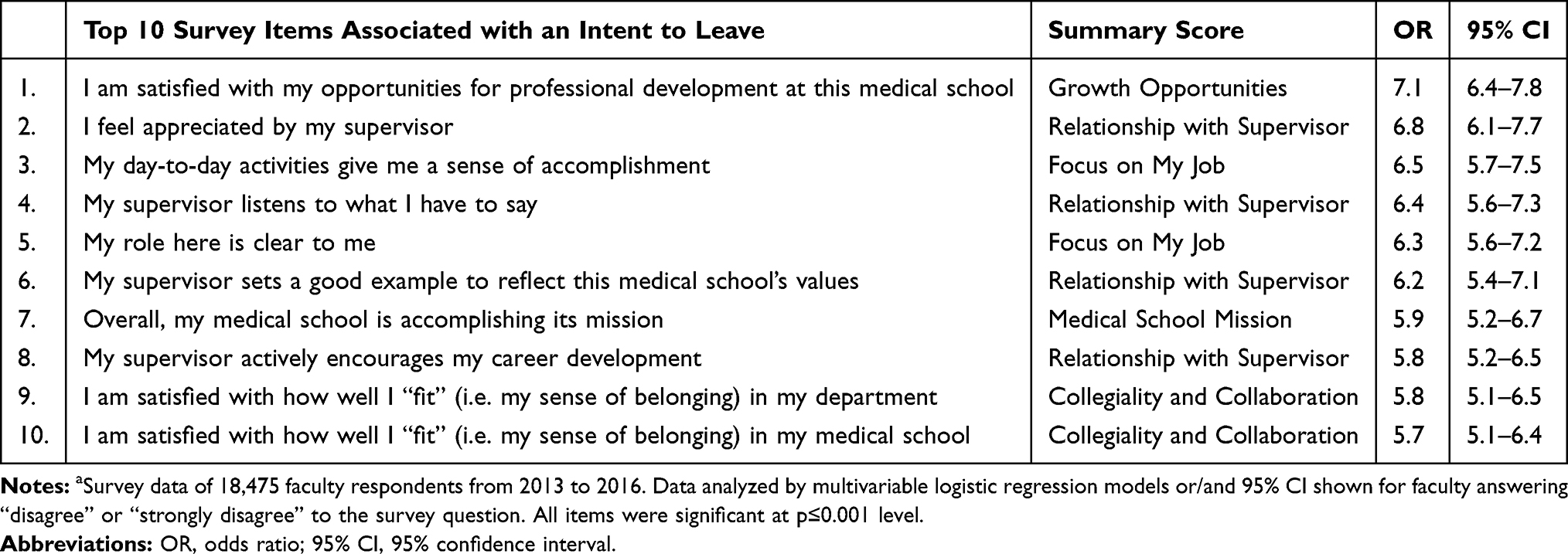 |
Table 2 Top 10 StandPoint Survey Items Associated with Expressing an Intent to Leave |
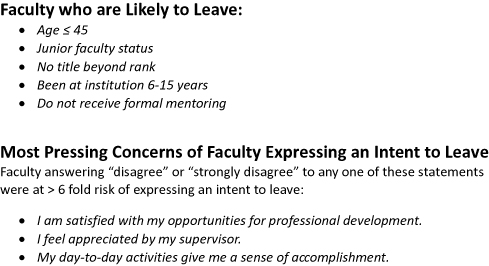 |
Figure 3 Summary of key study results from Figure 1 and Table 1. Our study suggests a profile of the faculty member most likely to express an intent to leave. The characteristics are shown. These “at-risk” faculty are far more likely than control faculty to disagree with the statements listed. ©2018 Association of American Medical Colleges. |
Results were also analyzed by the faculty department-type and whether or not faculty were actively engaged in clinical care activities. When faculty from clinical departments and basic science departments were analyzed separately, results were similar to those obtained for the entire cohort (Table 3). Unlike results from the entire cohort, when basic science faculty were considered separately, there was no difference between at-risk and control faculty regarding compensation and benefits and relationship with one’s supervisor. Summary scores associated with an intent to leave were also similar when faculty performing clinical vs non-clinical work were analyzed, irrespective of their department (Table 3). Non-clinical faculty in a clinical department (eg basic scientists in a department of internal medicine or surgery) also demonstrated similar results (Table 3). Lastly, in conducting all regression analyses, the potential for differences between institutions was assessed. Clustering effects between institutions revealed no significant findings.
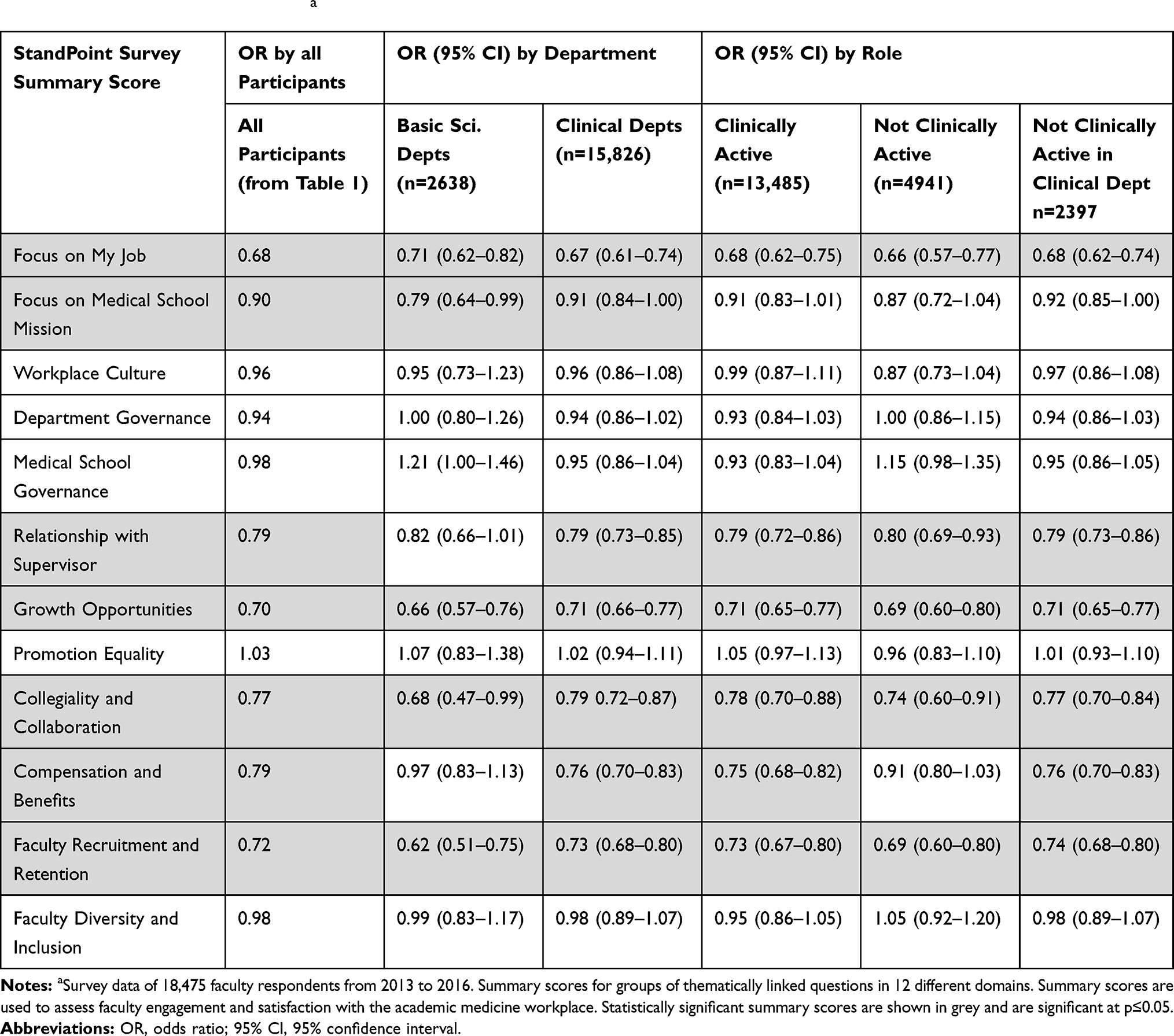 |
Table 3 Multivariable Logistic Regression Models of Intent to Leave Based on StandPoint Survey Summary Scores Evaluated by Department Type and Faculty Rolea |
Discussion
Retaining valued faculty once they have expressed an intent to leave is challenging for institutional leadership.2–4,9,10 We have observed that faculty often declare their intent to leave after it is a “done deal”, leaving the home institution scrambling to put together retention packages that are expensive and often unsuccessful. This study used a large, nationally representative database to demonstrate a profile of faculty who are most likely to express an intent to leave (Figure 3). This profile can inform departmental leadership about faculty at-risk of leaving, providing an opportunity for discussions and interventions before the faculty member finalizes his/her plans. This study also identifies key attitudes that are more common to faculty expressing an intent to leave than in faculty not intending to leave. These attitudes highlight concerns about opportunities, supervisory relationships, and satisfaction with day-to-day activities. Leaders who address these concerns may improve faculty retention and provide a more engaging academic workplace climate that may prevent faculty from “looking”.
Faculty expressing an intent to leave had an identifiable profile (Figure 3). At-risk faculty were likely to be <45 years of age and at junior faculty (assistant professor) rank. They were likely to be at their institutions for 6–15 years compared with faculty at the institution for shorter or longer time-periods. Younger faculty were more likely to express an intent to leave regardless of rank or promotion tract (Figure 2A and B). Further, at high risk of expressing an intent to leave were tenure track faculty at the institution 6–15 years (Figure 2C). This is somewhat expected and likely represents the uncertainty associated with nearing promotion for faculty on the tenure track.
Faculty who participate in self-defined formal mentorship were less likely to express an intent to leave. The importance of mentorship has been demonstrated in several recent studies and has been linked to faculty satisfaction, vitality, climate, and productivity.15–17 Mentorship is widely regarded as a key component in retention of faculty at academic medical centers.18,19 Despite the known value of mentoring, StandPoint Surveys reports that only 30% of faculty are engaged in formal mentorship.20 In addition to mentorship, our data are consistent with prior work demonstrating that having an administrative title beyond academic rank is protective of expressing an intent to leave.8 Leadership appointments may anchor faculty at an institution in a way that protects them from “looking”. Our data support the idea that after several years as an assistant professor, faculty with continued formal mentorship who are provided added responsibilities have more positive feelings about their future at their institution. Not unique to academic medicine, continued support along with added responsibility is common themes contributing to successful common life transitions such as from adolescence to adulthood18 Division chiefs, department chairs, and faculty development leaders play important roles in the successful transition of faculty from junior to senior faculty status. Our data suggest that proactive programs aimed at this important transition could improve faculty retention.
Several summary scores contained questions that were associated with the intent to leave. As a reminder, summary scores are thematically linked sets of 3–5 survey items dealing with topics relevant to faculty life. The summary scores and results of multivariable logistic regression shown in Tables 1 and 3 demonstrate that the nature of one’s everyday work, opportunities for growth, relationship with one’s supervisor, among other factors, are highly associated with expressing an intent to leave. These concerns are not unique to medicine or academic life. They are considered key facets of talent retention strategies across industries.22–24 When the top 10 survey items associated with an intent to leave were examined, key themes emerged. Major concerns regarding career development opportunities, relationships with supervisors, and day-to-day feeling of accomplishment were more common in faculty expressing an intent to leave. While the summary score for faculty compensation was significantly different between at-risk and control faculty (Table 1), the individual questions on compensation were not in the top 10 most predictive survey items.
The most important issues associated with an intent to leave that were identified in our study are similar to concerns highlighted in studies of faculty burnout.25–28 The consequences of faculty burnout are critically important and include medical errors, limited productivity or personal tragedy. This study may suggest that institutional efforts to decrease faculty burnout and create/foster a climate of wellness and engagement may also change faculty attitudes about leaving an institution.
It was particularly striking that all four survey items within the “Relationship with Supervisor” summary score were included in the top 10 list of predictive survey items. This is the only summary score achieving 100% inclusion of questions in the top 10. The strength of the relationship between employee and supervisor is also seen as key to talent retention in other industries.19–21 Characteristics of healthy relationships between faculty and their supervisors include modeling institutional values, demonstrating appreciation for, and actively listening to faculty, and supporting their career development. By recruiting division and department leaders who manifest excellent interpersonal skills, rather than focusing on a candidate’s research accomplishments, financial acumen, and pedigree, institutions may be able to improve faculty retention.
Perhaps more surprising than what topics were included in the top 10 list are the concerns that did not make the list: satisfaction regarding compensation, governance, and workplace culture. These concerns, while important to faculty, did not distinguish faculty who are considering leaving the institution. Compensation concerns were significantly important to faculty, particularly clinical faculty who expressed an intent to leave, but did not make the top list of contributing factors. Institutional practices of responding to the intent to leave with packages that include increased compensation may be missing the most pressing underlying issues.
Data from StandPoint Surveys, previously known as Faculty Forward, have been used in other studies to explore the link between faculty engagement and retention. Pollart et al studied clinical faculty and examined the relationship between clinical faculty members’ self-reported time in each core mission area.8 They determined that it was the satisfaction with the time spent, and not the amount of time, that determined an intent to leave. They felt this may represent an inappropriate distribution of time in the patient care and educational mission areas.8 These findings are consistent with our study’s finding about the importance of role clarity and a sense of daily accomplishment. Our data would support an ongoing dialogue between supervisors and faculty about their faculty’s responsibilities at the institution, allocation of effort, and satisfaction with their day-to-day work.
While women were statistically more likely to express an intent to leave than men, women were not included in the at-risk faculty profile for several reasons. The margin of women expressing an intent to leave was very small. In addition, we feel that the reasons women leave an institution are more complex than can be captured from the questions posed in this survey and require a survey or qualitative interviews that are dedicated to addressing women’s concerns.5 We were therefore reluctant to draw conclusions based on inadequate inquiry. We feel that what drives women to leave an institution requires a more specific, dedicated study; our study addresses attitudes that are gender independent.
In this study, basic scientists were slightly more likely to express an intent to leave than clinical faculty (Figure 1). In addition, non-clinically active faculty in a non-tenure track position had the highest proportion of faculty expressing an intent to leave of any group. Note should be made that our cohort had far more clinical faculty than basic science faculty (Clinical Department faculty n=15,826; Basic Science Department faculty n=2,638). Nevertheless, the difference in the proportion of faculty expressing an intent to leave is statistically significant. Basic science faculty reported less concern than their clinical peers about compensation and benefits (Table 3), indicating that other concerns are more important determinants of their intent to leave. This study is unable to adequately assess the complicated issues surrounding basic scientists’ attitudes about their jobs and career development; additional research in this area is needed.
Based on our findings, several common-sense approaches could be instituted that may change outcomes (Figure 4). Our data support prior studies demonstrating that junior faculty should receive formal mentorship from an early stage.15–19 In addition, faculty should have opportunities for career-enhancing activities at their institution or as offered by their professional societies. A robust annual review process for each faculty is a good way to provide performance feedback, recognize achievements, and prepare career development priorities for the upcoming year. Institutions should actively work to minimizing day-to-day faculty frustrations to provide a satisfying environment that promotes wellness and a sense of accomplishment. Given how important faculty relationships with their supervisor emerged to be in our study, we suggest that supervisors including chiefs and chairs be chosen to have well-developed interpersonal skills such as active listening, positive role modeling, and demonstrating appreciation and recognition when appropriate. These qualities are not easily identified by search committees or obvious on a curriculum vitae and require a deeper dive into relationships, attitudes, and priorities through methods such as behavioral interviewing. Based on our data, it is possible to administratively alert chairs when faculty fit the profile we defined in our study (Figure 3) and then act to proactively mitigate attrition. However, it is better if these actions are ongoing and part of a faculty development strategy rather than a reaction to an expressed intent to leave or fulfilling a characteristic profile.
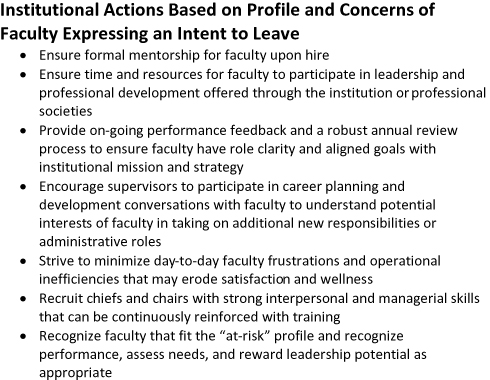 |
Figure 4 Suggested proactive institutional approaches to improving faculty retention that are based on our study findings. Our study identified a profile of the faculty member most likely to express an intent to leave and highlights the concerns that distinguish faculty expressing an intent to leave from those who planned to remain at their institution for the next 1-2 years. Study findings are presented in Figure 1 and Table 1. |
This study has several limitations. Most importantly, it cannot be determined if the faculty who expressed an intent to leave followed through with their intention. Additionally, the survey does not directly provide insight into the basis for their intent. We cannot assign a causal role to the differences in attitudes expressed in the survey between at-risk and control faculty. It is possible that other workplace frustrations or personal factors, such as a spouse taking a new job, contribute to their intentions. Clearly, perceptional and outcomes data on retention would strengthen our conclusions. Further, qualitative data from exit interviews or focus groups could provide deeper insights into retention trends. However, the large number of responses within the Standpoint Surveys dataset is a strength of this study and reinforces the associations identified.
Conclusion
Using a large, nationally representative cohort, this study identified the characteristics and attitudes of medical school faculty who are at risk of leaving their institutions. Faculty expressing an intent to leave were <45 years old, at a junior faculty rank, and likely to be at their institutions between 6 and 15 years. Faculty having an administrative title and formal mentorship were less likely to express the intent to leave. Top concerns of at-risk faculty relate to supervisory relationships and growth opportunities rather than compensation or governance. Based on this study, institutional leaders have new information to develop a proactive strategy for retaining valued faculty and lessen financial and human costs of faculty departures.
Abbreviations
AAMC, Association of American Medical Colleges; OR, odds ratio; Robust SE, robust standard error; 95% CI, 95% confidence interval; ELAM, Executive Leadership in Academic Medicine.
Ethical Approval
The American Institutes for Research, on behalf of the AAMC, approved this study.
Acknowledgements
The corresponding author wishes to acknowledge the Hedwig van Ameringen Executive Leadership in Academic Medicine (ELAM) Program for Women. This study represents Dr. Zimmermann’s ELAM institutional action project. Dr. Zimmermann’s ELAM Learning Community, ELAM of the South (EOS) and Dr. Darshana Shaw, provided inspiration and encouragement during the design and performance of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dorsey RE, Van Wuyckhuyse BC, Beck CA, Passalacqua WP, Guzick DS. The economics of new faculty hires in basic science. Acad Med. 2009;84:26–31. doi:10.1097/ACM.0b013e3181904633
2. Satiani B, Williams TE, Brod H, Way DP, Ellison EC. A review of trends in attrition rates for surgical faculty: a case for a sustainable retention strategy to cope with demographic and economic realities. J Am Coll Surg. 2013;216:944–953. doi:10.1016/j.jamcollsurg.2012.12.052
3. Lowenstein SR, Fernandez G, Crane LA. Medical school faculty discontent: prevalence and predictors of intent to leave academic careers. BMC Med Educ. 2007;7:37. doi:10.1186/1472-6920-7-37
4. Durso SC, Christmas C, Kravet SJ, Parsons G, Wright SM. Implications of academic medicine’s failure to recognize clinical excellence. Clin Med Res. 2009;7:127–133. doi:10.3121/cmr.2009.856
5. Westring AF, Speck RM, Dupuis Sammel M, et al. Culture matters: the pivotal role of culture for women’s careers in academic medicine. Acad Med. 2014;89:658–663. doi:10.1097/ACM.0000000000000173
6. Dewa CS, Loong D, Bonato S, Thanh NX, Jacobs P. How does burnout affect physician productivity? A systematic literature review. BMC Health Serv Res. 2014;14:325–335. doi:10.1186/1472-6963-14-325
7. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283:516–529. doi:10.1111/joim.2018.283.issue-6
8. Pollart SM, Novielli KD, Brubaker L, et al. Time well spent: the association between time and effort allocation and intent to leave among clinical faculty. Acad Med. 2015;90:365–371. doi:10.1097/ACM.0000000000000458
9. Pololi LH, Krupat E, Civian JT, Ash AS, Brennan RT. Why are a quarter of faculty considering leaving academic medicine? A study of their perceptions of institutional culture and intentions to leave at 26 representative U.S. medical schools. Acad Med. 2012;87:859–869. doi:10.1097/ACM.0b013e3182582b18
10. Schloss EP, Flanagan DM, Culler CL, Wright AL. Some hidden costs of faculty turnover in clinical departments in one academic medical center. Acad Med. 2009;84:32–36. doi:10.1097/ACM.0b013e3181906dff
11. Dandar VM, Field JP, Garrison GF. Promising Practices for Promoting Faculty Engagement and Retention at US Medical Schools.
12. Bunton SA, Corrice AM, Pollart SM, et al. Predictors of workplace satisfaction for U.S. medical school faculty in an era of change and challenge. Acad Med. 2012;87:574–581. doi:10.1097/ACM.0b013e31824d2b37
13. Wai PY, Dandar V, Radosevich DM, Brubaker L, Kuo PC. Engagement, workplace satisfaction, and retention of surgical specialists in academic medicine in the United States. J Am Coll Surg. 2014;219:31–42. doi:10.1016/j.jamcollsurg.2014.03.027
14. Brubaker L, Wagner S, Novielli KD, et al. Challenges in academic obstetrics and gynecology departments. Obstet Gynecol. 2013;122:1092–1099. doi:10.1097/AOG.0b013e3182a9c24f
15. Mylona E, Brubaker L, Williams VN, et al. Does formal mentoring for faculty members matter? A survey of clinical faculty members. Med Educ. 2016;50:670–681. doi:10.1111/medu.2016.50.issue-6
16. Spence JP, Buddenbaum JL, Bice PJ, Welch JL, Carroll AE. Independent investigator incubator (I3): a comprehensive mentorship program to jumpstart productive research careers for junior faculty. BMC Med Educ. 2018;18:186. doi:10.1186/s12909-018-1290-3
17. Walensky RP, Kim Y, Chang Y, et al. The impact of active mentorship: results from a survey of faculty in the Department of Medicine at Massachusetts General Hospital. BMC Med Educ. 2018;18:108. doi:10.1186/s12909-018-1191-5
18. Geraci SA, Thigpen SC. A review of mentoring in academic medicine. Am J Med Sci. 2017;353:151–157. doi:10.1016/j.amjms.2016.12.002
19. DeCastro R, Sambuco D, Ubel PA, Stewart A, Jagsi R. Mentor networks in academic medicine: moving beyond a dyadic conception of mentoring for junior faculty researchers. Acad Med. 2013;88:488–496. doi:10.1097/ACM.0b013e318285d302
20. Byington CL, Keenan H, Phillips JD, et al. A matrix mentoring model that effectively supports clinical and translational scientists and increases inclusion in biomedical research: lessons from the university of Utah. Acad Med. 2016;91:497–502. doi:10.1097/ACM.0000000000001021
21. Lee TK, Wickrama KAS, O’Neal CW, Prado G. Identifying diverse life transition patterns from adolescence to young adulthood: the influence of early socioeconomic context. Soc Sci Res. 2018;70:212–228. doi:10.1016/j.ssresearch.2017.12.001
22. Martin J, Schmidt T How to keep your top talent. Harvard Business Review 2010 May. Available from: https://hbr.org/2010/05/how-to-keep-your-top-talent.
23. Olenski S. 7 Tips to better employee retention. Forbes. March 3, 2018. Available from: https://www.forbes.com/sites/steveolenski/2015/03/03/7-tips-to-better-employee-retention/#3b1976bb452b.
24. Caramela S. How to improve millennial employee retention. Business.com. April 27, 2018. Available from: https://www.business.com/articles/improve-millennial-employee-retention/.
25. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251:995–1000. doi:10.1097/SLA.0b013e3181bfdab3
26. DeOliveira GS
27. Kuhn CM, Flanagan EM. Self-care as a professional imperative: physician burnout, depression, and suicide. Can J f Anesth. 2017;64:158–168. doi:10.1007/s12630-016-0781-0
28. Shanafelt TD, Noseworthy JH. Executive leadership and physician well-being: nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92:129–146. doi:10.1016/j.mayocp.2016.10.004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.