")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Characteristics, Management and In-Hospital Clinical Outcomes Among Inpatients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease in China: Results from the Phase I Data of ACURE Study
Authors Liang C, Mao X, Niu H, Huang K , Dong F , Chen Y, Huang K, Zhan Q, Huang Y, Zhang Y, Yang T , Wang C
Received 14 September 2020
Accepted for publication 7 January 2021
Published 25 February 2021 Volume 2021:16 Pages 451—465
DOI https://doi.org/10.2147/COPD.S281957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Chen Liang,1 Xihua Mao,1 Hongtao Niu,2– 4 Ke Huang,2– 4 Fen Dong,2– 5 Yahong Chen,6 Kewu Huang,7,8 Qingyuan Zhan,2– 4 Yin Huang,1 Yaowen Zhang,1 Ting Yang,2– 4 Chen Wang2– 4,9
1Chinese Alliance for Respiratory Diseases in Primary Care, Beijing, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3National Clinical Research Center for Respiratory Diseases, Beijing, People’s Republic of China; 4Institute of Respiratory Medicine, Chinese Academy of Medical Science, Beijing, People’s Republic of China; 5Institute of Clinical Medical Sciences, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 6Department of Pulmonary and Critical Care Medicine, Peking University Third Hospital, Beijing, People’s Republic of China; 7Department of Pulmonary and Critical Care Medicine, Beijing Chao-Yang Hospital, Beijing, People’s Republic of China; 8Department of Respiratory Medicine, Capital Medical University, Beijing, People’s Republic of China; 9Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Ting Yang
Department of Pulmonary and Critical Care Medicine, China-Japan Friendship Hospital, No. 2, East Yinghua Road, Chaoyang District, Beijing, 100029, People’s Republic of China
Email [email protected]
Chen Wang
Chinese Academy of Medical Sciences and Peking Union Medical College, 9 Dongdan 3rd Alley, Dong Dan, Dongcheng, Beijing, 100730, People’s Republic of China
Email [email protected]
Purpose: The study aimed to give a comprehensive overview of characteristics and evaluate in-hospital clinical outcomes among hospitalized acute exacerbation of chronic obstructive pulmonary disease (AECOPD) patients in China using data from the AECOPD inpatient registry (ACURE).
Patients and Methods: The ACURE is an ongoing, national, multicenter, observational registry. Participants enrolled during phase I stage (1st September 2017 to 25th February 2020) of ACURE with confirmed AECOPD diagnoses were studied. Descriptive analyses were conducted to describe features and occurrences of in-hospital clinical outcomes of AECOPD inpatients in real-world China.
Results: A total of 5334 AECOPD inpatients from 163 sites in 28 provinces or province-level municipalities were included. Among all participants, 78.8% were males and the median age was 69.0 [interquartile range (IQR): 63.0– 76.0] years. The proportions of current and former smokers were 23.6% and 44.2%, respectively. The median age at COPD diagnosis was 64.0 (IQR: 57.0– 71.0) years and 88.7% participants demonstrated at least one comorbidity. During stable period, only 56.9% subjects received pharmacological therapies and the influenza vaccination rate was 2.9%. During hospitalization, 99.5% subjects received pharmacological treatments and antibiotics were prescribed to 90.9% participants. The all-cause in-hospital mortality was 0.1% and no significant difference was found across hospital categories.
Conclusion: Clinical features of Chinese AECOPD inpatients were different from those of other populations. In real-world China, the clinical management during stable period was unsatisfied, whereas therapy during hospitalization was effective regarding in-hospital clinical outcomes regardless of hospital category.
Keywords: registries, demography, therapeutics, disease management, hospital mortality, public health
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by chronic and irreversible airflow limitation, which remains a significant global health problem due to its high prevalence and mortality.1 Although often underdiagnosed, it was estimated that 174.5 million adults had prevalent COPD and 3.2 million died from COPD worldwide in 2015.2 In China, the prevalence of COPD was 8.6%, corresponding to 99.9 million COPD patients aged 20 years or older in 2015.3 The economic burden imposed by COPD is also unignorable. Globally, COPD is predicted to be the 7th cause of disability-adjusted life years by 2030. In China, COPD has already become the 2nd cause of disability-adjusted life years among chronic diseases since 2001.4
Acute exacerbation of COPD (AECOPD) has been defined as events characterized by deterioration of respiratory symptoms leading to change in regular treatment.5 These events are common among COPD patients and have placed substantial burden on patients, health services and society. AECOPD is the major cause of hospitalization among all COPD patients.6 Hospitalization discharge accounted for over 70% of COPD-related medical expenditures in the United States (US).7 In China, the indirect burden is even heavier considering the premature mortality and productivity losses of patients and their family members.4 Acute exacerbations deteriorate patients’ physical functions and have profound negative effects on their quality of life.8,9 Among some patients, recovery may not be achieved in a short period of time or forever, which could prevent them back to workplace.10 As reported by Seemungal et al,11 about 7% of AECOPD patients could not recover to their pre-exacerbation pulmonary function levels within 3 months.
Due to the considerable burden of AECOPD, thoroughly understanding of the characteristics and clinical outcomes of AECOPD patients is required to help optimize clinical management and improve their prognosis. There were a few studies exploring characteristics, healthcare resource usages and clinical outcomes among AECOPD patients.12–17 However, results varied across countries. To our knowledge, there is still a lack of studies on this topic in China with large sample sizes in real-world setting. This study aimed to give a comprehensive overview of characteristics and evaluate in-hospital clinical outcomes among patients hospitalized with AECOPD in real-world China using data from the AECOPD inpatient registry (ACURE).
Patients and Methods
Study Design and Participants
The ACURE is an ongoing, national, multicenter, observational registry designed to describe the characteristics and explore the prognosis and clinical management of hospitalized AECOPD patients in real-world setting (ClinicalTrials.gov identifier: NCT02657525). It started from 1st September 2017 and planned to recruit 7600 in-hospital AECOPD patients with a 3-year follow-up. Study sites could be classified as tertiary general, tertiary traditional Chinese medicine (TCM), secondary general and secondary TCM hospitals according to the 3-tier system and hospital types.18 The phase I data collection ended on 25th February 2020. Participants underwent screenings at admission to confirm the eligibility for enrollment. The eligibility criteria have been described elsewhere.19
The protocol of ACURE19 has been approved by the ethics committee of China-Japan Friendship Hospital (approval number: 2015-88). The ACURE was conducted in accordance with the Declaration of Helsinki. All participants have signed the informed consent before enrollment.
Procedures and Measurements
At admission, each eligible subject was given an in-depth interview to collect the demographics, smoking history, medical history, management of disease during stable period, etc. Physical examinations were also conducted. Demographics included age, sex, education level, and body mass index, which was transformed from the height and weight measurements. Regarding smoking history, participants were characterized as current-, former- or non-smokers. Smoking beginning age, smoking cessation age (if former smokers), tobacco type and the amount of smoking per unit time were collected for current and former smokers. The amount of smoking per unit time for various tobacco types was standardized to the number of cigarettes (one cigarette was equivalent to one gram of tobacco or half of a cigar).20 Then, the intensity of cigarette smoking (pack-year) was derived from the number of cigarettes smoked per day and the smoking duration. Medical history including hospitalization and emergency room visiting due to AECOPD in the past year were asked for each subject. Respiratory symptoms in the past month were assessed using the COPD assessment test (CAT), which is an 8-item questionnaire used to measure the impact of respiratory disease on patients’ health status. The score of CAT ranges from 0 to 40, with 0 indicating the best health status while 40 as the worst.21 And the minimum clinically important difference of CAT was 2 points.22
During hospitalization, treatment and auxiliary examination results including laboratory and lung function tests were recorded if available. Corticosteroids were further classified as inhaled corticosteroids (ICS) and systemic ones according to the administration route. Systemic corticosteroids were defined as corticosteroids administered orally or by injection and distributed through the whole body.23 The daily and total dosage of systemic corticosteroids were also analyzed (standardized to the dosage of prednisone).24 All auxiliary examinations were conducted in local sites and the results were uploaded to the database by investigators. If laboratory data were unavailable during hospitalization, the most recent results within 3 days before admission were used for imputation. If multiple tests were conducted after admission, the earliest one was used. While for lung function test, the data were all derived in stable state and we chose the latest result for analysis if multiple tests were available before discharge. If no data available before admission and during hospitalization, the last result within 30 days after discharge was used. To ensure the quality and uniformity of spirometry data, training on performing spirometry was provided to each study site by professional doctors from central site. Severity of airflow limitation was classified into four grades based on the 2017 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report: GOLD 1 [forced expiratory volume in one second (FEV1)% predicted≥80], GOLD 2 (50≤FEV1% predicted<80), GOLD 3 (30≤FEV1% predicted<50) and GOLD 4 (FEV1% predicted<30).5
At discharge, physicians recorded the discharge diagnoses and clinical outcomes including death, intensive care unit admission, CAT score and total direct cost for each participant. The discharge diagnosis of AECOPD was made by physicians based on subjects’ signs and symptoms, family and medical histories (eg, previous diagnoses of COPD), irritant exposures, and former or in-hospital tests including lung function tests and chest imaging.19,25 The previous diagnoses of COPD were made by physicians according to the GOLD lung function criteria.5 Comorbidities were defined as diseases other than AECOPD based on discharge diagnoses and were further classified as pulmonary and extrapulmonary ones according to the affected systems. Total direct costs were transformed to US dollars using the average exchange rate in 2019 (one US dollar was equivalent to 6.90 yuan) because most subjects were enrolled in this year.
Statistical Analysis
For continuous variables, mean and standard deviation were described for data with normal distribution, while median and interquartile range (IQR) were used to depict skewed data. For categorical variables, frequencies and percentages were demonstrated. For group comparisons, analysis of variance was used for normal distributed variables, Kruskal-Wallis test was applied for skewed variables, while Pearson’s chi-squared test or Fisher’s exact test were conducted for categorical variables. Bonferroni correction was used to adjust for multiple comparisons.
Statistical significance was defined as achieving a two-sided P-value of less than 0.05. All statistical analyses were performed by Stata version 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Results
During the phase I stage of the ACURE, a total of 5334 AECOPD inpatients were enrolled out of 6335 subjects underwent screening for eligibility. The flow chart of obtaining the study population is shown in Figure 1. They were from 163 sites in 28 provinces or province-level municipalities around China. And all of the seven geographical areas in China were covered.
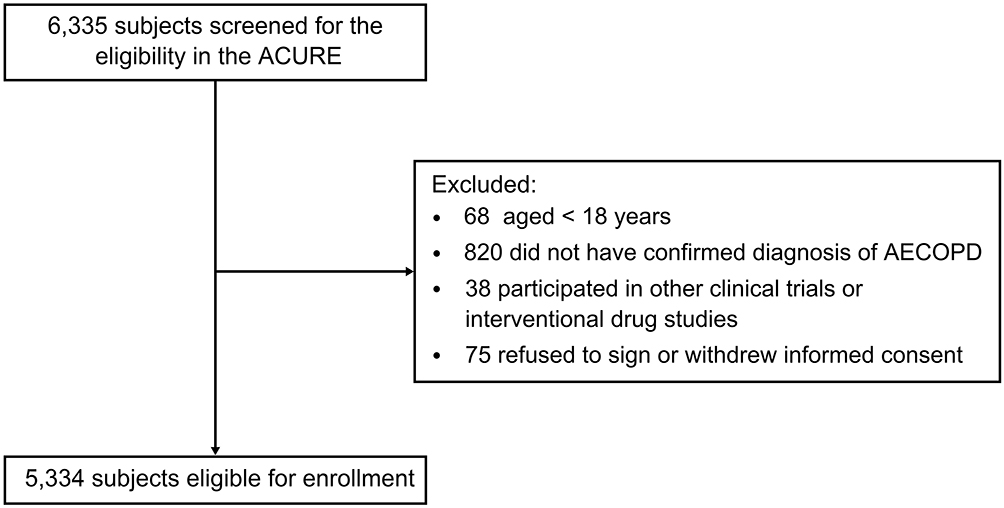 |
Figure 1 Flow Chart of Obtaining the Study Population. Abbreviations: ACURE, acute exacerbation of chronic obstructive pulmonary disease inpatient registry; AECOPD, acute exacerbation of chronic obstructive pulmonary disease. |
Demographics and Smoking History
Among the 5334 subjects, 4010 (75.2%) were from tertiary general hospital, 698 (13.1%) were from tertiary TCM hospital, 612 (11.5%) were from secondary general hospital and the other 14 (0.3%) were from secondary TCM hospital. The demographics and smoking history of the study population were summarized both in total and by hospital category (Table 1). The subjects from secondary general and secondary TCM hospital were combined due to small sample sizes.
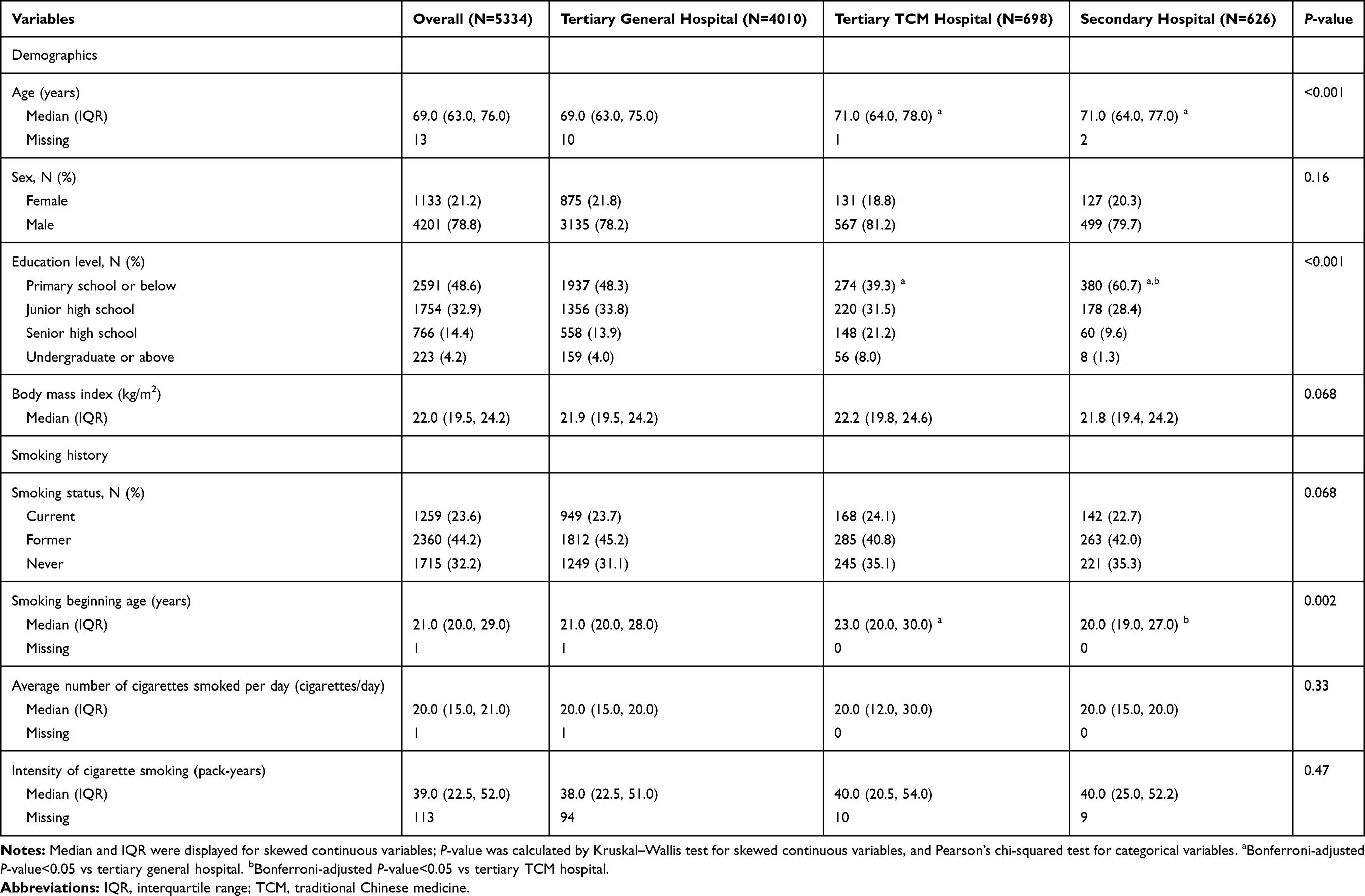 |
Table 1 Demographics and Smoking History at Admission of Study Population |
Among all participants, 78.8% were males and the median age was 69.0 (IQR: 63.0–76.0) years. Regarding smoking history, 23.6% (1259) subjects were current smokers, whereas 32.2% (1715) subjects were never-smokers. For the 3619 current or former smokers, they began smoking at a median age of 21.0 (IQR: 20.0–29.0) years and smoked 39.0 pack-years on average with a median consumption of 20.0 cigarettes per day.
Medical History and Laboratory Finding
The median age at COPD diagnosis was 64.0 (IQR: 57.0–71.0) years among all participants. In the past year before admission, 1549 (29.0%) subjects experienced two or more hospitalizations and 1295 (24.3%) subjects visited emergency rooms frequently (≥2 times) due to AECOPD. The CAT questionnaire was scored over 10 points by 90.5% participants in the recent month before admission. Among 3882 subjects with spirometry data, the majority of subjects were classified as GOLD 2, 3 and 4 stages (30.3%, 41.5% and 23.3%, respectively). Overall, 88.7% subjects demonstrated at least one comorbidity. Two thirds of in-hospital AECOPD patients were complicated with pulmonary comorbidities and 70.0% subjects reported extrapulmonary comorbidities (Table 2).
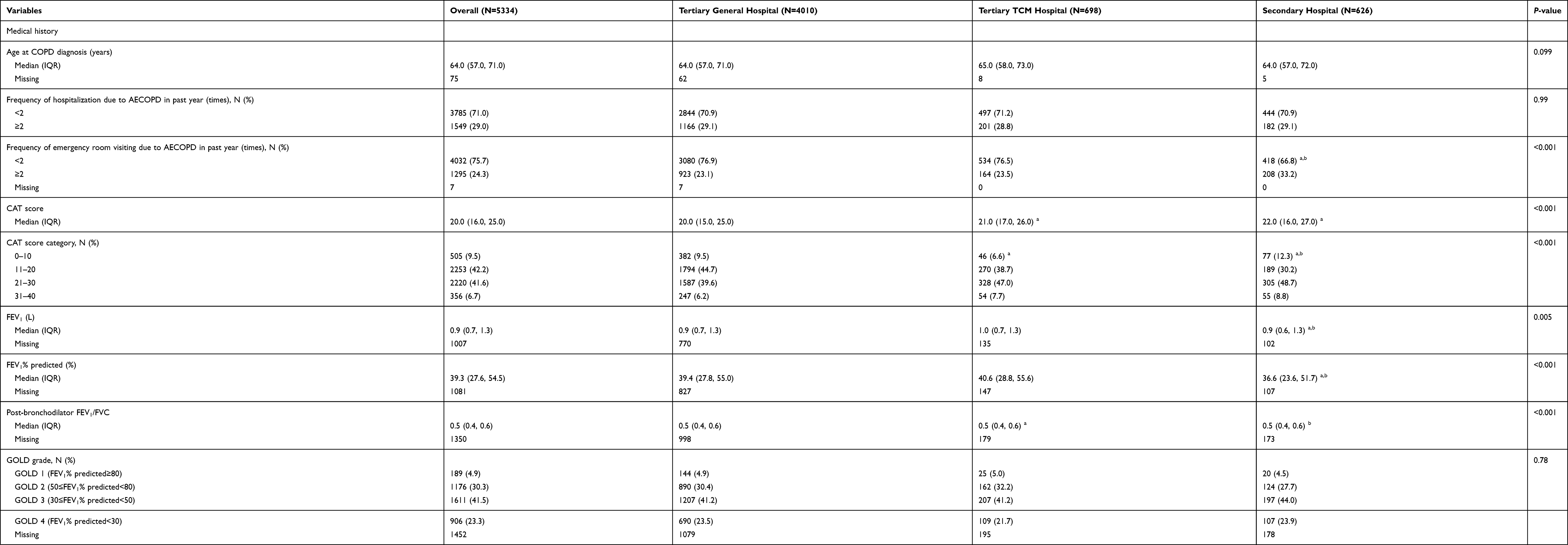 |
Table 2 Medical History and Laboratory Finding of Study Population |
Among the 3822 subjects with blood eosinophil count results at baseline, 17.4% had eosinophil over 300 cells per microliter blood, while 45.1% subjects had eosinophil below 100 cells per microliter blood. The distribution of blood eosinophil count was similar in all hospital categories. Among 2338 subjects with arterial blood gas results before receiving respiratory support, 18.9% had PaCO2≥50 mmHg and no clinical significance was found across hospital categories. Detailed information of laboratory finding is shown in Table 2.
Usage of Treatment
During stable period, 56.9% subjects received pharmacological treatments (Table 3). The combined inhalation therapy [long-acting beta2-agonist (LABA)/long-acting muscarinic antagonist (LAMA) or ICS/LABA/LAMA] was the most common one and was reported by 33.0% of subjects. Only 2.9% of participants had previously received influenza vaccine to prevent AECOPD.
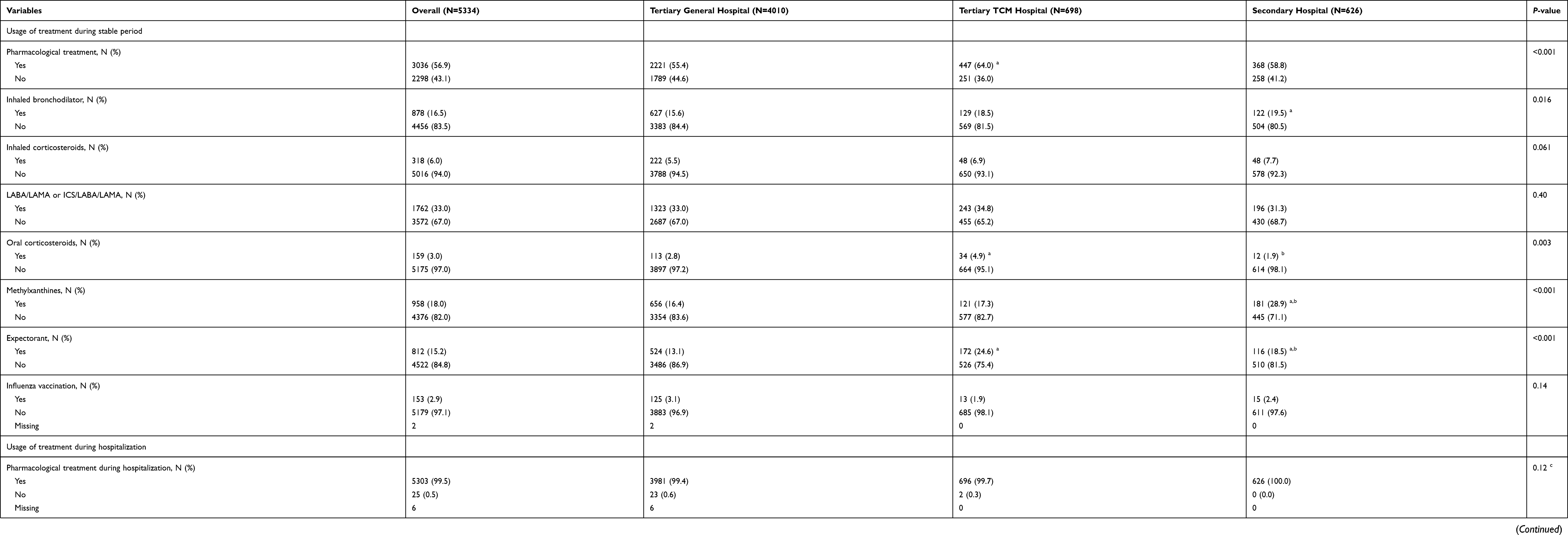 |
Table 3 Usage of Treatment During Stable Period and Hospitalization of Study Population |
During hospitalization, 99.5% subjects received pharmacological treatments. Overall, short-acting inhaled bronchodilator, corticosteroids, antibiotics and methylxanthines were given to 72.7%, 78.8%, 90.9% and 72.7% of subjects, respectively. The proportion of subjects using short-acting inhaled bronchodilator was the highest in secondary hospitals, whereas was the lowest in the tertiary TCM hospitals. Subjects in the tertiary general hospitals were more likely to use corticosteroids compared to those in the tertiary TCM (80.3% vs 72.3%) and secondary hospitals (80.3% vs 76.0%) (all P<0.05). The proportions of participants prescribed inhaled and systemic corticosteroids were 66.3% and 36.9%, respectively. Among participants receiving systemic corticosteroids, the median daily and total dosage of systemic corticosteroids were 50.0 (IQR: 50.0–50.0) mg and 266.7 (IQR: 175.0–400.0) mg, respectively. For respiratory support, 82.7% subjects received oxygen therapy (including conventional or high flow), noninvasive or invasive positive-pressure ventilation during hospitalization. A total of 4034 (75.6%) subjects took oxygen therapy as the highest level of respiratory support, whereas 6.8% and 0.3% required to take noninvasive and invasive positive-pressure ventilation, respectively. The proportion of subjects receiving respiratory support was the highest in tertiary general hospitals, whereas was the lowest in the tertiary TCM hospitals. Detailed treatment information is shown in Table 3.
In-Hospital Clinical Outcomes
The overall all-cause mortality during hospitalization was 0.1%, which corresponded to eight cases of death (Table 4). No significant difference was found across hospital categories. Among all participants, 2886 (54.3%) stayed in hospital for no longer than 10.0 days and the median total cost was 1424.3 (IQR: 1027.3–2013.0) US dollars. On average, subjects in tertiary TCM hospitals had the longest length of stays and heaviest total direct costs during hospitalization. In total, 83 (1.6%) subjects were admitted to intensive care unit. At discharge, CAT questionnaire was scored ≤20 points by 89.6% subjects. Compared with admission, the median change of CAT score was −7.0 (IQR: −12.0– −3.0) at discharge, which had already exceeded the minimum clinically important difference of the CAT. The decreases of CAT score were less significant among subjects in tertiary general hospitals as compared to those in tertiary TCM and secondary hospitals (medians: −7.0 vs −9.0, P<0.05).
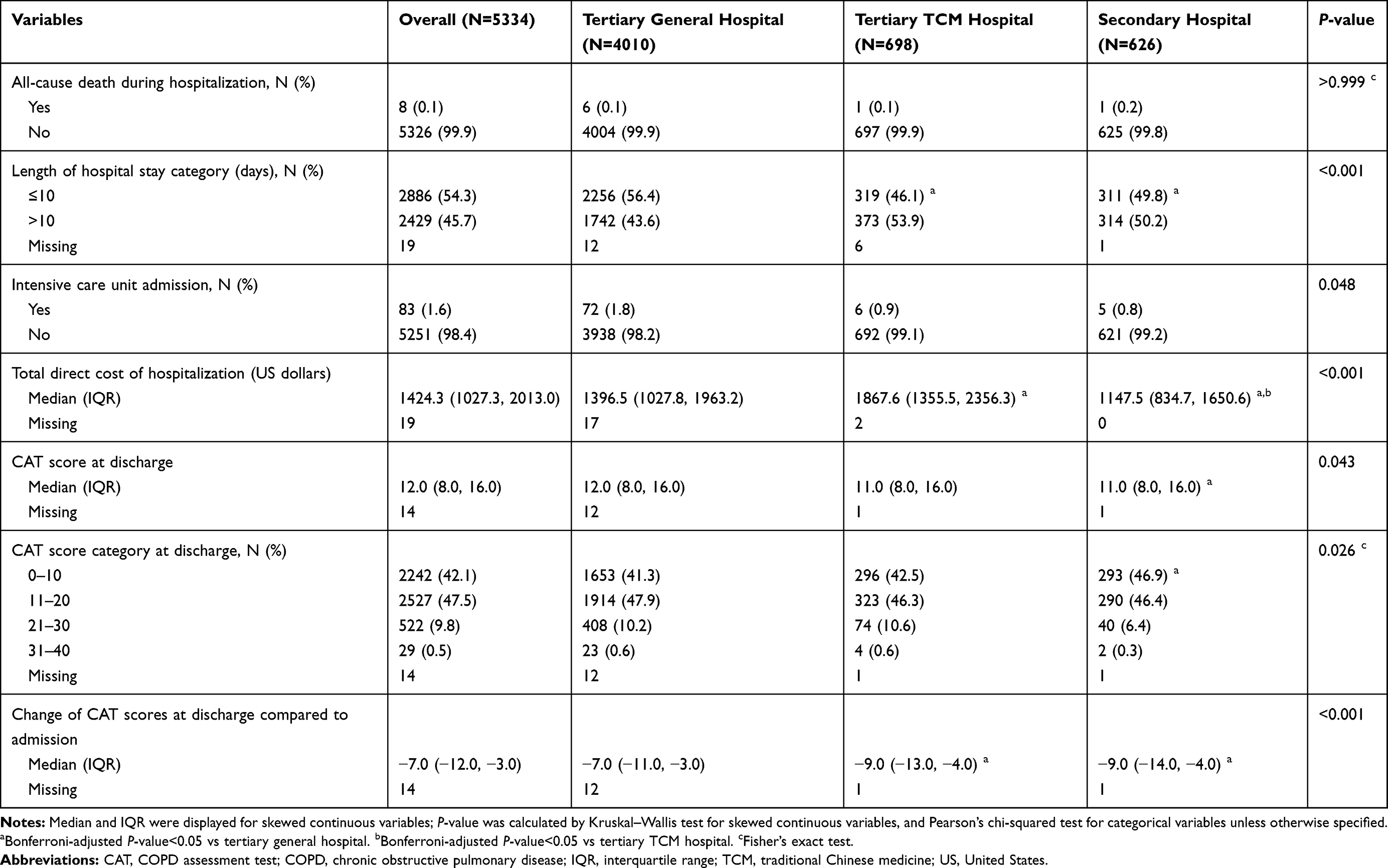 |
Table 4 In-Hospital Clinical Outcomes of Study Population |
Discussion
To our knowledge, this is the first and largest study to explore the characteristics and in-hospital clinical outcomes among Chinese hospitalized AECOPD patients in real-world setting. We found that some characteristics including smoking and medical history were different among Chinese AECOPD inpatients as compared to those from other countries. China is the largest nation of tobacco manufacturing and consumption. About 30% of tobacco are produced and consumed in China.26 Although the rate and amount of smoking among patients hospitalized with AECOPD were high, they were lower compared to those in some other countries (rate ranges: 82%–96%, average amount ranges: 40–56 pack-years).13,14,27,28 Smokers often demonstrate more severe symptoms, such as dyspnea and cough, than non-smokers.29 And the dose-response relationship between tobacco consumption and severity of COPD has been established worldwide.4,30,31 Therefore, we supposed that the clinical prognosis of Chinese AECOPD inpatients would be better, but still could be improved by conducting education of smoking cessation. The age at COPD diagnosis was relatively older in Chinese AECOPD patients as compared to those from other countries including Russia and India.28,32 It was most likely due to the delayed diagnosis of COPD in China. As reported by Zhong et al,33 only one third of subjects classified as GOLD 1 stage at screening had been diagnosed with respiratory diseases previously. Another study stated that Chinese patients used to visit physicians until symptoms were intolerable,4 which was consistent with our finding that over 90% subjects experienced moderate to very high level of impact on daily activities imposed by COPD in the past month before admission. More efforts should be put on spreading knowledge of COPD and reducing health-care disparities in order to achieve early diagnosis and timely treatment, which could ultimately improve patients’ clinical prognosis. The proportion of AECOPD inpatients with at least one comorbidity was higher in our study than that in Sweden,34 Russia,28 and Singapore.35 Comorbidities have found to cause increased hospitalizations, healthcare costs, and mortality.36 In addition, comorbidities also impose difficulties on therapy of COPD.1,37 Generally, the comorbidities should be treated according to usual standards regardless of COPD. However, excess attention should be paid to avoid polypharmacy and the interaction of different drugs should be taken into account when making the care plan for COPD patients with comorbidities.1
The clinical management during stable period was unsatisfied among COPD patients in China, and there was still a gap between current practice and guidelines including GOLD. For pharmacological treatment, all COPD patients were recommended to take at least one medication during stable period in order to alleviate symptoms and reduce the occurrence of adverse outcomes.1 However, only 56.9% of participants received pharmacological treatment in stable period before this admission. Economic status, delayed diagnosis, insufficient health education, and low compliance might contribute to this phenomenon. Unlike hospitalization, COPD has not been included in the scope of outpatient reimbursement for residents’ medical insurances in most areas.38 In China, COPD therapy was unaffordable for some previously diagnosed patients in stable periods. According to Fang et al,4 the cost for pharmacological treatment in stable periods (443–738 US dollars per year) is a huge economic burden for patients’ families and themselves, especially for those living in rural areas (the per capita disposable income in 2019: 2322 US dollars).39 Regarding vaccine, yearly influenza vaccination has been recommended by guidelines and World Health Organization with the evidence of having the ability of reducing acute exacerbations, all-cause mortality and economic burden among COPD patients.1,40,41 However, vaccine administration rate in our study was only 2.9%, which was greatly lower than that in other countries (ranges: 12%–75%).40,42–45 This could be attributable to the sparse knowledge of vaccination acquired by Chinese COPD patients and the fact that influenza vaccine has not been covered by medical insurance policy in most regions.46 Considering the advantages of pharmacological therapy and influenza vaccination during stable period, Chinese physicians should provide more information on self-management to COPD patients according to their health status in routine clinical practice. And we suggest the coverage of outpatient COPD therapy and influenza vaccination in medical insurance to prevent poor outcomes among COPD patients.
During hospitalization, almost all subjects received pharmacological treatments. Antibiotics was prescribed to more than 90% subjects and no significant difference was found across hospital categories. However, a systematic review reported that the effect of antibiotics on AECOPD patients remained controversial.47 Identifying the subgroup of patients which could benefit from antibiotics would be meaningful for preventing antibiotics abuse at the same time of ensuring treatment effect. For example, C-reactive protein, procalcitonin or clinical symptoms have previously been explored to guide antibiotics prescription.48–50 However, data on Chinese AECOPD population were generally limited and with small sample sizes. For corticosteroids usage, the average daily and total dosage among subjects using systemic corticosteroids were slightly higher than those recommended in GOLD guideline regardless of hospital category. However, the evidence in current guideline was based on data from European population.1 Further studies were required to explore the optimal dosage of systemic corticosteroid in Chinese population. Respiratory support is recommended by the GOLD guideline for treatment of AECOPD inpatients.1 Although subjects’ status was similar regarding arterial blood gas results across hospital categories, we found that the respiratory support was used much less in the tertiary TCM hospitals, and most likely to be applied in the tertiary general hospitals. Physicians in TCM hospitals may have different treatment habits compared to those in general hospitals. However, the awareness and skills of applying respiratory support should be improved in Chinese physicians from tertiary TCM hospitals.
The prognoses of Chinese AECOPD inpatients were well regarding in-hospital clinical outcomes, suggesting that treatment during hospitalization was effective. The in-hospital mortality was only 0.1% in our study, which was significantly lower than that in the US.15,47 However, we should take care whether there was a wasting of resources. For example, some patients could visit a lower level of hospital to save medical resources under the policy of establishing a hierarchical medical system. In our study, the median total direct cost of this hospitalization was 1424.3 US dollars, accounting for 13.7% of the per capita gross national income in 2019 (10,410 US dollars).39 We observed that the total direct cost was the lowest among patients admitting the secondary hospitals, whereas no difference of in-hospital mortality was found across hospital categories. As for the recovery of symptoms, the decreases of CAT score among patients admitted in all kinds of hospitals exceeded the minimum clinically important difference, implying that AECOPD patients could receive adequate treatment in any kind of hospitals. In addition, although effectiveness of AECOPD treatment was achieved, we still need to consider if the treatment could be more specific to patients’ clinical features to reduce side effects and alleviate burden of patients, especially for patients with comorbidities.
Our study had several strengths including: (a) We utilized the data from ACURE, which is the first and largest registry of patients hospitalized for AECOPD in real-world China. Therefore, the sample size of our study is large, and covers a wide range of AECOPD patients including those aged 20–39 years. (b) Our study provides extensive description for characteristics, disease management and in-hospital outcomes of this population, which gives a comprehensive overview of the natural course of in-hospital AECOPD patients in China. Besides the strengths listed above, our study also had several limitations. First, the spirometry data were incomplete during hospitalization since lung function test is not recommended for these patients. However, we recorded information of patients with suspected AECOPD at admission after informed consent acquisition. Spirometry data at stable status before hospitalization or during follow-ups were allowed to be used as a substitution and for further confirmation of AECOPD diagnoses. Second, the ACURE only collected the frequency of severe AECOPD in the past year without moderate exacerbation history, so we were unable to assess the GOLD ABCD classifications among patients, which is useful for guiding therapy. However, the occurrences of moderate and severe acute exacerbations were prospectively recorded during follow-ups. And the consistency of clinical practice with the GOLD recommendation could be assessed in the future. Third, we only evaluated in-hospital clinical outcomes in current analysis, because the ACURE study is still ongoing and many subjects have not completed follow-ups. Outcomes after discharge will be evaluated in the future.
Conclusion
Clinical features of Chinese AECOPD inpatients were different from those of other populations. In real-world China, the clinical management during stable period was unsatisfied, whereas therapy during hospitalization was effective regarding in-hospital clinical outcomes regardless of hospital category. Subgroup of patients which could benefit from each specific treatment and features associated with the necessity of visiting a higher level of hospital should be further explored to optimize medical resources and reduce clinical burden of Chinese AECOPD inpatients.
Data Sharing Statement
The datasets analyzed in the current study will be available from the corresponding author on reasonable request after the completion of ACURE.
Acknowledgments
The authors thank all participants, staff and investigators involved in the ACURE from all participating sites for their efforts in providing and collecting the data used in this study.
Author Contributions
C. Liang had full access to all of the data in this study, conceived the analysis, and takes responsibility for the integrity and the accuracy of analysis. Concept and design: C. Liang, H. Niu, F. Dong, Y. Chen, Kewu Huang, Q. Zhan, T. Yang, C. Wang; Data collection and management: C. Liang, X. Mao, Ke Huang, H. Niu, F. Dong, Y. Chen, Kewu Huang, Q. Zhan, Y. Huang, Y. Zhang, T. Yang, C. Wang; Statistical analysis: C. Liang, X. Mao, Y. Zhang; Drafting of the manuscript: C. Liang; Clinical interpretation of results, critical revision of manuscript for intellectual content, agreement on the journal to which the manuscript being submitted, approval of the final manuscript to be submitted, and agreement to be accountable for the contents of the manuscript: all authors.
Disclosure
The authors report no conflicts of interest in this work. The ACURE study is funded by the Chinese Academy of Medical Sciences, basic scientific research business fee fund of central level public welfare scientific research institutes-Research on Prevention and Control System of Chronic Airway Diseases (grant number 2019TX320005), National Key R&D Program of China (grant number 2016YFC1303900, 2016YFC1304300), CAMS Innovation Fund for Medical Sciences (CIFMS) (grant number 2018-I2M-1-001). The funders of the study had no role in study design, data collection and management, data analysis, data interpretation, writing of the manuscript, and the decision to submit the manuscript for publication.
References
1. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2020report). Global Initiative for Chronic Obstructive Lung Disease (GOLD) Committees. Available from: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf.
2. Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
4. Fang X, Wang X, Bai C. COPD in China: the burden and importance of proper management. Chest. 2011;139(4):920–929. doi:10.1378/chest.10-1393
5. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2017 report). Global initiative for Chronic Obstructive Lung Disease (GOLD) Committees. .https://goldcopd.org/wp-content/uploads/2017/02/wms-GOLD-2017-FINAL.pdf.
6. O’Donnell DE, Aaron S, Bourbeau J, et al. State of the Art Compendium: Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease. Can Respir J. 2004;11(Suppl B):7b–59b. doi:10.1155/2004/946769
7. Simoens S. The economic burden of COPD exacerbations. COPD. 2010;7(3):159–161. doi:10.3109/15412555.2010.485098
8. Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5):1418–1422. doi:10.1164/ajrccm.157.5.9709032
9. Donaldson GC. COPD exacerbations {middle dot} 1: epidemiology. Thorax. 2006;61(2):164–168. doi:10.1136/thx.2005.041806
10. Tesfaigzi Y, Meek P, Lareau S. Exacerbations of chronic obstructive pulmonary disease and chronic mucus hypersecretion. Clin Appl Immunol Rev. 2006;6(1):21–36. doi:10.1016/j.cair.2006.02.001
11. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–1613. doi:10.1164/ajrccm.161.5.9908022
12. Berkius J, Nolin T, Mardh C, Karlstrom G, Walther SM. Characteristics and long-term outcome of acute exacerbations in chronic obstructive pulmonary disease: an analysis of cases in the Swedish Intensive Care Registry during 2002–2006. Acta Anaesthesiol Scand. 2008;52(6):759–765. doi:10.1111/j.1399-6576.2008.01632.x
13. Kobayashi S, Hanagama M, Ishida M, et al. Clinical characteristics and outcomes in Japanese patients with COPD according to the 2017 GOLD classification: the Ishinomaki COPD Network Registry. Int J Chron Obstruct Pulmon Dis. 2018;13:3947–3955. doi:10.2147/COPD.S182905
14. Abadias Medrano MJ, Yuguero Torres O, Bardes Robles I, Casas-Mendez LF, Barbe F, de Batlle J. Exacerbations of chronic obstructive pulmonary disease: an analysis of the care process in a regional hospital emergency department. Medicine. 2018;97(31):e11601. doi:10.1097/MD.0000000000011601
15. Tabak YP, Sun X, Johannes RS, Gupta V, Shorr AF. Mortality and need for mechanical ventilation in acute exacerbations of chronic obstructive pulmonary disease: development and validation of a simple risk score. Arch Intern Med. 2009;169(17):1595–1602. doi:10.1001/archinternmed.2009.270
16. Molinari N, Chanez P, Roche N, Ahmed E, Vachier I, Bourdin A. Rising total costs and mortality rates associated with admissions due to COPD exacerbations. Respir Res. 2016;17(1):149. doi:10.1186/s12931-016-0469-6
17. Breyer-Kohansal R, Hartl S, Breyer M-K, et al. The European COPD audit: adherence to guidelines, readmission risk and hospital care for acute exacerbations in Austria. Wien Klin Wochenschr. 2019;131(5–6):97–103. doi:10.1007/s00508-019-1441-5
18. Li X, Huang J, Zhang H. An analysis of hospital preparedness capacity for public health emergency in four regions of China: beijing, Shandong, Guangxi, and Hainan. BMC Public Health. 2008;8(1):319. doi:10.1186/1471-2458-8-319
19. Pei Z, Sun Y, Wang S, et al. Estimating mortality among inpatients with acute exacerbation of chronic obstructive pulmonary disease using registry data. NPJ Prim Care Respir Med. 2020;30(1):28. doi:10.1038/s41533-020-0186-y
20. Gu D, Kelly TN, Wu X, et al. Mortality attributable to smoking in China. N Engl J Med. 2009;360(2):150–159. doi:10.1056/NEJMsa0802902
21. Jones PW, Harding G, Berry P, Wiklund I, Chen W-H, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
22. Kon SSC, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. doi:10.1016/S2213-2600(14)70001-3
23. Wan ES, Qiu W, Baccarelli A, et al. Systemic steroid exposure is associated with differential methylation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(12):1248–1255. doi:10.1164/rccm.201207-1280OC
24. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
25. Clinic M COPD diagnosis and treatment. Mayo Clinic. Available form: https://www.mayoclinic.org/diseases-conditions/copd/diagnosis-treatment/drc-20353685.
26. Zhang J, Ou J-X, Bai C-X. Tobacco smoking in China: prevalence, disease burden, challenges and future strategies. Respirology. 2011;16(8):1165–1172. doi:10.1111/j.1440-1843.2011.02062.x
27. Esteban C, Castro-Acosta A, Alvarez-Martinez CJ, Capelastegui A, Lopez-Campos JL, Pozo-Rodriguez F. Predictors of one-year mortality after hospitalization for an exacerbation of COPD. BMC Pulm Med. 2018;18(1):18. doi:10.1186/s12890-018-0574-z
28. Arkhipov V, Arkhipova D, Miravitlles M, Lazarev A, Stukalina E. Characteristics of COPD patients according to GOLD classification and clinical phenotypes in the Russian Federation: the SUPPORT trial. Int J Chron Obstruct Pulmon Dis. 2017;12:3255–3262. doi:10.2147/COPD.S142997
29. Li X, Wu Z, Xue M, Du W. Smoking status affects clinical characteristics and disease course of acute exacerbation of chronic obstructive pulmonary disease: a prospectively observational study. Chronic Respir Dis. 2020;17:1479973120916184. doi:10.1177/1479973120916184
30. Xu F, Yin X, Shen H, Xu Y, Ware RS, Owen N. Better understanding the influence of cigarette smoking and indoor air pollution on chronic obstructive pulmonary disease: a case–control study in Mainland China. Respirology. 2007;12(6):891–897. doi:10.1111/j.1440-1843.2007.01178.x
31. Halbert RJ, Isonaka S, George D, Iqbal IA. Interpreting COPD prevalence estimates. Chest. 2003;123(5):1684–1692. doi:10.1378/chest.123.5.1684
32. Gaude GS, Bp R, Chaudhury A, Hattiholi J. Outcomes associated with acute exacerbations of chronic obstructive pulmonary disorder requiring hospitalization. Lung India. 2015;32(5):465–472. doi:10.4103/0970-2113.164150
33. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC
34. Johansson G, Mushnikov V, Backstrom T, et al. Exacerbations and healthcare resource utilization among COPD patients in a Swedish registry-based nation-wide study. BMC Pulm Med. 2018;18(1):17. doi:10.1186/s12890-018-0573-0
35. Cao Z, Ong KC, Eng P, Tan WC, Ng TP. Frequent hospital readmissions for acute exacerbation of COPD and their associated factors. Respirology. 2006;11(2):188–195. doi:10.1111/j.1440-1843.2006.00819.x
36. Cavaillès A, Brinchault-Rabin G, Dixmier A, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–475. doi:10.1183/09059180.00008612
37. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
38. Xu Z, Zhao Z. Suggestions of including COPD into the scope of chronic disease outpatient reimbursement for residents’ medical insurance. Unity. 2018;216(03):60.
39. Statistics N The per capita disposable income in China. National Bureau of Statistics. Available form: https://data.stats.gov.cn/easyquery.htm?cn=C01.
40. Mereckiene J Seasonal influenza vaccination in Europe - overview of vaccination recommendations and coverage rates in the EU member states for the 2012–2013 influenza season, technical report. Eur Centre Dis Prev Control Web site. Available form: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/Seasonal-influenza-vaccination-Europe-2012-13.pdf.
41. Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015;147(4):894–942. doi:10.1378/chest.14-1676
42. Ciblak MA. Influenza vaccination in Turkey: prevalence of risk groups, current vaccination status, factors influencing vaccine uptake and steps taken to increase vaccination rate. Vaccine. 2013;31(3):518–523. doi:10.1016/j.vaccine.2012.11.022
43. Singapore Moh. MOH clinical practice guidelines 2/2017 chronic obstructive pulmonary disease executive summary. Ministry of health Singapore. Available form: https://www.moh.gov.sg/docs/librariesprovider4/guidelines/copd-cpg-2017_summary-card.pdf.
44. Cerezo Lajas A, Gutiérrez González E, Llorente Parrado C, Puente Maestu L, de Miguel-díez J. Readmission due to exacerbation of COPD: associated factors. Lung. 2018;196(2):185–193. doi:10.1007/s00408-018-0093-y
45. CDC. Flu vaccination coverage, United States, 2014–15 influenza season. Available form: https://www.cdc.gov/flu/pdf/fluvaxview/NFID-coverage-2014-15-final.pdf.
46. Wang Q, Yue N, Zheng M, et al. Influenza vaccination coverage of population and the factors influencing influenza vaccination in mainland China: a meta-analysis. Vaccine. 2018;36(48):7262–7269. doi:10.1016/j.vaccine.2018.10.045
47. Vollenweider DJ, Frei A, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease.. Cochrane Database Syst Rev. 2018;10:Cd010257. doi:10.1002/14651858.CD010257.pub2
48. Butler CC, Gillespie D, White P, et al. C-reactive protein testing to guide antibiotic prescribing for COPD exacerbations. N Engl J Med. 2019;381(2):111–120. doi:10.1056/NEJMoa1803185
49. Cook R, Lyon-Maris J, White A. C reactive protein testing in general practice safely reduces antibiotic use for flare-ups of COPD. BMJ. 2019;367:l5991. doi:10.1136/bmj.l5991
50. Wang J-X, Zhang S-M, Li X-H, Zhang Y, Xu Z-Y, Cao B. Acute exacerbations of chronic obstructive pulmonary disease with low serum procalcitonin values do not benefit from antibiotic treatment: a prospective randomized controlled trial. Int J Infect Dis. 2016;48:40–45. doi:10.1016/j.ijid.2016.04.024
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.