")
Back to Journals » Infection and Drug Resistance » Volume 16
Characteristics and Occurrence Scenarios of Staff Exposed to SARS-CoV-2 Omicron in Shanghai Lingang Fangcang Shelter Hospital, CHINA
Authors Li Z, Liang T, Zhang J, Song G, Leng Y, Qiao L, Zhan Y, Zhang W
Received 11 January 2023
Accepted for publication 16 March 2023
Published 21 March 2023 Volume 2023:16 Pages 1619—1628
DOI https://doi.org/10.2147/IDR.S402282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Zhanjie Li,1,* Tangying Liang,2,* Junji Zhang,3 Ge Song,4 Yinzhi Leng,5 Li Qiao,6 Yiyang Zhan,7 Weihong Zhang1
1Department of Infection Control, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Hematology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Department of Infection Control, Suzhou Municipal Hospital, Suzhou, Jiangsu, People’s Republic of China; 4Department of Infection Control, Changzhou No. 2 People’s Hospital Affiliated to Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 5Department of Infection Control, Nanjing Hospital of Chinese Medicine Affiliated to Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 6Department of Quality Management, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 7Department of Geriatrics, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yiyang Zhan, Department of Geriatrics, The First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Road, Nanjing, 210029, Jiangsu, People’s Republic of China, Tel +86-18912972893, Email [email protected] Weihong Zhang, Department of Infection Control, The First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Road, Nanjing, 210029, Jiangsu, People’s Republic of China, Tel +86-13585108553, Email [email protected]
Objective: To analyze the characteristics and occurrence scenarios of occupational exposure of staff in the Shanghai Lingang Fangcang Shelter Hospital.
Methods: We collected the data of 80 staff with occupational exposure (including doctors, nurses, cleaning, security guards, and maintenance staff) in the Shanghai Lingang Fangcang Shelter Hospital from April 5 to May 20, 2022. The basic information of occupational exposure, factors influencing different occupational exposure types, ways to discover occupational exposure, discovery places of occupational exposure, and specific occurrence scenarios were compiled and analyzed among these data.
Results: Occupational exposure mainly occurred in nurses (37, 46.25%), and cleaning (21, 26.25%). After the occurrence of occupational exposure, 20 staff (25%) did not know the occurrence time. Moreover, occupational exposure types were listed from high to low proportion as follows: broken protective clothing (56, 70%), mask loosening or displacement (13, 16.25%), skin exposure (6, 7.5%), and sharp object injuries (5, 6.25%). Occupational exposure was discovered mainly through self-discovery (56, 70%), while other discovery ways were majorly colleague discovery (12, 15%) and infection control supervisor discovery (12, 15%). Furthermore, occupational exposure was discovered principally in the public area (53.75%) and the office area (25%) of the cabin, but the proportion of mask loosening or displacement (38.46%) and skin exposure (50%) was also high in the first unloading area. Broken protective clothing occurred in the following scenarios: scratching while working in the cabin (37, 66.07%) and not knowing its occurrence time (25%). The occurrence scenarios of mask loosening or displacement were mainly not knowing its occurrence time (6, 46.15%), self-discovery (3, 23.08%), and at the time of removal (3, 23.08%).
Conclusion: Targeted training and prevention of occupational exposure should be performed to decrease infection risk and ensure staff safety in Fangcang shelter hospitals.
Keywords: Fangcang shelter hospital, occupational exposure, characteristics, scenarios, SARS-CoV-2 Omicron
Introduction
Since the first detection in South Africa in November 2021, the Omicron variant of novel Coronavirus Disease 2019 (COVID-19) has spread rapidly across the world and replaced the Delta variant to be the dominant mutant strain.1,2 Starting from March 2022, the Omicron-dominant COVID-19 epidemic has spread in Shanghai, causing enormous challenges to the control of the epidemic in Shanghai.3 Fangcang shelter hospitals can greatly reduce the risk of intra-household and community transmission by admitting a large number of asymptomatic and mild COVID-19 patients,4 which is one of the key measures to control the epidemic in Wuhan5 and Shanghai, China. Nevertheless, fangcang shelter hospitals are mostly simply built by converting single, enclosed, and large-scale buildings such as exhibition halls, stadiums, and large warehouses. Therefore, relative to general hospitals or infectious disease hospitals, fangcang shelter hospitals are characterized by short construction periods, simple facilities and equipment, complex environments, and numerous staff and admitted patients.6 Moreover, the variety of staff increases in fangcang shelter hospitals because plenty of cleaning, security guards, and maintenance staff are required in addition to doctors and nurses.7 In these contexts, there is more uncertainty about the occurrence of occupational exposure in fangcang shelter hospitals.
Due to the magnitude and the complexity of COVID-19 management, it poses a significant challenge to clinical treatment and care pathways. Under these circumstances, many medical professionals go to work with psychological and physical barriers, and the risk of occupational exposure is greatly increased.8 Effective prevention of occupational exposure of medical staff is the key to maintaining the endurance of medical treatment.9 During the COVID-19 prevention and control period, studies related to occupational exposure have mainly focused on medical workers who have been infected with COVID-19.10,11 However, some high-risk operations or behaviors that may lead to infection have been ignored. This study retrospectively collated and analyzed the characteristics and occurrence scenarios of 80 cases of occupational exposure (high-risk behaviors that may lead to infection) in a large fangcang shelter hospital during the current Omicron epidemic in Shanghai, with a view to providing a reference for the prevention and control of occupational exposure in other fangcang shelter hospitals.
Methods
Research Subjects
The Shanghai Lingang Fangcang Shelter Hospital consisted of 13 cabins with 13,608 beds, of which 8 cabins with 7308 beds were taken over by the Jiangsu Provincial Aid Shanghai Medical Team during its operation from April 5 to May 20, 2022. Eighty staff that experienced occupational exposure during the takeover of cabins by this team were included as study subjects, including doctors, nurses, cleaning, security guards, and maintenance staff. Inclusion criteria: staff with reported occupational exposures. Exclusion criteria: although reported as occupational exposure, it is not a true occupational exposure.
Research Methods
Occupational exposure refers to exposure to risk factors that may lead to infection.12 It includes the following types: broken protective clothing, mask loosening or displacement, skin exposure, and sharp object injuries (including stab wounds from contaminated or clean sharp objects). It is required to use an online questionnaire system to report occupational exposures, and then have a dedicated person follow up and verify the reported person to rule out false occupational exposures. The details of the staff with ture occupational exposure were collated to analyze the basic information about occupational exposure, factors influencing different occupational exposure types, ways to discover occupational exposure, discovery places, and specific occurrence scenarios.
Occupational Exposure Reporting Process
The Hospital Infection-Control Department of the Jiangsu Provincial Aid Shanghai Medical Team set up a special team for the disposal of occupational exposure and formulated the basic information of occupational exposure reporting (including name, telephone number, cabin, occupation types, and occupational exposure types). In addition, the department designed and produced a two-dimensional code through the “Wen juan xing” (https://www.wjx.cn/newwjx/manage/myquestionnaires.aspx), online questionnaire system which was printed and pasted in protective equipment removal areas. The infection control supervisors (received standardized training) were in charge of scanning the code for filling and reporting. A total of 123 occupational exposures were received for reporting.
Occupational Exposure Screening and Detailed Information Collection
A dedicated person collects the number of reported occupational exposures through the backend of the online system daily, and checks them one by one to filter out the real occupational exposures. A total of 80 personnel who met the definition of occupational exposure were screened from 123 reported personnel. We also designed a detailed questionnaire on occupational exposure using a questionnaire system (including name, age, gender, telephone number, workplace, cabin, occupation types, the first time working in the cabin or not, the occurrence of occupational exposure in the past or not, occupational exposure types, treatment measures, whether to know the occurrence time of the occupational exposure, and a brief description of the specific occurrence scenario of the occupational exposure). Staff who are eligible for occupational exposure are contacted by a dedicated person to collect and check details.
Exposure Pathways
There were three ways to discover occupational exposure: self-discovery, colleague discovery, and infection control supervisor discovery (inspection).
Exposure Sites
Occupational exposure was discovered in four places, including first unloading area, second unloading area, the office area in the cabin (nurse station and treatment room), and the public area in the cabin (other areas in the cabin beside the office area).
Statistical Analysis
Data were organized using WPS2022 software and processed using SPSS 20.0 software. Count data were summarized as number of cases and percentages, and their differences were compared using the χ2 test. p < 0.05 was considered a statistically significant difference. Graphpad 9.0 software was used for plotting.
Results
Basic Information of Occupational Exposure
Among the 80 staff with occupational exposure, 43 (53.75%) were male and 37 (46.25%) were female, with ages of ≤ 30 (39, 48.75%) and 31–40 (33, 41.25%) predominantly. For occupation types, occupational exposure occurred most often in nurses (37, 46.25%) and cleaning (21, 26.25%) and less often in security guards (5, 6.25%) and maintenance staff (4, 5%). In addition, only 2 (2.5%) of the staff with occupational exposure worked in the cabin for the first time, and 20 (25%) did not know the occurrence time of the occupational exposure. Moreover, the proportion of occupational exposure types was listed as follows from high to low: broken protective clothing (56, 70%), mask loosening or displacement (13, 16.25%), skin exposure (6, 7.50%), and sharp object injuries (5, 6.25%). The details are listed in Table 1.
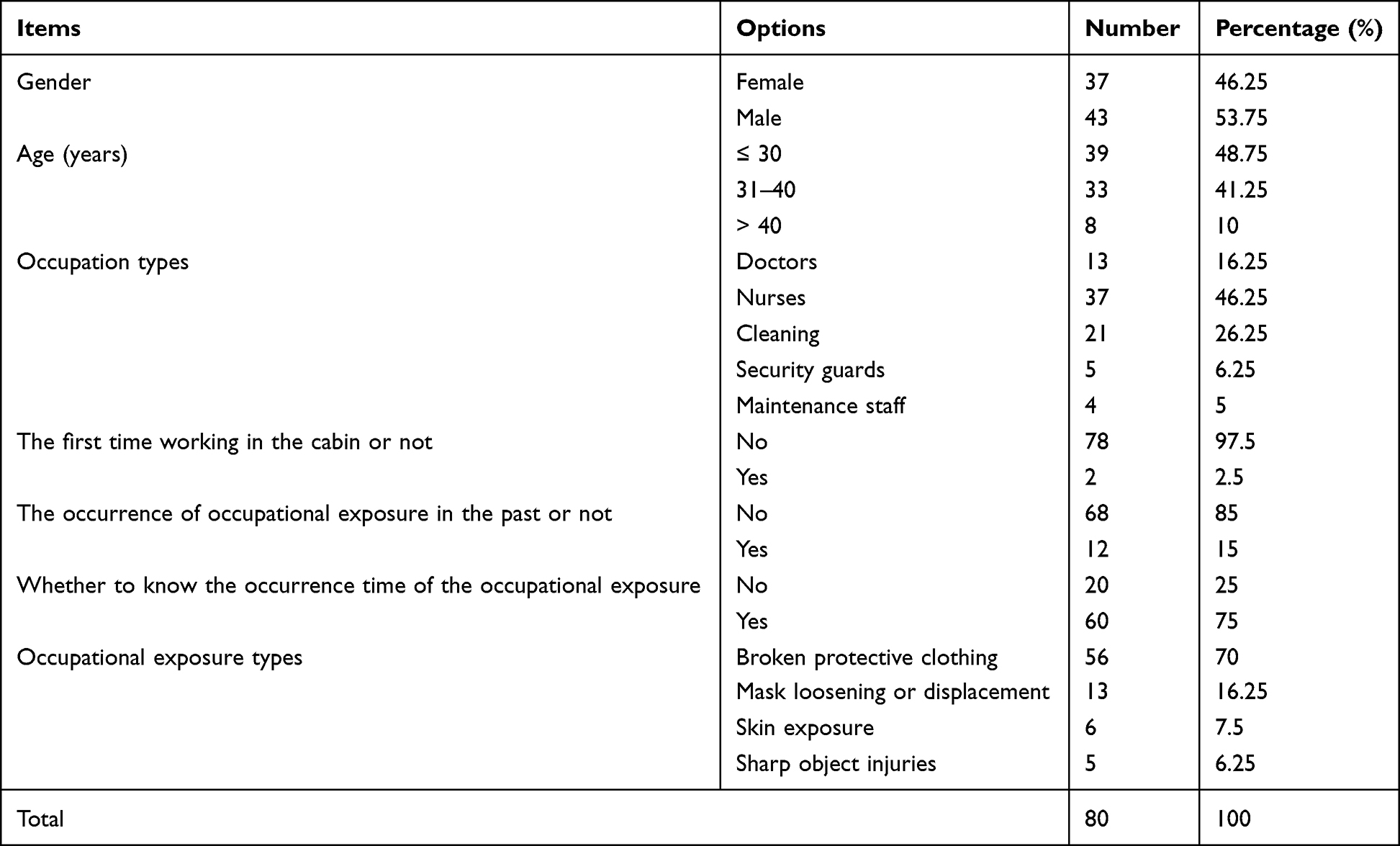 |
Table 1 Basic Information of Occupational Exposure (n = 80) |
Factors Influencing Different Occupational Exposure Types
Gender, age, occupation types, the first time working in the cabin or not, the occurrence of occupational exposure in the past or not, and whether to know the occurrence time of the occupational exposure were not the factors influencing different occupational exposure types, without statistically significant differences (all p > 0.05; Table 2).
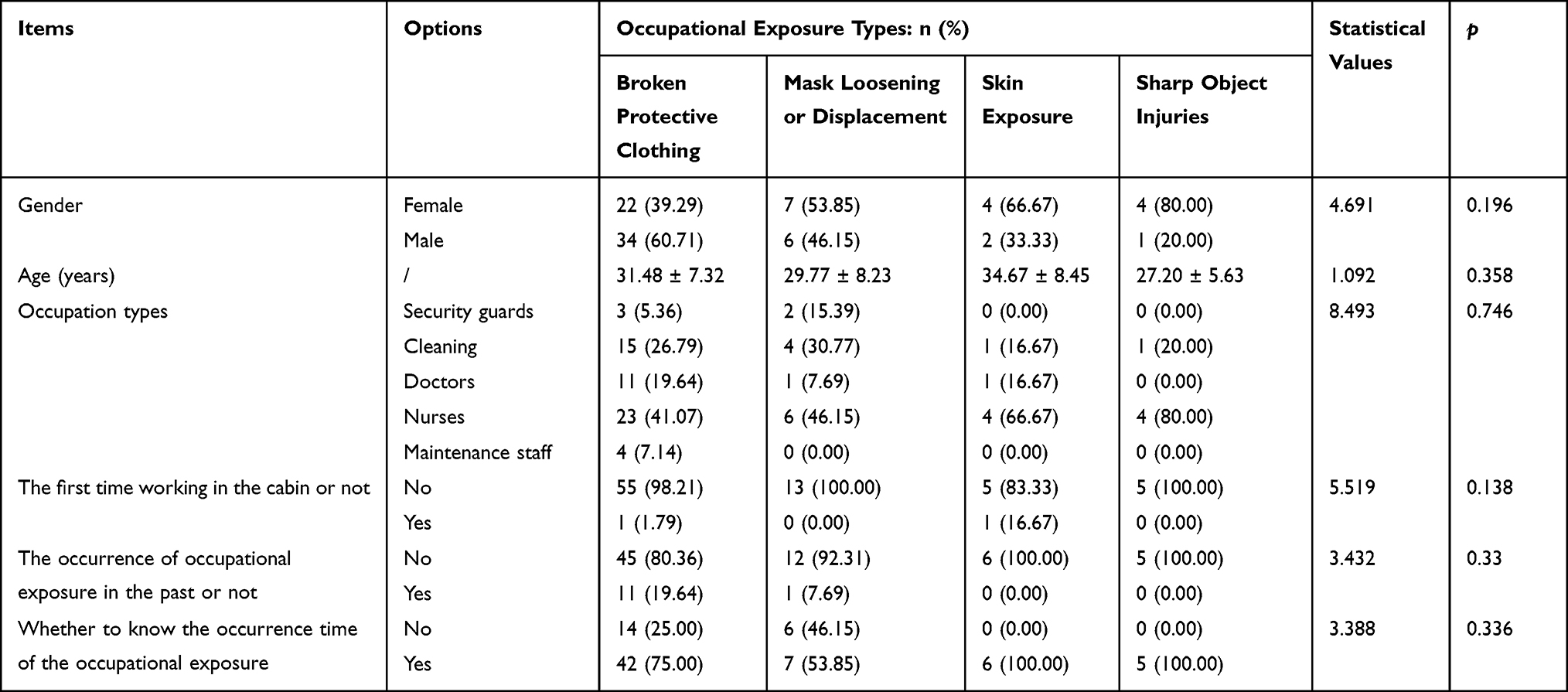 |
Table 2 Factors Influencing Different Occupational Exposure Types |
Discovery Ways of Occupational Exposure
Occupational exposure was majorly discovered via self-discovery (56, 70%), followed by colleague discovery (12, 15%) and infection control supervisor discovery (12, 15%). In detail, skin exposure and sharp object injuries were all discovered through self-discovery, broken protective clothing was principally discovered by the staff themselves (40, 71.43%) and colleagues (12, 21.43%), and mask loosening or displacement was discovered by infection control supervisors (8, 61.54%) and the staff themselves (5, 38.46%) (Figure 1).
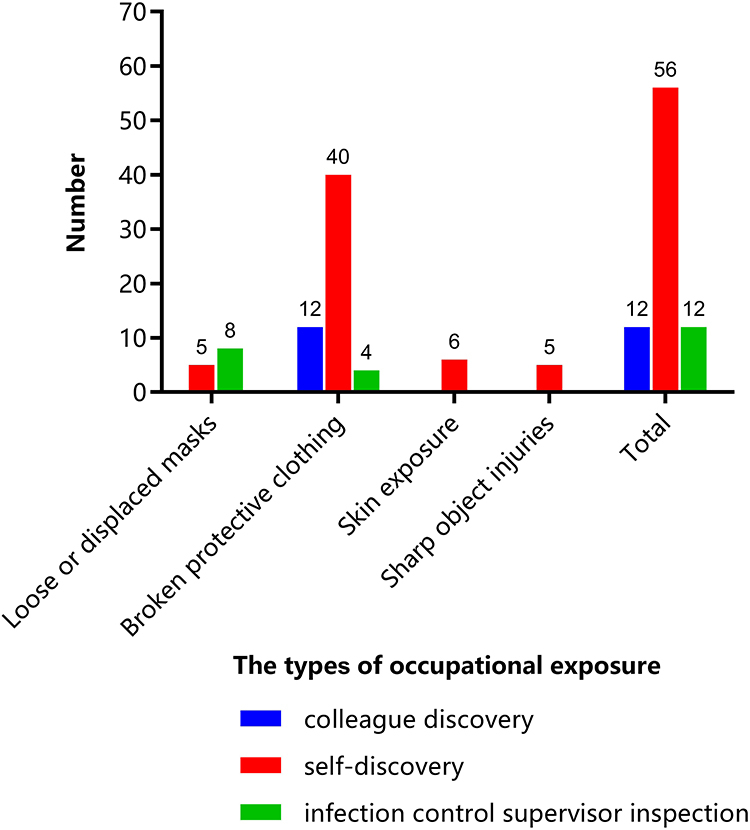 |
Figure 1 Discovery ways of occupational exposure (n = 80). |
Discovery Places of Occupational Exposure
All cases of occupational exposure were mostly discovered in the public area (43, 53.75%) and the office area (22, 25%) of the cabin. Specifically, broken protective clothing was dominantly discovered in the public area (36, 64.29%) and the office area (15, 26.79%) of the cabin. The discovery places of mask loosening or displacement were primarily in the first unloading area (5, 38.46%) and the office area (5, 38.46%) of the cabin. In addition, the discovery places of skin exposure were mainly in the first unloading area (3, 50%) and the public area (2, 33.33%) of the cabin. Likewise, sharp object injuries were chiefly discovered in the public area (2, 40%) and the office area (2, 40%) of the cabin (Figure 2).
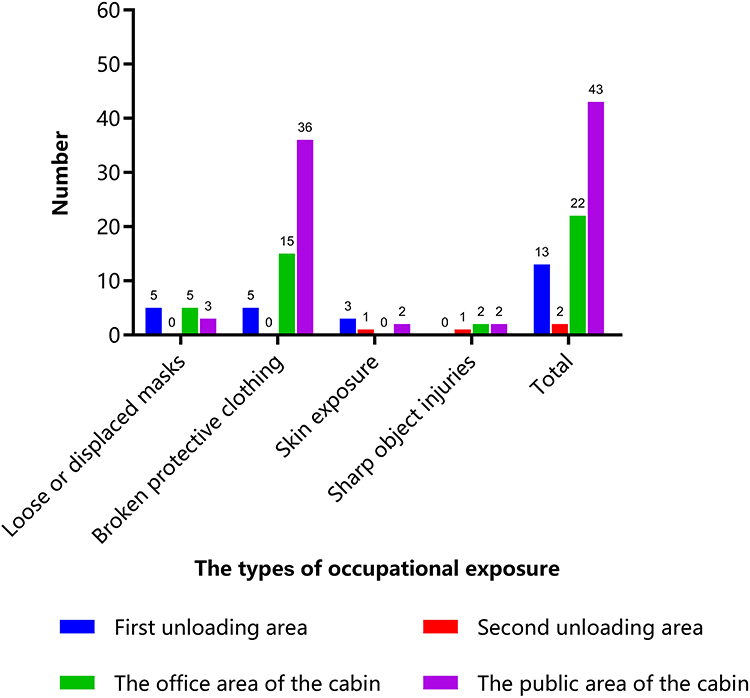 |
Figure 2 Discovery places of occupational exposure (n = 80). |
Specific Occurrence Scenarios of Occupational Exposure
Among occupational exposure, the main occurrence scenario of broken protective clothing was scratching while working in the cabin (37, 66.07%), with 14 subjects (25%) not knowing its occurrence time. With regard to mask loosening or displacement, most often the subjects did not know its occurrence time (6, 46.15%), and some cases were discovered by the subjects themselves (3, 23.08%) and caused at the time of removal in the first unloading area (3, 23.08%). Additionally, skin exposure occurred at the time of removal (3, 50%) and was caused by broken gloves (3, 50%). One of the sharp object injuries (20%) was a needlestick injury (Table 3).
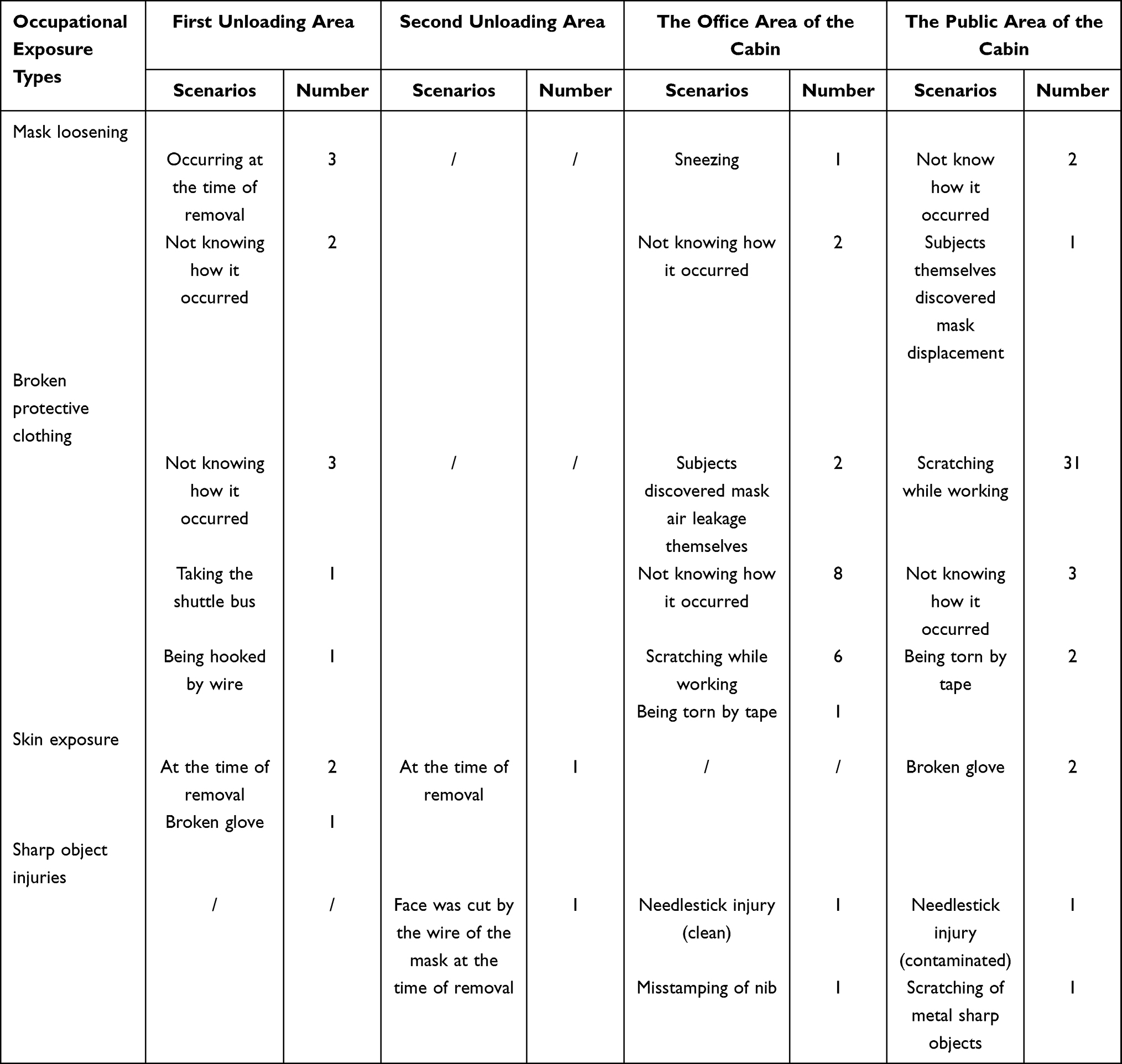 |
Table 3 Specific Scenarios of Occupational Exposure (n = 80) |
Discussion
This study observed that the occupationally exposed staff in the Shanghai Lingang Fangcang Shelter Hospital were dominated by nurses (37, 46.25%) and cleaning (21, 26.25%). Nurses accounted for the largest number of occupational exposure, which is similar to the post distribution of occupational exposure in Wuhan Huoshenshan Hospital in 202013 and in hospitals in daily situations.14 “COVID-19 Fangcang Shelter Hospital Setting Management Specification” (No.22 [2022]) issued by the Joint Prevention and Control Mechanism of the National Health Commission requires fangcang shelter hospitals to be at least equipped with staff at a bed-to-nurse ratio of 1: 0.2 and a doctor-to-nurse ratio of 1: 5, as well as one policeman, two security guards, and one cleaning staff for every bed. Therefore, the maximum number of nurses, the large inspection area of cabins, and the high patient turnover rate are correlated with the most occupational exposure in nurses. In addition, our cabin has a 4-hour shift schedule and a large number of cleaning staff, who need to be engaged in collecting medical waste, cleaning and disinfection, issuing meals, and so on. Nonetheless, the cleaning staff in fangcang shelter hospitals activated in the emergency in this study were recruited temporarily, who lacked general medical knowledge and went on duty after emergency training. In this case, they are lacking in basic knowledge of the mode of transmission of COVID-19, waste disposal, and personal occupational protection skills compared to the cleaning staff in hospitals,15 which may be the principal cause of a higher number of occupational exposure occurring in cleaning. The high number of total cleaning staff and their occupational exposure is a characteristic of large fangcang shelter hospitals, which requires a focus on training and education for this population. Moreover, it was manifested in this research that gender, age, occupation types, and the first time working in the cabin or not were not the factors influencing different occupational exposure types, indicating that there are no exceptions to the occurrence of different occupational exposure types and that all population should strictly implement relevant protective requirements and measures to avoid the occurrence of each occupational exposure type to the greatest extent.
The data of this study elucidated that “self-discovery” was the most frequent way to discover occupational exposure, but “colleague discovery” and “infection control supervisor discovery” were also essential for the discovery of occupational exposure. In particular, the “infection control supervisor discovery” method accounted for 61.54% (8/13) of the cases with the highest risk of mask loosening or displacement, and the “colleague discovery” and “infection control supervisor discovery” methods constituted 28.57% (16/56) among the most common ways to discover broken protective clothing. This reminds us that in fangcang shelter hospitals, it is necessary to raise the awareness of staff for self-examination and early discovery of occupational exposure, as well as to highlight the importance of mutual care among colleagues and regular examination of each other. Of note, the inspection by infection control supervisors can reduce the risk of infection by discovering some occupational exposure early, especially mask loosening or displacement, and intervening as early as possible, which is also an effective way we cannot ignore. Meanwhile, in our study, occupational exposure was discovered mainly in the cabin area. Likewise, a certain proportion (16.25%, 13/80) of occupational exposure, particularly mask loosening and displacement [38.46% (5/13)] and skin exposure [50% (3/6)], was also discovered in the first unloading area, which is mainly attributed to the fact that some masks can be loosened or displaced due to irregularities in the operation or too large movements at the time of removal. Indeed, the removal of protective equipment is more prone to contamination than the wearing of protective equipment. Consequently, special attention is warranted to prevent self-contamination and decrease environmental contamination when contaminated protective equipment is removed.16 In the actual work of fangcang shelter hospitals, it was noted that some security guards and cleaning staff wore multiple boot covers or wrapped several loops of tape around their bodies, resulting in deformed movements, prolonged removal time, and increased risk of the occupation during the removal process. Field research on the clinical treatment of COVID-19 patients disclosed that plenty of staff attached special importance to the process of wearing because they believed that the more layers, the thicker, and the tighter they wore, the better. Nevertheless, scientific protection actually emphasizes fitness rather than number the most.16
Of the occurrence scenarios of occupational exposure in this study, 20 cases (25%) were unaware of when and how occupational exposure occurred, concentrating on subjects with broken protective clothing (14, 17.50%) and mask loosening or displacement (6, 7.50%). When discovered, the subjects might be exposed to the hazardous environment for a period of time and the risk of exposure is undoubtedly greater with mask displacement. Accordingly, self-examination, mutual examination, and inspection should be strengthened in terms of frequency and intensity, thus discovering occupational exposure as early as possible and promptly dealing with them. In addition to the case of not knowing the occurrence time, mask loosening and displacement among occupational exposure mainly resulted from forward sliding of the over-The-head strap of masks at the time of removal and self-discovery of mask displacement or air leakage in the cabin. Hence, it is suggested that staff must strictly check whether the mask elastic band is tightened and conduct the tightness test when wearing a mask, as well as pay close attention to masks for any abnormalities. Furthermore, when working in the cabin, staff should take notice of the range of head and face, avoid talking loudly, and reduce the frequency of speaking. Broken protective clothing was majorly triggered by scratches for various reasons under working conditions and worn-out soles of protective clothing by being soaked during walking due to too wet ground caused by rain leakage on rainy days or too much disinfectant, which is concurrent with the findings of related research in isolation wards.17 Because the cabin space is relatively large and there are a large number of beds, transfer vehicles, equipment, and so on, it should be emphasized to staff to move slowly and steadily to minimize the scratch of protective clothing, as well as make an emergency plan for rainy days. Meanwhile, disinfection frequency should also not be too intensive, and the blower can be utilized to relieve the ground humidity if necessary. There were three dominant skin exposure scenarios: broken gloves (3, 50%), the touching of skin by the outside of the protective clothing during the removal in the first unloading area (2, 40%), and the touching of face by the outside of the mask during the removal in the second unloading area (1, 10%), which is similar to common causes of skin exposure in isolation wards.18 Previous research19,20 reported the monitoring of environmental contamination during hospitalization of patients with sars-cov-2 infection and suggested that surface contamination might be one of the main routes of sars-cov-2 transmission. Moreover, another study21 sampled the protective equipment of medical staff in isolation wards and detected positive specimens, illustrating that it is still unrelenting to repeatedly strengthen training and assessment on donning and doffing protective equipment to reduce the risk of cross-infection. Among the five cases of sharp object injuries, only one case was stabbed by a needle after measuring the blood glucose of patients, and the remaining four cases were poked or scratched during non-contact with patients, which is clearly different from the sharp object injuries in the daily work of ordinary medical institutions22 and also reflects the characteristics of fangcang shelter hospitals. In brief, in the cabin, doctors and nurses also need to carry supplies, distribute box lunches, and dismantle and pack in addition to a small number of diagnostic and treatment operations. This indicates that in fangcang shelter hospitals, staff also need to pay attention to their own safety in addition to ensuring medical safety.
In the face of a public health emergency or even a pandemic, occupational exposure is the main factor that causes the number of medical staff to plummet, as many are quarantined for safety reasons even if no infection occurs at the time.23,24 This study summarizes the distribution and characteristics of occupational exposures of staff during the emergency activation of a temporary square-cabin hospital for the treatment of patients with high infectiousness. It also introduces the working model and experience that can detect and intercept the risk of occupational exposure early, which can provide guidance for similar situations encountered again in the future. This is a very good addition. This study has some limitations, it mainly reflects the occupational exposure characteristics and occurrence scenarios of large square cabin hospitals that are temporarily set up. Medical institutions as well as small medical sites may have different occupational exposure characteristics and need to respond flexibly with specific situations.
Conclusions
In summary, occupational exposure mainly occurs in nurses and cleaning in fangcang shelter hospitals. Additionally, “self-discovery” is the most common discovery route, whereas “colleague discovery” and “infection control supervisor discovery” are also crucial, especially for the highest risk of mask loosening or displacement. The discovery place is mainly inside the cabin and in the first unloading area. For the occurrence scenario, there is less occupational exposure caused by clinical operations but more occupational exposure attributable to factors such as the unawareness of the occurrence time, irregular removal of protective equipment, and other non-clinical operations. As a consequence, targeted training and prevention of occupational exposure should be conducted based on the inherent characteristics of occupational exposure in fangcang shelter hospitals to reduce the risk of infection and ensure staff safety.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The First Affiliated Hospital of Nanjing Medical University approved this study.(Ethic number: 2022-SR-315). All methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from the study participants.
Acknowledgment
We would like to acknowledge the reviewers for their helpful comments on this paper. Zhanjie Li and Tangying Liang are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by The third Outstanding Young and Middle-aged Talents Training Program of Jiangsu Provincial People’s Hospital (YNRCQN0314); Young Scholars Fostering Fund of the First Affiliated Hospital of Nanjing Medical University (PY2022017).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Cai J, Deng X, Yang J, et al. Modeling transmission of SARS-CoV-2 Omicron in China. Nat Med. 2022;28(7):1468–1475. doi:10.1038/s41591-022-01855-7
2. Viana R, Moyo S, Amoako DG, et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in Southern Africa. Nature. 2022;603:679–686. doi:10.1038/s41586-022-04411-y
3. Lin JS, Teng XY, Cao Q, Tang J, Ma EX, Chen EZ. Research on the construction and application of information system in large-scale fangcang shelter hospital under COVID-19. J Jinan Univ. 2022;2022:1–7.
4. Wang X, Fang J, Zhu Y, et al. Clinical characteristics of non-critically ill patients with novel coronavirus infection (COVID-19) in a Fangcang Hospital. Clin Microbiol Infect. 2020;26:1063–1068. doi:10.1016/j.cmi.2020.03.032
5. Pan A, Liu L, Wang C, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. 2020;323:1915–1923. doi:10.1001/jama.2020.6130
6. Li LY, Ye Q, Cai M, et al. Expert consensus on prevention and control of infection in makeshift hospitals. Chin J Nosocomiol. 2022;32:1–10.
7. Zhang M, Wang L, Yu S, Sun G, Lei H, Wu W. Status of occupational protection in the COVID-19 Fangcang Shelter Hospital in Wuhan, China. Emerg Microbes Infect. 2020;9:1835–1842. doi:10.1080/22221751.2020.1803145
8. Capalbo C, Aceti A, Simmaco M, et al. The exponential phase of the Covid-19 pandemic in central Italy: an integrated care pathway. Int J Environ Res Public Health. 2020;17(11):3792. doi:10.3390/ijerph17113792
9. Gao HM, Tian LY, Li L, et al. Questionnaire survey on occupational exposure of health care workers working in COVID-19 isolation wards of designated hospitals in 2020. Chin J Nosocomiol. 2020;30:3219–3223.
10. Li G, Hu C, He Q, Liu J, Xiong N, Wang H. Apparent and occult infections of medical staff in a COVID-19 designated hospital. J Infect Public Health. 2020;13(10):1453–1455. doi:10.1016/j.jiph.2020.07.005
11. Al Maskari Z, Al Blushi A, Khamis F, et al. Characteristics of healthcare workers infected with COVID-19: a cross-sectional observational study. Int J Infect Dis. 2021;102:32–36. doi:10.1016/j.ijid.2020.10.009
12. Chunhui L, Xun H, Gadfly C, et al. Expert consensus on personal protection in different regional workplaces of medical institutions during the new crown pneumonia epidemic. Chin J Infect Control. 2020;19(03):199–213.
13. Yu LC, Wang JX, Chen W, et al. Patterns and practice management of occupational exposure of medical staffs in coronavirus disease 2019 isolation wards. ChiN J Infect Dis. 2020;38:761–766.
14. Peng LL, Liu CL, Zhang WP, et al. Investigation on blood-borne occupational exposure of medical staff in 30 hospitals of a Province from 2019 to 2020. Chin J Nosocomiol. 2022;32:1239–1242.
15. Wei CL, Yuan JX, Wang H, Pu ZS. Investigation of the awareness of cleaning staff of hospitals about the knowledge of COVID-19. Chin J Disinfect. 2021;07:559–560.
16. Fu Q, Zhang XY, Li SW. Strategies for risk management of medical staff’s occupational exposure to COVID-19. Chin J Nosocomiol. 2020;30:801–805.
17. Wang YW, Huang X, Zeng LM, et al. Health care workers’ occupational exposure related to the treatment of COVID-19. Chin J Infect Control. 2020;19:1082–1087.
18. Cao Q, Cui FH, Han Y, Su JZ. Analysis of risk factors for occupational exposure to COVID-19 in 27 medical staff. J Prevent Med Chin People’s Lib Army. 2020;38:100–102.
19. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;323:1610–1612. doi:10.1001/jama.2020.3227
20. Cheng VCC, Wong SC, Chen JHK, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. 2020;41:493–498. doi:10.1017/ice.2020.58
21. Song ZG, Chen YM, Wu F, et al. Identifying the risk of SARS-CoV-2 infection and environmental monitoring in Airborne Infectious Isolation Rooms (AIIRs). Virol Sin. 2020;35:785–792. doi:10.1007/s12250-020-00301-7
22. Tang ZY, Wu AH, Huang X, et al. Infectious occupational exposure of medical staff in Xiangya Hospital. Chin J Nosocomiol. 2020;30(18):2864–2868.
23. Maltezou HC, Dedoukou X, Tseroni M, et al. SARS-CoV-2 Infection in healthcare personnel with high-risk occupational exposure: evaluation of 7-day exclusion from work policy. Clin Infect Dis. 2020;71(12):3182–3187. doi:10.1093/cid/ciaa888
24. Liu H, Wang Y, He HY, et al. Experience of comprehensive interventions in reducing occupational exposure to COVID-19. J Infect Public Health. 2021;14(2):201–205. doi:10.1016/j.jiph.2020.12.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.